| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 185 |
| Yesterday: | 251 |
| This Week: | 185 |
| Last Week: | 2221 |
| This Month: | 4773 |
| Last Month: | 6796 |
| Total: | 129372 |
Chapter five Empirical research on childhood traumas
 |
|  |
| 
| Books - Female hard drug-users in crisis |
Drug Abuse
Chapter five Empirical research on childhood traumas
5.1 Introduction
Kaplan (1991) points out that perversion is not only a strategy for surviving social gender identity problems but also a problem-solving strategy for coping with childhood traumas (for explanation, see chapter 2). The gender-identity conflicts of female drugusers - one part of female perversions - are about adaptation to traditional sex roles and controlling their lives or being out of control. Female drug-use as a general perverse strategy has been subdivided into four problem-solving strategies: anaesthesia, flash, submission and performance (see chapter four). This coming chapter is devoted to the other part of the female perversions, the kind of childhood traumas that the subjects have experienced. The frequency of the traumas, their number and the predictive qualities of these childhood traumas all come under investigation.
In past years, research into the prevalence of childhood traumas has supplied the following data.
Dutch research indicates that about 16% of 'normal' women have experienced sexual contact with relatives in their childhood against their will. Half of them suffered later from negative psychological effects (Draijer, 1988).
International research, although using somewhat different criteria to establish the fact that incest or sexual abuse had taken place, indicates that 18% to 20% of "normal" women have experienced sexual abuse by relatives in their childhood (Finkelhor, 1979, Russell, 1983).
Clinical studies show that about one third of women who undergo psychiatric treatment have experienced sexual abuse in childhood (Rosenfeld, 1979, Nicolai, 1990). Studies among female drug-addicts also show that about one third of the women have a history of childhood sexual abuse (Carson, Coucil & Volk, 1988, Cohen & Densen-Gerber, 1982, Roshenow Corbett & Devine, 1988, Schaap, 1988). Herman (1981) found that 35% of the women who were victims of father-daughter incest abused alcohol and/or drugs compared to 5% of the women with a 'seductive' parent.
Briere (1984) studied a random sample of 153 female "walk-in's" to a local Counselling Programme and found that the group formed by former sexual abuse victims (n= 67) were significantly more likely than non-abuse clients (n= 86) to have a history of alcoholism (27% versus 11%) or drug addiction (21% versus 2%).
Research also found a relationship between sexual abuse and prostitution (Silbert & Pines, 1983, James & Meyerding, 1977).
The incidence of sexual abuse committed by an acquaintance before the age of sixteen is 39% among prostitutes (Vanwesenbeeck et al, 1989).
Prevalence research on childhood physical abuse (R6mkens, 1989) among 1016 women found that one quarter of the women had been physically abused as a child. Before the age of twelve they were beaten, some of them once in two months, some of them once a week. The physical abuse included hard and repeated beatings, kicking, being locked up and thrown downstairs. For part of the group the abuse was very severe, including strangulation attempts, wounding with a knife or a pair of scissors, and burning.
Research design
The goals of the VKC in 1987 were to give shelter, offer crisis-intervention and refer women to treatment centres for further treatment. Because referral to other centres was only possible when women were both in need of treatment and motivated to undergo treatment I investigated whether or not childhood traumas predicted the treatment needs of the women. Some research subjects may possibly profit from referral to treatment centres more than others and the kind of childhood trauma the woman has experienced might be related to her need of treatment. As mentioned in the introduction to this study the focus of this particular piece of research lies on the individual research subject and her treatment needs and not on measurement of the treatment-outcome.
This chapter begins with an investigation into the frequency of occurrence and average number of cases of childhood sexual abuse, physical abuse and other traumatic events; the subsequent part of the chapter consists of the application of a prediction analysis based on the statistical method of multiple regression analysis.
In this study the focus lies on negative stressful childhood experiences. It is therefore necessary to investigate the victimization of the woman as a girl or as a young adolescent of sixteen years or younger. Draijer (1990) and Vanwesenbeeck et al.(1989), investigating childhood sexual abuse, have also used the age of sixteen as criterium. Another reason for applying sixteen years as criterium is that many of the research subjects left the parental home when they were sixteen. James (1980), who studied 136 female prostitutes, found that sixteen was the average age at which the women left home for good.
Childhood traumas are used as a set of predictor variables. These variables were measured at the time of the client's admittance by administrating the semi-structured interview (see appendix two). The outcome variables are 'time between discharge and first re-admission within a year after discharge' and 'number of re-admissions within a year after discharge'. These variables may provide an impression of the treatment needs of a female drug-user. For instance, if a female drug-user returns to the VKC soon after discharge, she makes clear that she is in need of further treatment and is not able to cope with her problems without the VKC's support. A speedy return to the VKC and a number of re-admissions within the space of a year might indicate motivation for further treatment.
Most women who are re-admitted (n=26) returned to the VKC within three months (n=11), six women within three to six months, six women within six to nine months and three women within nine to twelve months (sd =103).
Most women who were re-admitted (n=26) were re-admitted once or twice within a year (n=20), three were re-admitted three times within a year and four were re-admitted four times or more (sd=1,5). One research subject returned to the VKC in crisis seven times within a year.
In the present study 'crisis intervention', operationalized as 'length of stay at the VKC' is statistically conceived as an interacting variable. Twenty-six research subjects stayed at the VKC for less than thirty days, the other twenty-six of the group stayed for thirty to ninety days (maximum period at the VKC).
5.2 Methods
Subjects
All clients who were admitted to the Women's Crisis Centre between June 1988 to August 1989 were asked to participate as research subjects. One person refused. Some of them stayed in the Centre for such a short time that it was not possible to collect any data. The remaining subjects gave permission (informed consent) for their data to be used for research. The background characteristics of the subjects (see chapter three) are as follows:
On average the research subjects are thirty years old. The majority of the subjects is of Dutch origin. Their socio-economic background is lower class and lower-middle class. They are poorly educated. Half of the subjects has children. Three-quarters of the subjects has no housing and is not covered by the Dutch National Health Service.
Most of them are multiple drug-users. On average they have been using hard drugs for a period of eleven years. The predominant method of drug-use is intravenously. It is likely that about 30% of the intravenous drug-users is HIV-infected.
Almost all subjects are involved in prostitution (90%). Many of them become prostitutes out of necessity (see paths to prostitution and addiction, Chapters One and Three) because they need the money for drugs. The crises that force the subjects to seek help are social, psychological, psychiatric or medical in nature. Generally speaking there is more than one crisis situation.
Setting
The Women's Crisis Centre (VKC) provides an in-patient feminist treatment service for six female drug-users temporarily in crisis. The treatment services of the VKC are aimed at a crisis intervention that takes no longer than a few weeks (maximum length of stay is three months).
Assessment
Briefly summarizing, traumas belonging to the DSM-III-R category of post-traumatic stress disorder (PTSD), are characterised by three groups of symptoms: re-living an aspect of the trauma; avoiding anything likely to remind one of the trauma and a state of hyper-arousal (Gersons, 1992). In this chapter the traumatic events themselves that may cause these psychological consequences are mapped out by analyzing the interviews of the research subjects including their answers to questions about negative sexual or physical childhood experiences (the semi-structured interview is included in Appendix Two). The next chapter consists of an investigation into the nature of the psychopathology.
The following list of childhood traumas includes childhood traumas meeting the DSM-III-R criteria of a traumatic event (incest, physical abuse, rape) and the DSM-IIIR axis IV criteria of psycho-social stress events (e.g. mental abuse/cruelty, parent's divorce, quarrelling between parents and foster care/adoption). For the sake of convenience the term 'childhood traumas' will be further used in the present study to refer to both traumas and psycho-social stress events.
Given below is a list and explanation of the traumatic events reported by the research subjects:
1 Incest by a parent/relative
As far as defining the sexual abuse is concerned, I have applied the criteria defined by Roshenow et al. (1988) who investigated sexual abuse among substance abusers. They considered a patient to have been subject to sexual abuse if the following conditions were met:
- the patient was 16 years old or younger when the sexual abuse first occurred;
- the sexual contact involved direct physical contact with unclothed genitals rather than mere exposure or a verbal request;
- the perpetrator was at least five years older than the patient or was otherwise more powerful than the patient;
- the victim experienced the event either at the time or afterwards as unpleasant;
- the victim did not experience the event as resolved during childhood.
The incest traumas of the research subjects varied. Some were abused at a very young age, before they were four years old. Some were abused when they were ten or older. The application of force also varied, one research subjects was threatened with knives, others were mentally forced to keep the incest secret. Some research subjects who told other people about their experiences were not believed. One person was placed in a children's home when she told others about incest with her father.
In the majority of cases the incest was committed by the father or stepfather. In all cases the incest was experienced as traumatic.
2 A brother or sister was subjected to incest
Sexual abuse within a family causes psychological harm not only to the victim, but also to siblings who witness the sexual contact between brothers and mother (one research subject) or know that their brother or sister is victim of sexual abuse. One research subject knew that her father abused her sister, and discovered her sister in the act of trying to commit suicide. Another subject, who cared for father and sisters, in fact mothering them, was told when she was about fifteen by a sister that her father abused all her sisters. She felt completely betrayed by her father whom she loved very much and asked herself why he had not abused her and how it was possible that she had not known anything about it. She also felt betrayed by her sisters because they had not told her about it. Her whole former life felt like a lie and when she could no longer live with this reality she started to use drugs.
Another client says that her father has sexually abused both her sisters, one older and one younger. Her father was an alcoholic and physically abused all his children. Her relationship with her father is ambivalent, she loves him and would like to be treated as a good daughter, but she is also afraid that he will sexually abuse her. It is not clear why he did not abuse her, or whether it is true that she was not sexually abused. These days she has an alcoholic partner. Her former boyfriend physically abused her and she once tried to commit suicide.
The experiences of the research subjects vary from traumatic events to severe psychosocial stress events. Often the combination of events, the lack of trust in the parental home or the foster-care that sometimes follows parental abuse causes severe psychosocial stress.
3 A parent/relative physically abused the research subject
Many subjects were physically abused. The abuse included being thrown downstairs, attempts to drown the subject in a washstand, strangulation attempts and beating with a heavy object.
4 A parent/relative subjected the mother or a brother or a sister to physical abuse
Sometimes only one person in the family is the victim of physical abuse. One research subject describes her father as a quiet, distant man with a great love for animals. Her mother is a very caring and loving person who never complains, though she does suffer from a great deal of stress. Mother's only problem is that she cannot talk about her problems. Her father, on the other hand, talks quite easily. Mother and father are always quarrelling, and father beats mother up. When she is twelve, her parents divorce. At the age of fourteen she leaves home, becomes pregnant and has an abortion. Another research subject describes a similar story. As a baby she is adopted. Her foster-mother - who is infertile - is an alcoholic. Her foster-father, a quiet man, regularly beats her mother. When she is older, she is beaten by both foster-parents. At the age of fourteen her foster-mother dies from the consequences of alcohol abuse. The research subject is placed in a institution. At the age of sixteen she is on the street. In combination the above stressful events cause severe psycho-social stress.
5 An acquaintance or unknown person has raped the research subject
One research subject and her girlfriend were raped at the age of ten and her girlfriend was murdered. She was able to escape, but did not dare talk about it.
Several research subjects were raped by a 'gang' of boys. One research subject was first raped by an unknown person while she was collecting money. She later told her father and from then on her father started sexually abusing her.
6 A person not related to the family physically abused the research subject
Only one research subject experienced this negative psycho-social stress event. She was placed as a baby in a children's home because of a legal measure. Her mother was a prostitute and lost custody of the child. At the age of five, she went to live with foster parents. Her foster-father beat her. She was an outcast in the family. Nobody else was physically abused. Her foster-father and her foster-sisters called her a bastard. She met her mother when she was fifteen and lived with her for a few months. They quarrelled. She also visited her father, who was an alcoholic. At the age of sixteen she started using drugs; she felt strong and independent after drug-use. Nobody could dominate her any more.
7 The research subject herself physically abused a member of the family
This negative event refers to aggressive behaviour of the research subject towards her brother, sister or her mother's new boyfriend. The child is then labelled as 'difficult' or 'troublesome'. The mother asks the Child Welfare Council to intervene. The Council places the difficult child in a children's home.
The consequences of the 'difficult' behaviour thus make it a psycho-social stress event in the life of the research subject.
8 Mental abuse/cruelty within the family
The subjects described the attitude of a (religious) father as cruel. For example, the father who committed incest with his daughter also gave her presents and went out with her. The research subject says: "He had a relationship with me as if I was his wife." Her mother was jealous, angry and sad. Her father dominated family-life. When he was at home, the atmosphere became very tense. Another subject says: "My father abused me psychologically, but I don't remember any of it. I have erased it from my memory". She suffers from amnesia concerning certain periods in her life .
9 Parents' divorce
Usually the occurrence of parental divorce is a serious psycho-social stress factor. In the life of the research subjects this event is sometimes more than merely stressful, it is traumatic, because the consequences of the divorce are so negative. Sometimes the mother starts drinking, sometimes she gets a boyfriend who beats her and the children. Sometimes the step-father sexually abuses the children. As the research subjects say, life changed after the divorce and for some of them became unbearable. They became unruly or misbehaved to such an extent that they were placed in an institution.
10 Continuous quarrelling between parents
According to the DSM-III-R, axis IV "quarrels within the family" is a light psychosocial stress factor. A chronically bad marriage between the parents is a moderate psycho-social stress factor. Most research subjects who experienced "quarrels between parents" also describe their parent's marriage as chronically bad. The atmosphere indoors was always tense: "as long as I remember tiffs and wrangles polluted the air". Some research subjects describe their father as a hard, distant and rigid man and their mother as too soft, caring or easily influenced. One research subject suspects that her father killed himself because of the quarrels with her mother. In her case it was the father who was soft, easy-going and nice and the mother who was dominant.
11 Death of a parent
Usually the death of a parent is an extreme psycho-social stress factor. Some research subjects experienced the event as traumatic because, as the example above shows, the parent committed suicide. Sometimes the parent's death was preceded by a long and drawn out illness with the research subject having to care for the patient while still a young child. Sometimes the consequences of the death of a parent are doubly traumatic, for example when, after the death of the mother, a brother or sister commits suicide.
12 Death of a brother or a sister
Death of a sibling is usually a serious or extreme psycho-social stress factor. For two research subjects the event was traumatic because in one case it was a case of suicide and in the other a prolonged period of illness.
13 Father of research subject is unknown
This event, father unknown, in itself a moderate or severe psycho-social stress factor, is complicated by the fact that sometimes the siblings of the research subjects are of different fathers. For example, the research subject knows that she and her brother have the same unknown father, but the following children all have different fathers. The mother has had a string of boyfriends, neglects the children and the older children have to rear the younger children. They suffer from emotional neglect. Another research subject did not see her father from birth. Her mother divorced her father when she was fourteen days old. She had a stepfather who physically abused her. As a teenager she went looking for her real father. She met him when she was fourteen but was disappointed to find him very indifferent towards her.
14 Research subject had no contact with father
One research subject loved her father very much and was traumatized when the father was forced by the mother to leave. Circumstances in the family altered dramatically after the departure of the father, the only "safe" person the research subject had.
15 Mother was a prostitute
The fact that the mother is a prostitute is probably not in itself a severe psycho-social stress event, although it could generate feelings of shame. However, the consequences of the mother's profession could cause severe psycho-social distress. Both research subjects felt themselves emotionally neglected, sometimes their mother has burdened them with feelings of guilt, because she said the only reason she engages in prostitution was for the children, in order to give them presents or expensive holidays.
16 Parents' alcohol abuse
Research subjects called parental alcohol abuse a severe psycho-social stress factor and sometimes traumatic, because mother or father neglected the children and household, sometimes became aggressive and physically abused children or partner.
17 The research subject is placed in foster care
The above examples of traumatic events show that in some cases a child is placed in a children's home or in foster care, because it is too difficult, or because it tells "lies" about sexual abuse by a parent. In other cases, the child is placed in foster care after the death of a parent, sometimes as a judicial measure. The child usually experiences the parental rejection as very painful and traumatic.
18 The research subject was adopted or reared by grandparents
The events of adoption or rearing by grandparents in itself do not cause severe psychosocial stress. In one case, the subject did not know she was adopted. Her stepmother told her in a quarrel she was adopted, after which the subject ran away. In another case the rearing by a grandmother was stressful because the mother constantly interfered and there was continuous quarrelling and physical abuse.
19 The research subject's family belongs to an extreme religious cult
The families of two research subjects belonged to a religious cult, one to the "Norwegian Brothers" and one to an extremely religious Baptist group. As psychological after-effects of their severe and anxiety-provoking upbringing they described suffering from internal feelings of being worthless, a nobody. One subject recalled that until the time of her first menstruation she had slept in one bed with a brother who was four years younger than herself. Her parents then forbade her to sleep next to him any longer and made her very angry. When she was thirteen, her parents disowned her brother and forbade her to have contact with him.
Procedure
The data was collected on the day after admission to the VKC.
Data analysis
In order to investigate the predictive qualities of childhood traumas measured at 'baseline', I applied multiple regression analysis. The optimal model is one which enables the most to be predicted using the minimum number of variables. For that purpose I use the method of regression analysis which, on the basis of variables measured at base-line, predicts the outcome variables. Because it happens that in this study more than one predictor variable was applied, I investigated how the optimal combination of predictor variables could be reached, which would be still statistically relevant.
To get an insight into the relative importance of variables in predicting the outcome variables, the standardized regression coefficient (Beta) is convenient. The unstandardized regression coefficient (B) is functional when the formula is applied in practice. The regression coefficient's (B) confidence intervals are 95%. The confidence intervals are applied to provide an estimate of the value of the regression coefficient. Although now and then p-values are mentioned - for example when differences between women who are not re-admitted and women who are re-admitted are studied and the hypothesis 'both groups are not alike' cannot be rejected -, usually 95% confidence intervals are applied and these intervals are reported in the tables of appendix 1.
The multiple correlation coefficient (MR) is the Pearson product-moment correlation coefficient between the set of predictor variables on the one hand, and the outcome variables on the other. MR squared indicates the percentage of explained variance, identical to the meaning of the Pearson correlation squared. Statistically significant relationships are reported (0.05 level).
The procedure was as follows: all predictor variables entered the regression equation one by one and were tested to see whether or not they were able to predict an outcome variable (singular analysis); next, all variables pertaining to childhood traumas entered the regression equation (multiple analysis), after which the variables not meeting the criterium for removal (p < 0,05) were gradually eliminated.
The multiple regression equation was repeated, entering the interacting variable "length of stay" in order to investigate whether or not this particular the intervening variable influenced the relationship between predictor variables and outcome variables.
For the sake of readability of this study, most tables have been included in appendix one.
5.3 Results
5.3.1 Childhood traumas
The research subjects have suffered many traumatic events in their childhood. The most frequent traumas are: rape, physical abuse, parents' divorce and incest.
Table 5.1 shows the distribution of childhood traumas.
| kind of traumatic event | readmitted (n=26) | nominal numbers (n=52) | % of total (n=52) |
| incest | 53% | 17 | 33% |
| incest of sibling | 67% | 6 | 11,5% |
| par/rel. phys. abuse | 40% | 20 | 38,5% |
| phys.ab.m/sibling | 40% | 5 | 10% |
| rape | 50% | 22 | 42% |
| phys.ab by unkn.p. | 1 | 2% | |
| phys.ab.by r.subj. | 50% | 2 | 4% |
| mental abuse/cruelty | 50% | 2 | 4% |
| divorce | 39% | 18 | 35% |
| parents quarrel | 37,5% | 8 | 15% |
| death of a parent | 45,5% | 11 | 21% |
| death of a sibling | 33% | 3 | 6% |
| father unknown | 67% | 6 | 11,5% |
| no contact father | 1 | 2% | |
| mother prostitute | 2 | 4% | |
| alcohol abuse | 38,5% | 13 | 25% |
| foster care | 64% | 11 | 21% |
| adopt/rear.gr.par. | 75% | 4 | 8% |
| religious cult | 50% | 2 | 4% |
Table 5.1 Childhood traumas of readmitted research subjects (n=26) and percentages and nominal numbers of childhood traumas of the total group (n=52)
Number of childhood traumas
The research subjects' average number of childhood traumas is three (sd 1.6 with a minimum of 0 and a maximum of 7). For the variation of childhood traumas see figure 5.1.
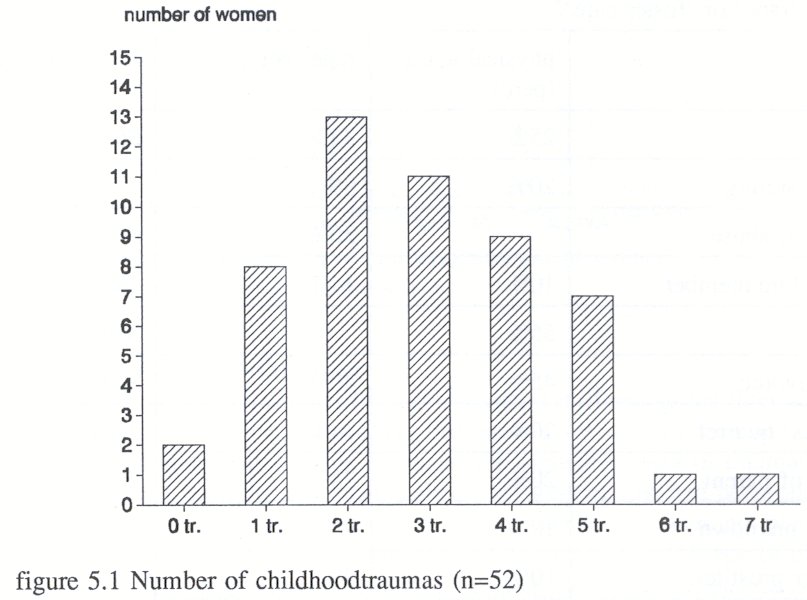
With regard to the number of childhood traumas, the group of women who were readmitted does not differ from the group who were not re-admitted within a year. Nor is there a connection between the number of childhood traumas and days in treatment.
Significant multiple traumas
Women who have experienced 'physical abuse', 'rape' or 'placement in foster care' have experienced significantly more traumatic events than women who did not experience these traumatic events, see table 5.2.
| kind of trauma | Spearman correl. | approx. signif. |
| physical abuse | 0,24 | 0,04 |
| rape | 0,24 | 0,05 |
| foster care | 0,39 | 0,02 |
Table 5.2 Spearman correlations of childhood traumas whose presence means that it is likely that the research subject did experience significantly more traumatic events.
Draijer (1988) found that people with a double trauma have more serious psychological disturbances than those with a single trauma. For this reason I investigated whether or not there is some pattern in the combination of other childhood traumas besides 'physical abuse', 'rape', or 'placement in foster care'.
Figure 5.2 shows the distribution of other traumas when a women experienced 'physical abuse', 'rape' or 'foster care'.
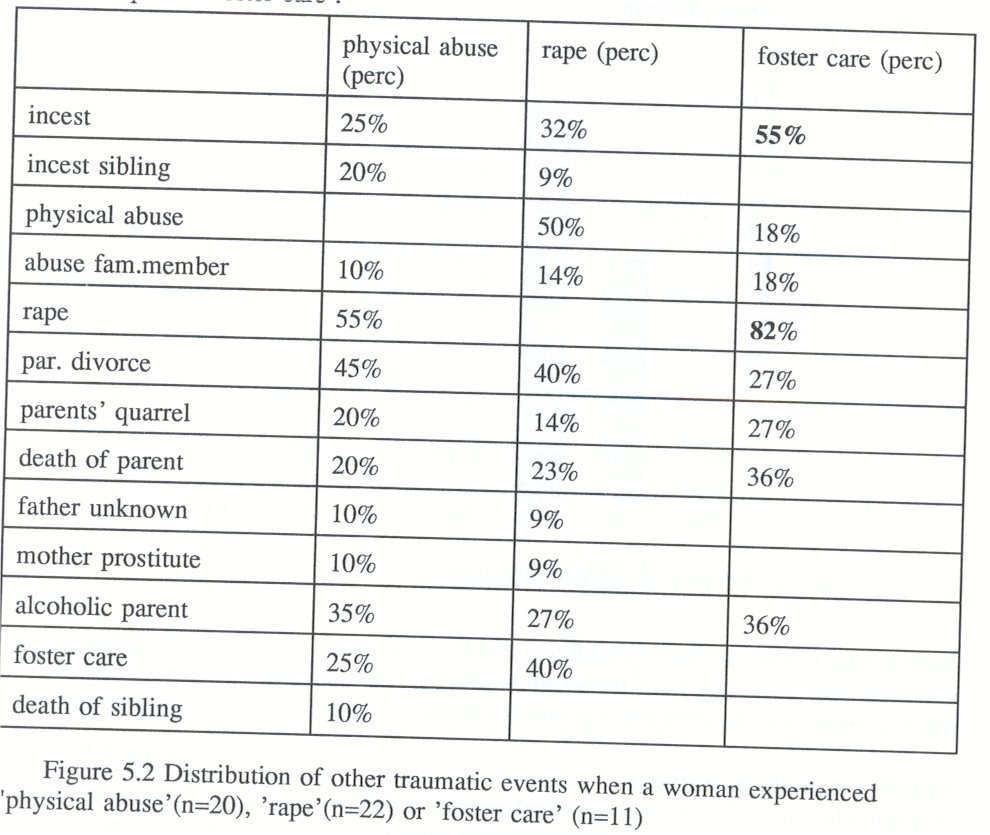
The above table shows that female drug-users who have been placed in foster care were more likely to be raped than women who were not placed in foster care. This relationship is also statistically significant (p=0,00, Pearson chi-squaretest). Of the eleven women who were placed in foster care, nine were raped and five suffered from incest (some experienced rape and incest).
According to the Pearson chi-square test there was no other significant relationship between the traumatic events.
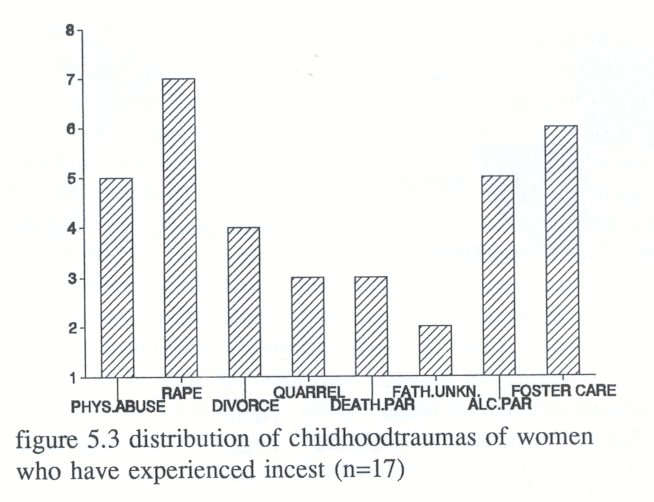
Although women with incest as childhood trauma have not experienced statistically significant more childhood traumas, the distribution of other childhood traumas besides incest is nevertheless given, because incest is, according to research, an important factor in the background of female drug-users (see figure 5.3).
Interdependency of childhood traumas
The previous statistical analyses showed that the occurrence of one of the three abovementioned traumas signified that it was likely that women who experienced one of these traumas had suffered more than average traumata (the average number of traumas was three). It also appeared from the statistical analysis that women who had been placed in foster care were more likely to be raped than the other women who were not placed in foster care. Some further analysis was conducted to investigate the existence of clusters of traumatic events. The data regarding childhood traumas was statistically analyzed (HOMALS), but there did not appear to be any statistically significant pattern or cluster of traumatic events. This means that the coherence between childhood traumas is arbitrary. This result is very important and will be mentioned in the discussion.
5.3.2. Prediction analysis of childhood traumas
No childhood trauma as such is able to predict time between discharge and re-admission to the VKC ( see table 5.3 and 5.3.1, appendix one).
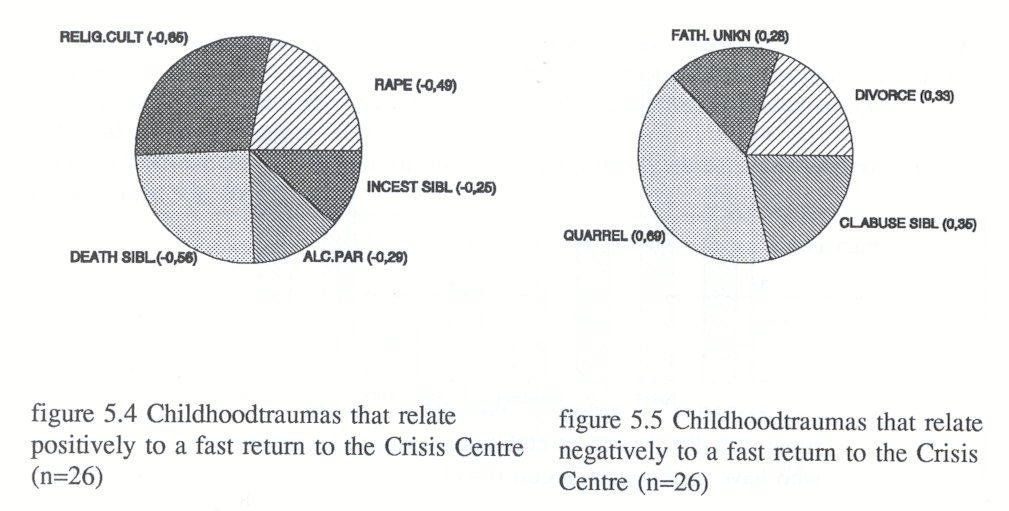
In combination, the childhood traumas predict re-admission at the Women's Crisis Centre quite well: r=0,87;p=0,00. Multiple regression analysis makes clear that some childhood traumas predict a speedy return to the Crisis Centre and some childhood traumas predict just the opposite. Figure 5.4 shows the childhood traumas that relate positively to a speedy return to the Women's Crisis Centre; figure 5.5 shows the childhood traumas that relate negatively to a speedy return to the Crisis Centre (see for data, table 5.4 and 5.4.1).
Childhood traumas and number of re-admissions
No childhood trauma as such predicts the number of re-admissions to the Women's Crisis Centre (see table 5.5, Appendix One). Multiple regression analysis shows that 'incest with sibling' somewhat predicts the number of re-admissions (r=0,24; p=0,10).
5.4 Discussion
The frequency, average number and severity of childhood traumas evoke the picture of the research subjects living in a trap for the rest of their days, with scarcely any opportunities to ameliorate their position.
On average the research subjects had experienced three childhood traumas. 'Incest', 'physical abuse','rape' and 'parents' divorce' happened most frequently.
The research subjects who experienced physical abuse, rape or foster care had experienced significantly more traumatic events. So when subjects have experienced one of these three traumatic events it is likely that they have been subjected to more than three traumatic events. Especially distressing, but nevertheless not remarkable, are the experiences of the research subjects who were placed in foster care (11 out of 52): nine of them were also raped (statistically significant) and five experienced incest. Placement in foster care is often a consequence of parental abuse or neglect.
The incidence of incest among research subjects (33%) is more than twice as high as among "normal" female population (Draijer, 1988) and equals the rate of incest found among psychiatric patients (Rosenfeld, 1979) and among female drug-users (Cohen & Densen-Gerber, 1982).
The incidence of sexual abuse committed by an acquaintance before the age of sixteen is somewhat higher among prostitutes (39%, Vanwesenbeeck et al, 1989), but some of these events are classified in the present study as rape (for example when the acquaintance does not belong to the family).
The physical abuse registered in the present study is of similar nature as Romkens(1989) described in her study of physical abuse, including being thrown downstairs, attempts to drown the child in the washstand, strangulation attempts and beating with a heavy object. In the present study the incidence of physical abuse is one and a half time as high as in Romkens'. This higher incidence could be caused by measurement: I measured the incidence of physical abuse until the age of sixteen, while Romkens lists the physical abuse of subjects of twelve and younger.
It is remarkable that besides the coherence between the childhood traumas of 'physical abuse', 'rape' and 'foster care' going together with more than three traumas and the significant relationship between 'foster care' and 'rape' there is, according to the HOMALS-analysis, no clustering of childhood traumas. This could mean that it would be wrong for researchers or therapists only to focus on one childhood trauma, for example incest. The present study shows that the research subjects have experienced a wide range of traumatic events, each one possibly as important as the other. On the other hand, this result could also refer to failures in the research design, for example the omission to incorporate 'age' as an important variable. Also no further differentiation took place with regard to the specific traumatic events, because the number of research subjects is small (n=52). It could be that further differentiation of the incest trauma would have produced other results. For example, with regard to incest Draijer (1988) showed that four abuse-indicators could be applied: unwantedness, negative perception, subjectively experienced inequality and involuntariness.
Initially, when I started this research, I thought that women who had experienced incest would return to the VKC more quickly than other women. This idea was based on some clinical examples in the VKC. My presumption about a fast return of women with incest traumas was also based on literature that showed the serious psychological consequences of an incest trauma. I thought it possible that the after-effects of the trauma might motivate or force the women to seek help. A short period between discharge and re-admission would prove the treatment need of women with the childhood trauma of 'incest'. This results show that there is indeed a relationship between childhood traumas and re-admission, because the re-admissions could be predicted quite well, but a relationship between the incesttrauma and a speedy return to the VKC is lacking.
Given the above results, it is not immediately evident why some particular childhood traumas ('rape', 'an alcoholic parent', 'death of a sibling', 'parent having incest with a sibling' and 'the family belonging to a religious cult') rather predict a faster return to the Women's Crisis Centre while others do not.
Viewing the data from the perspective of the strategy of 'having control over one's life', it appears that, in one way or another, all the childhood traumas which are responsible for a quick return to the Crisis Centre concern loss of control. 'Rape', 'an alcoholic parent', 'death of a sibling', 'parent having incest with a sibling' and 'the family belonging to a religious cult' might confront the child with a feeling of helplessness, painful grief, sadness and lack of parental comfort. It is possible that the above-mentioned childhood traumas lead to greater feelings of loss, powerlessness, emotional neglect, inner directed aggression, guilt and shame than other childhood traumas do.
Research subjects who have experienced 'quarrelling parents' as a childhood trauma witnessed perhaps a symmetrical fight between the parents, with both parents taking an equally strong position. Perhaps they attributed the problems they experienced to the parents' failing instead of to their own badness. It is also possible that the family, in spite of the quarrels, provided opportunities for relationships based on attachment. Contrary to children who experienced physical or sexual abuse, they might not feel overwhelmed by loss.
Examining the different effects of childhood traumas on the outcome criteria of this study, research by Carmen, et al. (1984) among files of 188 male and female psychiatric patients may possibly throw some light on the question of why these specific traumas predict a fast return.
The study by Carmen et al. (1984) showed that it is the way the victim of physical and sexual abuse deals with aggressive feelings that causes her or him to become a psychiatric patient. Inwardly directed aggression, including self-mutilation and suicide attempts, are related to childhood sexual abuse. Patients with a childhood sexual abuse trauma suffer more from inwardly directed aggression than patients who did not experience sexual abuse. Those who direct their aggressive feelings outward still believe they are able to influence their life, that taking control over their life is worthwhile.
In accordance with the study by Carmen (1984), the different effects of childhood traumas could be interpreted as a reflection of the way in which the research subject copes with problems. It is possible that the victimized research subjects anaesthetize their feelings and submit themselves to substance abuse or the violence of a partner. Perhaps a recurrence of assault, rape or physical abuse takes place quickly after discharge, again they find themselves in crisis and are dependent on support of the Women's Crisis Centre.
It could be that the research subjects with such childhood traumas as 'quarrelling between parents', 'divorce' and 'own abuse of other family members' have experienced more attachment and allow themselves more aggressive feelings and a more forceful stage-performance strategy as 'junky' and prostitute.
| < Prev | Next > |
|---|