| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4.1% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 175 |
| Yesterday: | 251 |
| This Week: | 175 |
| Last Week: | 2221 |
| This Month: | 4763 |
| Last Month: | 6796 |
| Total: | 129362 |
Chapter Seven.. THE ROLE OF THE MEDICAL PROFESSION
 |
|  |
| 
| Books - The Social Control of Drugs |
Drug Abuse
Chapter Seven.. THE ROLE OF THE MEDICAL PROFESSION
The apparent inconsistencies in the application of the criminal label have been a constant source of attention and interest since Professor Edwin Sutherland first brought out his treatise on White Collar Crime. The inconsistencies had of course been well known before that; perhaps epitomised in that beguiling and time-honoured phrase that there is one law for the rich and one law for the poor, but it was left to Sutherland to develop the concept and present it in a more academically respectable form.
Observers interested in pointing to the practice of police arrests are likely to notice police using dogs at the intersections of motorways examining the belongings of hitch-hikers, perhaps for traces of cannabis or other drugs, whilst on the motorways themselves drivers exceed the speed limit with apparent impunity. One group is the subject of police activity, whilst the other is ignored; yet speed kills on the motorways, so we are told, and cannabis like most of the other drugs is relatively harmless if taken in sufficiently small quantities (unless of course one is driving under their influence! ).
It is not for us to say that the police should not try to prose-cute those who illegally possess drugs; it is after all against the law, and their job is to enforce the law. They may believe that large quantities are being transported up the motorways—although, again, large quantities would more probably go in the cars themselves—but the main point is that police activity often appears to be directed primarily at those offences which rarely cause loss of life whilst in some part ignoring others which are potentially more dangerous. Moreover, one type of offence can involve a victim whilst the other is consensual or a victimless crime. In spite of these differences the legal system of control has provided special powers to deal with drug offenders (a point to be discussed later) but comparatively little attention is given to others who may be equally involved in the overall pattern of drug taking, i.e., the medical profession who supply the drugs. In this chapter I want to examine these differences and the key to the explanation lies, I think, in the medical profession's defini-tion of their role in relation to drug taking and its attendant medical problems.
All professional groups, and particularly the medical profession, attempt to define their role in terms of having a repository of specialised knowledge about a defined social problem.' If this knowledge is seen to be directed towards the public good the profession can then legitimately claim to be the sole arbitors and represent that group's interests. In this way the profession can also claim sole responsibility for that group and the profes-sion's status is defined in those terms. To retain that authority it becomes necessary constantly to define the problem within the profession's terms which means resisting redefinitions which could give the repository of specialised knowledge to another group. Once a redefinition occurs which encompasses another area of specialised knowledge then authority changes too. So, for example, when social workers claim to have knowledge which could redefine the problem of maladjusted children they are implicitly removing the responsibility for treatment from the psychiatrist in the child guidance clinic. Similarly when psychia-trists redefined the problem of 'mental illness' in terms of a breakdown in the normal pattern of childhood emotional developments they reduced the authority of the church who saw the illness as an evil visitation from a deity. When a redefinition occurs hostility is likely to develop between the competing groups which shows itself in terms of accusations about defects in practice. In this sense Terence Johnson is surely right when he argues that "No group is more morally outraged than a profession when laymen put forward opinions on occupationally related matters."2
The medical profession have until recently been able to claim sole responsibility for the drug taker because of the obvious relationship between addiction, the pharmacological properties of the drugs themselves and because the source of supply to the addict comes from the medical profession. Pharmacologists may know more about the properties of the drugs but as they do not directly supply or claim to treat, their authority is diminished. It was no accident then that the Rolleston Committee was composed almost entirely of medically qualified members. There was the occasional pharmacological member present but his main function seemed to be to give specialized support to the main character parts. Similarly, Lord Brain himself was a medical doctor as were most of the members of his committee. This meant that up to about 1965 the medical profession had a virtual monopoly about claims to treat the drug taker, and in the same way that a person with a broken leg automatically consults a doctor because no-one else is a serious contender for the treatment of broken legs, so up to 1965 no-one else was a serious contender to treat addiction.
Once authority is established all questions of aetiology and prognosis can be defined within those terms of reference. When the doctor/addict relationship was discussed by the Rolleston Committee questions of aetiology were included, and it did not occur to the Committee that they were not the right people to discuss these matters. The first Brain Committee using the same models refused requests for changes because they could not accept a different aetiological view and saw it in terms of occupations involving much nervous strain. It was only when authority was lost that there began a search for new 'causes' of addiction, this time in terms of social pathologies of broken homes or defective relationships or demands for immediate gratification. A shift in the authority has also demystified an area of the medical profession; they can no longer claim that all their members are equally competent as only a few can now prescribe opiates for the drug takers. This in turn had its own repercussions, notably a shift in what William Goode calls the corporate bargain. This point will be discussed later.
The medical profession's claim to be the sole authority has in practice exerted a considerable influence over the legal system of control. This, in spite of the fact that until 1955 a large part of the known addict population were from the medical and allied professions.3 So, for example, in 1923 Regulations were withdrawn which had previously forbidden doctors to prescribe maintenance doses of drugs for their own habit and in 1926 the Rolleston Committee was careful to make recommendations which would be acceptable to the profession as a whole. Even now, few controls exist over the prescribing of barbiturates and attempts to introduce such measures are strongly resisted. It is almost as if the profession is determined not to lose this last vestige of authority too, in spite of demands from many quarters to cut back supplies.
One of the best known examples of the influence of the medical profession occurred with the proposed heroin ban in 1955. This is a useful study in itself on the ability of a sectional group to exert pressure on the decision making process, but it is also an exemplary case of the profession zealously preserving its right to control its own use of drugs by its claim to be responsible for the social problem.
On the 18th February 1955 the Government suddenly announced that no further licences for the manufacture of heroin would be issued after 31st December 1955. In April, Lord Mancroft for the Government told the House of Lords that "the manufacture and export of heroin will not be permitted after December, except for small quantities used for scientific purposes." This decision was to give effect to a resolution adopted at the 18th session of the United Nations Economic and Social Council, urging that all governments should prohibit the manu-facture and export of heroin except for scientific purposes. Lord Mancroft later gave 5 reasons for the ban. Firstly, because heroin was one of the most dangerous drugs known and gave rise to an addiction problem of world-wide gravity. Secondly, it was easy to handle and therefore easy to smuggle. Thirdly, the existence of a serious black-market in heroin required the taking of exceptional measures. Fourthly, countries struggling with the problem agreed that if manufacture were illegal the task of suppressing the traffic would be easier; and finally, less dangerous substitutes were available.
The decision to ban heroin was not as completely revolutionary as it may first have appeared. As far back as 1931, the Expert Committee of the League of Nations noted that "heroin can in our opinion . . . be entirely dispensed with.'" On the 6th January 1949 The Times, in an editorial, said that "it is clearly the duty of the medical profession to examine again the therapeutic value of the substance . . . Since 1931 the profession has been deprived of heroin in some 26 countries without evident disadvantage . . . In'short, morphine or some related drug can always be used as effectively as heroin." In 1950 the World Health Organisation asked its member states to give their reasons for "the necessity for the use or the dispensibility of heroin . . ." The then Minister of Health, Aneurin Bevan, asked the Medical Advisory Com-mittee whether there were sufficient grounds why the Govern-ment should not support the ban. Their advice was "definite and decisive that it is justifiable to ban heroin." In 1953, the British Medical Journal, which had always taken a lively interest in these matters, listed 2 arguments for the continued use of heroin; that its physiological effects were more pleasurable, and that it pro-duced less nausea and vomiting than morphine. It concluded that "if these are the only indications for the use of heroin in preference to other drugs, they do not perhaps constitute very convincing arguments for its indispensibility in comparison with the cogent reasons for its abolition."
When the ban was announced, numerous letters of protest appeared in the medical journals, and The Times. In the British Medical Journal alone 17 letters appeared, with only 1 in favour, or at least proposing a compromise by suggesting that consultant physicians should countersign all heroin prescriptions. This suggestion was quickly dismissed by a subsequent letter saying that it was doubtful if consultants were more responsible anyway. Most of the doctors' letters complained of "intolerable inter-ference with doctors' liberties", and one thought the W.H.O. was a "sinister organisation bent on world government by any means in their power." The British Medical Journal shifted its position and hoped "the Government will see the wisdom of having second thoughts on the subject [since] it seems improbable that [the ban] would assist world-wide control."
Some writers saw the influence of the United States in the Government's decision as part of the American policy of trying to prohibit world-wide use of all narcotic drugs. As Britain produced 70% of the world's supply of heroin, this was an obvious target for a U.S. attack. One letter in the British Medical Journal on 17th December 1955 summed up the view and suggested that if the U.S.A. was involved, it had little to be worried about from Britain. "Let us try to put the matter in its true perspective. It has been officially stated that the total exports of heroin from the United Kingdom for the 12 months ending 30.9.55 were valued at £261. There are said to be over 100,000 heroin addicts in the United States alone. Now, even if the total heroin exported from the U.K. went to America, which is improbable, this deadly load would not really go far in victualling a heroin orgy. I make it less than /d. worth of heroin per known U.S.A. addict per annum. I cannot help feeling there may per-chance be some other source of supply which is not so readily or altruistically to be extinguished so easily."
Both sides of the argument were clearly stated in the House of Lords Debate on 13th December 1955. Lord Moran in favour of the ban quoted a letter from a late president of the American Medical Association saying that, "American experience is that nobody objects to the ban on heroin except the addict. The medical substitutes are entirely satisfactory." Lord Waverly, a former Home Secretary, argued that it was wrong for the Government to deprive a doctor from prescribing what he genuinely believed was necessary and in the best interests of his patients. Meanwhile, pressure from the British Medical Associa-tion continued and the Home Secretary received a deputation against the ban.' In June 1955 the B.M.A.'s representative body passed a resolution praising the value of heroin in glowing, almost unctuous terms. "That this meeting protests against the threatened withdrawal of the most excellent sedative heroin which is of estimable value in so many conditions . . ." The Lancet had adopted a more moderate course throughout. It noted that Britain was pledged to the United Nations to solve world problems and it was only by give and take that we could do this. The medical profession seemed, on the other hand, to be saying two separate things; firstly, that their right to prescribe what they wanted was no concern of anyone else, least of all the Government, or secondly, that the case for banning heroin had not been proved and it would be a mistake to lose its value for the sake of a small number of addicts in Britain, or a larger number in the U.S.A.
In December 1955 the Government gave way. On 13th December, Lord Jowett put down a motion for debate that "in view of the apparent conflict of expert medical opinion over the banning of heroin in this country, the period of the present licences to manufacture should be extended pending the institu-tion of further enquiries . . ." He also said he would question the right of the Secretary of State to prohibit manufacture. The question was submitted to the Law Officers for their considera-tion, and they concluded that Section 9 of the Dangerous Drugs Act conferred a power to control, as opposed to prohibit, manu-facture. Prohibition would not only prevent improper use, but proper use too. On 26th January 1956 the Home Secretary informed the House of Commons that "the Government has been advised that it is not possible under the present law of the country to prohibit manufacture of heroin." However, imports and exports were to be prohibited. The Leader of the Opposition, Hugh Gaitskell, asked if this meant that manufacture was to be permitted permanently, but the Home Secretary replied that licences to manufacture were only issued for 12 months anyway. That appeared to be the end of the matter, and nothing more was ever said.
The retention of this right to use heroin was shortlived as the 1967 Act allowed heroin to be prescribed for addicts only by doctors holding a licence issued by the Secretary of State. Yet the second Brain Committee spelt out in clear and concise terms that it considered the growth of heroin addiction in Britain to have been caused by the activities of a few over-prescribing doctors. In spite of this warning nothing was done by the profession itself, and there followed, in the words of one observer, "deafening silence".8
The Times in 1970 also thought that the medical profession had been responsible for the increase in drug taking yet the interesting point for our purposes is to ask why the medical profession was not criminalized as were the drug takers them-selves. Why, in fact, were legal controls directed at one group to produce special powers of search and arrest under the 1967 Act (see Chapter 8) whilst the medical profession was treated in a much more gentlemanly way. It is true that the profession lost its automatic right to prescribe opiates under the 1967 Act and that tribunals were established in 1970 but this did not stop members substituting other types of drugs such as methedrine and other amphetamines. Neither did it give the G.M.C. additional authority to deal with over-prescribing which after all was the accusation that The Times and the second Brain Report made against the profession.
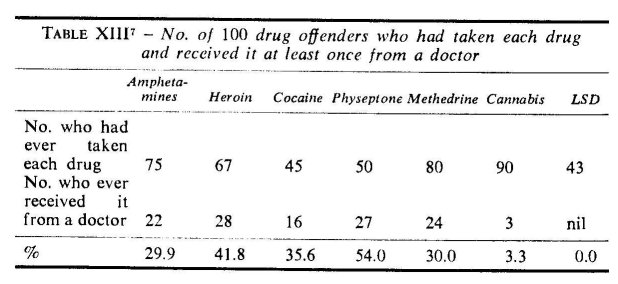
It is doubtful if we shall ever know the full extent of over-prescribing in the years prior to 1970. Some indications can be gauged from a study of a population of 100 drug offenders convicted at Bow Street Magistrates Court and Westminster Juvenile Court during the months of February to April 1968, i.e., before the treatment centres became operative. Seven drugs were listed on a schedule, and each subject was asked if he had ever taken these, and if so did he ever receive them from a doctor. Table XIII shows that only 41.8% of those who had ever taken heroin had received it from a doctor; there was an even lower percentage for those who had taken oral amphetamines, cocaine or methedrine. A small percentage said they had received cannabis on a doctor's prescription but this was tincture of cannabis, supplied in liquid form.
Those who had ever taken any of these drugs at least once a day for seven consecutive days were asked if they relied solely or partly on a doctor's prescription for this drug during that period. The result is shown in Table XIV.
This table shows that only 16 out of 51 daily users of heroin received these drugs wholly or partly from a doctor, and only 10 out of 43 for methedrine. A comparison betwen Tables XIII and XIV shows that there is a discrepancy between the figures of those who had ever received heroin from a doctor and those who were daily users. In other words, 28 people had received heroin from a doctor, but only 16 had ever taken it daily. The remaining 12 had presumably led the doctor to believe they were addicted to heroin as there is no other reason for prescribing it. Similar results are shown for other drugs. One cocaine user said he had only taken cocaine once, but received it on a doctor's prescription each day and sold it for extra methedrine. If these offenders are to be believed, some were using wholly illicit supplies and others receiving licit supplies but not using them. The population is, however, a small one and taken mainly from the Piccadilly Circus area of London, so it is unlikely to be representative of drug users in general. However, other studies have shown how comparatively easy it was to obtain supplies during this period. One such study quotes a Canadian who came to England and received supplies the day he landed. "I knew about this doctor, and several others before arriving. I said I was an addict, which I wasn't at the time, and I told the doctor I was using 4 grains of heroin a day, and that if possible I would like to be treated as a 'registered' addict. The doctor replied 'Certainly% it was a shock you know; I mean it was easy to get it."8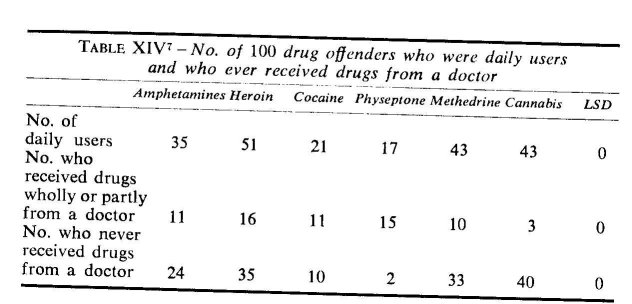
The Advisory Committee's report on Amphetamines and LSD notes that the misuse of injectable methedrine in 1967/68 cannot be fully understood without reference to two doctors who were responsible for prescribing in 1 month virtually all the methedrine misused at the time. One prescribed 24,000 ampoules to 100 patients, and even when the General Medical Council had recommended that his name be erased from the Medical Register, he lodged an appeal and continued to practice and prescribe for 4 more months. As far back as 1964 a question in the House of Commons asked the Home Secretary if he was aware that a doctor recently prescribed 800 drinamyl tablets a day for a family in Lancashire.
Even when there was a general agreement in October 1968 to stop prescribing methedrine, it was reported that some doctors circumvented this by prescribing amphetamine sulphate powder instead. This was the first time this drug had been prescribed in that form, and it was left to pharmacists themselves to issue an edict stating that prescriptions for amphetamine sulphate powder would no longer be dispensed. This edict was of some historical significance as it was the first time in 128 years that the Pharmaceutical Society had made such a decision. It was only later that the B.M.A. took up the matter and decreed that its members should not prescribe this powder.9
Tempting though it may be to think in terms of a small number of black sheep in a white sheep profession, Baroness Wootton believes that the 'grey sheep' ought to be reckoned with. The grey ones are those who prescribe rather more than the average, or seem unaware even of the implications of their prescribing activities. It was left to a few doctors to take the initiative themselves, and a small group in the Ipswich area argued that there were no medical reasons to continue with the use of amphetamines, and they believed it was in everybody's interest if they stopped issuing prescriptions.
Lord Cohen the president of the General Medical Council has said the law allows the G.M.C. to take action either where there is a criminal conviction against a doctor, or where a complaint has been made to the Council that a doctor is guilty of serious professional misconduct. The penalty in both these instances is to remove the doctor's name from the Register. Lord Cohen did not think the G.M.C. was strictly concerned with over-prescribing except where this amounted to serious professional misconduct. If a doctor over-prcscribes but thinks this is the right treatment, he is not guilty of misconduct or, "in other words, something done in good faith, even if done wrongly, cannot be regarded as serious professional misconduct."
To deal with improper prescribing as such, the President said new legislation would be required and the G.M.C. would have to be given additional powers. These would take account of cases where over-prescribing was alleged, even though the facts did not appear to raise a question of serious professional misconduct. Powers would also have to be given to direct or recommend that a doctor's right to prescribe should be withdrawn. The Advisory Committee on Amphetamines and LSD thought that the G.M.C. should be given these extended powers to deal with over-prescribing, but during the debate on the 1971 Act, the Government thought that the matter should not be allowed to rest with the G.M.C. The Home Secretary did not think the G.M.C. or its Disciplinary Committee were ready-made bodies suitable for enforcing any new restrictions and the law should therefore intervene. The basic difficulty about leaving the matter to the G.M.C. was that apparently terms like 'irresponsible prescribing' covered a wide variety of possible practices ranging from infamous conduct at one extreme, to poorly judged but bona fide attention at the other. The G.M.C. would need new resources to investigate irresponsible prescribing which would require new legislation. The Home Secretary also thought that the G.M.C. procedures would take longer to operate than the special machinery of the new Act. Lord Cohen has argued that the G.M.C. is not a police force, but a body solely concerned with certain types of misdemeanours which existed long before drug addiction became a problem. Even so, it is difficult not to agree with one M.P. who thought that whenever possible professions should discipline themselves, or with another—who is also a member of the medical profession—who thought that the profession had only itself to blame for the changes made by the 1971 Act.1°
It is nonetheless particularly interesting to compare the speed with which special powers were given to the police and the comparatively gentle pace at which the over-prescribing doctor was controlled. The doctor who prescribed 24,000 ampoules of methedrine to 100 patients in 1 month was still able to practice medicine at the end of that month, but the drug taker was subject to the search and arrest procedure, and if he sold one of these ampoules was liable to imprisonment. It is not difficult in these circumstances to echo Professor Quinney's remark when he argues that the criminal law is "formulated and administered by those segments which are able to incorporate their interest into the creation and interpretation of public policy."11
In line with current thinking there have been attempts to see these doctors as 'pathological prescribers' or as the black sheep in an otherwise white profession. This of course ignores Barbara Wootten's point of the numerous 'grey sheep' which may exist in rather large numbers. The regulatory mechanisms within the profession—which are themselves an important subsection of the sociology of law and one with which Max Weber was specifically concerned—help to promote the pathological prescriber image. When some 'pathological prescribers' were identified they were expelled from the profession amid consider-able drama. In functionalist terms the process seems to operate in the form of moral assassination or moral excommunication of the deviant members and the whole situation becomes over dramatized in such a way that the profession itself is left purified and immune to further criticism.12 So in London in the late 1960s 2 doctors who were thought to have over-prescribed drugs in large quantities were typical victims of such assassination ceremonies, or ritual cleansing as it seemed at the time. Of course the press and the Courts also play a part, one by banner head-lines and widespread coverage, the other by pronouncements which functionally attempt to redevelop social solidarity between the profession and its clients. Unhappily for the profession the process of purification was incomplete on these occasions as some measure of control was still exerted by the 1970 Act.
The relationship between the legal system of control and what Terence Johnson calls the "collegiate functions" of the medical profession, i.e., the G.M.C., is as yet still unclear. It is only possible to speculate about their influence after the 1964 Act as so many questions remain unanswered and are likely to remain so as long as negotiations are secret and take place in private. It would have been particularly interesting for example to know the nature of the negotiations after the 1964 Act when "profes-sional interests" were said to be involved.
Professor Quinney's perceptive remark about the formulation of law is an acknowledgement to that school of sociology which sees the criminal law as being connected with interest and power. Austin Turk's model of criminalisation is also based on the conflict theory of society when he says: "If law is seen as largely a pattern of conflict among parties seeking to protect and improve their life chances . . . then legality becomes an attribute of whatever words and deeds are defined as legal by those able to use to their advantage the machinery for making and enforcing rules. Political power determines legality."" Neither should it be seen that this approach is one conjured up by modern sociologists with an anarchist axe to grind. W. G. Carson points out that A. V. Dicey shared similar views when he said: " . . . it must at once be granted that in matters of legislation men are guided in the main by their real, or apparent interest. So true is this that from the inspection of the laws of a country it is often possible to conjecture, and this without much hesitation, what is the class which holds or has held predominant power at a given time."" Like Dicey, Quinney sees the criminal law as developing only by securing the interests of particular segments, supporting one group at the expense of others.
This perspective fits easily into the study of drug abuse. The medical profession, being a powerful group, were able to protect themselves, whilst the drug takers being less powerful quickly became the subject of a criminalisation process. There appears at first glance to be much in this argument, but as yet there are still many gaps in our knowledge which need closer examination than can be given here. What, for example, was the role of vested interest groups, such as the drug manufacturers? Some manu-facturers obviously supplied the methedrine which was being prescribed in 1968, but how and in what way did they influence the decision to ban it? Would the control of barbiturates in the 1970 Act reduce the amounts being prescribed, and if so what would the reactions of the manufacturers be? Or lastly, to what extent did vested interests affect the early control of drugs? We have already noted that the earliest control. was particularly acceptable since most of the drugs did not grow in Britain anyway, but how, and in what way, did groups encourage this selectivity? No clear answers can be given at this stage except to note that manufacturers have rarely been involved in the centre of any dispute. Perhaps their views were never sought."
If a straightforward conflict model cannot be realistically applied then how can we account for the lack of criminalization of a group who were said to be mainly responsible for the drug problem? The clue seems to lie in the notion of the 'moral centre'.
Troy Duster has provided a valuable account of how certain social classes are more susceptible to having the immorality of their behaviour underlined. Although he is concerned wholly with the American system of drug control, the relevance for Britain will soon be apparent. Duster argues that despite the even social class distribution of drug addicts in the U.S.A. in the 1900s, there was nevertheless a difference in the way the lower class addicts were regarded.16 He cites two interesting examples of the differences in moral interpretation of addiction. The first is from an article in the American Journal of Clinical Medicine in 1918. The author, G. Swaine, classifies addicts in two classes, but whereas he sees addiction in one class as being a vice, in the other it is an incubus. "In class 1 we can include all the physical, mental and moral defectives, the tramps, hoboes, idlers, irres-ponsibles [and] criminals. In these cases morphine addiction is a vice as well as a disorder resulting from narcotic poisoning . . . In class 2 we have the many good citizens who have become addicted to the use of the drug innocently and who are in every sense of the word 'victims'. Morphine is no respecter of persons and the victims are doctors, lawyers, ministers . . . women . . . all of whom realise their conditions and want to be cured. In these cases morphine addiction is not a vice but an incubus . . ."
Or again, this time from a different author in 1920: "Drug addicts may be divided into 2 general classes. The first class is composed of people who have become addicted to the use of drugs through illness associated probably with an underlying neurotic temperament. The second class which is overwhelmingly in the majority . . . have become addicted . . . through association with habitues and they find in the drug a panacea for the physical and mental ills that are the result of the lives they are leading. Late hours, dance halls and unwholesome cabarets do much to bring about this condition of body and mind."
Notice how in the first example Swaine calls those in class 1 "mental and moral defectives" but those in class 2 are "good citizens who have become addicted to the use of the drug 'innocently' ”. In the second example there are those who became addicted "probably due to an underlying neurotic temperament"; others "as a panacea for . . . mental ills [due to] . . . the lives they are leading." One class is given a clinically and morally neutral aetiology; the other has the moral twist of the term 'panacea' and the subtle condemnation in the phrase "the result of the lives they are leading."
The focus of Duster's argument is that a shift in the class structure of American addicts produced a corresponding shift in the moral interpretation of addiction. Duster points out that when the addict in the U.S. came to be perceived as predomi-nantly young, male, working class and negro, "the bridge between law and morality was drawn". This is similar to Becker's
1,0 point when he drew attention to the 1937 Marihuana Tax Act as being a racist act since most of the Marihuana users were then negroes. Duster, however, carries the point a stage further by concentrating on the shift in evaluating the moral implications of addiction. He argues that certain social categories are the least vulnerable to the charge of immorality, so that when the stage is set and the conditions are ripe for labelling immorality, the effectiveness of the law in bringing about these presents a basically different problem. He argues that, "so long as an activity is engaged in predominantly by those in the 'centre' social cate-gories, the likelihood of moral condemnation for the activity is miniscule for it is the 'centre' of society which establishes the criteria for moral condemnation."17
The importance of Duster's work in pointing to the centre is to illustrate how different problems are presented to the designators when they are concerned with labelling the centre's behaviour as immoral. This is not a structuralist argument as such in that the centre has a right to define conduct as legitimate, but that social orders can be maintained by appealing to legitimacy so that consensus occurs at a symbolic level. Hence the issue is about perception and has to be seen inside the frame-work of the sociology of knowledge. As an analytical tool it is imprecise as the boundaries of the centre can never be clearly formulated although its value lies in the way in which it can point to certain groups such as the Court, the Police and the medical profession who can be said to epitomize the centre's values.
In Britain the medical profession is so obviously part of the centre that Duster's argument needs no illustrative material to support it. Duster was, however, mainly concerned with the American addict but the point has immediate appeal to the British medical profession. The additional complication here is that the medical profession are not only from the centre but have the important function of having sole responsibility for the drug takers who they were producing. Furthermore they were equally responsible in their defined term for the barbiturate addicts who were not the subject of control, and who too were thought to be from the moral centre. The dangers of total control would mean affecting both groups as well as affecting the service given to a whole range of other patients. Alternatively, excessive control could affect the corporate bargain which means a mandate and high status are given to professions in return for guarantees that the profession will not exploit its clients. Once adjustments in the corporate bargain become necessary we can be sure they will involve discussions of a lengthy and protracted nature, for excessive control would be as damaging as too little.
The particular difficulties then of criminalizing the medical profession involve not only the problems of underlying behaviour at the moral centre but of disrupting a system in which only certain segments are seen to need control. One can only speculate that the medical profession was a willing party to the 1967 and 1970 Acts which imposed a restriction on prescribing and introduced the tribunals, and the profession may have been pleased to off load those segments which had begun to tarnish a glossier image. In contrast the drug takers possessed none of the medical profession's qualities; they had shifted from the centre since the 1920s, were hostile to basic norms to the point of being unrepentant deviants and could not claim to have a repository of special knowledge which was directed toward the public good. Criminalization for them was comparatively easy.
We are now in a position to make a theoretical link between this and the previous chapter and relate the changes in the legal controls to the changes in the drug takers and the lack of criminalization of a profession who were said to produce the problem. Several legislative changes first require a shift in the basic social components of the group to be controlled. New controls will be facilitated when that group is not of the centre, is hostile to basic norms and whose hostility and behaviour is unrepentant and visible. Conversely groups are able to resist controls if they are of the moral centre and can claim to have other knowledge directed to the public good. Once they resist control they are then able to resist criminalization.
Much of this analysis seems to fit in well with W. G. Carson's study of factory legislation.18 Carson has shown how violators of the Factory Acts in contemporary Britain are frequently given a number of warnings before being prosecuted, and even when a prosecution occurs the offenders are dealt with in a gentlemanly way. The annual reports on factory legislation rarely convey the moral overtones of the Criminal Statistics or the reports of the Prison Department. In this context, the factory owners, being A businessmen, are obviously 'useful' members of society since they are among the main producers of wealth. Coming from the centre, they too are hard to criminalize. In fact the terminology used to describe factory violators is similar to that used to describe the technical offenders in the 1930s. They were 'technically' rather than 'morally' guilty and like the serious motoring offenders of today are described as having had 'accidents' to avoid the moral hectoring which so many other offenders receive.
The idea that the centre's values can offset severe moral condemnation has been well known by many people who have appeared before the Courts; offenders who are unemployed and bailed will try to find work before reappearing at Court to show they can be perceived as 'useful' members of society. This useful-ness is, of course, defined in terms of the values of the centre. Scott and Lyman have also shown that the problems for many people who appear in Court are to provide accounts and excuses which are seen as legitimate in terms of the value patterns and moral beliefs of a power structure personified in the Court of Law.'9 If one can also add a peculiarly centre type argument to appeal to the Court in language which they understand, the chances of escaping moral condemnation are greater. The tech-nical offenders of the medical profession can always plead 'over-work' or 'excessive bureaucratisation' to account for their lapses.
Such a view is likely to be understood and to receive a sympa-thetic hearing, especially if the offenders are also able to plead devotion to more 'useful' duties such as curing the sick or running a business. In other words, the system works to maintain agreement at symbolic level despite the existence of conflict.
This analysis is obviously incomplete and should only be considered as a tentative step in a largely uncharted field. Subsequent sociologists might, for example, see difficulties in attempting to combine in any theoretical way the studies on factory legislation with studies on the legal control of the professions. Though shading into each other, they could be analytically different. It may be, for example, that the structure of professional organisations, with each member being an individ-ually separate professional person, casts them into a different sociological category from the factory owners and other business entrepreneurs. The latter cover a wider distribution of the class system, have a less complete representation in any bargaining procedure, and their activities may not always be seen as 'socially useful'. In this way different considerations may operate and different compromises need to be made.
REFERENCES
1. Johnson, T., Professions and Power, Macmillan, 1972.
2. ibid., p. 57.
3. lt is particularly interesting to note that few pharmacists have been addicts although they have similar access to drugs as doctors. E.g. in 1936 for the 137 addicts from medical and allied professions 127 were medical practitioners, 3 were dentists and 2 were veterinary surgeons. There were only 5 pharmacists.
4. For a full discussion of the report see The Lancet, 1931, i, 191.
5. Home Office Statement, llth July 1955.
6. See Parliamentary Report on Second Reading of 1970 Drugs Prevention of Misuse Bill, 16.3.70.
7. Tables from Bean, Philip, 'Social Aspects of Drug Abuse' in Journal of Criminal Law, Criminology and Police Science, Vol. 62 No. 1, March 1971. Reprinted by special permission of the Journal, copyright C 1971 by Northwestern University School of Law.
8. Gillespie D. et al. 'Drug Dependence and Drug Abuse in England' British Journal of Addiction, Vol. 62, p. 165.
9. See Hansard 16.3.70.
10. Apparently the problem of over-prescribing is not confined to Britain. In 1956 in Paris there were said to be 768 addicts with a mean age of 37 years; 275 of these received their drugs from a doctor. In a study of these addicts the author concluded that "disagreeable as the admission may be, it must be recognized that the real origin of many cases of drug addiction is the incompetence of the attending doctor". Apparently only 10 of these 275 addicts supplied by the medical profession had been justified in receiving supplies at all. See Annual Report of the Permanent Central Opium Board, 1956.
11. Quinney, R. The Social Reality of Crime, Little Brown, 1970, p. 39.
12. I am grateful to Dr. Roy King for suggesting this point.
13. Turk, A. Criminality and Legal Order, Rand McNally, 1969, p. 32.
14. Dicey, A. V. 'Law and Public Opinion in England during the 19th Century' quoted by Carson, W. G. in 'The Sociology of Crime and the Emergence of Criminal Laws', a paper given to the British Socio-logical Association, 1971.
15. See particularly Becker, H. Outsiders, op. cit., p. 135—l46, for an account of how the American Hempseed Industry successfully lobbied Congress during the proceedings of the Marihuana Tax Act.
16. Duster, T. The Legislation of Morality, The Free Press, 1970, p. 10.
17. ibid, p. 238.
18. Carson, W. G. 'White Collar Crime and Enforcement of Factory Legislation' British Journal of Criminology, 1970.
19. Scott, M. and Lyman, S. 'Accounts, Deviance and Social Order' in Douglas, J. (ed.) Deviance and Respectability, Basic Books, 1970.
| < Prev | Next > |
|---|