| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 174 |
| Yesterday: | 251 |
| This Week: | 174 |
| Last Week: | 2221 |
| This Month: | 4762 |
| Last Month: | 6796 |
| Total: | 129361 |
Chapter 17 Suicide Among Hospitalized Opiate Addicts
 |
|  |
| 
| Books - Epidemiology of Opiate Addiction in United States |
Drug Abuse
The Epidemiology of Opiate Addiction in the United States
Chapter 17
Suicide Among Hospitalized Opiate Addicts
CARL D. CHAMBERS AND JOHN C. BALL
Introduction
The Lexington Hospital treated43,215 opiate addicts between May29, 1935, and January1, 1967. Thirteen of these addicts committed suicide during hospitalization. This study is a description of these thirteen suicides.
With a suicide rate of three per ten thousand, hospitalized opiate addicts commit suicide more frequently than the general population (1 per 10,000 ) but less frequently than inmates in prisons(5.5 per 10,000)1 and less frequently, than mental hospital patients ( 38 per 10,000 ) .2
As addicts were admitted to the hospital either as voluntary patients who could exercise their prerogative to leave at any time or as prisoners confined for specified periods of time, this dichotomy of patients provided a frame of reference for the study. Of the77,076 separate admissions to the hospital,74.6 percent were voluntary admissions.
Hospital Status and Suicide
Although voluntary and prisoner patients have almost identical access to the various hospital facilities and treatment services and face the same institutional restrictions while in the hospital, two factors differentiate the two. First, the voluntary patient may terminate the treatment process at any time by requesting a discharge, while the prisoner patient must remain for the period of time stipulated by the court. Second, the prisoner patient has usually undergone withdrawal from drugs before arriving at the hospital. Each of these factors could affect the suicide rate. Therefore, an analysis of the association of hospital status with suicide was undertaken.
Suicides Among Voluntary Patients
Five of the addict patients who committed suicide had voluntarily sought hospital admission for treatment of their addictions and could have requested discharge and left the hospital as an alternative to suicide. None of these five patients had histories of any prior suicide gesturing, and none engaged in any gesturing in the hospital prior to the suicide event, nor were any sufficiently depressed during the treatment process to be diagnosed as suicide risks requiring special precautionary measures ( e.g. seclusion or 24-hour observation).
Although these five suicides had been using drugs for an average of9.8 years, none of them had ever been withdrawn from drugs. Three of the five did commit suicide during the initial detoxification process, and two of these were undergoing barbiturate as well as opiate withdrawal. In the absence of contrary data it may be assumed that the physiological and psychological discomfort they were experiencing as the result of detoxification had an effect on their decision to commit suicide. The reason for choosing suicide instead of leaving the hospital remains obscure.
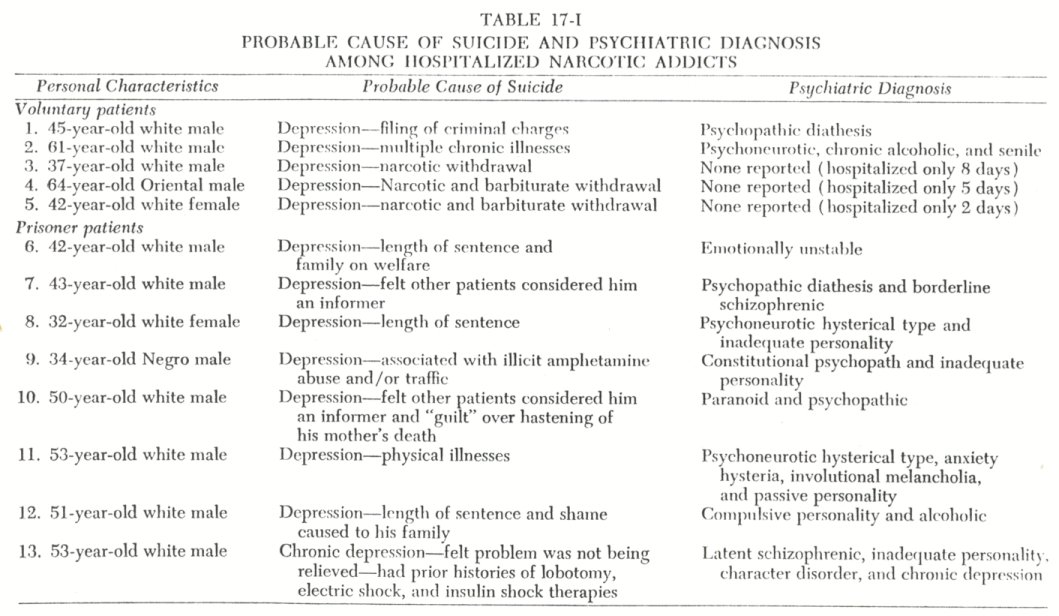
Withdrawal discomfort, however, would not appear to be present for the remaining two suicides among voluntary patients. Both victims had completed the prescribed withdrawal treatment. Indeed, both had been in the hospital for longer periods of time than the average voluntary patient. They were hospitalized93 and106 days before committing suicide, while the average period of hospitalization for37,411 voluntary admissions between1935 and1960 was52.8 days. The probable cause of death for these two suicides was recorded as depression resulting from the filing of criminal charges against the patient and as depression resulting from chronic and irreversible physical illnesses ( Table 17-I ).
Suicides Among Prisoner Patients
The eight prisoner patients who committed suicide had been sent to the hospital for periods of time ranging from eighteen months to five years. Five of these prisoners committed suicide within the first sixty days of their sentences. This could indicate difficulties in adjusting to the hospital or to a prisoner status, although all of them had prior experience of being incarcerated or hospitalized. In two of the remaining three cases, the anticipation of readjustment to society may have contributed to their suicides, since both were within sixty days of completing their sentences.
The physical and psychological discomfort associated with drug withdrawal would not appear to have been a significant contributing factor in the suicides among the prisoners. Four of the eight were not addicted when admitted, three had completed their prescribed withdrawal treatment, and withdrawal was not attempted with one' patient who was critically ill. In addition, seven of the eight had previous withdrawal experience, and four of them had prior "cures" in this hospital 3
In contrast to the absence of suicide cues among the voluntary patients who committed suicide, 62.5 percent of the prisoners who committed suicide were (mown to have histories of gesturing or had been specifically diagnosed as suicide risks by the treatment staff. Half of the prisoners ( but only one of the voluntary patients) spent sufficient time contemplating suicide to prepare a suicide note.
Data from the four suicide notes written by the prisoners and from the official reports concerning the suicides indicate that the probable cause of the suicides was as follows: three were depressed over the lengths of their sentences, three were depressed over problems they were having within the hospital ( e.g., two of them were "afraid" the other patients thought they were informers and the third was having some unspecified difficulty because of his involvement in an illicit amphetamine-using group), one was diagnosed a chronic depressive with a paranoid complaint, and the remaining victim was reported as depressed because of physical illness.
Comparing the addiction patterns of the voluntary and prisoner patients who committed suicide, the following similarities, or differences, were noted. Both groups were made up of addicts with long histories of drug addiction and both groups began drug use after attaining adulthood. The prisoners, however, usually began their drug use for "kicks" or out of curiosity, while the voluntary patients usually reported a medical reason for onset. Most of the prisoners had obtained their drugs from illegal sources, while the voluntary patients usually had legal sources of supply. The prisoner patients, as a group, had a longer history of addiction and more attempts at cure than the voluntary patients. The latter group began their drug use approximately twelve years later than the prisoners, and they had not previously sought treatment. The prisoner patients had extensive criminal records, while the voluntary patients did not. In neither group was there any consistency as to method, instrument, or physical location chosen to complete the suicides. Prisoner patients, however, were more likely to engage in suicide gesturing prior to committing suicide, and they were more likely to leave suicide notes."
Comparison with Other Addict Patients
Female patients commit fewer suicides than male patients. Eleven of the thirteen suicides have been males. Thus, the male suicide rate of 3.2 per 10,000 may be compared to a rate of 2.2for the females.
The younger patients have not committed suicide. None of the thirteen were under thirty years of age; three were in their thirties at the time of suicide, four in their forties, four in their fifties, and two were in their sixties. The range in age at time of death was from thirty-two to sixty-four years with a mean of 46.7. These patients were, then, considerably older than the general addict hospital population.
Suicide was somewhat less common among the Negro patients. The suicide rate among the Negroes was three per ten thousand compared with the white rate of four per ten thousand. In addition to these suicides there was one Oriental male who killed himself.
Religious preference was not associated with suicide. Of the thirteen addicts five reported themselves as Catholics, five were Protestant, two were Jewish, and one reported he had no religion.
No evident relationship between social class and suicide was found among the addict patients. In considering this question, three variables were analyzed: father's occupation, the addict's education, and his occupation.
Data were available on fathers' occupations for ten of the thirteen suicides. Of these ten fathers four had been skilled workers, two had been unskilled or semiskilled workers, two had been farmers, and two had been professionals.
Data was available on level of educational attainment for twelve of the suicides. Of these, two had completed college, two had completed eleven or twelve years of schooling, and the remaining eight had completed eight or fewer years.
In tabulating the suicides' former occupation, it was found that six were unskilled or semiskilled workers, two were professionals, two were in clerical-sales occupations, one was a farmer, and two had supported themselves through illegal means. A comparison between addicts' and their fathers' occupation indicated downward occupational mobility in at least 38.5 percent of the cases. To what extent, if any, downward mobility can be attributed to their addiction cannot be ascertained. Both occupational categories, as near as possible, refer to the dominant lifetime occupation.
Neither parents' marital status nor the subjects' marital status were related to the incidence of suicide among these hospitalized addicts. Data pertinent to childhood home status was available for twelve of the thirteen addict-suicides. Of these twelve, 83.3 percent had been reared in intact homes. With regard to the addicts themselves, six had intact marriages, three were separated, two were widowed, one was divorced, and one was single.
The patients who committed suicide were not different from the hospital population with regard to place of residence. Thus, by census region, 34.2 percent of the hospital's patient population had come from the Northeast, 33.3 percent from the South, and 29.8 percent from the North Central region. The distribution of suicides was not significantly different, with 46.2 percent being from the Northeast, 38.5 percent being from the South, and 15.4 percent being from the North Central region. Most of the suicides (84.6%) had lived in Standard Metropolitan Statistical Areas, as had most of the hospital population.
Somewhat surprisingly, the general physical condition of the patients was not related to suicide. Acute or serious physical illness was not a significant factor in these suicides.,' Only three of the thirteen addicts were experiencing physical illness at the time of suicide.
Ten of the thirteen suicides had been hospitalized a sufficient length of time to receive psychiatric evaluations. All of those evaluated had a recognizable psychiatric deviancy existing concomitantly with their drug addiction. The majority, 80.0 percent, had more than one concomitant diagnosis. Thirty percent of these with psychiatrically diagnosed deviations had been previously institutionalized in mental hospitals. None of these psychiatrically labeled addicts had a favorable prognosis.
The Suicide Event
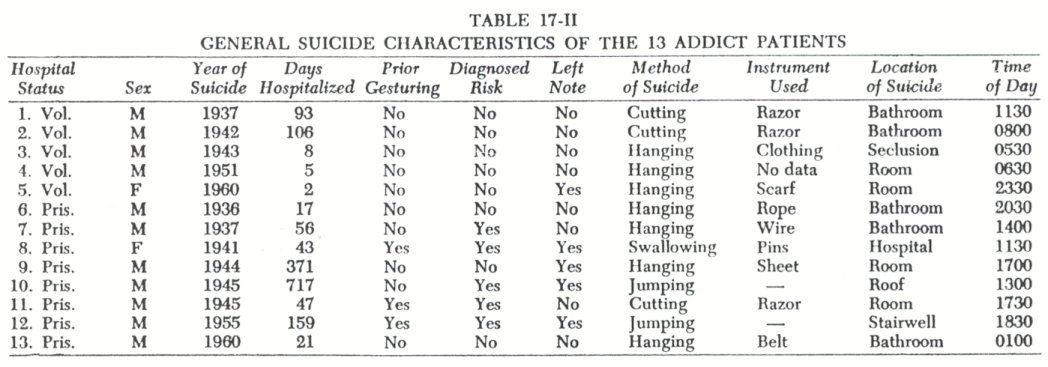
Suicides have occurred as early as the second day of hospitalization and as late as two years after entering the hospital. The mean number of days hospitalized for this group of thirteen addicts was 126.5 days ( or a little over 4 months). Although the suicides occurred over a 26-year period, 46.2 percent did occur during the period of World War II (1941-1945).
A variation as to the time of year during which the suicides occurred was noted. Of the suicides, two occurred during the first quarter of the year, seven during the second quarter, one during the third quarter, and three during the last quarter of the year. More suicides occurred in April ( 30.8 ) than in any other month. There were no significant differences in the time of day chosen to commit suicide. During the time period 12:01-6 A.M., 15.4 percent committed suicide; 30.8 percent did so between 6:Ol.and 12 n.rz.; 30.8 per cent did so between 12:01 and 6 P.m.; and the remaining 23.1 percent committed suicide between 6:01 and 12 P.m.
Of the thirteen patients two had previously attempted suicide in the hospital, one had threatened but not attempted suicide in the hospital, and two others had been diagnosed as suicide risks at some time during the hospitalization period. Thus, 38.5 percent of the suicides had presented suicidal clues to the professional staff at some time prior to committing suicide.
Only five of the thirteen addict patients left suicide notes. Three of the notes were to family members, and the other two were to staff members of the hospital. Only three of the notes were available for analysis. One dealt with a fear of not being psychiatrically ready to leave the hospital, a second with despondency over physical symptoms, and the third with the shame caused to his family by his being an addict.
Of the thirteen addicts seven hanged themselves, three cut their throats, two jumped from high places, and one swallowed open safety pins. Five committed suicide in the ward bathrooms, and four did so in their own treatment rooms. One suicide occurred in a seclusion room, and one occurred in the surgical ward of the general hospital section. The remaining two suicides were jumps from high places, one from the roof and one down a stairwell.
Addiction History
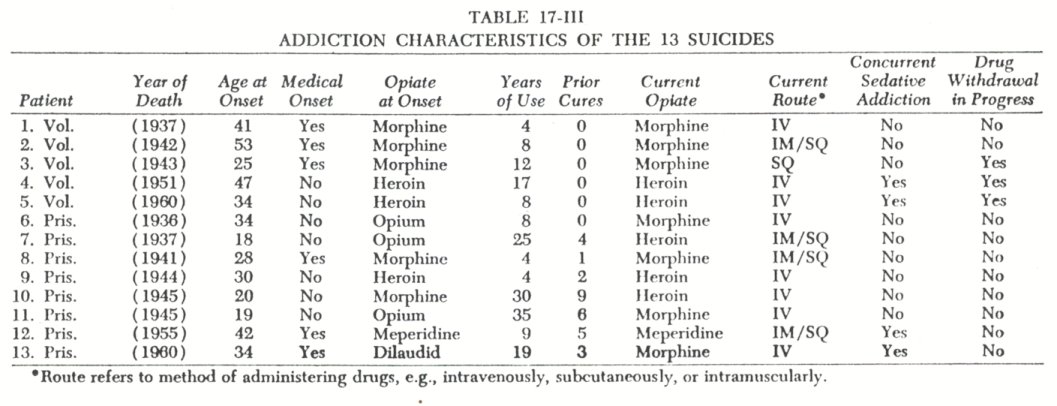
As addicts the thirteen patients who committed suicide could not be considered inexperienced to addiction, but they were somewhat inexperienced in the treatment of addiction. The patients reported addiction durations of four to thirty-five years. The average addiction duration was 14.1 years for these thirteen patients. Only 53.8 percent, however, reportedly had interrupted their addiction careers with attempts to cure themselves of their narcotic dependencies. No patient with prior experience with withdrawal committed suicide during this process, but three of the six patients who had no prior experience with narcotic withdrawal did commit suicide during the primary detoxification process.
Four of the suicides were dual addicts, being addicted to sedatives as well as opiates. Two of these four were patients inexperienced in even opiate withdrawal, and both committed suicide during the concurrent opiate-sedative withdrawal process.
Only three of these thirteen addicts had begun their drug abuse prior to becoming adults. The ages at which these addicts reported their first drug abuse ranged from eighteen to fifty-three. The mean age at onset of drug abuse for the thirteen addicts was 32.7 years. Medical onset situations were reported by 46.2 percent of the addicts as the reason for initial drug abuse; the remaining 53.8 percent reported they first abused drugs for "kicks" or out of curiosity. The thirteen suicides, in comparison to contemporary addicts, began their drug abuse rather late in life, and they more frequently reported medical onset situations. Thus, an analysis of hospital admissions in 1965 showed chat less than 10 percent of the addicts attributed their onset to medical problems.
The six addicts with medical onsets began their drug abuse with legally manufactured drugs under a physician's direction. They did not use any of the illegally manufactured drugs or purchase drugs from an illegal source at any time during their addiction careers. The seven addicts who began abusing drugs for "kicks" or out of curiosity did so primarily with illegal drugs and continued to do so throughout their addiction careers. Continuing the comparison, the "medical addicts" began their drug abuse late in life ( 37.2 versus 28.9 years of age) and had been addicts only half as long as the "nonmedical addicts" ( 9.3 versus 18.1 years).
Conclusion
Suicide is more prevalent within total institutions than in the general population, but suicide rates also vary according to the character of a total institution. The purpose of the present study was to analyze suicides which have occurred within one unique total institution: an inpatient medical and psychiatric hospital for opiate addicts.
The Lexington Hospital began admitting narcotic addicts for treatment in 1935. By 1967, 43,215 addicts had been admitted, and thirteen of these committed suicide during their hospitalization. This rate of suicide, three per ten thousand, is considerably less than rates reported for other inpatient psychiatric facilities and prisons. The rate is, however, approximately three times greater than that for the general population.
An analysis of the thirteen suicides indicates that suicides among hospitalized opiate addicts usually do not occur among the younger addicts or among the novice addicts. Suicides do occur in both sexes, in the Caucasoid, Negroid, and Mongoloid races, and among patients from all social and familial backgrounds. In addition, it was found that suicide is not associated with prisoner or voluntary status in the hospital, time of day, nor psychiatric diagnosis at admission.
As with the general population, the probable causes of suicide among hospitalized narcotic addicts are diverse. Among addict patients these causes include ( a ) the psychological and physiological discomfort of drug withdrawal, ( b ) physical illness not related to addiction, ( c ) difficulties of institutional adjustment, ( d ) the inability to accept the severity of legal punishment for crimes related to addiction, and ( e ) the inability to cope with the personal problems addiction brings to the addict and his family.
Although the suicide rate among hospitalized addicts was found to be three times that of the general population, there are indications that suicides occur even more frequently before and after hospitalization. To investigate this hypothesis, fifty female opiate addicts consecutively admitted to the Lexington Hospital were physically examined for visible signs of suicide gesturing." In this sample 14.0 percent had visible signs of prior suicide gesturing. These visible signs consisted primarily of sharp instrument wounds on the forearms. Further evidence of intent would undoubtedly be uncovered if case history material were investigated.
In addition, several studies have reported a high suicide rate among opiate addicts after hospitalization. Mason reported a suicide rate of eighty-five per ten thousand among opiate addicts of both sexes during the first year after hospitalization.' O'Donnell conducted a follow-up study of 266 Kentucky opiate addicts who had been treated at the Lexington Hospital andfound that the suicide rate was 263 per 10,000.8
Notes
1. Data from Dr. Ernest C. Siegfried, Medical Director, Federal Bureau of Prisons, indicated that for the five-year period from 1963 to 1967 suicide was the fifth leading cause of death in federal prisons, with a rate of 5.5 per 10,000.
2. For studies of suicide in mental hospitals see Levy, Sol, and Southcombe, R.H.: Suicide in a state hospital for the mentally ill.Journal of Nervous and Mental Disease, 117:504-514 1953, and Temoche, Abelardo> Pugh, Thomas F.,
and MacMahon, Brian: Suicide rates among current and former mental institution patients.Journal o f Nervous and Mental Disease, 138:124-130, 1964.
3. Although the prescribed hospital detoxification process usually requires less than two weeks, there is evidence that a stable level of certain physiological variables does not occur until four to six months after withdrawal. Thus, technically, six of the eight prisoners could have still been under withdrawal effects when they committed suicide.
4. An accurate suicide rate, over time, by status cannot be determined, since the 43,215 addicts have had 77,076 admissions to the hospital, and addicts are admitted as voluntary patients and return as prisoners and vice versa. Computing from each admission, however, the prisoner suicide rate of 4 per 10,000 is four times greater than for voluntary admissions.
5. For reports of concomitant serious illness among suicides see Dorpat, T.L.,et al.: The Relationship of Physical Illness to Suicide. In Resnik, H.L.P. ( Ed. )Suicidal Behaviors. Boston, Little, Brown and Co., 1968, pp.209-219.
6. This research was undertaken by Sheldon S. Stoffer and John C. Urbaitis. 'Mason, Perey: Mortality among young narcotic addicts.Journal of the Mount Sinai Hospital, 34:4-10, 1967.
7. O'Donnell, JohnA.: Narcotic Addicts in Kentucky. Washington, U.S. Government Printing Office,1969, Ch. 2.
| < Prev | Next > |
|---|