| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 174 |
| Yesterday: | 251 |
| This Week: | 174 |
| Last Week: | 2221 |
| This Month: | 4762 |
| Last Month: | 6796 |
| Total: | 129361 |
Chapter 19 Conclusion
 |
|  |
| 
| Books - Epidemiology of Opiate Addiction in United States |
Drug Abuse
The Epidemiology of Opiate Addiction in the United States
Chapter 19
Conclusion
JOHN C. BALL AND CARL D. CHAMBERS
In 1928 Charles E. Terry and Mildred Pellens published a comprehensive review of the problem of drug abuse in American society. In their classic work,The Opium Problem, they traced the historical development of the problem from Colonial times to the first decades of the twentieth century. They found that the use of narcotic drugs was widespread throughout the United States; that morphine and heroin were the principal drugs of addiction; and that many persons were addicted as a consequence of medical treatment but that many more were initiated to drug use by curiosity, a desire for excitement, or through association with underworld contacts. They concluded that the chronic use of narcotic drugs was a national problem in that there were serious social consequences with respect to criminality, unemployment, poverty, disease, and both physical and mental debilitation. In sum, it was found that there was a pervasive inability on the part of most opiate addicts to pursue an acceptable or socially rewarding way of life.
What has happened to the American drug problem since 1928 has been a central focus of the present volume. The topic can perhaps best be reviewed by considering both changes in the drugs of abuse and changes within the addict population itself.
Drugs of Abuse
The outstanding change which has occurred during the past several decades with respect to drugs of abuse has been the discovery and commercial exploitation of a plethora of new products-the barbiturates, tranquilizers, amphetamines, and hallucinogens. These new drugs have had general acceptance by the medical profession, and their ethical use has been widespread. Concomitant with their legitimate medical use, however, there has rapidly developed an illicit traffic and widespread abuse. Thus, in the1970's we are confronted with the prospect and reality of a continual increase in the number of Americans who resort to the illicit use of the various "dangerous drugs."
The increased medical use of the psychotropic drugs and the related misuse of these same drugs by the public represents a new historical phenomenon. The number of mood-altering drugs which are available, both licitly and illicitly, surpasses that of any previous historical period. Furthermore, self-administration of these "dangerous drugs" is increasing, although endemic misuse appears to be still confined to particular segments of the population. There is, however, scant reason for optimism. An ever increasing number of potentially dangerous drugs are being produced, and many of these are being misused by the public.
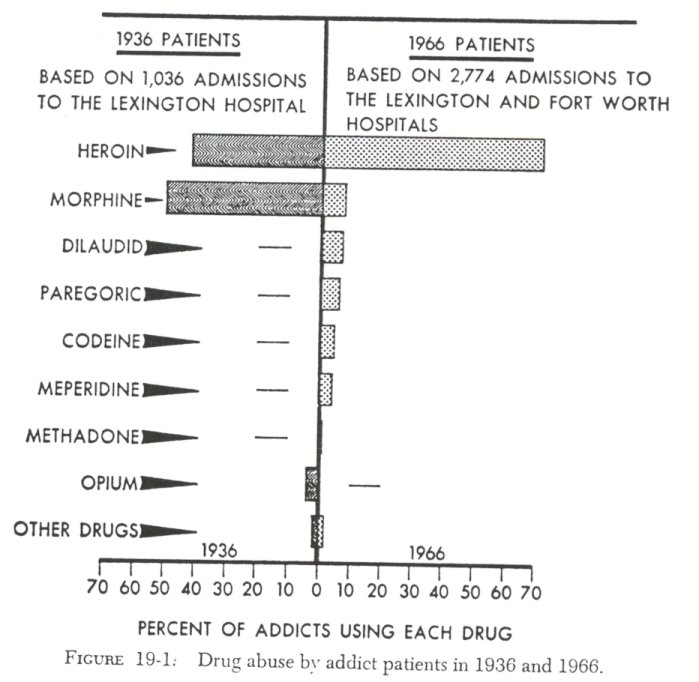
With respect to the opiate drugs two principal changes hale occurred in the United States during the past forty years. First, heroin has become the predominant opiate of abuse, whereas formerly it was morphine and opium. Second, synthetic narcotic analgesics have been manufactured for medical use. This pharmacological advancement has increased the number of opiatelike ( or opioid ) drugs which are available to physicians, but it has also increased the number of opiates which a-re being abused. Two such synthetic analgesics are methadone and meperidine. Both of these are cross-tolerant with morphine, and both produce physical dependence. Closely associated with the continual introduction of new opioid drugs has been the persistent hope of discovering an analgesic drug of comparable efficacy to morphine but without its addiction liability. It now seems unlikely that such a pharmacological discovery is imminent and, furthermore, it appears that even such a significant discovery would not materially alter the principal patterns of drug abuse in America.
How the patterns of opiate abuse have changed in the United States can be seen by comparing the principal drugs used by addict patients at the Lexington Hospital in1936 with those of different opiate drugs being widely abused has markedly increased.
Lastly, with respect to changes in common drugs of abuse, a few comments are pertinent with respect to marihuana. Use of this drug has markedly increased in the United States since the 1930's. Among metropolitan opiate addicts, marihuana is now the common illicit drug of initial use. In addition, the smoking of marihuana has spread to college communities. Use of this illicit drug presents a special case in that this rather mild hallucinogenic substance has no recognized medical use; it is neither legally grown nor manufactured in the United States. The smoking of marihuana, then, is something quite different pharmacologically and historically from the abuse of the opiates or the "dangerous drugs."
Changes in the Addict Population
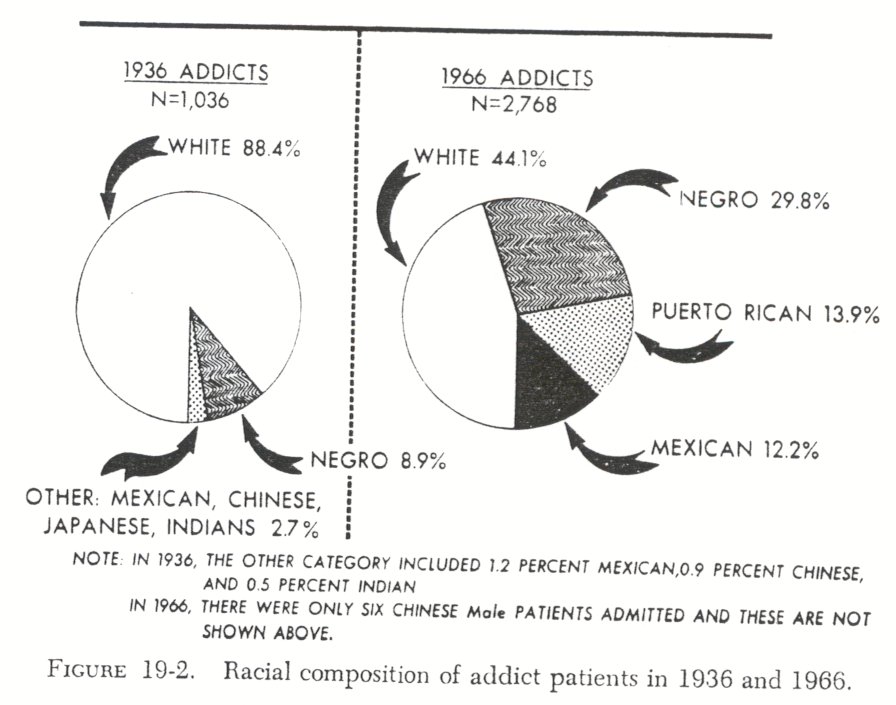
The major demographic change which has occurred in the addiction problem during the past forty years has been the shift from a predominantly white male population to one that is largely composed of minority groups-Negro, Puerto Rican, and Mexican-American. As late as 1936 Pescor reported that 88 percent of Lexington patients were white, and most of these were native born of native parents. By 1966, 56 percent of the addict patients being admitted to the two federal hospitals were from these three minority groups ( Fig. 19-2 ) .
This marked increase in opiate abuse among certain minority groups in the United States has been associated with the continuing concentration of our population in large cities. It is the Negro and Puerto Rican youth of these cities who are most likely to become addicts; those who live outside metropolitan centers are relatively immune. Thus, the Negro population in the Southern states has continued to have an exceptionally low incidence of opiate abuse, while addiction among Negroes in New York, Chicago, and Los Angeles has increased.
In addition to tracing the natural history of opiate abuse within discrete segments of American society-Southern white, metropolitan black, Chinese males, Puerto Rican youth, Mexican- Americans-it is important to recognize that individual drug abusers are quite heterogeneous with respect to their life careers. Thus, one finds "street" addicts who pursue a hectic way of life which encompasses petty theft, odd jobs, and dependency. There are also, however, both successful and unsuccessful professional addict criminals-drug sellers, con men, and pimps who enjoy a high income and who are infrequently arrested, as well as those who are less affluent and continually incarcerated. There are addict prostitutes, both those who were soliciting before turning to drugs and those who entered prostitution as a means of obtaining money for drugs. There are marginal addicts who have been gainfully employed and who are motivated to discontinue drug use once medical treatment is provided. There are addicts who function quite well on drugs and others who do not. Lastly, there are solitary physician and nurse addicts who covertly practice the self-administration of opiates, and there are other professionals who engage in proselytizing and sale of drugs. All of these individual types are a part of the contemporary problem of drug abuse in the United States.
Etiology and Prevention
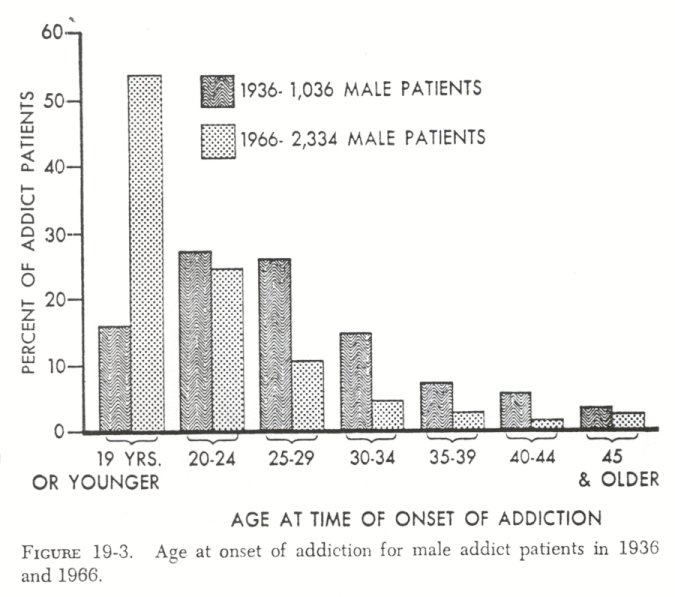
Certainly one of the most significant epidemiological changes which has occurred in the United States with regard to the problem of opiate addiction has been the increased incidence of drug abuse among adolescents in our metropolitan centers. This striking historical decline in the age of onset of opiate use may be seen from comparative hospital data. In 1936 only 16 percent of 1,036 male Lexington patients from throughout the United States began their opiate use before age twenty. By 1966, 53 percent of 2,334 male patients were nineteen years of age or younger when onset of opiate use occurred ( Fig. 19-3 ). During a thirty-year period the etiological nexus almost completely changed-from a situation in which only 16 percent began drug use as adolescents to one in which 53 percent began to use opiates while they were adolescents.
The American drug problem, then, has become an adolescent phenomenon with respect to etiology. Most boys now start theiropiate use while they are teenagers-between thirteen and nineteen years of age. Thus, many boys commence their use of drugs while they are students. In this regard it should be noted that most contemporary addicts have smoked marihuana prior to their first use of opiates, so that their initial use of illicit drugs commences at an even earlier age than the above figures indicate. It is now evident that junior high school students in our largest cities represent a high-risk population with respect to drug abuse. The risk is particularly acute in certain minority-group neighborhoods-Negro, Puerto Rican, and Mexican-American although the problem is certainly not confined to any geographic area or culture group.
With regard to prevention it seems unlikely that any type of educational program will, of itself, be efficacious in reducing the incidence of drug abuse among adolescents. Most drug users are not uninformed about the dangers and delights associated
with particular drugs. Quite the contrary! They are often most knowledgeable persons in this regard. Furthermore, it appears that we have projected our own rationalistic notions upon teen age users or potential users. We assume that the fifteen-year-old boy will harken to our admonitions and carefully consider the future consequences of his present peer-group recreational behavior if only he can be properly taught. But these moralistic assumptions about youthful behavior are illusory, as can be seen from the continued persistence of juvenile delinquency, drunkenness, illegitimacy, venereal disease, and other problems of adolescents. It simply cannot be said that education alone will eradicate any of these problems, although the expectation that it will do so persists.
A more realistic approach to the prevention of drug abuse would appear to be based upon establishing effective social controls among local neighborhood and community residents. For, so long as pushers remain on a street, addicts congregate in buildings along the street to "shoot" heroin, and twelve-year-old boys are used as runners, it seems quite unrealistic to believe that classroom instruction will insulate the adolescent from drug abuse.
| < Prev |
|---|