| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 185 |
| Yesterday: | 251 |
| This Week: | 185 |
| Last Week: | 2221 |
| This Month: | 4773 |
| Last Month: | 6796 |
| Total: | 129372 |
Chapter six Empirical research on psychological characteristics
 |
|  |
| 
| Books - Female hard drug-users in crisis |
Drug Abuse
Chapter six Empirical research on psychological characteristics
6.1 Introduction
In the previous chapter the average number of childhood traumas and the predictive qualities of the traumata were investigated. It appeared that the research subjects had experienced an average of three childhood traumas and that the childhood traumas 'rape', 'physical abuse', 'parental divorce' and 'incest' occurred most frequently.
This chapter is devoted to the kind of psychopathology that was found among the research subjects, the predictive qualities of the different psychological variables and the coherence between childhood traumas and psychopathology.
As was shown in the Introduction to the present study, there is research evidence to suggest that women suffer more from psychological complaints than men (SCP, 1992). There is also considerable evidence to suggest that drug-users - male and female - suffer from some kind of psychiatric disorder. The co-existence of psychiatric illness and substance abuse disorder is referred to as 'dual diagnosis' (Ganguly, 1990). As is mentioned in the Introduction to this study, the question of whether drug-use precedes psychiatric illness or is a consequence of it is an example of the 'Chicken and the Egg'. In the context of the present study it is impossible and quite unnecessary to solve this question. Drug-use and psychiatric illness are viewed in this study as perverse strategies to survive gender identity problems and childhood traumas (see Chapters Two and Four).
In order to relate the results of the present chapter to other research results I will briefly summarize the most important data of the research on psychiatric disorders among drug-users (see also the Introduction of present study) and on the coherence between childhood traumas and psychopathology.
Summarizing the international research, it was found that drug-users suffered in particular from depression (40% to 60%), and anxiety disorders (10 to 17%). Dutch research (Van Limbeek et al., 1991; Hendriks, 1990) showed that drug-users suffered from anxiety disorders, including agoraphobia, social phobia and panic disorder (37% to 69%) and depression (15% to 37%).
The results on the Symptom Checklist-90, administered to 202 drug-users (Korf & Hoogenhout, 1990), show a considerable variation of psychiatric symptoms and complaints: part of the group has as many complaints as the 'normal' population, part of the group equals or exceeds those of psychiatric out-patients.
Research in the United States on health and mental health problems of groups that are likely to use drugs and/or alcohol - the groups of homeless men and women - give evidence to show that 17% of the women suffer from schizophrenia, 24% from an affective disorder and 44% from an anxiety disorder. Almost half of the women suffered from an addiction, 17% used drugs, 32% alcohol (Breaky et. al. 1989).
On the basis of the literature some coherence between the two sets of variables - childhood traumas and psychopathology - might be expected. With regard to the psychological after-effects of childhood traumas, research evidence shows that childhood traumas including sexual abuse are related to mental disorder. For instance, twice as many women with psychological complaints or addiction have a history of sexual abuse than the average 'normal' woman (Draijer, 1988). About one third of female psychiatrical patients and female addicts have experienced childhood sexual abuse (Rosenfeld, 1979, Nicolai, 1990, Carson, Coucil & Volk, 1988, Cohen & DensenGerber, 1982, Roshenow, Corbett & Devine, 1988, Schaap, 1988).
Women who were abused as children may suffer from depression (Gelinas, 1983), from post-traumatic stress disorder (Goodwin, 1985; Lindberg and Distad, 1985 and Bezemer, 1986), from dissociation disorders (Putnam et. al. (1986) or other psychiatric disorders.
Draijer (1988) found that people with double traumas have more serious psychological disturbances than people with single traumas. Women who have experienced such childhood traumas as neglect, sexual and physical abuse and repetition of traumatic events at an older age suffer a cumulative pathogenetic effect (Draijer, 1988). On the basis of this research evidence I expected firstly to find some coherence between the two sets of variables and secondly that certain traumatic events, such as rape and physical abuse as well as the diagnosis post-traumatic stress disorder would predict a speedy return to the VKC.
Research design
In this chapter I shall begin by investigating the seriousness of the psychological problems and the kind of psychological disturbance; in the second part of this chapter I shall give a prediction analysis based on the statistical method of multiple regression analysis. Finally I shall give an integral analysis of the coherence between childhood traumas and psychopathology.
The psychiatric disorders and the results from the psychological questionnaires were used as a set of predictor variables and as separate variables. These variables were measured at the time of the client's admittance to the VKC. The outcome variables
are: 'time between discharge and first re-admission within a year after discharge' and 'number of re-admissions within a year' (see Chapter 5 for explanation of these criteria).
In the present study 'crisis intervention', operationalized as 'length of stay at the VKC' is statistically analyzed as an intervening variable (see Chapter 5 for explanation of this criterium).
6.2 Methods
Subjects
52 research subjects participated in this study. The background characteristics of the subjects can be found in Chapter Five.
Setting
The Women's Crisis Centre (VKC) provides in-patient feminist treatment service for six female drug-users at a time who find themselves in crisis. The treatment services of the VKC are aimed at a crisis intervention that takes no longer than a few weeks, with the maximum length of stay being three months.
Assessments
The subjects were evaluated on the day after their admission at the VKC. The following instruments were administered by trained psychologists.
The Symptom Check List-90 - in short SCL-90 -, consisting of 90 questions, is a multi-dimensional indicator of psychopathology based on the subject's self-appraisal. This questionnaire, developed in the United States (Derogatis, 1983) has been translated into Dutch, adapted and standardised (Arrindell & Ettema, 1986). The psychological questionnaire covers a wide range of complaints typical of psychiatric out-patients. The 90 items cover somatic and psychological complaints on eight dimensions (the score range is based on the norm group of women psychiatric out-patients n=1074, Arrindell & Ettema, 1986):
- anxiety (ANX), a patient suffers from complaints which go together with anxiety such as a heightened vegetative arousal, nervousness and panic attacks; score range from very low (10-16) to very high (> 44);
- agoraphobia (AGO), a person experiences phobic anxiety, he or she fears open spaces; the score range from very low (7) to very high (> 31);
- depression (DEP), a person complains of sombre feelings, lack of energy, absence of self-esteem; score range from very low (16-29) to very high (> 69)
- somatic complaints (SOM), somatic symptoms which go together with functional disorders; score range from very low (12-17) to very high (> 47);
- distrust and interpersonal sensitivity (SEN), complaints that concern dissatisfaction with oneself in relation to other persons; score range from very low (18-25) to very high (> 70);
- insufficiency of thinking and acting (IN), a person suffers from obsessivecompulsive behaviour, for example acting compulsively; score range from very low (9-13) to very high (> 37);
- sleeping problems (SLA); score range from 3 to 15
- rage/hostility (HOS); kinds of aggression, irritability and resentment; score range from very low (6) to very high(> 19).
A subject fills in a score on a seven point-scale that differs between very low; low; below average; average; above average; high and very high.
The Beck Depression Inventory (in short BDI) is a self-report questionnaire, consisting of 21 questions (Beck et al, 1961, Bouman, Luteijn, Albersnagel & Van der Ploeg, 1985). The scores of the questionnaire refer to the existence of depression and the seriousness of the depressive complaints. According to Wiggins (1973) the BDI happens to be a cumulative measurement model that resembles the clinical picture. The seriousness of the depression increases along with the number of symptoms (Van den Hoofdakker, 1987). BDI's rule of thumb is that women generally score two points more than average and men two points below average. The BDI' scale is a 7 point scale and the score range differs from 2 to 37 (Bouman et. al. 1985).
Psychiatric diagnoses were obtained using the third version of the Diagnostic and Statistical Manual (DSM-III; American Psychiatric Association, 1980). The DSM-III-R diagnostic system uses five axes. The first axis describes the clinical syndrome and mental states that cannot be attributed to mental disorder but need attention. The second axis describes personality disorders and specific developmental disorders; the third is concerned with somatic illness; the fourth determines the weight of last year's psychosocial stress factors; the fifth axis reports last year's highest level of social functioning. In clinical practice the first two axes are generally used in order to diagnose mental disorder. All research subjects could be diagnosed as suffering from Psychoactive Substance Use Disorders. On the basis of this diagnostic category, no distinction was possible between the research subjects. As the above studies (see 6.1) have shown that it is a question of the co-existence of addiction and other psychiatric disorders, this present study is concerned with a rough distinction in co-existing psychiatric pathology, applying the following three diagnostic categories of the DSM III-R axis I: depression NOS(311.00), post-traumatic stress disorder (309.89) and psychosis NOS (309.89). Although there was in some cases more than one other psychiatric disorder, for example, a research subject suffered from depression and post-traumatic stress disorder, for clarity's sake a choice has been made on the basis of three specific questions: whether or not the research subject is psychotic, whether or not the subject is depressed and finally whether or not the research subject is suffering from a post-traumatic stress disorder. Where the depressive disorder was dominant, this diagnostic category was chosen, although some criteria were met from the diagnosis of post-traumatic stress disorder. Where the post-traumatic disorder was dominant, this category was applied, although there was evidence of some overlap with the depressive disorder. For clarity's sake each research subject received only one diagnosis besides the diagnosis of substance abuse disorder. The following explaination should make the chosen diagnostic categories clear.
The diagnosis of 'depression NOS' was applied because the research subjects did not completely meet the criteria for Major Depressive Episode (296) or Dysthymal disorder (300.40) and because exclusive criteria existed for both diagnoses. The diagnosis of 'post-traumatic stress disorder' was applied, even though the research subjects also suffered from 'dissociation'. However, because not all the criteria of dissociatioe disorder were met, this diagnosis was not applied. Moreover, Multiple Personality Disorder, a kind of dissociatioe disorder, was not diagnosed, because this disorder was not included in the DSM-III-R.
The diagnosis of 'psychosis NOS' was applied, because there was not enough data to justify a more specific diagnosis and because there were some excluding criteria. In addition, psychoactive substance-induced organic mental disorders and drug-induced psychosis were ruled out.
Procedure
The collecting of data started in June 1988.
The 52 participating subjects were interviewed on the day after their admission to the Women's Crisis Centre (the semi-structured interview can be found in Appendix Two). At the same time, they also filled out some psychological questionnaires. Most of the participants of this study were under the influence of methadone both at the time of the interview and when filling in the questionnaires.
Three psychologists, including myself, trained in diagnosing according to DSM-III, did the interviews and psychodiagnostic research. A Mental Health Service psychiatrist gave a second DSM-III-R diagnosis of the group that was re-admitted in the Women's Crisis Centre. He based his diagnosis on files. The agreement with regard to the diagnosis between the first and second assessor was 80%.
On request, the results were reported to the research subject. The data collection based on interviews and psychological questionnaires was finished in August 1989. Staff of the Crisis Centre registered dates of admission and discharge. This registration was checked by staff of the SDA. The registration and counting of readmissions was done by the Centre's staff and checked by staff of the SDA.
Data analysis
In order to investigate the predictive qualities of psychological variables measured at 'baseline', the method of multiple regression analysis was applied. This method is explained in the previous chapter.
In order to compare the psychological complaints that were found with the reference groups, statistical averages and standard deviations were determined. The extent of the difference between research subjects (o) and reference group (r), which is clinically often more interesting than statistical significance, was determined according to the following formula:
A difference of .80 or more is perceived as large. A difference of .50 is judged as medium and a difference of .20 as low (Cohen, 1977).
In the multiple regression analysis, the integral analysis uses all significant predictor variables and subsequently gradually eliminates the non-significant variables.
6.3 Results
6.3.1 Psychological complaints
SCL-90 and BDI
The psychological self-observation questionnaires SCL-90 and BDI were used in order to investigate psychological/psychiatric complaints. Figure 6.1 shows the distribution of psychological complaints. The group of women of the Women's Crisis Centre was compared to a group of 'normal' women and women who are in out-patient psychiatric treatment (see table 6.1, appendix one).
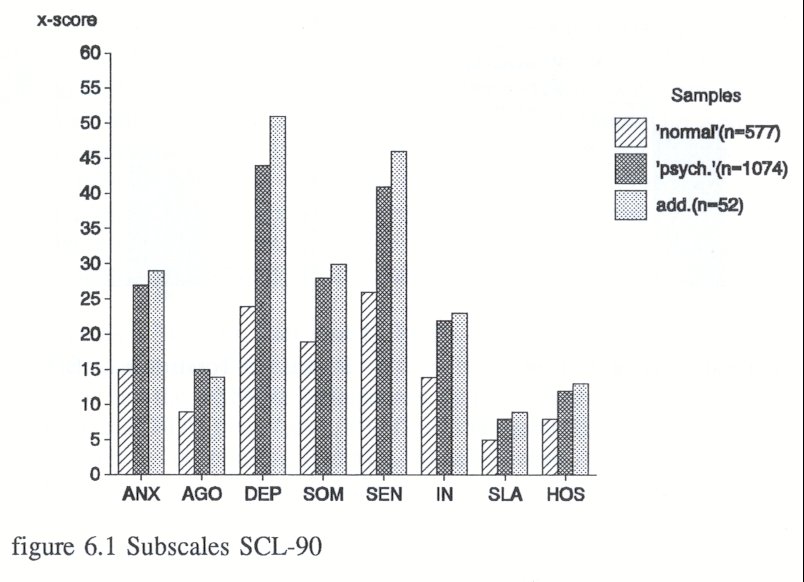
With the exception of sub-scale AGO (agoraphobia), the research subjects' scores are higher than those of female psychiatric out-patients. Cohen's formula was applied to determine whether the differences between the scores of the diverse samples were minimal, medium or high. Female drug-users at the VKC scored higher (somewhere between minimal and medium) than female psychiatric patients on the sub-scales of depression and sensitivity. As figure 6.1. shows, the VKC's female drug-users score higher on all scales than the 'normal women'. The scores of the SCL-90 clearly show that the female drug-users who stay at the VKC are suffering from such psychiatric complaints.
The figures 6.2 and 6.3 show the total scores on SCL-90 and BDI for the different groups. (The table is included in Appendix One, table 6.1).

The research subjects score much higher than female psychiatric patients on the BDI, and according to Cohen's formula the difference is large (0,80). The differences between the VKC's female drug-users and the female psychiatric patients on the SCL90 are minimal. The group of women who were re-admitted (n=26) does not differ significantly from the group of women who were not readmitted (n-26) with regard to scores on BDI and SCL-90 (see table 6.2, Appendix One).
The distribution of the DSM-III-R scores is shown in figure 6.4:
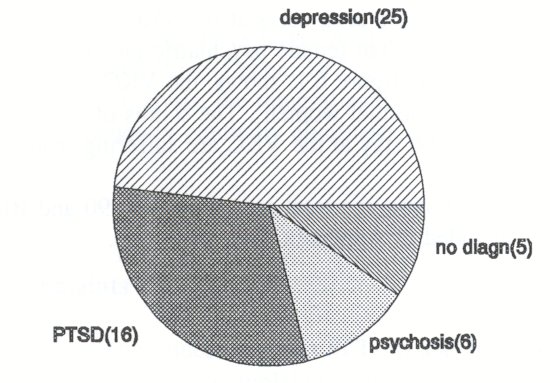
Figure 6.4 Distribution of depression, posttraumatic stress disorder and psychosis of addicted women (n=52)
For the sake of clarity only one co-existent axis I diagnosis (co-existing with the psychoactive substance disorder) is made (see section 6.2 for explanation).
With regard to DSM-III R diagnoses, the group of women who were later re-admitted to the VKC does not differ significantly from the group of women who were not. Depression occurred 13 times in the group of women who were not re-admitted as opposed to 12 times in the group who were. Post traumatic stress disorder occurred 8 times in each group. Psychosis was diagnosed 3 times in each group. In the group of women who were not re-admitted there were two cases in which no diagnosis was made, and in the group of who did return, three cases.
Connection between SCL-90, BDI and DSM-III R diagnoses
According to the Spearman correlation co-efficients of the psychological questionnaires SCL-90 and BDI and the DSM-III R diagnoses, there is some positive connection between SCL-90 and BDI (r=0,67;p=0,00). This is not remarkable, because both questionnaires refer to 'depression' (the SCL-90 as sub-scale). This connection (r=0,67) between SCL-90 and BDI could also mean that both questionnaires measure the same thing, namely severity of psychiatric complaints.
There is no connection between BDI and DSM-III R diagnoses. This is not remarkable because the BDI measures the severity of depression and the DSM-III R refers to the kind of psychiatric illness.
SCL-90 and the DSM-III R diagnosis of 'depression' are slightly positively connected (r=0,28;p=0,02), SCL-90 and post-traumatic stress disorder are negatively connected (r=-0,40;p=0,00). The first result can be easily explained: the SCL-90 also measures depression. The second result could be a consequence of the choice of registering only one diagnosis: depression or post-traumatic stress disorder. Presuming that the SCL-90 particularly refers to depression, besides which the scores on this subscale were very high anyway, this result means that the research subjects with the diagnosis of 'post-traumatic stress disorder' were not dominated by depression but by anxiety, re-experiences of traumatic events and dissociation.
There is no connection between psychological questionnaires and psychosis. (This data is recorded in Appendix One, Table 6.3).
6.3.2 Prediction analysis of psychological complaints
The next question is whether the psychological variables measured at baseline predict the time between discharge and re-admission to the VKC and whether these variables predict the number of re-admissions within one year.
The psychological questionnaires BDI and SCI-90 could not predict the number of days between discharge and re-admission, nor could they predict the number of readmissions within one year.
However, the diagnoses of 'depression' and 'post-traumatic stress disorder' were able to predict the period between discharge and relapse into crisis (re-admittance within three months, six months, nine months or twelve months). When depression or post-traumatic disorder was diagnosed, the time between discharge and re-admission was shorter than without these diagnoses. Regression analyses for both diagnoses showed that the diagnoses could reasonably predict the period that a woman could survive without the help of the Women's Crisis Centre once discharged (r=-0,56;p=0,0l, the figures are included in Appendix One, Table 6.4).
The post-traumatic stress disorder( r=-0,65; p=0,00) is a relatively stronger predictor variable than depression (r=--0,51; p=0,02). These results could mean that women with both diagnoses experience a greater treatment need or have a more favourable, trusting attitude towards treatment and could be more easily motivated to other, long term treatment agencies. In short, they respond well to in-patient crisis intervention, they want more treatment and they are not the stereotypical 'untreatable' heroine prostitute. The other group of research subjects, the women with the diagnosis of 'psychosis', although not 'untreatable', could possibly need other treatment facilities than the Women's Crisis Centre provides.
Psychological complaints and number of re-admissions
The relationship between the psychological variables (questionnaires and diagnoses) and the number of re-admissions within a year was not significant.
Coherence between childhood traumas and psychopathology
The connection between childhood traumas and psychopathology was so slight that no conclusions could be drawn. The only Spearman correlations between childhood traumas and psychopathology that met the criterium of significance were the following: - 'incest with sibling' and post-traumatic stress disorder
(r=-0,24;p=0,04).
- 'incest with sibling' and depression (r=0,25;p=0,03 ).
- 'father unknown' and post-traumatic stress disorder (r= 0,24;p=0,04).
- 'father unknown' and psychosis (r=0,25;p=0,04).
- 'quarrel between parents' and post-traumatic stress disorder (r=0,41,p=0,00).
- 'quarrel between parents' and depression (r=-0,30;p=0,01)
- 'placement in foster care' and post-traumatic stress disorder (r=0,27;p=0,03).
6.3.3 Integral prediction analysis
The integral analysis shows that some predictor variables can predict the return to the Women's Crisis Centre quite well (mr=0,90; r square=0,82, see Table 6.5, Appendix One). I have divided the significant predictor variables into two groups. One group (see figure 6.5) predicts a fast return to the Crisis Centre; the other group of predictor variables predicts a longer stay outside the Crisis Centre ( see figure 6.6).
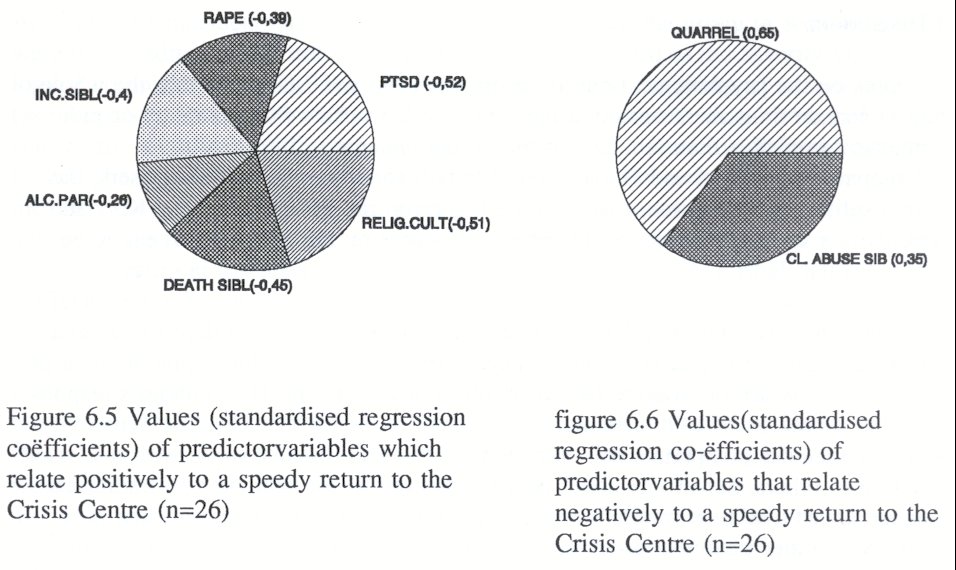
Figures 6.5 and 6.6 show that the diagnosis of 'post-traumatic stress disorder' predicts a fast return to the Women's Crisis Centre quite well. The other diagnostic category, depression, has been eliminated in the integral analysis and appears to be a less forceful predictor variable. Physical abuse was also eliminated as a predictor variable.
Of all predictor variables the variable 'quarrel between parents' is the most forceful predictor variable. This variable predicts that women with that kind of trauma stay away from the Women's Crisis Centre longer without support. The other variable that predicts a longer period of absence, 'client physical abuses other members of family', is a less forceful predictor (r=0,35). 'Divorce' as predictor variable has been eliminated in the integral analysis.
Integral analysis and number of re-admissions
There has been no integral analysis of the two sets of predictor variables and this outcome variable, because no variable as such, or set of variables, earlier predicted the number of admissions.
6.4 Discussion
The scores on the psychological questionnaires SCL-90 and BDI show that the whole group of female drug-users treated at the VKC (n=52) suffers from as many or more psychiatric complaints than female psychiatric out-patients.
Compared with Korf and Hoogenhout's (1990) study among 202 drug-users, the research subjects in this present study score higher on the SCL-90 than did Korf and Hoogenhout's sample. The above differences in scores on the SCL-90 can easily be explained. First, Korf and Hoogenhout's respondents (1990) were not in crisis. Secondly, the research subjects in the present study live in conditions of more social deprivation and isolation than those of Korf and Hoogenhout. Social deprivation and isolation are conditions that might cause psychological distress. Thirdly, the women of this present study are on average two years older than Korf and Hoogenhout's respondents. The scores on SCL-90 also show an elevated score on the sub-scale Sensitivity. Sensitivity includes complaints that represent distrust and dissatisfaction with one's self in relation to others. Sensitivity could be a factor in drop-out behaviour in traditional substance abuse treatment programmes. Some research subjects mentioned that they felt humiliated in other treatment programmes. They were treated as a "junky with junky tricks". The therapists of the Women's Crisis Centre on the other hand have an attitude based on trust and acceptance. Perhaps the most important factor in conquering the distrust of the female drug-users is that the therapists do not ask them to change. They accept them as being addicted, they accept their need of prostitution.
Three DSM-III-R diagnoses were applied to the research subjects: depression NOS, post-traumatic stress disorder and psychosis.
The DSM-III R diagnosis of depression (almost 50%) occurred most frequently, followed by post-traumatic stress disorder (about 32%). Of the 52 research subjects, six suffered from psychosis (11%); five women obtained no axis I diagnosis. Compared
with international research the present study found the same amount of depressive disorder as in other studies, but twice as many anxiety disorders (in the present study only one specific kind of anxiety disorder was used, the post-traumatic stress disorder). It may be concluded that the range of psychopathology among the research subjects is within the range of psychopathology that other researchers found among drug-users. Generally speaking drug-users suffer frequently from depression (drug-use could be a kind of self-medication to alleviate feelings of depression) and, moreover, women are more likely to suffer from depression than men. It is not therefore remarkable that depressions within this group of female hard drug-users are more severe than those within the group of female psychiatric patients. In addition, the research subjects are a group of women who, at the time of admission, are in the grip of a crisis which they do not know how to solve. The crisis situation in itself could aggravate the feelings of depression.
The kind of psychopathology that more than three-quarters of the research subjects present (depression and post-traumatic stress disorder) is treatable, for instance via a cognitive-behavioural approach or Multi Modal Therapy (Lazarus, 1973, Kwee & Lazarus, 1986).
Given the presence of co-existing psychopathology we may now ask ourselves whether the contra-indications of the 'regular' mental health institutions may need to be reconsidered. This subject is further questioned in the next chapter.
According to statistical analysis (Pearson-chi-square test), the group of women who were not re-admitted did not differ significantly with regard to the severity of psychological complaints and psychiatric disorders compared to the group of women who were (see Appendix One, Tables 5.1.a and 5.1.b) The present results show nevertheless that statistically significant differences among the women who were re-admitted could be found. The psychological questionnaires (BDI, SCL-90) did not predict any outcome measure, though the diagnoses did predict the period between discharge and readmission quite well. It is presumed that women with the diagnosis of depression and post-traumatic stress disorder who return more quickly to the VKC than women who suffer from psychosis are more able to profit from the VKC approach, and may profit from referral to other treatment agencies. It is also possible that women with the diagnosis of 'psychosis' could profit from another approach, perhaps from some kind of sheltered accommodation or 'bed and breakfast' facilities. In addition we may also ask ourselves whether a 'harm reduction' approach might not improve conditions for this group of women, particularly a kind of experimental drug-dispensing programme. This would prevent prostitution out of necessity.
This study gives no clear answer to the question of whether or not there is a connection between childhood traumas and psychopathology. Statistical analysis minimally corroborates the hypothesis that childhood traumas and psychopathology are connected. This result contrasts sharply with what other researchers have found, namely that the combination of physical and sexual abuse causes more psychopathology than the experience of one traumatic event (Bryer et.al. 1987).
The integral analysis delivered a somewhat surprising picture, namely that 'quarrel between parents' was the most forceful predictor of the two sets of predictor variables. This variable predicts a longer stay outside the VKC without support. It could be that this result confirms the hypothesis that women who are able to direct energy and aggression outwards are better able to cope with problems (see Chapter Four for an explanation of different strategies). Another explanation is that this traumatic event is the least traumatic of all nineteen traumas or that women with this trauma have experienced some attachment within the family.
Finally, the predictor variable 'post-traumatic stress disorder' and certain traumatic events such as 'rape', 'death of a sibling', 'alcoholic parent','incest with a sibling' and 'religious cult' predict a fast re-admission to the VKC and evidence the need of treatment as well as the wish to be treated. Some of these events are traumas - rape, death of a sibling, incest with a sibling -, some, such as 'alcoholic parent' and 'belonging to a religious cult' would probably be categorized as a severe psycho-social stress event. But perhaps these events are traumatic because of the context of parental neglect and rejection.
Although the present study shows that psychopathology and childhood traumas predict the outcome variables quite well, it remains to be seen what the influence might be of a third variable: the social position of the female drug-user. The research subjects are in a worse social position than the female drug-users of the general sample (Korf & Hoogenhout, 1990), they also suffer from more psychopathology. It is possible that social position and psychopathology are slightly connected. The present study has not statistically analyzed this connection because there was not much differentiation between the subjects with regard to social position: three quarters of the subjects had no housing, no medical insurance and no state benefit. So 'social position' did not seem a variable that would make a division in subgroups possible.
| < Prev | Next > |
|---|