| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 174 |
| Yesterday: | 251 |
| This Week: | 174 |
| Last Week: | 2221 |
| This Month: | 4762 |
| Last Month: | 6796 |
| Total: | 129361 |
Chapter 6 Nativity, Parentage, and Mobility of Opiate Addicts
 |
|  |
| 
| Books - Epidemiology of Opiate Addiction in United States |
Drug Abuse
The Epidemiology of Opiate Addiction in the United States
Chapter 6
Nativity, Parentage, and Mobility of Opiate Addicts
JOAN C. BALL AND WILLIAM M. BATES
Note: Reprinted from Social Problems, Vol. 14, Summer 1966, pp.58-69, with special permission of The Society for the Study of Social Problems.
A persistent sociological thesis in both European and American studies of deviant behavior is that crime is associated with urbanization, migration, and residential mobility. In 1890 Gabriel Tarde observed that the rapidly expanding cities of Europe were centers of criminality and that "these capitals and great cities [were] having an irresistible attraction for the outcasts and scoundrels of the country, or the provinces, who hasten to them."' Emile Durkheim reported, in 1897, that high suicide rates were to be found in the metropolitan areas of France .2 By 1927 Pitirim Sorokin concluded that criminality in Western societies had been increasing and that territorial, horizontal, and vertical mobility were related to this increase of crime.3
Contemporary sociologists continue to pursue this question of the association of crime and mobility. Although it is well established that there is a preponderance of crime in urban areas,' it is recognized that the association of specific types of criminality to mobility-as well as to such other factors as sex, race, age, oroccupation-is a matter for empirical ascertainment 6 Thus, it is necessary to separately investigate the phenomenon of homicide, gang behavior, embezzlement, or prison recidivism if accurate descriptions or testable hypotheses pertaining to mobility are to be made.
Previous studies of narcotic drug addiction in the United States suggest that there is an association between residential mobility and the incidence of addiction: that addicts come from mobile unstable families," that addicts in metropolitan slums are migrants from other regions,' that areas of high drug use are also areas of marked residential mobility," that addicts migrate to urban centers to secure drugs,9 or that addicts move to metropolitan zones in transition in order to avoid detection.lo
It seems worthwhile to outline the logical relationships which may obtain between narcotic drug use and population mobility before describing the research procedure of the present study. Five preliminary factors require delineation: the family in which the addict was raised, the neighborhood or area in which he lived, the addict himself, migration or mobility of the addict prior to addiction, and his mobility after addiction. With respect to the addict (and not his family of orientation), three associations may be posited: (a) that he was mobile before addiction, (b) that addiction or drug use preceded mobility, and (c) that mobility is related to the etiology or continuation of addiction by means of an intervening variable-residence in a transient mobile area, primary group association with migrants, inability to pursue employment when addicted, or other variables. Each of thesethree statements may also be applied to the addict's family of orientation. Thus, it may be that the parents' mobility or residence in an area of high mobility was related to the subsequent drug use of their son or daughter. In addition to the distinction between the addict and his parents when considering mobility, it is necessary to note that an addict's residence in an area of high residential mobility is different from whether or not he is himself mobile."
The Research Problem
The study was designed to answer the following question: Do narcotic drug addicts come from migrant or mobile families and do they become transients after the onset of addiction? The first part of the question refers to the association between mobility and the commencement of drug use, while the latter part refers to the particular circumstance of whether or not the person is mobile after he became addicted to narcotics.
The two associations mobility before or after addiction-are empirically independent in that either, or both, may obtain. Yet, the two associations are sequential and related in the sense that mobility antedating drug use may affect mobility after addiction. In addition, the question of whether or not there is a cumulative effect of mobility after addiction has several theoretical ramifications. Thus, does the deviant once mobile become increasingly mobile? Is there adownward drift associated with a transient way of life as the addict gets older? Is mobility related to membership in the addict subculture? Is instability of residence a necessary consequence of life in a subculture in which drugs are not legally obtainable and arrests frequent? Or, conversely, does the addict once addicted stay close to a known supply of drugs? Do the members of the deviant subculture band together, at least in the sense of effecting a common identification asaddicts, and in this symbiotic relationship
realize a type of accommodation which precludes the necessity of mobility?
The Addict Sample and Data
The 925 addict patients at the hospital in Lexington on October 11, 1962, vvere selected for study, and data were compiled from each patient's medical record. These 925 hospitalized addicts were generally representative of the 2,709 addict patients admitted to the Lexington hospital during 1962, with certain qualifications. The population studied contained a larger proportion of prisoner patients, as contrasted with voluntary patients, and it included patients admitted prior to 1962 who were still hospitalized in October, 1962.12 The daily hospital population was employed in the present study for practical reasons pertaining to the identification of subjects and sample size; in addition, this selection procedure did not exclude the most permanent portion of the addict hospital population-those who were hospitalized through 1962.
Data, were abstracted from the medical records pertaining to each patient's sex, race, date of birth, parentage, nativity, exact address at time of first admission to the Lexington hospital, and, if applicable, residence at each subsequent admission.
A scrutiny of the records raised the question of the validity of the residential information provided by voluntary patients." A separate investigation of this question was undertaken, showing that 99 percent of the voluntary patients admitted by prior written application had given the same home address at the time of admittance as that to which their letter of authorization was sent." It was concluded that the residential data were valid.
Demographic Characteristics of the Addict Population
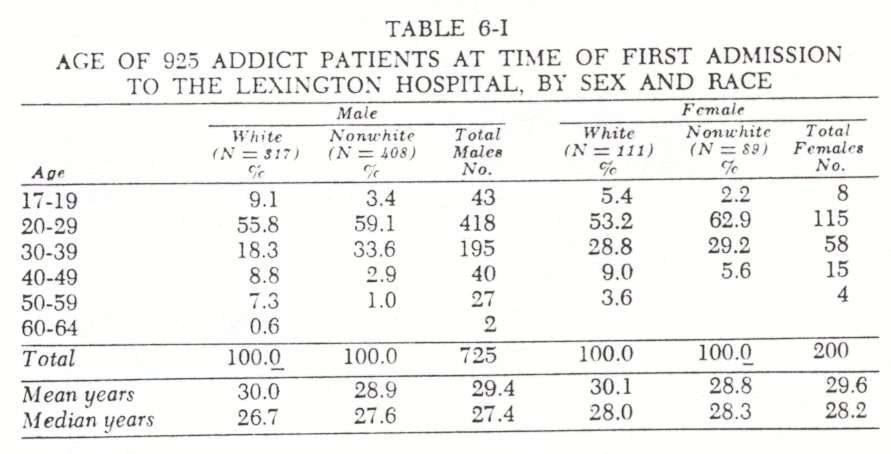
Of the 925 addict patients 725 were male and 200 female.With respect to race 44 percent of the males were white and 56 percent nonwhite. The comparable figures for the two hundred females were 55 percent white and 45 percent nonwhite. The nonwhite classification included three Chinese males and one American Indian female; otherwise, these were Negro patients.
Age at time of first admission to the Lexington hospital was not significantly different between the sexes or the two racial classes ( Table 6-I ) . The median age by sex and race at first admission was between twenty-six and twenty-eight years. Although 63 percent of the patients had a first admission before age thirty, the older group was not unrepresented. The number of white addicts admitted after age forty was significantly greater than the number of nonwhite addicts (P < .001) .
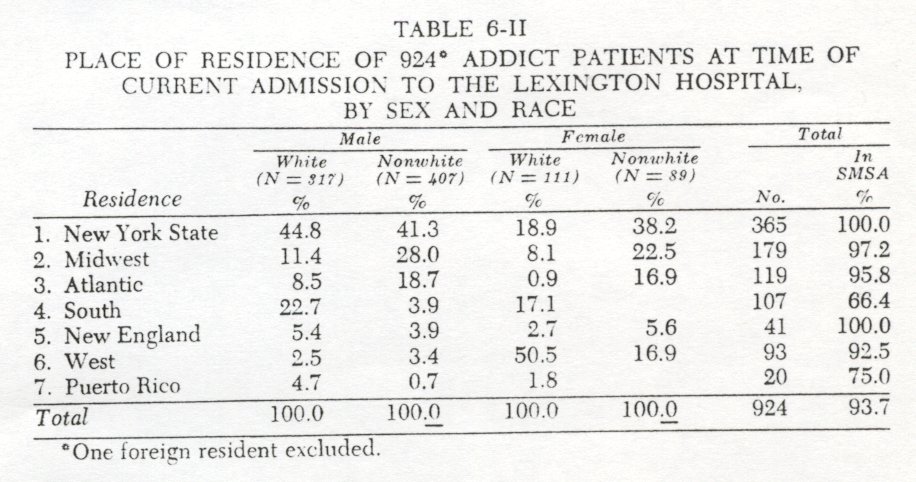
The 925 addicts were predominantly metropolitan by place of residence; 94 percent were from Standard Metropolitan Statistical Areas (Table 6-II) . By state or region 39.5 percent were from New York, 15 19.4 percent from the Midwest, 16 12.9 percent from five Atlantic States and Washington, D.C.,1' 11.6 percent from the South,i$ 4.4 percent from New England,"' 10.1 percent from the West," and 2.2 percent from Puerto Rico."
The regional variations by sex and race (Table 6-II) reflect meaningful differences in both patterns of addiction and administrative procedures. With respect to the latter the Fort Worth hospital usually receives male addict patients from west of the Mississippi River, while all female addicts are hospitalized at Lexington. Thus, a more appropriate measure of the incidence of hospitalization by state or region would be the annual number of admissions to both the Lexington and Fort Worth hospitals. In the present study of mobility, attention is on state or region primarily as these are related to the migration or mobility of addicts.
Two quite different regional patterns of narcotic addiction exist. One pattern of drug use is centered in northeastern metropolitan areas. These addicts come predominantly from the most disadvantaged minority groups-Negroes and Puerto Ricans-and are heroin users. The other pattern of narcotic addiction is typified by the southern addict who is white, more frequently from urban or rural areas (as contrasted with SMSA's ), and commonly usingmorphine, codeine, or paregoric rather than heroin.22
Nativity and Parentage of Addict Patients
Data on the nativity and parentage of the925 addict patients provided a means of tracing migration and mobility over a period of two generations. The following four variables were employed: 1) state (or country) of birth of each parent, 2) place of birth of subject, 3) residence of subject at time of first admission to the Lexington hospital, and 4) residence at time of subsequent hospital admission (if applicable). The analysis of these data considers changes from 1 to2, 2 to 3, and 3 to 4.
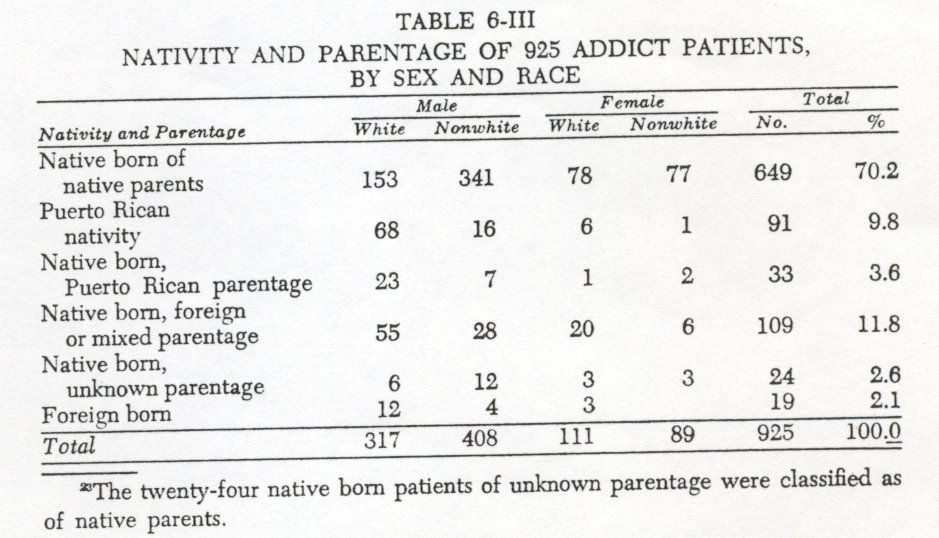
Of the 925 addict patients 97.9 percent were native born and2.1 percent foreign born. Of the native born 88 percent were of native parentage and 12 percent of foreign or mixed parentage. 23 In 1960, the United States population was 5.4 percent foreign born, and14.3 percent of the native born were of foreign or mixed parentage. The addicts, then, were not different from the general population with respect to foreign or mixed parentage, although they were less likely to be foreign born.
The Puerto Ricans were, however, overrepresented in the addict population. Of the906 native-born patients, 13.7 percent were of Puerto Rican nativity or parentage (Table 6-III) . This is seven times their proportion in the U.S. population." 'With respect to nativity alone, 10 percent of the native-born patients were from Puerto Rico.
When race, nativity, and parentage are considered together, the addict population comes disproportionately from certain minority groups of American society. Of the 906 native-born addict patients, 47.8 percent were nonwhite of native parents, 13.7 percent of Puerto Rican birth or parentage, 12 percent of foreign or mixed parentage, and only 26.5 percent white of native parents.
Migration of Addict Patients and Their Parents
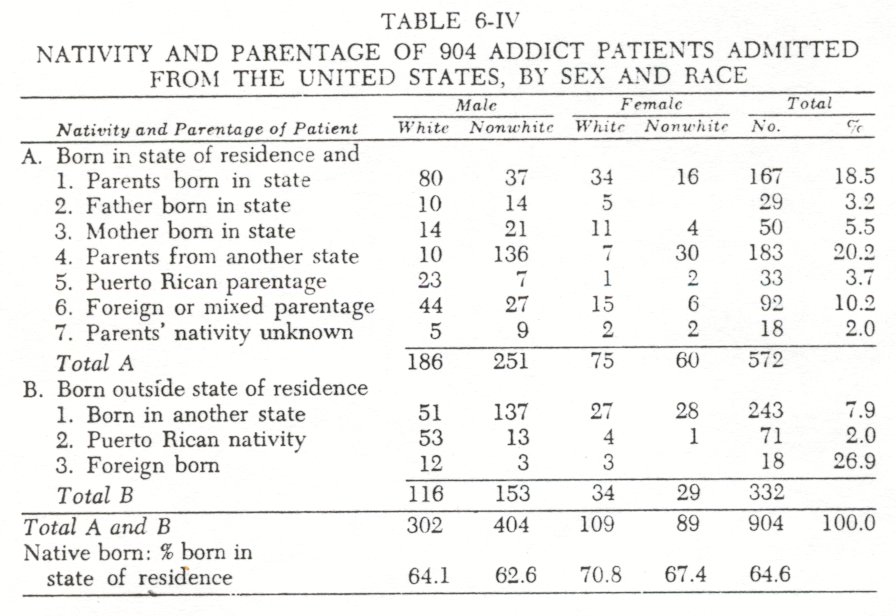
The available data afford a means of analyzing intergenerational mobility of the addict population. ( Intergenerational mobility was operationally defined as a difference between thepatient's state of birth and that of either parent.) Of the 904 patients admitted from the United States,=s 572 were born in their state of residence ( 63.3% ) . And of these, 43 percent also had one or both parents born in the same state ( Table 6-IV). The Negro addicts=' were from more migrant families than the whites. Intergenerational migration was twice as frequent among the Negroes -69.6 percent as contrasted with 39.4 percent for the whites. The association of race andmigration o f parents within the United States is even more marked when the intergenerational migration of the Puerto Rican and foreign parents is excluded, since the latter migration is more common among the whites. Thus, of the 429 native born addicts of United States parentage who were not mobile from birth to current hospitalization ( Table 6-IV Part A: 1 through 4 ), 64.3 percent of the nonwhites were born in a state different from either parent, contrasted with 9.9 percent of the whites.
Mobility: From Birth to First Lexington Hospitalization
Of the 925 addicts 35.1 percent were mobile from birth to first Lexington hospitalization. Thus, some two-thirds of the patients were born in the same state from which they were first admitted. A regional cross-tabulation of this mobility from birth to first Lexington hospitalization revealed that the male residents from New York and the Midwest were more mobile than the addicts from the South or the five Atlantic states. Thus, 40.2 percent of the New York and Midwest males were mobile ( i.e., their state of birth was different from their state of residence at time of first hospitalization), contrasted with 28.3 percent of the males from the South or Atlantic states.
The appropriate comparison with census data is afforded by an analysis of mobility from birth to current hospitalization, rather than from birth to time of first admission; the former procedure makes possible a comparison of mobility by census year, nativity, and age of subject, while the latter does not. Still, while the onecomparison is technically preferable to the other, the substantive difference is slight, since 60 percent of the addict population consisted of first admissions. (The question of mobility from first to current-1962-hospitalization is considered separately below.)
Mobility: From Birth to Current Lexington Hospitalization
Of the 886 native born addict patients who were residents of the continental United States z' in 1962, 64.6 percent were born in their state of residence. In 1960 the percentage of the native born U.S. population aged twenty to thirty-nine who were born in their state of residence was 62.8 percent for males, 64 percent for females, 64.5 percent for whites, and 55.2 percent for nonwhites .28 The present addict population, then, was not more mobile from birth to present residence than the U.S. population. Indeed, the nonwhite addicts were somewhat less mobile than the nonwhite population (Table 6-IV).
Inasmuch as there was greater mobility among the addicts who were residents of New York from birth to first hospitalization and inasmuch as they constitute 40 percent of the hospital population, a separate analysis of this group was undertaken. Of the 310 male addicts from New York State, 142 were white and 168 were nonwhite. The percentage of the white and nonwhite addicts who were born in New York was, respectively, 60.4 and 59.3.29 Compared with the New York City population in 1960, the white addicts were more mobile and the nonwhite addicts markedly less mobile from birth to present residence. The percentage of white males in New York City aged twenty to thirty-nine who were born in state of residence in 1960 was 71.53°-some 11 percent less mobility than among the white New York addicts. This higher mobility of the white addicts is primarily due to the Puerto Ricans, as fifty of the fifty-six white New York addicts not bornin the state were born in Puerto Rico. Thus, if New York residents of Puerto Rican ancestry are excepted, the white addicts were less mobile from time of birth than the comparable New York City population.
In New York City only 32.3 percent of the nonwhite males aged twenty to thirty-nine in 1960 were born in the state. The nonwhite or Negro addicts,81 then, were notably less mobile than the comparable population of New York City, as 59.3 percent of these addicts were born in the state. Although the Negro addicts from New York were themselves less mobile than the Negro population of the city, they were predominantly first generation New Yorkers. Thus, of the ninty-nine Negroes born in New York, only 25.3 percent had one or both parents born in the state. Comparable census data pertaining to parents' state of birth is not available, but there is no reason to suppose that this intergenerational mobility exceeds that of the nonwhite general population of New York City.
Of the 310 male addicts from New York, 92 (29.7%) were of Puerto Rican nativity or parentage. Some two-thirds of thesesixty-two patients-were born in Puerto Rico. Thus, addiction among the Puerto Ricans admitted to the Lexington hospital from New York is predominantly among migrants. The contrast with the Negro addicts from New York is striking, for the latter patients were New Yorkers by birth whose parents were migrants from the South. The Puerto Rican patients, however, were not more mobile from place of birth to residence in 1962 than the 629,430 Puerto Ricans living in New York City.82
Residential Mobility of Addict Recidivists
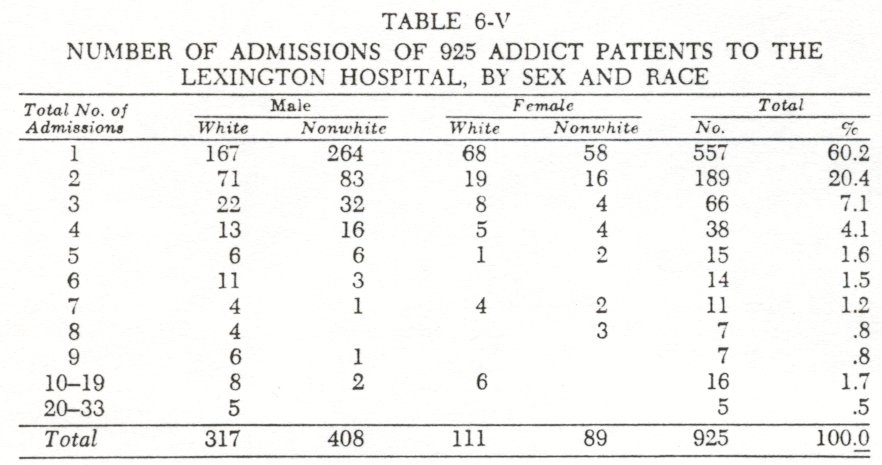
Of the 925 addict patients 60 percent were first admissions to the Lexington hospital, 20 percent were second admissions, and 20 percent had three or more admissions (Table 6-V). The residential data afforded a means of delineating and analyzing the mobility of the recidivists from time of first admission to 1962. From purpose of analysis, the 368 recidivists were divided into two groups: (a) those with two admissions, and (b) those with three or more admissions.
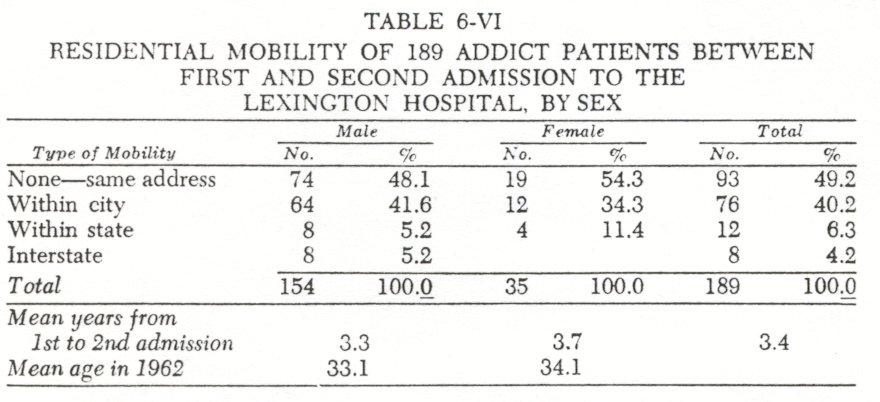
The 189 addict patients who were hospitalized at Lexington for a second time in 1962 were 3.6 years older than the 557 first admissions. With respect to characteristics other than age, sex, race, and place of residence- the two groups did not differ significantly. The mean time between first discharge and second admission to Lexington for the recidivists was 3.4 years.
With respect to residential mobility in this three-year period, the two admission recidivists were not more mobile than the U.S. population. A comparison with census tabulations indicated thatthese addict recidivists were less likely to be interstate migrants than the general population but as likely to be local movers. Thus, of the 189 addicts of both sexes, 49 percent resided at the same address in the three-year period, 40 percent had moved within the city, 6 percent had moved within the state, and 4 percent were interstate migrants ( Table 6-VI). By comparison, in a oneyear period, 30.2 percent of the U.S. male population aged twenty-five to thirty-four were movers; this included 19.9 percent local movers, 4.7 percent intrastate movers, and 5.6 percent interstate migrants." During this one year ( April 1961-April 1962 ), then, 10.3 percent of the U.S. males aged twenty-five to thirty-four were out-of-county migrants, while only 10.5 percent of the addicts were out-of-city migrants during the three-year period. Further, in a five-year period, 1955 to 1960, 17.4 percent of the U.S. population aged five years and over in SMSA's were out-of-county migrants.3#
Local residential mobility among the 189 addicts is similar to that of the U.S. population, although there were indications that the addicts would be less mobile than the general population if unemployment, socioeconomic status, race, and city were controlled. With respect to the U.S. population in 1960, 44.1 percent had moved to a different residence since 1957 ~5 Of unemployed males aged twenty-five to thirty-four in the United States, however, 41.6 percent were movers in a single year.3ó Considering that 46 percent of the 725 male addicts were unemployed or engaged in illegal pursuits, that Negroes in the Northeast and North Central Census regions are almost twice as mobile as whites, and that manual and service workers are more mobile than white collar workers," it is reasonable to conclude that the 189 addict recidivists were no more likely to be either local movers or outof-county migrants than the comparable U.S. population.
Mobility of the Multiple Addict Recidivists
Of the 925 addict patients at the Lexington hospital on October 11, 1962, 179 had from three to thirty-three admissions. Thus, some one-fifth (19.4 percent) of the hospital population consisted of these multiple recidivists. Analysis of mobility within this group has particular significance, as it may suggest long-term effects of narcotic addiction upon stability or instability of residence as well as indicate whether the multiple admission addicts differ from those who were not recidivists 38
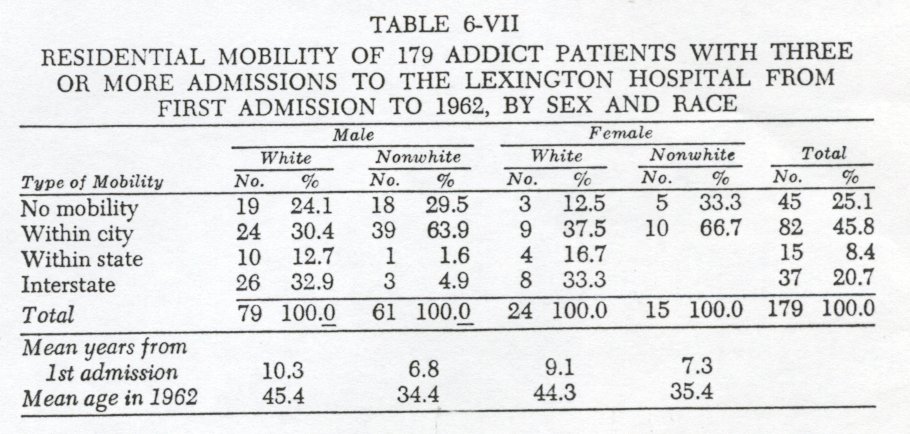
The addict patients with three or more admissions were similar to the first and second admission groups with respect to parentage, nativity, and mobility from birth to first admission, except that intergenerational migration was less among the former (i.e., the multiple recidivists were more likely to reside in their parents' state of birth). The sex, race, and regional composition of the multiple,recidivist group were also quite similar, with the exception of the increased representation of southern white addicts in this group $y As expected, the multiple recidivists were older in 1962 (Table 6-VII). Unexpectedly, however, they were not younger at time of first Lexington hospitalization. Indeed, the white multiple recidivists-but not the Negroes-were older at first admission than patients first admitted in 1962.4° Principally, this reflects the older age at which southern addicts were first hospitalized.
The pattern of residential mobility among the 179 multiple recidivists differed markedly by race but not by sex. Of the seventy-nine white male addicts, 46 percent were out-of-citymigrants during the ten-year period, contrasted with 7 percent of the sixty-one Negro males. Conversely, the Negro addicts were more frequently local movers-64 percent versus 30 percent among the males.
Of the 179 multiple recidivists, 37 were interstate migrants. The question arises as to whether or not these were frequent movers. Analysis of these thirty-seven interstate migrants showed that 49 percent had made only one such move and only three patients had moved four or more times. With respect to intrastate migration, the findings on the number of moves per addict were similar: only a minority of the 142 multiple recidivists (who were not interstate migrants) were mobile within state during the 9year period (10.6%), and of the 15 who moved, only 3 moved more than twice.
A cross-tabulation of region, age, and number of hospital admissions was undertaken among the seventy-nine white male multiple recidivists to ascertain whether any of these variables had a particular association with mobility. It was found that the thirty-eight male white addicts from the South were more often interstate migrants than the non-southerners (42% versus 24%) but that this was a consequence of a longer period between first and present hospitalization-thirteen years for the southerners versus eight years for the non-southerners. Although white male addict patients with ten or more admissions to the Lexington hospital were also more frequently interstate migrants than those with fewer admissions, their advanced age (60.5 years) and longer period between first and current hospitalization (19.1 years) precluded further statistical comparison. It may be that this increased mobility among the older patients is related to the similar increased mobility of the aged in the U.S. population."
From an analysis of the available data, it is concluded that the multiple recidivist addicts were somewhat less mobile than the U.S. population. Thus, in a ten-year period, 29.1 percent of the 179 addicts were out-of-city migrants (Table 6-VII), contrasted with 35.8 percent of the U.S. population who were migrants in a five-year period.'' An additional analysis of mobility from birth to first admission and from first to second admission supports the findings that these addicts were not a mobile population .43
Interpretation of the Research Findings
An unequivocal answer to the question of the mobility of narcotic drug addicts in the United States is suggested by the data: Drug addicts are not more mobile from birth to the onset of addiction than the U.S. population, and they do not lead a transient way of life after their initial hospitalization. Despite this general statement of the absence of association between drug addiction and mobility, quite distinct patterns of population movement were found among the several ethnic groups.
As previous studies have indicated, narcotic addiction is essentially an urban phenomenon concentrated in the largest cities of the United States. In these urban slums, narcotic drug abuse is most prevalent among the more disadvantaged minority group members, particularly Negroes and Puerto Ricans. The Negro addicts of the present study were second-generation migrants to the northeastern metropolitan centers, whereas the Puerto Rican addicts were first-generation migrants. In both instances the addicts were not more mobile than their respective base populations-northern Negroes or New York City Puerto Ricans.
The white addicts were not only themselves stable in place of residence since birth but there was considerable intergenerationalstability. Among those white patients who did move, out-of- county migration was frequent; conversely, among the Negro patients, intracity mobility was the dominant change of residence noted. These racial differences in mobility patterns are similar, though more marked, than those of the U.S. population reported in the 1960 census.
Surprisingly, there were no notable sex differences in mobility among the 925 addicts studied. Indeed, the females appeared to be a microcosm of the male macrocosm with regard to mobility patterns. This is somewhat surprising in view of the prevalence of prostitution among the female addicts .'4
In considering the findings of the present study and in reviewing the criminological literature, it appears that the relationship of mobility to crime and deviant behavior has been oversimplified and ambiguously presented. Thus, it is not sufficient to note that deviant individuals come from neighborhoods with high rates of residential mobility; it must be demonstrated either that these persons were themselves mobile or that their deviance is related in a definite manner to the instability of others.
It seems likely that the urbanization of western society, with its attendant mobility, has been instrumental in prompting the belief that crime is associated with instability of residence. In addition, the stereotype in literature and folklore of the nefarious foreigner may not have been without its effect. The outlaw, the cutthroat, the spy, the bandit, the prostitute, and the pirate have commonly been regarded as outsiders-as mobile persons without roots who invade the local community to prey upon the citizenry.
The extent to which residential mobility is an attribute of crime or follows as a consequence of crime is a question that can most effectively be answered within an empirical framework in which specific types of crime or deviant behavior are studied. The evidence amassed to date indicates that the vast bulk of urban crime is committed by local residents. It may be that particular crimes or modes of deviant behavior are associated with the prior, or subsequent, mobility of the person involved. From the present study there is no evidence that such a relationship exists amongdrug addicts in the United States.
1. Tarde, Gabriel. PenalPhilosophy. Boston, Little, Brown and Co., 1912, p.338.
2. Durkheim, Emile: Suicide. Glencoe, Ill., The Free Press, Appendix 1.
3. Soroldn, Pitirim: Social Mobility. New York, Harper and Brothers, 1927, pp.381f., 527-528.
4. Clinard, Marshall B.: Sociology of DeviantBehavior. New York, Holt, Rinehart and Winston, 1963, Ch. 3.
5. Wolfgang, Marvin E., Savitz, Leonard, and Johnston Norman (Eds.):The Sociology of Crime and Delinquency. New York, John Whey and Sons, 1962, Section IV.
6. Chein, Isidor, Gerard, Donald L., Lee, Robert S., and Rosenfeld, Eva: TheRoad to H. New York, Basic Books, 1964, pp.47-57, 125.
7. Anslinger, H. J.: Narcotic addiction as seen by the law-enforcement officer.Federal Probation, 21:34-41, 1957; Finestone, Harold: Cats, kicks, and color.Social Problems, 5:3-13, 1957.
8. Dai, Bingham: OpiumAddiction in Chicago. Shanghai, China, The Commercial Press, 1937, pp.76-79; Clausen, John A.: Social and psychological factors in narcotics addiction.Law and Contemporary Problems, 22:34-51, 1957.
9. Lindesmith Alfred R.: Narcotic Addiction. In Burgess, Ernest W., and Bogue, Donald J. (Eds.) : Contributionsto Urban Sociology. Chicago, University of Chicago Press 1964, p. 627.
10. Faris, Robert E., and Dunham, H. Warren:Mental Disorders in Urban Areas. Chicago, University of Chicago Press, 1939, Ch. VI, pp.110-123.
11. For a discussion of this topic see Clausen, John A., and Kohn, Melvin L.: The ecological approach in social psychiatry. American Journal of Sociology, 60: 140-151, 1954.
12. Of the 925 patients . . . 499 were prisoners and 426 were voluntary admissions. Of the 499 prisoners 23 7 were admitted to the Lexington hospital before 1962.
13. For Federal prisoners the presentence report and collateral data provided ample verification of the subject's place of residence.
14. Of 574 voluntary Lexington first admissions in 1961, 402 were admitted with prior written authorization. A 25 percent random sample of these 402 addict patients showed that 97 of the 98 had the same address on their application for admission as that given at the time of hospitalization.
15. All but 6 of the 365 addicts from New York State were residents of the New York, N.Y. SMSA; these 6 were from upstate SMSA's.
16. The East North Central Census Region: Wisconsin, Michigan, Illinois, Indiana, and Ohio.
17. Delaware, Maryland, New Jersey, Pennsylvania, and West Virginia.
18. The following states: Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, Tennessee, and Virginia.
19. Only Massachusetts and Connecticut were represented in the hospital population.
20. This includes states west of the Mississippi River.
21. These were residents of Puerto Rico at time of current-1962-hospitalization.
22. See Chapter 5.
23. The twenty-four native born patients of unknown parentage were classified as of native parents.
24. The 1980 population of Puerto Rico was 2,349,544; in addition, 892,513 persons of Puerto Rican birth or parentage lived throughout the U.S. in 1980. Thus, 1.8 percent of the U.S. population ( including Puerto Rico) was of Puerto Rican nativity or parentage. U.S. Bureau of the Census: U.S. Census ofPopulation: 1960, Subject Reports, Puerto Ricans in the United States. Final Report PC ( 2 )1D, Table 1, p.2.
25. The twenty patients admitted from Puerto Rico were excluded in order to effect a comparison with the 1960 census data.
26.In Table 6-IV all of the 251 male nonwhite addicts "born in state of residence" were Negro, and 59 of the 60 female nonwhites were Negro.
27. Excluding Puerto Rican residents in order to facilitate census comparison.
28. U.S. Bureau of the Census: U.S. Census of Population: 1960, Detailed Characteristics, United States Summary, Final Report PC(1)-1D, Table 161.
29. This was percentage of native born who were born in state of residence; this was 84 of 139 for the whites and 99 of 167 for the non-whites.
30. U.S. Bureau of the Census: U.S. Censusof Population: 1960, Detailed Characteristics,New York, Final Report PC(1)-34D, Table 98.
31. Of the 168 nonwhite patients, 167 were Negro; one was a foreign-born Chinese addict.
32. In 1960, 69.8 percent of the New York City population of Puerto Rican ancestry were born in Puerto Rico. U.S. Bureau of Census: U.S. Censusesof Population and Housing: 1960, Census Tracts. Final Report PHC(1)-104, Part 1, Table P-1, p.23.
33. Mobility of the Population of the United States, April 1961 to April 1962.Current Population Reports, Bureau of the Census, Series P-20, No. 127, January 15, 1964, p.14.
34. U.S. Bureau of the Census: U.S.Census of Population: 1960,General Social and Economic Characteristics, United States Summary, Final Report PC( I )-1C, Table 141.
35. bid., Table 113.
36. Current Population Reports. op. cit., Table 5, p.27.
37. Ibid., pp.1,8.
38. This contrast between recidivists and first admissions is not merely a comparison between patients who were recidivists in 1962 with those who will become recidivists (the 1962 first admissions) in the future, since most of the first admissions do not return to the hospital. The yearly readmission rate for Lexington male addicts from 1935 through 1949 was between 36.5 percent and 50.8 percent. Thus, 56.8 percent of the 11,744 male addicts admitted during this fifteen-year period have not returned to the hospital.
39. Of the 557 first admissions . . . 7.0 percent were from the South; of the 179 multiple admission addicts, 28.3 percent were from the South.
40. The 79 white male multiple recidivists had a mean age at first admission of 34.5 years; the mean age of the 24 white females was 34.0 years.
41. Current Population Report, op. cit., p.3.
42. U.S. Census o f Population: 1960, General Social and Economic Characteristics, United States Summary, Final Report PC(1)-1C, Table 101.
43. Thus, 64.4 percent of the 177 native-born multiple recidivists (2 were foreign born) were born in their state of current residence.
44. On the geographical mobility of prostitutes, see Lemert, Edwin M.: Social Pathology. New York, McGraw-Hill, 1951. pp.241,275,280.
| < Prev | Next > |
|---|