| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 174 |
| Yesterday: | 251 |
| This Week: | 174 |
| Last Week: | 2221 |
| This Month: | 4762 |
| Last Month: | 6796 |
| Total: | 129361 |
Chapter 11 Negro Opiate Addiction
 |
|  |
| 
| Books - Epidemiology of Opiate Addiction in United States |
Drug Abuse
The Epidemiology of Opiate Addiction in the United States
Chapter 11
Negro Opiate Addiction
CARL D. CHAMBERS AND ARTHUR D. MOFFETT
Introduction
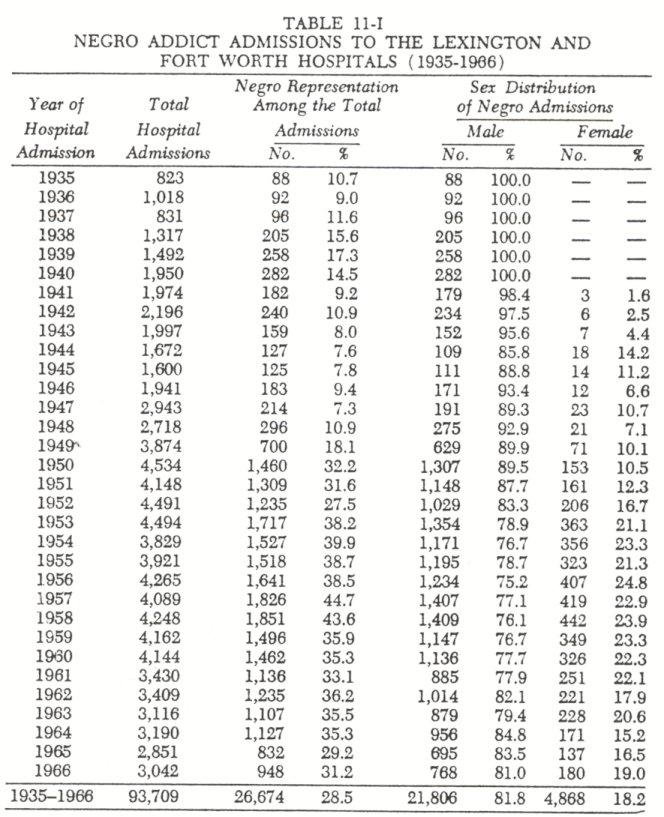
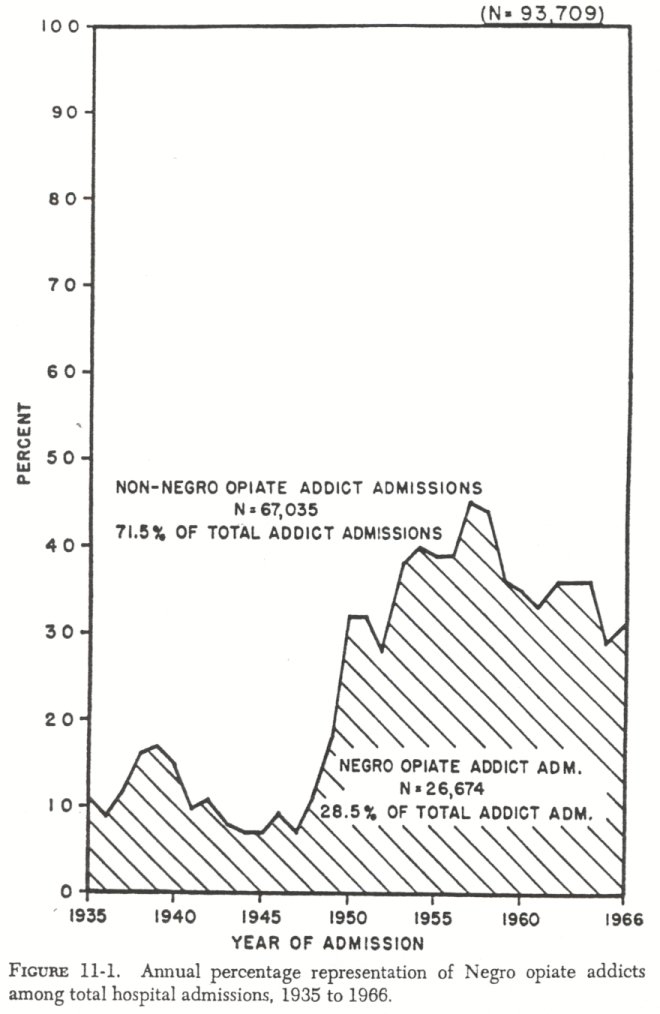
RECENT lay and professional writings have popularized the concept that narcotic use is widespread among Negro metropolitan dwellers. An analysis of the representativeness of Negroes among admissions to the two hospitals substantiated this concept. Negroes have been represented in the hospitals' addict populations since their opening. During1935, Lexington's initial year of operation, Negroes represented approximately 10 percent of the total U. S. population and10.7 percent of the total admissions for treatment of narcotic addictions.By 1966, however, while the Negroes still represented only approximately, 10 percent of the nation's population, they constituted 31.2 percent of the addict admissions to the two treatment facilities. This increase reflects a significant aspect of Negro-white differences in addiction prevalence.
During this same period of time the Negroes were in the process of moving from the rural South to metropolitan settings in the North and West, and this internal migratory flow terminated with Negroes being concentrated in the central cities of the metropolitan areas (Hauser,1966). Sociologically there seems little reason to question that these internal migrations and new settings are likely to produce environmental deprivations, individual and group alienations, deviant subculture identifications and associations, and the ready accessibility of narcotics generally associated with high rates of narcotic experimentation. This report was written to fulfill two needs: document any evolutionary patterns which are associated with Negro opiate addiction and to describe the contemporary Negro addict.
Part 1. TheEvolutionary Patterns (1935-1966)
From1935 through1966, 26,674 admissions of Negro opiate addicts were recorded at the Lexington and Fort Worth treatment facilities. These26,674 Negro admissions represented28.5 percent of all the admissions to the two hospitals. Regardless of the treatment facility, addict-patients share several dichotomous statures which provide the researcher with convenient frames of reference relevant to evolutionary patterns in hospital admissions.' The first part of the study was designed to produce the answers to six suggested questions:
1. Did the incidence of Negro opiate addiction change significantly between1935 and1966?
2. Did the sex distribution change significantly within the Negro opiate addict population between1935 and1966?
3. Did the incidence of recidivism among Negro opiate addicts after hospital treatment change significantly between1935 and1966?
4. Did the incidence of the seeking of voluntary treatment among Negro opiate addicts change significantly between1935 and1966?
5. Have the ages of Negro opiate addicts changed significantly between1935 and1966?
6. Has the Negro opiate addict population been distributed geographically throughout the United States?
Empirical data was available to document the answer for all six questions relevant to evolutionary change?
1. An analysis of incidence as measured by the annual number of treatment admissions to both hospitals indicates the incidence of Negro opiate addiction did change significantly between 1935 and 1966. As would be expected, treatment admissions for Negroes were at their lowest during the first years after the facilities were opened. The incidence of opiate addiction among Negroes reflected only minor increases during the period of 1935 through 1948. During 1949 a major incidence increase was recorded with the number of Negro admissions more than double the number admitted during 1948. The number of admissions doubled again during the following year (1950 ) . From 1950 through 1957 there was again a relatively stable period of increases in the incidence of hospital admissions.The incidence ofNegro opiate addiction, as measured by admissions for the treatment of this addiction, was at its highest in 1958. From that time there has been a general decrease in the number of Negroes being treated at the two hospitals, with the number of admissions stabilizing at approximately one thousand per year.
The total number of hospital admissions by Negro opiate addicts ( N=26,674 ) indicates theseNegro addicts have been responsible for28.5 percent ofall ofthe treatment admissions to bothof the hospitals. Negro addict-patient representation within the total admissions to the hospitals has followed much the same evolutionary pattern as did their incidence. Negro admissions comprised only 10.7 percent of all the hospital admissions during 1935 but had risen to 31.2 percent in 1966. In general, Negroes appear to have become overrepresented within the opiate addict population shortly before 1950. Since 1950 Negro addicts have contributed approximately one-third of all of the hospital admissions.
2. An analysis of sex distribution as measured by this distribution within the annual treatment admissions to both hospitals indicatesthe sex distribution within the Negro opiate addict population did change significantly between 1935 and 1966. Al though females have always been underrepresented in the Negro opiate population, the incidence of Negro females addicted to the opiates increased steadily between 1941, the first year they were accepted for treatment, and 1953 ( Table 11-I ) . By 1953, 21.1 percent of all the Negro admissions were for females, and this distribution has remained relatively constant to the present.
The total number of hospital admissions by Negro females addicted to opiates ( N=4,888 ) indicates that thesefemale addicts have been responsible for 18.2 percent of all of the Negro admis sions ( Table 11-I ) . In general, these Negro females have not differed significantly from the male opiate addicts in their mean age at hospital admission or in whether they return to the hospital for treatment after becoming readdicted. Negro females have, however, significantly more often sought this treatment for their addictions voluntarily rather than being sent as federal prisoners (Xz=39.222; P=<.001).
Admissions of Negro females was at its highest during the period from1956 to1960. During this period the representation of females was highest;23.5 percent of the total Negro admissions and39.9 percent of all Negro female admissions(1941-1966 ) occurred.
3. An analysis of the incidence of recidivism as measured by the annual number of readmissions among the total admissions to both hospitals indicatesreaddiction arid subsequent readmission to the hospitals (recidivism) did change significantly between 1935 and 1966 ( Table l I-II ) . Although there were no readmissions during the initial year of operation, by the second year (1936 ) 6.5 percent of all the Negro admissions were for addicts who had become readdicted to opiates. By the third year (1937 ) 14.6 percent of all the Negro admissions were readmissions. The incidence of readmissions generally increased through 1949, at which time 28.3 percent of all the admissions for Negro opiate addicts were readmissions. During 1950 and 1951 the incidence continued to increase, but the proportion of recidivists to those being treated for the first time decreased by almost one-half. Significant increases of over 100 percent in the number of addicts being treated for the first time during this period had the effect of significantly reducing the proportionate representation of recidivists. By 1952, however, the proportion of recidivists had again increased to approximately one-third of all the admissions. Readmissions were numerically the highest in 1958, when 788 recidivists were readmitted for treatment. The proportion of recidivists to first admissions was also the highest during this period, with 43.1 percent of all admissions during 1959 being readmissions. At no time since 1954 have readmissions comprised less than one-third of all admissions.
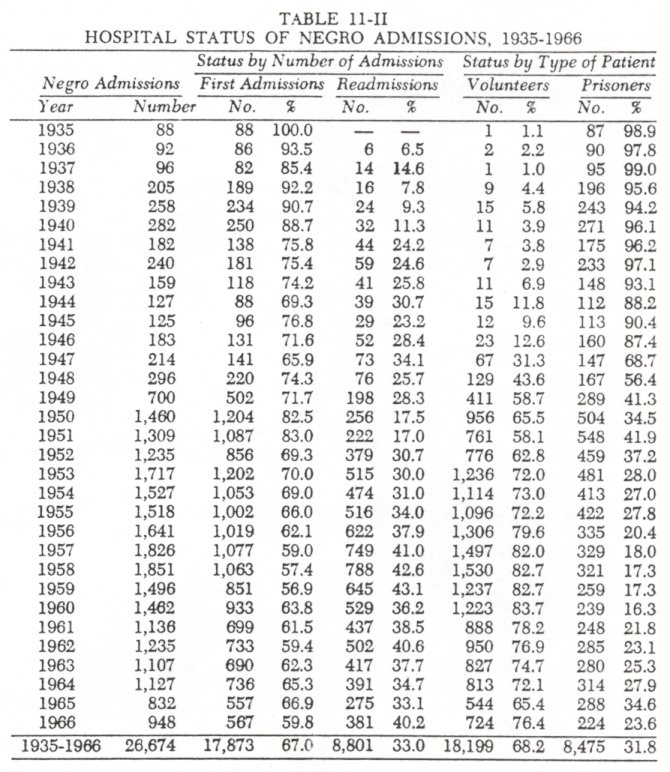
The total number of readmissions to the hospitals by Negro opiate addicts ( N=8,801) indicates that recidivists have accounted for 33.0 percent o f all the Negro admissions to bothhospitals.
4. During the period under study (1935-1966 ), both of the hospitals provided no-cost confidential treatment to opiate addicts requesting the service. An analysis of the incidence of Negro addicts voluntarily seeking this hospitalization revealed one of the most significant evolutionary changes. During the first decade (1935-1944 ) only 4.6 percent of all Negro admissions were the result of addicts voluntarily seeking treatment. The remainder, 95.4 percent, were federal prisoners under forced treatment. By the last decade (1957-1966) the situation was reversed. During this latter period 78.6 percent of all Negro admissions were voluntary ones. The highest incidence of voluntary admissions occurred in 1960, when 83.7 percent of all Negro admissions were voluntary ones.
The total number of voluntary admissions to the hospitals by Negro opiate addicts ( N=18,199 ) indicates that voluntary admissions have accounted for 68.2 percent o f all Negro admissions.
It is significant that recidivists, regardless of their sex, were more likely to return to the hospitals voluntarily than as prisoner patients. Recidivists were also more likely to be volunteer-patients than were the Negro addicts being treated for the first time. As was reported earlier, there is a sex difference in these patient statuses. Females more frequently seek treatment voluntarily than do the males. The mean ages of the two patient status groups do not differ. The mean age for all volunteer-patients is 29.12 years as compared to 29.88 years for all prisoner-patients.
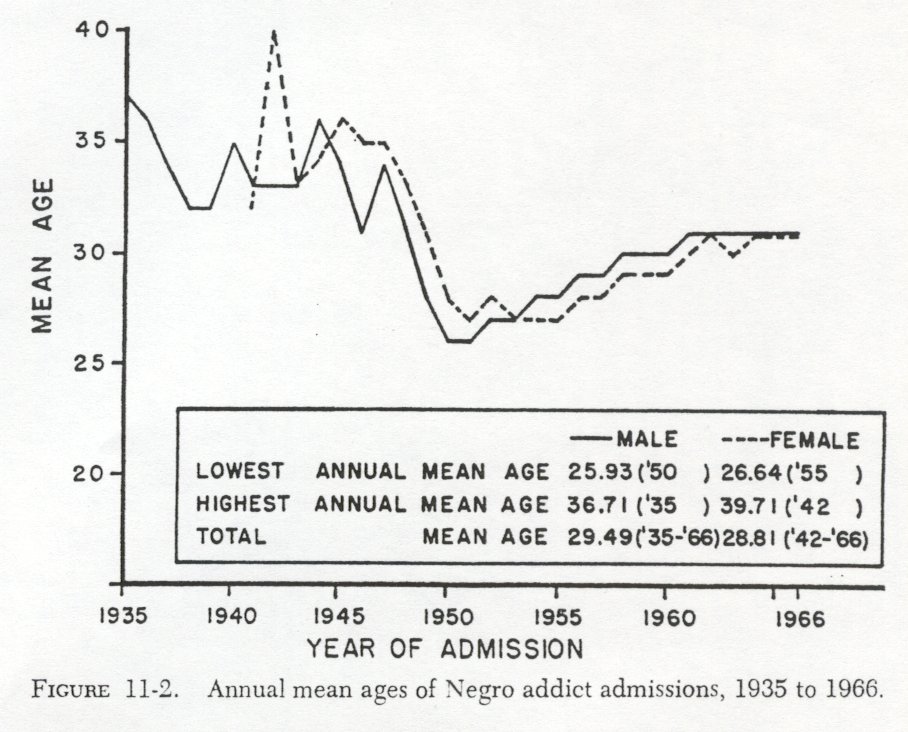
5. With the total admissions to the hospitals each year for basic comparison groups, an analysis o f mean ages at admission indicates that significant changes have occurred. In 1935 the mean age at admission for all Negro opiate addicts was 36.71 years. By 1966 this mean age had decreased to 31.23 years ( Table 11-III and Fig. 11-2). This decrease in age at treatment also reflects a general decrease in the age at onset of opiate abuse .8 Negro opiate addiction has come to be associated with the younger age groups.
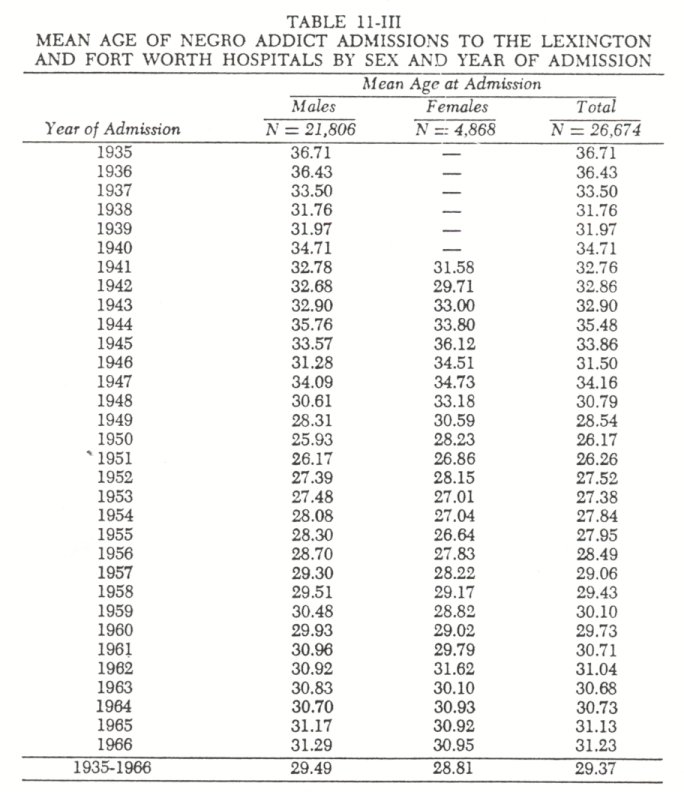
Negro opiate addicts, at least as reflected by the above measure, were youngest during the early1950's. In1950 and 1951 the mean ages for all Negroes admitted for treatment were 26.17 and 26.26 years, respectively. By the latter part of that decade, the mean age stabilized at approximately thirty years and has remained at that level to the present. Thus, the pattern was one of decrease in the mean age from thirty-six to twenty-six years(1935-1950 ) and then one of increase from twenty-six to shirty years(1951-1966 ) .
The mean age for all Negro addict admissions(1935-1966 ) was29.37 years. A by-sex comparison failed to produce any significant mean age differences. Regardless of sex the initial years when treatment became available produced the older mean ages. After these initial years the ages of both sexes converged and have remained generally the same since1950. The mean age for all male admissions was29.49 years, and for females it was 28.81 years.
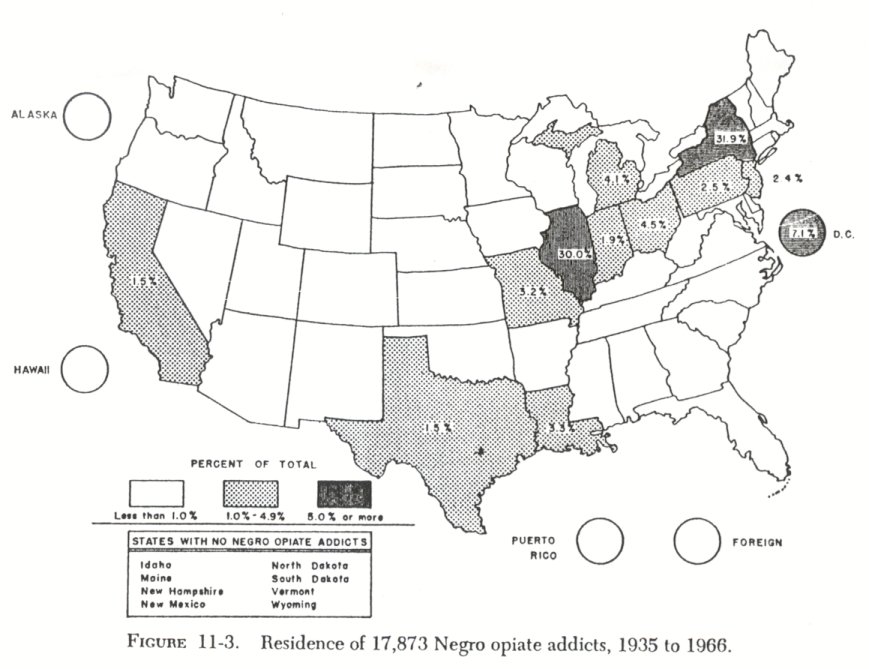
6.Negro opiate addicts have not been geographically distributed throughout the United States ( Fig.11-3 ) . New York and Illinois have contributed62.9 percent of all of the Negroes admitted for treatment. Over 90 percent of a$ of the Negro opiate addicts were found to have been concentrated in only nine of the states and in the District of Columbia. Eight states have contributed no Negro addicts.
The incidence of opiate addiction among Negroes residing in southern states has always been low. Only 10.6 percent of all Negro addicts admitted to both hospitals have resided in any of the fourteen southern states.
Summary
Statistically documented answers to the six questions concerning patterns of change among Negro opiate addicts have been presented. Measurements derived from analyses of Negroes admitted for treatment of their opiate abuse revealed the following:
1. The incidence of Negro addict admissions ranged from a low of88 (1935 ) to a high of1851 (1958 ) . Their representation within the total admissions ranged from7.3 percent (1947) to 44.7 percent (1957 ) . By these measures Negroes first became overrepresented in the opiate addict population shortly after World War II and have remained so to the present.
2. Females have always been underrepresented in the Negro opiate addict population. Prior to 1950 the Negro opiate addict population was approximately 10 percent female. Around 1950, however, this representation doubled and has remained at approximately 20 percent to the present.
3. Recidivism (readdiction and subsequent readmission) has always been high. Readmissions began the second year the hospital at Lexington was in operation. At one time (1959 ) re cidivists accounted for 43.1 percent of a full year's admissions to both hospitals. One-third of all admissions have been for recidivists.
4. Negro opiate addicts in any appreciable numbers did not seek treatment voluntarily until after World War II. The contemporary Negro addicts, however, do seek treatment voluntarily. From 1935 to 1945, 95.4 percent of all Negro admissions were for prisoners. From 1960 through 1966, however, 75.3 percent were for voluntary admissions.
5. Negro opiate addiction has come to be associated with younger age groups. The mean age for all admissions during the first two years the hospital was in operation (1935 and 1936 ) was over thirty-six years. By the last two years studied (1965 and 1966), the mean ague had decreased to only slightly over thirtyone years. There have been no significant changes in the mean age of Negro admissions during the past decade.
6. Negro opiate addiction is not a problem throughout the United States. No Negro addicts were found in eight states, and only 10.6 percent of the Negro addicts had resided in southern states. New York and Illinois contained the greatest concentration of Negro addicts ( 31 .9% and 30.0% respectively). Over 75 percent of the Negro addicts were found to reside in New York ( 31 .9% ), Illinois ( 30 .0% ) , the District of Columbia ( 7 .1% ) , Ohio ( 4 .5% ) , and Michigan ( 4.1% ) .
Part 2. Contemporary Negro Addicts
During 1965, 832 Negroes were admitted as addict-patients to the two hospitals. This Negro addict-patient group represented 29.2 percent of the total number of patients admitted during that year. Given the fact that Negroes represent 10 percent of this country's total population, the overrepresentation of Negroes among the addict population of this study is obvious.
Within this Negro addict population 83.5 percent were males and 16.5 percent were females' Among the addicts 66.9 percent were admitted for treatment of their addictions for the first time, While 33.1 percent were known recidivists ( readmissions ) . Using the U. S. Census Bureau criteria, 72.4 percent of the males and 77.3 percent of the females had been admitted from the Middle Atlantic or East North Central geographical regions.' Within these regions 99.0 percent had resided in Standard Metropolitan Statistical Areas, principally New York City and Chicago.
At the time these addicts were admitted to the hospitals, there were two basic mechanisms whereby an addict could be admitted: as a voluntary admission which included the right to leave the hospital at the patient's discretion or as a prisoner admission with a specific sentence which had to be served prior to discharge or release.' Of the 832 Negro addicts 65.4 percent were admitted under the voluntary admissions category and 34.6 percent were prisoners.
To extend and supplement the data which were normally collected in the routine administrative and medical procedures, ninety--eight consecutive male admissions from New York and Chicago and fifty-seven consecutive female admissions, of whom 82.4 percent came from New York and Chicago, were individually interviewed. Since there is a concentration of Negro addicts in SMSA's in northern areas, it could be assumed that the 155 interviewed subjects would be representative of the majority of the Negro opiate addicts, and therefore, generalizations about the problem of Negro addiction would be warranted.
The plan of the study was to ascertain, wherever possible, anysignificant differences between the known Negro addict-patient cohort and the Negro in the general population, and to ascertain any significant differences between the Negro male and female addicts. At the same time, it was hoped parameters pertinent in the process of addiction could be isolated.
Preadmission Factors
In ascertaining the presence of both natural parents in the home prior to a subject's fifteenth birthday, it was discovered that 67.7 percent of the subjects had experienced a broken home situation. Females were more likely than males to have come from broken homes, with disintegrations noted as 71.9 and 65.3 percent, respectively.'
The subjects' formal education levels were as follows: 38.0 percent had completed high school or advanced beyond that educational level, 53.5 percent had started but failed to complete high school, and 8.4 percent had some formal schooling but had not entered high school. Although the differences were not statistically significant," the data indicate males more frequently than females ( 40.8% and 33.3%, respectively) had completed high school.9
The majority ( 84.5% ) of these opiate addicts had experienced a marital situation. Among the males, 80.6 percent were or had been married. As for the females, conjugal situations were reported by 91.2 percent. Although the percentages of marriages did not exceed those which would be expected for this age group within a nonaddicted population, the percentages of marital disintegrations did." The data suggest that 48.1 percent of male addict marriages but 90.4 percent of the female addict marriages were intact at the time of admission to the hospital."
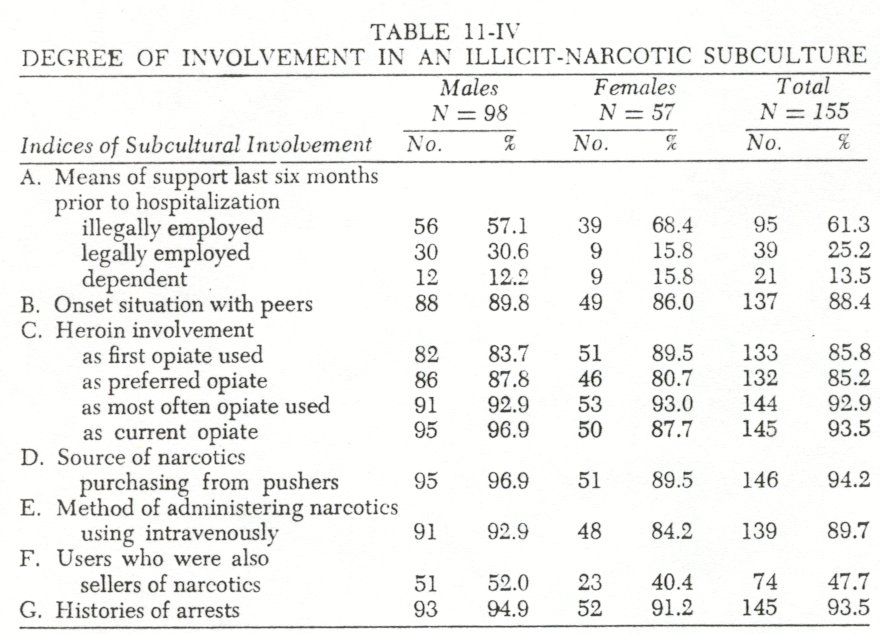
Data pertinent to the dominant means of financial support during the sixmonth period prior to the hospital admission indicated there were no statistically significant differences between males and females. The distribution of financial means of support should, however, be noted. For example, only 25.2 percent of the sample had been legally employed, while 61.3 percent had been supporting themselves through illegal means or had spent the major portion of the six months prior to hospital admission incarcerated.
The remaining 13.5 percent were totally dependent upon their spouse, family, or social welfare programs for their support ( Table 11-IV).
Addiction Factors
THE ONSET SITUATION. Regardless of sex the most prevalent onset situation included peer involvement. In 88.4 percent of the cases the subjects first experimented with opiates while in the company of a peer who was already using opiates. In 38.7 percent of the cases this experimentation occurred in a group setting. If this experimentation occurred with only one peer, males as well as females usually experimented in the company of a male peer. Of the males experimenting with only one peer, 93.8 percent experimented with a male peer and only 6.2 percent with a female peer. Of the females experimenting with only one peer, 71.9 percent experimented with a male peer and only 28.1 percent with another female.
In this sample the initial use of narcotics was not attributable to physicians prescribing the drug or other medically related situations, as only 3.9 percent of the subjects attributed their addictions to medical onset situations. 12
Reports from 5.2 percent of the subjects ( N=8 ) indicated a first experimentation in a family context. In the consanguine situations ( N=6 subjects), it was reported that an older brother had provided the experimental opportunity, and in the conjugal situations ( N=2 subjects), husbands had provided the initial opiates to their wives.
THE OPIATE USED. Heroin was overwhelmingly the initial opiate used (85.8%), was the preferred opiate for continued use ( 852% ), was the opiate most frequently used during addiction careers ( 92.9% ), and was the most frequent opiate diagnosed as the current opiate at the time of admission for treatment for addiction ( 93.5 ) . This pattern of opiate use was noted regardles of controls for sex.
THE OPIATE SOURCE. In ascertaining where the subjects had secured their opiates, it was determined that 94.2 percent had procured their opiates from an illicit source ( pusher ) . Although the differences were not statistically significant, males more frequently than females had resorted to illicit sources.
ML-MOD OF ADMINISTERING THE OPIATES. AS most of the subjects were addicted to heroin, it was anticipated that the most common method of administering the opiates would be intravenous injection. The findings reinforced this expectation, with 89.7 percent of the subjects using the intravenous route. Although the differences were not statistically significant, males more frequently than females used the intravenous method of administering their opiates.
CORRELATED DRUG Use. A history of marihuana use was found to be prevalent among these known opiate addicts. Of these addicts 83.9 percent admitted having used marihuana during their drug experimentations." Among males 92.9 percent reported having used marihuana. Among the females, however, only 68.4 percent reported histories of marihuana use.
In this sample of known opiate addicts, marihuana usage patterns were evident: ( a ) regardless of sex, marihuana use was more prevalent than nonuse, but only a small percentage (13.8 ) of these users continued to use marihuana with any frequency after beginning the use of opiates; and ( b ) males more frequently than females (92.9 versus 68.40 used marihuana as part of their drug experimentations and more frequently continued their marihuana use throughout their opiate experimentations (13.39 versus 8.8% ) .
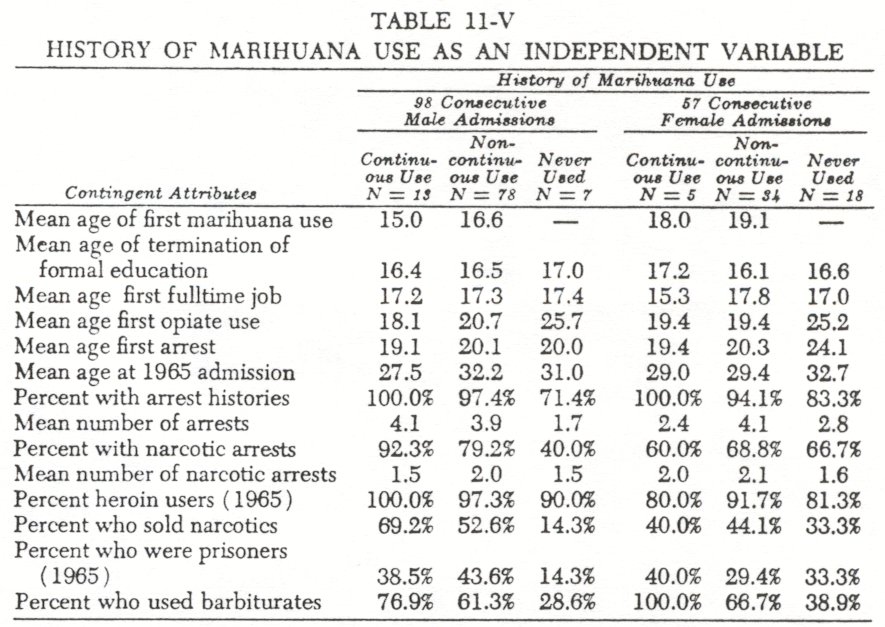
Previous research conducted with Negroes in the general population had indicated that a history of marihuana use made an individual more liable to opiate addiction." It therefore became necessary to view portions of the data in relationship to marihuana history as an independent variable ( Table 11-V ).
Among those subjects who did smoke marihuana while still in school ( N=68 ), 57.4 percent did complete their high school educations, and of those subjects who did not smoke marihuana, at least while still in school, 65.5 percent were also "dropouts." It was noted, however, that the males who smoked marihuana, more often than the females ( 60.4 versus 33.30, engaged in this behavior prior to terminating their education. Thus, analysts could assume these opiate addicts had been adolescent marihuana smokers who had not only evoked physiological and psychological risks, whatever they were, but had also evoked the potentially more dangerous risk of becoming inextricably involved in a subculture where drug use and criminal behavior were accepted norms.
Attendant to and reinforcing this assumption was the criminalinvolvement of these marihuana users. Almost all, 98.5 percent, of the marihuana users had arrest records, and 75.8 percent of them were marihuana smokers prior to arrest. Indicating a high degree of involvement within a deviant subculture, 47.7 percent of the addicts were found to have sold drugs. Of these pushers90.5 percent had histories of marihuana use. The data indicate that at least for the possible reduction of opiate addiction among metropolitan Negroes, optimum intervention into the process would have to occur during the early school years and would have to focus on the liabilities attendant to marihuana use.
Controlling for the extent of marihuana use and nonuse, it was discovered that continuous use of marihuana, infrequent use of marihuana, and no use of marihuana could be considered definitive of three distributed subcohorts.
Continuous use of marihuana, in this rank order of apparent liability, was most frequently identified with the earliest ages of marihuana experimentation, the earliest ages for terminating education, the earliest ages of opiate experimentation, and the earliest ages for arrests. In addition, this cohort manifested the highest potential for being arrested, for having narcotic arrests, for becoming heroin user, for becoming sellers o-_ narcotics, and for barbiturate experimentation. In most of these areas the reverse was noted for the cohort in which no marihuana experimentation occurred, and the infrequent marihuana users most often fell between the two extremes.
Widespread barbiturate use was also indicated with60.6 percent of the subjects reporting such a history. Although the differences are insignificant, females more frequently than males reported barbiturate abuse. For females61.4 percent reported histories of barbiturate use, while only59.2 percent of the male opiate addicts engaged in this type of concurrent abuse.
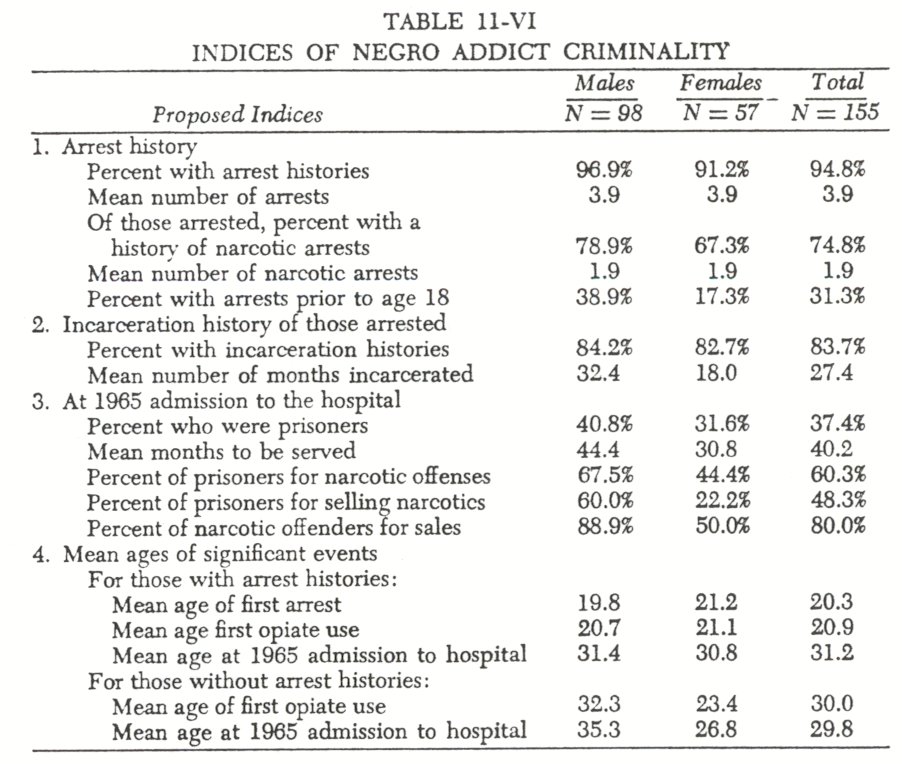
Criminality Among Addicts
Previous research had documented the association between addiction and criminality." The present study provided an opportunity to amplify our knowledge of this association. Of the 155 addictpatients94.8 percent reported arrest histories, and this group had a mean of3.9 arrests. Of those arrest histories74.8 percent had a mean of1.9 arrests for specific narcotic offenses. Of those with arrests83.7 percent had been incarcerated. Of those arrested31.3 percent reported being arrested prior to age eighteen." A comparison of mean ages suggests, at least within the limitations of this comparative technique, thatfirst arrest preceded the first use of opiates.
Within the male cohort96.9 percent of the subjects reported histories of arrest,38.9 percent reported arrests prior to age eighteen, and81.6 percent had been incarcerated. Of those with histories of arrests78.9 percent had been arrested for narcotic offenses. At the time of admission to the hospital,40.8 percent of the males were admitted as federal prisoners or probationers to serve a mean sentence of 44.4 months. Among these prisoner admissions 67.5 percent were to serve sentences for violations of the narcotic laws, primarily the sale of narcotics. Sixty percent of all male prisoners and 88.9 percent of the narcotic offenders were sentenced for the sale of narcotics. A comparison of the mean ages at which the first arrest and the first use of opiates occurred suggests, among males, that arrest preceded first use of opiates.
Within the female cohort 91.2 percent of the addicts reported histories of arrest, 17.3 percent reported being arrested prior to age eighteen, and 75.4 percent had histories of incarceration. Of the female subjects with histories of arrest, 67.3 percent had been arrested for narcotic offenses. At the time of admission to the hospital, 31.6 percent of the subjects were admitted as federal prisoners or probationers, and the mean sentence they were to serve was 30.8 months. Among these prisoner patients 44.4 percent were to serve sentences for narcotic offenses and, as was the finding with the male cohort, the sale of narcotics was a prevalent offense. Twenty-two percent of all the female prisoners and 50.0 percent of the female narcotic offenders were being incarcerated for the sale of narcotics. A mean age comparison suggests that the first use of opiates, among females, precedes the occurrence of the first arrest. None of the prisoner admissions, either male or female, was currently incarcerated for a crime of violence.
Past criminality was a dominant pattern even among the 62.6 percent of the addict-patients who were not prisoners or probationers. Among the male voluntary admissions 94.8 percent reported histories of arrest, and of these, 70.9 percent had been arrested for violating narcotic laws. Female voluntary admissions did not differ significantly, with 87.2 percent having been arrested, and of these, 67.6 percent reported specific narcotic arrests.
The data suggest, at least among Negro subjects, that addicts rarely escape having extensive arrest records and their addictions rarely escape detection by the police ( see also Robins and Murphy, 1967 ) . It is also suggested that at least among males official detection of criminal deviancy precedes opiate experimentation. Given a sex differential in law enforcement, it was expected that males would be arrested earlier, have more arrests, be incarcerated more frequently, and would have longer sentences imposed than their female counterparts. This expected sex differential was found.
The selling of narcotics might be indicative of a more complete involvement in the addict subculture. In this addict group 47.7 percent admitted to having sold narcotics. Although the differences were not statistically significant, males more than females ( 52.0 versus 40.4, respectively) reported that they had sold narcotics. Thus, within these cohorts of opiate addicts, the selling of opiates was a widespread phenomenon.
Controlling for only those male subjects who admitted to having sold narcotics, 31.4 percent of these "pushers" supported themselves financially with their sales. Again, controlling for only those females who sold narcotics, 72.7 percent had at some time derived their major financial support from pushing narcotics. Thus, it was apparent that although female addicts as a group are less likely to resort to selling narcotics, if they do sell narcotics; they frequently use this method as their primary source of income.
Preadmission Event Sequence: The Processes to Addiction
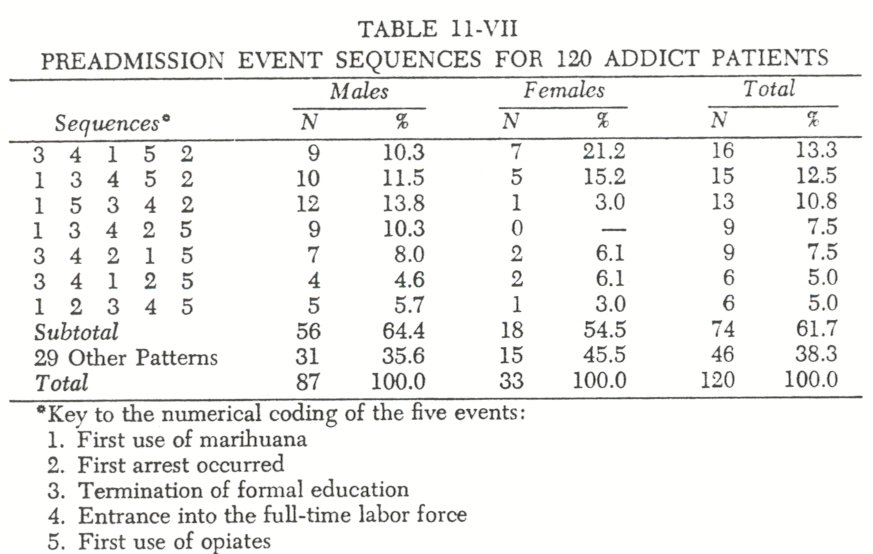
Within the interviewed sample, data were available pertinent to the age at which five events occurred: ( a ) when the first use of marihuana occurred, ( b ) when the first arrest occurred, ( c ) when formal education was terminated, ( d ) when entrance was made into the full-time labor force, and ( e ) when the first use of opiates occurred.
Alternative placement of these five events produces 120 possible sequential patterns. An analysis of each interviewed subject's preadmission experiences revealed that 77.4 percent of the subjects had experienced all five events. The 120 subjects utilized only 36 of the possible 120 sequence patterns, and 61.7 percent of them ( 64.4& of the males and 54.5 of the females) had utilized only 7 of the possible sequence patterns.
In controlling for sex, the most frequently used sequential TABLE 11-VII pattern for males was: the first use of marihuana, the first use of opiates, termination of formal education, entrance .into labor force, and first arrest. Females were found to have used the following sequential pattern more than any other: termination of formal education, entrance into the labor force, the first use of marihuana, the first use of opiates, and first arrest ( Table 11-VII).
Summary
This chapter has demonstrated the homogeneity of the contemporary Negro opiate addict cohort. Comparisons of prehospitalization attributes (e.g., consanguine home status, marital status, formal education, and means of economic support) produced minor distribution differences, but these differences were not consistently affected by the experimentally independent variable of the sex of the addict. Comparisons of these attributes with normal Negro groups revealed the addicts ( a ) were more likely to have come from a broken home, ( b ) were more likely to have been school dropouts, ( c ) were more likely to have been married, ( d ) were less likely to have kept a conjugal relationship intact, and ( e ) were less likely to have been legally employed. Thus, the addicts could be considered to be deviants even within the environment of the metropolitan area.
1. Such variables as race, sex, admissions number, patient status, and so forth.
2. One additional evolutionary change, the incidence of concurrent sedative abuse and addiction reported in Chapter 8, could be included here as the seventh pattern.
3. See the next section for empirical verification. The finding is also reported in Chambers, C. D., Moffett A. D., and Jones, J. P.: Demographic factors associated with Negro opiate addiction.International Journal ofthe Addictions, 3(2): 329-343, 1968.
4. The U. S. Bureau of the Census (1960) reported that the Negro population above age fourteen was 52.7 percent female and 47.3 percent male. This indicates a marked underrepresentation of females in the addict cohort.
5. The U.S. Bureau of the Census defines the Middle Atlantic Region as including New York, New Jersey, and Pennsylvania and the East North Central Region as including Indiana, Illinois, Michigan, Ohio, and Wisconsin.
6. These two basic mechanisms are administratively separated into the following categories: a volunteer, a committed volunteer, a federal prisoner, a federal probationer, and a prisoner awaiting trial.
7. The chi-square comparison between male and female addicts is not statistically significant. The incidence of broken homes was, however, higher than that reported in previous research. In the research sample in St. Louis, 49.3 percent of the normal Negro males came from broken homes, and 50.0 percent of their addicted sample reportedly experienced this situation. No comparable statistics are available for Negro females. See Robins, L., and Murphy, G.: Drug use in a normal population of young Negro men.American Journal of Public Health, 57:1580-1596, 1967.
8. For the purpose of statistical comparisons the chi-square test was used throughout this paper. Significance of any comparison was determined at the P-.05 or greater level.
9. The mean age for the Negro male addict-patients at the time of 1965 admission to the hospitals was 30.5 years. Comparison with die Robins and Murphy sample of normal Negro male population in their early 30's indicates that the addicts from New York and Chicago were more likely to have completed high school than the addicts is the St. Louis study ( 40.8 versus 18.2% ) but less likely to have completed high school than the nonaddicts in the study ( 40.8
10.Census statistics for 1960 reveal that 82 percent of the Negro population above age fourteen had experienced a marital situation. The sample revealed no significant chisquare values between the sexes. Among the addict sample the marital disintegrations were 35.1 percent, while the disintegrations among normal Negroes did not exceed 33 percent; U. S. Bureau of the Census: Nonwhite Population By Race.1960 Final Report PC ( 2 )-1C, p.9.
11. There is a chi-square difference between the sexes of R=-22.786, P[.001.
12. The reader is directed to Dai, B.: Opium Addiction in Chicago. Shanghai, Commercial Press, 1937; and Pescor, M.: A Statistical Analysis of the Clinical Records of Hospitalized Drug Addicts. PublicHealth Reports, Suppl. 13. Washington, Government Printing Office, 1943, for historical references where the initial use attributed to physicians and/or paramedical reasons for addiction was above 30 percent.
13. During this time period 1,510 white addict-patients were admitted for treatment. Of these only 82.8 percent had histories of marihuana use, suggesting Negro opiate addicts are more likely to have used marihuana in their processes to addiction. The comparison between the sexes was significant ( X' = 10.170, P<.Ol ).
14. Robins and Murphy, op. cit.
15. O'Donnell, J.: Narcotic addiction and crime.Social Problems, 13:374-385, 1968.
16. Robins and Murphy, op. cit., reported that29.0 percent of their normal Negro male sample had official juvenile delinquency records and that 80.? percent of their Negro male addict sample were found to have juvenile records.
| < Prev | Next > |
|---|