| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 174 |
| Yesterday: | 251 |
| This Week: | 174 |
| Last Week: | 2221 |
| This Month: | 4762 |
| Last Month: | 6796 |
| Total: | 129361 |
Chapter 5 Two Patterns of Opiate Addiction
 |
|  |
| 
| Books - Epidemiology of Opiate Addiction in United States |
Drug Abuse
The Epidemiology of Opiate Addiction in the United States
Chapter 5
Two Patterns of Opiate Addiction
JOHN C. BALL
Note: Reprinted fromThe Journal of CriminalLaw, Criminology and Police Science, 56:203-211, 1965.
Evidence from the present study and a review of the literature support the thesis that two quite distinct .patterns of narcotic drug addiction exist in the United States at the present time. One addiction pattern is followed by young heroin users who come predominantly from metropolitan centers and are engaged in illegal endeavors. The other pattern is typified by the middleaged southern white who uses morphine or paregoric and obtains his drugs through legal or quasi-legal means. The heroin pattern of addiction has increased markedly since World War II and is currently associated with minority group status. The second type of addiction preceded the passage of the Harrison Act in 1914 and has, in the subsequent years, decreased materially.
The medical records of3301 addict patients discharged from the hospitals at Lexington, Kentucky, and Fort Worth, Texas, during the 1962 fiscal year were analyzed with a view toward delineating these two patterns of drug addiction. A part of the study consists of a comparison of this1962 population with the hospital population in1937.
The Changing Pattern of Opiate Use in the United States
Opium has been extensively used throughout much of the world since preclassical times. Its use has been associated with a diversity of cultural patterns (medical, religious, literary, and criminal) and has, in modern times, often reflected the technical and scientific advances in medicine and pharmacology with respect to the particular drug taken and the means of administration employed by the user. Thus, the invention of the hypodermic syringe facilitated both the medical and nonmedical use of opiates in the United States after 1856. The practice of opium smoking became somewhat of a vogue among the demimonde of San Francisco after 1868 and spread rapidly thereafter throughout the country. The discovery of a new opium derivative, heroin, in Germany, in 1898, had a far-reaching effect upon twentieth century drug addiction in the United States.' In addition, government prohibition has affected the use of narcotic drugs. The Harrison Act of 1914 and subsequent Federal and state laws have had a pervasive and continuing effect upon the availability of opiates and similar synthetic drugs. In sum, drug addiction as a medical problem and behavioral phenomenon is entwined in the fabric of society and, consequently, is affected by changes in society. From the end of the Civil War to the passage of the Harrison Act in 1914, the use of opiates in the United States was widespread and virtually uncontrolled. Tern and Pellens estimated that a minimum figure for the United States was 264,000 addicts in 1920.' Opiates were readily available during this period from druggists, some physicians, and over-the-counter sales in general stores. The illicit traffic within the country was, apparently, negligible and confined to such prohibited opiates as smoking opium after 1909; but information is meager in this regards
The Harrison Act of 1914 had two effects upon drug addiction in the United States. First, it largely eliminated the indiscriminate sale of opiates through legal channels. And second, it had the indirect effect of making the illicit sale of opiates, and especially heroin, profitable. Thus, an illicit pattern of drug use was superimposed upon the preexisting licit, or uncontrolled, pattern of opiate use.6 What has happened to these diverse but related types of narcotic addiction during the past twenty-five years is the subject of this paper.
Selection of the Hospital Population of 3301 Patients
Two types of addict patients were admitted to the Lexington and Fort Worth Hospitals: voluntary patients and prisoners.' The voluntary patients constituted the majority (84.6% in 19628) . They were voluntary with respect to their admission and in that they could leave at any time after treatment had begun. The addict prisoners had been sentenced by federal courts and were serving designated sentences.'
The subjects selected for study were all female and male addict patientsl° discharged from the two hospitals between. July 1, 1961, and June 30, 1962. There were 2713 males and 5&1i females discharged during this twelve-month period. The figure of 3301 refers to the number of individuals discharged from the hospitals, not the number of separate discharges. This distinctionis of some significance, as there were 230 more discharges than persons; that is, some6 percent of the patients were at the hospital more than once in1962.11
A comparison of the addict patients at the two federal hospitals in1962 with the addict patients at the Lexington Hospital in1937 is meaningful because in1937 the Fort Worth Hospital had not opened, and therefore, male addict patients from throughout the United States were sent to the Lexington Hospital. This comparison between the1937 and1962 addict populations is only possible with respect to male addicts, since female addicts were not admitted until1941.
First Drug Diagnosis of 3301 Hospitalized Addict Patients
Only persons addicted to narcotic drugs and synthetic analgesics are eligible for voluntary admission and treatment at the two federal hospitals.12 At the time of admission each patient is given a medical examination, and subsequently, on the basis of clinical evaluation on the withdrawal ward, the physician records a drug diagnosis. This diagnosis indicates the drug or drugs used by the patient immediately prior to hospital admission and for which treatment was provided. A patient may have one, two, or three separate drug diagnoses depending upon whether he was using or addicted to one, two, or three drugs at the time of hospitalization.
The first drug diagnosis commonly refers to the narcotic drug use which provides the legal basis for hospitalization as well as to the drug of primary addiction. Thus, a patient who was addicted to heroin before admission and was not using other drugs would have only a first diagnosis of heroin addiction. If he were also using barbiturates, this would be recorded as a second drug diagnosis. If he were using heroin, Dilaudid, and barbiturates and his principal opiate use was heroin, he would have a first diagnosis of heroin use, a second of barbiturate use (if this were of second importance), and a third indicating Dilaudid use. A patient may then have one, two or three separate drug diagnoses. All addict patients have at least a first druig diagnosis in as much as drug use is the reason for hospital admission.
The second drug diagnosis usually refers to a concomitant addiction to a narcotic drug; 26.1 percent of the 3301 patients had such a diagnosis. A third diagnosis (present for 2.0% of the patients) would only be recorded if the patient were addicted to, or using three drugs.
In the subsequent analysis, attention is directed to the first hospital drug diagnosis, as it indicates the principal drug used by patients. The second (and third) drug diagnosis is not without clinical significance, but it affects only some one-fourt of the patients.
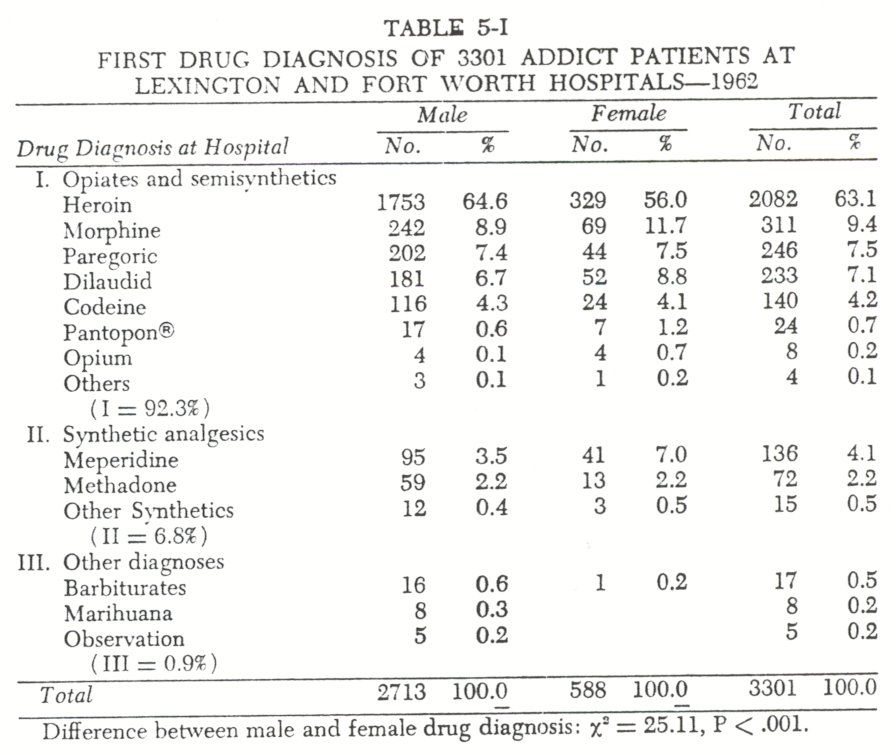
Of the 3301 addict patients discharged in 1962, 63.1 percent had a first drug diagnosis of heroin use prior to admission (Table 5-I) . The next most frequent drug used was morphine (9.4%) , followed by paregoric, Dilaudid, codeine, meperidine, and methadone. The remaining drugs listed in Table 5-I were used b1· less than 3 percent of the patients. Thus, 97.5 percent of the addict patients were diagnosed as using seven drugs; five of these were opium derivatives, two were synthetic analgesics.
The overall similarity of narcotic drug use by female and male patients was more striking than the small differences tabulated, despite the fact that the sex difference was statistically significant. Females were generally addicted to the same drugs as the males, and in both instances heroin was the predominant drug of addiction.
With respect to the thirty patients who were not diagnosed as addicted to opiates-Classification III, Table 5-1-eight were marihuana users, and seventeen were barbiturate users; five were "under observation for addiction." It should not be inferred from this that the use of marihuana and barbiturates is negligible among the 3301 addicts. A sizeable proportion, perhaps a majority of these patients, have smoked marihuana,l3 but the hospital drug diagnosis commonly makes reference only to their opiate addiction. Of the 3301 patients 21.0 percent had a secondary drug diagnosis which specified that barbiturates had also been used prior to hospitalization. 14
Several drugs under federal control were conspicuous by their absence. There were no first drug diagnoses of cocaine, metopon, or peyote use."
A comparison with Pescor's tabulation" of the 1,036 maleadmissions to the Lexington Hospital during the 1937 fiscal year reveals that the use of heroin during this 25-year interval has increased (from use by 43.3% of the male patients to use by 64.6%), while the use of morphine has markedly decreased (from 50. 7 % to 8.9%). It appears that two principal changes have occurred in drug use among these patients since 1937. First, there has been a decrease in the use of morphine and a corresponding increase in the use of opium derivatives or synthetic analgesics. Second, the use of the underworld drug of choice-heroin-has increased until it is now the principal addicting opiate in the United States."
To what extent this change in drug use during the 25-year period reflects a shift in the composition of the hospital population itself, or to what extent it is due to changes in the availability of particular opiates, is uncertain. It seems evident, however that both of these changes are important, since the number of patients treated has increased (from 1,036 to 3,301), and their social characteristics are now quite different from 1937; further, new drugs have come into manufacture and use.
Demographic Changes in the Pattern of Opiate Addiction
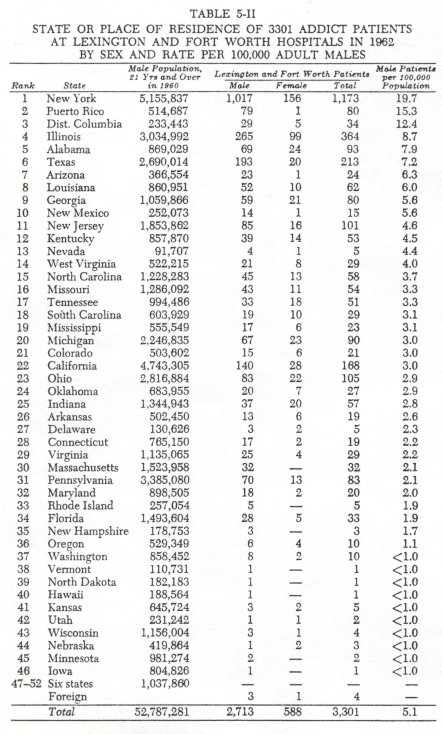
In considering narcotic addiction as a national problem, it is meaningful to note and consider the geographic distribution of patients at the two U.S. Public Health Service Hospitals. The rate of male addict patients per 100,000 population for each state is shown in Table 5-II. New York, Puerto Rico, and the District of Columbia have markedly higher rates than the rest of the United States. The first twelve states (10 states, the District of Columbia, and Puerto Rico) contribute 70.9 percent of the male narcotic patients at the two federal hospitals. Conversely, there were no patients from six states: Alaska, Idaho, Maine, Montana, South Dakota, and Wyoming.
A comparison of the 1962 geographic distribution with Pescor's data reveals a marked change in the hospital population.In 1937 the highest rates of admission were from the southern states.18 Thus, what has occurred since 1937 has been a substantial increase in the number of patients from northern metropolitan centers." The rates of hospitalization for patients from New York and Illinois now exceed those for any of the southern states. Still, the high southern rates of admission have continued, although their relative quantitative significance has diminished because of the recent influx of young addicts from the largest cities.'
The change in place of residence of the addict patients between 1937 and 1962 has been accompanied by shifts in age and race. The median age of the 2713 male patients in 1962 was 30.2 years, and the mean was 33.5 years. The range was from seventeen through seventy-eight years. Patients less than thirty years of age constituted 49.3 percent of the total male population. In 1937 the median age of males was 38.3, the mean 39.1. Only 19.7 percent of the male patients were under thirty years of age?1 Thus, the median age has decreased by eight years. During this period the median age of males in the United States has remained fairly constant: in 1930 26.7 years, in 1940 29.1, in 1950 29.9 and, in 1960 28.7.
The racial and ethnic composition of the hospital populationhas altered markedly during this 25-year period. In 1937, 88.4 percent of the male patients were white, 8.9 percent Negro, 1.2 percent Mexican, and, together, Chinese, Japanese, and Indian were 1.5 percent." In 1962, 51.0 percent of the male patients were white, 30.4 percent Negro, 12.2 percent Puerto Rican, 4.9 percent Mexican, and others 1.5 percent. There has, then, been a notable increase in the number of addicts from the minority groups in American society.
First Drug Diagnosis of Patients From Twelve States
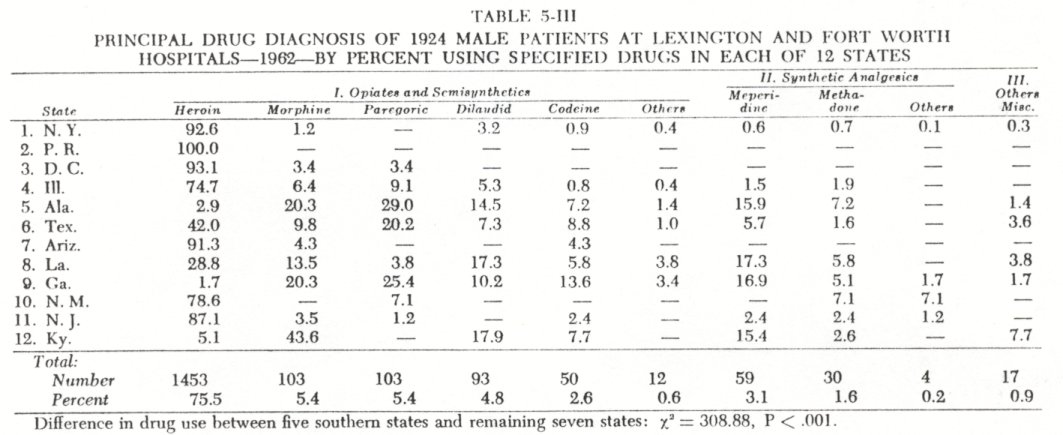
States with high rates of narcotic addiction-as here measured-fall into two contrasting patterns with respect to drug use. One pattern consists primarily of the use of heroin; this drug is neither legally manufactured nor sold in the United States. This is the dominant pattern of use in New York, Puerto Rico, the District of Columbia, Illinois, New Jersey, Arizona, and New Mexico (Table 5-III) .
The 'second pattern of drug use consists of the use either of opiates other than heroin or synthetic analgesics. Of the twelve states (or places) with highest discharge rates from the two hospitals in 1962, most of the addicts were not using heroin in five of these states. This pattern of addiction which, for want of a better name, may be termed a southern pattern, inasmuch as it is most evident in this part of the country, is exeinplified by Alabama, Georgia, and Kentucky. From each of these states, 5 percent or less of the patients were using heroin.
It may be noted that there is a heroin belt along the Mexican border states of Arizona, New Mexico, and Texas. In the case of Texas, and Louisiana to a lesser extent, it appears that the heroin pattern of use is being superimposed upon the older pattern of paregoric, morphine, codeine and Dilaudid use.
A further delineation of these two principal patterns of drug use is afforded by a comparison of age, race, and prisoner status among patients from the two groups of states. The median age at admission of patients from New York, Puerto Rico, the District of Columbia, and Illinois was, respectively, twenty-seven, twenty-four, twenty-nine, and thirty years; the comparable median figures for Alabama, Georgia, and Kentucky were forty-three, forty-three, and forty-four years. With respect to racial or ethnic composition, some two-thirds of the patients from New York, the District of Columbia, and Illinois were Negro or Puerto Rican .2' Conversely, among the patients from Alabama, Georgia, and Kentucky more than 90 percent were white.25
That the heroin pattern of drug use is more closely associated with criminal endeavors than the older nonheroin pattern may be inferred from the fact that 91.3 percent of the male prisoner patients have a first drug diagnosis of heroin use, while only 59.5 percent of the voluntary patients were heroin users. Even more revealing is the fact that the voluntary male patients used 96.0 percent of all drugs other than heroin reported in the first diagnosis.
Interpretation of Research Results
The two patterns of drug use reported here would appear, in part, to be a continuation of those described by Lawrence Kolb (1928 ), by Terry and Pellens (1928 ), and subsequently by others. Kolb classified addicts into two groups: dissipators and those medically indueed.2g Terry and Pellens inThe Opium. Problem primarily depict the nonheroin user who secures his drugs through legal or quasi-legal channels, although they do refer to the increasing use of heroin in the underworld. 27 More recently, Chapman has described both the southern addict group and thelarge city addicts from minority groups?8
What has occurred since the 1920's is the increased use of heroin among addicts and the concentration of this type of addiction among Negro, Puerto Rican, and Mexican 211 youth in metropolitan slum areas. Thus, of the Negro, Puerto Rican, and Mexican patients discharged from the two hospitals in 1962, 92.9 percent of the males and 94.3 percent of the females were heroin users. By contrast, only 37.3 percent of the white males and 25.2 percent of the white females were heroin users. As Clausen has observed, addiction in the United States has now become "clearly entwined with minority group status."3°
More detailed information pertaining to the two general patterns of opiate addiction is evident from the initial results of two follow-up field studies of former addict patients at the Lexington Hospital. In a follow-up study of 266 former addicts from Kentucky, it has been found that most of these white former patients secured their morphine, Dilaudid, or codeine, as well as considerable quantities of barbiturates, from legal or quasilegal sources." Conversely, in a follow-up study of 245 former patients from Puerto Rico, the predominant drug is heroin, and it is secured through illegal sources. 2
A comparison with the active file of the Federal Bureau of Narcotics reveals that their population of 47,905 addicts is quite similar in composition to the prisoner population at the Lexingtonand Fort Worth Hospitals, but not to the voluntary population.
Thus, 92.7 percent of the 47,905 addicts in their file were heroin users; their addict population is 18.2 percent female, and 72.7 percent Negro, Mexican, or Puerto Rican." Underrepresented or excluded from their compilation is a considerable group of nonheroin addicts."
Conclusion
Analysis of the medical records of 3301 addict patients discharged from the Lexington and Fort Worth Hospitals in 1962 reveals that two quite distinct patterns of opiate addiction exist in the United States. One pattern of addiction consists of heroin use among metropolitan youth who came predominantly from the minority groups in American society. The other pattern of addiction consists primarily of middle-aged whites who use opiates other than heroin or synthetic analgesics; this second pattern 4f addiction is concentrated in the southern states.
A comparison of the addict patients at the two hospitals in 1962 with the 1937 hospital population described by Peseor reveals that marked changes have occurred during this 25-year period. The male patients are younger by some eight years. The use of heroin prior to admission has increased, while the use of morphine has decreased. The proportion of the patients who come from northern metropolitan centers has increased notably; still, high rates of hospitalization have continued from many of the southern states. Thus, the major change has been the increasing preponderance of heroin addicts from the minority groups of ourlargest cities.
1Terry, Charles E., and Pellens, Mildred-The Opium Problem. New York, Bureau of Social Hygiene, 1928, Ch. 2; Dai, Bingham: OpiumAddiction in Chicago. Shanghai, China, The Commercial Press, Ltd., 1937, Ch. 1 and 2; Eddy, Nathan B.: The history of the development of narcotics.Law and Contemporary Problems, 22:3-8, 1957.
2. Four principal federal statutes control narcotic drugs and marihuana use in the United States. These are the Narcotic Drugs Import and Export Act, as amended (21 U.S.C. Sec. 171-185 [19581); the Harrison Narcotic Law (26 U.S.C. Sec. 4701et seq. [19581); the Narcotics Manufacturing Act of 1960 (21 U.S.C. Sec. 501 (Suppl. 19621); and the Marihuana Tax Act (26 U.S.C. Sec. 4741et seq. [ 19581 ) .
3. For a discussion of the factors affecting the change in public attitudes toward opiate addiction during the past century see Isbell, Harris: Historical Development of Attitudes Toward Opiate Addiction in the United States. In Farber, Seymour M., and Wilson, Roger H. L. (Eds.) : Conflictand Creativity. New York, McGrawHill, 1963, pp.154-170.
4. Terry and Pellens,op. cit., p.41.
5. Ibid, 1; Eldridge, WilliamB.: Narcotics and the Law. Chicago, American Bar Foundation, 1962, pp.7-9.
6. In addition, the passage of the Harrison Act resulted in a redefinition of opiate addiction; it became a criminal endeavor rather than a mere social problem. See Eldridge,op. cit., p.9.
7. The prisoner classification as herein employed includes both prisoners and probationers.
8. Of the 2,713 male patients 2,277 (83.9%) were voluntary; of the 588 female patients 516 (87.8%) were voluntary.
9. The federal prisoners may or may not have been sentenced for offenses pertaining to the narcotic laws, but they may be sent to Lexington or Fort Worth if there is evidence that they were addicted to narcotics.
10. Following hospital usage the tern patient herein refers to any resident, whether voluntary patient or prisoner.
11. Of the 3,301 patients 3,093 (93.7%) were discharged only once in 1962, 189 twice (5.7% ), 16 three times (0.5% ), and 3 patients were at the hospital four times during the year.
12.Persons who habitually used the following drugs were eligible for treatment by the Public Health Service: cocaine, coca leaves, codeine, Dicodid®, Hycodan®, Dilaudid, heroin, marihuana, laudanum, meperidine, methadone, metopon, morphine, opium, Pantopon, paregoric, peyote, NU-2206, and any other narcotic drug which may be brought under the Harrison Narcotic Act.
13. For a discussion of this issue, see Chapter 7.
14. Of the male patients 19.8 percent had a secondary drug diagnosis of barbiturate use; of the females 26.7 percent had a similar secondary diagnosis. For a discussion of research findings pertaining to opiate and barbiturate addictions, see Chapter 8.
15. There were, however, six second drug diagnoses of cocaine use and one of peyote use.
16. Pescor, Michael J.: A Statistical Analysis of the Clinical Records of Hospitalized Drug Addicts. PublicHealth Reports, Suppl. No. 143, 1943, p-24.
17. Of the 47,905 addicts in the Federal Bureau of Narcotics Active File in 1963, 92 ^ percent were heroin users.
18. Computing rates of hospitalization per 100,000 males twenty-one years of age or older from Pescoi s data, the twelve leading states in 1937, in order, were ( a ) Louisiana (13.9 ) , ( b ) Texas ( 8.2 ) , ( c ) Kentucky ( 8.0 ) , ( d ) District of Columbia ( 7.0 ) , ( e ) Oklahoma ( 5.2 ) , ( f ) Georgia ( 4.5 ) , ( g ) Tennessee ( 4.2 ), ( h ) Arkansas ( 3.9 ), ( i ) Florida ( 3.6 ), ( j ) Missouri ( 3.8 ), ( k ) South Carolina ( 3.3 ), and (1) Alabama ( 3.1) . These rates were computed from Table 2 of Pescor's study ( op. cit.), using 1940 census data. ( Pescor grouped 18 states together under "AD Others" which precluded the computation of rates for these states from which the fewest patients were received; it seems unlikely that any one of these 18 states would be among the first 12 states if the rate were computed.)
19. The present data refers only to state of residence, but from hospital records it is known that most admissions from New York and Illinois come from New York City and Chicago, respectively; Barclay, Martha G.: Comparative Statistics of Addiction. Master's Thesis, Department of Hygiene and Public Health, University of Kentucky, 196.3, p. 32.
20. The rates of patients admitted from the southern states for the 1937 fiscal year and the rates of patients discharged from the southern states for the 1982 fiscal year are quite similar. Thus, the southern pattern of addiction has continued. What has changed is the increased rate of admission from states with large metropolitan areas, such as New York and Illinois.
21. Pescor, op. cit., p.28.
22. ibid., p.26.
23. In Texas and Louisiana the southern pattern of opiate use by white middle-aged males continues, while at the same time, the youthful Spanish. spealang heroin addicts are appearing at the Fort Worth Hospital.
24. of the 1,311 male patients from New York, the District of Columbia, and Illinois, 65.6 percent were Negro, Puerto Rican, Mexican, or nonwhite.
25. Of the sixty-nine male patients from Alabama, sixty-three were white and six Negro; of the fifty-nine male patients from Georgia, fifty-eight were white and one Negro; of the thirty-nine male patients from Kentucky, thirty-seven were white and two were Negro.
26. Kolb, Lawrence: Drug addiction.Archives of Neurology and Psychiatry, 20:171-183, 1928.
27. Terry and PelIens, op.cit, Ch. 1 and 2.
28. Chapman, Kenneth W.: Drug addiction: the general problem.Federal Probation, 20:39-44, 1956.
29. That is, of Puerto Rican or Mexican parentage.
30. Clausen, John A.: Drug Addiction. In Merton, Robert K., and Nisbet, Robert A. (Eds.) : ContemporarySocial Problems. New York, Harcourt Brace 8c World, 1961, Ch. 4, pp.181-221. In this regard Chein and Rosenfeld state: "Areas of high incidence of juvenile drug use are the most deprived areas of the city, where family life is most disrupted, where the population is of the lowest socioeconomic status, and where often discriminated against ethnic groups (in New York City these are Negroes and Puerto Ricans) are highly concentrated." Juvenile narcotic use.Law arid Contemporary Problems, op. cit., p.53.
31. O'Donnell, John A.: A post-hospital study of Kentucky addicts--a preliminary report.Journal o f the Kentucky Medical Association, 61:573-577 and 604, 1963. In a study of 457 meperidine (Demerol) addicts, Rasor and Crecraft found that the majority of these addicts secured their drugs through legal sources and that 50 percent came from the southeastern states. Rasor, Robert W., and Crecraft, H. James: Addiction to meperidine (Demerol) hydrochloride.Journal o f the American Medical Association, 157:654-657, 1955.
32. See Chapter 10.
33. Federal Bureau of Narcotics, Statistical Data on Active Narcotic Addicts in the United States as of June 30, 1963.
34. Admission of voluntary patients to the Lexington and Fort Worth Hospitals is, by law, confidential.
| < Prev | Next > |
|---|