| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 174 |
| Yesterday: | 251 |
| This Week: | 174 |
| Last Week: | 2221 |
| This Month: | 4762 |
| Last Month: | 6796 |
| Total: | 129361 |
Chapter 18 Absence of Major Medical Complications Among Chronic Opiate Addicts
 |
|  |
| 
| Books - Epidemiology of Opiate Addiction in United States |
Drug Abuse
The Epidemiology of Opiate Addiction in the United States
Chapter 18
Absence of Major Medical Complications Among Chronic Opiate Addicts
JOHN C. BALL AND JOHN CHAPMAN UR13AITIS
The long-term effects of opiate addiction remain essentially unknown. Although the acute effects of heroin use and the related major medical complications of heroin addiction have been studied,' the precise sequelae of chronic opiate addiction, apart from the infections and fatalities associated with careless self-administration of adulterated drugs, are still obscure= The issue is of contemporary relevance because of the continued prevalence of opiate addiction in the metropolitan centers of the United States and the increasing use of opiates (particularly methadone) in the long-term out-patient treatment of addicts.'
Method
A sample of chronic opiate addicts from the Lexington Hospital was selected for study. It consisted of the 31 male patients who had been admitted to the hospital twenty or more times since it opened in 1935-from a total of 34,043 male addicts treated through 1966. These repeated admissions provided a detailed and voluminous clinical history on each patient, and it was soon evident that the sample included only chronic opiateaddicts.
Results
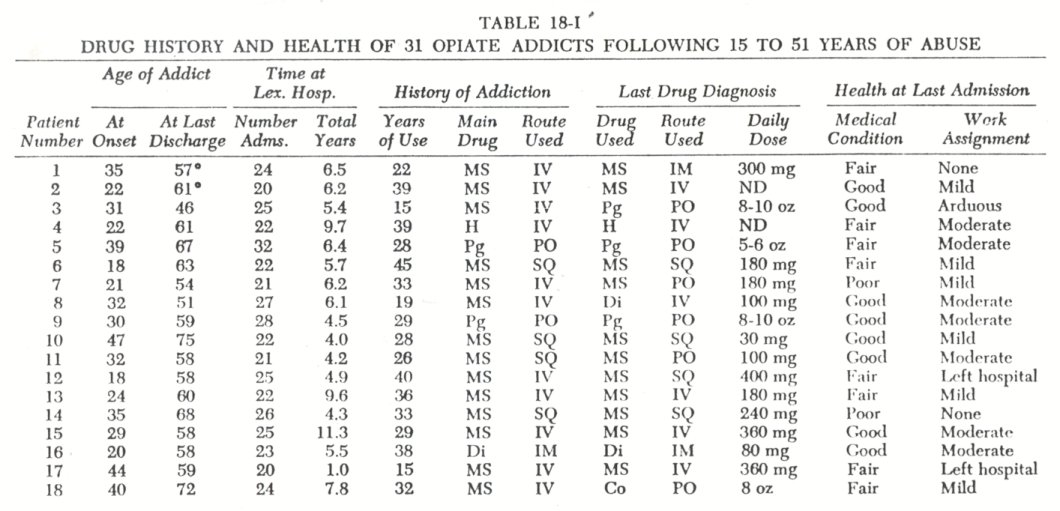
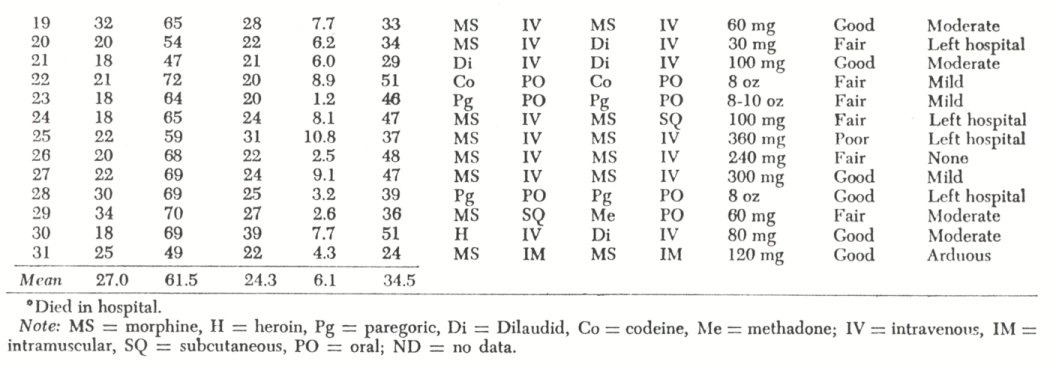
The thirty-one male addicts were all white, predominantly from the South, typically started use of narcotics in their twenties, and had used opiates for some thirty-five years prior to their last admission. The principal drug of addiction was morphine, and it was commonly taken intravenously ( Table 18-I ) .
With respect to treatment, most of the thirty-one patients were voluntary admissions to the Lexington Hospital; 21 of their first admissions were voluntary, and 80 percent of their 754 total admissions were voluntary. Commonly, treatment was terminated against the medical advice of the staff, and the patient left the hospital after several weeks to resume opiate use. At the time of their last admission their mean age was sixty-one years, and they had had from nineteen to thirty-eight prior admissions for treatment of addiction. Although these thirty-one male patients were selected on the basis of multiple admissions, they were not different from the hospital population with respect to either the preponderance of voluntary admissions (as opposed to federal prisoner admissions) or the common practice of leaving the hospital against medical advice.
In reviewing the extensive medical records of the thirty-one addict patients, particular attention was given to the physical examination and clinical notes of each patient's last admission. In this regard the following were enumerated: daily dose of opiates used prior to hospitalization, method of administration, concurrent use of barbiturates, blood pressure, serology and other clinical data, presence of specified disease, evidence of any medical reason for drug use, and whether or not the patient received special treatment on the withdrawal ward. Following this review we classified each patient's general medical condition and recorded the hospital work assignment designated by the physician. This latter measure was employed because the type of work assigned by the physician is based upon the patient's physical condition and capacity.
At the time of their last voluntary admission twenty-one of the thirty-one addicts were physically dependent upon y opiates, and nineteen were also using barbiturates. In no instance was there evidence of a medical reason for drug use. Furthermore, these patients did not give a history of a medical reason for their continuing drug abuse.
Of the thirty-one male addicts, fourteen were in good health, fourteen were in fair health, and three were in decidedly poor health when examined during their last admission to the hospital. Of the three who were ill, one had a cardiac condition, one had arthritis, and one was suffering from severe malnutrition. On the withdrawal ward only the malnutrition case required special treatment; all others were withdrawn from either one or both drug habits ( opiates and barbiturates) at the usual schedule, without incident. In addition, twenty-two of the twenty-seven who remained in the hospital were given a work assignment by the medical staff. From medical and psychological records there was no evidence of overt psychosis in any of the addicts.
Discussion
Initially we expected that a study of the thirty-one patients who, over a thirty-two year period, were most frequently hospitalized at Lexington for their addiction would result in the selection of a chronically ill and debilitated group. It seemed likely that the end result of extended opiate abuse would be physical and perhaps mental deterioration.
This did not occur. Instead, we found that twenty-eight of the thirty-one patients were still in average or fair medical condition for their age after a lifetime of opiate addiction. Although three patients were ill at their last admission, this was not attributable to drug use, with the possible exception of the malnutrition case. Two of the thirty-one patients died at a later time in the hospital (from subarachnoid hemorrhage and cardiac failure), but there was no reason to relate this to prior opiate use.
That twenty-two of the sample were morphine addicts and only two had used heroin as their principal opiate seems significant inasmuch as morphine is legally manufactured for distribution in the United States while heroin is illicitly produced and usually adulterated. In this respect it seems evident that opiate effects per se must be differentiated from the medical complications associated with the hectic way of life pursued by youthful heroin addicts. While there is ample evidence that the
aberrant way of life followed by most heroin abusers has both acute and chronic medical consequences ( i.e., tetanus, overdose, hepatitis, endocarditis ), there is insufficient scientific basis for maintaining that the long-term use of opiates-in and of itself is related to any major medical condition. The issue (drug effects versus secondary effects) is of contemporary relevance inasmuch as opiates are being prescribed for the long-term maintenance treatment of addict patients.
Finally, we considered the possibility that our sample of thirty-one Lexington patients was atypical in that these addicts had survived, while other addicts might not, a lifetime of opiate abuse. The contention that these thirty-one cases ( who were
unselected except for multiple admissions) were somehow different from other chronic opiate addict patients seems untenable for two reasons. First, during twenty or more hospital admissions spanning the adult years of the patient, there was no medical indication that these thirty-one addicts were atypical. Second, the general absence of major medical complications among most addicts treated at the Lexington Hospital seems relevant, as it substantiates the present finding that it is the secondary effects of opiate use that are the principal medical problem.
1. Louria, Donald B., Hensle, T., and Rose, J.: The major medical complications of heroin addiction.Annals of Internal Medicine, 67:1-22, 1967.
2. Sapira, Joseph D.: The narcotic addict as a medical patient.American Journal of bfedieine, Q5:555-588, 1968.
3. Dole, Vincent P., Nysx·ander, Marie E., and Warner, A.: Successful treatment of750 criminal addicts.Journal of the American Medical Association, 206:27082711, 1968.
| < Prev | Next > |
|---|