| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 174 |
| Yesterday: | 251 |
| This Week: | 174 |
| Last Week: | 2221 |
| This Month: | 4762 |
| Last Month: | 6796 |
| Total: | 129361 |
Chapter 7 The Association of Marihuana Smoking With Opiate Addiction
 |
|  |
| 
| Books - Epidemiology of Opiate Addiction in United States |
Drug Abuse
The Epidemiology of Opiate Addiction in the United States
Chapter 7
The Association of Marihuana Smoking With Opiate Addiction
JOHN G BALL, CARL D. CHAMBERS, AND MARION J. BALL
Note: Reprinted fromThe Journal of Criminal Law, Criminology and Police Science, 59:171-182, 1988.
The question has been repeatedly raised as to whether the smoking of marihuana cigarettes leads to opiate addiction in the United States.' Extreme viewpoints have been advanced. Marihuana use has been viewed as an insidious and invariant precursor of opiate addiction and enslavement= Conversely, it has been regardeZ1 as an innocuous narcotic with beneficial social qualities.$ These extreme positions may now be dismissed as polemical statements without substantiation.4 Still, the question remains: To what extent and under what conditions is marihuana smoking associated with a subsequent addiction to opiates?
The logical possibilities with respect to the association of marihuana and opiate drugs may be depicted as shown in Figure 7-1.
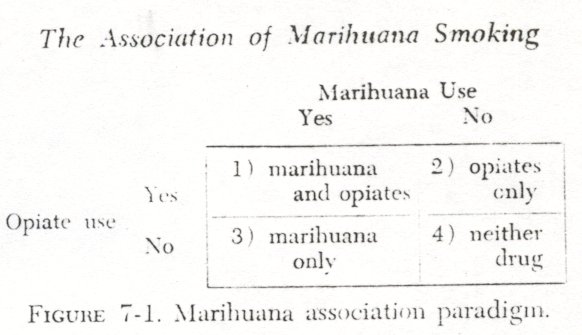
Box 1 includes users of both marihuana and opiates; Box 2 those who use opiates but not marihuana; Box 3 those who only use marihuana; and Box 4 consists of those who use neither marihuana nor opiates. The nondrug using population-the normal or control comparison-is found in Box 4 which, presumably, includes the major portion of the United States population. The question of association involves Boxes 1, 2, and 3. The opiate only category, Box 2, is relevant, as it indicates no association between marihuana and opiates, as does Box 3, the marihuana only category. Thus, a positive association is found only in Box ï,
There are two principal ways of considering the association of marihuana and opiate use. The first is an epidemiological or community approach: to determine the prevalence of marihuana use in a given population, such as a city or state, and then to record the prevalence of opiate use within the marihuana group as well as in the population selected. This community-based approach has been effectively employed in St. Louis by Robins and Murphy.' It is pertinent to note that such epidemiological studies take a broad view of the question from the community level to the target subjects-the telescope is focused upon the community.
The second general approach in considering the association of marihuana and opiate use is to focus upon the target subjects themselves, to start with the positive association. This has been a traditional method in both medicine and sociology: to study the clinical disease state or the deviant individual. In the present study this second approach is employed. Analysis of a national sample of opiate addicts was undertaken in order to ascertain whether or not marihuana smoking was associated with their addiction-the telescope was focused upon the target subjects.
Because of the current interest in the topic of marihuana use in the United States and the concomitant confusion as to popular versus scientific sources of data, it may be pertinent to state explicitly the scope and purpose of this paper. The precise research question under investigation is: Given existing social conditions and laws, is the smoking of marihuana in the United States associated with die subsequent use of opiate drugs? If so, under what conditions? If not, under what conditions?
Subjects and Source of Data
The subjects were 2,213 addict patients admitted to the Lexington and Fort Worth hospitals during 1965. The 2,213 addicts included both voluntary admissions and federal prisoners, males and females, Negroes and whites, laborers and housewives, prostitutes and physicians, lawyers and forgers, and drug sellers as well as users. Forty-six of the fifty states were represented, and the range in age was from sixteen to seventy-five years. In sum, this hospitalized population reflects the diverse subgroups which comprise the universe of known opiate addicts in the United States.
The principal source of data was the admission summary sheet completed by a clerk at the time each patient enters the hospital. Further information was available from patients' medical records; this included a medical history, current drug diagnosis, psychiatric diagnosis, employment experiences, criminal history, family relationships, educational records, and other varied clinical and administrative documents. An extended interview was conducted with 337 of the subjects at the Lexington hospital in 1965 to secure additional information related to drug use. From these interviews a reliability check of the admission data was undertaken.
Early in 1965 additional information with respect to marihuana use, age at first arrest, and age at first opiate use became available on all new admissions to the two federal hospitals. Specifically, each patient «vas asked (a ) whether he had ever used marihuana, ( b ) at what age he was first arrested, (c) at what age he first used opiates, (d) present drug used, (e) method of administration, and (f) from whom drugs were obtained. The present study is focused upon an analysis of these six items from the revised admission summary sheet, although reference is made to other sources of data as seems appropriate.
The Distribution of Marihuana Use in the United States
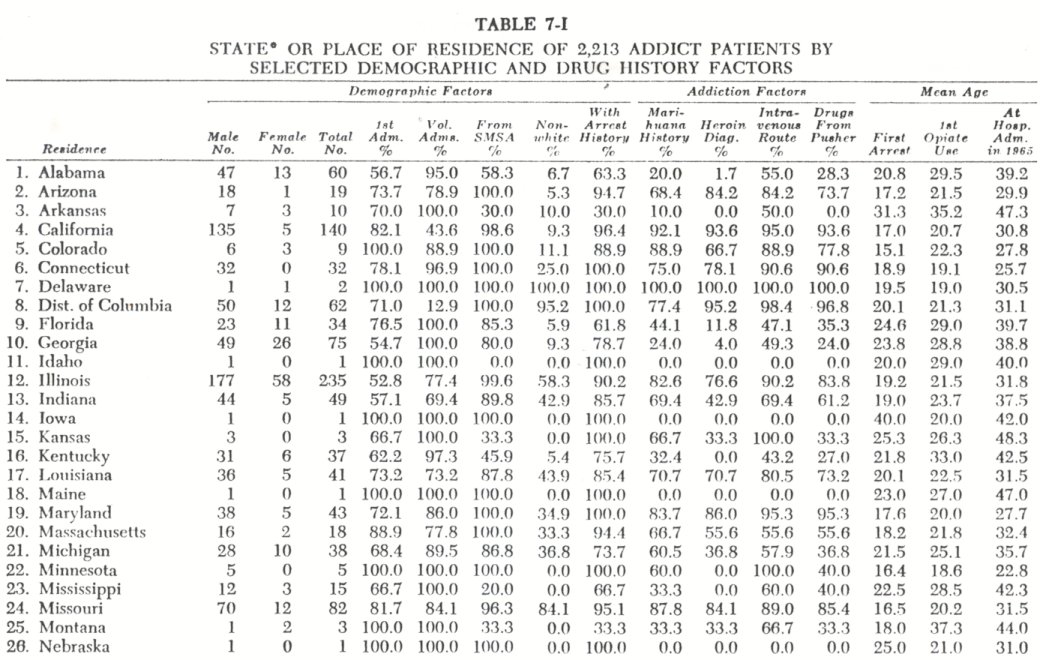
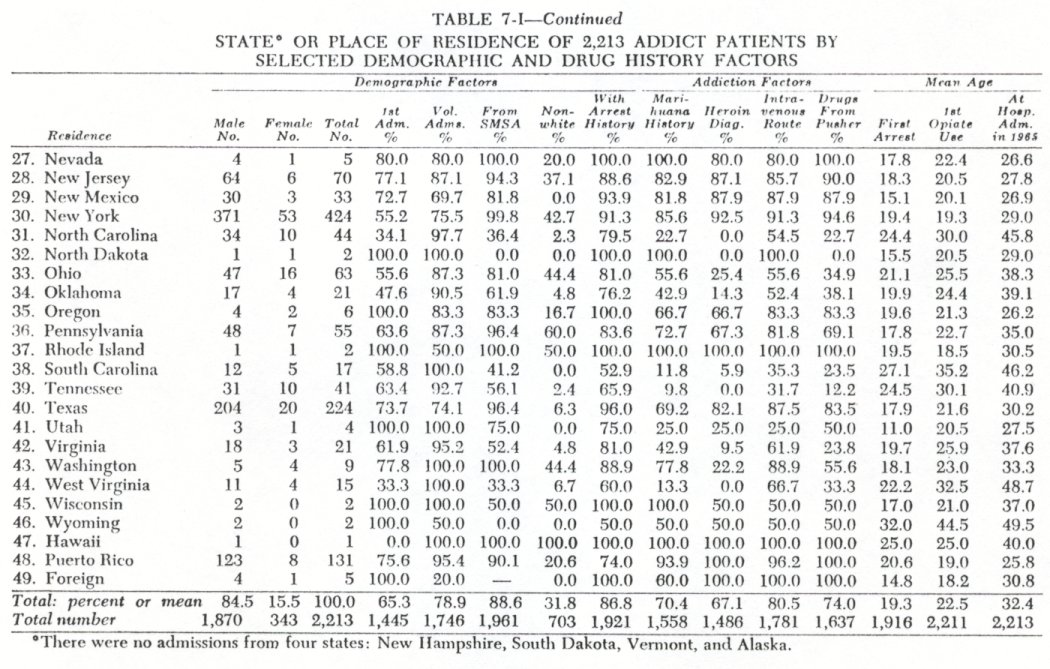
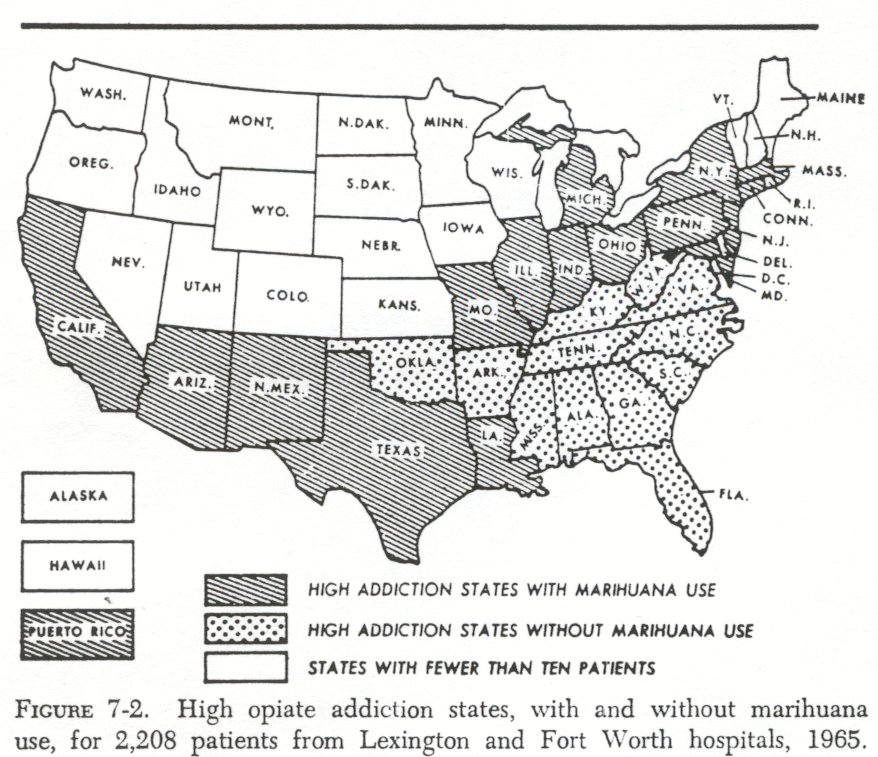
In Table 7-I the percentage of subjects with and without a history of marihuana use is tabulated for each state. Three types of conditions were found to exist with respect to marihuana and opiate use in the United States (Fig. 7-2) . First was the positive association between marihuana and opiate use found in sixteen states, the District of Columbia, and Puerto Rico. In each of these high addiction states, more than 50 percent of the subjects have used marihuana as well as opiates. The sixteen marihuana statesconsist of two contiguous sets. Five of the marihuana states border on Mexico or the Gulf of Mexico: California, Arizona, New Mexico, Texas, and Louisiana. The other eleven marihuana states are located in the Eastern-Midwestern metropolitan belt, on the Atlantic from Boston to New York to Washington, D. C. and westward from Pittsburgh to Chicago to St. Louis. Included within this grouping of states are the District of Columbia and Puerto Rico.' (The marihuana states are those with ruled lines on map in Fig 7-2.)
A second type of association is found in twelve states wherein most of the opiate addicts have never used marihuana. Theseopiate only states (shown by dots in Fig. 7-2) are found in the South and constitute a regionally based area from Miami to Oklahoma to Virginia. In Chapter 5, the pattern of drug abuse in these states has been referred to as the southern pattern of opiate addiction in the United States. It involves the use of opiates other than heroin and it is not associated with marihuana use.
The third condition, or type of association, shown in Figure 7-2 is that of low addiction states with or without marihuana use. The twenty-two states shown in white are low addiction areas on the basis of admissions to the Lexington and Fort Worth hospitals in 1965. Most of these states also have low rates of opiate addiction as computed from the active file of the Federal Bureau of Narcotics. There are, then, two quite distinct patterns of opiate use in the United States. The first pattern of addiction is associated with marihuana use and is concentrated in the metropolitan states-New York, Illinois, California, and Texas. The second pattern of opiate use is that found in the Southern states, and it is not associated with marihuana smoking. The question arises as to why marihuana use is associated with the one pattern of opiate addiction, but not the other?
High Addiction States with an Illicit-Drug Subculture
In the metropolitan centers in which marihuana and heroin use are prevalent, an illicit-drug subculture exists. Marihuana smoking and heroin use can only be steadily pursued in an environment in which there is continuous contact with underworld sources of supply, since neither drug can be legally prescribed nor dispensed in the United States. Although the structure and dynamics of the addict subculture as an enduring group and cultural process, as distinct from an individual and psychological experience, has still to be adequately investigated, some of the basic facets are well known. The importance of learning to smoke marihuana7 or to use a needle when injecting heroine the dominant influence of the adolescent peer-group in the commencement of drug use,° the association of opiate addiction with crime," the difficulty of rehabilitation," and the high death rate among addicts have all been described." In the present analysis the intent is to delineate some of the relevant characteristics of addicts who inhabit the illicit-drug world, contrast them with what may be termed licit-opiate addicts, and consider the probable significance of marihuana use among these two types of addicts.
In sixteen states the District of Columbia, and Puerto Rico, most of the addicts had a history of marihuana use and were also diagnosed as dependent upon heroin at hospital admission in 1965. There was, then, a close association between the use of the two illicit drugs, marihuana and heroin, among residents of the marihuana states. Of the 2,213 addicts, 1,759 were residents of these sixteen states, the District of Columbia, and Puerto Rico, and of these addicts 80 percent had used marihuana and 82 percent were heroin users.
The concentration of the addicts from the marihuana states in metropolitan areas was marked. Over 59 percent of the 1,759 addicts were from the twelve largest Standard Metropolitan Statistical Areas in the United States; only 3.8 percent lived outside of SMSA's.
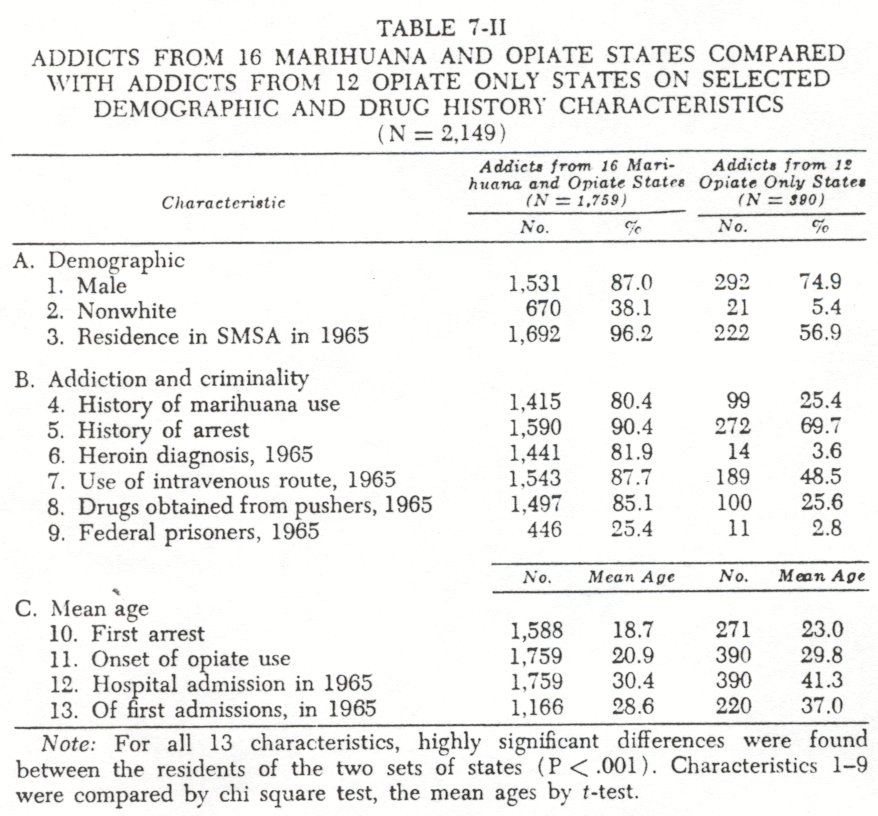
With respect to sex, race, and age, the addict residents of the marihuana states were 87 percent male, 38 percent nonwhite, and had a mean age of 30.4 years in 1965 (Table 7-II) .The significance of minoritygroup status is underrepresented by the nonwhite percentage as this does not include the Puerto Rican and Mexican-American addicts.
The extent of involvement by these metropolitan addicts in the illicit-drug subculture is seen from the data on criminality and addiction history. Over 90 percent of the 1,759 addicts from the marihuana states had been arrested; the mean age at time of first arrest was 18.7 years. In 1965, 25 percent of these addicts were federal prisoners at Lexington or Fort Worth, while many of the voluntary admissions were under legal pressure from local authorities.'
The mean age at onset of opiate use for these 1,759 metropolitan addicts was 20.9 years. The dominant opiate used in 1965 was heroin, by 82 percent of the addicts, and it was commonly ( by 85%) procured from underworld peddlers. The intravenous route of administration was utilized by 88 percent of these addicts. In sum, these young adults had had an early involvement in both delinquency and marihuana use before they became further enmeshed in the illicit-drug subculture to the extent of using opiates.
The question of the sequence of events-marihuana, delinquency, opiate use-requires elaboration. From interviews with 337 patients, a stratified sample of the 2,213 subjects, it was found that the dominant sequence of events as determined from mean ages was marihuana smoking, arrest, and then opiate use. The respective mean ages for these three events were marihuana use at seventeen, arrest at nineteen, and onset of heroin use at twenty.
For the entire sixteen marihuana states, the District of Columbia, and Puerto Rico, the mean age at first arrest was less than the mean age of first opiate use in thirteen of the states and the District of Columbia; in the case of New York it was nineteen years for both and in Puerto Rico it was reversed ( Table 7-I ) . A separate analysis of sequence for the 1,755 individuals supported the finding based on means. 14
High Addiction States With a Licit-Drug Subculture
The twelve states shown in the dotted areas of Figure 7-2 are high addiction states in which less than 50 percent of the patients had a history of marihuana use. The southern, or opiate only,states have a licit-drug subculture in the sense that legally manufactured drugs, such as morphine, Dilaudid, and paregoric, are used, and these are not secured from underworld sources of supply. In these states, then, a quite different pattern of drug abuse obtains-and neither marihuana nor heroin use is prevalent.
The southern opiate only pattern of addiction is less markedly a metropolitan phenomenon than within the marihuana states. Although 57 percent of the 390 addicts were residents of SMSA's, in six of the twelve states more than half of the addicts were from outside SMSA's. This pattern of addiction is, then, less concentrated and less metropolitan than the illicit-drug type.
Of the 390 addicts from the twelve opiate only states, 75 percent were male and only 5 percent were nonwhite. At the time of hospitalization in 1965, their mean age was 41.3 years. This older age was not simply a result of recidivism, as the age at onset of opiate use (29.8 years) and the mean age of first admission patients,in 1965 (37.0 years) were both significantly older than that found among the addicts from the marihuana states.
A markedly different type of involvement in a drug subculture is evident among the 390 addicts from the twelve opiate only states. Although from states with high addiction rates, only 3.6 percent of these Southern residents were heroin users at time of hospital admission in 1965. Further, most received their drugs from doctors or drugstores-only 26 percent secured their drugs from underworld pushers. Also, the intravenous route of administration was employed by less than half of these addicts."
With respect to criminality, the 390 southern addicts were less likely to have an arrest history, and if arrested, this occurred at a later age (23 years). Among the 70 percent who had been arrested, this event commonly preceded the onset of opiate use, although the fact that 30 percent were without an arrest should be noted. As might be expected, few of these addicts were federal prisoners-only 2.8 percent.
In these twelve opiate only states only 25 percent of the 390 addicts had a history of marihuana use. Although by the operational definition employed, marihuana use could not be prevalentin any of these states, the fact remains that there were twelve high addiction states in which marihuana use was uncommon. In addition, these same twelve states were characterized by a different pattern of subcultural involvement.
Within-Area Comparison by Marihuana History
The gross differences obtained between residents of the marihuana and opiate only states, although important in themselves, tend to obscure the issue of the positive association of marihuana smoking with opiate addiction. In order to transcend the marked effect of region, a within-area comparison of marihuana users and nonusers, controlled for sex and race, was undertaken.
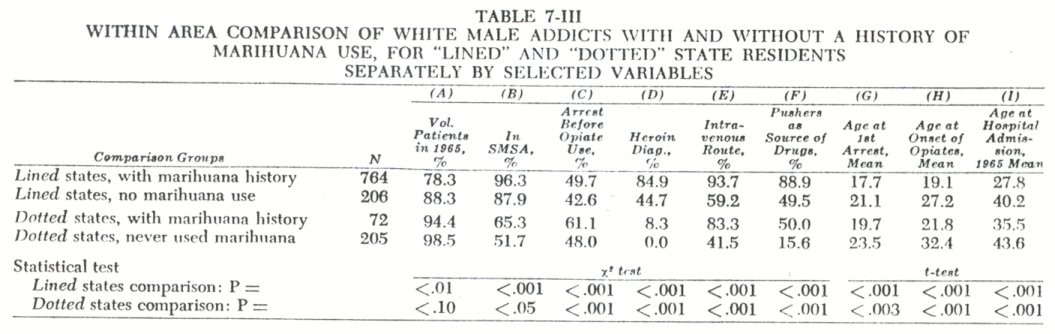
Of the 970 white male addicts from the sixteen illicit-drug states, 77.8 percent had a history of marihuana use and 21.2 percent had never used marihuana (Table 7-III) . Those who had used marihuana were more likely to be metropolitan residents, arrested at an earlier age, and arrested before the onset of opiate use. The 7 64 marihuana users were twice as likely (85 versus 45 ) to be heroin addicts, to use the intravenous method of administration, and to secure their drugs from underworld pushers or sellers than the 206 addicts without a history of marihuana use. In addition, the earlier age at arrest (17 years), at onset of opiate use (19 years), and of Lexington or Fort Worth hospitalization (27 years) of the marihuana group indicates that marihuana use is associated with an early age of entrance into a deviant subculture. Statistically significant differences on all nine variables between the addicts with a marihuana history from those without such a history are presented in Table 7-III.
There were 277 white male addicts from the twelve opiate only states. Of these, 26.0 percent had a history of marihuana use and 74.0 percent had never used marihuana. The seventy-two marihuana users were more likely to be metropolitan residents, more often arrested before the onset of opiate use, and arrested at an earlier age (19 versus 23 years). The marihuana users were more than three times as likely to be securing their drugs from pushers and twice as likely to be taking drugs intravenously. Heroin addiction was uncommon in these twelve states; only six heroin users were included among the 277 addicts. As in the previous comparison within the lined states, the addicts with a marihuana history were notably younger at first arrest, at onset of opiate use, and at time of 1965 hospitalization ( Table 7-III ) . Within the dotted states, then, those addicts who had a marihuana history were significantly different from those without such a history, on eight of the nine variables compared. These differences were often marked-age at onset of opiate use was ten years earlier for the marihuana subjects-and in all eight instances they were in the same direction as in the previous comparison within the lined states.
A similar statistical comparison between marihuana users and nonusers was undertaken for the nonwhite and female addicts. The 703 nonwhite addicts were almost exclusively Negroes 1° from the lined states residing in metropolitan areas. Thus, the only meaningful comparison of the nonwhite addicts was between the marihuana users and nonusers in the sixteen lined states. There were 561 male Negro addicts from these states; 502 of this number ( 89.5 ) had a history of marihuana use, and 59 did not have a marihuana history. Meager but statistically significant differences between the 502 users and the 59 nonusers were found with respect to use of heroin ( 94% versus 85%), use of the intravenous route ( 95Á versus 88x ) , and securing opiates from pushers ( 96% versus 86%). More meaningful age differences between the two male Negro groups were found. Among the 502 addicts with a history of marihuana use, the mean age at first arrest was 18.5 years, mean age at onset of opiate use was 20.1 years, and the mean age at the time of hospitalization for addiction in 1965 was 30.2 years. The comparable mean ages of the 59 Negro addicts without a history of marihuana use for these three events were first arrest, 20.6 years; onset of opiates, 24.0 years; and current hospitalization, 32.8 years; each of these age differences was statistically significant. 17
Of the 109 Negro females from the sixteen lined states, 83 had used marihuana and 26 had not. All 109 subjects were residents of SMSA's in1965. For the comparisons other than age, the only statistically significant difference was with respect to intravenous use-those with a marihuana history were more likely to be using opiates intravenously(94% versus73%) . The other differences were in the same direction as reported in Table7-IYI, al though not statistically significant. With respect to the three age variables, the marihuana group was younger at first arrest(19.8 versus22.9 years), younger at onset of opiate use(20.2 versus24.1 years), and younger at time of hospitalization at Lexington (292 versus32.2) .18
In sum, the Negro addicts who had used marihuana were notably different from those who had not by a younger age involvement in deviancy-arrest, onset of opiate use, and hospitalization for addiction. The other intergroup differences (on variables A, C, D, E and F, Table7-III), even if statistically significant, were attenuated by comparison with the differences noted between the white marihuana users and nonusers who were residents of these same sixteen states, the District of Columbia and Puerto Rico.
Marihuana Use Among White Female Addicts
Of the119 white female addicts from thelined states,66 had used marihuana and53 had not. Those female addicts with a history of marihuana use were more likely than those without such a history to be metropolitan residents(97% versus87%) , twice as likely to be heroin users(82% versus45%) , using intravenously(85% versus47%) and securing their drugs from pushers(89% versus49%). Again, there was marked evidence of earlier involvement in deviancy among the marihuana users: mean age at first arrest(19.4 versus23.9 ), mean age at the onset of opiates(19.3 versus27.4 ), and mean age at1965 hospitalization(26.8 versus35.6 ).19
The female addicts from the twelvedotted states were less likely to have used marihuana than those from thelined states.Of the ninty-two white female addicts from thedotted states, only twelve had a history of marihuana use. These twelve were three times more likely to be using drugs intravenously(83% versus25%) and three times as often securing drugs from underworld pushers(50% versus15%) . The two groups did not differ (in terms of statistical significance) with respect to voluntary status at the hospital, residence in SMSA, (although75% of users versus 51% of nonusers were SMS A residents), or heroin addiction .z° As in all previous within-area comparisons, the addicts with a history of marihuana use became involved in deviancy at an earlier age than those who did not use marihuana. The mean age at first arrest for the12 white female marihuana subjects was23.9 years, mean age at onset of opiate use was 23.0 years, and mean age at Lexington hospitalization was31.8 years. The comparable figures for the eight), white female addicts without a history of marihuana use from the twelvedotted states were: first arrest,28.9 years; onset of opiates,32.7 years; and1965 hospitalization,43.5 years. 21
Interpretation of the Research Findings
The present research findings provide inferential evidence that marihuana smoking has become more common among opiate addicts in recent years. The older age of the655 addicts without a history of marihuana use(40.3 ), when contrasted with the1,558 who had smoked marihuana(29.1), provides substance for such an interpretation. Furthermore, the absence of references to marihuana use among opiate addicts by Terry and Pellens 22 and Pescor's findings in1937 that only a few Lexington patients had used marihuana before opiates seems significant when contrasted with the dominant pattern of marihuana use followed by opiate abuse reported by Fort ,23 Finestone,'4 Chein 28 and Ball 26 in morerecent years. The available evidence suggests, then, that marihuana smoking has increased among opiate addicts in the United States.
A further general comment concerning the significance of dependence upon specific opiate drugs is relevant. At the time of hospitalization in 1965, 1,486 of the 2,213 patients were diagnosed as heroin users. The other opiates being abused were morphine (by 201 addicts), Dilaudid (135 ), paregoric (131), meperidine (108) , codeine (86) , and the remaining sixty-six patients were using methadone, Percodan®, Pantopon, opium, cocaine and Numorphan®. The association of heroin dependence with a history of marihuana use within each of the two regional high addiction areas has been delineated. What is not apparent, however, is the extent to which opiate use may be drug-specific for some persons. Thus, most of the 129 meperidine and methadone users have never used heroin, and only 16 have ever used marihuana. The point being that within the general addict population one finds particular drug-specific behavioral patterns which appear to insulate the individual from other types of drug abuse. 27
As to the issue of association, marihuana smoking is seen as a predisposing influence in the etiology of opiate addiction in the United States. Among metropolitan residents of the high addiction eastern and western states, opiate use .is commonly preceded by the smoking of marihuana cigarettes and arrest. Thus, both marihuana use and delinquency are predisposing factors within the metropolitan host environment.
But what is the relative effect of marihuana use with respect to subsequent addiction? Is it of greater import than delinquency, or an unstable home? An adequate answer to this question is not possible. Still, enough is now known about the association of marihuana and opiate use to delineate the dominant relationship of these two events.
The incipient addict is predisposed to opiate addiction by his use of marihuana for the following reasons: marihuana is taken for its euphoric effects-it produces a high; both marihuana and heroin are only available from underworld sources of supply; both are initially taken within a peer-group recreational setting; both are illegal; the neighborhood friends with whom marihuana use begins are often the same friends who initiate the incipient addict to the use of opiates. A principal effect, then, is one of differential association-becoming part of a drug-taking group.
In considering the association of marihuana and opiate use, attention has been focused only upon the type 1 situation depicted in Figure 7-1. It has now been shown that a type 2 situation also prevails in the United States-opiate addiction without marihuana use. It is evident that there are several patterns of behavior which lead to drug addiction. Data of the present study support the conclusion that marihuana use is closely associated with opiate addiction in the high drug use metropolitan areas of the East and West but not associated with opiate addiction in twelve southern states.
1. For a discussion of this issue see the Report by the President's Commission on Law Enforcement and Administration of justice:The Challenge of Crime ina Free Society. Washington, D.C., U.S. Government Printing Office,1987, pp.224225.
2. Anslinger, Harry J., and Tompkins, William F.:The Traffic in Narcotics. New York, Funk & Wagnalls,1953, pp.20-22.
3. Solomon, David:The Marihuana Papers, New York, Bobbs-Merrill Company, Ins.,1986, pp.13-21.
4. The smoking of marihuana cigarettes does not necessarily lead to opiate addiction or adverse effects for some persons. On this latter point see the Mayor's Committee on Marihuana:The Marihuana Problem inthe City of New York. Lancaster, Pennsylvania, Jaques Cattell Press,1944, p.38; also see Howard Becker's case report of adverse effects: Becoming a marihuana user.American Journal o f Sociology, 59:241, 1953.
5. Robins, Lee N., and Murphy, George E.: Drug use in a normal population of young Negro men.American Journal of Public Health, 57:1580-1598. 1987.
6. Puerto Rico, although not contiguous to these states, is closely tied to the East Coast by virtue of migration and rapid air transportation.
7. Becker, Howard, op. cit., note 4, at pp.235-242.
8. Ball, John C.: The Onset of Heroin Addiction in a Juvenile Population: Implications for Theories of Deviancy. Paper read at the annual meeting of the American Sociological Association, August 31, 1966, p.4.
9. Chein, Isidor, Gerard, Donald L., Lee, Robert S., and Rosenfeld, Eva:Tile Road to N. New York, Basic Books, 1984, Ch. 5.
10. Finestone, Harold: Narcotics and criminology.Law and Contemporary Problems, 22:69-85, 1957; O'Donnell, John A.: Narcotic addiction and crime.Social Problems, 13:374-385, 1986.
11. U.S. Department of Health, Education and Welfare:Rehabilitation in Drug Addiction. L4ashington, D.C., U.S. Government Printing Office, Revised, 1984.
12. See Part IV.
13. Levine, Jerome, and Monroe, Jack J.: Discharge of narcotic drug addicts against medical advice. Public Health Reports, 79:13-18, 1984.
14. Of the 337 addicts in the stratified sample, complete sequential data was available on 210; the principal reason for omissions were no arrest or no marihuana use, particularly among the 167 females included in this sample. Of the 210 addicts, 182 ( 87%) had used marihuana before opiates and 28 (13% ) had first used it after the onset of opiate use. With respect to the sequence of marihuana use and arrest, 142 (68K) used marihuana first, while 68 (32%) were arrested first.
15. See Chapter 9 for a discussion of this topic.
16. Of the 703 nonwhite addicts, 699 were Negro, 2 Chinese, 1 Hawaiian and 1 Filipino.
17. The t-test probabilities were arrest, P <.05; onset, P <.001; hospitalization, P <.005.
8 The probabilities were (t-test) <05, <Ol, and <08.
19. Probabilities (t-test): <.003, <.001, and <.001.
20. Only three of the ninety-two females were heroin users in 1965.
21. Probabilities (t-test): <.02, <.001, and <.001.
22. Terry, Charles E., and Pellens, Mildred: The Opium Problem. New York,Bureau of Social Hygiene, 1928.
23. Fort, John P.: Heroin addiction among young men. Psychiatry, 17:251-259, 1954.
24. Finestone, Harold: Cats. kicks, and color. Social Problems, 5:3-13, 1957.
25. Chein, ct al., op. cit., Ch. 6.
26. See Chapter 10.
27. Rasor, Robert W., and Crecraft, H. James: Addiction to meperidine (Demerol) hydrochloride. Journal of the American Medical Association, 157:654 657, 1955.
| < Prev | Next > |
|---|