| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 193 |
| Yesterday: | 251 |
| This Week: | 193 |
| Last Week: | 2221 |
| This Month: | 4781 |
| Last Month: | 6796 |
| Total: | 129380 |
CHAPTER VI PATHOLOGY TOLERANCE—DEPENDENCE—WITHDRAWAL
 |
|  |
| 
| Books - The Opium Problem |
Drug Abuse
Whatever the school of thought as to the general nature of chronic;; opium intoxication and whatever the theory advanced in explanation of its mechanism, every one is agreed that individuals in this condition can take increasingly large amounts of the drug, amounts that would be fatally poisonous to the unaccustomed individual. This characteristic commonly is designated as tolerance and indicates an artificially established resistance or immunity to the drug in question.
In order for tolerance to be established, a variable period of time s' is required and the increase in dosage as a very general rule must be quite gradual in the beginning. The degree which this tolerance may reach is very great and practically every text-book cites cases (, in which, in comparison with the usual minimal fatal dose, this tolerance has reached an astounding point. Such cases, however, while of passing interest, have no especial significance, as they indicate, in degree only, a difference in the ability to withstand poisonous doses.
This tolerance constitutes the only fundamental characteristic of chronic opium intoxication that is generally conceded. There are those, however, who include as an important and universally present feature 's and as developing pari passu with tolerance an organic or functional dependence, as evidenced by the withdrawal phenomena, which requires the continuous taking of the drug in order to maintain equilibrium or a state of being which to the individual concerned, is normal. Others, admitting the existence of tolerance, deny or minimize the development of a dependence and claim that the withdrawal symptoms - evident upon stoppage of the drug are simulated or if existing at all exaggerated in order to obtain the drug.
Before presenting the reports of work dealing with tolerance, it ' seems advisable briefly to consider a question concerning which there has been some disagreement, namely, the ability of codein to stimulate the development of addiction. Acknowledging that the crude drug and its derivatives, morphin and heroin, possess this characteristic, certain writers, however, deny that it is possessed by codein. In other words they claim that as an evidence of dependence the withdrawal phenomena observed in abstinence from other opium preparations do not appear in the case of codein withdrawal or they are so slight in degree that they require no special consideration.
The controversy arising from this difference of opinion seems to have centred chiefly around two points,—first, whether or not codein is a desirable substitute for morphin or heroin in the treatment of chronic intoxication to these drugs by lessening very materially the withdrawal phenomena and by being itself easily discontinued; second, whether or not codein should be included in the restrictions thrown around the distribution of opium derivatives, in view of the alleged absence of the qualities possessed by other opium preparations. Thus, the report of the Committee on Narcotic Drugs of the Council on Health and Public Instruction of the American Medical Association, composed of Drs. Haven Emerson, George W. McCoy, Thomas S. Blair, and' Alfred C. Prentice, made at the 1921 meeting of the Association in Boston,' included the following item among its opinions presented for consideration:
"4. The use of apomorphin and codein rarely if ever leads to the development of addiction to these drugs. Their physiological effects are such as to preclude the probability of their becoming of any importance as habit-forming narcotic drugs. The committee recommends that the American Medical Association respectfully urge on Congress such amendment of the Harrison Law as will permit the prescribing of apomorphin and codein by physicians without limitations which it is recognized as suitable to impose on those prescribing other habit-forming narcotic drugs."
The report of this committee was commended by the Reference Committee on Reports of Officers which recommended its continuance. The report of the Reference Committee was adopted by the House of Delegates.
Kengla,2 1895, reports the treatment of a case of morphinism where the morphin was rapidly reduced and codein substituted. He states that in several weeks the patient was getting nothing but water hypodermically. This case was an office patient. The patient is reported' as having suffered but very little.
Bouma,3 1903, reasoning from the experiments of Faust that the virtually complete recovery of injected oxalic acid in the excreta of dogs explained the fact that tolerance to this substance was not developed and that conversely the ability of the organism to destroy morphin accounted for the tolerance to this drug which his animals developed, undertook to show whether tolerance to codein appeared after continued administration over a long period and whether, provided such tolerance was produced, the organism could acquire an increasing ability to break up and destroy the codein. He records the details of his experiments on dogs and comes to the following conclusions:
"It is seen that 4/5 of the codein injected is excreted in the urine and feces, mainly with the former, that on continued administration of codein the organism does not develop the ability to destroy the codein, and that instead of a chronic intoxication to this substance rather an increased sensitiveness appears.
"If we compare the behavior of the organism toward the two substances which are so closely related chemically, morphin and codein, we shall find that the hydroxyl group of morphin esterized in codein forms the basis for the fermentative and oxydizing splitting off, which leads to the destruction of the morphin molecule. Also in my codein experiments the organism could create no new factors for the destruction of the codein.
"According to the results of my experiments as well as the tests made by Faust in his experiments with oxalic acid, it is indisputably shown that an explanation of the fact that chronic intoxication does not appear after the continuous administration of codein may be sought in the inability of the organism to destroy this morphin derivative."
Babel,4 1905, found that a pigeon, which had been treated with morphin for ten months and was able to tolerate a dose greater than the minimal lethal dose, died four hours after the injection of a dose of codein.
Sollier,5 1905, states:
"We too often forget that the derivatives of opium are all the same from the point of view of intoxication and that they do not differ at all from the point of view of tolerance and of the patient's resistance, except as a result of the method of their introduction into the body."
In 1920," in commenting on the use of substitutes for morphin during suppression, he states that the use of such drugs is based on the erroneous assumption that there are substitutes for opium. In whatever form this latter occurs, nothing can replace it and this must not be forgotten. Such substitutes are, however, frequently advocated by fallacious statements which offer certain opiate preparations as inoffensive and above all incapable of setting up tolerance,—a mistake no less disastrous because there is no derivative of opium, not a single opiate preparation whatsoever, which does not inevitably lead to chronic intoxication.
In more recent correspondence Sollier again emphasizes this fact in the following paragraph:
"There is no derivative of opium, in spite of the pretended virtues of pantopon, paveron, opon, etc., which does not produce tolerance under the same conditions as morphin."
In 1913' Sollier reported a case of pure chronic codein intoxication, stating that although codein in order of toxicity comes next to morphin but third as a soporific, it is not much used by these cases probably because its analgesic properties are slight. The case which he reports is that of a physician 72 years old who took codein for rheumatism reaching a daily dose after about 3 years' use of 2 grams. In treating this case Sollier reduced the drug more slowly than usual, taking 8 days to withdraw it entirely. The symptoms, he states, were the same as in morphin withdrawal, but less intense,—insomnia, sweats, bilious stools, nausea, weakness, pain in the legs, etc. Several crises occurred as did other symptoms during convalescence. Recovery occurred as in the case of morphinists. At the end of 4 weeks the patient slept 5 or 6 hours at night. He states that the withdrawal symptoms are the same for all derivatives as are the symptoms of intoxication. The duration of the body's reaction to withdrawal is practically the same for all opium preparations and the return of the body functions to normal occurs in the same order. The elimination of codein is accompanied by the same phenomena as that of morphin and progresses in the same way with eliminatory crises.
Langer,8 1912, working on the recovery of heroin and the establishment of tolerance to this drug calls attention to the double action—narcotic and stimulating—which is seen in heroin and codein. He states that up to that time little work had been done toward determining how these two attributes are affected during continued injections. He states that the decreasing narcotic action observed in heroin is analogous to the action of codein as stated by Bouma. The latter, he says, while interested chiefly in the stimulating action of codein, noticed a gradual decrease in the narcotic action upon the continued administration of even doses. He assumes that Bouma used large doses in which the narcotic effect was effaced in some degree by the stimulating effect, but states that Bouma should have observed—if no tolerance to the narcotic component appeared—the struggle between narcosis and stimulation described by Schroeder in the higher doses as well. He points out the desirability of carrying out further experiments with smaller amounts of codein while studying from the clinical aspect tolerance to the narcotic principle of this drug. This partial tolerance to the narcotic property of morphin ether and ester, he states, is not easily reconciled with the hypothesis that tolerance to morphin depends alone on an increasing disintegration in the body.
Pettey,° 1913, says as to the development of tolerance to codein:
"The only essential difference presented by users of various preparations of opium is in the time required for the disease to be confirmed, and in the prognosis. One of these differences is that codeine and heroin can be used for a longer period without formation of addiction than any of the other preparations of opium."
Lambert,10 1914, says:
"A few cases of heroin and codeine addiction have come under the writer's care, one patient taking 30 grains of codeine a day."
In 191511 he states:
"The impulses leading to the addiction of codeine, morphine and opium arise from the desire for narcotic forgetfulness rather than for a stimulation of personality."
In 1922,12 Lambert reports that in a series of 1,593 users of narcotics studied by him 17 "had the codein habit."
Myers,'3 1915, from a study of cross-tolerance to codein, heroin, cannabis indica and chloral hydrate in dogs already tolerant to morphin, reaches the following conclusions:
"1. A marked crossed tolerance exists to codein and to heroin in dogs habituated to morphine, in so far as effects upon the respiratory center are concerned.
"2. A slight crossed tolerance exists between codein and morphine, and between heroin and morphine in regard to their actions upon the tissues governing equilibrium.
"3. Dogs tolerant to morphine when given codein or heroin have increased intestinal peristalsis.
"4. No evidence of crossed toleration to cannabis indica or to chloral hydrate exists in dogs tolerant to large amounts of morphine.
"5. The experiments cited show that a cross tolerance may exist between closely related drugs but that this tolerance is evidenced only on those functions in which the drugs have a common selective action."
"As far as this study shows, therefore, a crossed tolerance involves only those structures upon which the drugs exert effects mutually alike."
Wilcox," 1917, states that codein is much less likely than morphin to produce addiction and in 1917 Potter'' makes the same statement, while in 1918 Bastedo 16 states that codein is not "a vicious habit drug."
Cushny,n' 1918, states:
"No tolerance is acquired for codeine even after long use, and patients may in fact appear more susceptible to the drug, a dose which at first gave relief now causing nausea and vomiting. It is possible that this may indicate a tolerance of some parts of the central nervous system, which is not shared by the vomiting centre."
"Codeine is much less often used than morphine in therapeutics. It is of comparatively little value in allaying pain or excitement, but has been found of benefit in the sleeplessness of melancholia. It is used not infrequently as a sedative in cough, and, as has been stated, in diabetes. There is little or no tendency to form the codeine habit, and it has been suggested as a substitute for morphine in morphinomania, but has not proved efficient in this condition."
White,78 1918, states in connection with the substitution of certain drugs in the treatment of chronic opium intoxication:
"It is necessary to call attention to the danger of cocaine for this purpose. Codeine has also sunk into disuse and the synthetised derivatives of morphine, heroin, dionin and peronin cannot be said to be any better. Their use is founded on a wrong theory and is fraught with danger. Cases of serious addiction to codeine and heroin have been reported."
Baumm,1° 1919, observed no chronic intoxication as a result of the use of eukodaI, a new codein derivative, in about fifty cases.
On the other hand, Alexander,20 1920, reports a case of eukodalism.
Biberfeld,21 1920, reports on the effect of the codein derivatives, eukodal and parakodin, on a rabbit and a dog and concludes as follows:
"1. Eukodal paralyzes the respiration much more strongly than morphin, but it is less poisonous than heroin; the general narcosis is likewise greater but more transient than after morphin.
"2. Rabbits do not become addicted to eukodal (respiration and cerebrum), in dogs the sedative action quickly disappears upon repeated injections and the stimulating action peculiar to large doses then appears.
"3. Parakodin acts more strongly on the respiration than codein, less strongly than eukodal and morphin; dogs exhibit an addiction to the sedative component of the action.
"4. Eukodal and Parakodin paralyze the isolated rabbit intestine."
Watson,Y2 1922, reports on an original questionnaire study among the physicians of Maryland to the effect that from 700 replies to 1,250 inquiries "no case of codein habit had ever been seen in Maryland." He concludes:
"Codein is one of our most useful and most commonly prescribed drugs. It is not a dangerous drug. No detailed account of a death from it has been found. No textbook gives the lethal dose. It apparently is not habit-forming. Known for ninety years, and extensively used for more than thirty years, only four cases of habit are mentioned in the literature. One of these cases is questionable, and the other three so easily cured as to make them negligible. Codein was used on an enormous scale in the United States for twenty-five years without restrictive laws, with apparently no habit formation. To a large extent, it displaces the use of morphin and heroin, which are habit-forming. Its inclusion in the Harrison law seemingly misbrands the drug and the physician who prescribes it, and imposes an unnecessary hardship on the physician, patient and druggist and useless expense on the government. Unless some as yet unreported evidence of habit comes to light, codein should be eliminated from the Harrison law."
Williams,23 1922, says:
"Yet, if neither heroin nor morphin is available, the habitué can get a somewhat similar effect—can at least avert the worst phases of withdrawal suffering—by large doses of either codein or dionin. He would not have his suffering and craving entirely relieved, but would have them very decidedly mitigated. And if the use of these drugs were continued, he would presently reach a stage in which he would be comfortable and without the old craving so long as his system was saturated with codein or dionin. This condition would be a very decided step toward recovery, because codein and dionin do not produce a `habit' of any such intensity as do morphin or heroin, and may be quickly reduced and withdrawn without any very great discomfort to the patient."
Gunn,24 1923, in a review of the literature on tolerance to non-protein substances, states:
"Habit and tolerance are common in man to heroin, rare to codeine."
"To sum up the question of acquired tolerance to these morphine alkaloids, it may be said that tolerance is acquired easily to morphine, less easily to heroin, and with great difficulty to codeine."
Rogues de Fursac and Monestier,25 1924, report the development of addiction to codein in a young woman who was given codein and potassium iodide in the course of treatment for asthma. The codein caused in this case a distinct euphoria which led her, as tolerance developed, to increase the dose up to 1.0 g. a day. Menstruation ceased as the higher doses were reached. Treatment induced withdrawal symptoms milder in degree than those usually seen in cases of morphinism, but characteristic in type—insomnia, diarrhea, cramps in the leg muscles, etc., and return of menstruation.
The authors question, in view of the occurrence of such eases, the wisdom of excluding codein—under the French law of 1916—from the regulations governing the sale and distribution of other opium alkaloids.
Sollman,28 1926, in comparing morphin and its esters, says:
"In principle, all morphine esters are presumably capable of producing addiction; but practically the difference between them is very large. This depends on the quantitative response: the more powerful is the narcotic effect of the alkaloid, the more easily is the habit induced and carried on, and the more difficult is it to break. Heroine is rather more powerful than morphine, and the addiction is consequently somewhat more serious. The narcotic action of codeine is so slight that it is not very tempting to addicts, and really narcotic doses would be inconvenient to administer, and disproportionately expensive, so long as its sale is restricted. If restrictions were removed, however, so that it could be procured in unlimited quantities the situation might become very different. With medicinal doses of codeine, the psychic effects are so slight that they would scarcely be recognized by the patient; and there is therefore no temptation to increase the dosage; and the codeine can be withdrawn without much reaction on the part of the patient.
* * * *
"Codeine Addiction.—The rarity of this may be judged by the report of Watson, 1922, that replies from 700 physicians, including sanitaria and prisons, do not record a single case of codeine-addiction. Only three cases are found in the literature, and these were so mild that they could be broken in a few days without marked abstinence symptoms. The dose recorded was 2 gin. per day (cf. also Pelz, 1905; Petteys).
"Derivatives of codeine with more marked narcotic action produce addiction (`eukodal' and `parakodin'; Biberfeld, 1920 and 1921). The acquired tolerance does not extend to the convulsant action."
In a report by Terry,20a 1927, on studies conducted by J. W. Cox for the Committee on Drug Addictions, dealing with the per capita use of opium, coca leaves and their derivatives, and the variations observed in the per capita figures, two cases of codein addiction are recorded as follows:
"Inquiry among the Montgomery physicians as a whole failed to indicate experience with codein addiction or belief in its existence except in one instance. This physician reported in detail two cases of codein addiction, the main features of which follow.
"The first case, a man thirty-seven years old, had been addicted to the use of codein for about twelve years. During this time he had used no other opium derivatives, excepting for a short period during the survey year, 1923-24, when he supplemented his codein with morphin. When, however, the federal agents interfered with his orders for morphin he returned to the use of codein alone. He used, during the survey year, 4.108.5 grains of codein sulphate, about eleven grains a day.
"The other case was a woman, forty-four years old, who was known to have been using codein hypodermically since 1918. For the first year or two it was understood that she used one grain daily. During 1922 and 1923 she used about two grains a day, and in 1925 she was using four grains a day.
"Both of these cases, their physician stated, had been treated unsuccessfully and when withdrawn from the codein showed the same symptoms as those resulting from morphin abstinence, presenting the same difficulties of treatment and the same tendency to relapse."
To return to the main subject under discussion, the reader will find the most important opinions as to the mechanism of chronic opium intoxication as evidenced by tolerance, dependence, and withdrawal symptoms, whether or not supported by evidence comprised in records of experiments or observations, set forth below. However, we would point out that we are handicapped in attempting to cover this material, an appreciation of which depends to a very great degree upon the correct interpretation of highly technical laboratory methods and procedures. It is manifestly impossible, however desirable it may be from some viewpoints, to quote in full the details of technique of the individual experiments. We have sought, therefore, in the brief presentation which follows merely to acquaint the reader with the chief theories and pieces of work relating to this important aspect of the problem, hoping to stimulate both a more critical review of the complete works quoted and original speculations.
W. Marmé-1883.2T
In a study of the fate of morphin in morphinized dogs, Marmé detected the presence of oxydimorphin in an extract of the lung and liver and came to the conclusion that morphin in chronic intoxication is changed to oxydimorphin, a toxic substance causing, when not neutralized by further morphin, the abstinence symptoms. Marmé maintains that on the injection of a sufficiently large quantity, oxydimorphin produces symptoms similar to those exhibited on the withdrawal of morphin from a morphinized body. From these observations Marmé appears to conclude that the oxydimorphin requires increasing amounts of morphin to neutralize its toxic action and on the other hand neutralizes the effect of the morphin.
According to Du Mez: 28
"This theory, however, appears to be untenable in view of the fact that Donath," Stark' and Marquis,` respectively, operating under similar conditions, could not identify oxydimorphin in either the blood or urine of dogs in which tolerance to morphin had been established. Furthermore, it has been shown that oxydimorphin prepared from morphin with the aid of certain plant juices (Bougault ") or by the action of various oxidizing agents in alkaline solution (Schutzenberger,n Nadler," Polstorff ") does not possess the properties assigned to it by Marmé. Magendie V found it to be inactive when administered by mouth to dogs in doses of 0.36 grain, while Kreis" observed that it had a very weak morphin-like action. When given intravenously, the latter found that it produced weakness which soon developed into stupor. Toth found it to be inactive when administered by mouth or subcutaneously. He attributed the effects observed by Marmé to emboli, formed, in his opinion, as a result of precipitation which occurred when oxydimorphin was injected into the blood stream. Additional investigations demonstrating the relative inactivity of oxydimorphin and the erroneousness of Marmé's conclusions have been reported by Kobert,V Diederich,b Puschmann; 3 and Gioffredi." "
E. Hitzig-1892.43
In a report on the relation between morphin withdrawal symptoms and the stomach, stimulated by the observation of symptoms of morphin poisoning in a dog that had fed on the vomitus of another dog suffering from acute morphin poisoning, this author experimented with a patient in withdrawal and determined that about half of the morphin introduced hypodermically was eliminated through the stomach and that in withdrawal there was a relative hyperacidity, which, he stated, was responsible for many of the disagreeable symptoms which occur in this state. He further speculates as to the possible reflex origin of other symptoms than those relating to the stomach, having their origin in the stomach nerves which, he states, are subjected to the effect of morphin by reason of the rapid passage of the blood into this organ.
C. Gioffredi-1897-1900.44 45 46
Gioffredi claims that "all will admit that morphin tolerance can be explained in two ways: (1) It is either due to a morphological or simply a functional modification of the nervous system in such a way that it does not react to the drug in the same manner and to the same degree; (2) or that the organism has acquired the power of rendering the poison harmless either by rapid elimination of the drug, destroying it or by acquiring active immunity similar to the case of bacterial toxins."
In 1897 44 he published a report of experiments which he carried on in this connection, in which he states that while it is impossible to obtain an immunity to cocain and atropin, it is possible to obtain with morphin a progressively increasing tolerance to very large doses, approaching a true immunity, if not identical with it. He also states, as a matter of still greater importance, that the serum of morphinized dogs has an antitoxic action of value in poisoning by morphin, sufficient to neutralize the effect of double the minimal fatal dose.
From these experiments he draws the following conclusions:
(1) It is possible to accustom the dog to withstand very high doses of morphin,—much greater than the minimal fatal dose—which closely resembles the artificial immunization to bacterial toxins.
(2) A specific antitoxin is formed in the blood of a dog thus immunized, which is capable of neutralizing the lethal action of a dose of morphin double the minimal fatal dose.
(3) While the antitoxin is being formed in moderate quantities, with increasing tolerance to morphin, the anatomical lesions common in slow poisoning are not entirely avoided.
(4) It is not possible to accustom dogs to cocain and atropin. But, on the other hand, they become more and more sensitive to their action and die before the minimal fatal dose is given.
In 1899 47 following his original experiments on dogs, he continued the study in an attempt to explain the mechanism of this acquired immunity. After securing in a large dog a high degree of tolerance (7.5 g. morphin hydrochloride injected intravenously), he tested the antitoxic action of the serum of this animal in kittens which are more sensitive to morphin than are dogs. He found that a dose two and one-half times the minimal fatal dose could be rendered harmless in kittens.
"But," he asks, "although antimorphin serum has marked antitoxic properties in experimental poisoning, would it also have a prophylactic preventive action like anti-diphtheritic or anti-tetanic serum, etc., in diphtheria and in tetanus?
"This was a question whose importance was at once apparent and that it was necessary to solve; because only in the case of an affirmative answer could we compare immunization against a bacterial poison with immunization against a vegetable alkaloid. As a matter of fact, experiments carried on up to this time might more readily be considered in the light of pharmacologic antagonism between morphin and some substance in the antimorphin serum. If, on the other hand, the serum should confer for some time in kittens a preventive immunity against poisoning by morphin, it would have to be considered as entirely analogous to artificial immunity conferred against bacterial poisons."
As to its preventive action, he concludes from these experiments that when the serum is injected from ten to fifteen hours before the experimental poisoning, it protects kittens from fatal doses and that it appears as if the serum injection acts more efficaciously when given before the administration of the poison than when it is given at the same time. In certain cases the serum was able to neutralize the poison introduced ten days after the injection. He states, however, that the prophylactic effect is of but short duration, as it lasts only for from 10 to 15 days after the injection.
Further in a discussion of Marmé's theories as to the mechanism of tolerance and withdrawal symptoms, Gioffredi concludes on the basis of his experiments that the antitoxic properties of the serum of a morphinized dog are not due to the presence of oxydimorphin.
P. Sollier-1898.48
"The phenomena caused by morphin abstinence in cases of chronic opium intoxication have often been described, but we are yet to learn what they depend upon and through what mechanism morphin is eliminated from the body."
"The only theories which are worth being considered are those which are based on the chemistry of the morphinist.
"There are only two; and it is to be noted, however important this matter is, it has been neglected by most authors. The first originated with Marmé. This author claims that morphin is transformed in the body in contact with the oxygen of the blood into oxide of morphin; that this oxide is toxic and when it is injected into animals there are observed phenomena analogous to those of morphin abstinence. The symptoms noted at the time of withdrawal would, therefore, be due to this liberated oxide of morphin.
"There are two objections to this theory. It has not yet been proved that morphin is always and only changed into oxide of morphin in the body. Some investigators have found it in the form of morphin in the intestines of cases of long standing, which is surprising for so unstable a substance. In the analyses which I have had made by M. Winter of the fluids excreted at the time of withdrawal (bilious stools and vomitus), this view of the elimination of oxide of morphin was not confirmed but, even admitting this alteration in the body, there remains to be discovered why this oxide of morphin, which according to these theories accumulates in the tissues, causes no symptoms until one ceases to introduce morphin. Marmé states in explanation of this that the morphin recently injected neutralizes this oxide of morphin but this is an entirely gratuitous hypothesis. One cannot understand how the stored-up oxide of morphin, continually increasing in amount, can be neutralized by the regular amount of morphin. This explanation does not take into account, the reappearance of withdrawal phenomena in the form of crises, occurring more or less frequently and at intervals after withdrawal. Finally, poisoning by the liberated oxymorphin does not explain how the different symptoms are successively caused during withdrawal, while in experimental poisoning they are generalized and occur in all parts of the body at the same time. This theory, the chemical basis of which is but little substantiated, is therefore, entirely insufficient.
"The second theory, originated by Hitzig, is based on the fact demonstrated by Conrad and Alt that morphin in hypodermic injections quickly reaches the stomach, where it is partly eliminated, but under the influence of morphin saturation the stomach glands cease to function. When withdrawal is begun, their functioning begins again and a very acid gastric juice is secreted. There is a sort of inundation of gastric juice, loaded with hydrochloric acid, and it is, according to Hitzig, this hyperchlorhydria which causes the phenomena of withdrawal. Erlenmeyer, for this reason, advises a new method of treatment, having as its basis, the neutralizing with alkalines of this hyperchlorhydria, after having previously reaccustomed the stomach to withstand hydrochloric acid.
"This theory does rot hold in the presence of the clinical facts. First of all, even if morphin does pass rapidly into the stomach, this does not prove that this is the principal and the quickest means of its elimination.
"Neither is it in the stomach that morphin is stored up, for the most part, as everybody today admits that this occurs principally in the liver and the brain. In what form? This is of little importance for the time being. Besides, it is not surprising, for it is exactly what takes place with most poisons. But even admitting that the stomach glands are saturated to the greatest degree and that under the influence of withdrawal of morphin they throw out large amounts of acid gastric juice, it must be admitted that this is a curious hyperchlorhydria which is accompanied by sneezing, lacrimation, muscular cramps, spermatorrhoea along with bilious vomiting, diarrhoea and profuse sweats, to say nothing of the inequality of the pupils, which is so cômmon, the slowing of the pulse, which is constant, and the tendency to respiratory syncope. This second theory is no more satisfying than the first one.
"Let us see then if clinical observation will not teach us more than these theories which take into account only one more or less well demonstrated fact. Morphin continually used causes, after a while, a more or less marked lessening in the activity of the nervous system and an extremely marked reduction of the glandular secretions.
"Besides, one thing is especially striking: all the immediate phenomena of withdrawal and of demorphinization are characterized by the return of glandular functioning.
"The return of these functions does not take place at once in all of the organs at the same time. And if, at a given time, one observes at the same time symptoms of different kinds, once elimination is in full swing, one notices on the contrary that the different consecutive phenomena of withdrawal occur one after the other. Thus most frequently sweating or sneezing begin the scene along with yawning. Then the diarrhoea begins. At first, ordinary feces, then, very often, pure bile, then semi-bilious yellow diarrhoea. Mucus vomiting (gastric juice), then bilious (when there is any) only occurs when the diarrhoea has begun and stops before the latter does. Then follow the spermatorrhoea, salivation, cramps in the muscles. Each glandular apparatus thus comes into the scene in turn without there being any predetermined order in this succession of phenomena, which vary with each individual and in degree according to the saturation of the different organs with morphin.
"It is impossible to compare the poisoning produced by oxymorphin in healthy subjects with that which takes place, according to Marmé, when oxymorphin is liberated in morphinists, for the organs are not at all comparable in these two cases. The principal thing in the second instance is not the action of the oxymorphin on the organs but rather the elimination of oxymorphin by these organs.
"That oxymorphin causes general phenomena or symptoms in the case of certain organs such as -the heart and respiratory apparatus, where morphin is not stored-up, I will admit. But that it causes the return of organic functioning, I cannot believe, unless this return of functioning is considered only to be due to the elimination of oxymorphin from the body. But the important thing, according to my way of thinking, is precisely this elimination of toxic products stored-up in the glandular apparatuses regardless of the nature of the products. In other words, instead of regarding the phenomena of demorphinization as pathologic and due to the poisoning, I regard them on the contrary as physiologic and due to the elimination of the poison which thus permits the return of glandular functioning. And this is so true that if, at the time of withdrawal, certain glands have not begun again to function, their return is preceded by evidence of localized secretion. The return of glandular functioning is absolutely the chief characteristic of demorphinization.
"Another clinical observation should be made; it is what takes place at the time when an evacuation is about to occur; it matters but little what organ is affected, the intestines, the stomach, salivary glands, etc. The patient is nervous, has a general feeling of discomfort, the heart is slow, the need of morphin or at least of some stimulant is felt. Then, as soon as the evacuation takes place, relief immediately follows.
"But if this premonitory discomfort were only a general discomfort, it might. prove that the body was being poisoned by a new lot of liberated oxymorphin. But this is not the case; the discomfort is above all, local, and the painful sensation experienced by the patient is always of the same nature. It is a feeling of painful tension of engorgement. This engorgement is, besides, perfectly real and is shown in the liver, for example, which increases in volume and becomes painful to the point, often, of true hepatic colic. It is, therefore, the glands which are the seat of these phenomena and when their hyperemia ends, through an evacuation of their contents, the local discomfort and also the general discomfort ceases.
"What takes place in the glands and why do they begin to function again? Is there any need of invoking the toxic action of liberated oxymorphin? None at all. The withdrawal of morphin amply suffices to explain this phenomenon of returned functioning. In fact morphin acts on the glands in two ways,—by paralyzing the nerves which affected them and by saturating their cells, where it remains, probably changed. From the time the morphin injections are stopped what should happen and what in reality does happen? The nerves recover their activity; through other influences the glands begin again to function. But they are no longer in a normal condition. The cells of these glands and their excretory canals are modified, changed and unable after their more or less prolonged inactivity to secrete easily. The products of secretion experience difficulty in traversing the altered endothelium. Hence, the turgescence of the glands and the sensation of painful tension as when there is, for some reason or other, retention in a normal gland.
"But this is not all and the retention is still further increased by the fact that old and altered endothelial cells become detached in the culs-de-sac and obstruct them, and this obstruction is increased by a similar desquamation in the excretory canals which are thus more or less obliterated. This explains why, whenever there is an evacuation, there is immediate relief. This also explains why the heart is overworked and gives way when the effort of elimination occurs in many parts of the body at the same time.
"Hence, the renewed activity of the glandular nerves when the use of morphin is stopped; under this influence, there occurs marked formation of new cells of the glandular endothelium, desquamation of the superficial layers of this endothelium and of that lining the excretory ducts, glandular turgescence, painful production of secretory products, relief caused by the evacuation of these products-such is the group of phenomena which enables us to understand the symptoms of demorphinization.
"Do these successive phases correspond well to what happens and is this endothelial desquamation, which I believe I am the first to mention and to consider a matter of importance in the explanation of these phenomena, a real occurrence? To convince ourselves, we need only observe what takes place in the case of organs accessible to direct observation. From the beginning of withdrawal, the tongue which was clean becomes covered with a yellow white coating. This consists of nothing but dead superficial epithelial cells which become detached after a few days, leaving the papillae exposed; these are sometimes so denuded that they bleed. I have seen more than once in morphinists of long standing a furfuraceous or even scarlatinal desquamation when there have been profuse sweats, that is to say, when the sudorific glands have been much affected. There can also be observed, as I have done several times, similar phenomena of desquamation in the deeper organs such as the intestines giving rise to a pseudo-membranous enteritis. It is logical to suppose that the same thing happens in the whole glandular apparatus when the nature of the subjective and objective phenomena of one kind or another is seen.
"There is, therefore, no need of calling into play a special poisoning either by oxymorphin or by hydrochloric acid to explain the painful phenomena of morphin withdrawal and the different somatic symptoms that it prevents.
Suppose for a moment that what happens in mumps, for example, happened in all of the glands of the body at the same time or consecutively but quickly, and we would have the picture of morphin withdrawal. It all resolves itself into a physiologic mechanism corresponding to the anatomic changes in the tissues saturated with the morphin.
"But the interest in this point of view does not alone consist in supplying a simpler and more plausible theory for these phenomena. It allows us to explain easily the occurrences noted during demorphinization, such as the eliminatory crises, the advantage of rapid withdrawal, the uselessness and the danger of so-called sedatives or so-called substitutes, the gravity of relapse during a convalescence from a rapid cure; it allows us finally to establish the basis of a rational and truly pathogenic treatment for morphinism."
* * * *
"Eliminatory Crises.—At the time of withdrawal, all the glands are the seat of a more or less abundant hypersecretion lasting for two or three days; then little by little this state subsides, when suddenly a state of discomfort, analogous to that of withdrawal but much less severe, occurs, which is accompanied by a new hypersecretion of one or more glands which brings relief. This crisis lasts twenty-four to forty-eight hours and following it, convalescence progresses more rapidly, organic activity is greater and certain apparatuses, which until then had been functionally inactive, take on again very active functioning.
"These crises may thus occur several times at very irregular intervals and in lessening degree during convalescence.
"Chemical theories are unable to explain this intermittence. Nor may poisoning by oxymorphin or the hyperchlorhydria at the time of withdrawal explain how, when withdrawal has been accomplished, phenomena analogous to those which accompany withdrawal again occur. Admitting, on the other hand, the mechanism which I have set forth, these things are easily explained and become a part of the general pathology. It amounts, as I have said, to a true epithelial and endothelial desquamation of the mucous membranes saturated with morphin, whose glands have ceased to function under this influence. At the time of withdrawal, a violent organic reaction, which causes the reawakening of glandular activity, leads to the elimination of the greater part of the cells which have been affected by the poison. But the underlying layers are not yet grown. They suffice for a certain period for the glandular functioning, but with the active growth of the deeper layers, the second layer of cells are, in their turn, thrown off whence is produced an eliminatory crisis analogous to that of withdrawal. The same phenomena thus occur several times just as happens in the skin affected by an infectious disease, as an eruptive fever. After the throwing off of the first epidermic layers, there is a throwing off of the underlying layers from time to time, until the skin has been completely renewed in its elements. Similarly, in demorphinization, this phenomenon takes place not only in the skin but in all the organs and principally in the glands; the stomach, intestines, liver, skin, etc. The eliminatory crises are nothing but consecutive desquamations of the glandular organs.
"It is interesting to see during how long a period these crises occur, for their termination corresponds to the return of the organs ad integrum. For from six weeks to two months after withdrawal they may occur and sometimes even longer. Hence, the necessity of keeping morphinists under treatment for at least six weeks, or risk exposing them to relapses. In truth, among the symptoms which occur with the appearance of these crises is seen the desire for morphin and it is easily seen how dangerous it is to leave a morphinist to himself, while he is subject to affections which are able to reawaken his desire for the drug."
E. S. Faust-1900.49
Faust believes there are two possibilities as to the way in which tolerance may be induced.
(1) By dulling the nervous system against the effect of the drug so that a given amount is no longer able to produce the same degree of reaction.
(2) By the creation in the body of an ability to make the morphin ineffectual either through transmission or destruction.
He endeavored therefore to find out which of the above was responsible for the acquired tolerance, by observing, in the case of dogs, how much of the consumed morphin was again excreted from the body.
On the basis of his experiments Faust reaches the following conclusions:
"Under normal conditions a portion of the injected morphin is destroyed in the body of the dog. From the feces the only excreta to be considered in relation to unchanged morphin, I could recover in acute poisoning only about 70 per cent. of the amount injected.
"On repeated injections the ability of the organism to destroy the morphin normally increased up to a certain degree. On further gradual increase of the dosage over a longer period of time, finally the point is reached where the whole amount of injected morphin is destroyed.
"However this ability to destroy the morphin is not unlimited.
"In those animals which were given gradually increasing doses daily, the action was the same as the above after larger doses.
"However, death followed the too rapid increase in the dosage, as in the case of morphinists and opiophagists under similar circumstances as long as the poison is not destroyed, its characteristic action develops.
"From these facts I have concluded that in so-called morphin-tolerance it is not a tolerance of the cells or a dulling of the cell toward the action of the morphin, but an increasing ability on the part of the organism to destroy the morphin.
"This conclusion is supported by the results of my oxalic acid experiments. "Here we are concerned with a substance which under ordinary circumstances does not undergo destruction in the body. It was shown that even on the administration over a long period of time of gradually increasing doses no destruction of the oxalic acid took place. After 26 days-92-95 per cent. of the injected oxalic acid was recovered in the urine. Therefore the organism gave rise to no destruction. It was not able to create new factors under whose influence a destruction of the poison could have taken place."
L. Hirschlaff-1902-1903.5° 51 52
Hirschlaff, in an article reporting experiments on animals aiming toward the production of an antitoxic serum analogous to the diphtheria and tetanus antitoxins for combatting morphin poisoning, rehearses how little work is available bearing on the production of immune serum in the case of simple plant poisons, especially those which have been defined chemically, stating that what is known about them is essentially of a negative character. He states that from the very accurate findings of Faust, with whose work he did not become familiar until after the completion of his own investigations, "it is more probable that the belief of the Ehrlich school in opposition to the antitoxin formation•for alkaloids is incorrect at least respecting morphin."
Hirschlaff reports that he tested the protective action of the serum of morphinized rabbits first on a series of normal rabbits and later on a series of normal mice. Although the experiments with the normal rabbits appeared to be encouraging, he changed to mice for the reason that he found that his minimal lethal dose was too low in the case of the rabbits. From these experiments he concludes 53 that
" ... with long treatment of animals with increasing doses of morphin, protective substances are formed in the blood which are able to protect other animals from acute poisoning with a positively fatal dose of morphin or a multiple of the same, exactly analogous to the antitoxic sera which have been made against bacterial toxins."
Here Hirschlaff speculates as to the possibility of Ehrlich's side-chain theory offering an explanation of the mechanism of the phenomenon. In a later, undated monograph 5f printed subsequently to a criticism of his theories by Morgenroth, in which he reports further experiments, Hirschlaff states:
"On the basis of the results of these experiments, I thought I was justified in accepting the hypothesis that the basis for morphin tolerance in chronic morphinism must be found in a phenomenon analogous to that generally accepted today, in the immunity against infectious diseases according to Ehrlich's investigations. Therefore, I was led to the following consideration: If we accept the hypothesis that acute morphin poisoning takes place analogously to bacterial intoxication, that the haptophore group of the morphin molecule attaches itself to the side-chain of the body cells; if further, it is agreed, that in the case of chronic morphin tolerance, the receptors produced in excess by the body cells are thrown off and are then caught and broken up, as it were, in the blood and haptines freely surround the morphin, which is constantly being replaced, so that the toxophore group of the morphin molecule cannot now possibly get near the nerve cells, then the following theory concerning withdrawal symptoms, for the occurrence of which we have not yet been able to account theoretically, is explained by these hypotheses which are completely corroborated by facts. It can easily be demonstrated that new receptors are formed in the first stage of chronic morphin tolerance so that the organism can break up the morphin as it appears before it can reach the nerve cells. But the longer the abuse of morphin continues, the more this ability to produce side-chains is exhausted; therefore, disagreeable secondary reactions appear, because all of the morphin can no longer be made harmless and there is a continuous enhancement of the attraction, i.e., of the morphin necessary to produce a sufficient amount of side-chains. If treatment of morphinism is attempted in an organism in which the production of protective substances is lessened because the necessary attraction is lacking, then symptoms of poisoning must appear, since the whole amount of morphin, even though reduced, can no longer be bound by circulating receptors; and these withdrawal symptoms can be paralyzed only by either setting in motion the whip, which has heretofore caused the production of side-chains, viz.:—supplying quantities of morphin, or joining to the organisms the protective substances which are obtained from the foreign blood of animals, which were still producing side-chains at the time the serum was withdrawn."
As a further study of the protective action of the serum of morphinized animals, Hirschlaff reports that he carried on another group of experiments with about 150 rabbits and 400 mice.
The following table gives the results in percentages of Hirsehlaff's experiments with the four groups of mice:
From this table, the author states:
TABLE VII
| Groups |
% of total living |
No dead |
% under morphin living |
0.0012 g. incl. dead |
% over morphin living |
0.012 g. excl. dead |
| Morphin Mice | 16.7 | 83.3 | 27.8 | 72.2 | 15 | 87 |
| Normal Serum-Mice | 30.3 | 69.7 | 50 | 50 | 15.8 | 84.2 |
| Goat-Immune Serum-Mice | 26.9 | 73.1 | 41.7 | 58.3 | 18.6 | 81.4 |
| Rabbit-Immune Serum-Mice | 45.1 | 54.9 | 65.5 | 34.5 | 31 | 69 |
"It can be seen that the morphin sensitized serum exercises a weak but distinctly positive action against acute morphin poisoning of the mice, provided that the dose of morphin is not too large, i.e., that it lies between the M.L.D. and the dose certe efficax. The relatively high figures with which the normal serum mice in Table II (see above table) are concerned, are, as above noted, plausible and, for the greater part, to be accounted for by the fact that the number of these tests equals only about half of those of the other series."
"According to the way that I have supplemented and modified the results of my first experiments, I should like to raise the question as to whether the protective power of the morphin protective serum, which has been demonstrated experimentally to be positive, but always relatively slight, could not perhaps more readily be explained on a theoretical basis. In this connection, I should like the following to be considered:
"1. The chemically defined poison used, in this instance, to produce the protective bodies differs from the bacterial toxins in that, once introduced into the animal body, it does not multiply or increase in toxicity, so that the formation of the protective substance is limited by the impossibility to introduce more than, at the most, twice the absolute fatal dose, on the gradual increase of the poisoning in the animal. In the case of bacterial toxins where 100,000 times the absolute fatal dose can easily be introduced into the animal by gradual tolerance or immunization, for that reason, the protection obtained must be a correspondingly higher one.
"2. If the theory described above of the withdrawal symptoms on the basis of immunity is right—and it stands and falls naturally, with the proof of the protective action of the morphin serum—then the formation of protective bodies in the animals treated with increasing doses of morphin is dependent on their chemical behavior. In man, as you well know, %-1 year goes by before the characteristic symptoms in chronic opium abuse appear as signs for the cessation of the formation of protective substances; the older the individual, the weaker the constitution, the more quickly the symptoms of opiumism or withdrawal appear. Somewhat similiar conditions obtain in animals. The formation of protective bodies can flourish in animals only when the state of health of the animal is good and as long as disagreeable secondary symptoms of morphinism are not observed. I am inclined to believe that the relatively unfavorable results of the goat protective-serum experiments can be traced back, for instance, to this point, since both of the goats used at the time the serum was taken were in a very bad condition clinically... .
"3. The protective action, which is attributed to the morphin immune serum in acute morphin poisoning is considerably greater than in analogous immunity tests with bacterial toxins. While the bacterial toxin in the animal requires a certain incubation period to be effective, the organism in the case of acute morphin poisoning, within a few minutes, is overtaken by the whole amount of poison introduced; and it is decided within a half-hour, as an average, whether or not the protective bodies, present or set up, will be able to withstand the onset of the morphin haptophore group. In the gradual process of bacterial intoxication, usually extending over hours and days, the reaction of the organism in regard to the struggle of the protective bodies against the toxin group is far less. For this reason the clinical use of the morphin immune serum is of value in chronic morphin poisoning or in the treatment of morphin withdrawal, but not in acute intoxication. If, therefore, the usefulness of the morphin immune serum against acute morphin poisoning proved to be very slight on further tests, still the field of chronic morphin poisoning or treatment of morphin withdrawal presents much more favorable opportunities for the use of morphin immune serum, since, in this case, the secretion of the poison in the body or the approach of the haptophore group of the poison toward the body cell, as the clinical symptoms show, takes place slowly, by degrees, and within the time period, obviously, always in small amounts.
"If we have felt that we had to confine, in this way, the action of the morphin immune serum to a theoretical basis, I should like to refer once again to the positive side of the matter by the following reflection which, in my opinion, admits of explanation only in the theory of the formation of protective bodies in chronic morphin intoxication. It has been shown with certainty by Faust, Marquis, etc., and finally by Totze in a very careful piece of work ... that in acute morphin poisoning the greatest part of the morphin introduced in the body could be detected in the body organs or their secretions. On the other hand, in chronic morphin poisoning only a very small, insignificant part of the morphin is recovered in the body or its secretions, yet the amounts introduced are very much larger than in acute morphin poisoning. There must take place, accordingly, a destruction of the morphin in the body in chronic morphin intoxication, since a change of the morphin in the body cannot be substantiated at all or at most only in very small amounts. On the other hand, Antenruth has shown that in corpses the morphin in acute poisoning can be detected unchanged in large amounts, even after three years. In other words, the destruction of the morphin takes place only in living and not in dead animals. Therefore, we must assume that it is the living molecule of albumen which, In the sense of Ehrlich's immunity, causes the destruction of the morphin. Perhaps this supposition is still more plausible when we consider that morphin is traced back in its formation, undoubtedly, to the molecule of albumen, i.e., plants."
"In conclusion, I do not wish to omit reference to the fact that the morphin immune serum has already been used clinically in a series of human cases. Next to the experiments, which several other authors have made with the preparation made by the firm of J. D. Riedel under the name of "Eumorphol" and on which a report has not yet been made, besides the tests on insane already published, I myself have had an opportunity to treat. a small number of pure morphinists and without exception, cured them by means of the morphin immune serum. A detailed clinical report of the first four cases observed by me has just appeared in the Zeitseln•ift fur Krankenpflege. As a resume of that, I may state that. (1) Every case, without exception, was completely cured; (2) no harmful secondary reactions at, all appeared on the use of the immune serum; (3) in all cases an alleviation of the discomfort of the patient as well as an easier course of withdrawal could be noted. The results of these clinical experiments may, therefore, be considered positive."
Mavroj annis-1902 as
"At the suggestion of Prof. Kalikounis we carried on a series of experiments on rabbits for the purpose of demonstrating that tolerance to morphin was due to production on the part of the organism of substances which exercise an antagonistic action toward that alkaloid. We tried to morphinize the animals in such a way that they could tolerate doses larger than the fatal dose; then we endeavored to find out if their serum had antitoxic properties.
"With the negative results obtained by different workers who had studied the question of tolerance to other alkaloids than morphin and especially those of Chavigny who had experimented with morphin, it was seen that in any case the antitoxic properties of the serum of morphinized animals would be quite weak. It was therefore necessary carefully to find out the minimal fatal dose of morphin hydrochlorate for the rabbits."
* *
"We further observed that the aqueous extract of the brain of morphinized animals, introduced the day before through the alimentary tract was capable of protecting the animals against the absolutely fatal dose, when the brain extract of fresh animals had no effect on the same dose of the alkaloid.
"Thus our experiments show that the serum and the brain extract of morphinized animals possess weak, but real antitoxic properties toward morphin. These properties are transitory and not very lasting, as the animals which received the anti-morphia serum ten days previously could not resist the fatal dose."
J. Morgenroth-19035°
"Contributions on the discovery of new antitoxic sera, the action of which is directed against poisons of known chemical composition, are accorded careful scrutiny by all who have worked in this field and have followed the work of late years. In most cases such experiments fail from the first because of the absence of a tolerance (Gewohnung) to the poison and of the resulting impossibility of a systematic immunization. Further, the positive results so far obtained in this direction have not proved valid—Bashford has shown that a specific immunity against solanin, such as Pohl thought he had established, does not exist and Bashford and Besredka were just as unsuccessful in producing specific antibodies against Saponin. The work of Toulouse and d'Evelyn, who endeavored to produce an anti-alcohol serum through immunization, still remains a scientific curiosity, proof for which has not yet been established. Therefore, to describe accurately the present status of the question, it must be stated that an antitoxin has not yet been obtained by immunization, with poisons of known chemical composition. Ehrlich's side-chain theory is applicable here insofar as it recognizes, for the present, a fundamental and characteristic difference of the true toxins from the alkaloids; toxic glycosides, and toxic inorganic compounds and seeks to find an explanation for this difference in the peculiarity, thoroughly established by experiment, in the manner in which both classes of substances are distributed and attached. A sharp separation of the material into two groups, as Graham has done for the crystaloids and colloids, will in no way establish it and, as today these two classes of substances seem connected, we can also take into account the possibility that the sharp limits between the two classes can be one day wiped out. The theory that one or another alkaloid has possibly a group which can be attached by suitable receptors of the cell is, in itself, harmless.
"Morphin was most suitable for the immunization tests, on account of the known intoxication symptoms and it was fortunate that Hirschlaff recently made immunization against morphin the subject of a thorough study and thus sought to supplement the valuable work of Faust who would not consider the possibility of the formation of an antitoxin."
The author does not agree with Hirschlaff as to the dose certe efjtcax stating that 0.01 g. morph. hydroch. "far from kills every mouse" and upon experimentation decides that this dose should be 0.014 g. for a 15 g. mouse. Furthermore, in order to eliminate the possibility of any protective action residing in normal rabbit serum, when injected into mice in quantities equalling 1/30 to 1/l6 of the body weight of the animal, he runs controls, treated with normal rabbit serum, and thinks that he observes a condition which Hirschlaff considers as a true effect of his antitoxic serum. He concludes, therefore, that the dose certe efficax should be at least 0.0165 in order to preclude any protective action from the rabbit serum.
He then proceeds to the tests of the serum of immunized animals on the mice, according to Hirschlaff's method and concludes as follows:
"We can sum up the results of our experiments by stating that, apparently, the positive result of Hirschlaff's experiments is only accidental, in raising the resistance by the injection of serum, which accounts for the fact that the doses used by him are generally not absolutely fatal. Whether in morphin tolerance it is a question of the formation of an antitoxin or only the destruction of the poison, possibly by oxidation as Faust maintains on the basis of his interesting experiments, has so far not been decided, and the decision must be reserved for further experiments which will not be. long awaited."
In his undated monograph previously referred to 57 Hirschlaff discusses Morgenroth's criticism of his work as follows:
"If I compare the results of my present experiments carried on in the chemical factory of J. D. Riedel, which covered approximately 150 rabbits and 400 mice and which I can here only briefly summarize, since a detailed publication containing the protocol will follow, with those of Morgenroth, I must, of course, admit that in my first figures chance did play a considerable role; but, on the other hand, I am inclined to point out that also Morgenroth's figures were influenced by chance, and this unfavorably. Further experiment on the animals has shown unequivocally that the true results of these observations are not so favorable as the first series seemed to indicate, but that, after all, they give positive results in spite of Morgenroth's negative figures. And further it is shown that Morgenroth's results are influenced by the facts; 1—that the number of rabbits sensitized as well as the number of control mice tested with the sensitized serum are too small, and, 2—that the doses of 0.012-0.018-0.024 g. morphin per 15 g. mouse used for the tests are too far apart to throw into bold relief all phases of the protective action of the serum to be tested."
M. Cloetta-1903.58
Cloetta does not accept the theory of antibody-formation similar to that in bacterial infections as the basis of the mechanism of tolerance nor does he agree with Faust that the destruction of morphin in the body offers the explanation. Working with rats and pigeons he endeavored to learn whether the capacity for increased destruction grew proportionately to tolerance. Although he found it possible to produce tolerance, he observed no increased power of destruction of morphin and therefore deduced that the "nature of the tolerance is not in intimate and causative relationship to the ability to destroy morphin."
Cloetta gives the following as possible bases upon which to explain the mechanism of tolerance:
1. Leukocytosis.
2. Decrease in ability of brain cells to combine.
3. Peculiar cell immunity in which the protoplasm under the effect of the poison no longer reacts with a functional disturbance in consequence of a tolerance for the stimulus.
The author studied each possibility by experimental investigation.
After examining the first, possibility, namely, leukocytosis, he found that in normal animals the injection of morphin caused a reduction of the leukocytes and this reduction was generally in proportion to the intensity of the poisoning—but in immunized animals there was no essential change in the behavior of the leukocytes. He further found that no destruction of the morphin occurred through the leukocytes and that, therefore, tolerance was not dependent on these conditions,
The author then takes up the second possibility as an explanation of the mechanism for tolerance, stating:
"Is the tolerance due to the death of the receptors, that is, do the brain lipoids gradually lose the ability to combine the morphin and thus cause the influence of the poison to be diminished? I attempted to test this possibility by mixing the brain of an immunized animal with morphin and then centrifuging it out again with the addition of a solution of NaCl."
While the results of this experiment were positive in a certain sense, Cloetta accounts for this fact to his own satisfaction and turns to the last possibility as one offering the most promise. The following is his summing up:
"From my observati,nis it seemed to me a question of a gradual accustoming of the protoplasm to the influence of the poison in the case of chronic morphin poisoning. No protective action was indicated in the body of chronically poisoned animals. This tolerance of the cells, among which the cells of the brain occupy first place on account of their particularly strong ability to absorb morphin, seems to be quickly acquired, but is also quickly lost again, as happened in the case of the experiments on immunized pigeons and rats, when only an interval of two days (without the supply of the poison) was sufficient to make the brain cells again considerably more sensitive to the effect of the poison. Now, since the brain is normally able to combine morphin, it may also be assumed that, with this cell tolerance, the ability to combine increases sooner. The morphin has ceased to be a foreign constituent part of the brain lipoids. They take it up at an increased rate and this increased ability of the brain to combine with the morphin is also the reason for the increased destruction of the same. This is not a cause of immunity, but an accompanying phenomenon of the same, occasioned by the peculiar tolerance of the protoplasm. Therefore, this should not he spoken of as occurring through the death of the receptors, but rather through an increase and simultaneous decline of the susceptibility of cells for the toxophore group of morphin."
G. Argentina-1905.59
The object of this author's experiments was the verification of the results of Mavrojannis described above in order to compare the latter's method of immunization with that of Gioffredi. He morphinized two rabbits, one according to Gioffredi's method and one according to that of Mavrojannis, and then tested the protective action of the serum and of the brain extract of these rabbits each on a series of four normal rabbits. The rabbit immunized according to Gioffredi's method, weighing 1650 g., was started on a very small dose of morphin and increased gradually over a period of about two months until it was able to tolerate 80 cg. The rabbit immunized according to Mavrojannis's method, weighing 1220 g., received first a venesection and was started immediately on 30 cg. and rapidly increased until at the end of about a month it was able to tolerate 70 cg.
From the results of his experiments Argentina concludes:
1. "That Mavrojannis's method should not be preferred, because best results are obtained with the slow and gradual morphinization of the animals. The serum prepared from these animals is found to be much more active than that prepared from animals made tolerant to very high doses within a short time.
2. "That the brain extract of morphinized animals is capable of neutralizing the minimal fatal dose of morphin. However, it is always less active than the serum and it is also necessary to use a larger amount in order to derive the protective effects of the serum. But I had occasion to note that if the doses of the extract are greatly increased, fatal results will follow. This may not easily be explained. It can only be stated that this result is caused by the tissue of the nervous system."
D. Mirto-1905.6°
A different approach to the subject of tolerance on the basis of antibody-formation as in the case of bacterial poisons is made by Mirto, who is rather doubtful as to the significance of the positive results of his investigations as to the sero-precipitation .reaction in chronic morphin intoxication and the latter's value as a means of detecting morphin.
In a series of controls the author found that there were sufficient electrolytes in 1 cc. of a 1% solution of morphin hydrochloride to keep the globulins of 2 drops of normal rabbit serum in solution but insufficient to keep a larger quantity of globulin in solution. In regard to the serum of morphinized rabbits he found that no precipitate was formed until the rabbits were given from 25 to 35 cg. morphin hydrochloride per day. Beyond this daily dose, when 2 drops of the morphinized rabbit serum was added to a one per cent solution of morphin hydrochloride, the solution often becomes opalescent almost instantaneously.
"After being from 20 to 30 minutes in the thermostat at 37 degrees, it became turbid. In a second phase, the formation of a finely granular precipitate was observed after 30-45 minutes at 37 degrees. After 45-60 minutes and at the most one hour and a half, it changed into a white flaky precipitate. Thus we observed the characteristic phases of sero-precipitation reactions. In general the reaction took place more rapidly and distinctly with the serum of rabbits which had received a greater amount of morphin hydrochloride. The normal rabbit serum, fresh and yellow-lemon colored, did not show, under the same conditions, any sign of turbidity or precipitation and remained clear for many hours in the stove at 37 degrees. It became turbid only after 12-24 hours.
"The above phenomena were observed in a one per cent solution of morphin hydrochloride in distilled water but did not occur in an analogous solution of morphin hydrochloride in 0.85% sodium chloride solution, even when larger quantities of morphinized rabbit serum were added."
"The sera of morphinized animals soon lost, after a day or so, their precipitating properities."
Repeating the experiment with codein and meconin he concluded that neither codein nor meconin became, under the same conditions as morphin hydrochloride, turbid or gave any signs of precipitation.
"All this, therefore, helped to show that, in chronic morphin poisoning, specific anti-bodies could be formed in the body which when coming in contact with the body generating them, (morphin hydrochloride) caused specific precipitation phenomena similar to what happens in the case of bacterial toxins. Therefore it was possible to conclude that the biological actions of the morphin and bacterial toxins were ;.dentical."
However, the author calls attention to an observation which he made by chance during his researches and which would give to his conclusions a different significance.
"In a robust normal rabbit which had been subjected to repeated and rather abundant bleedings, in the course of these experiments, we have noted, at a certain point, that even when one or two drops of its serum are added to one cubic centimeter of 1% morphin hydrochloride solution precipitation phenomena, as in the serum of morphinized rabbits, occur.
"The conclusion has been confirmed by experiments made on other rabbits. What explanation can we give for this new result? We said above that often there is no sharp distinction between a specific and a non-specific precipitation of protein, and that the difference is often due to the degree of concentration, temperature, and time at which precipitation occurs. Now in our case, while one cubic centimeter of a 1% morphin hydrochloride solution is sufficient to keep the globulins of two drops of normal rabbit serum in solution, it is not sufficient to keep in solution the globulins of the serum of rabbits subjected to repeated bleedings. This fact indicates that in the latter case the protein quotient of the serum, that is the ratio between the sero-globulin and the sero-albumin, has suffered a notable change.
"In other words, the globulins of the serum are increased, (in the same manner as has been observed by other authors in various other conditions such as fasting, etc.) in such a way that their precipitation occurs more rapidly. This can be considered identical to the precipitation which is observed by adding more than two drops of normal rabbit serum to one cubic centimeter of a 1% morphin hydrochloride solution.
"Now then, on the basis of these new facts what can we conclude from the preceding researches in which we observed the appearance of a sero-precipitation reaction, after a prolonged and increasing administration of morphin hydrochloride? What significance and what value can we attribute to the latter? We believe that the answer to this question is easy. In morphin habituation, an increase of globulins of the serum, occurs in the same manner as in other conditions, such as fasting, bleeding, etc. The sero-precipitation reaction which is observed is due entirely to this increase. This reaction has not, therefore, the meaning which was given above, i.e., the formation of a special antibody which, in the presence of the substance generating it, gives rise to precipitation phenomena; it is not specific since it will occur in conditions other than morphin habituation. Therefore, it cannot be used in the detection of morphin.
"If these researches lose much of their practical interest as a result of these conclusions, it seems to us that they open an unexplored path to the study of the physico-chemical relations which can be established between alkaloids, their salts, and the protein substances."
"The study of these problems is therefore of great interest and promises fruitful results, which, above all, may give a rational explanation of the selective action of the alkaloids for some special organs or tissues of our organism."
G. Marikovsky-1906.81
Because of the lack of agreement among investigators, Marikovsky undertook a series of experiments to study the protective action of the serum of morphinized rabbits and dogs on normal animals.
The author developed a new method by which he immunized a series of rabbits against morphin and which consisted in mixing with a fatal dose of morphin progressively decreasing amounts of potassium permanganate solution administered every three days. He also immunized a series of dogs using only the old method. From testing out the serum of these animals on guinea pigs, he concludes as follows:
"(1) The absolutely fatal dose of morphin for the mouse is greater than that established by Morgenroth and Hirschlaff.
"(2) Guinea-pigs lend themselves better than mice to the determination of the value of anti-morphin serum. Over 7 cg. morphin kills 100 g. guinea-pig.
"(3) If rabbits are simply treated with continuously increasing doses of morphin, this procedure is much longer and doubtful in results. Much better results can be obtained, in a much shorter time, by my modified procedure.
"(4) The life of the guinea-pigs poisoned with the absolutely fatal dose of the poison can be prolonged with the serum of the rabbits treated by the modified method, and they can be preserved even if the dose is not very much in excess of the absolutely fatal dose and the serum is administered immediately after the poison.
"(5) Moreover, the life of the animals poisoned with the absolutely fatal dose can be prolonged with the serum of a dog immunized up to a certain point."
Marikovsky was so encouraged by these results that he immunized 102 rabbits whose serum he administered to 2 morphinized dogs, rapidly withdrawing the morphin and substituting the serum.
The author states that during the administration of the morphin the dogs were uncomfortable, timid, and of a neglected appearance. However, after a few days of treatment with serum the dogs became brighter, more responsive and their coats took on again their usual gloss. It was especially noted that the second dog took on weight very rapidly. Later both of these dogs were used for other experiments.
Because of these good results in the dogs, the author desired to study the effect of the serum on human beings, i.e., morphinists; however, it was practical at that time for him to secure only two suitable cases and in both of these the tests had to be discontinued on account of disagreeable secondary symptoms.
The author concludes as follows:
"I do not maintain that I have accomplished very much, perhaps. But this much has been accomplished, that my investigations, perhaps in some measure, will contribute to shake the strong faith in Ehrlich's hypothesis—which moreover, is also attacked from other sides...."
W. Rubsamen-1908.°2
Referring to the work of Faust, Rubsamen questions whether the increasing ability to destroy morphin is the only cause of the increasing tolerance. He continues:
"The phenomenon of chronic morphin intoxication in man shows us that, on the subcutaneous injection of the poison, therefore on very active resorption and rapid access of the morphin to the central nervous system, the morphinist reacts to a dose which would be very large,—fatal to an intolerant person. Therefore, in order to explain tolerance toward the amount of poison circulating in the first quarter of an hour by an increased ability to destroy it, we must assume that the removal of the poison takes place very rapidly. So far, we have no basis on which to work for a consideration of these relationships; this can be accomplished only by a series of experiments on small animals, in which it is possible to use the animals in toto at different times after injections and to determine the total amount of the poison present at the given periods... . If we knew the speed with which morphin is destroyed in morphin tolerant animals, we could form an opinion as to how far into consideration as the basis for the chronic intoxication by morphin we could take, besides the increased ability to destroy the morphin, the susceptibility of the cells to the poison."
The author used white rats in his experiment, developing his own method for the determination of the amount of morphin present at a given time after injections. After determining that 60 mg. of pure morphin was absolutely fatal for an intolerant animal, he immunized a series of rats which were then killed and tested for morphin content.
The author then carried on a series of experiments to compare the conduct of the morphin in the organism of immunized animals with its behavior in intolerant animals. He concludes that immunized rats can destroy morphin more quickly than normal rats.
Rubsamen finally concludes that
".... at the time when the strongest symptoms of poisoning would be expected to appear in an intolerant animal, there is still enough morphin in the whole organism of an immunized rat to poison normal animals. Chronic morphin intoxication therefore seems to have two causes: first, on continued administration, the ability to destroy morphin increases as Faust has shown in dogs and I have corroborated in rats. Thereby the poison dose is partly diminished within the first hour, which could be effective for tolerant animals. But, in the first hour after injection, there still circulates such a great amount of poison without symptoms of poisoning that as a second cause of the insensibility of tolerant animals, we must accept a cellular immunity. On what this depends we cannot at present state."
C. Ferrai-1909.63
In connection with an investigation 84 as to the production of antibodies in chronic morphin intoxication, Ferrai observed a phenomenon which he considered significant and from which he concluded that under certain conditions, unlike the salts of other alkaloids (strychnin, cocain, codein) morphin salts exerted an anticomplementary action.
In a test involving complement fixation Ferrai noted that, while there was no hemolysis in the tubes in which the serum of a morphinized rabbit came in contact with a solution of morphin hydrochloride in the presence of fresh complement. and later sensitized sheep's cells, the same phenomenon took place, although to a less degree, in the control tubes containing normal rabbit serum and in those containing normal dog serum. On the other hand, there was complete hemolysis in the other control tubes containing the immune rabbit serum but no morphin and incomplete hemolysis in the tubes containing morphin but no rabbit serum. By varying the concentration of the morphin solution and the volume of the immune serum, Ferrai determined that the intensity of the phenomenon, at least within certain limits, was proportionate to the concentration of the morphin solution and the volume of the serum.
From his experiments, Ferrai concludes:
"1. Under special experimental conditions, morphin salts prevent the production of hemolysis in the hemolytic system,—guinea pig complement plus amboceptor from a rabbit immunized to sheep's blood plus sheep's cells.
"2. The nature of the phenomenon is anticomplementary; morphin has no action on the hemolytic amboceptor.
"3. The inactivation of the complement by the morphin takes place also at zero degrees.
"4. This anticomplementary activity common to the various morphin salts (hydrochloride sulphate, acetate) is not possessed by the salts of other alkaloids (strychnin, cocain, codein)."
M. Albanese-1910.86
Agreeing with Faust that in morphinism the morphin is completely transformed in the body, Albanese proceeded to investigate the seat of the transformation. The organ he selected for examination was the liver. He reports as follows:
"After killing a dog, which through daily increasing injections of morphin hydrochloride had become able to stand, without apparent effect, doses of more than one gram a day, the liver was removed. The liver was chopped up and reduced to a pulp and to it was added about one-half its volume of a physiologic sodium chloride solution and a few crystals of thymol (or better, if possible, a little silver fluoride), then there was added to this mixture 0.20 g. of morphin hydrochloride (to 100 g. of liver), and it was placed in an incubator at 38 degrees and stirred frequently. After seven or eight hours, by treating the mixture by a proper method of extraction, it was easy to recover from 0.16 g. to 0.17 g. of pure crystalized morphin, corresponding to almost the whole of the morphin given, except for the small unavoidable losses.
"It might, therefore, at first appear that the liver in tolerant animals, which is entirely unable to change even small doses of morphin mixed with it, in vitro, has nothing to do in vivo, either, with the destruction or transformation undergone by the morphin in the body. But if one stops a moment to think about the fact of which I have already spoken that the liver of morphinized dogs had even less effect on added morphin than that of normal animals, and if one believes the observations of Faust, that that amount of morphin which the bodies of tolerant individuals is capable of changing is not unlimited but proportionate to the maximal dose to which the animal has become tolerant (so that when a dose of morphin which noticeably exceeds the preceding dose is given to a tolerant dog, the surplus not only causes characteristic toxic symptoms but appears unchanged in products of elimination), the apparent contradiction which seems to exist from the recorded facts is very well explained and brings us to a new line of thought. One is, in fact, obliged to say that, even admitting that the liver is really able to acquire the ability to alter injected morphin (or at least to assist in its alteration) during the period of morphinization,—as long as the injections are continued,—this ability will be entirely used up,—saturated as it were,—in transforming the morphin circulating in the blood; so that there will not remain any of this ability available for the extra quantities which are artificially added in vitro. Thus it is easily explained how this organ during the period of the injections is not even able to alter small quantities of the poison which normally the liver does alter. From this arose the idea of investigating how the liver would behave, not during the period of morphinization, but rather after the stoppage of the injections, during the period of abstinence, that is to say when it would be supposed that the ability acquired through habituation, still persisting, was not used up or masked by the daily quantities of the poison administered.
"As a matter of fact, the result of the experiment at this time confirms the a priori reasoning.
"If, instead of using the pulp of a liver from a morphin tolerant dog killed while he still was receiving the poison daily, the liver of a dog was secured during the abstinence period, that is to say, from 48 to 60 hours after the last dose of from 1 to 1' g. of morphin hydrochloride had been given, and if after adding to it as before 0.20 g. of morphin hydrochloride (for 100 g. of liver), the mixture is treated for the extraction of morphin, there is crystallized out but a very small quantity of the alkaloid, rarely exceeding 0.02 g. to 0.03 g.
"Hence, it is indisputably shown, according to what I have just pointed out, that, in the transformation which morphin undergoes in the organism of tolerant animals, the liver plays an important rôle.
"Naturally it would not be proper to conclude that this organ is the exclusive seat of the phenomenon; and it is necessary carefully to compare the activity of the liver with that of other organs and tissues."
G. E. Pettey-1910.86
From clinical observations, Pettey. concludes, as an explanation of the mechanism of the withdrawal phenomena, that all of the dangerous and most of the painful symptoms incident to withdrawal are due to retained excrementitious matter and the extremely toxic condition resulting therefrom. He states that if the system could be freed from this material the opiate could be withdrawn without shock, collapse, heart failure, diarrhoea, or other dangerous symptoms and that the suffering would subside in a few days' time and could be controlled by some member of the belladonna group.
G. C. Berri and C. R. Belgrano-1911.87
These authors carried on four series of tests on rabbits to determine the ability of cocain and morphin to produce aggressins. After determining the minimal lethal dose, the peritoneal exudate was obtained from a rabbit which had been treated with morphin hydrochloride and injected in a series of rabbits, which were later treated with less than the minimal lethal dose. These rabbits plainly showed toxic symptoms and died. The second series of rabbits were given five injections of the exudate and then a dose of morphin slightly greater than the M. L. D. These rabbits survived. In the third series the rabbits were treated first with the serum of immunized rabbits and then with a dose of morphin slightly above the M. L. D. Two of three rabbits thus treated lived for five and seven days respectively, while the control rabbit died within fifteen hours. The fourth series were treated with immune serum, aggressin and slightly less than the M. L. D. These rabbits survived.
From these experiments the authors concluded:
"These data therefore lead us to the conclusion that the blood serum of a rabbit treated with aggressin of morphin possesses immunizing properties and we believe that we are in a position to state that it possesses antiaggressenic properties on the rabbit proper."
D. Morat-191108
Morat, in addition to reviewing Sollier's explanation of the mechanism of withdrawal, in connection with a discussion of the experiments which he carried on to discover the influence of toxic solutions on the
red cells and leukocytes before and during detoxication, gives the following on tolerance:
"Two hypotheses may be proposed according to whether one admits that the phenomenon of tolerance to the toxin is analogous to the phenomenon of microbic immunity and that it is the result, as Gioffredi believes, of the secretion of an anti-morphin, neutralizing the morphin, or whether one considers it as being due to the progressive and selective adaptation of the cells of the organism to the toxic product contained in the fluids.
"In the first instance, one might claim that just as an antitoxin injected into the body increases the hematopoietic and chemotactic reactions, so does the antitoxin of the organism, opposed to morphin and finding itself no longer antagonized during the course of detoxication by the daily equivalent supply of poison, cause in this organism an excessive reaction which is evidenced by the hyperleukocytosis with polynucleosis and by the various hematologic changes which we have described during the period of suppression.
"However, the existence of an antitoxin in the body of the morphinist, even though it has not been definitely disproved, does not seem likely, in view of certain experiments and particularly so from the fact that the serum of morphinists has not, according to Ehrlich, any antitoxic property against morphin. It appears, therefore, at this time, that the tolerance against morphin is alone the result of an adaptation of the protoplasm to new surroundings; the cells possess themselves of the toxic substance and incorporate it, modified or not, into their protoplasm. After that, every alteration in the toxic equilibrium of the body fluids causes in the cells of the body structural changes which express themselves by the occurrence in the blood of cellular debris and albuminoid products of protoplasmic disintegration.
"Besides this the experiments of Buchner have shown that certain principles resulting from the destruction of tissues and from the transformation of albumens, possess the same chemotactic properties as do bacterial toxins. We would attribute, therefore, to the products resulting from the transformation of tissues under the influence of the disturbed toxic equilibrium of the body fluids, a chemotactic rôle and the stimulation of the hematopoietic organs, evidenced during the first period of detoxication by the increase in red cells with an increased resistance and by the hyperleukocytosis with polynucleosis.
"The mononucleosis of the second period which is a real mononucleosis is the direct and logical continuation of the fundamental reaction just as occurs in the greater proportion of acùte infectious diseases. In morphin detoxication, the cause which produces the blood reaction, that is to say the process of cellular transformation, is always considerable and lasts for a certain definite period; this is why, following the fundamental reaction which stimulates the hematopoietic functions, there is always a reaction of the lymphoid organs evidenced by the mononucleosis. Slower to appear but lasting longer, this mononucleosis completes the work of the previous polynucleosis having for its function at the same time that of phagocytosis of the products of cellular disintegration and that of absorption of degenerated polyuuclears"
A. A. J. van Egmond-1911.6°
Referring to certain observations which he made on tolerant dogs in regard to the pulse frequency, van Egmond states:
"These observations are not without significance in regard to the theory of chronic morphin intoxication. Faust concluded on the basis of his studies on the recovery of morphin in tolerant and intolerant dogs that the body had the ability to destroy increasingly large amounts of the poison and that therefore the nervous system was protected against active doses of morphin. Another group (Cloetta, Rubsamen) maintain that in addition to the increased morphin destruction there must be an immunity of the cell to the poison. The above experiments show the latter to be true. For in tolerant animals the behavior of the vagal centre shows that a few hours after poisoning with even small doses of morphin there is enough morphin in the body to cause the individual centres to react. On the other hand there is no reaction on the part of the cerebral cortex and vomiting centre, even if the dose is a hundred times greater. The vagal centre is therefore the indicator for the presence of the active dose of morphin in the body at a time when other parts no longer react. It is of especial interest to note that two centres situated so closely together in the medulla oblongata behave so differently in chronic intoxication."
H. Langer-1912.7°
On the basis of a series of experiments in which he studies the question of whether or not heroin is capable of producing chronic intoxication, Langer concludes that tolerance cannot be explained alone by the ability of the body to.destroy the drug but must depend on the cellular dulling against the active poison. He bases his conclusion on his observation that while in chronic intoxication heroin is destroyed in gradually increasing amounts in the body, only partial tolerance to the narcotic property of the heroin and no tolerance at all to the stimulating property may be established.
H. Dorlencourt-1913.71
This author repeated the experiments earlier performed by Albanese on an intolerant animal and on animals showing varying degrees of tolerance. These experiments led the author to conclude that Albanese's work was corroborated and that the liver has the ability to destroy morphin, which ability increases at the same rate as that at which tolerance is established and is in proportion to it.
A. Valenti-1914.72
Valenti reports some experimental investigations dealing with certain phenomena observed through the use of the serum of morphinized dogs withdrawn from the drug. His preliminary review of the literature and his objects are set forth as follows:
"From an experimental standpoint as yet very few clarifying chapters on the investigation of chronic morphinism which pretend to furnish an explanation for the appearance of the severe disturbances which occur during the withdrawal period in individuals who are accustomed to the influence of this alkaloid, are beyond dispute, for the collected experimental data and hypotheses which have been advanced, concerning this much contended subject of chronic intoxication, are not sufficient to explain to us why, from time to time, symptoms of withdrawal appear.
"The fact that the system accustoms itself to destroying increasing quantities of morphin (Faust) relative to the increase of the accustomed ferment reaction of disintegration which regularly takes place in the tissues (Schmiedeberg) does not explain the condition. Equally unsatisfactory is Rubsamen's opinion that the cells become less and less sensitive toward the poison to account for the severe symptoms during the withdrawal period.
"On the other hand there are also the experiments undertaken for the purpose of determining whether the acquired immunity toward this alkaloid or others might be analogous to that of bacterial toxins. In this case we might attribute the toxic phenomena which are produced by the absence of the neutralized poison, to the hypothetic antimorphin theory of Gioffredi. Yet all these experiments lack sufficient demonstration.
"Indeed morphin, differing from other alkaloids, shows an anticomplementary power (Ferrai) in consequence of which, the salts of morphin retard the appearance of hemolysis in the hemolytic system—guinea-pig complement and the amboceptor of rabbits immunized to sheep's blood cells. In spite of all this, the experiments of Morgenroth, Cloetta, Mirto, and Ferrai show corresponding negative results in an attempt to establish the existence of antibodies in chronic morphin poisoning. They discredit therewith the scanty positive results in the immunizing of mice which Hirschlaff obtained by injecting them with the serum of rabbits which were accustomed to morphin.
"Marmé has advanced the theory that the symptoms of morphin withdrawal may be attributed to a product of oxidation of the alkaloid (dehydromorphin or oxidimorphin). This he showed in the liver and lungs of dogs which were treated with increasing doses of the poison. But other authors like Donath and Stark could find under the same trial conditions no trace of oxidimorphin in the blood and urine of animals treated with morphin. Moreover, it remains certain that this product of morphin oxidation, which is readily obtained either through the action of a vegetable oxydase on the alkaloid (Bougault) or through the influence of atmospheric oxygen on an alkaline substance separated from the morphin (Tolstorff), is very slightly toxic. According to some authors, it is absolutely inactive, while it is very readily removed and separated.
"The experiments of Albanese also show that the liver of morphinized dogs during treatment with morphin is of course not in a position to exercise, in vitro, any influence on the poison, that qualifies them during the period of withdrawal to destroy or change increasing quantities of it. These experiments may possibly supply us with suggestions relating to the question of tolerance but they tell us nothing about the incontestable appearance of the severe disturbances, which are evidenced on discontinuing the supply of the poison.
"In view of such scanty experimental data, a further study of this interesting problem seems indicated.
"I began therewith to determine whether the serum of morphinized dogs, from which the poison had been withdrawn, could cause disturbances of the circulation, when injected into the veins of normal dogs. Such disturbances appeared uniformly but in a more severe form in the toxic picture of morphin withdrawal."
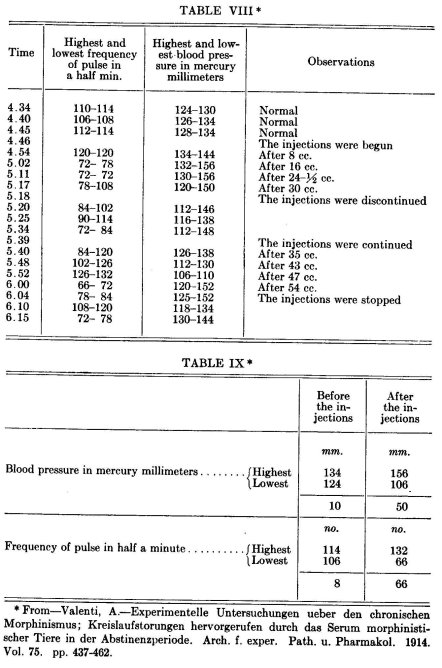
His procedure consisted briefly in introducing into the left carotid of a normal dog serum obtained from the blood of a dog which had been treated with morphin by daily hypodermic injections until a high degree of tolerance had been established. Certain circulatory disturbances followed the injection of this serum and were recorded as shown in his tables and graphs. A considerable number of experiments were carried on, in which dogs accustomed to different amounts of the drug were employed and in which the serum used was obtained after varying periods of withdrawal. The possibility of causing circulatory disturbances with the serum of a normal dog was considered and eliminated through control experiments.
In order to give the reader a concrete idea of Valenti's technique and his methods of recording, the following experiment has been selected as typical:
"In a healthy dog of 6 kilograms, the neck was opened, the carotid laid bare and the injections made into the right external jugular. Into this animal was injected the serum of a dog of 9,100 kilograms, which, beginning with 0.05 grams as a daily dose until, during a period of three months, 225 grams per day was reached, had been injected subcutaneously with a total of 55.12 grams of morphin chloride. After a three days' withdrawal of the morphin, a venesection was made of the femoral vein and 150 cc. of blood was collected, which, when centrifuged, furnished 60 cc. of a lemon-colored serum.
"In this ... experiment the table shows, still more clearly, the great variations between the minimal and maximal blood pressure and pulse rates and still more striking is the difference in the character of the pulse which would appear in one and the same unit of time, as the charts which I take from the record show."
From these experiments, Valenti closes his report with the following:
"Certainly these observations seem to be worthy of publication, even though for the time being they cannot be interpreted with certainty, because during the foregoing experiments I was also able to observe certain details which required further research.
"The only thing that can be accepted as unqualifiedly true is that the severe disturbances during morphin withdrawal, at least those affecting the circulation, cannot alone be due to the absence of the stimulus which morphin exercises on the organs—a stimulus to which the organs and especially the elements of the central nervous system, have become so accustomed that the absence of the poison is in a position to cause a defect in the daily functioning of the organs (Cloetta). Also the serum taken from morphinized dogs during the withdrawal period can bring about the very same disturbances of the circulation when it is injected into normal animals not accustomed to the stimulus of the morphin.
"Every other conclusion or hypothesis would be premature under the present conditions of the experiment. Therefore, I am limiting myself to grouping briefly the observed facts, the main points of which are as follows:
"During the injections of the serum from normal dogs into the veins of animals of the same species, no kind of noticeable circulatory disturbances is brought about. On the other hand, the serum from morphinized dogs in withdrawal causes constant disturbances of the circulation, which are characterized by a clear pulse arrhythmia with a tendency to an acceleration of the pulse and a lowering of the blood pressure. These fluctuations are in direct proportion to the doses of morphin to which the animal was accustomed and appear just as clearly when the serum from a morphinized dog, which has been withdrawn from the drug for some time, is injected.
"Similar disturbances of the circulation, as were observed as a result of the action of the serum, are seen in morphinized dogs during the withdrawal period. As a matter of fact, there can also be demonstrated in these a noticeable rising of the pulse beat, profound arrhythmia and arterial hypotension. All these appearances pass away in rapid succession, if the animal is again given morphin; again, a distinct morphin pulse is indicated as soon as the daily dose of the alkaloid, to which the animal was previously accustomed, is exceeded, entirely independent of the total amount given during the experiment.
"It is evident to every one without further continuing that, with the establishment of such facts, new problems arise. I am engaged in a study of them and hope that out of it will be drawn valuable conclusions."
In 1923 Valenti 74 supplemented these investigations by a study of the action of the blood of morphinized dogs during morphinization and withdrawal on the blood vessels. For this purpose he used Bissemski's technique—the auricular circulation of the rabbit—injecting small amounts of the blood of dogs before morphinization, after morphinization when they had reached a dosage of 1.5 g., after about three months' administration, and during withdrawal, and determining graphically in each case the vasoconstrictive strength.
Valenti gives the following conclusions:
"1. The blood serum of morphinized dogs during morphin abstinence obtained by immediate centrifugation of the blood extracted from three to four days after the last injection contains a large quantity of vasoconstrictors which are capable of causing a very intense and prolonged vasoconstriction of the blood vessels.
"2. These vasoconstrictors are not found in the blood serum during the period of morphinization; if present at all, they are only found in the same small quantities met even in normal' serum, and only produce a mild transitory vasoconstriction of the blood vessels.
"3. The quantity of these substances seems to be in direct relation to the quantity of morphin to which the animal was habituated, for the vasoconstrictive action is much more marked and prolonged as the dose of the alkaloid administered to the animal is increased.
"However, the presence of this large quantity of vasoconstrictors in the blood serum of morphinized animals during the period of abstinence does not only strengthen my original researches, but may also throw some light concerning the genesis of many disturbances during abstinence.
"With the total of these researches the obscure problem of the genesis of the grave symptoms arising during morphin abstinence seems to become clearer, and may sooner or later lead to satisfactory results from the point of view of rational therapy. The latter may be of great use at the present hour when the custom of the use of these drugs is assuming an aspect of a serious social problem."
K. van Dongen-1915.76
van Dongen accepts the conclusions of van Egmond in support of the theory that the ability of the organism to destroy increasingly large amounts of the drug is not the sole basis of the mechanism of chronic opium intoxication, but in addiction the cells of the body become progressively less sensitive to the action of the drug. This author proceeds to investigate in dogs and rabbits the reactions of the respiratory center and of the pupil which had not yet been studied in this connection.
van Dongen sums up as follows:
"If we compare the rapidity with which the different centers become tolerant to a given dose of morphin, for example 10 mg. per kilo, the following is true: This dose was given to `Fox' (dog number 2) from January 14 to February 13 (first to thirtieth day) ; the pupil became tolerant as early as February 1; on February 5, vomiting ceased; on February 9, evacuation of feces ceased; on February 13, neither narcosis nor slowing of the respiration was observed. The same procedure was observed when from February 13 to March 1, 20 mg. per kilo was administered. On February 19, the pupil was tolerant; on February 21, the vomiting center; on February 25, the evacuation of the feces ceased, and on February 27 there was observed no narcosis or respiratory reaction. In the dog `Jim' (dog number 1) tolerance followed in the same course and with the same rapidity.
"The experiments show ... that the narcotic action ceased when there was still a respiratory reaction. But the difference in time in the tolerance of both functions is not great in `Jim' and does not exist at all in `Fox.'
"The following represents the order in which these symptoms take place, beginning with the center which becomes tolerant most quickly and ending with that which usually does not become tolerant: pupil—vomiting--evacuation of feces—narcosis--respiratory center—emptying of stomach—vagal center.
"It can be seen that the centers which lie so closely together in the medulla oblongata as the vomiting center, respiratory center and vagal center behave very differently in morphin tolerance.
"The rapidity with which the different functions become tolerant to morphin is not parallel to the sensitiveness with which these functions react to the different morphin doses in intolerant animals.
"In the following table are given the smallest doses per kilo which produce in intolerant dogs the various symptoms, according to the experiments of van Egmond and myself :
| Vagal center | 0.04 mg. per kilo. |
| Nausea | 0.04 " |
| Vomiting | 0.1 |
| Evacuation of feces | 0.1 |
| Narcosis | 0.1 |
| Respiratory center | 0.1 |
| Emptying of stomach | 0.5 -1.6 |
| Pupil | 1.0 |
"It can readily be seen that nausea which disappears rather quickly in tolerance and the vagal reaction for which tolerance is not possible appear in intolerance in animals on the same very small doses, while the stomach action for which tolerance is possible to only a slight degree and the effect on the pupil which disappears most quickly in tolerance appear upon a dose 25 times greater.
"All of these observations support the conclusions drawn by van Egmond that as an explanation for morphin tolerance the increasing ability of the organism to destroy morphin advanced by Faust is not sufficient but that there must be a specific cell immunity which is developed by the different centers and organs with varying rapidity and which in general cannot be developed by the vagal center."
From his investigations on rabbits van Dongen concluded that these animals cannot be made tolerant to morphin. He studied the effect
on the respiratory center according to the same procedure used in the case of the dogs.
van Dongen gives the following as his final conclusions:
"1. In dogs the respiratory center becomes tolerant to morphin. There takes place a complete tolerance even to 1,800 times the originally active minimal dose.
"2. The central apparatus of the pupil in dogs may become completely tot Grant to large doses of morphin.
"3. The order in which in morphin tolerance in dogs the different centers no longer react to the morphin is pupil—vomiting—evacuation of feces—narcosisrespiratory center.
"The sphincter muscles of the stomach become tolerant only slowly and incompletely and in general the vagal center does not become tolerant.
"4. In addition to an increased destruction of the morphin there must also be accepted a `cell immunity' in explanation of morphin tolerance, which the different centers and organs develop with varying rapidity and which is absent in the vagal center.
"5. The rapidity with which the different centers and organs become tolerant to morphin is not parallel to the rapidity with which normal dogs react to morphin.
"6. Rabbits do not become tolerant to morphin as the experiments on narcosis and respiration show."
J. Biberfeld-1916.76
In a study of the specificity of morphinism, Biberfeld investigated the reaction of the cerebrum of morphinized dogs to scopolamin, heroin, and veronal.
The author found that in each of the three series two dogs which had been morphinized for about four to six weeks reacted normally to the dose of scopolamin, heroin or veronal. He concludes:
"The determination of the effectiveness of narcotic-substances, including not only alkaloids but also one of the fatty series, in dogs which have been addicted to large doses of morphin, shows that the addiction of the cerebrum of the animal is positively specific. It maintains its sensitiveness even towards the derivatives of morphin."
Biberfeld also undertook to determine. the effect of lipoid feeding on the establishment of tolerance. He found that the feeding of cholesterin did not influence the tolerance curve.
On the basis of the following statement this author also studied the immunizing effect of the previous injection of serum taken from morphinized dogs in normal rabbits and cats on the administration of morphin:
"As is known, now and again reports appear in the literature of experiments demonstrating the existence of some kind of `Immune substances' in the blood of animals which are addicted to alkaloids.... So far there has been no corroboration of these assertions. Still it is possible according to the above observations that the resistance to the morphin is carried over by the blood of the immunized animal to the others."
Finally Biberfeld tried to find out how long the tolerance remained after the cessation of injections. He found that if a short period was allowed to elapse (2 to 3 days) there was no variation in tolerance, but after a longer period-10 days—part of the tolerance had been lost.
In brief the author concluded that:
"1. The addiction to morphin observed in dogs upon continuous injections is specific; it does not even apply to diacetyl-morphin.
"2. The feeding of lipoids (cholesterin) does not affect the course of addiction
"3. Immunizing transferable substances are not constantly indicated in the blood of addicted animals.
"4. After about ten days elapse the cerebrum of addicted animals again reacts toward morphin; still there remains a sort of latent state of addiction—abstinence symptoms were not observed."
M. Grüter-1916.1G°
Grüter first reviews different theories relating to the fate of morphin in the body, covering the work of Orfila, Tauber, Kaufmann-Asser,
Faust, Cloetta, and Frankel. He then at considerable length describes the teratogenetic effects of certain drugs when injected into chick embryos, covering the work of Féré, Gaspard and Réaumur, Jan Tur and others. In these pieces of work he secs a definite relationship between the toxicity of various substances on the embryos and on the adult individuals. He points out that while Féré in his work sought to determine to what extent certain poisons produce deformities, lie sought on the other hand to test the influence of the development of
the embryo on the destruction of the injected alkaloids. He continues as follows:
. "Our experiments differ also as regards their extent in time. Féré contented himself with an observation period of 72-96 hours; I incubated the eggs much longer in order that larger and more differentiated quantities of cells might exert their effect on the alkaloids. In view of the entire arrangement of the experiments, this seemed the only possible way of obtaining exact quantitative particulars regarding the amount of the destruction and the conditions leading to it. In order to accomplish this successfully, we must first try to orient ourselves regarding the chemical processes which go on in the egg in the course of incubation.
Griiter then proceeds to a discussion of the chemistry of fertilization and development of the animal egg, quoting the works of Loeb, Warburg, Bohr and Hasselbach, and Escher, because, as he states:
... "the foundation of my investigation rests on these established facts. We have seen that the embryos are disturbed in their development by poisons in the same way as adult organisms. Numerous investigations have established that both oxidative and fermentative chemical processes go on in the incubated egg, and in the same proportions as in the adult individual. After all that, I considered myself justified in attempting to solve the question concerning the mode of the destruction of morphin and its derivatives in the animal organism by injecting those substances into eggs and exposing the latter to incubation under varying conditions."
After describing in detail his method of injecting solutions of morphin, heroin and codein, he describes his findings in detail in experiments with artificially incubated eggs, and his method of analysis for the recovery of the injected drug. He carries these experiments through under different conditions—with a normal supply of oxygen, with a reduced supply of oxygen and with an increased supply of oxygen. The discussion of his findings, together with his summary, is contained in the following:
"It is evident from all these experiments that there is no essential difference as regards the destruction of alkaloids between incubation with increased supply of oxygen and incubation under usual conditions. The active principle does not seem to be the available oxygen in itself; also, the previously formed ferments exert no destructive influence under the greater supply of O:. The determinative element is the development of the protoplasm, and manifestly a certain organization of the albumen does not suffice; there has to be a tolerably advanced differentiation in the cell formation and tissue-building in order that destruction of the alkaloids may set in. If this condition is fulfilled, then even the usual supply of oxygen in the atmospheric air may completely suffice for the destruction; at all events, the latter seems to be more complete when the embryo is completely developed and the supply of oxygen is more abundant, as a comparison of Experiments 2, 3 and 4 with Experiments 39 and 40 shows. Since, on the one hand, we may regard the injections into the incubated egg made in the manner described equivalent to chronic intoxication with morphin, etc., and on the other hand, the chemical influences appear to be the same as in adult animals, the results obtained permit us to draw certain conclusions as to the cause of the destruction of morphin in morphinism. It is, as we have seen, not just any organized protoplasm that receives it, but probably a completely developed cell-system which attains its development only at the end of the embryonic development. This may be evidence of the fact that the destruction takes place through a capacity of the nervous system which has been acquired under the influence of habituation. If, as a result of the chronic presence of morphin, ferments were formed, which had as their task the destruction of the same, one would expect that such processes would appear even in the earlier stages of incubation. But that is certainly not the case. The problem of the destruction of morphin seems, consequently, to possess a decidedly morphological basis, in which an oxidation evidently plays the chief rôle. In connection with the clinical results of morphin abstinence this circumstance is evidence for the fact that the cause of morphin destruction in morphinism is to be attributed to an acquired cell function of the central nervous system. And herewith I agree with Cloetta's conception of morphinism, or his explanation of the increased destruction of morphin observed in connection with it. With this conception we are able to connect the pharmacological fact that the sensitivity to the paralyzing effects of morphin among vertebrates increases with the higher development of the nervous system and also that addiction develops more easily in these more highly developed individuals.
"In addition, it is evident from my own experiments that morphin and heroin are in the main alike as regards their destruction. The fact that addiction was observed for heroin also is in accord with this. The Friihde reagent separates the morphin derivatives rather remarkably into two groups: morphin and heroin, which are eventually destroyed, react directly to it: codein and its nearest higher homologue, dionin, which, to our knowledge, are not destroyed in the animal body, do not react with the characteristic color to it directly, but only after formalin has been added. Babel thinks that in both cases, i.e. both in the destruction by the organism and in the Friihde reaction, this behavior is to be explained by the firmer binding of the ester. Heroin, also an ester, shows, however, as proved by our experiments, less resistance against destruction by the growing organism than morphin. Perhaps physical qualities play a part in this quantitative difference between the two alkaloids. Babel has already demonstrated the higher solubility of heroin in fat as against morphin. For comparison I determined the solubility in water, which I did as follows:
"Finely powdered heroinum basicum was placed in a cylinder and covered with distilled water. This was allowed to stand for 36 hours, being frequently shaken for about a minute. The solution was then filtered off, and 100 cc. of it allowed to evaporate in a weighed glass vessel, dried at 102°C. and weighed, whereupon it was discovered that:
100 cc. distilled water at 20°C. dissolve: 0.0922 heroin basicum
100 " "If it 0.0923 " "
"Winterstein obtained by the same method of determination the following figures for the morphin base:
100 cc. distilled water dissolve at 20°C.: 0.0264 morphin basicum
100 " if l4 " " 0.0250 "
100 " if" " " 18°C.: 0.0248 " "
"This considerably greater solubility of heroin as against morphin, in both media, water and fat, explains on the one hand the fact that this alkaloid penetrates more quickly than morphin into the cell and thus produces more quickly and more intensively its specific poisoning; and on the other hand, these physical relations probably exert a favorable effect on the complete destruction of heroin by the protoplasm. But in connection with the latter fact something else must be given consideration. We know that the higher individuals, especially human beings, are much less sensitive to codein and dionin than to morphin and heroin. The body becomes habituated to the first two substances only with great difficulty. There appears, consequently, to exist a definite relation between the manner of esterization on the one hand, and the effect and habituation, on the other. The alkyl closing of phenolhydroxyl is manifestly a very firm one. This is, therefore, the group in which lies the cause of diminished habituation or capacity to destroy, whereas the greater virulence and easier habituation, along with easier destruction, of heroin is explained by the fact that both acetyl groups are split in the' organism comparatively easily, as a result of which both hydroxyl groups become free and especially ready for reaction. Cloetta and Waser succeeded recently in demonstrating in typical manner for the same substance, tetrahydro—B—naphthylamin, this difference between acetyl and alkyl residue with reference to their capacity for being split off in the body. It was, in fact, a matter of the substitution of a hydrogen of an NH2 group.
"There still remains to be determined what becomes of the morphin and heroin when they are destroyed in the organism.
"The best known oxidation product of morphin is oxydimorphin, which forms readily in the case of an alkaline reaction through the influence of atmospheric oxygen and, in any case, in the presence of an oxydase. It is, however, not very probable that the oxidation of morphin in the animal organism should follow this course. Besides, this product would not escape demonstration by the Fr6hde reaction, since its reaction is identical with that of morphin. Corresponding to the degree of oxidation, however, there develop various decomposition products, which are chemically less well known. In all my experiments in which morphin was destroyed by the embryo, I observed an irregular Frbade reaction—namely, the reagent showed a pink coloring for a long time. This led me to think that a decomposition product of morphin or heroin might be the cause of it; for in all other investigations I did not find this reaction. Unfortunately, the quantities employed were much too small to permit any determination as to the nature of this decomposition product.
"Occasionally Marmé found in intestinal excrements and in extracts from the lung and liver of morphinized dogs, when the latter had had for some time subcutaneous injections of rather large but not fatal doses of morphin, a substance which did not turn violet with Frtihde's reagent, but pure blue and then green. In acute, fatal poisoning with morphin he did not find this substance. He believed that oxydimorphin was involved, the reaction for which had been thus given by Polstorff. Donath then showed that the Friihde reaction was the same for morphin and oxydimorphin; consequently, the substance described by Marmé could not be oxydimorphin. I, too, have twice seen this blue color with Fr6hde's reagent: once in the case of an egg which had grown mouldy while in storage (naturally, it was not included in the investigations) ; and the other time, when I had macerated pure morphin with PbS and water containing H,S for about two months, in order to see whether in the case of a possible colloidal solution of PbS, the latter could have any influence on the morphin. The latter case surely involves reduction processes, the first very probably ; for we know a number of such processes which may be started in inorganic and organic substances by means of mushrooms. Perhaps similar processes are involved in the findings of Marmé.
"SUMMARY.
"Solutions of morphin, heroin and codein, may be injected into fertilized and incubated hen's eggs without necessarily hindering the development of the embryo, if the dose of about 2 cg. is not exceeded.
"The conclusions arrived at by means of an extremely detailed technique as regards alkaloids so injected are as follows:
"If the embryo is completely developed, heroin is always completely destroyed, morphin 50-100%, codein not at all. Increased supply of O2 during the incubation also brings complete destruction of morphin.
"If the development has gone only about half way and death has then occurred, all the alkaloids are recovered in full. Hence it follows that a certain morphological stage of development is required for the two alkaloids to be destroyed.
"The embryo with injection is to be regarded as a chronically poisoned individual. In analogy with facts already established for the chronic poisoning of adult animals, destruction occurs here also only in the case of morphin and heroin. Codein remains unaffected.
"Experiments with increased and diminished supply of oxygen during incubation as well as other results are evidence of the fact that the destruction of the alkaloids, which has been described, is accomplished by the completely developed embryo by way of oxidation.
"The reason why morphin and heroin lead to addiction, and are incidentally destroyed, whereas codein and dionin do not, lies in the manner of the esterization of the phenolhydroxyl. That heroin is most easily destroyed—disregarding its greater solubility in water and oil—is evidently connected with the fact that both acetyl groups are easily split off in the body."
Walter M. Kraus-1918.77
"The object of this paper is to explain the cause of the nature of the symptoms of withdrawal in chronic morphinism. Briefly summarized, the symptoms are simply the opposite to those produced by the action of morphin.
"The reason that any vegetative symptoms appear is that, in the course of acquiring an increased tolerance to the drug, the threshold of irritability of the vegetative nervous system is gradually raised. Were this not so, two things would happen: there would be continual occurrence of symptoms while the drug was used in tolerated doses, and there would be no symptoms upon withdrawal.
"As has been shown in the first part of this paper, morphine causes functional depression."
"The explanation of this sudden reversal of symptoms lies in the fact that morphine taken as a habit-forming drug upsets the normal equilibrium between the sympathetic and the autonomic systems, establishing a new one. When this new equilibrium is destroyed by taking away the drug, symptoms naturally result."
"The symptoms which have been described are all attributable to the lack of the effect of morphine upon the organism—more particularly upon the vegetative nervous system. They are clearly the opposite to those produced by morphine, and thus serve as a further proof of the effects of its action."
A. G. Du Mez-1919.75
Du Mez, 1919, after a review of the literature, comes to the following conclusion as to the mechanism of tolerance:
"From the foregoing review of the literature, it becomes apparent that, up to the present time, all investigators have failed to demonstrate the exact nature of the factors that enable the system, in the case of either animals or human beings, to tolerate enormous doses of these drugs or to identify the substances that give rise to the withdrawal phenomena. The only knowledge of a positive nature that we really have, at present, concerning these problems is that the different organs and centers of the body acquire tolerance to morphin and heroin to a different degree and with varied degrees of readiness; that these drugs, as such, are excreted in the feces in diminishing amounts during the period of acquiring tolerance; and that there is evidently present in the blood serum of tolerant animals (dogs) during periods of abstinence, a substance or substances which, when injected into normal animals of the same species, causes the appearance of symptoms identical with the so-called withdrawal phenomena. Whether or not the disappearance of these drugs from the feces is due to their increased destruction in the organism is still an unsettled question. Attempts to solve this problem through a chemical examination of the excretions have led only to confusion, the literature being replete with contradictory results. Furthermore, it has not been proved that the destruction of morphin in the organism, if it does take place to an increased degree, is a causative factor in the production of tolerance. As stated before, it may be only a concomitant phenomenon."
E. J. Pellini and A. D. Greenfield-1920-1924.79 80
Pellini and Greenfield, believing that the work reported on antibody-formation in chronic opium intoxication had not been wholly satisfactory inasmuch as it was either conflicting or uncorroborated, undertook a series of experiments to determine whether the continuous taking of morphin caused the presence in the blood serum of a substance which had a protective action against morphin. In these experiments, the authors endeavored to determine whether the serum of • humans accustomed to morphin and that of morphinized dogs conveyed immunity to mice and cats.
Before undertaking the actual experiments, however, not feeling satisfied with the results of previous workers, they determined for themselves the minimal fatal dose for the mice, and found it to be between 0.3 and 0.4 mg. per gram weight of mouse.
In a series of 10 mice these authors injected 1 cc. of the serum, taken 8 hours after the last administration from a dog which had been made tolerant to 80 mg. over a period of three and one-half months. Three to four hours later 0.4 mg. morphin sulphate per gram weight of mouse was injected. Seventy per cent died within a four-hour period. The same procedure was followed in a second series, using the serum of a human case, whose blood was withdrawn three and one-quarter hours after the last administration. In this series the morphin sulphate was injected in the mice 18 hours after the serum. Seventy per cent of the mice died. Similar results were obtained with doses of 0.3 mg. morphin sulphate; out of 6 mice injected, three died and three survived.
The authors did not attempt to determine the M.L.D. for the cats, because of difficulty in securing a sufficient number, but on the basis of Gioffredi's work, namely, that he was able to protect young cats from doses varying from 0.05 to 0.14 g. morphin per kilo., they chose 0.07 and 0.08 g. per kilo. The serum of humans was used. Two cats to which 0.08 g. morphin sulphate per kilo. was given one-half hour before 10 cc. of the serum died within two and one-half hours. Of two cats to which the same dose of morphin was given simultaneously with the serum, one died and one survived. Of three cats to which 0.07 g. per kilo. was given a short period (within two hours) after the serum, one died within two and one-half hours and the other two died overnight. All six cats, to three of which 0.08 g. and to the other three 0.07 g. per kilo. morphin sulphate were given 18-24 hours after the serum, died within one and one-half to four hours.
The following is their summary:
"We wish to emphasize the following features of our work:
"1. The difficulty attendant in determining a minimal fatal dose of a drug, especially calling attention to the factor of uniformity of absorption of subcutaneous injections.
"2. That the minimal fatal dose of morphin sulphate for mice is a question which depends very largely on the technic followed; with our technic it proved to be between 0.3 to 0.4 mg. per gram weight of mouse.
"3. The acute stage of morphin intoxication has reached its height within four hours after the subcutaneous injection, and recovery usually occurs if this period is survived.
"4. That serum of the blood of a dog tolerant to morphin sulphate does not protect mice against a minimal fatal dose of morphin sulphate.
"5. That the serum of the blood of human addicts does not protect mice against a minimal fatal dose of morphin sulphate.
"6. That 100 cc. of serum of humans addicted to morphin did not protect cats from doses of from 0.07 to 0.08 gm. of morphin sulphate per kilogram regardless of the sequence or of the interval of time elapsing between the injection of the serum in relationship to the injection of the morphin sulphate.
"7. The morphin tolerance does not develop immunizing properties in the serum either of dogs or of human beings.
"It will be seen that our work gives results which are in direct conflict with the claims of Gioffredi, Hirschlaff and von Marikovsky, all of whom believed that they had established definite protective substances in the serum of morphin tolerant animals."
"The researches in immunology bearing on the nature and mechanism of serum immunity have in recent years tended to make it constantly more probable that such immunity is produced only by proteins, and that the tolerance established to certain vegetable alkaloids is of a totally different nature.
"Conclusion:-1. We consider that the definite conclusion to be drawn from our work, which, so far as we know, is the only work of this nature directly testing the question of immunity acquired by the human morphin addict, is that no substance is formed in the blood serum of a human being who has acquired a high tolerance to morphin, which is capable of conferring any degree of immunity to the toxic action of morphin on an animal into which it is injected.
"2. Likewise we have been able to show that the blood of a tolerant animal does not contain any protective substance against morphin."
Later in 1924, Pellini and Greenfield report 81 a study of the question of "whether any specified toxic substance is produced by morphin habituation." They continue:
"This question, which is closely related to the first, has a more direct practical bearing on the current theories of the nature of morphin addiction and the causation of withdrawal symptoms, and also on treatment. There has been considerable controversy on this subject, and a more or less widespread belief that there is such a substance, and that it is the cause of the well known symptoms of morphin withdrawal when no longer neutralized by the continued administration of morphin; and some methods of treatment of drug addiction have been founded upon this belief.
"The scientific basis for this conception originally rested upon the work of Marmé, who reported the finding of oxydimorphin in the feces, lungs and liver of dogs habituated to morphin. He further stated that oxydimorphin produced symptoms similar to those of morphin withdrawal, when injected into nontolerant dogs. Marmé's results have been disproved by numerous subsequent investigators.
"The belief is at present based solely upon the work of Valenti, who in 1914, reported a series of experiments in which he investigated the effects produced on the circulation of normal dogs by the intravenous injection of serum of the blood of dogs accustomed to increasing doses of morphin, and which were in withdrawal when the blood was obtained. Since his results have never been tested by other investigators, we have made the study of this question the subject of the present paper."
These authors morphinized a male dog, weighing 17.5 kg. over a period of ten months, beginning with a daily dose of 10 mg. morphin hydrochlorid administered subcutaneously, and reaching 2.75 g. during the last months. After electrocardiographic studies of the heart rate of other morphinized dogs at various stages of withdrawal, which led them to conclude that the heart rate rose after withdrawal to a maximum point reached in about forty hours, they drew the blood for the present experiment forty-one and one-half hours after the last dose had been administered. Electrocardiac observations were made on this dog.
To prevent the occurrence of circulatory variations from the degree of anesthesia, these authors were able to maintain a uniform rate of ether administration by employing the method devised by Dr. Ben Morgan. The serum of the morphinized dog was injected into the left external jugular vein, upon exposure, through a cannula. A control was also used, in which normal dog serum was injected into a normal dog.
The following table gives the heart rate and blood pressure readings. The authors continue:
"Comparison of the records obtained with normal serum and serum of the morphinized dog in withdrawal shows no such effects of the latter as were described by Valenti, but in view of the disparity between our results and his, we felt that additional work along somewhat different lines would be desirable, and next proceeded to electro-cardiographic studies. By this procedure, we were enabled to dispense entirely with anesthesia and thus avoid any possible disturbing factor that might be due to the anesthetic. Moreover, it afforded a more sensitive means of testing the heart and rhythm."
After a preliminary period of training a dog to undergo the injections without anesthesia, electrocardiographic studies were made first after normal serum and then after the serum taken from the morphinized dog in withdrawal had been injected, with all other conditions being identical with those of the preceding experiment. The authors state:
"Comparison of these results with those of the preceding experiment shows no effects from the serum of the morphinized dog in withdrawal comparable to those shown by Valenti.
"Besides studying changes in heart rate, the electrocardiograms were analyzed also for the maximum variations in the auricular complex, the ventricular complex, the complete cardiac diastole, the sequence and the rhythm of the heart. The results of the analysis did not show any effect that could be attributed to the serum of the morphinized dog in withdrawal and such variations as occurred were fully explained by respiratory sinus arrhythmia.
"Since the foregoing experiments were confined to a study of possible effects on the circulation, we thought it desirable to extend the scope of our investigation to include other studies which might throw light on the effect of the serum, such as possible effects on the central nervous system or on the chemical composition of the blood.
We therefore conducted, concurrently with our experiments on the circulation, two other series, in one of which we endeavored to ascertain by observation of the behavior and general symptoms of cats injected with such serum, whether any effects were produced, especially any referable to the central nervous system. Our technic in this series was as follows: The cats, which were not anesthetized, were placed in a box from which the head and neck alone projected; the external jugular vein was exposed just sufficiently to permit the insertion of a hypodermic needle, and 10 c.c of serum was quickly injected by means of a syringe. The cat was then immediately released, the whole procedure described taking not more than three or four minutes. The animal was then kept under close observation for an hour or more, being allowed to roam at will in the laboratory. Six cats were injected with serum, and Table 7 gives data regarding the dog serum used in each case.
"In all cases, the behavior of the cats was entirely normal, and they showed no effects from the injection of the serum.
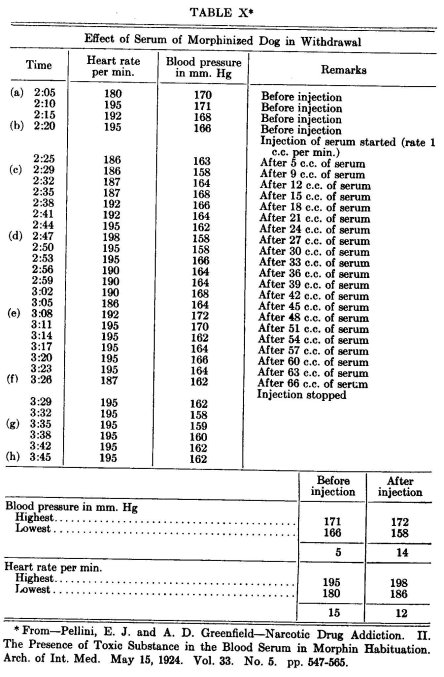
"Our final series consisted in analysis of the blood of morphinized dogs in withdrawal. The analysis of the blood was performed according to the methods of Folin and Wu and of Van Slyke. The blood used was obtained from the dogs and at the times described in.Experiments 2, 4, 5 and 6 of Table 7. Table 8 gives the results.
"TABLE 7-DATA REGARDING SERUMS USED FOR CAT EXPERIMENTS
| Experi- ment |
Period of addiction |
Daily dose of morphin at close of period |
Time of drawing blood after withdrawal of morphin |
| 1 | 3 months | 0.4 gm. | 2 days |
| 2 | 6 months | 3.0 gm. | 3 days |
| 3 | 3 months | 0.5 gm. | 2 days |
| 4 | 10 months | 2.75 gm. | 41½ hours |
| 5 | 1 year | 1.0 gm. | 3 days |
| 6 | 1 year | 1.0 gm. | 18 hours |
"The foregoing results are well within the range of normal dogs' blood.
"Before comparing our results with those of Valenti, it may be desirable to make a few comments on his report. One of the features of his results to which he attaches great significance is the marked increase in range of variations in blood pressure and heart rate, after injection of the serum of a morphinized dog in withdrawal, as compared with the range in the normal period before injection. His method of obtaining this result from his records is to select the highest and lowest points, wherever they may occur in the normal period and in the period
"TABLE 8-CHEMICAL ANALYSIS OF THE BLOOD OF MORPHINIZED DOGS IN WITHDRAWAL.
| Dog 2 | Dog 4 | Dog 5 | Dog 6 | |
| mg | mg | mg | mg | |
| Nonprotein nitrogen | 30.0 |
31.0 | 29.0 | 28.8 |
| Urea |
17.2 | 15.0 | 15.4 | 13.4 |
| Creatinin | 1.2 | 1.5 | 1.2 | 1.2 |
| Uric acid |
1.0 | 1.0 | 2.3 | 2.0 |
| Sugar | 110.0 | 104.0 | 75.0 | 76.9 |
| Whole blood chlorids |
450.0 | 544.5 | 475.0 | 585.0 |
| Carbon dioxid |
52.2% | 50.0% | 52.0% | 56.6% |
after starting the injection, respectively, and compare the differences. We find a few instances of errors made by him in the selection of these figures from his records, but this does not affect the general nature of his results. In reporting that phase of our work, which was an attempt to duplicate his, we adopted the same method in order to permit of exact comparison, but we were unable to appreciate the significance of this particular feature of the results.
"Examination of his tables shows that, in the majority of instances, the extreme high and low points of both the heart rate and blood pressure occur at various points in the progress of the experiment, and that both the heart rate and the blood pressure range up and down throughout the experiment, rather than following a definite and consistent course. It is hard to conceive of any substance which, when injected at a uniform rate into the veins of an animal, would be capable of producing such an irregular effect. Similar effects can be produced by substances which are rapidly absorbed and excreted, when not administered uniformly. It is well known that ether administration, when not under exact control, will produce these effects. It will be noted that, as already stated, Valenti does not specify the form of anesthetic used in his experiments. It appears, however, that in his control experiments, using normal dog serum, he reports much smaller variations, and we are unable to offer any explanation of these observations. In our work, as will be seen from our tables, we obtained no results showing any substantial difference, as regards variability in heart rate or blood pressure, between the effects of the serum of a morphinized dog in withdrawal and those of normal dog serum. The slight differences occurring were more marked following the injection of normal serum.
"Another feature of Valenti's reported results on which he lays much stress is the arrhythmia, which he states is produced by the injection of the serum of a morphinized dog in withdrawal. We have given sections of his tracing which he selected as showing three different types of arrhythmia. We have also given sections of our tracings for comparison. Our results do not correspond with his, as the tracing of our experiment with such serum shows no arrhythmia. The variations of rhythm shown in our tracing of the dog injected with normal dog serum are of the type obviously associated with respiratory changes.
"The electrocardiographic method is, of course, much better adapted to show these features of the heart action than the mercury manometer, and it is naturally to be expected that if arrhythmia were produced, it would be plainly apparent in the electrocardiograms. Our electrocardiographic studies show no abnormal arrhythmia. Such changes in rhythm as appear are, in the first place, uniform in all our electrocardiographic experiments, and, in the second place, clearly respiratory, as may be seen by comparison with the respiration curve. It is worthy of note that in the electrocardiographic experiments no anesthetic was used.
"Valenti finds that the degree of circulatory disturbance produced by the injection of the serum of the morphinized dog in withdrawal is directly dependent on the total amount of morphin consumed during the addiction period. The largest total amount consumed by any of the dogs from which he obtained serum for injection was 69.95 gm. The serum in the experiments on the circulation presented by us was obtained from a dog that had received a total of 168.62 gm. If his conception is correct, our results should have been much more pronounced than his. The same reasoning applies in a measure to the question of the length of time of withdrawal of the morphin. While Valenti claims that the serum is equally effective when the blood is drawn at any time from thirty-six hours to twenty days after stoppage of morphin administration, we ascertained by electrocardiographic studies that there was a definite time at which the circulatory disturbances in the morphinized dog were at their maximum, and the serum used by us was obtained from blood drawn at that time.
"We feel that our work on cats and blood analysis is corroborative of our negative findings. We also feel that the conclusions reported in our first paper of this series have a definite bearing on the question now under discussion. We there reported that the serum of morphin addicted dogs and humans had no protective effect against a minimal fatal dose of morphin. If there was any toxic substance in the blood causing circulatory changes which, as Valenti claims, could be neutralized in its physiologic effects by the administration of morphin, it is difficult to conceive the nature of such substance unless it is either chemically or physiologically an antidote to morphin. Our previous work shows conclusively that no such substance is present.
"A notable point in Valenti's report is the statement that the circulatory disturbances in morphinized dogs can be suppressed, and the normal circulatory condition restored, at any time from thirty-six hours to twenty-one days after withdrawal, by administration of the previously accustomed daily dose of morphin. He emphasizes the fact that this effect cannot be produced by any amount less than the previous daily dose, and that it is only when this amount is exceeded that the typical `morphin pulse' becomes evident. Such persistence of tolerance as he reports is directly contrary, not only to the generally known facts in the case of human beings, but also to the results of careful experiments on animals by competent investigators. Cloetta, experimenting on rats and pigeons, found that these animals lost their tolerance as early as two days after the withdrawal and that the previous daily dose, if of a size fatal to a normal animal, proved fatal to these previously tolerant animals after this lapse of time. Van Egmond shows that in dogs accustomed to tolerate 1 gm. of morphin daily, the vagus still responds to the injection of minute doses. He found it possible to change the heart rate from 120 to 80 per minute by a dose of 0.04 gm., while doses as small as 0.00008 gm. per kilogram in these same animals showed an appreciable effect. Van Dongen and Tamura also found that the vagus center does not become tolerant to morphin. In the course of our work, we found that profound general effects were produced by the injection, three days after the withdrawal, of a previous daily dose of 1 gm., and these were noted very promptly, being quite pronounced within twenty minutes or less time.
"We feel that Valenti's failure to give important details of his technic (e.g. the anesthetic used), the peculiar way in which he arrives at his conclusions by selection of figures from his records, and the impossibility of rationally reconciling his results with those of other workers who have investigated different aspects of the effects of morphin tolerance, and whose conclusions have met with general acceptance, lend weight to the conclusions to be drawn from the consistently negative results of our own work. We feel that our technic was such as to eliminate possible extraneous factors that may have influenced Valenti's results, and that the conditions under which our work was performed were even better calculated to obtain clear positive results from any toxic substance that might be present in the blood.
"Conclusions.-1. No toxic substance is formed in the blood of dogs habituated to morphin which is capable of producing circulatory disturbances in normal animals into which the serum is injected.
"2. We find no evidence that any toxic substance is present in the blood as a result of morphin habituation."
H. C. Lane-1920.82
Lane reports, as follows, a method for detecting chronic opium intoxication by means of a hemolytic reaction:
"The finger of a suspected opiophagic patient is stabbed with an automatic lance. The blood is drawn into a Gower's blood pipet holding 2 c.c. This is expelled into a small test tube five by one cm., containing one c.c. of normal saline solution. This is repeated for five more saline tubes. The tubes are numbered 1-2-3-4-5-6. Shake each tube gently immediately after the blood is introduced. Prepare two more saline tubes and number them 7 and 8. If any shreds or clots of blood should be present, remove them with a sterile platinum wire. As a rule they will not be present.
"Tubes 1 and 2 are controls, containing only saline solution and blood. To tubes 3 and 4 add .2 c.c. of a 1-100 solution of morphine sulphate in distilled water. The solution should be neutral, it must not be either acid or alkaline, therefore it should be tested with red and blue litmus paper and with phenolphthalein and methyl orange indicators. To tubes 5 and 6 add 2 c.c. of a 1-200 solution of morphine sulphate made with a good grade of the drug in distilled water. Tubes 7 and 8 contain the blood of normal individuals.
"After standing at room temperature out of the light for some twelve to twenty-four hours or even less, tubes 1 and 2 (controls) show complete inhibition of hemolysis with a clear supernated fluid. Tubes 3 and 4 show almost complete inhibition of hemolysis with a very cloudy supernated fluid. This flocculent flaky appearance is the positive test for a drug habitué. Tubes 5 and 6 show a modified flocculent appearance of supernated fluid. Tubes 7 and 8 (true controls of normal blood) show a clear supemated fluid with complete inhibition of hemolysis. I would like to caution the investigator that upon agitation of the tubes, the flocculent deposits settled to the bottom of the tubes. The tubes should be placed against a black background, in order to accurately interpret the results, as a clear bright light obscures the readings.
"It is also possible that the reaction takes place with any of the narcotic drugs such as heroine, codeine, and others. The blood of a drug user has amboceptor with at least one narcophore binding cell which has an affinity for the drug the patient is taking. This is a rapid method of testing the blood of a drug addict, as the blood does not have to be passed through the lower animals to secure antiserum. All the glassware should be sterile, the technic is simple and any one can do the test. The test may also be done with rabbit serum which has been sensitized with the blood serum of a drug habitué. I do not state that this test is perfect but in the course of time it should be made an aid to diagnosis."
E. S. Bishop-1920.88
"Tolerance or an immunity to the toxic effects of narcotic drugs are primary and striking characteristics in the development of addiction. An antitoxin or antidotal substance is the recognized mechanism of their production in most diseases admittedly developing these characteristics. I have adopted the hypothesis, therefore, that an antidotal substance is manufactured by the body as a protection against the poisonous effects of narcotic drugs constantly administered. Such a substance, manufactured in the body, being antidotal to morphine, might well possess toxic properties of its own, exactly opposite in manifestation to those possessed by morphine and other opiates. Toxic substances exactly opposite to opiates in their action might readily account for the severe withdrawal signs, parallel in their extent to the extent.of opiate insufficiency, and resembling in their characteristics the manifestations of acute poisoning.
"A hypothetical antidotal toxic substance, manufactured by the body as a protection against the toxic effects of continued administration of an opiate drug, will therefore explain the well-known development of tolerance and immunity in these cases, and will account for the violent physical withdrawal signs. In a word, it will explain the disease fundamentals on a definite physical basis.
"Such an hypothesis will explain the stage of development of addiction before outlined. In the stage of tolerance the antidotal toxic substance has begun to make its appearance in the body and to protect it against slight narcotic excess, but its manufacture is not sufficiently established to continue longer than necessary to neutralize the narcotic administered. In the stage of beginning addiction, or beginning narcotic-need, its manufacture has become more developed and more constant and proceeds for a longer time after the discontinuance of the narcotic drug. In the stage of fully developed addiction, or absolute narcotic need, the manufacture of the antidotal toxic substance has become practically an established pseudo-physiological body-process, and will continue long after the administration of the narcotic drug for reasons into which I have gone elsewhere. In other words, in narcotic drug addiction some antidotal toxic substance has become a constantly present poison, and the narcotic drug itself has become simply the antidote demanded for its control. In brief, fundamentally and basically, narcotic drug addiction is a condition presenting definite physical phenomena, symptoms, and signs, due to the presence within the body of some autogenous poison requiring narcotic drug for neutralization of it or of its effects.
"This explains the phenomena of the mathematical exactness with which the minimum daily need can be estimated under experimental conditions, and with which doses less than the amount of actual body need relieve existing withdrawal signs in definite proportion to the amount of opiate administered. In exact proportion as the drug of addiction is present in the body to neutralize or oppose some antidotal poison, is the patient free from withdrawal symptoms and from physical craving for the narcotic drug.
"The development and existence of such mechanism in the body of the opiate addict is suggested also by the apparent continuance of tolerance to opiate existing after long periods without drug in individuals who had previously suffered from addiction-disease, and in the susceptibility of the former sufferer subsequent to the arrest of his physical need for opiate, to the re-establishment of that need by the subsequent administration of the drug."
K. Schübel-1920.84
This author studied the changes in the chemical composition of the central nervous system and in metabolism in general not only during chronic opium intoxication but also during withdrawal in four dogs. From his observations of the variations in the nitrogen, purin and phosphoric acid elements in the urine and feces, he concludes as follows:
"The severe symptoms which are observed during morphin withdrawal have primarily a gastro-intestinal origin. They are functions of the digestive organs. If the morphinist continues to take the poison `secretion narcosis' becomes greater. If the supply is interrupted there is a sudden hypersecretion which in turn acts as a strong stimulant. In addition to this peripheral action on the digestive apparatus there are also involved alterations in the central rervous system in connection with the production of withdrawal symptoms.
"The findings resulting from my experiments on metabolism in dogs, especially the simultaneously increased elimination of purin base and phosphoric acid, supports my opinion that the central nervous system undergoes alterations in its normal composition on long continued morphin administration, which during addiction, because this is formed very gradually, produces no severe symptoms. But the sudden interruption of the morphin supply has the effect of a sudden lack of an integral part of the nerve cell which•produces the given severe symptoms. We make no mistake in assuming that the basic morphin or its decomposition products can replace other basic substances of the nerve cell during addiction. The omission of this new basic constituent of the nerve cell produces alterations in the chemistry of the cell and functional disturbances which are distinguishable without further analysis."
C. C. Wholey-1913-1922.
From the writings of Wholey, from his replies to our questionnaire, and from recent correspondence, we have taken the following:
"Opiumism is a chronic drug intoxication resulting from the use of opium or its derivatives to a stage of abnormal tolerance, and characterized by pathologic somatic and psychic changes, chiefly chemico-metabolic, secretory and neuropsychiatric, in nature."
* *
"Opiumism ultimately brings about a neuro-psychopathic state which more or less permanently and profoundly alters the personality. This alteration is probably induced by the pathologic effect of the drug upon the body chemistry. The psychopathology evidences itself by the varying degrees of dependency, delinquency, and often of depravitÿ, noticeable in victims of this disease-condition. "This artificially induced psychopathologic state is similar to, if not identical with, that found in many cases of so-called psychopathic personality or constitutional inferiority. In one case the condition is induced, in the other it is inherent. Although opiumism may induce, as stated above, alteration and deterioration of personality, it must not be thought that every such degenerate state, in victims of the drug, was brought about by its use; in many of them, this inferiority existed before the drug was taken and frequently accounted for its beginning use. "We assume the unity of the organism and the common evolution of soma and psyche. When an opiate drug is taken (with or without the knowledge of the patient) to the point of physical tolerance, or in other words, to such an extent that the body cells cannot function comfortably without it (`cell dependence'), withdrawal symptoms develop on abstinence from its use, and a psychopathologic status has been established. But if the taking of the drug continues, this psychopathology becomes more and more firmly fixed. With larger doses and longer use `cell dependence,' of course, increases in intensity. It is obvious that when an individual continues the use of the drug deliberately, there is an added element of character weakness, or deterioration present.
"When the human organism has become definitely adjusted to the drug (the length of the period of adjustment varies with the individual), it has become the pivotal point around which interest chiefly revolves; without the drug craving and bodily discomfort supervene. The emotional tone has become abnormal, maintained as it is, upon an artificial metabolism. Normal sensations are obtunded, or shut out; and the sense of well-being, or coenesthesia, does not correspond with reality. The sensory system does not report correctly, thus perverting judgment, and coloring emotion. One has but to recall the instantaneous transition from despondency to exuberance when an overdue dose has been administered. Again the individual will insist that the drug is beneficial, though he is on the brink of mental and physical collapse.
"In any state of illness the emotional tone is changed and judgment, therefore, impaired to some extent. But in opiumism this false emotional status, kept up by the drug, becomes, as it were, chronic, and the victim's outlook upon economic, social and other relationships conforms to a false sense of well-being, or security."
In discussing Bishop's theory of an antitoxic substance, Wholey 88 states that Bishop does not emphasize sufficiently the part played by the nervous system in the symptomatology of opiumism, and that the nervous system through constant inhibitions becomes pathologic in its reactions. Whether the toxic effect on the nervous centres is due to the opium or to an antitoxic substance, or not, we have a disease syndrome which must be "treated in the light of nervous and psychic deterioration." He states that while we must not lose sight of organic disturbances and the treatment they require, back of all such disorders, "whether secretory, trophic or cardiovascular, there exists a deranged nervous system, the etiologic factor in their causation."
"By locking up the secretions and otherwise interfering with the normal metabolic action of the organs, including the nervous system and brain, morphin induces a disturbed or painful coenesthesia—a sense of general bodily discomfort—. which may become unbearable."
"Opium intoxication differs from that of the other common chemical or bacterial intoxications, in that it is so intimately bound up with the individual's adaptations to his environment. The peculiarity of this drug is its obtunding of all sensory avenues, upon which the individual depends, for accurately putting himself in touch with his surroundings; it causes his senses to misinform him, on the side of euphoria or well-being, thus producing an ever increasing lowering of his threshold of resistance to painful or unpleasant sensations of situations. As a result of his habitual obviation of effort by further insensitization, he sidesteps the normal effort to meet the common difficulties and obligations of life.... Thus is brought about that character deterioration which is always seen in the drug addict and which varies according to the individual's original fibre. The higher mental qualities constituting character regain their former vigor only after a lengthy absence from the drug and when complete organic rehabilitation has taken place. This delayed character (will power, proper ethical value, etc.) re-establishment is, to my mind, the main factor in the causation of relapses."
"A physiologic and psychic need for continuance has usually been established, before the morphinist finally reaches the place where he realizes his condition sufficiently to seek a physician; he has undergone marked changes in body chemistry, and in mental processes and in estimation of ethical values. He presents the picture of abject neurasthenia. He is afraid to continue his drug and has no courage to contemplate the discomfort of discontinuing it. His nervous and mental degeneracy manifests itself largely in fear, which dominates his conduct. He fears death, he fears his ability to carry through the day's work; he is afraid of falling into poverty, and is obsessed by the fear that he will not sleep. This factor of fear makes for the continuance of the habit and accounts largely for many relapses when the drug has seemed to be successfully withdrawn.
"The comparison of opiumism with any other toxic disease (except those arising from other narcotic habit-forming drugs), or bacterial disease, must take into account the intricate habit involvement uniquely existent in narcotic drug addiction. Aside from the mere routine matter of getting a patient off his drug, there would practically be no opium problem, if it were not for the habit involvements and abnormal memory-associations which have been set up by the use of the drug. A neuro-psychasthenic state has been produced by the use of the drug during the stages of habit formation. If it were not for the peculiar memory-associations having to do with the comfort and sense of security induced by the drug, and to the fixed habit of turning to it, either as a bolster, or a solace, its victims would resort to the customary channels for the care and treatment of the resulting psychoneurasthenic states, just as they would have done if their illness had resulted from other causes. If other toxic, or germ-born diseases were rigidly comparable in their effects with those of opiumism, we ought to see some evidence of a desire for experience under circumstances similar to those under which relapse to opium occurs. If the peculiar residue of psychic pathology produced by opiumism were specific in character, I should not look for its assuagement by such chemically different drugs as alcohol, cocain or tobacco (the last where the symptoms are mild).
"Any individual may become addicted to the excessive use of narcotic drugs. The majority of my cases represent the average individual with the average heredity and environment. These have generally acquired their habit accidentally. It is, therefore, fallacious and unjust to refer without qualification to drug users as a class inherently neurotic and degenerate."
In amplification to his reply to our question as to the nature of chronic opium intoxication, whether physical or mental, Wholey writes as follows:
"One cannot draw a sharp line of distinction between physical and mental factors in analyzing the basis of addiction to narcotic drugs. The basis, in certain cases, may be regarded as purely physical for a longer or shorter time, depending upon the constitution of the individual, as in tic douloureux. But often, in such cases where the circumstances call for the use of the narcotic, it is only a question of time before a pathologic psychic condition is established. In my mind, this constitutes the real basis for the narcotic habit. I believe that normally the appetites and cravings originate largely in visceral activities and are dependent upon the normal functioning of the autonomic system (including the ductless glands) along with that of the viscera; in other words, the James-Lange theory of the emotions enables us to explain the pathology of narcotic addiction more satisfactorily than any other theory. It is because of the pathologic reactions, which are set up in the autonomic visceral system, that abnormal cravings are established. Because of this fact, these cravings are so difficult to eradicate, and produce such a profound impression upon personality equations and character-integrity. This is because the autonomic element is injected into the situation. A condition is precipitated which reduces every individual to a psychopathologic basis comparable to, if not identical with, that of the hysteric. Craving for the drug occurs under conditions similar to those under which symptoms of hysteria arise, in one who shifts to this mode of reaction, where normal adjustment seems impossible. The difference lies in the fact that the narcomaniac seizes upon the drug, and the hysteric retreats behind his protecting symptom. There is a great individual difference in the rapidity with which the foundations of the personality present evidence of giving way to the subtle attacks of the narcotic; one is able to gauge the stability and resistance of a given individual's character and mental makeup, with remarkable accuracy, by checking up the degree of facility with which he succumbs to the pathologic modes of reaction typically set up by the use of the drug. In the inherently unstable, the drug plays quick and generally permanent havoc—showing itself in the fact that these individuals rarely make a successful recovery, after coming definitely under the domination of the drug; few of them are able again to make successful social adaptation. It is the cases who belong to this type who constitute the menace to an understanding of drug addicts generally, and it is this class which is so unsuccessfully and so unintelligently handled. Nothing short of prolonged institutional care, under conditions such as might be had in farm colonies, where they could learn trades or pursue other avocations under protection and discipline, will, as a rule, give them any chance for a successful rehabilitation. A further evidence of the marked involvement of the autonomic system, is furnished in many ways. As an individual comes more and more under the domination of the habit, his desires and cravings and ambitions all become merged into the one big concern of his existence—the procuring of the drug and the maintaining of the narcotic state. The deep-seated inroads made upon his personality is evidenced in his loss of the instinct of self-preservation. He ceases to be provident. Things seem promising when they are not so and reality is entirely colored by the abnormal outlook created by the drug. Among the physical evidences of involvement of the autonomic system we find cessation of menstruation in the female with atrophy of the mammae, and in both sexes, very commonly, a marked interference with, if not a complete loss of, normal sexual feeling. These glandular functions and instincts are under the control of the autonomic system. Among `withdrawal' symptoms we have very commonly the appearance of such involuntary autonomic phenomena as sneezing and yawning. Further evidence of the autonomic control of the patient is furnished in the instances where even very intelligent and, apparently, well-meaning persons will secretly take the drug throughout their treatment and undergo considerable discomfort, when they cannot help but know that the circumstances will be revealed and their reputation and money lost."
F. Hildebrandt-1922.88
The work of this author consists in a study of the changes in metabolism in rats caused by thyroid, thyroidectomy and the chronic administration of morphin. In his study of the effect of chronic mor-
phin administration, experiments were made on eight rats, the details of which he gives as follows:
"Half of these were kept on the same food while the food was varied for the other four, and the experiments were made at least 12 hours after the last feeding.... Where we began with a dose of about 10 mg. per 100 g., at the height of immunization 60-100 mg. morphin hydroch. per 100 g. rat was injected daily. Especially in the first eight days of immunization the desire for food was considerably diminished, and the animals often ate scarcely half of their bread and milk ration. Otherwise, when they were once addicted to the morphin, even on high doses, they behaved normally again after 1 to 2 hours. The skin of the back under which the injections were made was dry and brittle and lost the hair in spots.
"First let me report on the experiments on the four rats during immunization in a state of fasting. They were young animals still in the growing stage. On June 18th, the morphin injections were begun. The animals increased up to the beginning of July, when their metabolism was studied in two-hour experiments,
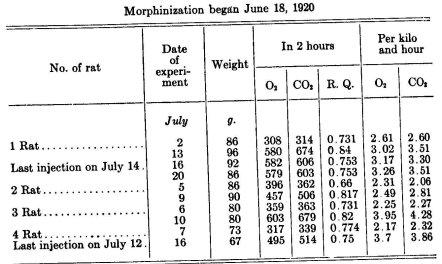
about 15-20% in weight, an indication of the fact that their growth was practically uninterrupted by the administration of the morphin."
The results are given briefly in table form on the preceding page. The author continues:
"In consideration of the results of these and all other experiments we can establish three points:
"1. A reduction of metabolism, which cannot be further explained. There must be taken into consideration the narcotic action of the morphin and a change in the behavior of the animal in the nature of a diminished spontaneous mobility. For both there is known at present no basis, and therefore, as above mentioned, we have always refrained from making an injection on the same day as the experiment was made, in order not to vitiate our results with the acute narcotic action. An after effect on the day following injection could be avoided, as the animals had maintained themselves in the beginning of the morphin administrations after about ten to twelve hours and later even after one to two hours. Our rats appeared perfectly normal on the days for experiment and no different in their behavior from addicted animals. During morphinisation the weight remained the same for a long time, in many (young, growing rats) it continued so, in a few grown animals there was a slight decrease.
"2. In the final states of the morphinisation—in general after about four weeks—there appeared suddenly a rapid loss in weight, the rats were cachectic and at the same time the metabolism rose considerably beyond normal.
"3. Both actions show that the chronic administration of morphin interferes in some way with the mechanism of metabolism. This is true also of the observations on the respiratory quotient. In comparison to the normal it is greatly increased. Therefore the same point may be established as in the case of the thyroidectomised animals. Here also the same question arises: primary increase of the consumption of carbohydrates, interrupted glycogen formation, or increased mobilization of glycogen. As a further possibility for discussion there is an increased CO, elimination (as the result of a CO, retention through the narcotic action of the morphin) on the day following the injection. If we consider this last possibility first, it does not seem necessary to explain the high respiratory quotient. If this is right, we should expect especially in the first part of the morphin addiction, i.e. after the first injection, an especially high respiratory quotient, since the recovery from the acute morphin poisoning always proceeds quickly with the degree of addiction, with which there is always associated a short CO, retention. But as a matter of fact the opposite is the case: the further morphinisation advances, the higher the respiratory quotient.
"What is the case then with the interrupted glycogen fixation and the increased mobilization of the glycogen? If again we proceed from the hypothesis that the sugar is not fit for consumption in the organism when it does not originate in glycogen, then there can be no interruption of the glycogen fixation for the respiratory quotient may not be high, since the carbohydrates offered to the organism can be consumed only with difficulty. The possibility of an increased mobilization appears very plausible, as glycosuria is often observed after morphin. But on further reflection this hypothesis is also untenable: from the experiments of Luzzato on dogs and rabbits it has been found that in the first place very toxic doses of morphin must be used in order to produce a glycosuria, from which there is obtained at the same time a considerable amount of albumen. Further there is involved only a transitory phenomenon which disappears with the cessation of the morphin action, and in the third place the important thing for us is that we succeed in completely preventing the appearance of glycosuria by cautious addiction to morphin. As pointed out above, we made no injections on the days of experiments. That the morphin would still cause sugar mobilization on the day following the injection is highly improbable and according to Luzzato's experiments can be disregarded. Besides we always began the immunization with small doses and in this regard observed no glycosuria, which again is in accord with Luzzato's experiments. Consequently it would be inconsistent to account for the high respiratory quotient by increased sugar mobilisation. Rather we should accept the hypothesis that it is a question of a primary increase in the consumption of the carbohydrates."
In relation to the similarity between the chronic administration of morphin and thyroidectomy, the author states:
"If we compare the action of the chronic administration of morphin with that of thyroid feeding and thyroidectomy, we find that the treatment with morphin over a long period has the same effect on the metabolism of the rats as the removal of the thyroid gland. In both cases there is a reduction of the metabolism which in both cases we can attribute with apparent certainty to a primary increase in the oxidation of the carbohydrates.
"Then the question was—do thyroidectomy and long-continued morphin administration act similarly in other respects?
"We have mentioned above experiments on thyroidectomized rats in which the high respiratory quotient was lowered by thyroid feeding and the total metabolism was raised. If then we succeeded in obtaining this also in morphinized animals by supplying thyroid, we could draw a further analogy. As a matter of fact this was the case:
"The respiratory quotient of the rat concerned was on the 12th day of morphin administration on the five observation hours 1.04, 0.984, 0.98, 0.87 and 0.80. With the same daily dose of morphin injected, 2 g. thyroid daily was fed for three days. On the fourth day the course of the respiratory quotient was considerably lowered-0.904, 0.803 and 0.758 in the first three observation hours. In spite of the great loss in weight (22 g. in four days since the beginning of the thyroid feeding) the total metabolism also increased. In each of three hours before the administration of the morphin 880 mg. 02, on the twelfth day of morphinization 779 mg., after three days' thyroid feeding plus morphin 813, mg. On the basis of per kilo and hour the result on 22 g. loss in weight would naturally be considerably greater."
Hildebrandt also studied the sensitiveness of rats chronically treated with morphin to 02 deficiency, which he describes as follows:
"From the experiments of the Asher school, it was found that thyroid-fed rats showed a greatly increased sensitiveness to 02 deficiency, those without thyroid glands, on the other hand, bore the 0, deficiency comparatively well. If rats chronically treated with morphin behave as thyroidectomized animals, then a further support is obtained. The order of experiments was the same as that used by Rippstein. Two rats—one thyroidectomized or treated with morphin and one normal—were placed under a bell-jar and the air slowly was exhausted. In order to eliminate a subjective error one of the animals was always identified by a piece of ribbon; judgment as to symptoms was left to neutral observers who did not know what the ribbon signified. The findings of Asher were completely confirmed. The thyroid-fed animals died on merely one pressure while the normal showed comparatively light symptoms. On the other hand the thyroidectomized animals differed considerably from the normal. The final state on a pressure of 350 to 300 mm. Hg. was uniformly characteristic. On higher pressures during the first five minutes of the experiment the behavior of the animals often varied. More often they sat there apparently exhausted only shortly to run around again in lively manner trying to escape. On the other hand in the lower pressures the difference between the normal and thyroidectomized or morphinized animals was not noticeable.
"The following brief protocol serves as an illustration:
July 1 morphin rat weight 143 g. Pressure Normal rat weight 160 g.
On June 18 immunization began.
Daily injections of 80 mg. No injection on the day of observation.
Dyspnoea 450 Dyspnoea
Dyspnoea—sits in normal position 380 Very strong dyspnoea
Spontaneous stimulation still No ataxia Lies flat on its stomach
Complete recovery 330 Ataxic
305 Labored breathing, moribund Pressure to normal
Spasms then gradual recovery
"Two further experiments on morphinized and normal rats had the same results. "In relation to their sensitiveness to 0, deficiency therefore the rats treated chronically with morphin and the thyroidectomized rats behaved similarly."
Hildebrandt concludes as follows:
"A series of analogies have been obtained as to metabolism of thyroidectomized rats and rats treated chronically with morphin:—a decrease in the metabolism, higher respiratory quotient which in both cases could be explained with greater probability by a primary increase in the absorption of carbohydrates, a further decrease in the high respiratory quotient upon thyroid feeding and less sensitiveness toward 0, deficiency.
"Evidently the same mechanism is involved. But as long as we do not know in what way individually the thyroid gland and thyroid deficiency affect the metabolism we cannot say how the parallelism operates.
"Whether there is a further similarity between the effect of thyroid deficiency and that of chronic morphin supply or whether we may assume that the action of the morphin influences metabolism in spite of the thyroid—in a sense a restraining of its function—remains to be seen."
F. A. Loofs-1922.87
"Since it has been proved through the different investigations (Cloetta et al.) that it is not a question of immunity in the sense of Ehrlich's side-chain theory, the question naturally arises: What chemical constituent of the cell has the ability to bind the morphin through an affinity of the molecule for alkaloids and other similar bodies? Then the toxicity could be explained by the binding of the morphin, if it takes place within the cell, the disappearance of the toxicity (and also the morphin disturbance) could be explained by the breaking away of this substance attached to. the morphin from the cell and the protective effect by the distribution of this substance in the blood before the effect on the sensitive cells. An increased protective effect in addiction could then be explained by the increased appearance of this substance naturally `related' to the morphin.
"Such a cell constituent actually exists. This is lecithin. Lecithin contains in the molecule a base which is closely related to the alkaloids and is relatively easily split up, cholin. On the basis of the'fact that in the breaking-down process in the brain, especially in epilepsy, cholin appears in the medulla oblongata fluid (according to Hoppe-Seyler, 8th edition, page 204) and on the basis of the general conception of the cell metabolism, we must assume that the lecithin molecule is in a state of alternating formation and breaking up of the cholin; that therefore there is a certain lability in the connection between distearylglycerinphosphorous acid portion on the one hand and the cholin on the other. The morphin molecule can appear in this labile state and according to the degree of its affinity replace the cholin. Chemically, as my Herr Geheimrat Paal confirmed in personal discussion, there is sufficient probability for this statement. Cholin and morphin are both basic alcohols. A decision as to this possibility could be brought about only from experiment. I have undertaken investigations along these lines."
"A further support for this hypothesis may be found in the fact that a large part of the withdrawal phenomena may be explained by the inundation of the organism with cholin crowded out from its natural relationships, and a further
portion of the symptom-complex may be explained by the impoverishment of the cell in lecithin according to which we can easily understand the characteristic loss of general tonus. Cholin, toxic in large amounts, pharmacologically belongs to the muscarin group. A pseudomuscarin is formed from the cholin. It is further closely related to the far more poisonous neurin which is repeatedly detected in metabolism as a splitting-off product of cholin. The toxic effects of cholin are as follows: salivation, stimulation of the sympathetic (vascular disturbances) ; further, stimulation, of the intestinal vagus (diarrhea, vomiting, meteorism) ; and above all motor stimulation. In addition there is a specific affinity of the cholin for the outer skin which plays such an important rôle in the withdrawal toxicosis of morphinism (Ellinger, Minch. med. Wochenschr. 1914. p. 2336).
"On the basis of this hypothesis the picture of morphin addiction may be described as follows: The morphin which is administered for the first time is taken up in the lecithin molecule according to its affinity quota (cholin/morphin in proportion to the distearylglycerinphosphorous acid). This causes at first a disturbance in the cell equilibrium and pharmacologic action. The cell equilibrium is again obtained by the throwing off of the displaced cholin. If nothing more than this single dose is administered very soon the morphin is eliminated by the appearance of a fresh supply of the cholin (with or without alteration of the molecule). If in the meantime the discomfort appearing with the disturbed cell equilibrium leads to renewed administration of morphin, then a new part of the lecithin molecule is taken pp with morphin instead of cholin. Since one
part of the molecule is taken up with morphin, the possibility of a pharmacologic action of the morphin is thus lessened. This diminishing of the possible action increases with each time and is the origin of the addiction. The limit of the possible action is the complete taking up of the distearylglycerinphosphorous acid radical with morphin corresponding to the affinity quota. This is the point at which even the increased amount of administered morphin produces no
further effect. Rehabilitation in withdrawal follows upon the gradual replacement of the morphin by `normal' cholin. If this does not follow (lack of the supply of cholin), and if there is no supply of morphin due to withdrawal then there probably takes place continued breaking-up of the lecithin molecule. Corresponding to this the stage of acute withdrawal symptoms (the first 48 hours) may be considered as cholin poisoning and the second stage as severe cell injury through the breaking-up of the lecithin molecule. In the first stage the symptoms of a poisoning prevail, in the second stage those of a severe atony (loss of cell tonus due to lack of lecithin).
"On the basis of this hypothesis we should expect to obtain the following findings:
"1. Increase of cholin in the blood and in the excreta during morphin addiction. This is true especially in the first two days of withdrawal.
"2. Increase of glycerinphosphorous acid in the blood and the excreta in the second chronic stage of withdrawal.
"3. Therapeutic action of measurable cholin doses in the second stage of withdrawal.
"4. Pharmacologic inactivity of the distearylglycerinphosphorous acid ester of morphin.
"5. Determination of substitution products of morphin, which result from the binding of the morphin with parts of the lecithin molecule during addiction to morphin. Such a binding explains the attenuation of the toxicity of the morphin getting into the excreta and on the other hand its absence in the usual morphin test.
"It is quite conceivable that my investigation now in progress will lead to entirely different results. There is, however, no reason for not advancing beforehand a plausible working hypothesis. The Ehrlich side-chain theory for the most part has failed. The Wassermann reaction, however, is still at hand. It would be rather egotistical too for me to settle these ideas before experimental demonstration. For my part I am convinced that indications point in this or a similar direction and I should like to make sure of priority, especially as there is a long distance between the idea and proof."
Ernst Join-1923.88
The author approaches his subject from the general biologic angle of adaptation of the organism which he says is an active transformation of the original conditiôn in response to stimuli. Such an adaptation to repeated stimuli differs essentially from regulation or reaction of a temporary character. A morphological example is that of cardiac hyperplasia resulting from the repeated demands of physical exercise in contradistinction to the acceleration of the pulse and raised bloodpressure—regulation—resulting from an occasional demand on the organ. Such muscular adaptation—hypertrophy—always involves the repeated application of an unaccustomed stimulus. The same is true with functional adaptation where "each separate stimulus, whether it be food, a hormone, or a toxin, is answered by a reaction, whose general purpose is to restore the body, after a few undulations, to that uniformity in carrying on its manifold activities which seems to be an indispensable biological condition." From such stimulus and reaction the organism emerges in its normal state, but with unusual, injurious, or especially unphysiologic stimuli a qualitative or quantitative reaction of a different sort may be induced,—an acquired condition which we call addiction. Here the stimulative action takes the form of a limited injury to the organism or to some organ, in a narrow sense an analogue of morphologic adaptation. Examples of this are adaptation to temperature, rays of light, degrees of humidity, dietary changes, etc. and prolonged addiction results in hardening, acclimatization, etc., etc.
The author carries the idea further as follows:
"When there is a continual, unwonted stimulation from a chemical source, therefore from a poison, gradually, if there exists a possibility of efficiency in the single stimuli, which generally are less hurtful, an increased tolerance comes about,—a relative acquired resistance to the poison.
"This ability to resist the poison may be gained in numerous ways, by diminishing the sensitiveness and so dulling it—a doubtful idea so long as we are ignorant of its mechanism; or by detoxicating the body, whether the poison be rendered ineffective through removal, through incarceration, or through combination, whether it be rapidly removed by intensive elimination, or less of it admitted to the circulation, in case of oral administration, by reason of restricted absorption."
"If, in the course of clinical or experimental observation, the excretion of the poison diminishes in proportion to a constant increase in tolerance, the suspicion is aroused that it has been decomposed or transformed in the body, but this is not certain—it might always be brought about by diminished sensitiveness—so long as the blood and tissues have not been actually proved free from poison.
"If the amount of poison excreted in a given time increases along with increasing tolerance, there is less reason to think of decomposition or hyposensitiveness as the cause of tolerance, but of accelerated elimination rather or constantly diminished absorption, depending on whether the urinary or the fecal contingent increased during oral administration."
As an illustration the author refers to Cloetta's work on addiction of animals to arsenic, in which it was shown that there was a "local, intestinal immunity dependent on refusal to absorb."
The author continues:
"The mechanism of addiction is often found to be quite complicated. Frequently no satisfactory balance exists between intake, outgo, and residue in the body, and, as a criterion as to whether increasing hyposensitiveness is the cause of addiction, the question often arises whether the amount of poison in the body circulates without being active or whether the poison is active so long as it remains in the body.
"It was a remarkable advance when Faust showed that dogs, which soon were without the initial symptoms through receiving a daily subcutaneous injection of about two centigrams of morphin per kilogram, causing at first an amount of sixty per cent of the drug to be excreted in the feces, decreased gradually to an amount constantly smaller and then ceased entirely. At that time the organs contained no morphin, so that Faust conjectured intravital destruction. This possible destruction did not appear to later investigators an altogether satisfactory condition of addiction. In the first place it appeared that sufficient amounts of a well-dissolved poison might circulate without causing symptoms of a toxic character (Rübsamen); so then addiction to a poison need not be universal. A dog successfully addicted to large doses of morphin, who responded to twenty-three centigrams per kilogram without narcosis or vomiting or glycosuria (Luzzatto), once more acquired bradycardia on one milligram per kilogram, just before addiction. Thus the vagus centre constitutes a very delicate indicator for the circulation of effective amounts (Eginond). In this the succession in which the various centres and organs of the dog fall under addiction to morphin does not correspond precisely with that in unaccustomed animals (van Dongen). We find it quite the sanie in the case of heroin, whose spastic properties still remain irritant to dogs in spite of long addiction and of decomposition of a large share of the poison (Langer). According to Gunn and Heathcote the lethal dose of strophanthin for rats is thirty times as large as for rabbits, but the erythrocytes of both animals yield in the same way to strophanthin hemolysis. During strophanthin addiction cats manifest no sort of correspondence between the symptoms in the nervous system and those of the circulatory apparatus (Klein).
"All these instances teach us two things. First: although pronounced addiction may have taken place, any portion whatever of the organism may remain unaffected, may still react, may show sensitiveness. There exists, therefore, a specific response to addiction in the system, in the organ, in function. And in the second place: while, as in the vagus centres of morphin addicted dogs, there still remain tracts that are sensitive. These indications furnish pharmacological evidence that in these instances not decomposition of the poison, or at least not decomposition alone, lies at the root of addiction, but beside that, its ineffectiveness.
"Let us consider these two phenomena from the standpoint of clinical experience.
"Should the decomposition of the poison. prove to have been effected in addiction to the fullest extent, the large amounts of morphin required by the addict would work an injury rather to his economy than to his health. He must simply expect a certain percentage of morphin to be decomposed at once and so to have no effect on him, and must take more at the beginning by way of compensation. But experience teaches something more, namely the effectiveness of small doses even in confirmed addicts, but—and this is decisive—these doses have a brief duration of effect.
"In a morphin addict briefly observed by me it was very impressive to see that, when during a few hours' intercourse his speech every now and then grew weak and his bodily strength failed visibly, doses of one or two centigrams stimulated him again for an hour or so. So this amount of poison is exhausted sooner than normally, but it is still effective in the customary dosage.
"The second fact, that of selective, dissociated addiction, of the increased tolerance of special organs, is calculated to serve as a connecting link between addiction and .chronic poisoning.
"If mankind were universally addicted to a poison—in which event it would be perpetual—that would be a very remarkable, but a purely biological phenomenon without specifically medical interest. The medical interest lies in the fact of the man accustomed to a poison becoming sick. He is sick because the poison taken habitually, while it fixes certain cells and confers on them increased activity or passivity, also renders these or other cells unserviceable for other functions, non-resistant to other influences. The drunkard dies of cerebral alcohol poisoning no more readily than the unaccustomed man who takes the same amount, but he dies in his liver, which has become diseased in the service of other organs.
"His brain has become addicted, but not his liver. The morphinist has acquired a high tolerance in certain regions of the brain, but his cortical cells have not shared in the poison to such an extent that they have preserved their energy undiminished.
"Thus addiction is not clinically universal, but specific, restricted to certain organs or cells or merely to certain cell activities. Adaptation to an unphysiological stimulus is pathological, addiction is the disease. The unaccustomed man who reacts by an acute illness to the drinking of a quart of beer thereby demonstrates his possession of pristine health. The habitual drinker, who remains free from morbid symptoms on enormous amounts, thereby advertises his ill-health.
"Here arises a kindred question, namely, whether bodies immunized by having overcome infection and which likewise react to a disease differently from those unaffected, are therefore less healthy than these. The answer to this question depends, generally speaking, on how we define health in the narrow sense, whether and with how permanent injury the acquisition of immunity was attended.
"If addiction is affected by the poison chiefly in special organs, this resistance, when it consists in blunting, is not strong in relation to poison encountered. The alcoholic is not alone fortified against alcohol, the morphin addict against morphin.
"One of my patients, who was notably excited during morphin withdrawal and wanted to leave the institution, toward evening received eighty centigrams of luminal together with half a milligram of scopolamin. When I visited him two hours later he had arisen in order to urge upon me the impossibility of his remaining longer.
"The great susceptibility of the alcoholic to narcotization is a frequent experience and, since the brain consumes much of the narcotic and the heart tolerates little, illustrates excellently the fact of selective addiction "
After discussing addiction to nicotin and alcohol as evidenced by clinical observations and studies on animals, the author continues:
"If it is true that the tolerance arising from blunting of organic activity is not strongly specific for the poison tolerated, but that the increased tolerance is that which arises from chemical changes in the poison in the body, we can understand how this implies a special structure in the poison, a special atomic group as its object.
"So then the phenylhydroxyl group in the case of morphin is the object of the decomposition which we must regard as an accompaniment of addiction. Retention in a methyl group, as in codein, or in an ethyl group, as in dionin, interferes with decomposition and addiction (Bouma), with the latter naturally only so far as it depends on decomposition. But in case the phenylhydroxyl and alcohol-hydroxyl are acetylized, so that diacetylmorphin (heroin) is formed, it is well understood that the acetyl group is very easily broken up, allowing the effect of morphin to take place. And thus—the point of real importance—the body learns to break up this acetyl group, while with a single dose the greater part of the heroin appears unchanged in the urine, a smaller part in the feces (Langer). Babel showed that the organic substance of animals addicted to morphin is capable of decomposing heroin to a given extent, but not codein—an extension of Bouma's result. Double hydration of morphin to paracodin has a similar effect to acetylization. The product does not clinically cause codeinism. (A. Frankel) nor dioninism (Scherer), but, and this in animal experiments too, heroinism, paracodinism, eucodalism, dicodinism (Kiinig, Alexander, Biberfield, Hecht).
"It may be remarked as a corollary that the spastic poison, harmalin (from wild rue), seems to possess a very similar mechanical action in addiction to that of morphin (Flury), a fact the more noticeable because addiction to spastic poisons in the narrow sense is met much less frequently than that to narcotics, where, as, for instance, in the case of papaverin, addiction through increasing decomposition of the alkaloid is nothing unusual (Zahn).
"Regarding the location where morphin is broken down little is known. It is assured that the liver takes à foremost part here. This being so, several points of connection are revealed between addiction and the manner of application. Quite rightly those who take morphin by mouth generally are considered to offer a better prognosis than those who use it by injection."
The author then reviews the work of a number of investigators on addiction to quinin, atropin, phenylhydrazin, and pyrodin. Continuing he says:
"The proper estimation, not only of the mechanism, but of the actual state ,f addiction is a complicated matter when it involves the poisons of human indulgence, those which cause marked increase of pleasure and chiefly affect the nervous system, although arsenism in human beings and less frequently digitalism are included (Balz, Schubert). (Corresponding reports of animal experiments by Cloetta and Klein).
"As an example of the abuse of cocain in gratification, the difficulties may especially be illustrated which stand in the way of interpreting the central nervous effects of the poison, and so certain general points of observation may be won. The assertion frequently made of human addiction to cocain appears to depend upon confusion of the readily distinguishable conceptions of pharmacological tolerance and of psychic accustoming or passionate addiction. But recognition of this psychological condition does not furnish proof of actually acquired relative tolerance for the poison. As shown by experiments carried on together with Friinkel, even the large doses of cocain addicts and their attainment by gradual increase are not alone sufficient to explain this, for idiosyncrasy in many persons tallies with remarkable natural tolerance in others, and the increased use is explainable as a gradual stumbling onward, an increasing confidence in the poison and an augmenting inclination to reproduce its effect. Clinical tolerance should not be spoken of except where the statement specifically accompanies it that the initial dose had become incapable after a period of producing the cocain effect, that its effective period had perceptibly diminished—statements which have never been made to us, The fact is important in the light of these remarks that the cocain user, after a voluntary or compulsory interval of six or eight months without cocain, can resume without harm the same dose at which he discontinued before the hiatus. In morphinists, who begin anew so to speak on every reversion, this is inconceivable. In their case abstinence is sufficient, even a reduction for some days or a few weeks suffices to restore in large measure their sensitiveness to the poison; we have often even received the impression that the morphin addict, before returning to normal sensitiveness toward his poison, must pass through a stage of hypersensitiveness, a question which may perhaps find a clearer answer in animal experiments, because in human beings psychic influences always interfere.
"With the cocain addict it is different. After an intermission he must return to his large dose, a circumstance that stands in complete agreement with the results of animal experiments, where likewise no sort of addiction is produced, but frequently a sensitization (Ehrlich, Grode, Levy).
"A number of facts point directly to the absence of true tolerance. Together with Frantz I have studied the bodily phenomena after injection under uniform conditions of five centigrams of cocain into a large number of normal individuals and of cocain users, and thus have found that less can be said of general sensitiveness and insensitiveness to cocain in individuals than of a sensitiveness occasionally prevailing in certain organs or organic systems, and that cocain users complain, just as normal subjects do, sometimes of tachycardia in particular, sometimes of high blood-pressure, sometimes of tachypnea, tremor, and so on. The possible objection that in cocain users the phenomena of addiction belong less in the somatic field than in the psychic I might refute with Frankel by saying that cocain users who have devoted themselves passionately to the drug for years have sometimes been known to react to small, by no means, large doses of a pure preparation with the severest hallucinatory excitation, just as an unaccustomed person when poisoned medicinally necessarily undergoes the same psychic alterations.
"Although, therefore, in contrast with morphin, we consider a tolerance to cocain in the pharmacological sense as unproved, we are compelled to recognize explicitly the fact of a passionate addiction, which is often seen, and this leads us to a short discussion of the relations existing between psychic addiction and pharmacological tolerance. The foundation of abuse of a poison almost always produces either a physical or a psychic defect. In the former case the poison signifies, as for morphin, relief of pain, or as for heroin, cessation of dyspnea. The psychic defect is the same, and is felt as a torturing insufficiency and compensation sought in the habitual use of a poison in the endeavor to complete the personality by means of that poison. An accidental acquaintance with a pleasurable poison—sometimes on occasion of a war wound, a gallstone attack, an attack of hay fever—leads to subjection and permanent addiction. In the case of other toxicomaniacs the anamnesis can be traced as, without any physical determinant from without, they have tried the abuse of a poison and been pursued by it, and so have gone on from nicotin to alcohol, to morphin, to cocain, to heroin. When the habit of indulgence in a poison has fastened on an individual so that he has become a pharmacological addict in the sense above-defined, the situation becomes complicated for him as a toxicomaniac in that the poison which physical conditions compel him to use constantly becomes less effective, his dose must be increased, the danger of poisoning continually is augmented, but to discard the poison adds to the initial psychical symptoms of craving those of abstinence, which arises legitimately from abuse of the poison itself.
"Very certainly it is the symptoms of abstinence which characterize addiction, at least in every instance where the body cells have opportunity to react to the poison. (In case of arsenic, where addiction takes the form of progressive diminution of absorption, the deficiency symptoms do not appear.) That the addict tolerates ten or a hundred times his initial dose is therefore only one feature of addiction; that he requires it reduces to a very small value what at first was regarded as an acquisition, even marks addiction as pathological and distinguishes it from the natural immunity to poison. The severity of the symptoms of abstinence appears to be the converse of the degree of addiction and of the pleasure received from the poison. One of our morphin addicts wrote in his personal report :—`at the close of these two years the withdrawal treatment has accumulated and repaid in horror all that it has afforded of euphoria.' The resultant manifestations will be more or less characteristic according to the special effects of the drug. Addiction to veronal, for instance, will be followed by pertinacious insomnia, addiction to morphin, which, especially in neuropaths, has an indirect tonic effect from excluding inhibitions, by stimulating nearly all the outward vital activities, in case of heroin going so far as symptoms of abstinence in opposition to its principal effect, especially in dyspnea (Manguat,. Duhem).
"Suppression of administration, therefore, acts like a powerful specific poison, withdrawal, as Kobert says, resembles an intoxication. The symptoms of abstinence certainly justify the popular expression of the `second nature' of an addict, and call for recognition of the state of addiction as the establishment of a new equipoise.
"In discussing the concept and the diagnosis of the phenomena of abstinence, it should be said here that naturally it is an error to regard every complaint appearing during the period of poison hunger as a symptom of disease. In the first place, desire for the production of a euphoric state of mind is as far from being an abstinence symptom as is the wish for any other gratification formerly experienced. Thus the direct effects of the last dose of poison are to be left out of consideration, if, for instance, gastric disturbance following acute alcohol poisoning is not to be regarded as other than a symptom of abstinence. The same holds true for all forms of physical manifestation of chronic poisoning which appear unconcealed and unchecked during abstinence. Abstinence has to do with the perception of these manifestations, but is not their cause. Finally, the status quo ante must always be taken account of. When an asthenic person is tonically improved by use of arsenic, the annoyances attending discontinuance of the arsenic are not abstinence symptoms, but merely the return of the former condition after using the drug. This holds still more true for the cerebral poisons in psychasthenics, for instance in cocain users.
"The participation of psychic influences in addiction and withdrawal is sometimes overestimated from the medical standpoint, when, for instance, substitute injections are given in place of morphin. The direct quieting effect of such mystification is self-explanatory. Nevertheless only such morphin addicts can be misled longer than a few minutes as are beginners, dilletanti they might be called, in their poison. The true toxicomaniac quickly notes the fraud, but—and this is the point—not because his mental capacity is so great, but because the body cells concerned have acquired such a preeminent power of discrimination, as is proved by a reversal of the procedure.
"The morphin addict, Z., who was suffering intensely on the second day of withdrawal, received two centigrams of morphin under the pretence that it was an injection of another kind. He continued to complain, begged for an injection of morphin, and soon fell asleep lamenting constantly that his morphin should be given him.
"Here let me say a few words about withdrawal. Strictly speaking, withdrawal is disuse where an actual condition of addiction has preceded. Biologically considered, the problem necessarily consists in restoring sensitiveness for the poison in question. It may be asked whether return of sensitiveness could be promoted by special measures, by changes in the organism, by production perhaps of nonspecific stimulation. The possibility of such reactionary changes is shown by the studies of Freund and Gottlieb. Biberfeld produced brief interruptions of morphin addiction in dogs by blood-letting and parenteral protein injections. From the clinical aspect Beringer reports withdrawal of morphin as abridged and facilitated by oral administration of protein. It might seem to us as though the essential factor of withdrawal is that of time, and that during this period the patient stands most in need of psychic treatment. The question of rapid or gradual withdrawal cannot be determined in advance by rule. An important factor must be given foremost consideration in settling it, concerning which Levinstein, the originator of the rapid form of treatment, argues that in the gradual process the finally successful withdrawal of the last doses causes but few less symptoms than cutting off the entire dose by a sudden withdrawal. Experiments with a view to bringing about abandonment by means of specific antisera have all proved disappointing. In this field there is a radical difference between substances without and with the character of antigens (Lewin, Morgenroth).
"All phenomena of adaptation ought occasionally and if only by way of imagination to be viewed from the standpoint of teleology. We may ask whether the phenomena of addiction discussed here have anything to do with design, when by design we understand the total of the forces directed to the preservation and the ordered conduct of life. We see at once that this biological view of design does not harmonize with a strictly clinical one. It is undoubtedly clinically unintentional when a soporific, a laxative, a febrifuge, or whatever may be no longer proved effective in the original dose: but all these remedies are poisons to the organism as a whole and it stands on the defensive against them. The body misunderstands our therapeutic aim, if it may be so expressed, and in many cases circumvents it by rendering such increased dosage necessary because of partial detoxication or hyposensitiveness as is no longer practicable on account of the toxic effects. The general purpose of life is plainly directed in this respect to the object of maintaining health, even though it be by destructive means. Here another and compensatory principle may at any time enter, the principle of selective distribution of drugs, according to which the cells, which Virchow has shown discharge normally the function of autonomous nutrition, in disease possess themselves of the greater part of the medicament, a process characterized by Jacoby as a new basal law of pharmacology. Jacoby instances the fact that in joint disease a quantity of salicylic acid goes to the joints which in health would flow to the central nervous system. `So the sick are less subject to poisoning than normal individuals.' Protection against poisoning by means of pathologically altered organotropy is manifest once more in the well-known fact that hypnotics are tolerated by patients in states of agitation in far larger amounts than normal.
In animal experiments Gensler found larger amounts of the hypnotic, neuronal, in the brain in artificially produced states of excitation than in the controls. The state of agitation is therefore to be regarded as functionally the antagonist of the hypnotic, and through it—the reverse of the above instance—the brain is able to guard the other organs against poisoning. It is possible at any rate that the fact, not studied systematically, but frequently observed empirically, of tolerance raised in advance on the part of many patients to `their' drugs (arsenic, for instance, in anemia, chorea, pemphigus), is connected with such pathological selection as to paralyze, at least partially, those consequences of addiction which are unfavorable to therapy."
O. Wuth-1923.89
From clinical observations and experimental studies, Wuth developed an hypothesis as to the origin of the withdrawal symptoms. He was impressed with the similarity between the symptoms of morphinism and those of hypothyroidism and the symptoms of morphin withdrawal and those of hyperthyroidism and states that "in morphinism it is a question primarily of disturbances in the vegetative nervous system in addiction and withdrawal, of such a kind that in addiction the parasympathetic tonus seems to be increased and in withdrawal the sympathetic."
The author further concludes that the thyroid gland plays an important rôle in the pathology of morphinism and that the action on this gland seems to be produced through the central nervous system. After covering the symptoms during addiction and withdrawal the author continues as follows:
"If first we consider these symptoms we are impressed at once with the fact that in general they are conditioned by a tonus variation of the vegetative nervous system. A second evident point is the similarity between certain of these symptoms and those in conditions where the thyroid gland had been disturbed. A number of symptoms of addiction show a similarity to those in hypothyroidism while many of the phenomena in withdrawal offer a striking similarity to the symptoms in thyrotoxic diseases. Thus there is the dryness of the pale, cold skin, the trophic disturbance of the hair, teeth and nails, constipation, impotence, slow heart action, lower blood pressure, and in many respects the variations in the psychical behavior—all symptoms which we observe also in hypothyroidism. Still more suggestive are the symptoms of the withdrawal period to those of the picture in thyrotoxic conditions; here as there we may observe the warm skin with profuse perspiration, dilated pupils, diarrhoea, palpitation of the heart, tremors and psychomotor stimulation.* A few of the more unusual symptoms appearing during withdrawal as well as in hyperthyroidism are: hemorrhage of the mucous membrane, disturbance of accommodation, double vision, disturbance in walking, muscular pains, pains in the joints, albuminuria, glycosuria, increase in temperature ("Intermittens der morphinsucht," Levinstein).
"Therefore obviously we are concerned with vegetative neurotic disturbances which show a certain similarity to disturbances which may be attributable to hyper- or hypothyroidism. We must now, according to the facts, determine what supports this purely clinically observed hypothesis in respect to the roles played by the vegetative nervous system and the system of blood glands in the pathology of morphinism.
"First as to the pharmacodynamic action of morphin we may see that there is a central hypalgetic effect, that it influences the cerebral cortex, the cough and respiratory centers,'the swallowing and vomiting centers and the vasomotor and heat regulating centers. Of the further known effects of morphin there is the contraction of the pupils, the slowing of the heart action, the bladder spasms as a result of the increased tonus of the vagus. Also the increased secretion of the gastric juices after the administration of the morphin causes a stimulation of the vagus as it is checked by atropin. The sympathetic salivation is checked by morphin. Therefore in general morphin acts as a parasympathetic stimulation, and a sympathetic check, but still there are exceptions. Morphin lessens the excitability of the vagus terminating in the intestine and increases the spinal tonus of the nervus splanchnicus. It cannot be asserted that morphin acts electively on the sympathetic or parasympathetic system. At least we may with apparent justification draw upon the results of pharmacologic investigation as to the facts that morphin has a definite effect upon the vegetative nervous system and that in general the action stimulates the parasympathetic and checks the sympathetic without meantime falling into the old error of the antithesis of the pharmacologic susceptibility of both of these systems. We should not omit reference to the fact that it is a question not only of pharmacologic analysis but also of investigation on the subject of addiction. For example it is known that the secretion of gastric juice is increased on the administration of morphin, it is checked on the chronic abuse of morphin and in the withdrawal period it is again Increased. Further it should be noted that in all patients we do not find the above described symptoms by any means. Also in the withdrawal period unusual individual differences may be noted. Just as different kinds of animals so also individuals show entirely different behavior toward morphin; in many the morphin has only a stimulating action. It would be interesting to investigate the question as to whether or not this different behavior is conditioned perhaps by the whole vegetative-endocrine organization."
The author then reviews certain experimental work dealing with the interrelationship of thryroid action and morphin effect, quoting the work of Hunt, Gottlieb, Hildebrandt, Boeck, and also the work of Guber and Valenti, which he states point to the fact that the thyroid gland plays an important part in the pathology of morphinism. He continues:
"Still the question may arise as to whether we should consider the action on the thyroid as a direct one or whether there is an influence on the vegetative centers. The question is extremely difficult and can be decided from a purely clinical-empirical basis. The pharmacologic effects as they are so far known of morphinism (effect on the cough and respiratory center, swallowing and vomiting centers, vasomotor and heat regulating centers, reduction of oxidation, Leake) indicate a central action. The significance of the thyrotoxic and sympatheticotonic symptoms, insofar as the related experiments are not contrary to this conception may be applicable here only to the neurogenic, post-traumatic Basedow, to diabetes insipidus after central organ sickness, to fear hyperglykemia and especially to the central nervous sensitiveness of the function of the thyroid with internal secretion. If we follow the above hypothesis we have to consider morphinism somewhat as follows: For physical, psychical or vegetative neurotic disturbances a dose of morphin is administered. The morphin has a numbing effect on the function of the thyroid and the related nerves and humoral organs (sympathetic, adrenal system). If the organism shows a tendency to recover again its endocrine vegetative balance it compensates. Accordingly it became necessary, in order to obtain the same action on repeated administration, i.e., to return the vegetative endocrine tonus again to the most desirable level, to reduce the tonus increase produced by the effort of the organism to balance itself. In other words—a larger dose of morphin is necessary to produce the same action. This condition forms one of the factors of addiction. Another may be found in the relatively reduced effect of the poison. From this we may recall the above experimentally determined fact that in thyroid deficient animals there is a lessened sensitiveness toward morphin and since the function of the thyroid is reduced in a certain sense by the administration of morphin, the sensitiveness to the poison is also reduced. If we proceed thus to a plausible explanation of a few of the important factors of the disease, of the `morphin hunger' and of addiction, we may be able to explain a series of clinical facts on the basis of this hypothesis. Among the early ones it is known that morphin, as Levinstein says, produces the same symptoms which it also attacks. And perhaps here we have one of the principal factors for the disease. We know that strict psychopaths complain of numerous vegetative neurotic symptoms and certainly these individuals form the majority of morphinists, certainly because these vegetative neurotic symptoms are attacked especially well by morphin. A clinical fact may also be explained by this hypothesis: our therapeutic ignorance in relation to the symptoms of withdrawal which, so to speak, is comparable to the lack of suitable treatment for Basedow's disease with its sympathetic and parasympathetic symptoms of irritation. What we lack is a drug which reduces the parasympathetic symptoms not only as atropin controls the individual symptoms (perspiration, diarrhoea, vomiting) but as a paralyzant on the endocrine vegetative tonus, i.e., sympathetic. I should like to state that perhaps the sketched hypothesis will lead to the further observation and analysis of the individual symptoms in morphinists, in place of considering them unavoidable complaints as well as the refusal in the future to be resigned to the lack of suitable therapeutic measures but rather undertake studies suited to the individuality of the case with drugs of the alkaloid series and products of inner secretion. In conclusion I should like to remark that this hypothesis in no way will explain the whole problem of morphinism but only a few of the important factors which perhaps also in other diseases—cocaine, alcohol,*—play an important role."
Sir W. H. Willcox-1923.90
"That the condition is caused by morphine and its allies is well known, and the symptomatology is well recognized as a definite symptom-complex. The explanation of why withdrawal symptoms occur is yet to be worked out. American observers, foremost amongst whom is Dr. E. S. Bishop, assert that the taking of morphine leads to the formation of an antidotal substance in the body, which neutralizes the large amounts taken by the addict. It is asserted that this antidotal substance is itself very toxic, and that it continues to be produced in the body if the drug is discontinued. At this stage withdrawal symptoms develop and they are only relieved by a further dose of the drug, which acts by neutralizing the toxic antidotal substance.
"This theory, fascinating as it seems in the ready explanation of the production of withdrawal symptoms, has not yet received adequate experimental confirmation. Professor W. E. Dixon, in an address on the drug habit (British Medical Journal, November 19th, 1921), states that neither morphine nor any other drug causes antibody formation. On the other hand, Valenti rendered dogs tolerant to morphine and found that on suddenly stopping the drug typical withdrawal symptoms occurred. He alleged that injection of the serum from dogs showing withdrawal symptoms caused similar symptoms to develop in normal dogs.
"Professor Dixon suggests as an explanation of withdrawal symptoms that nerve cells, after prolonged narcosis, become on reawakening hyperexcitable, and that a further dose of drug is necessary to allay this condition. The fact that increasing quantities of morphine and cocaine are required by addicts can be accounted for by the increased power of destroying these drugs which is developed by the tissues of the addict.
"Another explanation of addiction disease which, I think, should be the subject of pathological research, is the probability that definite changes of a degenerative type occur in the nerve cells of the brain, and that this pathological change leads to the formation of abnormal channels of transmission of nerve impulses, whereby abnormal physical and mental effects are produced. It is well known that toxic substances, such as chloroform, affect nerve cells, causing degenerative changes, demonstrable by Nissl's methods of staining, and it seems likely that similar changes may occur in drug addiction. This view of the subject offers an explanation of the incurable nature of drug addiction in patients who have taken large quantities of morphine, heroin, or cocaine for many years.
"Scientific research is sorely needed on the pathology of drug addiction, and there are hopeful signs of light being thrown on the subject in the near future, since special investigations are already in progress.
"The Ministry of Health has recently appointed a committee to inquire into the substitutes for cocaine and the possibility of drug addiction arising therefrom. It is hoped that valuable information may be forthcoming from this inquiry which will throw some light on the pathology of drug addiction."
J. A. Gunn-:--1923."
This author contributes a comprehensive review of the literature on tolerance to non-protein substances. In an introduction he states:
"It is now well known that, when acquired immunity is induced in warm-blooded animals to toxins, bacteria, or indeed to any protein substance, this immunity is accompanied by, and at least partly due to, the formation of specific antibodies in the blood or tissue fluids. No such antibodies are formed to nonprotein substances, though to some of the latter a high degree of immunity can be acquired. This fundamental distinction has been emphasized by the retention of the word `immunity' as applied to proteins, and by the restricted use of the word `tolerance' as applied to non-protein substances. While this difference in nomenclature is convenient and in part salutary, there is a danger that the distinction may overleap itself and fall on the other side; and this for two reasons. In the first place it has tended often to lead to a tacit and unjustifiable implication that the processes whereby an animal acquires tolerance to nonprotein substances do not occur in immunity to proteins; and, secondly, the distinction does not hold good for congenital immunity, because there is no doubt that congenital immunity both to protein and non-protein substances is in many, and possibly in most, cases due to an insusceptibility of the cells themselves to the toxic action of the substance, and independent of any antagonistic effect of the body fluids.
"While, therefore, it will be possible in the space of this review to deal only with tolerance to non-protein substances, the object of it is a twofold one. The subject of tolerance to drugs possesses its own interest and importance, but any considerable review of the whole subject has not to my knowledge been attempted since that by Hausmann in the Ergebnisse der Physiologie in 1907. This résumé deals largely with investigations subsequent to that date, and in the necessary selection of material I have chosen rather to consider in some detail only those instances of tolerance which have received some explanatory investigation, than to attempt to mention every known instance of tolerance. The primary object of this review is therefore to give a general survey, from a scattered literature, of the present state of knowledge of tolerance to drugs. But, in addition, it may serve a purpose of providing a brief statement of the methods, other than by antibody formation or phagocytosis (neither of which has suffered from lack of attention) whereby an organism can acquire immunity, for it is conceivable that even in the case of genuine "immunity" these methods of defense will be found to play a more important part than has hitherto been realized. In any case perhaps this introduction will help tô justify the title of the article, for it will be seen that tolerance to drugs is dependent mainly upon properties or activities residing in the cells themselves. All immunity is of course ultimately cellular for antibodies are formed by the cells, so that even the expression 'cellular immunity' is one only of convenience."
After a consideration of the works of the various observers, Gunn reaches the following general conclusions as to acquired tolerance to narcotics:
"The foregoing account of the present state of knowledge in regard to acquired tolerance to hypnotics would have little value beyond a mere catalogue of results, were no more general conclusions deducible from them. A wide survey seems however to reveal certain points of unanimity that may now be summarized, even if they be regarded in the meantime as merely provocative. Among drugs generally, it is chiefly to depressants of the central nervous system that tolerance can be acquired,—to alcohol, chloral, morphine, etc., rather than to e.g., codeine, strychnine or other alkaloids. When a substance combines a depressant action on certain parts of the nervous system with a stimulant action on other parts of the nervous system or with other physiological actions, it is to the former chiefly or only that tolerance is established. The experiments of Van Egmond, Van Dongen and Tamura with morphine, of Langer with heroin, and of Biberfeld with paracodeine are all in agreement on this point. In regard to these hypnotics therefore acquired tolerance is largely if not entirely due to the fact that certain parts of the central nervous system can acquire an increased resistance to the action of depressants. It may not be accidental to this that tolerance can be acquired the more easily in different animals in proportion to the higher development of the brain, e.g., in the order man, dog, rabbit, frog. The fact that some degree of tolerance can be acquired to alcohol, chloral, veronal, morphine, cannabis indica, hyoscine, substances with little or no chemical similarity but which agree in being cerebral depressants, suggests strongly that tolerance is more intimately connected with their actions on the nervous system, in which they agree, than with increased destruction of them, in the mechanism of which they must necessarily disagree. Experiments dealing with destruction of alkaloids, etc., by the tissues are not only negatively useless but may be positively misleading unless a very exact method of quantitative estimation is employed."
The author also states the following in regard to the destruction of drugs by the body tissues:
"One very important problem which has repeatedly arisen in the foregoing discussions relates to the methods by which drugs are destroyed in the body,—whether, for example, congenital tolerance is due to superior destruction of the drug by the more tolerant animal, and whether destruction can be increased by habituation. The experimental investigation of these problems is difficult because it is not an easy task to follow the fate of a drug quantitatively from the time of its injection to the time of its complete disappearance from the body, and this difficulty is reflected in the conflicting results which have been obtained. It is believed that alcohol, atropine, morphine, strychnine—to mention only a few drugs,—are partly destroyed in the body, that this destruction is due to ferment action, and that the liver is the organ usually chiefly responsible for the destruction. There is no difficulty in imagining that alcohol may be destroyed in the body, for according to some it is normally present in the blood in small quantities, and in any case is closely related to substances which the body normally destroys. On the other hand it can hardly be supposed that there are specific ferments in the body which are lying in wait in the hope that some day a suitable alkaloid will be presented to them for attack. It is highly probable therefore that if alkaloids are destroyed by ferments, the usual business of those ferments is to destroy substances normally occurring in the body, e.g., decomposition products of proteins, amines, etc. It may well be that different animals, according to differences in their diets, etc., may have different powers of destroying alkaloids, and that congenital tolerance may be due sometimes to these differences.
"When it comes however to the questions (a), whether an animal can acquire by habituation a destructive action which it originally did not possess; or (b), whether it can by habituation increase such a power if preexistent, the difficulties are greater. In regard to the first question, the destruction of the benzene ring compounds may afford a parallel. The body can destroy the benzene ring of those aromatic aminoacids which enter into the composition of proteins, whereas the benzene ring of foreign aromatic compounds is usually left intact. The condition of alkaptonuria especially shows that when there is a congenital absence of the enzyme which destroys homogentisic acid, this ferment action is never gained throughout life, though the substance to be destroyed is being constantly formed from the food. This seems to be one certain example of the complete inability of the body to form a new enzyme in response to habituation.
"In regard to the second question, it is quite possible that ferment activity can be artificially increased, because animals fed for a long period on one particular kind of food may develop an abnormal ferment activity for this particular food. The difficulty in regard to, e.g., alkaloids would seem to be this. The ferment that destroys them is one that presumably normally destroys some other substance and it is difficult to imagine how this ferment can be increased by the minute quantities of alkaloid (e.g., of nicotine) which enter the circulation. In other words, one would imagine that there would be even larger fluctuations from day to day in the amount of substance that the ferment normally destroys than would be afforded by the addition of the alkaloid.
"At all events these considerations would seem to urge a caution against accepting results which have claimed to show an augmentation of destruction of alkaloids given in small amounts and for short periods and especially those results which claim that a new power of destruction can be originated by habituation."
B. Legewie-1924 92
"A consideration of the mechanism of abstinence forms the most difficult part of the problem. Here as in tolerance the psychiatric literature especially is very meagre and it perhaps would not be inadvisable to review a few of the important opinions and results of investigation on the subject.
"A consideration of this question becomes difficult by reason of the complex nature of our conception of morphin tolerance. In this respect there are four main points to be considered which have become more or less prominent. In the first place we must consider the pharmacologic or toxic changes (euphoria, insensibility to pain, respiratory paralysis, etc.) which morphin produces in the central nervous system forming the characteristic symptoms of addiction. But this conception further signifies that one has become tolerant to the drug, since it produces no further marked effects and is no longer poisonous; but further it signifies that such a degree of addiction has been reached that the patient can no longer do without it on any basis, which bears a relationship to the fourth point to be discussed later; and finally in special cases there are peculiar symptoms due to the absence of the usual effect of a drug, when it is given in the same dosage, so that after a short time increased doses are required to obtain the same effect. In the third place in our conception of morphinism we have the marked abstinence symptoms and finally in the fourth place there is the morbid desire, an eager longing for further administration which the drug bequeaths to many men after they have become familiar with it. All of these four basic considerations of the pharmacologic action, of tolerance, of abstinence, and of morbid desire belong together and constitute what we understand to be morphinism when this or that cause is more prominently mentioned. Yet one explanation of the mechanism of morphinism must apply to them all. It is only through the fact that first the one partial symptom and then the other is brought into the foreground, that one seeks only to explain this as the most marked symptom, that we can understand that investigators always have obtained only partial results, which have not brought us really close to an understanding of morphinism. This is especially true of the experimental investigations in the field of pharmacology, where a number of individual pieces of work have been done, which, however, have not yet made us comprehend the whole picture."
* *
"I think that in the first place the immediate appearance of abstinence upon the withdrawal of the drug forces us at once to assume a direct dependence of abstinence upon the morphin. The next natural assumption appears to me to be that with the withdrawal of the morphin the body lacks a substance which has in the meantime become necessary for the carrying on of its work, a constituent, a means of subsistence. The morphin at first harmful becomes necessary to the body, necessary to life, and now can be dispensed with only at great expense to function. There appears a close relationship between the body and this drug for which it has to pay dearly since there is no permanent benefit. Physiologically speaking there must be a high physico-chemical affinity of morphin or its decomposition products for certain cells in the central nervous system. This is so apparent that the body in the beginning is not able to bind given amounts of morphin in its nervous system but can take on the ability to react only step by step; the body becomes educated to the new relationship and there develops tolerance. Also the cell function becomes modified through this changed cell relationship. If now the morphin is taken away there is produced a vacuum, a functional disturbance, abstinence, which is gradually compensated for again. The process is therefore reversible, but in this case the organism must again adjust to it. A very long period of time must elapse before recovery of the early balance in cell and organism.
"How far my hypothesis can be supported by early experimental work and whether they are in agreement I should like to consider briefly in the following."
After reviewing the literature, he states:
"If we summarize the results, we shall find that the action of the morphin brings about a change in the function of the brain cells in such a way that the morphin is bound in increasing degree by them and especially by their lipoid constituents and is destroyed in a sense, i.e., it cannot be recovered. There results a new functional unity which explains the one side of the mechanism of addiction. The question as to why increasing doses become necessary with time is also answered in the sense that the increased binding or ability to destroy of the brain itself makes possible a need for increased morphin supply. This means that the morphin has become a constituent necessary to life. It cannot be dispensed with easily. And upon the cutting off of the drug functional disturbances appear which are the abstinence symptoms. Thus we see how all of these questions are closely related and can be explained on the same basis. For this reason it occurred to me to consider and study critically at the same time all phases of the mechanism of morphinism in their close relationships to each other. Even the last item for consideration may be accounted for. The morphin craving is only an objective symptom of an especially rapid and intensive affinity of morphin for the cell in different men. From a psychological point of view, this morbid desire belongs to the field of psychopathology and is therefore a purely human problem, an expression of high psychical function. I should like to refer here especially to the excellent studies of E. Straus. But we must not overlook the fact that this question is dependent also updn the characteristic of the chemico-physical reaction of the brain cells in the sense that the problem of psychopathology is brought into direct relationship with organic processes.
"The foregoing conception of morphinism which was forced upon me on the basis of clinical facts, as I found in a review of the literature, was advanced twenty years ago in the experimental work of Cloetta. `The morphin has ceased to be a harmful constituent for the brain lipoid,' and in another place he says: `The increased binding and ability to destroy of the brain probably is conditioned by a certain need of the cell for this substance; and the withdrawal signifies a ceasing of the daily function of the organ.' Later Schübel and then Loofs supported these ideas.
"Naturally there are still difficulties. I have mentioned both main points before. When we say that the brain cell is educated in gradually increasing degree to bind the morphin, then we are considering this fundamental problem of addiction as that which it is, namely, as a fundamental biological characteristic of the living cell. As such it appears to he as life itself accessible to no further explanation. Every explanation must stop here. Even Faust had to say the body becomes educated to destroy the morphin in increasing degree and for the same reason the question as to how the one reacts this way and another that way to morphin is very difficult to answer. We can only come to the conclusion that in living cells there is a process, a chemico-physical one, which still depends on factors which we do not know and cannot demonstrate in the test tube. In the same way also the different behavior of the individual parts of the central nervous system have yet to be explained.
"If thus perhaps we never come to a satisfactory explanation my hypothesis may be considered only a modest contribution to a biological explanation of morphinism in consideration of a uniform conception of the whole range of the subject and the presentation of the most important work so far accomplished in this field."
A. Fauser and B. Ottenstein-1924." 94
These authors have developed an hypothesis demonstrated by animal experimentation concerning the mechanism of dependence and the related withdrawal phenomena, which is based on the physicochemical relationship between the drug and the body cell, in which the permeability of the cell membrane plays an important rôle.
The authors set forth the importance of the relationship between certain psychopathological symptoms and physico-chemical body changes. In a former paper 95 one of them, Fauser, had already expressed agreement with Schade's claim that certain sensations of "uneasiness," the "desires of pregnancy," etc., are due to a disturbance in the H-OH ionic relationships and Na-, K- and Ca-disturbances. They continue as follows:
"Among the abstinence symptoms observed in the different kinds of craving in addition to certain motor symptoms there are other distressing sensations of varying degrees of quality and intensity. The `craving' itself may be considered a mild `abstinence symptom' which induces the patient to take again the drug to which he has become accustomed—just as if it were a substance necessary to life. Without further reference to the empirical facts to be discussed later, the following hypothesis may be advanced at this point: The 'craving' and resulting 'abstinence symptoms' depend on the fact that the given substance becomes a constituent part of certain body cells so that a continuous supply is required in order that the cells may not be ionically disturbed ('craving'), or that the cells are changed in constitution—modified through addiction—, if their supply is withdrawn or appreciably lessened ('abstinence symptoms').
"For an understanding of this hypothesis we must examine the results of those who have studied the physical chemistry of the cell.... This brings into consideration the osmotic property of the cell and the question of permeability; I shall refer here simply to the fact that the permeability of different plasma membranes as well as of one and the same plasma membrane varies at different times and that it behaves electively towards the penetrating substance. In the laboratory experiments to be described later we undertook to obtain, according to the procedure of other authors (for example, H6ber) a model (artificial lipoid membrane) which duplicated the conditions in the cell and to test the measure of the permeability for the given alkaloid bases and their salts. In these experiments we were forced to the significant—in the light of our hypothesis—conclusion that some of these substances, particularly those with which we were concerned, morphin and cocain, differed considerably in regard to the speed with which they passed through the membrane. As we found upon a review of the literature (Rober) that some French authors—for entirely different purposes—had studied a long series of alkaloids, i.e., strychnin, quinin, brucin, and especially morphin, cocain, stovain, in relation to their permeability, let us examine the results already obtained by these authors; our own results which agreed with those just referred to and which we obtained according to the same procedure will be published later in a special report by Frl. Dr. O."
The French authors, they state, found that when a 1% solution of the substance was introduced into an artificial lipoid membrane there was a marked difference in the rapidity of transfer of stovain, cocain and morphin, the first being the quickest to penetrate and morphin the slowest.
In showing the relationship of these facts to their hypothesis they point out that clinically morphin deprivation shows itself very late, only after the drug has been used for six months or longer, that these symptoms are very severe when morphin is suddenly withdrawn, and that those of cocain develop rapidly and are only moderate in severity upon its withdrawal. They believe that these different effects depend perhaps on the differences in the rapidity of osmotic transfer of morphin on the one hand and of cocain on the other. They state:
"Surely we may entertain the idea that if the permeability of a substance through the plasma membrane into the cell is slow, it will take a long time for the substance—under the effect of an elective storage—to become a permanent constituent of the cell, but that on the other hand the disappearance again will be slow; if then through a sudden withdrawal of the accustomed drug, the flow of this constituent by which the cell is washed ceases, a long time is needed to restore the osmotic balance ... between the cell and the outside fluids (blood, lymph, tissue fluid) : the opposite is true in the case of slightly permeable substances. Therfore this indicates a close agreement between the above hypothesis and the experimentally determined facts."
They refer to Faust's theory of increase of oxidation as an explanation of the lack of morphin in the feces and ask if this is not due rather to a retention. Here they think is a therapeutic possibility, namely, the arbitrary modification of penetration velocity or the inducing of changes in cell permeability with thermic influences or the use of hypertonic solutions ("osmosis therapy") to favor the osmotic balance and thus reduce the duration and intensity of the abstinence symptoms.
In animal experiments designed to support their hypothesis, the authors state that they have obtained results similar to those of Wachtel 96 who found, in spite of the injection of uniform amounts, variable and uncontrollable quantities of morphin in different organs. In this connection they say:
".... Wachtel himself could not explain these confusing results—perhaps our hypothesis can throw some light on this apparent irregularity on the basis that there is a difference in the affinity (in a biologic sense) of morphin for different organs or organ cells (`elective behavior of the cell membrane', `elective storage'). Babel also thinks that certain brain cells show a, greater specific affinity for morphin than others and that the alkaloid is in direct contact with certain elementary constituents of the organs. Schiibel has expressed this behavior in chemical terms as follows: the chemically foreign body morphin replaces directly certain basic constituents of the given cells of the central nervous system. According to Fauser then the `morphin addiction' and `withdrawal' mean that on the administration of the morphin the morphin takes the place of a cell constituent and that then on sudden withdrawal there occurs a disturbance of the cell balance in a physico-chemical sense or an alteration in the physico-chemical state, according to which the functional disturbances of the cell as evidenced by the withdrawal symptoms may be explained. The explanation of morphinism, cocainism, etc., and the disturbances relating thereto, may have the same basis, therefore, as that of normal nutrition, of the H-OH, Na-, K-, Ca-balance, etc., and the related disturbances; the explanation of the `craving' and `abstinence symptoms' may be the same as the explanation of the 'normal hunger and thirst sensation,' of salt deficiency, of the sensation of shallow respiration and of the morbid appetite of pregnant women, .. .
"Here is involved a problem such as those frequently met in the new developments of science, especially in the field of biology: problems which belong to so many and different fields that a single head can, it is true, comprehend their general significance, but cannot alone master all of the technical relationships; this requires the combined effort of clinicians who from a most practical point of view are also trained in psychology and psychiatry and analytical and physical chemists."
T. Takayanagi-1924.°7
After reviewing the work of Faust, Rübsamen, and van Egmond relating to the fate of morphin in the body, the author describes as follows his experiments in which he sought to confirm Riibsamen's results by the application of a more accurate method of morphin determination: 98
"Some of the rats were injected once, others repeatedly, with morphin. At various intervals after injection they were killed, passed through a meat-chopper, and tested in accordance with my method, previously described, for the amount of morphin present."
"In the acute experiment a large number of rats were injected subcutaneously, some with 60 and some with 30 mgm. of morphin hydrochloride. The animals were killed after intervals of from 2 minutes to 6% hours. Usually, those rats which had received 30 mgm, of morphin showed, after % to 1 hour, severe symptoms of intoxication and were completely recovered after about 6 hours. Of the entire series receiving this dose but 2 died.
"From the amounts of morphin recovered it appeared that the morphin underwent a progressive destruction, and that after 6 hours the entire amount had been eliminated from the body. With animals of approximately the same size the destruction is somewhat proportional to the time, although a rather wide distribution of values was observed. The animals which received 60 mgm. were severely intoxicated and a number of them, as seen by the incomplete experiments, died within 3 to 4 hours. After a dose of 60 mgm. a rat cannot remain alive for more than 5 hours. Here also the destruction of morphin parallels the time factor, the destruction reaching a maximal value of 51%. None of the animals recovered.
"In order to addict the animals to morphin a large series of rats were given daily subcutaneous injections, the dose increasing from 6 to 30 mgm. During the treatment the weights of the animals were watched and the dosage was increased only when the animals maintained their weight and showed no severe symptoms of intoxication. In spite of this care a very considerable percentage of the animals died during the immunizing course, particularly when the procedure was being carried out during the colder months. The treatments for developing tolerance extended in some instances over 7 days, in others over 14 days. After this period of immunization was terminated some of the animals were given, subcutaneously, 30 mgm. of morphin, others receiving 60 mgm. After this dose they were sacrificed at intervals varying from 10 minutes to 3 hours. The amount of morphin present was determined as for the non-addicted rats. In none of the immunized animals were there visible symptoms of intoxication following the last injection.
"In all experiments, at one time or another, an amount of morphin was found to be present such as would have induced severe intoxication phenomena in non-addicted rats. Nevertheless the quantities of morphin found indicated a rate of destruction which very considerably exceeded that observed in non-tolerant animals. As a rule the rate of destruction in animals which had been immunized throughout a period of 2 weeks considerably exceeded that taking place in the animals subjected to immunization for but 7 days.
"These results agree with those reported by Rübsamen, although in the animals of the experiment here reported the rate of morphin destruction, both in the addicted and in the non-addicted rats, was considerably greater than that stated by Rübsamen, viz., that tolerance to morphin consists in a more rapid destruction of the alkaloid together with an increased immunity of the cells for the toxic agent."
J. D. Pilcher and Torald Sollmann-1924.9sa
In a study of the effects of solutions of morphin and its esters when introduced into the skin, these authors state that lesions similar to those produced by the local inoculation of foreign proteins are produced in susceptible individuals. Whether or not a high degree of tolerance to toxic actions of morphin in addicts extended to the local reaction was one of the interesting questions involved. They reached the conclusion that the local reaction is not at all modified by the acquirement of systemic tolerance; that it is the same in patients during the various stages of habituation and dishabituation as it is in normal individuals. On the contrary, this skin-test by intracutaneous injections is, they claim, remarkably uniform in the great majority of subjects, normal or addicts, irrespective of sex and color. Their method of procedure and observations are given as follows:
"The intradermal method was used in preference to the scratch methods, since the former not only acts with much smaller concentrations, but also permits a much better control of the quantity of solution introduced into the skin, and therefore gives more uniform results. The injections were made into the cutis of the flexor surface of the forearm, a sufficient quantity of the solution being introduced to produce an immediate distention wheal about 5 mm. in diameter. A control wheal was made with physiologic sodium chlorid solution containing 0.25 per cent. of tricresol; and the course of this was oompared with that of strictly similar wheals produced by the solution with the addition to morphin bydrochlorid, in the proportions of 1:1,000, 1:100,000 and 1:1,000,000. The latter solution gave either no reactions beyond that of the saline control, or only a minimal increase. The 1:100,000 solution always gave mildly positive reactions. With the 1:1,000 the response was always so marked that it was deemed superfluous to employ more concentrated solutions. This illustrates the lower sensitiveness of the scratch method, which gives at most slight reactions with the 1:1,000 solutions. A number of experiments were also made with a 1;10,000 solution, but as this gave no additional information, its use was discontinued. The total quantity of morphin introduced at a complete test, comprising three injections, is about 0.1 mg. (1/600 grain), so that there is no possibility of any perceptible systemic effect whatever; nor was any such effect ever noticed by either normal subjects, addicts, or exaddicts.
"OBSERVATIONS
"The injection sites were usually observed at five, fifteen, thirty, sixty and 120 minute intervals following the injection, the size of the wheal and of the erythematous area being measured. As the reactions subside, the outlines of the wheals and, to a less extent, of the areola become less and less distinct, so that accurate measurements are impossible. The reactions were then recorded as `fading' or `faded.'
"Normal Course of the Morphin Reactions—As has been stated, this is remarkably uniform, although minor quantitative variations are found, even in the same individual; for one thing, because it is not practical to introduce exactly the same quantity of the solution into the same area of skin. These accidental variations may be smoothed out by multiplying the observations; and since the conditions observed by us did not modify the course of the reactions, we may employ the medians of the entire series of about eighty subjects as a basis for the `normal course.' The phenomena are most typical when they are most marked, i.e., with the 1:1,000 solutions.
"Course of the Reaction to the 1:1,000 Solution.—There is a momentary stinging sensation, but exceptionally a little pain, Then the primary 5 nun. wheal, produced mechanically by the intracutaneous injection, becomes rapidly reddened, increases in size and is surrounded by a congested area of rather irregular outline.
The maximum intensity is reached in from five to ten minutes, seldom later. The wheal is then about 12 mm. in diameter, somewhat doughy, moderately raised above the surrounding skin, rather sharply circumscribed and fairly circular, but sometimes having a few pseudopods. It is surrounded by an erythematous areola having the diameter of from 4 to 6 cm.; bright or `angry' red near the wheal, paler and somewhat mottled toward the periphery. Usually the size of the wheal and the congested area were roughly proportional; i.e., the larger the wheal, the larger the congested area. There were exceptions, as illustrated by two experiments with the 1:1,000 solution: One subject, aged 55, had a wheal 1,6 cm. and a congested area 4 cm. in diameter; while a second subject, aged 23, had a wheal 1 cm. and a congested area 6.8 cm. in diameter. This variation is probably due to want of parallelism between the permeability and dilatation of the skin capillaries.
"Subsequent Course.—Usually within fifteen minutes after the injections, the phenomena begin to subside. The wheal becomes flatter and paler, and its borders are less distinct. The areola decreases in size and color. The fading progresses rather slowly. In an hour after the injection, the areola is quite faint, and the site of the wheal pale, and still indurated, but not elevated above the surrounding skin. Somewhat later, one and one-half or at most two hours after the injection, all visible trace of the reaction has disappeared."
The subjects used in the experiments were classified by the authors as follows:
"Group A: Current addiction: Five subjects who were receiving from 3 to 5% grains of morphin a day from the Narcotic Bureau.
"Group B: Abstinence symptoms: Eighteen subjects still receiving morphin or diacetylmorphin in reduced, but still large dosage (usually from 1 to 4 grains (0.065 to 0.260 gm.) on the day preceding the test), and showing abstinence symptoms, slight in about two-thirds of the patients, severe in the others.
"Group C: Complete withdrawal (short, i.e., of from ten to twelve days) : Ten subjects. Abstinence symptoms had completely disappeared.
"Group D: Complete withdrawal (intermediate, i.e., of from two to ten weeks) : Nine subjects.
"Group E: Complete withdrawal (long, i.e., of from six to seven months): Nine subjects.
"For comparison with these, we have two groups of nonaddicts:
"Group I, normal: Seventeen normal individuals who had never used opiates habitually, and many of whom had never received effective doses even therapeutically.
"Group II, therapeutic: Four subjects who had never been addicted to opiates, but who for therapeutic purposes had received several small doses in the hospital on the days preceding the test.
`The comparative results as to intensity and duration of the reaction may be illustrated by the observations for from five to thirty minutes after injection, as shown in Table I. The data for all the other periods have been similarly tabulated, but need not be reproduced, as they merely confirm the conclusions in Table I.
"A glance at the table shows the identity of the figures in each vertical column; i.e., the identity of the reaction of all the groups, as concerns the maximal or the minimal concentrations, or the intensity or duration of the response.
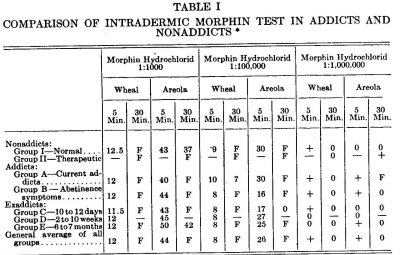
The numbers correspond to the median diameter in millimeters of the wheal or areo a in addicts, exaddicts, mad nonaddicts;
F indicates that the response has faded materially;
0, that 't had disappeared practically completely;
+ indicates a positive reaction, but too slight for measurement.
TABLE II
EXTREME VARIATIONS OF THE MORPHIN REACTIONS *
| Wheals | Areola | |
| Nonaddicts |
11-18 | 20-65 |
| Addicts |
||
| Group A | 14-14 | 30-45 |
| Group B | 9-20 | 14-60 |
| Exaddicts | ||
| Group C | 10-18 | 30-60 |
| Group D | 10-20 | 40-60 |
| Group E | 9-13 | 65-67 |
"COMPARISON OF THE MORPHIN TEST OF WHITE AND COLORED RACES
"Whether the greater resistance of the negro-skin to certain irritants such as light, and dichloridethylsulphide, extends also to morphin seemed worth investigating. We utilizea thirteen negroes of light to very 6.rk skins belonging to various addiction groups; but as we have shown that addiction does not alter the response, they may all be grouped together. The results are shown numerically in Table III. Only the numbers for the wheals of the five-minute period are reproduced.
TABLE III MEDIAN DIAMETER (MM.) OF WHEAL AFTER 5 MIN.
| Morphin hydrochlorid | |||
| 1:1000 | 1:100,000 | 1:1,000,000 | |
| White | 12 | 8 | 0 |
| Colored |
12 | 9 | 0+ |
| General average |
12 | 8 | + |
"The wheal response is evidently identical. The color of the areola cannot be differentiated sharply from the dark color of the surrounding normal skin of the negro, although it can be seen somewhat dimly. In the lighter mulattoes, the reaction is sufficiently visible for measurement, and then averages the same as in the white race."
The following are the authors' conclusions:
"1. Morphin administered intradermally produces a wheal surrounded by a congested area, the reaction increasing in intensity and duration with the concentration. The minimum concentration of 1:1,000,000 was effective in about one half the experiments. A 1:100,000 solution always produces a wheal and congested area.
"2. The reaction reaches the maximum in from five to fifteen minutes and disappears in from one to two hours.
"3. The reaction is in every respect the same in addicts and in normal individuals. Systemic tolerance of morphin, therefore, does not induce local (skin) tolerance.
"4. The reaction is identical in the young and in old adults; in males and females; in the white and negro races.
"5. The reaction is probably somewhat more marked in skins of fine texture.
"6. The presence of edema greatly lessens the wheal formation, and in extreme cases of edema, abolishes it."
A. G. DuMez and Lawrence Kolb-1925."
These authors undertook two groups of experiments to determine whether transferable immunizing substances are present in the blood serum of chronic morphin and heroin users. In the first group after finding the minimal lethal dose of morphin sulphate for white mice to be 0.45 mg. per gram-weight and that of heroin hydrochloride to be 0.2 mg. per gram-weight, the protective effect of the addict serum against these doses was tested in the mice. In the second group the protective effect of the addict serum was tested against increasing doses of the drugs, starting with a very low sublethal dose and ending with an absolutely fatal dose. The authors concluded that—
"Both groups of results . . . fail to show that the effect of subcutaneous injections of morphine and heroin addict blood sera into mice receiving lethal doses of the respective drugs of addiction differs from that produced by the injection of non-addict sera—a slight protective action being observed in both cases, as has been discussed. It is therefore concluded that the blood of human beings addicted to these drugs does not contain transferable immunizing substances."
Congenital Addiction.
Another interesting phase of tolerance is evidenced in so-called "congenital addiction," or the tolerance claimed to be exhibited by the foetus and the new-born child of a mother suffering from chronic opium intoxication during pregnancy. We are giving below the reports of such cases as our study of the literature and of our questionnaires revealed. These cases are mentioned generally without speculation as to the mechanism involved and quite regardless of the views as to the nature of tolerance held by the writers.
Ch. Fere-18S3.'"
Fere reported to the Societe de Biologie a case that Charcot tried to treat by rapid reduction,—a pregnant woman who was taking not more than 25 cg. of morphin a day. As soon as the dose was appreciably decreased the foetus became so violently active as to threaten abortion. For several months it was necessary to continue the drug and it was not stopped finally until a month after delivery. The child showed symptoms of chronic morphin intoxication after birth. He was normal in size but thin. His movements were jerky and he was very nervous, crying for sixty hours without sleeping. After this his symptoms abated and he recovered.
D. A. Zambaco-1884.101
Zambaco mentions this case of Charcot's and two others in which the children lived and were normal in development. He concludes that the danger lies in withdrawing the drug during pregnancy.
F. B. Earle-1888.102
Earle reports a case of a baby born at full term which, at the end of its third day, seemed particularly sensitive to motion, was pale and pinched and prostrate. Twelve hours later it died. The mother of this baby at the time of its birth was a chronic opium user.
In the discussion of Earle's paper, another physician reported attending a woman in confinement whose child, deprived of mother's milk, showed similar symptoms.
Further discussion of Dr. Earle's paper was reported as follows:
"Dr. Kiernan said that the influence of drugs like morphine on the maternal organism was exerted on the reproductive apparatus and the ovum. As has been shown by naturalists certain species of pigeons, whose ancestors had fed on poppies, were relatively intractable to opium. And the same fact was pointed out by Dr. Murrell about persons descendant from Bedfordshire (Eng.) naives, whose ancestors had used infusions of poppies, as a prophylactic against malaria. The infantile mortality among these people was not stated, but nervous diseases were relatively prevalent in these districts. As Morel had pointed out, narcotic habits in the ancestors produced descendants in whom the normal checks on excessive nervous action were removed, so that paranoiacs, periodical lunatics, epileptics, hysterics, congenital criminals, congenital paupers or otherwise degenerable beings, result. This influence was most strongly exerted, when the maternal ancestor was the one affected for, as Spitzka had shown, to her was committed the development of the ovum prior to conception and of the child subsequently. If either was interfered with by a habit, a being, defective in some respects, was the result. In dealing with the cases reported by Dr. Earle, the fact should be remembered that, as the researches of Ball, de Mont.eyel, Manning, Mays and those of Dr. Kiernan himself had shown, infantile mortality was very great among the neuropathic class. With regard to the direct influence of the opium habit in mothers and on the offspring, Dr. Amabile had shown the children of opium smokers were somewhat intractable to opium, but that such children were apt to die suddenly. . Dr. Alonzo Calkins had reported several cases illustrating the same facts as described by Dr. Earle. Dr. Levinstein found, by experiments on pregnant dogs and rabbits, that the use of opium during pregnancy produces either abortion or still-birth, or rapidly dying off-spring. Dr. Hubbard has discussed the very question raised by Dr. Earle and said that treatment of the opium habit must be postponed until it will not imperil mother or child. He reports cases presenting the same phenomena as described by Dr. Earle in which opium was given with the result of improving the physical condition of the children, who, however, grew up stupid. Dr. Kiernan was himself acquainted with two similar cases.
"As to treatment, the habitue would abort if deprived of opium. With regard to the treatment of the child, Dr. Hubbard believed that the smallest quantity of opium necessary to sustain the child should be ascertained in these cases. The child should be allowed to regain strength after which the dose should be reduced and the same treatment pursued as in other cases of the opium habit."
T. J. Happel-1892.1°3
Happel, whose theories as to the cause of symptoms noted in infants born of mothers suffering from chronic opium intoxication have been widely quoted, in his consideration of the existence of the sexual desire and function in women using morphin, describes several cases. He concludes that when the mother uses morphin habitually, the child is born with some defect of the heart, a congenital heart disease. "I do not pretend to assert that the use of morphin is the sole cause of these defects, but that when morphin is used to excess, in the large majority of cases, the deficiencies do exist."
The author states that the symptoms are restlessness, fretfulness, and cyanosis, but that the child is generally in good condition for the first twelve to twenty-four hours. However, the condition grows worse, unless the cause of the trouble is known or suspected and the free use of opiates and stimulants is begun. Happel believes that the condition is easily understood if the fact is kept in mind that the child is born an opium user, its blood is saturated with the drug, the mother has lived on it, and the foetus has developed under it.
Bureau-1895.1"
Bureau, in an article dealing with the chemical proof of the passage of morphin through the placenta, reports the confinement of Mme. G., age 33, in perfect health. She became pregnant in October 1887 and through severe pain in the pelvis and bladder began the use of morphin not long after and quickly reached a daily dose of eight or ten cgs. An ectopic pregnancy was diagnosed and a rupture of the cyst, with relief and ending of the pregnancy, occurred in January. By this time morphinism was established and two or three cgs. a day were used. In October 1888 pregnancy again occurred and was normally conducted until the seventh month when the urine contained a great deal of albumen. This improved on treatment and on July 20, 1889, the patient gave birth to a well-developed girl baby. The infant was fed by a wet nurse and grew and developed normally without any symptoms of narcosis or withdrawal. Meanwhile Mme. G. increased her daily amount of morphin to from 1 cg. to 1.20 cgs. a day. Menstruation continued regularly, as heretofore. In January 1893 it ceased and pregnancy developed with a great deal of bladder pain and albuminuria. She used at least 7.5 cgs. of morphin a day. Delivery took place November 19, 1893, of a normal girl baby, right posterior occiput forceps, without difficulty or injury. The baby died on the seventh day with symptoms of excessive nervousness, rapid breathing and convulsive movements. Post-mortem could not be made. She had nursed with difficulty.
In June 1894, pregnancy again took place while Mme. G. was using 1 g. of morphin daily. At about the fourth month the physician tried to reduce the dose and the patient cooperated, but complained of violent pain in the abdomen and that the foetus moved very actively when the drug was stopped. The attempt to withdraw the drug failed. Delivery occurred April 4, 1895, spontaneously after eight hours of labor. A girl baby weighing 3 kg. 750 g. The baby had a left club and a cephalic asymmetry. The left side was as if atrophied, the right side well developed. The infant was very nervous for the first week, a good wet nurse was found and at the time of writing nutrition was progressing well.
Immediately after delivery, in this instance the cord was tied and 130 gs. of placental blood was collected. This was tested carefully for morphin which was found present as indicated by positive reactions in five different tests. The author states that the passage of morphin through the placenta is not especially surprising, but he finds no record of the fact having been previously demonstrated.
Bureau states that in 1891 Furst wrote (Centralblatt f. Gyn. 1891, No. 3, p. 73) an article on the use of morphin in pregnant and parturient women and nurslings. He reported two cases of infants of a mother who was taking morphin throughout pregnancy where little or no effect was observed on the health of the children.
The author calls attention to the prolongation of pregnancy, according to his calculation two weeks, in the last instance in Mme. G. due he thought to the retarding of the setting up of uterine contractions by the drug.
American Textbook of Applied Therapeutics-1896.1°5
"Infants born of mothers who are morphinists have small chances of living. Happel attributes their low vitality to a congenital defect of the heart, a non-closure of the foramen ovale and the ductus arteriosus. In such cases, convulsions, cyanosis, and most alarming collapse often supervene shortly after birth, and large doses of morphine hypodermically are necessary for relief. The child has subsequently to be weaned carefully from the poison. The possibility of morphinism as a cause, has to be borne in mind when examining an infant suffering from the symptoms noted. The ultimate prognosis as to the child's growing up is, however, bad; and this may be considered fortunate, as the moral and mental strength of these children is so far below par as to make them liable to much subsequent' suffering."
T. C. Allbutt--1905.1“
"A curious assertion has been made by Dr. Happel, that the children of morphinists often show on birth the 'symptoms of withdrawal' of the drug; that they readily become cyanotic, and need morphia and alcohol to rear them. Dr. Crothers, in the same discussion . . . . added that these children not rarely become themselves morphinists or alcoholists in after-life. It must be difficult to distinguish between such a direct and specific influence and the more general forms of neurotic inheritance. Four cases recur to my own memory; in one case the child of a morphinist father was marked only by asthma, which probably was part of a neurotic inheritance independently of the morphinism; and the children of three morphinist mothers were fairly healthy. As the use of morphine diminishes sexual desire, the children of morphinist mothers are more commonly met with than of morphinist fathers. Such children are no doubt born in poison, and need most careful feeding and management to attain a fairly healthy state (Grossman). Erlenmeyer saw a healthy child born of two inveterate morphinists; but on the other hand he reports that many such children are sickly, frail, and bloodless."
Alexander Lambert-1907-1920.1°7 108 Lambert, 1907,1" quotes Happel and in 1920 1" writes:
"In some instances the children born of morphin-taking mothers become cyanotic twelve or twenty-four hours post partum and are restless and cannot be stilled in their crying. They seem to be suffering from lack of morphin and are blue babies. They frequently die unless they are given small doses of laudanum or some other form of opium. With this they thrive, but will continue to take a certain dosage of the narcotic to which the mother was addicted. One such patient who came under the author's care at ten years of age had from birth received small doses of laudanum. Both this child and his mother were easily cured, the child showing no different reactions, in kind or in degree, from an average child; he increased in vigor of mind and body very quickly and showed not the slightest sensation of craving for the drug."
Harrington Sainsbury-1909.109
"It has been established that the unborn child may acquire the habit from the mother; this is not surprising, seeing that the saturation of the parental system with morphia must involve a saturation of the system of the offspring. Such children after birth may show a restlessness and sleeplessness which resist ordinary treatment, but at once yield to a dose of morphia. No more striking object-lesson on heredity, and the directness of touch which exists between offspring and parent, could be given than this, and it is more valuable because the causal modus operandi is so on the face of things; the morphia absorbed, circulating in the blood of the parent, must by diffusion find its way into the circulation of the infant; the close contact between the two circulations of parent and offspring being adapted to this very end, intercommunication. But if this holds for one drug, opium, must it not hold for all drugs, alcohol, chloral, cocaine, etc., the activities of which depend on soluble substances?
"This, of course, is not the only way in which habit works via heredity, for the morphinist father tends to beget children whose vitality is, from the beginning, not only seriously impaired, but specifically biased. How could it be otherwise, since every influence within the body tells in the upbuilding of protoplasm, and since the composite protoplasm of the germ borrows its qualities from every form of protoplasm in the parental organism? That microcosm, the parent germ on the father's side, must therefore incorporate itself and pass on the morphia influence present at the time of its synthesis, and the difference between the maternal and paternal influences will lie in this, that the former will include, not only the last-named indirect synthetic element, but also the direct influence of the circulating poison."
C. C. Wholey-1912.11°
"A point worth noting here is that if a woman taking morphin in large amounts bears a child, the child is apt to be seriously dependent on the drug. Having obtained it through the mother's blood, he must now have it to prevent death from heart collapse. A case came to my notice lately in which such an outcome seems without doubt to have occurred."
A. Reiche--1912.111
Reiche, in an article dealing with the effect on the foetus of morphin administered to a pregnant dog, says that morphin could not be detected in the foetus. He believes, therefore, that it is questionable whether the poison is, in general, transmitted by the mother to the offspring. He states that large doses of morphin can imperil the foetus, by reducing the blood pressure of the mother and by disturbing the respiration of the child shortly before birth. It is well to consider that large doses of morphin taken by the mother can injure the child. But, as to how large these doses must be we can form no opinion, from investigations which have so far been made. One observation which Prof. Langstein made shows that a human foetus can develop without injury, although the mother is a high grade morphinist. The mother took daily 0.75-1.5 g. morphin hydrochloride during pregnancy. In due time, a well-delivered child was born. It was at first nursed by a wet-nurse. Four weeks later, when it had to be taken off for some other reason, it developed a short attack of cramps. However, it developed without injury. No pathological symptoms whatsoever are for the present noticeable.
George E. Pettey-1913.112
Pettey mentions a number of cases of congenital opium intoxication. Among them the following quotations and cases are of interest:
"Congenital morphinism is a rather rare condition. Comparatively few opium-using mothers conceive and fewer still of the children, born of such mothers, live beyond the third day after birth. This high mortality among the infants of such mothers is not unavoidable, but, managed as they usually are, a large majority of children born to such mothers, die on the second or third day after birth.
"This is due to the fact that the child's blood and tissues are as fully saturated with the narcotic, as are those of its mother; in fact, so far as the physical elements of the addiction are concerned, the child is as much an habitué as is its mother. Severance of the placental circulation, through which the child has been receiving the narcotic, shuts off that supply, and, if the drug is not administered to the child, it suffers the shock and collapse incident to the abrupt withdrawal of opiates from an habitue."
He describes a mother with two children, one of three years and the other one year old. The mother was addicted prior to the first conception. Both children had been put on an opiate for the first three days of life and afterwards had been nursed and so obtained the drug. She had continued to nurse the first one throughout the second pregnancy and up to the time of coming to the author.
Both mother and children were treated and recovered.
The author continues:
"Every child, born of an opium-using mother, should be given an opiate for the first three days after birth. After that the milk may be depended upon to contain enough of the drug to satisfy the demands of the child's system, or, if it is thought best not to allow the child to nurse, the administration of the opiate should be continued, until such time as the child is strong enough to stand the withdrawal. By this means their lives can be preserved.
"The quantity of opiate which the child will require to relieve its distress and to bring it up to what is a normal condition, will vary according to the quantity of drug which is being taken by the mother. The child's blood is as much saturated with the narcotic as is the blood of the mother, and the nerve-centers have acquired the same proportionate degree of tolerance for the opiate, that the mother's nervous system has.
"The relative size of the dose, however, will not hold good if the mother is taking more than 10 grains of morphine per day. It is not believed that the system will really appropriate more than 15 or 20 grains of morphine per day at the outside, and probably not much over 10 grains. What is taken, in excess of that amount, is really thrown off as waste and makes but little, if any, impression on the nervous system.
"A drug habitué who is taking regularly, and whose system has become accustomed to the effects of, as much as 20 grains of morphine per day, could inject almost any quantity above that with impunity. However, if the mother is taking only a few grains, or even 1 grain, of morphine daily, the child's system will be equally as toxic from its effects as that of the mother and the drug will be as much a necessity to its comfort as it is to the comfort of the mother.
"While it will not require so large a dose, for a child born to a mother who is using only a small quantity of opiates per day, the opiate is necessary to its comfort and its administration should be begun, as soon as abstinence symptoms make their appearance. It is a safe rule to begin with 1 drop of laudanum and repeat at intervals of one-half hour, until the child shows the effects of the drug, either by being put to sleep or being relieved from the distressing abstinence symptoms.
"The time that these symptoms may be expected to show themselves will depend upon the frequency with which the mother has been in the habit of taking the doses of her drugs. If the mother is taking but one dose of opiate in twenty-four hours, and the child is born a few hours after she has had her accustomed dose; of course, its blood will have in it the proportionate quantity of the opiate, and this will continue to keep the child quiet until the time, or probably a few hours beyond the time, for the succeeding dose to which the mother has been accustomed.
"But should the child be born just before the time for the mother's accustomed dose, it is evident that her blood and her system, as also that of the child, would be fairly well out from under the influence of the dose taken, say, eighteen or twenty hours, or probably twenty-three hours, before. In this case, the child would begin to suffer from the abstinence symptoms within a very short time after delivery, notwithstanding only one dose of morphine had been taken by the mother during each twenty-four hours.
"This condition should be inquired into, and, if the mother has taken her accustomed dose only a few hours before the severance of placental circulation, no opiate will be required for the child until the succeeding time for the mother's dose; then it should be given the child, as well as the mother.
"Again, the frequency with which the child will require these doses will depend upon the frequency with which the mother has been accustomed to taking the drug. The child's nerve-centers have been accustomed to the same periodic, narcotic sedation which the mother has been subjected to, and these periods have become fixed in its life to such a degree, that if the narcotic impression to which it has thus been accustomed is not kept up, the child will suffer abstinence symptoms, just as the mother would if she did not receive her accustomed dose at the time she had been taking it.
"These periods should be observed in the administration of the drug to the child, as well as the mother, as any attempt to interfere with them, at this stage, would result in serious illness of the child. When the child is two or three months old, both the child and mother may be safely taken off the drug by proper treatment, but no effort at withdrawal or even reduction of the drug should be made during the parturient month, either in the case of the child or mother.
"Mrs. M. J. came for treatment May, 1910. She had been taking McMunn's elixir of opium thirty-one years; is the mother of eighteen children; only the first two and the last one lived beyond the third day after birth. The first two children were born before she had become addicted to the opiate. During the third pregnancy she was threatened with miscarriage and McMunn's elixir of opium was given, to prevent it. During the last half of the period of gestation, the opiate was administered to her two or three times a day, and while it served the purpose of preserving the pregnancy, it also fastened the opium habit upon her and she was not able to throw it off.
"The child was fully developed and apparently perfectly healthy, but, on the day following its birth, it began to show signs of illness and it grew progressively worse and died forty-eight hours after delivery, in convulsions. Neither the physician in attendance nor the mother understood the necessity of giving the child an opiate, and none was given; the death was attributed to unknown causes.
"This pregnancy was followed by another within fifteen months, in which she was confined under the same management, with death of the child, within three days after birth, and this pregnancy by another and another, until this woman had given birth to fifteen children, while using an opiate habitually.
"All the children died within three days from their birth, most of them dying by the end of the second day. The same physician attended her in all these confinements, and both the mother and the physician looked upon the death of the children, as a natural consequence of the mother's condition and inevitable.
"In her last confinement she was attended by another physician, who appreciated the conditions under which the child was being brought into the world and understood the necessity cf protecting it from the shock incident to the abrupt withdrawal of the opiate. In order to do this, he gave paregoric in 10 drop doses and these were repeated at such intervals as were found necessary to keep the child comfortable and free from abstinence symptoms.
"The child was not allowed to nurse, but the paregoric was kept up for a few months and then gradually discontinued. This child is now a stout, healthy boy of 13 years, and the mother is firm in her belief that, had the same course been pursued with her other children, they would have lived also. They were all well developed and apparently normal children and showed no signs of illness or discomfort during the first twelve hours after birth, but, from that time on, their illness grew rapidly and they either went into complete collapse or died in convulsions, by the end of the third day after birth."
P. M. Lichtenstein-1915.113
Lichtenstein reviews two cases of chronic opium intoxication in nursing infants, following the post partum development of this condition in the mothers. In this connection, he states that when the mother suffers from chronic intoxication before the birth of the child,
the result will be either miscarriage, stillbirth, or the birth of a "child showing narcotic poisoning and with an inherited tendency toward taking narcotics."
H. A. Hare-1916.114
"When a mother is an opium-eater, the new-born child often suffers from collapse, on the second or third day after birth, owing to the lack of its customary dose of opium."
K. S. Howlett-1917.115
Howlett reports the case of a child born of parents suffering from chronic opium intoxication. As the mother had no milk, the child was fed artificially and did well from the beginning in every respect. At four years of age, the child was rosy and vigorous and had no perceptible neurotic tendency.
The author concludes that his observations would not indicate that the infant in utero was unfavorably affected by use of morphin by the mother.
W. A. Bastedo-1918.115
"Though it [morphin] is found in the fetal blood, it does not seem to affect the fetus, probably because the latter does not maintain its vitality, by its respiratory apparatus. The new-born babe of a habitue may, however, fail to breathe, or if it lives may require its habitual dose, if the amount excreted in the mother's milk is insufficient, or if the child is taken from the breast."
"Collapse for want of the drug has been reported, in infants born of habitues."
* * * * *
C. F. J. Laase-1919.1'7
"The mother of my patient was a woman of twenty-seven years, who had been addicted to opiates for over two years. Her general and physical condition was good. Her pregnancy was uncomplicated and uneventful. Its course was apparently uninfluenced by her addicted condition so long as opiate drug was supplied to her in the quantities necessary to maintain her free from the symptoms of opiate drug withdrawal, or body-need for opiates.
"Labor was accomplished during insufficient supply of narcotic drug, practically in a condition of withdrawal or drug-need. I had explained to her the inhibitory action of opiate, and she concluded that the opiate would slow her pains and prolong her delivery and might jeopardize the child's life. She, therefore, refused a normal supply of opiate during labor. She was in a highly excited state, when labor was finally completed, very restless, suffering from the usual distresses of opiate need, and just before the final pains attempted to jump out of the window to end the misery of combined labor pains and opiate deprivation. Labor pains were very energetic, and delivery was accomplished with little difficulty.
"The baby was a well-nourished, healthy appearing child. From the moment of birth, however, it was very restless. This restlessness is probably to be interpreted as early opiate need, due to the insufficient amounts of opiate taken by the mother just previously. The symptoms and signs of drug-need developed in the infant identically with those of its mother, in character and in sequence. The restlessness increased; it began to yawn and sneeze. Its face became pinched and its color poor. It drew up its legs as if in cramps, and cried out as if in pain. Its pupils became widely dilated. The chin was in a constant tremor reminding the observer of the chattering of an adult in a chill. Finally diarrhoea began, and the infant showed signs of collapse, with general convulsions.
"Nothing seemed to alleviate these symptoms, until finally a drop of paregoric in water was given, using a small eye-dropper to put the paregoric in the mouth. Five drops of paregoric were given at intervals of five to ten minutes, causing a progressive subsidence of the symptoms and a return to normal."
* * * *
"When lactation was fully established, the necessity for paregoric administration ceased. The infant apparently obtained its narcotic supply through the mother's milk. The mother nursed the child at regular intervals. Just before the time for nursing, the child would display a restlessness unlike that seen in normal children, which would subside immediately after nursing."
L. A. Van Kleek-1920.118
Van Kleek reports the following case of chronic opium intoxication in a new-born infant of a woman, aged 32, married 4 years, first pregnancy. She had developed the condition as a result of the use
of paregoric, codein, and later morphin administered for painful menstruation.
"When she first consulted me, she was in her third month of pregnancy, and taking between four and five grains of morphine sulphate daily. Her period of pregnancy was normal save for slight vomiting and a slight trace of albumin in the urine. Labor began at term and lasted twelve hours. The delivery was normal in the left occipital posterior position. During the labor it was necessary to increase the morphine to six grains. This administration of the drug had no effect on the character or frequency of the pains. The post-partum period was normal, the milk flow being established on the fourth day.
"Apparently normal male child weighing seven and one-half pounds. Cried well at birth. On the second day the child's condition became alarming without apparent cause. The pulse became weak and almost imperceptible; the skin was pale and bathed in cold perspiration; mucous membranes and extremities cyanotic; respirations rapid and shallow; vomiting and diarrhoea marked, the child presented a clinical picture of distinct surgical shock. The routine measures for the treatment of shock were tried without response. In view of the fact that the mother was addicted to the use of morphine the child was given three minims of Tincture Opium Camphorata and repeated in one-half hour for three times. The effect was almost like magic. The pulse and circulation improved, and skin became warm, the cyanosis disappeared, the vomiting and diarrhoea stopped. In fact in three or four hours the condition was very nearly normal. The condition appeared again on the third and fourth day, and at each time Tincture Opium Camphorata was given with the same results. After the milk came into the breasts, and the child began to nurse the condition did not reappear. The case was discharged from my care at the end of twenty-one days, both patients apparently well. Six months later I heard from the patient, she still continued using morphine, both she and the baby were in good health."
E. S. Bishop-1920.11°
‘`. . . . as to age in addicts there is no limit. I have seen an infant newly born of an addicted mother displaying the characteristic physical symptoms, signs and phenomena of body need for opiate a few hours after birth. . . . The infant undoubtedly developed addiction-disease prenatally, reacting in its unborn body against the presence of opiates, supplied through its mother's blood, exactly as is now demonstrated through experimental laboratory animals and by clinical study upon adults, this disease is always developed—through physical and constant reaction of the body, to the continued presence of opiates, however supplied. There have been many such cases, some of which are matters of medical record. This condition of prenatal development of addiction-disease exists, beyond dispute, and certainly cannot be explained upon grounds of conscious appetite or deliberate self-indulgence."
P. Sollier-1921.
In reply to a query as to the observance of chronic intoxication in the new-born, Sollier writes:
"I have not published anything on congenital morphinism but I have observed very definite cases where the new-born has shown withdrawal symptoms for several days or even died rapidly in spite of the administration of laudanum, the mother being in a state of intoxication at the time of delivery. I do not know of any special work on this important subject."
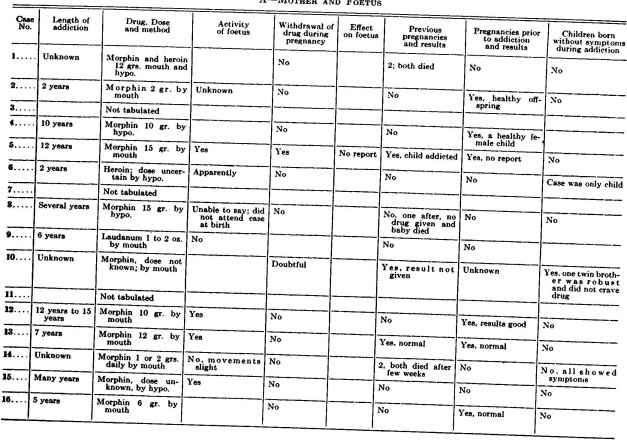
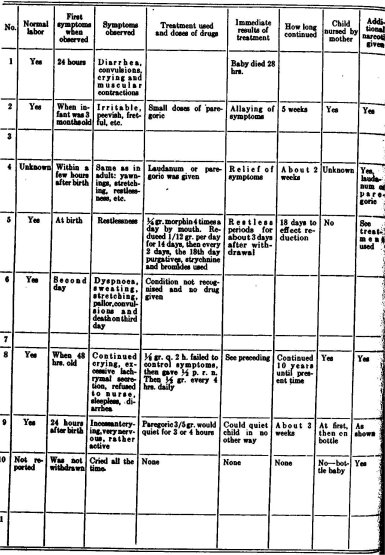
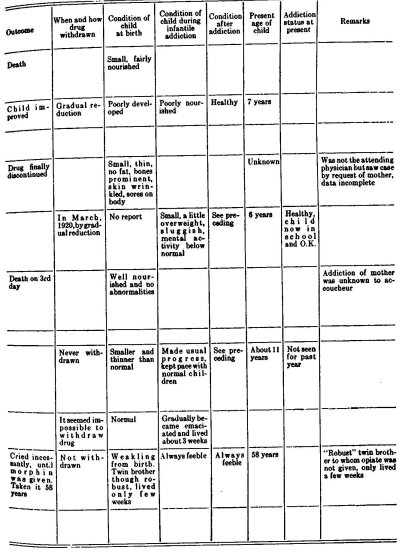
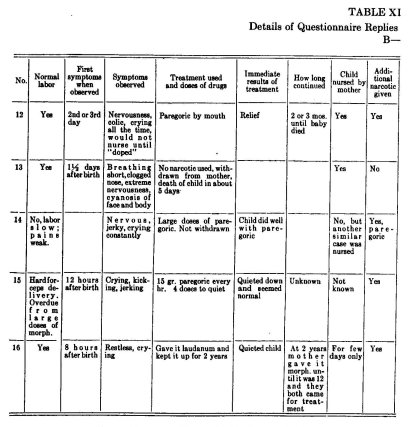
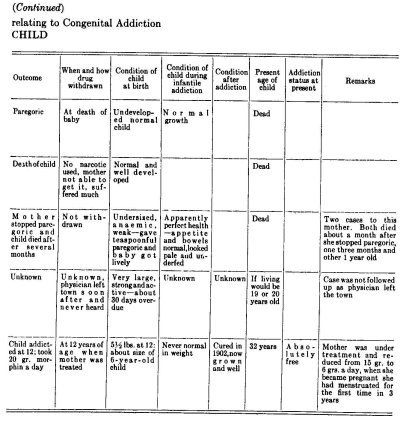
In addition to the above cases from the literature, reports have been received, in replies to our questionnaires, in which the following question was asked:
"Have you observed congenital narcotic addiction in infants of mothers addicted during pregnancy?"
Of the 570 replies received to this question, 51 or about 9% replied in the affirmative, 4 correspondents stated that they were uncertain, 2 that they had heard of such cases, while 513 or 90% replied in the negative.
To those replying in the affirmative, a supplemental questionnaire, dealing with the circumstances surrounding such cases and the phenomena observed was sent. Replies, in which the information sought was given in more or less detail, were received from 13 physicians as shown in the table.
In addition to the replies tabulated, letters reporting cases of congenital opium intoxication were received from four correspondents, in which the information supplied was insufficient to permit of its tabulation.
Requests for reports of knowledge of such cases were made in a separate questionnaire to present and former heads of narcotic clinics.
To this question, 10 replies were received, 2 in the affirmative, 8 in the negative.
From these two sources, therefore, 53 correspondents have reported the observation of such cases.
C. E. Sandoz-1922.12°
"When a pregnant woman uses morphine, the drug circulating in her blood goes over into the child's, so that babies of morphinist mothers show, some hours after birth, withdrawal symptoms identical with those of adults and which are often so severe that they die. Furthermore, cases are on record in which morphine, habitually taken by the mother after the birth of the child, has created in the latter a condition of morphinism which manifested itself by withdrawal symptoms when feeding at the breast was discontinued."
Résumé
On the basis of the evidence submitted in the three preceding chapters two conclusions may be drawn: first, that while the evidence of profound somatic and psychic changes is clear, no theory that has sought to explain the exact nature of the phenomena observed in the various stages of chronic opium intoxication either in human beings or in animals has adduced sufficient proof to warrant its unqualified acceptance on the bases usually required for scientific demonstration; second, in view of the preceding, research work along a number of lines is needed to establish unequivocal grounds for a complete understanding of this condition. This research should include clinical—general medical, psychiatrical, neurological studies—and laboratory experimentation dealing with all phases of the pathology involved and covering a sufficiently long series of cases to warrant the drawing of general conclusions.
Practically the whole controversy relating to the handling of this problem through prevention, alleviation, cure, or ultimate abolition has arisen from different conceptions of the mechanism of the phenomena recorded. It would appear, therefore, that the establishment of accurate knowledge as to the nature of the condition involved is a matter of fundamental importance and one which should claim
the first attention and effort of those who would seek upon a rational basis to assist in the problem's solution.
"The wheal response is evidently identical. The color of the areola cannot be differentiated sharply from the dark color of the surrounding normal skin of the negro, although it can be seen somewhat dimly. In the lighter mulattoes, the reaction is sufficiently visible for measurement, and then averages the same as in the white race."
The following are the authors' conclusions:
"1. Morphin administered intradermally produces a wheal surrounded by a congested area, the reaction increasing in intensity and duration with the concentration. The minimum concentration of 1:1,000,000 was effective in about one half the experiments. A 1:100,000 solution always produces a wheal and congested area.
"2. The reaction reaches the maximum in from five to fifteen minutes and disappears in from one to two hours.
"3. The reaction is in every respect the same in addicts and in normal individuals. Systemic tolerance of morphin, therefore, does not induce local (skin) tolerance.
"4. The reaction is identical in the young and in old adults; in males and females; in the white and negro races.
"5. The reaction is probably somewhat more marked in skins of fine texture.
"6. The presence of edema greatly lessens the wheal formation, and in extreme cases of edema, abolishes it."
1 American Medical Association—J. A. M. A. June 11, 1921. Vol. 76. No. 24. pp. 1669-1671.
2 Kengla, L. A.—Codein in the Treatment of the Morphine Habit. Occidental Med. Times. 1895. IX. pp. 541-544.
3 Bouma, J.—Uber Gewohnungsversuche mit Kodein. Arch. f. exp. Path. u. Pharm. 1903. Vol. 50. pp. 353-360.
4 Babel, A.—über das Verhalten des Morphiums und seiner Derivate im Tierkorper. Arch. f. exper. Path. u. Pharmakol. 52: 262-270. 1905.
5 Sollier, P.—Heroine et Héroinomanie. Press Méd. Nov. 4, 1905. No. 89. pp. 716.
6 Sollier, P.—Apropos de la Chimiothérapie du Morphinisme. Bull. gen. de Thérap. 1920. Vol. 171.
7 Sollier, P.—Un Cas de Codeinomanie pure. Rév. de Méd. Lég. 1913. XX. pp. 359-362.
8 Langer, H.—Ueber Heroinausscheidung und-gewohnung. Biochem. Ztschr. 1912. Vol. 45. pp. 221-238.
9 Pettey, G. E.—Narcotic Drug Diseases and Allied Ailments. 1913. 10 Lambert, A.—Osler and McCrae's Modern Medicine. 1914.
10 Lambert, A.—The Intoxication Impulse. Med. Rec. 1915. Vol. 87. pp. 253-259.
11 Lambert, A.—Nelson's Loose-Leaf Medicine. 1922.
12 Myers, H. B.—Cross Tolerance. Altered Susceptibility to Codein, Heroin, Cannabis-Indica and Chloral-Hydrate in Dogs having an acquired tolerance for Morphine. Jour. Pharm. and Exp. Therap. August, 1916. Vol. VIII. No. S.
13 Wilcox, R. W.—Materia Medica and Therapeutics. 1917.
14 Potter, S. O. L.—Therapeutics, Materia Medica and Pharmacy. 1917. "Bastedo, W. A.—Materia Medica; Pharmacology: Therapeutics. 1918.
15 Cushny, A. R.—Pharmacology and Therapeutics or the Action of Drugs. 1918.
16 White, William A.—Outlines of Psychiatry. 1918.
17 Baumm, F.—Unsere Erfahrungen mit Eukodal. Therap. Monatsh. 1919. Vol. 33. pp. 219-220.
18 Alexander, A.—Ueber Eukodalismus. Munch. med. Wchnschr. 1920. Vol. 67. p. 873.
19 Biberfeld, J.—über Gew6hnung an Kodeinderivate. (Eukodal u. Parakodin.) Biochem. Ztschr. 1920. Vol. III. pp. 91-104.
20 Watson, William T.—Is codein a habit-forming drug? J. A. M. A. May 13, 1922. Vol. 78 (2) No. 19. pp. 1478-1479.
21 Williams, E. H.—Opiate Addiction: Its Handling and Treatment. 1922.
22 Gunn, J. A.—Cellular Immunity: Congenital and acquired Tolerance to nonprotein Substances. Physiological Review. Jan., 1923. Vol. 3. pp. 41-74.
23 Rogues de Pursue, J. and M. Monestier—Un Cas de Codéinomanie. Annales de Médecine Légale. March 1924. Vol. 4. No. 3. pp. 119-124.
24 Sollmann, T.—A manual of pharmacology. 1926.
25 Terry, C. E.—To the Committee on Drug Addictions. A further study and report on the use of Narcotics under the provisions of federal law in six communities in the United States of America, for the period July 1, 1923 to June 30, 1924. New York, 1927.
26 Marmé, W.—Untersuchungen zur acuten und chronischen Morphinvergiftung. Deutsche Med. Wchnschr. 1883. Vol. 9. pp. 197-198.
27 Du Mez, A. G.—Increased Tolerance and Withdrawal Phenomena in Chronic Morphinism. J. A. M. A. April 12, 1919. 72: 1069.
28 Donath, J.—Das Schicksal des Morphins im Organismus. Arch. f. d. ges. Physiol. 38: 528-548. 1886.
29 Stark, E.—Untersuchungen Uber die Gewiihnung des thierischen Organismus an Gifte; Inaug. Diss. Erlangen. 1887; cited by Faust, Arch. f. exper. Path. u. Pharmakol. 44: 225, 1900.
30 Marquis, E.—Ueber den Verbleib des Morphins im thierischen Organismus, Pharm. Ztschr. f. Russland, 35: 549-552. 1896.
31 Bougault, J.—Oxydation de la morphine par le suc de Russula delica, J. de pharm. et de chim. 16: 49-52. 1902.
32 Schutzenberger, M. P.—Note sur quelques produits d'oxydation de la morphine sous l'influence de l'acide azoteux. Compt. rend. Acad. d. sc. 46: 598. 1858.
33 Nadler, G.—Ueber die Bildung des Oxymorphins bei vorsichtiger Oxydation des Morphins, Schweiz. Wchnschr. f. Pharm. 11: 417-419, 1873, 12: 38-42. 1873.
34 Polstorff, Karl—Die Einwirkung des Kaliumferricyanids und anderer schwa-cher Oxydationsmittel auf Morfin und "das Oxymorfin Schutzenberger's" Arch. d. Pharm. 217: 401-424. 1880.
35 Magendie—Cited by Reil, Materia Medica, Berlin, 1857, p. 257.
36 Kreis—Cited by Herrmann, Lehrbuch der experimentellen Toxikologie, Berlin, 1874, p. 381.
37 Toth, L.—Bemerkungen zur Erklarung der chronischen Morphiumintoxikation, Schmidt's Jahrb. 229: 135, 1891.
38 Kobert, R.—Lehrbuch der Intoxikationen, Stuttgart 2:995, 1906.
39 Diederich, Georg—Ueber Oxydimorphine und seine Wirkungen auf den Organismus, Diss. Gottingen, 1883; cited by Kobert, Lehrbuch der Intoxikationen, 2: 996, 1906.
40 Puschmann, A.—Ueber Oxydimorphin und seine Wirkung auf den tierischen Organismus: Diss. Gottingen, 1883; cited by Kobert, Lehrbuch der Intoxikationen, 2: 996, 1906.
41 Gioffredi, Carlo—Recherches ultérieures sur l'immunisation pour la morphine, Arch. ital. de biol. 31:398-411, 1899.
42 Hitzig, E.—Morphium Abstinenzerscheinungen und Magen. Berl. Min. Wchnschr. 1892. XXIX. pp. 1237-1240.
43 Gioffredi, C.—L'Immunité artificielle par les Alcaloides. Arch. Ital. de Biol. 1897. V. 28. pp. 402-407.
44 Gioffredi, C.—Récherches ultérieures sur l'Immunization pour la morphine. Arch. Ital. de Biol. 1899. V. 31. pp. 398-411.
45 Gioffredi, C. L'assuefazione sperimentale alla Morfina. Gior. Intermaz. delle Scienze med. Napoli. 1900. V. 22. pp. 790-796.
46 Loc. cit.
47 Sollier, P.—La Démorphinisation. Mécanisme physiologique. Conséquences au point de vue thérapeutique. Presse Méd. Apr. 23 and July 8, 1898.
48 Faust, E. S.—Uber die Ursachen der Gewiihnung an Morphin. Arch. f. ezper. Path. u. Pharmakol. 1900. Vol. 44. pp. 217-238.
49 Hirschlaff, L.—Ein Heilserum zur Bekampfung der Morphiumvergiftung und ühnlicher Intoxicationen. Berl. Blin. Wchnschr. 1902. pp. 1149-1152; 1174-1177.
50 Hirschlaff, L.—Zur klinischen Anwendung des Morphinheilserums. Ztschr. f. Iirankenpfl. 1903. Vol. XXV. pp. 467-473.
51 Hirschlaff, L.—Uber das Morphin-Heilserum. (Eumorphol-Riedel.) "Loc. cit.
52 Loc. cit.
53 Mavrojannis—Etudes sur le mécanisme de l'accountumance it la morphine. Comp. Rend. Heb. des Séances et Mémoires de la Soc. de Biol. 1902, pp. 930-932.
54 Morgenroth, J.—Zur Frage des Antimorphinserums. Berl. Klin. Wchnschr. 1903. Vol. 40. pp. 471-474.
55 Hirschlaff. L.—Uber das Morphin-Heilserum. (Eumorphol-Riedel.)
56 Cloetta, M.—Uber das Verhalten des Morphins im Organismus und die Ursachen der Angewiihnung an dasselbe. Archiv. fur. exper. path. u. pharm. Dec. 17, 1903. 50 pp. 453-480.
57 Argentina, G.—Contributo alla immunizzazione per morfina. Gazz. d. oQoedali e. d. clin. Apr. 16, 1905. Vol. 26, pt. 1. p. 484-485.
58 Mirto, D.—Sul significato della siero-reasione precipitante nell' assuefazione alla morfina e sul suo valore conic mezzo di riconoscimento della morfina. Arch. farm. sper. Siena. Sept., 1905. V. 4, No. 9, pp. 406-418.
59 Marikovsky, G.—Immunisierungs und sero-therapeutische Versuche dem Morphin gegenüber. Centralbl. f. Bakteriol., Parasitenk u. Infektionsk. 1906-7. Vol: 43. p. 494-507.
60 Rubsamen, W.—Experircentelle Untersuchungen liber die Gewiihnung an Morphin. Arch. f. exper. Path. u. Pharmakol. 1908. Vol. 59. pp. 227-244.
61 Ferrai, C.—Sul Potere Anticomplementare Della Morfina. Pathologies. September 1909. Vol. I. pp. 505-511.
62 We have been unable to locate a report of the original investigation.
63 Albanese, M.—Sur la Transformation de la Morphine dans l'Organisme des Animaux habitués au poison. Arch. ital. de Biol. 1910. Vol. 53, pp. 439-444.
64 "Pettey, G. E.—A rational Basis for the Treatment of Narcotic Addiction. New York Med. Jour. Nov. 5, 1910. V. 92. pp. 915-917.
65 Berri, G. C. and C. R. Belgrano—Aggressive Rispetto Alla Cocaina Ed Alla Morfina. Annali Dell 'Instituto Maragliano. 1911. V. 5. pp. 42-49.
66 Morat, D.—Le Sang et les Sécrétions au cours de la morphinomanie et de la Désintoxication. Thèse de Paris. 1911.
67 van Egmond, A. A. J.—Ueber die Wirkung des Morphins auf das Herz (zugleich ein Beitrag zur Frage der Morphingewohnung). Arch. f. exp. Path. u. Pharm. 1911. Vol. 65. pp. 197-213.
68 Langer, H.—Ueber Heroinauscheidung und -gew5hnung. Biochem. Zeitschr. 1912. Vol. 45. pp. 221-238.
69 Dorlencourt, H.—Étude sur la Déstruction "in Vitro" du Chlorhydrate de Morphine, par les Organes d'Animaux accoutumés et non accoutumés. Séances et Mémoires de la Soc. de biol. 1913. Vol. 74. pp. 895-897.
70 Valenti, A.—Experimentelle Untersuchungen ueber den chronischen Morphinismus; Kreislaufstorungen hervorgerufen durch das Serum morphinistischer Tiere in der Abstinenzperiode. Arch. f. exper. Path. u. Pharmakol. 1914. Vol. 75. pp. 437-462.
71 From—Valenti, A.—Experimentelle Untersuchungen ueber den chronischen Morphinismus; Kreislaufstorungen hervorgerufen durch das Serum morphinistischer Tiere in der Abstinenzperiode. Arch. f. exper. Path. u. Pharmakol. 1914. Vol 75. pp. 437-462.
72 Valenti, A.--Salle cause dei disturbi dell'astinenza morfinica nei morfinisti, Gazz. Internaz. Medico-Chirur., 1923, Vol. 28. pp. 217-218.
73 van Dongen, K.—Beitrëge zur Frage der Morphingewiihnung. Arch. f. Physiologie. 1915. Vol. 162. pp. 54-66.
74 Biberfeld. J.—Zur Kenntnis der Morphingewiihnung. II. Mittleilung. Über die Spezificitiit der Morphingewiihnung. Biochem. Ztschr. 1916. Vol. 77. pp. 283-297.
75 Grüter, M.—Ueber die Zerst6rung von Morphin und Morphinderivaten bei der Entwicklung von Hühnerembiyonen. Arch. f. exper. Path. u. Pharmak. 1916. vol. 79. pp. 337-360.
76 Kraus, Walter M.—An Analysis of the Action of Morphine upon the Vegetative Nervous System of Man. J. Ner. and Men. Dis. Vol. 48, No. 1, July 1918.
77 Du Mez, A. G.—Increased Tolerance and Withdrawal Phenomena in Chronic Morphinism. J. A. M. A. April 12, 1919. 72: 1069.
78 Pelliui, E. J. and A. D. Greenfield—Narcotic Drug Addiction. I. The Formation of Protective Substances against Morphin. Arch. of Int. Med. Sept. 15, 1920. Vol. 26. p. 279.
79 Pellini, E. J. and A. D. Greenfield—Narcotic Drug Addiction. II. The Presence of Toxic Substances in the Blood Serum in Morphin Habituation. Arch. of Int. Med. May 15, 1924. Vol. 33. No. 5. pp. 547-565.
80 Loc. cit.
81 Lane, H. C.—New Method for Detecting Drug Habitués. N.Y. M.J. Aug. 14, 1920. Vol. 112. p. 222.
82 Bishop, E. S.—The Narcotic Drug Problem-1920.
83 Schübel, K.—Stoffwechselversuche an Hunden wiihrend der GewShnung an Morphin und wiihrend des Morphinhungers. Arch. f. exp. Path. u. Pharm. 1920. Vol. 88. pp. 1-29.
84 Wholey, C. C.—The Inadequacy of Bishop's Antitoxin Hypothesis to Explain fully the Symptomatology in Morphin Addiction. J.A.M.A. March 1. 1913.
85 Hildebrandt, F.—Über Veriinderungen des Stoffwechsels nach chronischer Morphinzufuhr Arch. f. exper. Path. u. Pharm. 1922. Vol. 92. pp. 68-95.
86 B7 Loofs, F. A.—Ober die Mtiglichkeit einer klinisch-chemischen Kontrolle des Morphinismus. Bemerkungen zur Theorie der Morphin-gewtihnung. Ztschr. f. d. g. Neurol. u. Psychiat. 1922. Vol. 79. pp. 433-462.
87 Joël, Ernst—Zur Pathologie der Gewtihnung. Therap. Gegenwart. 1923. Vol. 64. p. 397-403; 441-447.
88 Wuth, O.—Ueber Morphinismus. I. Die Entstehung der Krankheitserscheinungen. Munch. med. Wchnsch. Oct. 12, 1923. V. 70, N. 41. pp. 1266-68.
89 * Incidentally it may be noted that most of the Basedow psychoses show stimulation.
90 * Chronic abuse of alcohol produces disturbances of the thyroid (Sarbach).
91 GWillcox, Sir W. H—Norman Kerr Memorial Lecture on Drug Addiction. British Med. J. Dec. 1, 1923. No. 3283. pp. 1013-1018.
92 "Gunn, J. A.—Cellular immunity; Congenital and acquired Tolerance to nonprotein Substances. Physiological Review. Jan. 1923. Vol. 3. pp. 41-74.
93 Legewie, B.—Delirium bei Morphinismus. Zugleich ein Beitrag sur Frage der MorphingewShnung. Ztsch. f. d. ges. Neurol. u. Psychiat. 1924. Vol. 89. p. 558-578.
94 Fauser, A. and B. Ottenstein—Chemisches und Physikalisch-Chemisches zum Problem der "Suchten" und "Entziehungserscheinungen," insbesonders des Morphinismus und Cocainismus. Ztschr. f. d. g. Neurol. u. Psych. 1924. Vol. 88. p. 128-133.
95 Otteustein, B.—Tierexperimentelle Untersuchungen zum Problem der Suchten und Entziehungserscheinungen, insbesonders des Morphinismus. Arch, f. exp. Path. u. Pharm. Vol. 100. p. 349-352.
96 Fauser, A.—Versuch einer Begriindung von Zusammenhüngen zwischen gewissen elementaren psychopathologischen Symptomen und physikalischchemischen Zustandveriinderungen des KSrpers. Ztschr. f. d. ges. Neurol. u. Psychiat. 1923. Vol. 81. pp. 497-516.
97 Biochem. Ztschr. 1921. Vol. 120.
98 Takayanagi, T.—Uber das Schicksal des Morphins im Tierkeirper. II. Mitteilung: Uber die Zerstiirung des Morphins im KSrper gewiihnter und ungewtihnter Ratten. Arch. f. exper. Path. u. Pharm. 1924. Vol. 102. p. 183-187.
99Takayanagi, T.—Eine Methode zur quantitativen Bestimmung des Morphins in K5rperflussigkeiten und Organen. Arch. f. exper. Path. u. Pharm. 1924. Vol. 102. p. 167-175.
100 Pilcher, J. D., and Torald Sollmann—The skin-reaction to morphin. A.M.A. 1924. Reprinted from Archives of Internal Medicine, April, 1924. Vol. 33, pp. 516-524.
101 DuMez, A. G. and Lawrence Kolb—Absence of Transferable Immunizing Substances in the blood of Morphine and Heroin Addicts. Public Health Reports. V. 40. No. 12. March 20, 1925. p. 548-559.
102 Fere, Ch.—De la morphinomanie au point de vue de la grossesse et de la ne du foetus. Communication it la Societe de Biologie. Semaine Medicale. 1883. p. 294.
103 Zambaco, D. A.—Contribution a l'etude de la morphinomanie. Encephale. Paris. 1884. IV. pp. 658-683.
104 Earle, F. B.—Maternal opium habit and infant mortality. Med. Standard. Chicago. 1888. III. pp. 2-4.
105 Happel, T. J.—Morphinism in its relation to the sexual functions and appetite, and its effect on the off-spring of the users of the drug. Med. and Surg. Rep. 1892. LXVIII. pp. 403-407.
106 "Bureau—Accouchement d'une morphinomane; preuve chimique du passage de la morphine a travers le placenta; reflexions. Bull et mem. Soc. obst. et gyn. de Paris. 1895. pp. 356-362.
107 Wilson, J. C. and A. A. Eshner—American Textbook of Applied Therapeutics. W. B. Saunders. 1896.
108 Allbutt, T. C—A System of Medicine. The Macmillan Co. 1905.
109 Lambert, Alexander—Osler and McCrae's "Modern Medicine." 1907. 'Lambert, Alexander—Nelson's Loose-Leaf Medicine. 1920.
110 Sainsbury, Harrington—Drugs and the Drug Habit. E. P. Dutton. 1909.
111 'Wholey, C. C.—Morphinism in some of its less commonly noted aspects. J. A. M. A. June 15, 1912. V. LVIII, No. 24. pp. 1855-1856.
112 Reiche, A.—Ueber den Einfluss einer trachtigen Hundin gegebenen Morphiumgaben auf den Hundefoetus and den saugenden Hund. Ztschr. f. Kinderh. 1912. Orig. IV. pp. 542-545.
113 Pettey, George E.—Narcotic Drug Diseases and Allied Ailments. Tenn. J. A. Davis Company. 1913.
114 Lichtenstein, P. M.—Infant Drug Addicts. N.Y. M.J. Oct. 30, 1915.
115 Hare, H. A.—Practical Therapeutics. Lea & Febiger, 16th ed. 1916.
116 Howlett, K. S.—Drug Addiction and Newborn. J. Tenn. M. A. Apr. 1918.
117 Bastedo, W. A.—Materia Medica: Pharmacology: Therapeutics. W. B. Saunders Co. 2nd Ed. 1918.
118 Laase, C. F. J.—Practical Application of the Facts of Narcotic Drug Addiction Disease. Med. Rec. Aug. 9. 1919.
119 Van Kleek, L. A.—Symptoms of Morphine Withdrawal in an Infant. Amer. Med. Jan. 1920. pp. 51-52.
120 Bishop, E. S.—The Narcotic Drug Problem. The Macmillan Co. 1920.
121 'Sandoz, C. E.—Report on morphinism to the Municipal Court of Boston. Jour. of Crim. Law and Criminol. May 1922. Vol. XIII. No. 1.
| < Prev | Next > |
|---|