| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 193 |
| Yesterday: | 251 |
| This Week: | 193 |
| Last Week: | 2221 |
| This Month: | 4781 |
| Last Month: | 6796 |
| Total: | 129380 |
CHAPTER V PATHOLOGY - SOMATIC AND PSYCHIC CHANGES
 |
|  |
| 
| Books - The Opium Problem |
Drug Abuse
SOMATIC AND PSYCHIC CHANGES
In reviewing the literature on the somatic and psychic changes that may take place in chronic opium intoxication, we find practically no general pathologic studies. On the contrary, it is apparent that the great majority of investigators have been stimulated by interest in only one or another aspect of this condition. This may be due in part to the fact that uncomplicated cases seldom come to autopsy for the reason that rarely, if one may judge from the certified causes, does death result from chronic opium intoxication. Further, in many cases of death of chronic users the obvious presence of an intercurrent, acute condition and ignorance on the part of the last medical attendant of the existence of the opium intoxication lead to the omission of any reference to the latter as either a direct or contributory cause of death.
Whatever the reasons, reports of pathologic findings in general have been scanty, disconnected, and incomplete, making it impracticable to attempt any anatomic or physiologic grouping of such findings. We have selected, therefore, for separate consideration in a later chapter that portion of the material dealing with pathology which especially refers to the mechanisms of tolerance, dependence, and withdrawal. The balance is presented in chronologic order, regardless of relationships, leaving the reader to evaluate and correlate it as he sees fit.
Writers who have treated the subject of chronic opium intoxication in a general manner very frequently have combined their handling of symptomatology and pathology so intimately as to make it impossible to separate them. In the writing of textbooks and special articles on the clinical handling of these cases, this is natural if not inevitable. The reader, therefore, is referred to the chapter on symptomatology for the views held by general writers on pathology which have not been included in this chapter.
Among the earlier writers very little, if any, definite pathology is described, and much of it is doubtless the result rather of speculation than of post-mortem findings.
Alonzo Calkins-1871.1
Calkins quotes Hill and Oxley to the effect that following the deprivation of the drug, "glandular degenerescence, rickets, a hydropic tendency or albuminuria will likely ensue."
H. H. Kane-1882.2
This author, in dealing with the effects of opium smoking, without any details as to morphologic tissue changes, describes at considerable length symptoms and functional disturbances, both somatic and psychic. He emphasizes intellectual degeneration and glandular alterations. He states that the urine contains mucous fibrillae, epithelial cells and an increase in the earthy and alkaline phosphates with a specific gravity of 1.004 to 1.015. In twenty examinations he states that he found no albumin or sugar, but that morphia in varying quantity was always present. Catarrh of the throat and nose, conjunctivitis with burning and excessive lachrymation were not uncommoi. Amenorrhoea is common. The color of the habitual smoker is pallid, while herpes and other trophic changes are rare. The sweat is sometimes profuse, stains the body and bed linen a brownish color and has an odor of opium.
Daniel Jouet-1883.3
Jouet, while not discussing the mechanism of tolerance or offering any explanation therefor, mentions an interesting fact in this connection. He states that individuals who show an intolerance for morphin as indicated by nausea, vomiting, vertigo, weakness, etc., develop, if they persist in the daily use of the drug, marked cachexia, which is not like morphinism and which causes death very much more rapidly than does morphinism. Others, he states, for reasons more or less well known, succumb after the first few injections, and in still other morbid states, such as insanity, the phenomena of morphinism and especially those of withdrawal do not occur at all.
W. von Tschisch-1885.34
This author administered morphin sulphate to eight dogs; to two of these he gave acute poisonous doses, the dogs living only a few hours. In the others he induced chronic poisoning which lasted from 28 to 62 days before the dogs were put to death. The total amount of drug in grains and the sizes of the doses administered to the dogs subjected to chonic intoxication, together with the autopsy findings, follow:
"Dog No. 3 received 135 grains (XXVIIX5)
PP IP 4 " 150 " (XIV X 5 VIII X 10)
/I PI 5 2/ 170 (IV X 5 + XV X 10)
" 6 " 200 PP (XX X 10)
IP PP 7 134 (II X 10 + XXI X 5 + HI X 3)
PP 11 8 PP 125 IP (XIV X 5 + XV X3)
"The Roman numerals indicate the number of doses, the Arabic the size of each dose. As evident from the table, the doses were administered either daily or every other day, in rare cases only every third day.
"The autopsy disclosed hyperemia of the brain and the spinal cord only in the cases of acute poisoning.
"I begin now the description of the ganglionic cells, since the alterations in those showed themselves characteristic and constant to a higher degree. When the spinal cord of dogs No. 3, 4, 5, 6, 7, 8 was examined, whether in fresh or hardened state, the alterations in the cells were always sharply defined. Cells of normal appearance occurred either extremely seldom or not at all. These alterations were as follows.
"The protoplasm of the cells is swollen, turbid; the entire body has a more or less rounded form; the processes are either not visible at all, or their number has decreased; of the processes still present some appear attenuated and very short; such cells take the carmine stain rather intensively. The majority of the cells in No. 3, 4, 5 have the appearance just described.
"Another alteration of the cells, which occurs in all cases, though only in small quantity, is vacuolization: clear spaces, varying in size and almost round in shape, have formed themselves in the more or less altered protoplasm of the cells. The vacuoles have the appearance of cavities, or again, the protoplasm of the cells seems hollowed out, as it were. It is possible to follow up the transition stages from small vacuoles to such as occupy almost the entire body of the cell; there remains, therefore, of a cell affected in the latter way only a crescent-shaped rim. In one cell several vacuoles are observable, which give the cell the appearance of a structure hollowed out in a different fashion, or again, when the vacuoles pierced through the entire surface, the cell has a sieve-like appearance. The vacuoles take neither the carmine nor the osmic acid stain; when greatly magnified (Hartn. 3/10 ??), they looked like cavities traversed in all directions by very fine, whitish fibers intersecting each other. Vacuoles occur also in the substance of the processes; the processes themselves were generally wanting in cells which were extremely vacuolated. Cells with numerous and large vacuoles occurred but rarely; cells with one or two vacuoles occurred more frequently.
"A third type of alteration of the ganglionic cells is the fine-grained degeneration of their protoplasm with complete absence of processes. The nucleus is surrounded by a fine-grained mass, which takes the carmine well; this mass passes over into the surrounding tissue without definite boundaries, or else, it is inclosed by an empty space. Such cells are distinctly reduced in size—the entire amount of protoplasm is sometimes smaller than the nucleus; sometimes only the nucleus is to be seen, without a trace of protoplasm or perhaps surrounded by a few fine granules. Cells altered in this manner occur in considerable numbers in all cases.
"In all cases there are present in great numbers cells of rounded form with processes altogether missing; their protoplasm takes a very weak carmine stain, and consequently, in cross-sections stained with carmine, these cells are sharply distinguished by their coloring from the surrounding tissue. Such cells appear almost homogeneous, and only occasionally do they appear granular at the edges. It is absolutely impossible to isolate them, since their protoplasm falls to pieces at the slightest maltreatment. Vacuoles are not visible in these cells.
"Finally, in cross-sections from the spinal cord of dogs No. 7 and 8, it is possible to see various transitions from such pale cells to completely hollow spaces of rounded form lying in the tissue. Sometimes the pale protoplasm in a cell appears partly homogeneous, partly fine-grained, and the entire cell does not take up all the space left in the tissue; sometimes, in another cell, the entire protoplasm appears granular, but part of it is paler than the rest; sometimes there is present in place of the cell a scant number of small pale granules and extremely fine, short, pale fibers; or again, only the latter are represented; finally, one may see completely empty discs in the tissue. From the observation of these transition-forms, therefore, we can only draw the conclusion that we have before us in a given case remnants of nerve-cells; also, only in this way is it possible to understand in what manner these cells perish completely.
"Only the cells just described are without nucleus; in all the rest the nucleus is always preserved.
"The cells in all the spinal cords, therefore, are variously affected: in the spinal cords of dogs which have perished of chronic poisoning rarefaction of the cells is most pronounced; in the spinal cords of those which died of less chronic poisoning the turbid swelling of the cells is most prominent. All other alterations are common to all cases.
"The nucleus is preserved in all cells except those which appear rarefied; nevertheless, only in a small number of cells—and this in the case of dogs No. 3 and 4—does it show no sharp pathological alterations. In the majority of cells the alterations are characteristic and peculiar.
"As already mentioned, the nucleus—with the exception of an extremely small number of cells--always stands out very distinctly in the midst of the entire protoplasm; it always appears as a perfectly round, gleaming, colorless, double-rimmed disc, filled, without exception, with large granules of irregular shape, which take the carmine stain well. These granules are almost always of the same size, and only seldom is it possible to discover near them a few very tiny granules. As a result, the nucleus is always especially distinct in lightly stained cells. In a small number there may be seen nuclei whose bright, gleaming disc contains very few, small granules, which take the stain weakly. Such nuclei occur as much in well-preserved cells, which take the stain well—in which, therefore, the nucleus appears much paler than the protoplasm—as in the cells whose protoplasm has suffered most alteration through one of the above-described processes. The granules which fill the disc are usually uniformly distributed; however, there also occur cells in which the granules lie along one edge of the disc only, whereas the other edge is entirely free or else contains but very few tiny grahules. The nuclear corpuscle can be discerned only in the best preserved nuclei. The altered nucleus is sometimes surrounded by a comparatively brighter ring of protoplasm. Nuclei altered in this fashion are present in all the spinal cords—the longer the duration of the poisoning the greater their number, it seems. In the spinal cords of dogs No. 7 and 8 many cells have no nucleus at all, or else the latter is represented by a small number of pale, small granules.
"After acute poisoning (cases 1 and 2) the alterations in the cells are by far not so characteristic. Neither in isolated cells of the fresh spinal cord nor in cross-sections of the hardened one is a fibrillar, granular structure to be seen in the protoplasm; the protoplasmic processes are preserved for a short stretch only and in but few cells. The protoplasm of many cells is swollen and turbid; the body has a more or less spherical form. Beside cells altered in this fashion there are seen others which take the carmine stain intensively, have a small circumference, and are, as it were, hollowed out at the edges by small vacuoles.
"As regards the vascular system, the following alterations appear in No. 3, 4, 5, 6, 7 and 8. First of all, the phenomena of a more or less considerable hyperemia strike the eye. In the vessel-walls there are seen a multiplication and swelling of the nuclei, especially noticeable in the capillaries, where these nuclei project into the lumen of the vessel and cause it to disappear almost entirely. In a small number of specimens there are seen in the vessel-walls small, birefringement granules of fatty nature and rounded form. In the subadventitial spaces there is always visible an enormous number of white and red blood corpuscles.
"In cross-sections of the hardened spinal cord there occur considerable accumulations of red blood corpuscles near the vessels and also independently of them—without exception in the gray substance. Hemorrhages were particularly numerous in spinal cord No. 5.
"In addition, there are seen in the gray substance, especially in proximity to the vessels of spinal cords No. 5, 6, 7, 8, small, homogeneous, structureless masses of a plasmatic exudate, which not only destroy the connection between the elements of the subjacent tissue and even impair their integrity—the fragments of nerve-cells and nerve-fibers found in and near these masses are evidence of this—but also infiltrate the tissue to a considerable extent. Not a single time did I see large masses of the plasmatic exudate; sometimes, however, numerous accumulations of the exudate were visible in one and the same cross-section. In specimens of the fresh spinal cord, granular and fatty_ granular cells occurred in proximity to the vessels in all cases, and in especial abundance in the spinal cords No. 7, 8.
"In the gray substance of all the spinal cords, and particularly of No 5, 6, 7 and 8, the complete absence of nerve-fiber processes was striking. Everywhere there were products of a fine-grained detritus, which accumulated more especially where the nerve-reticulum was altogether destroyed, so that in places the entire field of vision was occupied by the detritus; everywhere the nerve-reticulum has lost the distinctness of its outlines. Only a small number of its fibers took the carmine stain, and even this only for a short distance.
"In general it may be said that specimens with cells that had suffered most alteration showed most distinctly pronounced alterations in the vessels and in the nerve-reticulum, although at times—in No. 5, for example, where the number and extent of the hemorrhages appeared the greatest—the cells, in comparison with other numbers, were not so considerably altered. A more complete and more constant relation is observable between the alterations of the nerve-cells and those of the nerve-reticulum."
B. Ball-1887.4
Ball gives the following account of an autopsy of a patient who died thirteen days after withdrawal of the drug.
On autopsy most of the organs appeared normal. There were no
valvular lesions of the heart and no dilatation of the ventricles. The myocardium was pale and showed histologically a beginning fatty degeneration of its fibres but this was only slight. The orifice of the aorta was small (0.019 cm.) ; otherwise the aorta was normal. Microscopic examination of the central nervous system showed no alteration of the nervous elements. There was a slight congestion of the bulb and of the pia mater. There was a pronounced oedema of the brain.
The kidneys and liver were normal in appearance but some of the liver cells showed beginning fatty degeneration. Thus the fatty degeneration of the heart mentioned above was the only important lesion and this was not enough to have caused death.
The chemical examination showed a more interesting fact. Undoubted traces of morphin were found in the brain, spleen, and kidneys, but especially in the liver the drug appeared to be stored up. From washing this organ with water and alcohol, a solution was obtained which gave very positively all the tests for morphin. Apparently, a considerable amount was stored up in the body.
Washings of macerated liver showed the presence of morphin by the following tests, Bouchardat's—iodide of potassium, Marmes—double iodide of cadmium and potassium, Hessler's—double iodide of mercury and potassium, Frohde's sodium molybdate and sulphuric acid and also the perchloride of iron test.
Thus, the author states, after thirteen days of abstinence, there was still morphin stored up in the body. It would appear, therefore, that this poison may remain a long time in the viscera and that its presence in the organs may explain by a sort of auto-intoxication the late symptoms which are sometimes observed in morphinists, long after the withdrawal of the drug. Cases, he states, have been known to die in collapse several days after apparent cure.5
Pilliet-1887.8
Pilliet, referring to pathologic studies on dogs, states that two adult dogs were injected daily with morphin for three weeks, increasing 1 centigram every two days, until at the end of this time they were getting 10 cgms. daily. By this time the animals had lost their appetite and were in a state of habitude. Abscesses developed and they were killed before suppuration could cause complicating lesions.
Aside from skin and subcutaneous changes near the seat of the injections, the liver showed fatty degeneration, the cut surfaces being opaque and glistening. The course of the change was traced. It began as an intracellular steatosis which was present and equal over all the lobules. There the fat collected in droplets in the cells near the subhepatic vein. In other parts there were small areas around the portal veins where the cells were not distended with fat. There was no trace of embryonic infiltration or of proliferation of the connective tissue.
The author reports finding fatty degeneration of the liver, less marked than in these dogs, in two morphinists, one a case of tabes and the other a case of cancer of the uterus. The brain examined in different places showed many granular bodies between the white and gray substance, bodies which were also collected in masses in the corona radiata. In the gray matter the external neuroglia and the small cells seemed normal but the layer of large cells showed a considerable decrease of these elements as compared with normal dogs, in which they are very numerous. There was no connective tissue proliferation. The muscles and other tissues appeared normal. The author states that other alkaloids and certain mineral poisons cause a similar steatosis of the brain and liver, so that the changes observed are not specific.
Saratschow-1895.6a
Tschisch reports the work of Saratschow relative to histologic changes in the central nervous system in acute and chronic morphin poisoning. In what follows the abstract is given in full:
"The author, on the invitation of the writer, set himself the task of checking and elaborating the investigations of the latter regarding the alterations in the central nervous system in connection with morphin poisoning (Ueber Veriinderungen des Riickenmarks bei Vergiftung mit Morphium, Atropin, Silbernitrat and Kaliumbromid. Virchows Archiv. Bd. C. Referat im Neurol. Centralbl. 1885), employing for this purpose the latest methods of fixation and staining ; in addition, the author studied the condition of the central nervous system after a fairly long period of continued poisoning with morphin. Saratschow discovered indubitable alterations in the central nervous system in connection with both acute and chronic poisoning (longest test-156 days). In the case of acute poisoning the vascular alterations were more distinctly marked than in chronic poisoning. These were: dilatation and hyperemia of the vessels, thickening and homogeneous clouding of the capillary walls, increase in size of the endothelial nuclei; coagulated exudation with form elements in the subadventitial spaces of the larger vessels. In chronic poisoning the author found alterations of a degenerative character; the greatest alteration occurred in the ganglia of the anterior cornu of the spinal cord. The author, having made a careful study with regard to the significance of the vacuolization in the ganglion cells, came to the conclusion that the vacuolization of the nerve cells is not to be regarded as a similar symptom from the point of view of its origin and its significance; that it is undoubtedly a pathological symptom. No pathological alterations were found in dogs who were put to death a month after the discontinuance of the administration of morphin; since in every other respect the animals had been subject to the self-same conditions, and since the method of fixation and staining was likewise the same, the absence of alterations ascertained by the author serves as further confirmation of the fact that it really is the morphin that causes the alterations in the central nervous system attributed to it. Although the alterations found by the author greatly resemble in general those observed in connection with poisoning through other poisons, as e.g., with lead and quicksilver poisoning (N. M. Popoff) etc., nevertheless, the picture of the alterations due to morphin poisoning is so characteristic, that Saratschow draws the conclusion therefrom that 'the presence of characteristic and specific alterations due to morphin poisoning may not yet be denied.' "
American Textbook of Applied Therapeutics-1896.7
"The symptoms produced by an habitual indulgence in opium in any of its forms—no matter how introduced into the system—may conveniently be divided into two great classes, namely, those produced on the body and the effects on the mind of the victim. Of these, the mental deterioration is the most serious by far. The effects on special organs or on the constitution as a whole, even after the victim has been accustomed for years, it may be, to enormous doses of the drug, scarcely ever assume so grave a form that he may not be cured of the evils in a comparatively short time. The chief difficulty of the whole treatment of opium-eating or morphin-injection, or any of the rarer forms of indulgence in the narcotic, lies in the great resistance that the patient's mental perversity offers to any attempt at cure. It is the craving for the unnatural stimulant that must be fought; if this craving is overcome, all the rest is comparatively easy."
"In the earlier stages mental brilliancy, lasting as long as the stimulating effect of the drug persists, is sometimes noted. Some of the best speeches and a few excellent literary productions are said to have owed their inspiration to opium. However, that may be, the physician rarely sees the victim in that stage. When the morphinist consults him, not generally of his own volition, but induced to do so by the vigorous persuasion of his friends, whom he cannot easily refuse, as his habit generally makes him dependent on them, he is in most instances a physical wreck; often his finances are in the same condition, and his morality is weak. This latter statement refers, however, chiefly to his morality in respect to the habit. About opium and morphin these people always lie. When they cannot obtain the drug by fair means, the other kinds are resorted to without scruples. Stealing the drug or the money for it, forgery of prescriptions, and bribery of attendants are some of the means resorted to; otherwise the victims may be of excellent moral character. It is seen, therefore, that the craving or appetite for the poison is the cardinal point in the whole horrible habit, and, as already mentioned, the physician will have to devote his energies chiefly against this craving, and in trying to overcome it he will find the greatest difficulty."
Franz Nissl-1897-98 7
In a preceding article published in the same year, the author calls attention to a distinction which he makes between chronic poisoning and subacute maximal poisoning. He says that in inducing experimental poisoning time is not the only factor, the amount of the dose being another, and that it is his opinion that most of the experiments performed to date are more fitly designated as subacute maximal poisonings than as chronic poisonings. He continues:
". . . In this kind of poisoning the process extends from a few days to months, according to the poison selected. As long as possible, the animal receives daily the maximal quantity of poison which, it has been decided, will just not jeopardize any longer the life of the animal through the individual dose. The experiment ends with the death of the animal. The amount of the maximal dose for each poison is easily ascertainable by means of experiments suited to the purpose. In my experience, if the maximal dose has been chosen correctly, death occurs in the individual animals, treated with the same poison, at about the same time. Subacute maximal poisoning yields the clearest, most distinct results; it is, therefore, the most suitable method for investigating the action of the poison. The experiment in subacute maximal poisoning is, therefore, primarily a preparatory experiment. If by means of subacute maximal poisoning exact information has been obtained as to the mode of operation of a poison, the amount of the dose which will not immediately endanger life, as well as the limits of the habituation to the poison, which generally develops, and if the preparatory experiment has shown which kinds of cells resist the poison most and least, then the real experiments in poisoning can be made, i.e., experiments in .acute and chronic poisoning; in both of these, again, various degrees may be produced. The form of chronic poisoning which is of special importance to us is the one in which a dose which of itself will not produce any violent symptoms is administered for as long a time as possible."
In an article dealing with the anatomy and histology of the nerve cell, and the pathologic changes which it undergoes in experimentally induced poisoning, the author states:
"It should never be forgotten that acute maximal poisoning is an extremely brutal form of invasion, and that this kind of poisoning is primarily a preparatory experiment, as I have explained elsewhere. For this reason it is entirely superfluous to fear that the conditions of cell-degeneration which I have described and pictured may perhaps appear only in quite isolated and sporadic cases. That such is not the case is seen at once from the investigation of those gray foci (Herde) in which cells of similar structure are close to each other. To be sure, as regards those classes of cells which inhabit the gray masses without being closely packed, or which are found singly amidst other cells, as is the case with the motor cells, the situation is somewhat different; it would then be just a matter of a poison which, like the tetanus toxin, for example, acts directly on the cells of the motor class.
". . . The cells altered by morphia show essentially different conditions from those shown by the elements—just described—which had undergone alcohol poisoning. First to be emphasized here is the fact that the unstained substance of the cells is distinctly altered. It has become only slightly stainable. We, therefore, observe in the tissue long dendrites—mostly apical processes—consisting entirely of unstained substance. But the stained substance, on the other hand, is also altered. It is decidedly rarefied a little; in particular, the intensively stained parts are much less strongly colored. In general, the stainable substance is, as a whole, more weakly tinged, and the individual portions of the substance have become smaller. It is difficult to come to a very definite decision with regard to these points, as on account of the alteration of the uncolored substance the colored parts no longer stand in clear relief against the uncolored. The nuclei, too, become smaller and appear to be more darkly colored. At the same time, they frequently lose their roundness and become slightly oblong. Altogether the poisoned cells are decidedly smaller, narrower, the basal parts more angular, and the dendrites proceeding from here show more distinctly."
J. Ewing-1898.7°
The author reports the autopsy findings in cases of chronic morphin poisoning with superimposed acute poisoning, in the following:
"Morphine Poisoning.—The present series includes three cases of poisoning by morphine.
"Case I.—Male, 45 years. Had been addicted to the use of the drug for several years, finally using 16 grains of morphine hypodermically injected, each day, and had suffered in an extreme degree from the general symptoms referable to this habit. Was said to have eaten nothing for one week before death. After a very large injection, quantity unknown, was brought to hospital in coma, dying within a few hours with typical symptoms of morphine poisoning.
"Autopsy six hours after death. There was moderate fatty degeneration of heart-muscle, liver, and kidney. The lungs were very cedematous, and the viscera showed marked venous congestion. The pancreas was very atrophic, being largely replaced by fat. There was considerable oedema of the brain.
"Fixation, Lang's fluid, 24 hours.
"The chief feature of the changes revealed by Nissl's stain was a marked diminution in the quantity of chromatic substance in nearly all cells of the central nervous system. The chromatic bodies in the cells of the cord, medulla, cerebrum, and cerebellum, were very deficient in size and number or often entirely absent. Purkinje's cells were very faint, showing a few small, narrow chromatic bodies, very regularly arranged in concentric rings. Nuclear changes, as a rule, were not noted.
"In the medullary nuclei, there were some cells still retaining chromatic bodies of considerable size but markedly subdivided. In some of these cells the nuclei were shrunken and often eccentric.
"The quantity of yellowish granular pigment was much more abundant than usual in most regions of the central nervous system.
"Case IL—Female, age 24 years. Had been addicted to the moderate use of the drug for a few months only, but was able to attend regularly to her work as dressmaker. In a fit of despondency she took a large quantity of morphine by mouth, and in spite of treatment, died twelve hours later, with typical symptoms of morphine poisoning.
"Autopsy six hours after death.
"There was extreme oedema of the lungs, and marked venous congestion of all viscera, but no other gross lesions of importance.
"Microscopical examination. Van Gehuchten's fluid.
"The stichochrome cells throughout the central nervous system showed changes which in many respects were peculiar. When examined with a low power, these cells appeared to have lost their normal distinctly striated appearance, many appearing diffusely and unevenly stained while their outlines were extremely irregular. When examined with a high power, the above peculiarities were found to consist in a marked subdivision of the chromatic bodies which were enlarged and very irregularly and minutely subdivided.
"In the medulla the large cells were extensively altered, further, by the appearance of clefts in the cell bodies, similar to those described in other conditions by Nageotti and Etlinger. In this region also the loss of chromatic substance was very uneven, some areas of the cells appearing completely bleached, others showing the minute subdivision, while in some spots the chromatic masses seemed fused together.
"The majority of the cell nuclei were shrunken and markedly eccentric, while the loss of chromatic substance was as a rule greatest about the nucleus. About many of the nuclei irregular masses and rods of chromatic substance were heaped. . . .
"Throughout the cortex changes of a similar character were noted. Purkinje's cells of the cerebellum were less affected than the cells of most other regions.
"The irregularity in the effects of the chromatolytic process, the ragged appearance of the cell borders, the appearance of clefts, and the frequency of central chromatolysis associated with eccentricity of nuclei, are the features peculiar to this case. The last mentioned abnormality is of special interest in connection with the well-known effect of morphine upon the peripheral nerve filaments.
"Case III was identical in all important respects with Case II."
G. Jacottet-1898.7`
Jacottet in a study of the changes in the brain cells, spinal ganglia and in certain experimental poisonings gives the following in connection with morphin poisoning:
"We find in the literature two publications on the medullary lesions caused by experimental morphinism. The author of one of these suggested by the Russian physician, Mierzejewsky, is v. Tschisch. The other is by Sarb6. The second work is the only one which we considered in our experimental study.
"We gave the morphin to our animals hypodermically in an aqueous solution of the hydrochloride.
"Observation V.
"A rabbit 2% months old, weighing 680 gs., received on April 7, 1896, 1 cu.cc. of a 1:500 solution of the drug. This dose was increased daily until the 29th of the same month when it was 6 cm." From this date until May 6 a 1:200 solution was used up to an average of five or six cm" daily. Then, from the 7th until the 22nd of May, the solution was increased in strength to 1:100; the amount of the solution injected each time varied from four to six Pravaz syringefuls. Finally from May 23 until death occurred, we made use of solutions of 3:100, given in the same amounts as the preceding.
"On the 19th of June the animal was chloroformed. "Its weight was 1220 gs.
"Total length of treatment 73 days.
"Total amount of pure morphin hydrochloride 2.53 gs. "Total gain in weight 540 gs.
"Observation VI.
"A rabbit, 5 months old, weighing 2,000 gs., received from April 11 to the 19th of June, 1896, exactly the same daily amount of morphin as No. V, but the intoxication was continued under the same conditions until August 7.
"On August 8 the animal was extremely thin and was chloroformed.
"Its weight was only 1,570 gs.
"Total length of treatment 118 days.
"Total amount of pure morphin hydrochloride 7.31 gs.
"Total loss of weight 430 gs.
"In these two animals at autopsy the brain and medulla did not show even meningina hyperemia observed by v. Tschisch ; macroscopically everything was normal.
"Microscopic Examination.
"Only the methods of Nissl. Sadowsky and Ramon y Cajal, make it possible to determine certain unusual conditions in the large cells of the anterior pons and of the lateral portions of the gray medullary substance. The remainder of the spinal axis was not changed. Here again we have to deal with a granular degeneration of the chromatin. This change in the protoplasm was very wide spread; it affected almost all of the motor elements of the brain. Here and there were found intact cells. In some instances the perinuclear chromatin bodies were most affected; in others those lying in the edges or prolongation of the cell.
"The partial degeneration of the chromatin, as seen in alcoholism and as Sarb6 describes it, was usual.
"The nucleus was never altered. The granulation of the nucleus was sometimes affected to a remarkable degree, but it was not broken. We did not observe 'homogeneous tumefaction' spoken of by our predecessor, although our rabbits had received much more morphin than had his. He had only given to one of his 0.09 gs. of poison in 42 days, and to the other he gave only 0.11 gs. in 71 days.
"Our studies on this state of chromatin of the intervertebral ganglia led us to the conclusion that they had undergone no appreciable change."
Ottone Barbacci-1899.7''
In an article dealing with the nerve cells in their anatomic, physiologic and pathologic relations, the author reviews the findings of several investigators in acute and chronic morphin poisoning in what follows:
"In connection with morphin poisoning Nissl found in the cells of the cerebral cortex a slight coloring also of the interstitial substance, so that here, too, the dendrites were visible for an unusually long stretch. The stainable matter is somewhat rarefied and all of it is more lightly colored. The individual stainable cells are also smaller than normal. The nuclei are smaller. more oblong, and appear darker than usual. The cells themselves are altogether smaller, narrower, their basal parts more angular, and the dendrites starting from here appear more prominent in consequence.
"The alterations found by Sarb6 were not very different.
"Saratchoff subjected dogs to acute and chronic poisoning. The alterations are predominantly in the anterior cornua of the spinal cord. They appear in slighter degree in the cells of the bulbus and the cerebral cortex. In acute poisoning the lesions show themselves principally as swelling of the cells, loss of the processes, and formation of vacuoles. In chronic poisoning granular degeneration of the protoplasm is predominant. The chromatic substance disappears more or less entirely; the protoplasm takes on a gelatinous appearance; the nucleus does not take the stain well; the contour of the cell becomes indistinct.
"In a dog which died of morphin poisoning amidst violent symptoms of excitement in the motor area, Caterina found the cells of the cerebral cortex, whatever their type, more or less seriously altered. Where the alteration had made most progress, there can be seen dispersed, trabecular remnants of the very pale protoplasm, throwing into relief the more heavily, though diffusely, stained nucleus. Forms of homogenization with atrophy of the nucleus and irregularity in the contour of the nuclear membrane also appear.
"Mankowsky (Russ. Archiv. f. Pathol. etc., Vol. 6, 1898) experimented with guinea-pigs, rabbits, white mice, and dogs. In each species one animal was subjected to acute poisoning, one to chronic, and a third was put to death while quite healthy; the same brain-parts were extracted from the latter for microscopic examination as from the animals experimented upon, i.e., the anterior cornua of the spinal cord, the ganglion cells of the medulla oblongata. the pyramidal cells of the cerebrum, and the Purkinje's cells of the cerebellum. In connection with acute poisoning, varying degrees of chromatolysis were observed; in the cell body these consisted of the atrophy of the Nissl bodies in the periphery of the cell and the alteration of their form and size in the center of the same, close to the nucleus. In the protoplasmic processes the chromatic cells are disintegrated. The entire cell becomes sinuate. The nucleus and the nuclear cell remain unaltered. In connection with chronic poisoning the chromatolysis in both the cell body and the processes attains the highest degree—atrophy of all differentiation whatever in the chromatophile substance. The latter becomes a powdery, irregularly dispersed mass. In the cell body as well as in its processes, there are formed in consequence vacuolar foci (Herde) free of chromatin. The processes, moreover, are heavily thickened. The contours of the nuclei become irregular, clot-like. The cell gives the impression of being in the process of decay; the cells of the cerebrum are most seriously affected.
"Trains induced acute, subacute, and chronic poisoning in dogs, rabbits, and guinea-pigs, and examined the various sections of the cerebro-spinal axis by means of various methods. In the acute cases he found minimal lesions. The elements retain their spinous investment, and only seldom does one see a few rosary-like swellings. A few elements show indications of incipient peripheral chromatolysis. In subacute poisoning there are pronounced diffuse alterations of the protoplasmic processes in the cerebrum and the spinal cord, consisting in a varicose condition which always begins at the finest ramifications. The axis cylinder is normal. Very few alterations in the cerebellum. Varicose condition of a few peripheral processes of the cells of Purkinje. Nissl's method reveals very slight alterations; a few cases of peripheral chromatolysis in the cells of the spinal cord, and powdery decay up to complete disappearance of the chromatin in the cells of the ganglia of the sympathetic. In chronic poisoning all these symtoms are intensified. In addition, there appears another alteration, not yet described—the presence of vacuoles in the protoplasmic processes; the author considers them a condition of oedema which attacks the process in a cellulipetal direction. Furthermore, there is incipient alteration of the neural process, which shows small nodules and swellings near the cell body. The elements showing most alteration are those in the cerebral cortex. All this was observed by means of Golgi's method; Nissl's method reveals peripheral chromatolysis in the spinal cord, which may go as far as the complete disappearance of the chromatic substance. Central chromatolysis or displacement of the nucleus is never seen; the intervertebral ganglia or those of the cerebellum show only slight alteration, but those of the sympathetic system show considerable—always by way of peripheral chromatolysis. The author draws the following conclusions from his investigations: Very important lesions are found in connection with morphia poisoning, and these increase with the duration of the action of the poison. These alterations begin at the finest ramifications of the dendrites and proceed towards the cell body and finally into the protoplasm. The absorption of the prickly processes usually precedes the appearance of varicose swellings. Normal cells can always be found between those which have suffered severe alteration. According to the author and contrary to the statements of the majority of other observers, the alterations perceptible by means of Golgi's method are more serious than those brought to view through other methods of staining the neural cytoplasm. The cells most altered are—in decreasing series—those of the cerebral cortex, those of the spinal cord, those of the ganglia of the sympathetic system, those of the cerebellum, and—least of all—the intervertebral ganglia.
"In two cases of chronic poisoning Jacottet found the intervertebral ganglia intact, while in the cells of the spinal cord he observed chromatolysis, which was at times perinuclear and again peripheral."
S. C. Fuller-1899.8
The author noted that in making red cell counts, using Gower's solus tion as a diluting fluid, there were found on microscopic examination in specimens from morphin users crystals closely resembling the smaller crystals of morphin sulphate. They were colorless, some needle-like, others tapering to a point and others forming narrow parallelograms. These crystals ranged in size from about 30 to 60 micro-millimeters in length and from 3 to 6 in width. The crystals were more abundant in cases using about 25 grs. of morphin daily and usually absent when less than 3 grs. was taken. Where crude opium or laudanum was being used the crystals were few or absent. Marked anemia was present in these cases. Experiments with morphinized rabbits, carried on by Prof. Rockwell of Boston University School of Medicine, showed the same phenomenon in three of five pairs of rabbits used. In two pairs of animals to which not more than 11/2 grs. of morphin were given daily the crystals were not demonstrated.
The author thinks that this phenomenon may prove valuable as a means of determining when the patient is off the drug.
L. E. R. Lancelin-1902.°
Lancelin in a study of the role of the leukocytes in infections during morphinism," states that in intoxications the body is weakened in all of its means of defence. Its various organs functionate less actively and less efficaciously, the large glands being altered in their elements. The liver cells degenerate and the organ becomes sclerotic; its functioning suffers and it becomes unequal to the task of neutralizing the noxious principles and the bacterial secretions. The kidneys are unable to throw off the daily waste, the glomerular filter is unequal to its task, its cells are so affected that poisonous products are reabsorbed and autointoxication is often added to the original intoxication.
In general, the secretory epithelium undergoes marked alterations which naturally affects the bactericidal qualities of their secretions.
It is principally, however, in lessening phagocytosis that toxic substances render the organism abnormally receptive. The /eukocytes, even admitting that they are sufficient in number, do not possess the necessary phagocytic activity and the conflict is most unequal.
The virus is not directly affected, but is assisted indirectly by the modification undergone by the body. Altering as they do the defences of the body, toxic substances hinder or prevent the destruction of the pathogenic organisms, which thus become more numerous than they would in a normal individual.
All of this, he states, applies in every way to morphinism. Morphin, in whatever form introduced, rapidly depresses the organism because of the enormous quantity which accustomed individuals take. Daily experience amply demonstrates this, when we see how easily the least wound suppurates and how frequently abscesses of all sorts develop. The vitality of their tissues is reduced to a minimum and healing takes place slowly.
Lancelin then undertakes experiments using eighteen rabbits and guinea-pigs and dividing the experiments into two series. In the first he studies the reaction of morphinized animals in the presence- of virulent organisms; in the second he uses organisms whose virulence has been attenuated by heat or ageing. In each of these experiments he uses three animals, one chronically intoxicated for at least a month, one intoxicated for eight days, and one control. In each instance he makes blood examinations and leukocyte percentage determinations and a brief microscopic examination of the lesions occurring in the different organs.
In review the author states that the morphinized animals show less resistance than the healthy animals and that if they recover the recovery is delayed. Especially was the depressive effect of the morphin shown when attentuated cultures were used. He states that it is not due to an increased virulence of the organism, as Bouchard has shown that protoplasmic poisons affect the development of the pathogenic organisms as well as the defence cells of the body. It is, he claims, in the body itself that the cause of the lessened resistance must be sought. He states:
"In the case of morphinism, the resistance of the body appears to be active, at least in so far as the leukocyte reaction is concerned. This reaction is intense and reaches in virulent infections as many as twenty or twenty-one thousand white cells to the cmm. In attenuated infections where the body's defense takes a longer time to become established, this reaction goes as high as twenty-six or twenty-seven thousand. These facts prove a normal functioning of the leukopoietic centers, which are probably not affected by the morphin."
After a series of experiments of considerable speculative interest but which perhaps were not carried out in a convincing number of animals he concludes:
1. "Infections act more quickly on a morphinized soil."
2. "The more rapid death of the animal is not due to an arrest of the leukocytic function."
3. "It is not in the quantity but in the quality of the leukocyte that the cause must be sought."
4. "Death is due to an arrest of phagocytosis resulting from the inhibition of the leukocytes by the morphin. The chemical proof of this is given in our last experiments."'
R. Krafft-Ebing-1904.12
"Morphine never injures so profoundly the psychic organ as does alcohol, but I have never seen a morphinist that was psychically intact. Intelligence, it is true, is practically spared, but the highest mental functions—character, ethic feeling, self-control, mental energy, and force—always suffer. The fully developed morphinist is an individual weak in character and will and without energy, who should receive, under criminal prosecution, the benefit of attenuating circumstances, and who in the care of his interests and duties should always be given help.
"In severe cases we find, in addition, weakness of memory, especially defect in the power of exact reproduction, difficulty of intellectual activity that may reach the degree of torpor, occasionally psychic depression reaching even marked dysthymia and taedium vitae, great emotionality, and, in general, profound deficiency of resistive power to affects; and besides, there may be episodically nervous restlessness, excitement, even attacks of fear due to vasomotor causes, and occasionally visual hallucinations."
"Symptoms due to sudden total abstinence occur after about six hours. The patients become relaxed, weak, incapable of standing, have symptoms like those of cholera nostras, profuse sweating, general tremor, painful anxiety, restlessness going on to weeping, raving, and violent demand for morphine, which immediately removes all troubles due to abstinence, and the patient may not hesitate to commit a crime to get the drug.
"Not infrequently, following these symptoms of abstinence, there is an hallucinatory delirium lasting several days—a true delirium of inanition, which, on account of its numerous analogies with alcoholic delirium tremens, may well be called the delirium tremens of morphinism (numerous visions of animals; episodically also obscene deliria, mainly of frightful content, agrypnia, tremor). In severe cases the symptoms of abstinence and inanition may reach a point of dangerous cardiac and respiratory weakness, collapse, and coma, and make it absolutely a vital indication to administer morphine.
"Symptoms of intoxication and abstinence in the form of elementary psychic disturbances, anorexia, and asthenia, may exist a long time, even months, after the drug has been withdrawn."
R. Luzzato-1905.13
In connection with a study of glycosuria produced by morphin, this author endeavored to find out the relationship of chronic morphin intoxication to this condition. His results, he states, were in accord with Faust's findings that all symptoms of morphin poisoning disappeared or became very much less acute with the chronic use of the drug. He concludes as follows:
"Glycosuria disappears with gradually developing addiction to morphin."
Stewart Paton-1905.14
"The mental symptoms of morphinism are varied and in the main have certain general characteristics which aid in the recognition of the disease. In the earlier stages, and before the patient has become a thorough slave to the habit, he is apt to show marked symptoms of hysteria. At times states of apprehensiveness and anxiety develop; the patient readily becomes flustered, often develops mild suspicions, is decidedly pessimistic and hypersensitive, affirms that old friends are forsaking him, that all his actions are misinterpreted. Soon ethical defects become more or less pronounced. A tendency to lie, particularly when questioned in regard to his failing, is developed, and as action becomes more difficult the fabrications increase in scope and variety. The sense of duty becomes more and more blunted till it finally disappears.... The whole character deteriorates and the defects are in many respects similar to those belonging to certain stages in alcoholism although they are altogether different from others.
... Hallucinations and delusions may develop, although they are not usually present unless the morphinism is complicated by alcoholism or the effects of some other drug.... Moreover, these patients are not uncommonly sufferers from psychitesthesias, paraesthesias, or less frequently hyperaesthesias."
Thomas C. Allbutt-1905.16
"Autopsy is rare in cases of uncomplicated morphinism. The only important point herein is the state of the heart. Schweninger and others allege that fatty degeneration of the heart is to be found in these cases after death. I have no positive facts to guide me to an opinion on this matter; but on clinical grounds I have seen no reason to suspect its presence, either in the course of malady or in a prevalent mode of death. To adduce, in proof of this assertion, cases in which other organic degenerations are found is to offer proof of too much or too little. The testimony of the best authors seems to be opposed to the belief that fatty heart is a direct consequence of morphinism. Wittowsky's papers are helpful in this aspect of the matter. The observations of Binz on the fall of blood-pressure in acute poisoning of animals by morphine have little bearing on chronic poisoning. Bell says that chronic poisoning by morphine promotes hepatic steatosis."
F. Chotzen-1906.1°
This author reports the histories of two cases who during withdrawal showed marked psychoses, the clinical picture of which was quite clearly amentia. He states:
"Nearly all authors agree that the chronic abuse of morphin, in contradistinction to other poisons, gives rise to no special psychosis (Levinstein, Erlenmeyer, Obersteiner, Heiberg, Deutsch, Wernicke, Krpelin, Ziehen, and others). When mental disturbances occur in chronic users of morphin, these are referred for the most part to contemporary complicating poisoning by other poisons, especially alcohol, chloral hydrate, and cocain (Jastrowîtz, Erlenmeyer, Kr.pelin, Ziehen, and others). On the other hand, in the opinion of authors in general, mental disturbances arise nearly always during abstinence, on sudden withdrawal, and without exception in confirmed addicts. The occurrence of these psychoses of abstinence seems to be limited to morphin withdrawal: the complications are of little moment, especially the most frequent one, due to the combining of cocain with morphin. This leads to no symptoms at all during abstinence, while chronic intoxication quite uniformly produces psychic disturbances: in this respect, as Kriipelin says, it most closely resembles alcohol. On the contrary, there is a decided contrast in this regard between it and morphin, which Ziehen particularly notes.
"The forms of mental 'disturbance in abstinence from morphin do not offer the well defined picture of a specific psychosis, yet they have by no means been sufficiently analyzed. For the most part they bear the mark, according to Levinstein's characterization, of the delirium tremens of mania for morphin. It becomes directly apparent, however, on examining the description of the psychoses occurring during abstinence from morphin given by a number of authors, that very different states are included there. All the writers have described anxiety states, depression, and mania."
. .. But it is very evident from the different descriptions, especially from the great variation in duration of the psychoses, that by no means are all the psychoses of morphin abstinence to be regarded alike, and therefore not all can be brought into comparison with the same object. We must expect the utmost, difference of conditions in morphin abstinence. Sometimes there are abnormal persons who become morphin addicts, such as Erlenmeyer refers to as disposed to certain neuroses and psychoses, Levinstein as nervous individuals. Jastrowitz describes a strong tendency, present in every crisis of delirium, to influences predisposing to the occurrence of abstinence psychoses. Whenever depression, ideas of compulsion, and the like have followed withdrawal, it can he safely assumed that they were present before using morphin, were in abeyance during that time, and reappeared on withdrawal,
"Sometimes also indications are apparent of a congenital psychopathy. Erlenmeyer and Jastrowitz describe hysterical symptoms as a regular manifestation. the former describes psychic disturbances of a purely hysterical nature, and Kriipelin has seen during morphin withdrawal a distinctly hysterical twilight condition with convulsions. But aside from this, pure abuse of morphin is rare, that use commonly being accompanied by abuse of chloral, alcohol, cocain, or chloroform. With the exception of cocain, it is doubtful if these take part in the causing of psychoses in abstinence, and at any rate they arc not uniform as to the form of the disturbance that occurs. They arc accompanied by a great multiplicity of congenital and acquired psychotic manifestations, but, because of the confusion of these, there is a strong probability of very complicated and obscure psychoses. The close resemblance also to alcoholic delirium tremens is certainly supported in many cases by more than a mere external similarity when alcoholism is a complication. I have seldom had an opportunity to see an uncomplicated case, but variations of alcoholic delirium have been noted everywhere in recent literature, sometimes very decided ones.
"Recently I have been privileged to see in close succession two chronic morphin addicts with well marked psychoses subordinated to a very definite clinical picture, that of amentia. In my belief this observation has nothing accidental about it, but it indicates that an analogy for the psychoses of morphin abstinence is to be expected far less in alcoholic delirium tremens than in the group of exhaustion psychoses and those related to them, an enlightening aid in understanding a large part of these psychoses."
* *
"Closely following withdrawal treatment occurred an acute psychosis, beginning with marked confusion, and characterized by complete disorientation, misconception of the patient's surroundings, restlessness, and fantastic delirium. At the same time a notable loss of strength occurred, so that speedy demise was prognosticated by the physicians. On improvement of the complete disorientation there appeared extreme delirious illusions of vision, afterward numerous auditory illusions, hallucinations of smell, and hypochondriacal sensations, all connected with wholly phantastic dream delirium and confabulations. Active, restless movement supervened, impulsive, altogether incoherent speech, and a strong tendency to be diverted, but nevertheless continual attraction to external impressions for the most part falsely conceived. His memory was much weakened and there was particularly extensive disturbance of apprehension. He failed to understand simple questions, heard wrongly, mistook himself for another person, misunderstood, and misinterpreted. Even in periods of rest illusory misconceptions were frequent as to his surroundings and perception of events. What he apprehended in part correctly was transformed in a characteristic way into very strange and impossible images, just as in dreams.
"His disposition changed constantly, being at one time excited, at another anxiously depressed, at another exalted with a tendency to ideas of grandeur.
"His strength was much depleted, his heart action bad, his speech without force and completely exhausted.
"After eight weeks a rapid improvement began, and in a few days he was cured and had completely recovered his insight.
"The entire course of this attack, the acute origin with physical failure, the prominence of the dream confusion, the great difficulty in apprehension, the illusional and hallucinatory falsifications of perceptions, the extreme restlessness, the duration of eight weeks followed by recovery, all these are the well known characteristics of the group of psychoses to which Kriipelin has given the name of `exhaustion psychoses,' and the instance related falls under the designation amentia.
"No other form of psychosis deserves consideration. No infection was present, the temperature only once reaching 37.8°. In disproof of katatonic disease stands the absence of all motor symptoms in the narrow sense, and in disproof of manic confusion the preponderance of disturbances. of perception and the concurrence of the psychosis with physical exhaustion.
"All these indications hold also for the second case, which ran its course entirely under medical observation. I myself merely had an opportunity of examining the patient once, and must therefore be satisfied with reporting the case briefly."
"These two psychoses correspond and afford typical examples of the form of disease described. There is no characteristic which enjoins their association or requires their separation. Especially do they agree with certain rare forms which stand out a little 'from the number of acute psychoses arising in connection with exhausting causes by reason of the fact that in them the disturbances of perception and the illusional dream life, the confusion and the absolute incompetence for any kind of associative effort rule in fact the whole picture and recur with invariable regularity in their etiology in connection with insufficient nourishment, constant loss of sleep, and business strain.
"But when again we find in the psychoses reported above a series of traits described by authorities as characteristic of the psychoses of morphia abstinence, this does not show a specific character in these psychoses, for these traits belong also to the exhaustion psychoses and show rather a correspondence of recognized morphin psychoses with those of exhaustion.
"So also the disturbance of speech which characterized both our cases is mentioned as an abstinence phenomenon (Levinstein). It is an almost constant attendant of the exhaustion psychoses referred to. In those too we find the development in two stages, a very stormy delirious initial stage and a later stage of repose, in which the associated insufficiency becomes most certain. Here occurs the tremor which Krapelin speaks of as found also in the delirium of collapse, and which Ziehen says is very frequent in all exhaustion psychoses. Thus the resemblance to alcoholic delirium which is always emphasized in respect to morphin psychosis, is pronounced also in these exhaustion psychoses. Actually in one of our cases, a young woman who certainly had not been drinking and who became ill herself only from insufficient nourishment and loss of sleep while fatiguing herself in the care of a sick relative, it was said in the beginning of her illness that she was 'typically delirious.' If it is possible for known cases of the acute delirium tremens of morphin users to correspond with the psychosis of collapse, so too the description of the chronic or milder forms reminds us of similar phenomena caused by exhaustion. Thus Erlenmeyer describes as a mild form of delirium tremens a half conscious dream condition of laughing, muttering, gesticulating (as in a dream) on the borders of hallucination, at other times numerous hallucinations and amnesia. Levinstein mentions a chronic form, developing in the period of intoxication and continuing into the period of abstinence, with changeable temper, generally settled cheerfulness, interrupted only for brief periods by anxiety states. Some individuals pass the day in depression, at evening are mildly excited and subject to sensory delusions, to tremor of the hands and muscular contractions. So they can be drawn out from their depressed or excited frame of mind. This description bears considerable resemblance to mild hunger delirium in course of pregnancy or the puerperium and other chronic wasting processes.
"We do not think that in the characteristics referred to we sec the signs of a special variety of morphin abstinence psychosis, but believe on the contrary that a part of this case coincides with the psychoses of other inanition processes."
"We might look for the origin of this psychosis in events which result also in `exhaustion' of the nervous system. Jastrowitz says that acute mental disturbances occur most readily in morphin abstinence when little nutriment is taken and loss of sleep, diarrhea, and agitation have still further depleted the body. The remotest cause of disease therefore lies in an intoxication of the body. In our two cases the illness followed withdrawal or coincided with it. Complications do not enter into the question here. In the first case morphin was taken during the last part of the time only in small doses and no new injury occurred: in the second case strenuous activity was entered on and a more decided degree of exhaustion resulted than when the patient began withdrawal. During this period the premonitory symptoms soon appeared and, after renewed excess of fatigue, the outburst of the severe psychosis. But here too the chronic morphin intoxication with its consequences must first have prepared the soil on which so severe a bodily and mental prostration could develop. In both cases the physical weakness was very decided, in the first case threatening life. Neither cocainism nor alcoholism can properly be charged with these psychoses, as has been said above. The symptoms supply nothing characteristic of either of these factors; on the contrary, they point entirely to the form of malady known as the result of exhaustive disease. And such is chronic morphinism with its severe infirmity. Great impairment of nutrition and metabolism constitutes a major symptom in morphin intoxication, and it is this which finally brings the body into the perils especially to be dreaded during withdrawal. Levinstein says that in nearly all patients a condition of weakness supervenes on the second or third day of withdrawal, which may precipitate a dangerous collapse when the withdrawal is sudden, and which indicates that violent psychic disturbances tend to follow abrupt withdrawal. The concurrence of physical and psychic disturbances leads to the conclusion that they spring from a common source, and the typical clinical picture in our two cases shows that this conclusion is justified. When Jastrowitz writes 'conformably to the recognized character of known forms of disease, obscure psychoses, sometimes mania, melancholia, or true paranoia do not arise, as in chronic alcoholics, as a consequence of withdrawal, either during or following it,' it may be remarked that withdrawal, by hastening physical collapse, favors also the corresponding psychoses, and that no pronouncement is valid respecting the psychoses of collapse, which are not reckoned in this connection. Therefore, when we undertake to enumerate the psychoses of morphin abstinence, we believe, with regard to psychopathic conditions and other complications, that in many cases consideration should be given primarily to the psychoses of the amentia group, as we prefer to call them with Stransky. "Certain predisposing causes also play a part here in my opinion. Both of the patients reported above were neurasthenics. These and sufferers from insomnia are especially susceptible, as Knipelin and Jastrowitz remark, to morphin. But in our experience it is also the neurasthenics who incline to develop exhaustion psychoses at the first opportunity. Repeatedly did we learn from our patients that they had previously had symptoms of chronic nervous exhaustion. In this way it seemed to us certain that in many instances patients who recover from amentia do not become altogether well, but still manifest nervous symptoms, as Racke and Stransky have also observed. This is where the danger of relapse exists for these patients.
"That those who become morphin addicts are plain neurasthenics and victims of insomnia affords an explanation of the remarkable fact that in chronic poisoning of the body there appears a symptom complex to which has been ascribed a very precise etiology, that of pure nervous exhaustion. If morphin does away with the fatigue symptoms of the neurasthenic, possibly at the same time it interferes with physiological regeneration and so increases the fatigue symptoms to the point of exhaustion. But this theory applies also to a single administration of the poison ; for the common view that recovery consists in the removal of certain metabolic products is placed on a secure foundation by the proof of an exhaustion antitoxin and an opposing antitoxin (Weichardt). Whether we believe that morphin exerts its peculiar effect by accumulating normal metabolic poisons or by forming specific poisons by its decomposition (Marme), the psychic disturbances in either case would be the results of a chronic intoxication like the other symptoms of morphin intoxication and abstinence, which latter Jastrowitz insists are not antithetical to the symptoms of poisoning, but are the same and have merely been retarded for a little while by fresh doses of morphin and its tonic effect. Such a tonic effect is recognized, although it is not known with certainty what it depends on. In the second of our cases it was clearly seen in the beginning of the illness, for after every injection the speech became once more forceful and the articulation distinct, but after the effect passed off was greatly diminished and uncertain. We see the same in chronic alcoholism in respect to the anxiety, the tremor, and other symptoms of abstinence. So the symptoms of abstinence are the regular symptoms of intoxication and their psychic components are to be regarded as products of chronic poisoning. Jastrowitz explains that chronic morphinism creates neurasthenia. Thus chronic poisoning indirectly produces the symptom complex of amentia. We also know from other clinical experiences that this symptom complex is evoked by toxic, especially by infectious influences. Consequently, although it is closely associated with exhaustion as a cause and is quite uncomplicated, as we must recognize, still the separation from cases of infectious origin cannot be substantiated. Nothing further will be said of this here; there may possibly be an opportunity elsewhere. Stransky and Strohmayer have recently treated this question amply, and the former agrees with the majority of authors that it is impossible to separate toxic infectious conditions from conditions of exhaustion, a fact borne out by clinical observation. The more hallucinatory form of confusion, which Kfapelin no longer distinguishes from the asthenic form, is often seen in acute infectious diseases. Easy transitions occur between the 'delirium of collapse,' amentia,' and 'infectious fatigue conditions,' and we especially see in chronic infectious diseases how the symptoms of exhaustion, which here find their physical correlation in cachexia, mingle with those we ascribe to intoxication.
"The symptoms of exhaustion are the expression of disordered nutrition, whose origin, apart from that in internal disturbances of metabolism, may lie in a toxic causation from without, whether from organic or from chemical poisons (see Stransky). If Stransky attributes amentia specifically to the indirect effect of organic poisons, the cases reported here furnish evidence that chemical poisons have precisely the same effect. Finally, as we see in the action of morphin, they produce the same cachexia as chronic infectious diseases, and in chronic morphinism with its severe gastrointestinal disturbances and its effect on almost every gland there is abundant opportunity for autointoxication by reason of secondary disturbances of metabolism. Of special interest here is the analogy between very frequent intoxication with a chemical poison and alcoholic intoxication. We must recognize too the exhaustion symptoms of the alcoholic cachexia (author); the symptom complex of this intoxication may also be distinguished from the amentia group. A difficulty arises here in separating Korsakoff's psychosis, which is closely related to this. This relationship is shown by the development of psychoses of the amentia group on a foundation of chronic alcoholism, and by the transition to it of cases of polyneurotic psychosis, in which the delirium is often designated 'asthenic.' We must recognize exhaustion symptoms, therefore, as the indirect result of poisoning by chemical poisons."
Otto Schtitz-1908.16a
The author presents the autopsy findings in a woman, 23 years, who suffered from an arthritis and died from morphin poisoning. The histologic findings are given in the following:
"In Marchi preparations from the upper level between the first and second cervical nerves there was considerable degeneration of the nerve fibres in the entire extent of the posterior columns and in the course of the nerve paths beside the cerebellum, evidenced by a variety of large round or more often irregular, sometimes distinctly annular, black spots. The posterior and anterior roots also were marked with black streaks.
"In Weigert-Pal preparations from adjoining regions, patches of degeneration of nerve fibres were perceptible, particularly in the posterior columns, and also isolated patches at the edges of the lateral columns. The patches were small, diffusely distributed, and stood in no perceptible relation to the course of the blood vessels. In the posterior column the columns of Go11 and of Burdach had undergone the same change. The areas of the afferent nerve roots were unaffected. In sections from the cervical cord at different levels, stained with hemalum-Van Gieson, picrocarmin. and nigrosin, there was perceived an increase of the glia in the column of Goll with increase of nuclei, appearing in small patches and coinciding with the degeneration. The blood vessels were unaltered. There were no signs of inflammation. The gray matter, particularly the ganglion cells, was unaffected.
"In the thoracic cord also the anterior and posterior roots, the borders of the lateral columns, and to a less extent the posterior columns in Marchi preparations were similarly degenerated. In sections treated by the other methods referred to above there were no pathological findings.
"In the lumbar cord the lateral and posterior columns were less degenerated, but the anterior and posterior roots very much so.
"Finally, thin plates were removed from the sides of the left forefinger, previously treated with Marchi, in such a way that the digital nerves were included with their branches. In nearly all the preparations nerve bundles were seen which were affected throughout. their whole length and so altered that they seemed to have been dyed a deep black. There was no appearance of inflammation or of atrophy. The muscle fibres were normal in size, transverse stripes, number and appearance of nuclei.
"So there was degeneration of the nerve fibres in the lateral and posterior columns throughout the whole extent of the spinal column, but diminishing from above downward and limited in extent; degeneration of the roots; disappearance of nerve fibres with mild sclerosis in the posterior columns of the cervical cord in the form of small scattered groups; degeneration of peripheral nerves.
"Anemic and cachectic conditions and diabetes were summarily excluded as etiological factors for spinal cord disease in this vigorous, well-nourished, far from bloodless girl. Chronic alcoholism did not come into consideration. So it would have been necessary to dispense with an acceptable explanation for the spinal cord findings if another chronic intoxication had not been established in the anamnesis."
John V. Shoemaker-1908.17
"The generative functions are depressed by opium, and in chronic poisoning the menses cease and men become impotent while under its influence. Passower has demonstrated that the abuse of morphine may occasion atrophy of the female organs. In a patient observed during two years it was inferred, from the early failure of menstruation, that the atrophic process began in the ovary. During the period named the uterus diminished in size by 1 2/10 inches and atrophy of the vulva was evident. The secretion of urine is lessened, but the bladder is often rendered irritable and urine is passed frequently in small quantities. On the other hand, partial paralysis, with retention, may occur. Althoff has proved experimentally that degeneration of the posterior columns of the cord in the dormal region was produced in dogs who had for a long period received hypodermic injections of morphine. This observation is in consonance with the clinical fact that morphine habitues, in some instances, manifest ataxic symptoms. This drug increases the amount of urea and phosphoric acid eliminated."
Ch. Achard, H. Benard, and Ch. Gagneux-1909.18
These authors report experiments and conclusions as to the action of morphin on the properties of the leukocytes and their value as a means of diagnosing morphinism. The article is given herewith in full except for the protocols of the experiments:
"After having read, in a recent article, of the action of anesthetics on leukocytes, it seemed interesting to determine that of another drug of a similar nature and the use of which is not less extensive in daily practicemorphin.
"This alkaloid diminishes both the resistance and the activity of leukocytes. It should be remembered that the resistance of these cells is measured by cytolytic deformities, produced by a hypotonic salt solution. As to its mechanical action, its value is estimated by the capacity for absorbing either foreign cells (sterile yeast of thrush), or dissolved substances, the incorporation of which into the protoplasm gives rise to vacuoles stained with neutral red (erythrophilic vacuoles); in vivo, after an injection of morphin, the resistance and activity of the white blood cells is lessened, but this effect is only transitory. This is especially clear as regards the activity of the cells."
* * * *
"In vitro, in very weak isotonic solutions of morphin, the white cells also lose their resistance and activity. We have even determined, with M. Ramond, that, when they have previously absorbed yeast or when they have been filled with erythrophilic vacuoles, remaining in the morphin solutions makes them give up these corpuscles and vacuoles. They are, therefore, manifestly sensitive to morphin.
"As the sensitiveness of the organism to the morphin becomes readily apparent and since tolerance to this poison is easily established, we have been led to investigate whether the sensitiveness of the leukocytes to morphin would vary as well, in individuals addicted to the alkaloid, as in those not addicted.
"In vivo, we observed that an injection of 4 cg. of morphin chlorhydrate, in a morphinist, scarcely affected the leukocytic resistance or activity, while the same dose, in an individual not addicted, clearly lessened these two properties."
"These results made us search further and measure the sensitiveness of the leukocytes to the morphin, in order to see if it would not be possible to identify the morphinized subjects in this way. With this in view, we placed the leukocytes in a series of alkaloid solutions and sought one that maintained a minimum leukocytic activity. The solubility of this solution gave the measure of the sensitiveness of the while cells to the morphin. This sensitiveness was noted, as well for the incorporation of the sterile yeast, as for the formation of erythrophilic vacuoles. The action of the yeast was perhaps more precise, but that of the neutral red was certainly simpler and seemed to us to suffice for the clinical investigations."
"In individuals not morphinized, we note that, with the yeast, the sensitiveness of the leucocytes to morphin is expressed by 500 and 400 and in morphinized subjects it is only 100 and 200; with the neutral red, its value is 500 in the former and 300 to 500 in the latter. You will note that the subject with the least tolerance to morphin, among the addicted ones, is also the one whose leucocytic sensitiveness is expressed by the lowest value in the two reactions.
"We know that young children are more sensitive to morphin than adults. But, we have also learned that their white cells are less tolerant to the alkaloid."
"The tolerance of the leucocytes for morphin continues for some time after suppression of the toxic substance, then it disappears. We observed this in an asthmatic individual, who was subjected for a few days to morphin injections.
About 15 days after the remedy was stopped, he still showed quite a leucocytic tolerance, but at the end of a month, he returned to normal."
* * * * *
"Heroin, which is a derivative of morphin, causes analogous reactions as far as the white cells are concerned.
"In vivo, it lessens in the same way the leucocytic activity."
"In vitro, the leucocytes undergo in the solutions of heroin of 1:200 a lessening of resistance and activity. But this sensitiveness to heroin is less also in a heroinist."
"In order to account for the specificity of the reaction, we endeavored to find out if, in spite of the chemical relationship between morphin and heroin, there was any difference in their action. But we found that the leucocytes of a heroinist acted like those of a normal individual with respect to morphin, and that, reciprocally, those of a morphinist reacted like those of an individual normal with respect to heroin."
* * * * *
"The measurement of the leucocytic sensitiveness to morphin and heroin, by the neutral red method, gave us confirmatory results."
* * *
"Summing up, the leucocytic reaction, which we designate under the name leuco-diagnosis, makes possible the identification of morphinism, the supervision of demorphinization, and the distinction between heroinism and morphinism "
O. Jennings-1909.19
Jennings states that "the morphia habit" is a "psycho-somatic affection" in which mental and physical troubles are interdependent, conditioned the one by the other. As to pathology, he states that Burnett has shown, by post-mortem examinations, certain microscopic changes described as follows:
"The stichochrome nerve cells stained diffusely and unevenly and were very irregular in outline, the chromatic bodies were enlarged and minutely and irregularly subdivided.
"The cells of the cortex and medulla were extensively altered, showing clefts of the cell bodies, uneven loss of, and minute subdivisions of, the chromatic bodies. In areas these bodies were massed and fused together. Their greatest loss was about the nuclei, but about some nuclei, the chromatic substance was heaped in irregular masses and rods.
"The irregularity of the chromatolytic process, the ragged cell borders, the clefts of the cells and the frequently central chromotolysis with the extruded or eccentric nuclei, were distinguishing changes in this case."
M. Chartier and D. Morat-1909.2°
The findings on the changes in the blood picture during chronic morphin and heroin intoxication as described by these authors are covered in Morat's Thesis of 1911, from which we shall quote at length. Therefore we shall not consider their joint paper here.
C. L. Case-1910.21
This author states that there is no structural pathology in chronic opium intoxication but that pathologic changes are entirely of a functional nature. The nervous system is under the benumbing influence of the drug and all vital functions are sluggishly and imperfectly performed. What is commonly spoken of as "the craving" is not a craving at all, but a physical condition.
E. Kriipelin-1910.22
"The psychic effects of morphin, so far as they are known at present, differ widely from those of alcohol, and consist in facilitating and stimulating intellectual processes and in rendering psychomotor activity difficult. This behavior, which has been confirmed by studies of morphin addicts, enables us to understand that morphin intoxication passes into a sort of pleasurable dreaming, in which confused shifting images take possession of the imagination, while at the same time a gentle relaxation fetters the limbs. Morphin, therefore, is by no means intrinsically a hypnotic, as physicians still generally believe. Rather do we understand that morphin addicts feel themselves stimulated under the influence of the remedy to mental work which they could not accomplish in their ordinary constant condition of purposelessness. But the most dangerous feature of morphin action" is unquestionably the peculiar, restful sensation of pleasure, which differs very markedly from that of alcoholic intoxication in the total absence of signs of psychomotor excitation, of conscious desire to be active."
"Still further, in certain cases a disease-picture may develop in consequence of actively increased agitation which bears a very close resemblance to the delirium tremens of drunkards, and in which the uncertain movements and the tremor of the hands is accustomed to appear in the same manner. In other cases the preponderance of auditory illusions suggests rather the delusional state of alcohol or cocain. Usually this state lasts only a few hours or at any rate not more than a few days: once only have I seen it prolonged over several weeks. Here an unmistakable abuse of alcohol had taken place with the object of withdrawal. The criteria of distinction from alcoholic delirium recently proposed by Abraham (exaltation with corresponding mixture of delirious outbreaks, slight disturbance of perception, of attention, and of orientation, positive insight into the disease) neither characterize the majority of delirious episodes in morphin addicts, nor differentiate them adequately from alcoholic delirium. The infrequency of such delirium, even in those markedly addicted, indicates that different influences are at work here from those usual in alcohol and cocain; perhaps one of the other drugs so freely used by morphinists should come into consideration here. Apparently morphin withdrawal favors the occurrence of such delirium, like feverish diseases or wounds. Now and then hysterical seizures are observed during the withdrawal period, with sensory illusions and convulsions.
"In other tracts also of the nervous system the tremendous overturning becomes apparent which is produced by withdrawal of the accustomed stimulant. There occur involuntary movements and spasms in the limbs, spasms of the calves, contractions of the limbs, trembling, asthmatic attacks, spasm of the diaphragm, convulsive cough, paresis of accommodation, tenesmus, vesical spasms and paralysis, rumbling, rattling and pain in the stomach, vomiting, cardiac palpitation, but especially fainting and dangerous collapse with sudden rapid diminution of heart action, which under some conditions recurs repeatedly and may directly end in death. The secretory activities, which have been depressed under the influence of morphin, exhibit a quick transitory increase of considerable extent: saliva, tears, and perspiration are secreted abundantly, and prolonged severe diarrhea occurs: sometimes albumen appears in the urine. Appetite declines greatly; the body weight rapidly diminishes. The severity of the symptoms of withdrawal varies to an extraordinary degree. It depends on the size of the dose, the duration of addiction, the general condition of the patient, and the .individual tendency. Sometimes the disturbances are limited to a little diarrhea, sweating, excitability, and insomnia, while in other patients the condition becomes exceedingly severe, threatening life. My experience, however, does not include an instance of withdrawal wholly without discomfort. When the manifestations are very mild or the health altogether undisturbed, morphin is unquestionably being supplied clandestinely. Once I learned of a deception of this sort by finding the patient, a colleague, enjoying a sleep when I paid him a visit."
Daniel Morat-191123
This author reports the most extensive pathologic studies of chronic opium intoxication which our search of the literature has revealed. These studies were made on patients undergoing Sollier's method of rapid reduction and detoxication. Morat's findings were the result of the study of thirty-four cases selected from one hundred forty-six. This selection was made in order definitely to exclude all cases suffering from intercurrent conditions—abscesses, malaria, acute alcoholism, syphilis, etc.—which might have vitiated the results.
To follow satisfactorily the blood changes, four specimens were necessary, the first before any reduction in the morphin, the second three days after withdrawal, the third fifteen to twenty days after withdrawal, and the fourth forty days after withdrawal.
The Blood in Morphinists and Heroinists During Intoxication.—In
these studies it was found that there were no marked changes in the blood during the intoxication—while the patients were taking their usual dose—and the pallor of some of these cases should be attributed to peripheral vasomotor phenomena rather than to anemia. Studied by the method of Hayem, coagulation was nearly normal although in many cases a delay of 10 to 15 minutes was noted.
Red Cells.—While the number of red cells was variable, most patients showed an increase—the count being generally about 5,000,000, —in one case 5,825,000. The increases were usually in young people who in general had many abscesses.
The hemoglobin was lowered varying between 0.90 and 0.70—in one heroinist 0.55. The size of the red cells was normal, only a few macrocytes and microcytes were found, the latter being the more noticeable. There was no poikilocytosis. The color of the red cells was normal and granular red cells as shown by cresyl-blue were not more common than in normal blood.
By the method of Vaquez 24 and Rubierre the resistance of the red cells as compared with normal blood was diminished. With the same solutions of NaC1 normal blood hemolyzes completely at 0.30, beginning hemolysis being at 0.38, while that of morphinists and heroinists completely hemolyzes at 0.36 with its beginning at 0.44.
White Cells.—Morphin intoxication does not affect the number of leukocytes which varies between 5,000 and 10,000. In cases with abscesses the number is higher-14,500 and 15,500 respectively in two cases.
The same is true of the differential count which remains normal except in cases with intercurrent infections. The polynuclear neutrophiles vary between 52 and 70 per cent. Eosinophiles vary from 0.5 to 3 per cent. We find sometimes, but rarely, a mast cell. The transitional forms vary between 0.5 and 4 per cent; the large mononuclears between 2 and 5 per cent. Finally, the average number of mononuclears is 8 to 12 per cent and that of the lymphocytes from 12 to 24 per cent.
In dry smears, however stained, there are generally found degenerative changes in a certain number of leukocytes. A long series of such examinations together with wet-chamber examinations in the same and different individuals indicate these changes are not artifacts. They are practically absent in normal blood while in morphinists 2 to 3 per cent of the polynuclears and many of the large mononuclears show alterations of shape and color, vacuoles in the nucleus and protoplasm, a reduction of the protoplasm to a reticulum and a scattering of granules in the polynuclear eosinophiles. These changes are also seen in wet-chamber specimens stained with cresyl-blue while staining with neutral red shows two to three per cent of the nuclei stained—an indication of death of the cell element.
The white cell resistance was studied by the method of Achard and Ramond 25 and after comparing a large number of counts of intoxicated patients with those of normal individuals, it was determined that the total figure expressing the resistance of the polynuclear leukocytes generally varies in intoxicated individuals between 280 and 400, having usually an average of between 290 and 360, while healthy individuals present a figure falling between 432 and 469. The figures expressing the resistance of the mononuclears, lower generally than the figure of the polynuclears, vary between 250 and 300 and are again lower in the case of intoxicated persons than those expressing the resistance of mononuclear leukocytes in normal individuals.
To sum up, cases of morphin intoxication offer lower leukocytic resistance than normal individuals.
The Blood of Morphinists and Heroinists during Rapid Withdrawal.
Coagulation takes place more rapidly even than in normal blood.
Red Cells.—During the period of reduction and especially in the first days of abstinence, definite morphologic changes occur in the red cells,—macrocytes, microcytes, poikilocytes and deeply colored red cells being found in much larger numbers than during intoxication. There is also an increase in the granular red cells which return to normal about the fifteenth day after withdrawal. The red cell count increases up to about the. fifth day of abstinence from 500,000 to 1,000,000 or more; then it decreases to normal or below by the eighth to twelfth day.
The hemoglobin in one cubic millimeter of blood, determined by Henocque's hematospectroscope and the double chamber of Hayem, is lowered during the reduction and withdrawal, reaches its original point again about the thirtieth day and still later returns to normal.
The percentage of hemoglobin in the individual red cell diminishes much more during the period of increased cell counts but increases again more rapidly than the hemoglobin content per cubic millimeter on account of the decreased number of red cells.
The red cell resistance, lessened during the period of intoxication, increases during withdrawal reaching its maximum about the tenth day; then slowly diminishes until the fortieth or fiftieth day when it reaches its original state, a little below that of the normal cell.
During the period of reduction and above all during the days which follow withdrawal, the total number of white cells per cubic millimeter undergoes an increase analogous to the increase of the red cells. It is important, however, to state that the leukocytes do not reach their maximum on the same day as the red cells. It is, in fact, three or four days after the latter that the curve of the white cell reaches its peak. It is but slightly increased during the reduction. The ascending curve of the leukocytes rises quickly from the beginning of withdrawal until about the fifth day after and remains stationary until about the seventh day. The number of leukocytes exceed the original number by an average of from 5,000 to 11,000, sometimes doubling and trebling it. Then the curve begins to descend more slowly than it rose, falls to the original figure on from the twentieth to the twenty-fifth day after withdrawal and thereafter remains stationary.
Leukocyte Picture.—Variations in the leukocyte picture follow in general a remarkably constant course which can be expressed thus:
1. During the period of reduction and of withdrawal, great polynucleosis.
2. During the period of convalescence, mononucleosis and eosinophilia, together with the appearance of abnormal specimens.
3. The return to normal on from the thirty-fifth to the fortieth day after withdrawal.
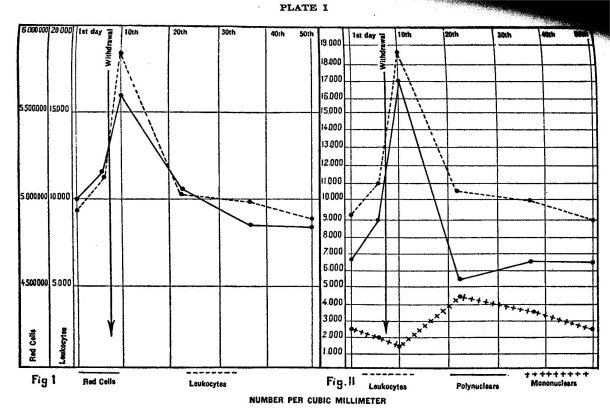
The red and white cell counts are shown in Plate I.
The author gives in detail the numerical, morphologic, and structural changes in the white cells at various stages of treatment and points out their diagnostic and prognostic significance. These and certain degenerative changes begin with the reduction of the drug and end with the completion of convalescence. The leukocytic resistance is lowered during the period of withdrawal.
The same hematologic changes were observed in a tolerant dog when withdrawn from the drug. These changes were also shown in two patients who had undergone gradual reduction treatment when, afterwards, they were subjected to the detoxication treatment of Sollier?s
In review Morat states-
1. "In red cells, a cell increase, an alteration of the cells, an increase in cell resistance and during convalescence, a complete return to the normal state.
2. "In the white cells during the period of withdrawal, a marked polynucleosis followed by a mononucleosis, the appearance during the mononucleosis of eosinophiles and abnormal forms, pronounced leukocytic changes, a lessening of leukocytic resistance and during convalescence a return to the normal state."
From now on, according to Morat, we definitely can recognize the similarity between these non-febrile reactions of the period of detoxication and the reactions in cases of acute infections which, however, have also an elevation of temperature, but which present polynucleosis during the acute period, mononucleosis with the appearance of eosinophiles and of large macrophages during convalescence, and also an increase in the red cell resistance and a decrease in the white cell resistance during the infection, with a return toward normal during convalescence.
Morat reports as a result of studies of the resistance of the red cells of persons suffering from chronic morphin or heroin intoxication as compared with those of healthy individuals as follows:
"The red cells of an individual intoxicated with morphin or heroin undergo, in solutions containing one or the other of these poisons, a hemolytic change of an equal degree to the change in the red cells of healthy individuals in the same solutions. There does not, therefore, appear to exist in the red cells of intoxicated individuals, a selective affinity toward one or the other of these two poisons. On the other hand, in a healthy individual, in morphinists and for the greater part in heroinists, at least in those of the latter class in whom the intoxication is recent, heroin is definitely more destructive to red cells than morphin."
His studies of the white cell resistance were inconclusive.
The secretions and excretions.—The Liver. Morat found that the area of liver dullness in intoxication was lessened as a rule in cases of long standing and normal or slightly enlarged in recent cases. Whether small or large the liver was sensitive and in some cases hepatic colic was noted. The author goes on to state that the liver function is retarded in chronic opium poisoning, the bile being diminished and urobilin and bile pigment appearing in the urine. He states that the glycosuria reported by certain authors was not observed by him.
Morat further states that in detoxication the liver function is excessive, the organ becomes tender and enormous quantities of bile are produced. This hyperactivity reaches its height about the time of complete withdrawal. He states that while this over-secretion of the liver quite reasonably might appear to be a means of getting rid of stored morphin Sollier was unable to recover morphin from the vomitus or stools at this time. He concludes that if morphin is excreted at this time it must be in the form of some derived product and that the greatly increased secretion of the liver is due to the detoxication treatment, to the release of the liver cells from the effect of the drug, and to increased nervous stimulation due to the removal of the drug's inhibitory action.
In the digestive tract the glandular elements likewise take on increased functional activity where formerly—during intoxication—they were inhibited. Salivation becomes intense and diarrhoea is a prominent symptom.
Albuminuria, the author states, does not result from chronic opium intoxication. During the period of suppression there is a marked oliguria, the urine is highly colored and contains phosphates and urates which persist often until the eighth day after withdrawal and are recovered from time to time during convalescence.
About fifteen hours after complete withdrawal there is often pain in the kidney regions, the oliguria becomes more marked with sometimes complete suppression of short duration. At this time the urine always contains albumen from ~/2 to 11/2 gms. per liter and often larger amounts. This albumen consists almost entirely of serum and lasts but a few days.
Microscopic examination of the urinary sediment shows granular or cellulo-granular casts, the cells being polyhedral mononuclears from the uriniferous tubules and irregular cells in process of destruction.
Free cells found in the urine are the polyhedral vesical cells, small cells of the kidney tubules and destroyed polynuclears.
The author believes that the albuminuria is not due to a passive congestion of the kidney because of the rapidity of its development or to vasomotor disturbances or to a nephritis of auto-toxic origin caused by the presence in the blood of the products of cellular disintegration. He attributes the albuminuria to what Feullié 27 describes as "leukopathic albuminuria."
Feullié states that in certain affections there exists in the blood "pathologic leukocytes" or sick leukocytes, which, finding in the kidney an excretory Organ, appear in the urine in the form of leukocytic casts and scattered cells. And, according to him, this leukocyte exodus through the kidneys causes albuminuria in several ways:
I. Directly through destroyed leukocytes.
2. Through the passage of albumen of the blood plasma, through the opening momentarily left by the leukocytes, during their diapedesis.
3. By the products set free in the blood by the sick leukocytes which act directly on the glomeruli, causing what Feullié calls "leukopathic glomerulitis."
It seems, therefore, that it is on the basis of this last theory that we must explain the albuminuria of detoxication:
The leukocyte changes observed in the blood of individuals during detoxication, the rapid appearance of the albumen, its appearance at the same time when the changes of the leukocytes in the blood are most marked, the presence in the urine of the leukocyte casts, the oliguria which one can explain by the obstruction of the urinferous tubules and which always ends with an outpouring of cellular débris, seem to place the albuminuria occurring in morphinists during detoxication in the group of leukopathic albuminurias described by Feullié 28
Morat states that the renal apparatus rapidly returns to normal on about the eighth day after withdrawal and kidney sequelae do not occur.
Abscesses, the Skin, the Teeth and the Sexual Apparatus. While many years may elapse without it, most cases of morphinism sooner or later develop infection with abscess formation in the localities most frequently used for the injections. These abscesses are painful, form slowly and usually contain a fetid pus rich in bacteria, generally staphylococci or streptococci. They may become confluent.
During detoxication when there is no suppuration and when all reason for infection has passed with the last injection from eight to twenty days after withdrawal new abscesses may develop. These are different from the preceding occurring in places where for long periods no injections have been made and they develop rapidly. The pus is benign or serous with few or no bacteria. The author considers them a phenomenon of counter-irritation due to the attraction of leukocytes to places where there existed previously a latent inflammation, insufficient in itself to produce an abscess. This sudden accumulation of leukocytes, the author states, can be explained by the presence in the blood at this period of degenerating leukocytes which find in these localities points of attraction.
The Skin. During detoxication there is an over-activity of the sweat glands which often becomes excessive.
Frequently after detoxication Morat observed a marked desquamation of the skin, principally on the forearms, hands, and legs. This is usually flaky but may occur in large strips. The nails during intoxication are dry and brittle and after withdrawal show definite transverse markings.
The teeth, always affected by the use of morphin, also suffer during detoxication.
The Sexual Apparatus. Although the sexual activity is inhibited as a rule in morphinists, the author has observed a number of cases where there was no alteration of the function. The same is true of the cessation of menstruation in women.29
F. McK. Bell-1911.3°
This author dwells more particularly on the psychic changes. He directs attention especially to the visions and hallucinations of the patient, his insomnia, ill-humor, despondency, transitory brilliancy, etc., inability for consecutive mental work and moral inertia; "he becomes untruthful, unreliable and unethical."
Physically, the author states, there is found fatty degeneration of the heart and liver in most cases, an anemia manifested by the ashy or leaden pallor, so well known. Nutrition suffers and the patients become thin and flabby, the pupils are small and react slowly to light. There is thirst and loss of appetite. He divides the effects into three states: First, "before the system becomes demoralized," the stage of exaltation; second, the stage of intoxication, when the physical and mental changes commence to manifest themselves, and third, the stage of cachexia with progressive weakness, emaciation, shrivelled, parchment-like skin, oedema of the extremities and nephritis. The disposition becomes morose and sullen and the patient is scarcely conscious of his environment.
A. A. Van Egmond-1911.31
In a study of the pulse frequency in chronic intoxication, van Egmond rendered tolerant a dog weighing 6.7 kg. by injecting 4 cg. morphin every two days. At the end of 16 days daily injections were given up to the.19th day. Van Egmond states:
`After this time the same dose of morphin no longer exerted any narcotic effect on the dog.... During this whole period observations were made as to whether there took place a tolerance of the vagal center to the dosage used. For this purpose after an injection the pulse was taken at first every five minutes and then, if there appeared a constancy, every hour. During the first doses in the course of about 20 minutes the pulse dropped from 140 to 50 and then to 60 and 80 and remained at this point for several hours. On the slower pulses there was noted irregularity. This condition remained unchanged usually for seven to nine hours or at the most there was a slight acceleration of about 10 beats. After 24 hours, on the other hand, the slowing of the pulse had completely or nearly completely disappeared. On the appearance of tolerance this picture varied only slightly. The dog which no longer showed nausea or narcosis reacted to every injection of morphin with a slowing of the pulse. In tolerant dogs the pulse action varied from the normal only by a very slight difference in duration. After 4 to 5 hours usually the pulse frequency increased. Also many times after one or two hours the pulse went back more quickly, if the dog which was no longer narcotized moved about the room. Also the degree of the slowing of the pulse appeared to be slighter after general tolerance set in, the number dropping between 80 and 100.
"Since it was not the object to produce a tolerance of the vagal center through the daily injection of a constant dose of 6 mg. per kilo, the doses were therefore increased. From November 5 to 10, 0.1 g., from November 11 to 25, 020-.5 g.; on November 30, the dose was 1. g. which was continued up to December 10. At the end of these experiments the dog weighed 4.4 kg. Therefore he finally reached a dosage of 023 g. per kilo.
"During this increasing tolerance from time to time there were days on which the dog returned to the old dosage of 8 mg. per kilo. At these times the pulse frequency was studied. Such examinations were made if there was complete tolerance at those doses so that the dog showed no vomiting, nausea or narcosis. The result was that the dog after complete tolerance to the subcutaneous injection of 1. g. morphin hydrochlorate reacted to an injection of the original dose of 4 cg. (1/25 of the tolerant dose showing no symptoms) with a slowing of the pulse from 120 to 80, which appeared within 25 minutes and lasted for 5 hours. The lower limit of the sensitiveness of the vagal center to morphin was determined: 1 mg. per kilo or 1/230 of the dose to which the dog was tolerant lowered the pulse frequency from 120 to 82 for a period of 21 hours. A dose of 0.08 mg. per kilo on the other hand acted only weakly; the pulse dropped from 122 to 114. Since the minimal dose at which a slowing of the pulse appeared in normal dogs was found to be 0.04 mg. per kilo, these experiments show that in the highest grade of tolerance of the whole body to morphin the sensitiveness of its vagal center to this poison frequently remains the same. There is a slowing of the pulse on the administration of a small dose of morphin after as well as before tolerance is established; the final value for this action does not increase at all or at most only slightly. In any case a strong reaction of the vagal center lasting for hours may be produced by the injection of 1/230 of that dose to which the, cerebral cortex and the vomiting center are completely tolerant. As pointed out above it is interesting to note that in intolerant animals the vomiting center reacts to practically the same small dose as the vagal center."
K. Schneider-1913.82
This author discusses the question of the etiologic relationship of addiction to the development of a psychosis in a case whose history he gives in detail. He states:
"While at least the acute form of cocain psychosis is undoubted, the possibility of producing psychoses is altogether absent in the case of morphin. Especially have the chronic morphin psychoses been abandoned by all the authorities. The earlier view taken of this was different. Thus A. Erlenmeyer, a student of morphinism from the very outset, was firmly convinced that chronic morphinism gives rise to psychoses with an absolutely bad prognosis. The majority of cases are incurable forms fitting in the picture of feeblemindedness. `The most frequent form of intoxication psychosis is madness. Ideas of persecution and of grandeur, with or without hallucinations, form the disease-picture, whose existence betrays the psychical weakness.' Out of fifty histories detailed by him he described only a single case in which pure morphinism led to an incurable psychosis . . ."
"Here again it is very questionable whether we ought to regard morphinism as the cause of the psychosis; a combination with some disease belonging to the dementia precox group is far more probable in the light of general experience. It is certain that we do not know the features of a typical morphin psychosis, and so we always stand in doubt regarding diagnosis; as Jaspers also says, 'in a given case the causal association is free from objection only when there is a typical psychosis frequently observed as connected with the poison. In any other case there is a possibility of our having to deal with quite a different psychosis in a person chronically poisoned in a similar way.'
"Must a 'chronic morphin psychosis' always take the form of a combination? The following case will not settle this question but it is so deserving of attention and so full of problems and mysteries that a searching narration and discussion may prove very rewarding."
"Now let us ask ourselves what manner of disease did this patient have, in the course of which so singular a psychosis can find a clinical place?
"To summarize briefly: a man psychopathic from youth, who used morphin occasionally from his twenty-third year, habitually from his twenty-seventh, and drank heavily besides, began to hear voices about his twenty-eighth year and to develop delusions, particularly those of a jealous nature. The voices were heard in his deaf right ear, in which rustling and music had previously been frequently heard. Breaking off both poisons produced no improvement; on the contrary, a very strange paranoid condition developed, having sensory illusions in all fields, particularly hearing, and this lasted till his thirty-sixth year. Then very suddenly all his ideas of grandeur and persecution ceased, complete insight regarding his disease was gained, and after six years' residence in the asylum the patient was discharged as practically cured and capable of resuming his occupation. But the sensory illusions remain almost unchanged, although they are no longer misinterpreted. Since his discharge the patient has become nearly as pronounced an addict again to morphin and heroin, and now presents nothing beyond the ordinary picture of a morphin addict, incapable of work, without energy, tormented by all sorts of neurasthenic complaints, degraded in his finer ethical feelings.
"The first point that attracts our attention is the coincidence of the psychosis with the development of a difficulty in hearing causing unilateral deafness ..."
* * * * *
". . . Even if we assume as a basis an individuality markedly psychopathic and manifestly paranoid, this psychosis, which moreover exhibits illusions of all the senses, is not susceptible of explanation as due to the ear disease. "If we exclude this possibility, only two others are left, so that all diagnostic considerations culminate in one question: is this an intoxication psychosis or a paranoid form of dementia precox complicated in its course and picture by intoxication? At the time the disease began undoubtedly Dr. N. had used much alcohol and morphin, assuredly also some cocain. In its beginning, with voices and delusions of jealous import and with the violent conduct resulting, the psychosis reminds one strongly of the delusions of alcohol or cocain. In the further course of a cocain psychosis it is natural to think at most of the paresthesia that accompanies it and the illusive conceptions they lead to, but of nothing further, and moreover after all Dr. N. took so little cocain that it does not seem credible this can be the origin of the entire psychosis. Alcohol would seem more probable, but even in the most carefully studied alcohol psychoses such an event has never been observed. The many systemic aspects, the long continuance of the psychosis with complete abstinence without the occurrence of alcoholic degeneration, the ten years of hallucinations in spite of continued insight, the remarkable character and purport of the actual delusions of hearing, the absence, to all appearance constant, of any signs of delirium, of any condition of clouded intellect, the lack of any alcoholic element in the personality of Dr. N. make the supposition of a paranoid alcohol psychosis likewise hard to entertain.
"Can morphin be the still operative source of injury, the cause of the psychosis? We have seen that the existence of chronic morphin psychoses is even more doubtful than that of chronic cocain psychosis. Even if we should grant that the cases of chronic morphin psychosis observed by Erlenmeyer did not rest on delusion, still we cannot bring his cases into accord with the case of Dr. N. He lays stress on the unfavorable prognosis (in contrast with the abstinence psychoses of morphinism) and the termination in incurable feeblemindedness. Also the circumstance that the renewed morphin intoxication does not cause the psychosis to light up again undoubtedly adds difficulty to the view of morphin as an etiological factor. It certainly, cannot be a typical instance of disease, experience argues against its being a morphin psychosis, but in the life of Dr. N. morphinism and psychoses of atypical forms so completely dominate the picture that the possibility of a causal relation cannot be entirely excluded.
"Or does a combination of intoxication and dementia precox exist, like that in Gr.ter's cases? Had not insight into the disease, complete correction of all illusory ideas been attained, there would be no doubt of such a combination, morphinism and dementia precox would be looked upon as independent children of a common degenerative origin. The nature of the sensory illusions, the thinking aloud, the senseless perversion of spoken words, the ideas of bodily influence, the strange sequence with its manifold physical content, the negativistic conception contrary to circumstances, the retirement within himself—these symptoms completely justified the diagnosis of `chronic paranoia' before the termination was known. Certainly there resulted no dissolution of personality, impairment of will-power was not observed, and the affective life remained undiminished. If it is beyond question that Dr. N. is defective in personality, and especially shows a degree of indolence and dulness in his reaction to this process, still it would be doing violence in the matter to see in his condition a schizophrenic defective state, that is absence of any mania, absence of any intimation of peculiarity and eccentricity, and the good-natured dulness does not exceed what is observed in other instances after years' use of morphin. There is no evidence of impaired personality in the form of dementia precox. But yet this psychosis does not conform to the type recently described by Krnpelin as paraphrenia, which occasionally develops in chronic alcoholic intoxication and which does little harm to the internal relationships of personality, giving rise to no clearly marked disturbances of disposition and will. Only the classical manifestations come up for consideration, but one of the principal symptoms is totally absent, the secondary occurrence of sensory delusions often appearing years after the onset of the disease. But what positively rules out the diagnosis both of dementia precox and of paraphrenia, even if a defective condition of this sort is admitted to exist in Dr. N., is the complete rectification of the delusions, the self-criticism and the insight into his disease, the undoubted recovery from the `madness' notwithstanding the sensory illusions remained. This ending certainly suggests rather an intoxication psychosis, although his remaining well in spite of renewed intoxication is out of accord with the supposition.
"Thus we are in no position to make a positive diagnosis. Perhaps the most probable solution, if the vague pseudo-diagnosis of `degenerative insanity' is held unsatisfactory, is the view that the use of morphin (combined, it may be, with alcohol and cocain) is the foundation of the superstructure of pronounced degeneration as the cause of this singular psychosis. In medical diagnosis throughout a determined effort is made in every instance to correlate all the symptoms. Are we not too radical in our dealing with chronic morphin psychosis? May not some cases possibly have been overlooked because of the preconceived, belief in their impossibility? Assuredly care is needed in admitting of `combined psychoses,' for this will lead in the end to absolute nihilism, to irretrievable disintegration, to abandonment of all system."
G. E. Pettey-1913.33
Pettey attributes the psychic changes in cases of chronic opium intoxication to causes other than the drug, as will be seen from the following extracts:
"There are very few drug users who have not made many and often very desperate efforts to extricate themselves from the thraldom of the drug, or who have not., by some circumstances or other, been deprived of their drug supply. These efforts at abandonment or periods of deprivation have brought upon them the sufferings incident to the disuse of the drug, and these have proved to he so excruciating and intolerable as thoroughly to convince them that the voluntary abandonment of the drug is entirely out of their power; that what they once blamed others for not doing, they are themselves unable to do.
"While such experience may have worked a radical change in their own opinions, they are well aware that public opinion--the irresistible moral force—has not undergone any such change. They are acutely, or possibly morbidly, sensitive to that fact, but they are not changed in their purposes in life, in their desire to have and retain the respect and confidence of their friends and the public in general.
"They still love life, and their good name is as dear to them as ever They feel confident of their own integrity and good purposes, but they know that the drug has become a necessity to them. They also know that if their use of the drug should become known the blighting sting of public opinion would lacerate their very souls; therefore, in order to shield themselves from criticism and censure, springing from what they now know to be misguided public opinion, they procure their drug and use it in secret.
"Thus they start out leading a double life, a life of deception, with a skeleton in the closet that must be kept constantly concealed from public gaze, but the motives which prompt them to that course are not dishonorable.
"Self-preservation is said to be the first law of nature. A man is justified under the law in taking the life of his fellow-man when necessary to preserve his own, and in the protection of his good name, which to a right-thinking man is as dear as his life, very great liberty of action is allowed.
"The acts that are held to be a perversion of character, manifested by many of these persons, are not due to the physiological effects of opium, or to any pathological condition induced by it. The use of this drug does not, of itself, beget degeneracy. This springs largely, if not altogether, from another source. This is clearly shown from the fact that drug users who are independent of such influences maintain their integrity, sustain their good name, and retain the respect and confidence of their associates."
"In studying the history of a large number of patients who were unquestionably of good character prior to the formation of the addiction, the author has found that the perverse traits of character were prominent or not just in proportion as the other influences herein mentioned were prominent or not.
"If the addiction was formed by one who was entirely independent and could secure and use the drug without being interfered with by anyone, he retained his integrity, his business and social standing, etc., to a fair degree, but when the habitue was dependent on some one else for his drug supply, and this one a person who did not understand the necessities of his condition, or when his family or friends, or those to whom he was subject, undertook to break the "habit" by withholding the drug supply or the means of obtaining it, or when adverse fortune made it necessary for the drug user to resort to deception and other such means to procure the drug, the perverse traits of character were very prominent.
"These perverse traits were present in proportion to the length of time and the degree of intrigue and deception the drug user had been forced to use."
"No greater mistake was ever made by well-meaning persons than to attempt to deprive of his drug supply one who is addicted to the use of morphine. Such efforts only serve to drive the drug user to secret and often immoral acts to procure his supply.
"The only proper and reasonable course is to recognize the condition as a misfortune—a disease, as it really is, and one which cannot be overcome by merely depriving the patient of the drug. It should also be borne in mind that it is a really hazardous proceeding to deprive a drug user of his drug supply, since dementia or death may be the result."
"As a result of attributing the perverse traits of character manifested by some morphine users to the effects of the drug, both the profession and the public have fallen into the error of looking upon all opium users as of the same class, and since the comparatively small number of perverts among them are the ones who have become most commonly known, they have made the reputation by which all are judged.
"Such a conclusion is erroneous, and the opinion based upon it is manifestly unjust. Drug users differ from each other as greatly as do other people.
"Some of them retain their moral character, their veracity, and even their reputation without blemish, while others become moral wrecks; but it is evident that other influences besides the effects of the drug are potent factors in bringing about that wreckage."
F. Reach-1914.84
Reach studied the effect of the chronic administration of morphin on the intestine of a dog by means of the Roentgen ray. He found that
... on continued administration of ... morphin ... there occurred a lessening of the inhibition of gastro-intestinal peristalsis without, however, reaching normal. On an increase in the dose the whole cycle was repeated. Withdrawal symptoms were not observed in relation to the gastro-intestinal tract, but were marked in connection with salivation. Finally it should be noted that without tation without blemish, while others become moral wrecks; but it is evident that the chronic effect of morphin are given with the reservation that there were involved only one animal and covered a period of injections of only ten weeks."
H. Dominick-191433
"The author reports on two morphinists in whom psychical phenomena were observed during withdrawal.
"In the first case the clinical, picture of hysteria could be traced to a psychopathological constitution.
"In the second case a true psychosis was observed. After the patient in the beginning had withstood the withdrawal well enough, there appeared in the eighth to ninth week a state of increased depression and restlessness. The patient became unreasonable, noticeably disoriented and ended in a state of delirium. After about a week the mental condition returned to normal, the whole condition of the patient improved, while the spirits remained labile for a long period. Seven or eight weeks later a considerable improvement was observed."
K. Van Dongen-1915.3°
This author reviews the work of van Egmond on the ability of the various nervous centres to become tolerant to morphin and undertakes to continue the investigation in relation to the respiratory centre and the pupil in dogs and rabbits.
Van Dongen used two dogs, weighing 9 kg. and 8.5 kg. respectively. First he studied the behavior of the respiratory centre and found the greatest inactive dose for the normal dog to be 1/20 mg. per kilo; the smallest active dose to be 1/10 mg. per kilo. Starting with a dose of 10 mg. per kilo, the dogs were rendered tolerant within a period of about 21/2 months at the end of which time they were receiving 200 mg. per kilo.
During the gradual development of tolerance the respiratory reaction varied; just as the narcotic effect gradually became less and of shorter duration, the slowing of the respiration and the subsequent acceleration subsided and both ran a shorter course.
Van Dongen describes the behavior of the pupil as follows:
"The minimal active dose in intolerant dogs is 1 mg. per kilo; there is no noticeable effect on the pupil at % mg. per kilo. In both dogs the pupil was dilated and did not react to light. ... As soon as tolerance to a given dose appeared, the degree of the mydriasis decreased and gradually the reaction to light followed. This (central) tolerance of the pupil appeared quite rapidly, more rapidly than the tolerance of the brain cortex (narcosis) and of the respiratory center. If the dose was increased there appeared again a mydriasis and a lessened reaction to light, which soon again decreased, etc."
From his experiments on the rabbits, Van Dongen concluded that the continued reaction of the respiratory centre to the morphin demonstrated the inability of the rabbit to become tolerant.
J. Biberfeld-1915.37
This author reports in a series of articles studies made from 19151921 on the variations in the amount of lipoid in morphin-tolerant
dogs, the specificity of morphinism, tolerance to codein derivatives and experimental detoxication.
In the first study, the author investigated the effect of morphin on the brain lipoids, in an attempt to determine quantitatively the variations in the amount of lipoid in morphin tolerance. For this purpose
lie employed four dogs which he had rendered tolerant to morphin, using normal brains for controls.
He concludes—
"that the brain of a dog which tolerates, let us say 2.5 g. morphin—about ten times the fatal dose shows no quantitative variation in its lipoid content. This may demonstrate, on the one hand, that these chemical components play no important role in the action of the alkaloid, and on the other hand, again, it shows how obstinately the brain protects its chemical constituents while under pathologic influences."
Henry Beates, Jr.-1916.38
Beates explains the psychical alterations as follows:
"Tissues endowed with the higher functions of man, such as the brain, heart, etc., respond to most trivial exciting influences. ... Conduct, therefore, is largely determined by the inherent sensitiveness of individuals.... It is because of this susceptibility that the highly organized and sensitive intellectual characters are prone to the narcotic habit. Men of action, achievement and progress feel the wear and tear of responsibility. They experience mental pain, an actual agony, and because narcotics blunt the sensorium we find them used for evident reasons.... By such types of brains too frequently is the law of habit regarded as escapable.... Habit is the unescapable consequence of repetition. ... Everybody should be taught that no narcotic can be used even once, and the equilibrium existing between the emotional, intellectual and volitional not be, at first, seriously disturbed.... Thus step by step the deluded and ambitious leader grapples with responsibilities and ... by this time the poisonous properties of the drug have blunted, the intellectual. The moral is now included and a character noted for integrity and reliability becomes weak and indifferent."
C. L. Dana-1918.3°
"Most addicts are constitutionally unstable persons, likely to be a burden or a menace to society anyway.
"Drug addiction does not lead to insanity or the serious psychoses needing custodial care. The percentage of such cases in State hospitals is very small. It is very large, however, in prisons and reformatories and it would seem as if drug addiction had more relations to crime and social waste than to psychiatry.
"The drug addict is not usually a mental defective, and a series of intelligence tests would not disclose large percentages of morons and imbeciles, as happens in certain other anti-social groups."
W. Hale White-1918.4°
"Morphine for the most part circulates in the blood as such, and is excreted almost entirely by the intestinal mucous membrane, and very slightly by the kidneys, but a small part of it is destroyed in the body, probably in the liver; if morphine is taken habitually, the amount so destroyed gradually increases, and this explains why some persons can take such large quantities. The fate of the other alkaloids is not known, nor are we aware of any direct action of any of the constituents of opium on the blood itself.
"The higher faculties are at first excited by small doses. In a few persons there is no incoordination in this excitement. The intellectual power and mental vigour are increased, and therefore the drug is taken by some people to enable them to do their mental work. Usually, however, the excitation does not affect the mind evenly; generally the imagination is powerfully and pleasantly excited, much more so than the faculties of reason and judgment, which are a little dulled. The expression on the face is one of happiness and comfort, and this corresponds with the condition of mind, which is in a state of peace, calm, and happiness. This is soon succeeded by sleep, which is accompanied by pleasant dreams, generally of an impossible nature. With some persons, however, the sleep is quite dreamless. This, which is the beginning of the depression of the highest centres, is soon followed by depression of the others, the higher being influenced before the lower, so that soon the sleeper does not respond to any sound, light, or cutaneous stimulation, nor does he feel pain."
M. C. Mackin-1919.41
"The mental symptoms of morphinism, as defined by Dr. Lents, who tabulated what he considers the most prominent changes in morphinism, are:
"First, diminished power of recollection, increasing amnesia or disability to recall past mental images and ideas.
"Second, diminished power of attention and volition.
"Third, diminished power of initiativeness and energy of conduct. "Fourth, diminished muscular power, frequently marked by trembling. "Fifth, blunting of the higher moral and ethical senses.
"Sixth, insomnia, loss of desire for sleep, and nutritive disturbances of the whole cortical sphere.
"These divisions undoubtedly describe the conditions which occur more or less prominently in every case and there are very few cases that escape special sense involvement. One cannot use morphin long without suffering from weakened, obscured ideas of duty and right relations to others; conceptions of truth and discriminations between truth and falsehood become more and more cloudy; egotism, selfishness, childish prevarication, are quite marked in the ma- jority of cases; a decreasing sense of honor, less pride in character and appearance follow; forgetfulness to carry out promises, suspicion of wrong from others, with delusions that they can conceal their condition and deceive friends and associates is an ordinary accompaniment of morphinism. A man previously truthful and honest who suddenly falsifies and does disreputable things without apparent motive may he expected to be under the influence of some powerful drug."
A. C. Buckley-1920.42
"Mentally there is a characteristic sluggishness, which disappears transitorily following each dose of morphine. As a rule, the patient loses interest in his accustomed pursuits, family and friends and seems generally indifferent towards everything but himself. Emotionally he is irritable when not indifferent. His judgment and consequently his idea of proportion are notably lacking. All sense of responsibility and regard for truth disappear; he will resort to all sorts of devices and sacrifice self-respect in order to obtain his desired drug. Insomnia and restlessness are persistent except while the patient is under the influence of morphine."
James M. Anders and John H. Musser-1920.43
"In cases of death from acute or chronic opium or morphine poisoning there is nothing distinctive in the pathologic appearances. In acute cases vascular congestion of the brain and membranes has been noted; but even in chronic cases the tissue degeneration and fatty and connective-tissue proliferations that are characteristic of alcoholism, are practically absent. Decided lesions are usually traceable to associated affections. The principal anatomic changes are those due simply to malnutrition. Thus, we have the emaciation and the shrunken appearance of cerebral anemia, the pallor and atrophy of the cardiac muscle and of the vascular walls. The dried and wasted structures, due to tissue starvation, are quite a contrast to the fat-infiltrated or degenerated, cirrhotic, and inflamed tissue of alcoholic inebriety. Direct destruction of parenchymatous cells is more evident in the latter.
"These may be in abeyance for some time, while the habit is forming and the doses are still slight. As the craving increases, the dose and its frequency increase to keep pace with the desire. Anemia gradually develops, with sallowness of the skin, wasting of the features and body, languor, weakness, functional deterioration, mental depression, anorexia, restlessness, insomnia, tremors, irritability, shyness, dilatation of the pupils (except when under the influence of the drug), and a characteristic propensity to lying. Cardialgia is often complained of by those who use opium pretty constantly. The associated vices of opittmism are less violent and inflammatory than those of alcoholism, and more secretive and speculative, such as gambling and sexual perversions. Itching is frequent, and especially after taking the opium or morphine. Attacks of chills, followed by pyrexia, with delirium and transient albuminuria (renal congestion) occur in some cases. Diarrhoea and dysentery have been observed in some instances. There may be also disturbances of the visual muscular apparatus. Sufferers from painful carcinoma in whom opium or morphine is required for steady use do not become, except in rare cases, true morphinomaniacs."
E. S. Bishop-1920.44
"It is my opinion that, however much increased oxidation aids in the handling of morphine, it is to the formation of an antitoxic substance that we look for the explanation of our clinical manifestations and for the classification of morphine-addiction, as a definite medical entity. This opinion is based on certain clinical manifestations of morphine effect and the symptomatology attending insufficient supply of morphine to those addicted, on certain phenomena observed during and following treatment, on the persistence of tolerance and on the susceptibility of the cured patient to the re-formation of addiction."
"What characteristic action exists in opiate or narcotic drugs which gives them this power to establish the above described mechanism? It seems to me, that it is, above all, their power to inhibit body function. They tend markedly to arrest metabolic processes. They inhibit glandular activity. They inhibit unstriped muscle activity and hence peristalsis. They, therefore, cause a slowing up of the glandular function and intestinal activity, and of elimination. This results in an accumulation of opiate in the body. It is this constant accumulation to which the body must become tolerant by the development of some mechanism for its protection.
"Autointoxication and Autotoxicosis —It is to the element of inhibition of function also that we must look for explanation of what is by far the most important element in the immediate picture presented by most individual cases. I refer to autotoxicosis and to auto and intestinal toxemia. The same power that locks up within the body the opiate drug, locks up the toxic products of tissue activity and tissue waste, of intestinal poisons and of insufficient metabolism. Autotoxemia itself is markedly inhibitory in its action, and contributes no little to its own increase and to the further development of narcotic disease.
"It is not. at. all impossible that any inhibiting poison, constantly present in the body, will sonic day be found to establish a mechanism of protection, similar to that of opiate addiction, and that some of the states now popularly and loosely classified under the general head of `autointoxication' will be recognized as really addiction-states, in which the body has become progressively tolerant of its own poisons. I believe that it can be demonstrated that some of the phenomena and manifestations at times observed in chronically inhibited and autotoxic individuals in whom there can be no suspicion of any opiate or narcotic element, are analogous to the phenomena of narcotic addiction-mechanism. It is not inconceivable that any inhibiting poison or toxin is capable of producing its own addiction-mechanism, and it has seemed to me that my own clinical familiarity with the action and reaction of narcotic, inhibiting, or addiction-forming drugs and of addiction-mechanism upon circulation, glandular and intestinal and other function has been of no little assistance in the interpretation, control and remedy of other chronic intoxications.
Upon the extent of inhibition of function and autointoxication, therefore, depend some of the immediately predominating manifestations in individual cases. They must be reckoned with and eliminated in the measure of addiction-disease in the individual sufferer. In many cases they contribute the immediate and compelling indications for rational therapeutic endeavor. To a considerable extent they determine circulatory efficiency and metabolic and glandular activity and balance. They largely control physical tone and physical reaction. Inhibition and intestinal and autotoxemia cause most of the physical and mental deterioration, and much of the incidental symptomatology so widely ascribed directly to narcotic drug effect. Upon the extent of their presence, therefore, depends greatly the clinical picture in the individual case. This doubtless accounts for the acidosis, noted by Jennings and others, inasmuch as it has been definitely proved that acidosis is commonly present in all conditions of functional depression and exhaustion.
"With inhibition and auto and other toxemia eliminated or reduced to a minimum, the patient can go through many years, an apparently normal man, well-nourished reactive in good physical tone, mentally sane and physically competent. Under these conditions he shows practically nothing abnormal as long as he gets properly administered, his accustomed narcotic drug, in the amount of its minimum physical requirement or body-need. His condition is often unsuspected by those nearest and dearest to him, and the popularly held opinion that narcotic addiction shortens life does not seem to be upheld by the facts in his case. Such cases as his are far more numerous than has as yet been realized.
"In the types of narcotic addicts most widely recognized, inhibition of function and autointoxication is marked, and the opiate drug is used in excess of body-need. The addict of his description becomes a deteriorated wreck, requiring high doses of opiate for the satisfaction of abnormal body-need, mentally and physically incompetent—the generally accepted picture of the so-called `dope-fiend' a deteriorated, degenerated, malnourished wretch, degraded, avoided and condemned.
"Inhibition of function and autointoxication should not be vague terms. They cause and are measurable by definite clinical evidence. They display manifest phenomena and symptoms, and become increasingly defined material entities, as the clinician looks for them as such. Much of inhibition of function and autointoxication and of their manifestations, has been recognized and taught under their own heading and in connection with conditions other than narcotic drug addiction-disease. That the influence and importance of inhibition of function and autointoxication in the development, and manifestations of the narcotic drug addict has escaped general and widespread recognition, is evidence of the small amount of unbiased clinical study, and of analytical clinical interpretation , of material physical phenomena, hitherto accorded to narcotic drug cases.
"I would not have it concluded that all symptoms and manifestations ar.sing .,. in the handling of a drug addict are due to the factors and elements I have discussed in this chapter. It must be always in the mind of the intelligent and conscientious physician, that he has in his care a human being with the same medical and psychical possibilities that must be taken into careful and complete account, as in the handling of any other sick person. There is an unfortunate tendency to overlook concurrent, or complicating or pre-existing conditions ' in the handling of the narcotic drug addict. These cases are often extremely complex and difficult to analyze, and for adequate comprehension and handling of them, the symptoms and manifestations they show should be appreciated in their true origin and character as they occur in each individual case."
H. Kogerer-1920.45
Kogerer made some studies of allergic reactions in morphinists. He used Hecht's method of testing on 15 cases and came to the following conclusions:
"1. The majority of the chronic morphinists show a perceptible hyposensitiveness to intracutaneous injections of morphine solutions.
"2. Some of these patients show an increase in sensitiveness during abstinence..
"It may be possible to determine objectively in a stubborn patient the diagnosis, which once happened in one patient. But in the great majority of cases the diagnosis is possible without this means. Much more important is the question whether we can draw prognostic conclusions at the end of withdrawal••; on the return of a normal skin reaction, somewhat with the idea as to whether we might expect a relapse of the permanent hyposensitiveness, with greater,' probability than in the case of patients who are left with a normal reaction. This is not to be determined, however, within the short period of observation.
"3. It is possible to determine a probable relapse by a comparison of the state of the skin after withdrawal and later."
C. E. Sandoz-1922.4°
"Although, through prolonged use, morphine becomes absolutely necessary for the comfort of the individual, this does not mean that it does him no harm. On the contrary, it is a poison which, if taken over a long period in large doses which, severally, do not produce striking symptoms, brings about a condition of chronic intoxication. This manifests itself in changes both mental and physical. The mental changes affect all three aspects of the mind: intellect, emotions, and will, especially the two latter. The memory becomes unreliable, particularly in regard to the sequence of events. Intellectual efficiency, above all that requiring initiative, decreases, but can be spurred on by morphine. The emotional tone shows marked ups and downs. Morphinists are now cheerful, hopeful, good-natured, now without ambition, irritable, arrogant, despondent. Despondency may be so marked that it leads to suicide. They become easily tired and will sometimes be overwhelmed by sudden drowsiness which makes them fall asleep in the middle of an occupation or conversation. They experience constant changes between times of relative well-being with relaxation and times of nervousness and restlessness. These changes are partly dependent upon whether the last dose of morphine is still acting sufficiently or not. This makes a regular and purposeful activity impossible and is one of the reasons why morphinists go down hill economically. But the main cause of this is perhaps the modification of their character. They become weak-willed, mentally `flabby,' shirk any effort, exhibit oversensitiveness to pains and annoyances. They lose all sense of responsibility, neglect their duties and live from hand to mouth. The circle of their interest narrows until it is finally reduced to morphine and the means of obtaining it. In order to secure the drug they will, if necessary, lie, cheat, steal, or do anything. Even if a morphinist is otherwise trustworthy, to rely on his word or his actions in regard to morphine would be, and too often is, a fatal mistake. But lying, cheating and the like are often tendencies of morphinists in matters which have no connection with their habit and seem to be due to a loss or deterioration of moral feelings. However, concerning this latter point, there are divergencies of opinion among those who have had wide experience with morphinists. It is very possible that absence of ethical feelings in many cases is not a 'loss' due to morphine but a primary `lack' which, in a large category of cases, is directly or indirectly at the root of morphinism.
"The most striking bodily changes in morphinism concern nutrition. The patients lose weight, often becoming emaciated, the tissues are flabby, the skin is pale and sallow, the hair is dry and falls out, the nails are brittle and the teeth have a tendency to decay. These disturbances of nutrition are probably partly caused by a deficient function of the stomach and intestines, due to the checking influence of morphine on the digestive processes. A stubborn constipation is generally present. The appetite is usually bad, especially for meat, their favorite diet being sweets and fruit. Among the other symptoms of morphinism we can mention the following: sleeplessness, palpitations of the heart, accompanied by a rapid and irregular pulse, fainting spells, disturbances of respiration, especially asthma. Profuse perspiration or the opposite, an extreme dryness of the skin, chilliness, all sorts of disagreeable sensations in the region of the heart, stomach, bladder and in the limbs. A symptom which is very frequent in inveterate cases is a decrease or loss of sexual desires, accompanied by impotence in men and loss of menstruation in women.
"However, the symptoms of chronic intoxication are more or less marked according to the cases, the amount of morphine taken and the duration of the habit being the main factors in its severity. Individual disposition and other factors, such as the mode of life, also seem to play a great role. Certain morphinists apparently withstand remarkably well the effects of prolonged and intense use of morphine, while others are very sensitive to it. All degrees are found between those who are wrecks after a few months and those who, in spite of large doses, do not show striking changes after several years or even decades. So that, contrary to the current belief, the appearance of a morphinist does not always betray his condition. There are cases, even of long standing, in which a morphine addict looks well and does not, when satisfied with morphine, suggest drug addiction. It is true that, in most inveterate cases, morphinism is suggested by the looks, but, even then, these have nothing so characteristic about them that they can be differentiated at first sight from the appearance of numerous other people who look sickly for a different reason. That which is characteristic of the morphine habitué are the changes which his condition and attitude undergo during the course of a day, according to whether he is in need of the drug
or not. After a `shot' he will look and act at his best, but when the effect of the morphine wears off he begins to break down. If a new dose is then taken the crestfallen individual undergoes a sudden revival and feels and looks a different being. If not, clear-cut and distressing withdrawal symptoms gradually develop. In contradistinction with other poison, then, cocain and alcohol in particular, it is
not when under the influence of the drug that the morphinist looks very abnor-
mal and is easily recognized; it is, on the contrary when he must go without it."
Paul Sollier-1923.47 48
Sollier, 1894-1923, in a number of different articles has described certain pathologic findings and speculated concerning others whose existence he has had no opportunity to establish.
For the most part, however, he limits himself to a consideration of changes which occur during withdrawal and, therefore, we are presenting this material in the next chapter. However, the following abstracts of articles by Sollier dealing with certain pathologic changes are included at this point inasmuch as they refer to the condition during intoxication as well as detoxication:
In the first article }' Sollier reviews the hematologic changes reported by Morat and describes further studies on the viscosity of the blood at different stages of intoxication and detoxication, making the following observations:
During intoxication when generally a red cell increase exists, the viscosity of the total blood is increased.
This increase is due particularly to the red cell viscosity, the plasma viscosity remaining normal.
During withdrawal the total viscosity increases still more, still due to the effect of the red cell viscosity much more than to that of the plasma.
Fifteen or twenty days after the withdrawal, the viscosity approaches normal which it reaches in from the thirtieth to the fortieth day when it goes below that of the period of intoxication.
He reviews the findings in a case of heroin intoxication and explains the phenomenon as follows:
Realizing that during the periods of reduction and of withdrawal patients are subjected to repeated purgation and have very abundant urinary and other discharges through glandular hypersecretion, it was thought that this hyperviscosity was due to a dehydration of the organism. However, the figures show that the plasma viscosity varies only very little proportionately while the red cell viscosity increases considerably.
The variations in the increased red cell count do not seem, on the other hand, sufficient to explain the degree of increase in the total blood viscosity. Apparently an additional factor must be sought. This factor is no other, according to the opinion of the author, than the morphologic and structural changes which were noted at the time of withdrawal, the friction of the red cells being very much increased, because they are deformed and torn.
These facts, which accord in every way with earlier observations as to the red cell resistance and the changes in the blood picture during detoxication, he believes, show that the clinical phenomena of morphin withdrawal depend on organic causes, of an origin analogous to that of certain infectious maladies, and that the psychologic symptoms that are seen in abstinence are the result of real organic disturbances, and not, as some still claim, of a vicious mental habit.
We quote the following extract from correspondence with Dr. Sollier, in which he describes certain deviations from normal susceptibility to certain infections during chronic intoxication and after withdrawal:
"During the period of intoxication, morphinists appear to escape infectious and epidemic diseases, grippe, pneumonia, colds. Their abscesses, although often very large, only occasionally take on phlegmonous characteristics. They contain only cocci and very rarely the ordinary pyogenic species (staphylococci or streptococci) .
"On the contrary after demorphinisation, sensitiveness to these maladies reappears.
"A similar increase in sensitiveness is evidenced toward morphin after detoxi- cation. Also in the case of early relapse, they are not able to reach their former doses and their decline is very much more rapid and marked than during the first intoxication." `B
In his last article in collaboration with Morat,5° Sollier discusses the digestive hemoclastic reaction, following Widal's technique as it occurs in chronic morphin poisoning and during detoxication.
They first review the profound effect on the liver function exercised by opium in chronic intoxication and the violent reaction that takes place in withdrawal as evidenced by the abundant production of bile, the diarrhoea, vomiting, presence of biliary pigments in the urine, etc.
It was these marked functional disturbances of the liver that stimulated their studies of the hemoclastic crisis in these cases. While certain phenomena usually present in this reaction were not observed—alteration in arterial tension, in coagulability and the viscosity of the blood—they did find a marked leukopenia during intoxication and also during detoxication after the injection of 200 g. of milk, though it ceased to develop between the twentieth and thirtieth day after the withdrawal of the drug. They give the details of two typical cases, one using morphin and the other heroin.
They also found that the leukopenia occurred after injections of the customary drug in either the usual large doses or in minute doses and also upon the administration of drugs of the veronal series.
They come to the following tentative conclusions:
"I. Morphinists and cases of other chronic poisoning in whom the function of the liver is distinctly affected by the poisoning alone, present after taking 200 cc. of milk a hemoclastic crisis characterized by a marked leukopenia.
"2. This crisis persists for a certain length of time after the withdrawal and does not disappear until between the twentieth and thirtieth day after the suppression of the morphin. The disappearance of the hemoclastic crisis in detoxication is a very certain index of good progress in the convalescence of the patient. It agrees further with other manifestations which we have pointed out as indicating the return of the normal functioning of the organism, with which it occurs simultaneously.
"3. These cases also show a definite leukopenia at the time of the injection of the morphin but this leukopenia bears no relationship to the amount injected because an infinitesimal dose in a morphinist accustomed to large doses causes the same leukopenic reaction.
"This explains how during total abstinence an infinitesimal dose as compared with the usual dose is sufficient to allay and arrest violent and painful reactions. It also explains how, in a morphinist from whom the drug has recently been withdrawn, a small dose of morphin is sufficient to set up in his organism a state which reawakens at once his dependence and creates a need which leads him to relapse. Therefore, we advise expressly never to give, even a long time after withdrawal, for any reason whatsoever in any form or in any dose, opium or above all morphin to a former chronic user.
"4. Hypnotics, always very harmful when they are added to morphin intoxication, cause when taken by a morphinist or even by a morphinist after detoxication the same hemoclastic phenomena which milk and morphin.cause. Hence it should be the rule never to combine during the course of morphin intoxication or to give as a substitute during detoxication narcotic or stupefying drugs of any kind."
M. Horiuchi-1923.51
The following brief abstract gives the author's findings on the effects of experimental chronic morphin poisoning on the suprarenals of tolerant rabbits:
"The pathological anatomy of chronic morphin poisoning, which is so widespread in China, has not yet been completely explained. The author gave rabbits daily a certain quantity of morphium hydrochloricum solution through subcutaneous injection. The animals showed distinct hyperglycemia and glycosuria and fell into a deep sleep for several hours. But gradually they became addicted to the initial dose of morphin, so that the dose was continually increased until the animals finally died of cachexia. Dissection revealed hypertrophy of the adrenals. The cortical layer was histologically expanded and the medullary cells were augmented in size and number. The chromium reaction of the medullary cells was not especially pronounced in comparison with control animals. It was, however, highly pronounced in animals in which several days had intervened between the dissection and the last morphin injection. In the author's opinion the hyperplasia of the cortex is to be understood as an active, appropriate adaptation of the organism against the hyperglycemia, because the adrenal cortex as well as the Langerhans islands of the pancreas act as a check against sugar metabolism. With regard to the hyperplasia of the medulla the author conjectures that morphin stimulates the sympathetic nerves, which would lead to the hypersecretion of adrenalin and, consequently, to the hyperactivity of the medullary cells."
Adolf F. Hecht-1923.52
The author states that Philippson was the first to produce urticaria in dogs by injecting morphin beneath the skin. He also reviews briefly the work of TürSk and Vari, Jadassohn and L. Rothe and that of Alice Stauber-Lehndorff, all of whom produced allergic reactions in the skin with morphin injections.
In his own experiments Hecht undertook first to study the disappearance of the reaction change after a single injection, and made observations on the reaction occurring on the intradermic injection of atropin and the possible relationship between sensitiveness to morphin and that to atropin. He then studied these reactions in addicted individuals before, during and after the withdrawal of the drug. After reporting his findings in detail he continues as follows:
"The results in studying morphin habitués are not reliable because, in the first place, the degree of sensitiveness before using morphin is unknown; further, the very cachexia attending severe morphinism may produce anergy; and finally the statements of patients respecting their behavior outside the institution are to be regarded with skepticism.
"But prolonged abuse of morphin considerably diminishes sensitiveness to morphin (cases 1, 5, 8), often in part, only the exudation (case 6) or only the erythema (case 9) being encountered. Cachexia alone was not sufficient evidence in case 4 of hyposensitiveness to morphin, for the equally cachectic case 2 had normal sensitiveness to morphin. The phenomena during withdrawal and after it are not reliable.
"Sensitiveness to atropin, evidenced nine times in 'sixteen cases, seems generally to be diminished, even when sensitiveness to morphin is normal, as in cases 2, 3, and 7. In case 10 the impression is received of a relatively higher sensitiveness to atropin and lower to morphin, and in case 2 the atropin reaction is constantly much more pronounced than in case 3, although both alike react forcibly and normally to morphin.
"No similarity exists between atropin and morphin in this respect, as might be expected from the contrasting behavior of the two substances after a single injection of morphin.
"The commonly observed allergy of the skin on the part of morphin habitués may, therefore, be due to a specific alteration of the skin, at least in the main, and this seems to me important in explaining morphin addiction.
Summary.
"1. A single injection of two centigrams of morphin altered the sensitiveness of the skin to morphin by causing it to diminish and later to increase. Its sensitiveness to atropin withstood alteration.
"2. A single injection of one milligram of atropin increased the sensitiveness to atropin, to be sure, but left morphin sensitiveness unchanged at the height of, its effect.
"3. Abuse of morphin diminishes the sensitiveness of the skin to morphin. Conclusions are not reliable in the period of withdrawal.
"4. Allergy of the skin to morphin throws light on the cause of morphin addiction (cell changes in part at least on a specific foundation)."
Erich David-1924.53
"The most prominent characteristic we find in the somatic disturbances of the first stage, the period of addiction, is depression of the whole biotonus. Very striking are the inhibition throughout the gastrointestinal canal and the complete inhibition of glandular secretion. Hence occur loss of appetite, constipation, diminution of urine, and impotence. These are all manifestations of increased sympathicotonus and of diminished parasympathicotonus. Increased sympathetic activity is evident also in distension of the bronchioles, in vasoconstriction, in raised body temperature, and in trophic changes in the skin, teeth, and nails. Still further noticeable is the augmented thirst which is a result of retention in the blood of crystalloid bodies and may likewise be traced to increased sympathetic action. On the other hand, it cannot be denied that the pupillary contraction and slowing of cardiac action are consequences of increased parasympathicotonus. All in all we have a depression of the entire biotonus and consequently as a rule enormous loss of weight. Thus the first stage is chiefly noticeable for increased sympathicotonus and decreased parasympathicotonus, but, as already shown, there are exceptions. It cannot be said positively that morphin acts selectively on either of the two systems. Furthermore, in case of some symptoms it is very difficult to tell whether sympathetic or parasympathetic excitation exists. The construction of the human organism is much too complicated for that. In the midbrain, besides the principal centres, we find certain other subordinate centres, and we recognize in addition numberless reflex arcs, partly in the brain, partly in the spinal cord, it may be traversing the whole periphery (the intramural system). We know well also how all the organs have a mutual influence on one another. I shall cite only one example. Wuth instances vesical spasm as a result of increased vagotonus. But this is not correct. For experimental excitation of the hypogastric plexus causes increase of sphincter tonus and diminution of detrusor tonus with retention of urine, while excitation of the pelvic nerve occasions relaxation of the sphincter vesicae and contraction of the detrusor with consequent expulsion of urine. Therefore in vesical spasm we are dealing with a purely sympathetic excitation. Corresponding with this, increased sympathetic activity also produces contraction of the pyloric sphincter, of the ileocolic sphincter, and of the internal anal sphincter, phenomena also observed in fact in morphin addiction. In all probability the condition in these last named instances is that of an intramural reflex.
"From all this it may be confidently asserted that, during the period of addiction, morphin acts chiefly as a stimulant to the sympathetic and an inhibitant to the parasympathetic. When Wuth reaches the opposite result the interpretation of his results is a matter, as he himself says, only of pharmacological analysis, not of studying addiction.
"The second stage, that of the acute symptoms of withdrawal, is marked by a complete revolution in the nervous system. It is very difficult to steer a course through the mass of phenomena. Increased parasympathetic effects alternate with increased sympathicotonus. While, in the first stage, parasympathetic diminution endeavors to counterbalance increased sympathetic action, now the impression is given that the parasympathetic preponderates greatly, while the sympathetic is unable with its diminished tonus to restore the lost balance. Sensations of heat and cold alternate, uncontrollable vomiting takes place, profuse diarrhoea, unprovoked perspiration, attacks of yawning and sneezing, unmanageable cardiac palpitation, polyuria, salivation dominate the picture.
"This stage passes gradually into the third, where we can trace indubitably the influence of a quickened parasympathetic and a depressed sympathetic. Polyphagia, priapism, sweating, diarrhoea, polyuria, reddened skin may be observed, also rapid heart action and enlarged pupils, both phenomena which, as in the first stage, indicate an excited sympathetic. On the whole, however, a decided preponderance of the parasympathetic. The whole organism seems exalted, hence a prodigious increase in weight.
"So we summarize:
"In stage 1 increased sympathetic and diminished parasympathetic. "In stage 2 sympathetic and parasympathetic indifferently.
"In stage 3 increased parasympathetic and diminished sympathetic.
"Let us pass now to manifestations in the psychic field.
"We endeavor in these days with Kretschner to take constantly into account the numerous factors which may enable us to explain the complete picture of a psychic disorder; in addition, for instance, to the constitutional cause, we should inquire into the character make-up, a possibly influencing event, the environment as respects internal secretions and infection, as well as any exhausting influences. Thus the psychic picture connected with morphinism also differs widely in different individuals. Invariably the kernel can be extracted from the complex of manifestations which bears a relationship to the changes of the general organism in the three different stages.
"Thus the diminution of organic tone in the first stage is accompanied by a depression of vital sensibility. The frame of mind is usually melancholic. The world seems colorless, hostile, every interest palls, no pleasure is taken in anything and the victim avoids human society altogether. Every event is taken more tragically than under normal conditions, the future appears black, all pleasure is gone from the present and finally come indifference to life, suicidal thoughts. Association of ideas is limited, there are long lapses in thought, thinking is onerous. The attention remains concentrated on one idea without being diverted. Within this idea too the attention is very vascillating. Thus a diminution occurs pf keenness of attention. Working capacity rapidly diminishes and the will becomes very weak. Initiative is lost, effort becomes difficult and slow, the bearing slouchy, and the patient lies around for hours without occupation. As regards plasticity of the dream fancies and the supposed euphoria so obtained, this is always manifested with special certainty after fresh administration of morphin and is probably the result of stimulating the nerve cells. Furthermore, this phenomenon becomes less prominent as addiction advances.
"After all, there is in this stage a close similarity to the melancholic phase of manic depressive insanity, as would be expected from the sluggishness of the whole organism.
"In the second stage the mental picture remains melancholic. On the other hand, the sluggish thinking of the first stage is replaced by a normal flow of ideas. Ideas flow incessantly through the head; the consciousness of not being able to control them and think them out is very annoying. Ability to concentrate is greatly reduced; the simplest reading or conversation fails to hold the attention. A vast unrest seems to be a most painful experience, and patients move about without finding rest day or night.
"I need only call attention to the great similarity of this condition to manic depressive mixed states.
"The third stage sometimes begins with increase of body weight. The world appears all at once in a wholly different light, joy is renewed in life, in nature,—in fact in all in which before no interest was felt. The frame of mind is prevailingly euphoric, but vacillating. Self-consciousness is exalted, the mental instability continues for a long time, weeks after even the patient is still incapable of work, uncontrolled and without power of concentration. Here there is a striking resemblance to the manic phase of manic depressive insanity.
"Wuth has called attention to the great similarity existing between our second stage and Basedow's disease.
"The vegetative midbrain centre naturally affects the entire endocrine system, and it is to be expected that disturbances in the latter will also cause disturbances in the ganglia at the base of the midbrain. The question whether morphin primarily affects the vegetative centres or the endocrine system in my view does not admit of a positive decision at present.
"I only will say in addition that, just as in Basedow's disease, a striking resemblance exists also between our second stage and Freud's anxiety neurosis, where in all probability a disturbance in the activities of the internal secretion of the sex glands must be assumed.
"So we may infer that in morphinism we have to do with an impairment of exogenous origin of the vegetative centres in the ganglia at the base of the midbrain which regulate metabolism. This seems to be the case also in the manic depressive psychoses, while in Basedow's disease and in anxiety neuroses primary changes in the endocrine system destroy secondarily the balance of the regulative centres and so produce a picture such as we see in the stage of the acute symptoms of withdrawal and in manic depressive mixed conditions."
C. C. Wholey-1924.54
"The conclusions reached in this paper are based on drug cases appearing in the routine of a general psychiatric practice. In number, the series embraces probably about the average percentage of such cases coming year by year to a neuropsychiatrist in an industrial community such as this. These patients were handled for the most part in the St. Francis and Western Pennsylvania hospitals. They were studied as psychiatric material, the history, environment and constitutional makeup being considered, as in the case of any other neuropsychiatric affection.
"It is customary to discuss the results of morphin and other habit-forming drugs along with the results of metallic poisons such as lead, or of the endogenous toxins of uremia, diabetes, etc., under the general caption of the toxic psychoses. While it is true that the narcotic, or habit-forming drugs, and alcohol, do produce toxic psychoses, the effects brought about by them are essentially different from effects following on the metallic and endogenous poisons. Drug addiction can never be understood, or successfully handled, until this fundamental difference between the action of the habit-forming drugs and that of other poisons- and disease processes is appreciated: The metallic and endogenous poisons produce their destructive effects, in the main, more obviously on the physical organism; these effects are generally demonstrable, and understood. The mental effects are secondary. The narcotic, or habit-forming drugs, on the other hand, produce degenerative effects primarily on the mind and character; .these arise early, and are more or less permanent. The effects on the physical organism in the case of narcotic drugs are largely functional, and generally eradicable."
* * * * *
"In whatever type of toxicity, metallic, endogenous, narcotic, etc., the obvious and necessary step is to correct, so far as possible, the damage to the physical organism. This correction of the physical condition constitutes, as a rule, practical restoration, or cure, in the case of non-habit-forming toxic injury, reaching, as it does, the essential source of the trouble. But in the case of the habit-forming drug, physical restoration is but the first step toward rehabilitation, or so-called `cure'; there still remains the mental damage, which constitutes the true dominant therapeutic problem.
"Narcotic drugs are used, therapeutically, for the alleviation of conditions affecting the nervous system; the relief of pain or of mental or emotional distress. We naturally, therefore, find their effects, when reaching a pathologic degree, on the nerve organism. In explanation of this pathologic result, it is well, first, to remind ourselves of the elementary fact that we feel and act in accordance with the information that we receive through our sensory nervous system; our special senses of sight, hearing, body surface sensibilities, etc., with all their highly elaborated end-organs. These, through their sensory connection with the brain, keep us constantly informed as to our environment. Under a similar nerve mechanism, we are kept informed as to the status of our own bodies, and personal identity, through the sensory impressions received from nerve terminals, or receptors, distributed in muscles, joints and viscera. Nature has provided no other mechanism by which the organism can inform itself as to its environmental condition or bodily states. In short, the human organism has to depend for self-preservation on this intricate nerve mechanism."
* * *
"In a state of normal health, a general sense of well-being prevails. This sense of well-being is a result of the sum total of all sensory impressions reaching the brain; it is made up of the continuous flow of sensations from all the organs of the body to the mind. This flow of sensations we term the general bodily cenesthesia. Unless disease interferes, the person is not aware of or disturbed by this cenesthetic functioning."
"This cenesthesia constitutes the source from which arise the incentives of behavior. In other words, conduct is the end-result of this underlying bodily tone or state of feeling. Under the influence of a narcotic drug, there is an obtunding of the general cenesthetic sense, along with the dulling of any specific pain for which the drug may be used. If this obtunding is continued for some length of time, there is a lowering of tonicity of the general cenesthetic ma, chinery, so that even the customary functioning of bodily processes cannot eventually proceed without inducing a sense of discomfort when obtunding ceases. There is general lowering of the person's capacity for withstanding pain or distress; he must continue obtunding his general sensibility in his effort to maintain a tolerable sense of well-being. This necessity, and instinctive effort on the part of the human organism to maintain itself in a bearable state of being, lies at the basis of addiction; it determines the psychology and behavior of the drug victim.
"Sympathetic System.—Considering more specifically the effects of an opiate on the physical organism, with the accompanying mental and character changes, we find it acting conspicuously on the vegetative, or involuntary, nervous system, with its endocrine extensions, the whole loosely termed at times the sympathetic system. This system, as we know, controls involuntary, or automatic, processes: cardiovascular, respiratory, digestive, secretory, etc., as well as ductless gland functions with their important biochemical relations to the organism. The cardiovascular system in an hàbitué soon adjusts itself to the support of an opiate. Morphin is a powerful and enduring stimulant of this system. As to the effect of prolonged stimulation, if the organism is supplied needlessly with something that supplants its own effort in any particular direction, it ceases to function in proportion to the substitution; in the morphinist, the support that the drug has imposed becomes evident, on withdrawal, through the tachycardia, sweating, etc., intervening, all indicative of some degree of circulatory collapse, at times fatal. This collapse, or effort syndrome, explains the cardiac distress and pain of withdrawal, and also explains much of the anxiety and feeling of dissolution and panic arising during the withdrawal stage. For these psychic manifestations of anxiety, etc., are constant accompaniments of heart embarrassment whatever the etiologic background—angina pectoris, heart flutter or acute indigestion. These symptoms are a result essentially of dysfunction of the nerve supply to the heart from the vagus, the great upper autonomic representative of the vegetative nervous system.
"Gastro-Intestinal Changes.—The digestive apparatus also is controlled by the vegetative nervous system. Here, in the addict, the organism adjusts itself to the obtunding changes imposed on the secretory and smooth muscle fiber nerve mechanisms by the drug; when the drug is suddenly removed, this pathologic adjustment is reversed, and there is a violent disturbance of integration in secretory and muscle functioning, evidenced in cramps, diarrhea, vomiting and general abdominal distress. Under the drug, constipation is almost universal in the morphinist; on withdrawal, an irritation is produced by the sudden exposure of the drug-obtunded neurosecretory mechanism to the demands of former normal functioning. A temporary overactivity is brought about, resulting in diarrhea. While the drug was being used, a pathologic adjustment could go on without awareness of abnormal processes, because of the narcotizing of the sympathetic receptors in the digestive canal. Such symptoms referable to the digestive apparatus evidence further the apparently selective action of opiates on vegetative processes. In this case, `both splanchnic and vagal components are involved.
"Changes in Reproductive Organs.—The functions of the reproductive organs, innervated mainly by the autonomic division of the vegetative system, present well-defined disturbances as a result of opium and its derivatives. Striking changes in both the physiologic and the psychic functions of sex come about. Cessation of menstruation occurs in the female, with atrophy and cessation of function of the mammae. Psychically, this is accompanied by more or less complete loss of all sexual desire, and of the emotions associated with sex. In the male, in advanced cases of morphinism, complete sexual impotence is frequently seen. Both sexes, in extreme addiction, are practically rendered emotionally asexual. On withdrawal of the drug, the individual is often overwhelmed by tumultuous sex desire."
"Such additional involuntary phenomena as yawning and sneezing occurring in withdrawal indicate involvement of the intricate autonomic mechanism brought into overactivity by the release of afferent nerves and receptors from the obtunding effect of the drug. Insomnia is practically universal after withdrawal. The physiologic phenomenon of sleep is a vagontonie condition according to Bauer. The autonomic mechanism controlling this recurring physiologic condition has been disorganized under the influence of the drug. The insomnia is incident on the difficulty of the reestablishment of the normal cycle of wakefulness and sleep, according to Higier."
"When the physiologic functions of the sexual realm are so interfered with, it is not surprising that mental and emotional disturbances should occur. The instinct of sex probably constitutes the chief source of our emotional life and personal conduct. The morphinist becomes indifferent, varying, in accordance with his original character make-up, toward ordinary family ties and obligations. There is a disappearance of those incentives grouping themselves about the family unit—ambitions of acquisition, desire for security against poverty. He becomes improvident and heedless of social esteem. Such character alteration seems to be definitely correlatable with physiologic changes in the realm of sex.
"We may remind ourselves that malfunction in members of the endocrine system, other than those of sex, produces mental and emotional pathologic changes. We have all seen the personality alterations attendant on myxedema, in which the thyroid gland is involved—the emotional dulness and mental defect, and the opposite alterations in hyperthyroidism; the mental sluggishness of acromegaly with its disturbed pituitary gland; the depression of Addison's disease with its basis of dysadrenalism. Such phenomena indicate the close relationship that exists between normal development and maintenance of personality, and balanced activity of the vegetative endocrine system.
"I have called attention to the dependence of the organism for its knowledge of environment and personal identity on the functioning of the general sensory nervous system. This applies both to the voluntary system, the sensorimotor, or cerebrospinal, and to the involuntary or vegetative system; the former putting us in touch with the external world; the latter informing us as to bodily states and personal identity. It has been pointed out that it is through the sensory associations, both somatic and psychic, implanted in the organism, that a habit is built up and maintained. Tobacco was cited to illustrate the manner in which a benign habit may take hold of a person. In this instance there was noted implication of the vegetative system of relatively insignificant character (the pleasurable sensations, etc.) ; insignificant because the associate-memory factors and conative states laid down remain largely within the control • of the volition, in the realm of insight, and outside the domination of automatic impulsion. A habit like tobacco using which does not seriously invade the involuntary nervous system is of benign character; it is when the involuntary, or vegetative, system is seriously invaded, placing the individual more or less outside the realm of volition and insight, that the habit becomes, as it were, malignant, and that serious, it may be ineradicable, alterations take place in the personality."
• • * * •
"In the addict, the mental and character deviations take on a particular coloring, varying with the original constitutional character make-up of the individual, and the relative sensitiveness of the different parts of his vegetative apparatus to the drug. Certain of these deviations can be definitely correlated with alterations in function of particular vegetative activities—as observed in connection with the physiologic changes in the realm of sex due to the drug. In general, the addict becomes timid, fearful, secretive and asocial. Just as the cardiovascular system in an habitué adjusts itself to the physiologic support of an opiate, so in the character realm the habitué adjusts himself psychically to the support of his drug; he finds in it an agent that artificially fortifies him for meeting pain or difficulties. In order to maintain his so-called drug balance, or state of satisfaction, he must continually increase his supporting drug. He is playing a losing game by the necessity of compensating artificially against the weakening of character that inevitably results from the removal of the necessity of meeting obligations and exigencies through the discipline of effort. The normal appetites and hungers by which the organism makes known its needs are to a degree neutralized. The cycles of hunger and appeasement, of wakefulness and sleep, of work and rest, are broken in their normal sequence, and cease to guide the individual along self-preservative lines. He may be chronically exhausted, but realization of the fact may be shut off, and therefore unheeded.
"The drug has the effect of lulling the victim into a sense of security out of keeping with obvious facts of reality. His conduct is determined by these false convictions; the future holds no menace, yet the sheriff may be at his door; he plans confidently for impossible undertakings, though in imminent danger of death from some obvious organic disease. Because of these false convictions, which have gradually and insidiously established themselves in the addict's mind, he often acquires the belief, amounting to a delusional idea, that the drug must be good for him. (In some persons, these beliefs and convictions are of slow growth—over years; in others the altered personality becomes rapidly established.) All this disruption of the processes of thought, and of the vegetative functions that underlie emotional and instinctive reactions constituting the essence of personality, cannot long continue without the fairly permanent establishment of a psychopathologic status. At times, the alteration of personality and judgment becomes so fixed that insight cannot be reestablished and return to the drug will be inevitable, except under restraint."
"Summary.—Habit-forming drugs produce different and more complicated pathologic changes than those produced by other toxins and infectious agents.
"Morphin produces its most serious effects through its action on the vegetative nervous system.
"Habit-forming drugs induce a distortion of normal reflex activities in both sensory and psychic spheres.
"The substitution of a psychopathic status is maintained by increasing the obtunding drug to offset the ever,decreasing compensatory efforts of the organism.
"Because of the overwhelming dependence of instinctive and emotional life on visceral and endocrine functioning, instinctive and character deviations follow prolonged disturbance of their activities with more or less permanent changes resulting in the entire personality. This mechanism, I believe, is the essential lesion in narcotic addictions.
"The theory here suggested supplies a basis for the understanding of narcotism on which the entire symptomatology can be adequately explained."
R. Schoen-1924.55
After studying the effect of a single dose of morphin on the blood reaction 56 and basal metabolism in normal human beings, the author investigated the behavior of basal metabolism and blood reaction in addiction. The addicted patient on whom the observations were made was a young man suffering from mild parkinsonianism without tremor when at rest. The behavior of basal metabolism, blood reaction, respiration and pupils was observed regularly and recorded' graphically.
Schoen discusses the results of his observations as follows:
"Extension of the investigation to the condition following regularly repeated doses of morphin led to the surprising result that both the reduction of basal metabolism observed after the first dose of morphin and the acidosis of the blood arise and disappear in addiction with extraordinary rapidity. In this respect they stand in sharp contrast to the effect on respiration and the pupils, which maintained undiminished strength in the same series of experiments. These striking, yet familiar conditions seem to me to prove the relationship of the reduction in basal metabolism to acidosis, which before could only be conjectured. The occurrence of acidosis after morphin is rendered possible by the paralysis of the respiratory centre and the resulting accumulation of carbonic acid in the blood. The direct cause, however, resides in the acid products of metabolism, which are due to reduced oxidation. When this diminution of basal metabolism ceases, acidosis disappears from the blood. The close dependence of altered urinary reaction en the reaction of the blood is shown afresh by their behavior in addiction, as well as by the absence of a fixed relation between the alveolar carbonic acid tension and the blood and urinary reactions, as Endres supposes, so soon as the sensitiveness of the respiratory centre is diminished. While the carbonic acid tension remains completely uninfluenced by addiction, the blood and urinary reactions behave very differently from before.
"In those unused to morphin the secretion of hydrochloric acid by the stomach immediately after administration of morphin is regarded as a compensatory action due to acidosis. This theory is also supported by our experiences of addiction. Schubel demonstrated, for instance, that in dogs this hypersecretion disappears very early in addiction and a `secretion narcosis' occurs. This may be explained naturally by the disappearance of acidosis.
"For a general understanding of the morphin addiction which Faust's experiments show to be due in part to rapid destruction of morphin in the bodies of animals the fact is of unquestionable importance that the initial reduction of metabolism very quickly gives place in presence of addiction and then is seen to undergo a transformation to. increased metabolism. Without discussing this intricate problem, it may be conjectured that this increase in metabolism contributes materially to the rapid destruction of morphin as a cause of addiction.
"The object of the reports given has been to study the influence on the blood reaction of diminished sensitiveness on the part of the respiratory centre as the general respiratory mechanism of the blood reaction. Analysis of the changes observed threw light also on the reaction of morphin, the agent used. If paralysis of the respiratory centre by this alkaloid is taken as the principal point of consideration, the alterations occurring in the blood and urinary reactions, probably that also in the gastric juice, may be explained as secondary consequences, as likewise—a connecting link to increased carbonic acid tension in the bloodmorphin myosis (Wieland and Schoen). The altered metabolism which precipitates the condition of acidosis in the blood seems unconnected with the respiratory centre. This is especially shown by the different conduct of these in addiction. Campbell's observations have demonstrated succinctly that hyperventilation from alkalosis produces increased metabolism, and that acidosis and alkalosis on their part, in presence of decided paralysis of the respiratory centre, may cause metabolic changes. Although experience with morphin seems on the other hand to show the acidosis to result from the diminished basal metabolism, still the contemporary occurrence of an altered blood reaction (on paralysis of the respiratory centre) and of metabolic alterations is a phenomenon of more general significance.
"If we are very far from a uniform explanation of the action of morphin, at least the way is plain in which we can simplify the complicated picture by throwing light upon the mutual relationship of certain of its phenomena."
"In human beings at rest basal metabolism was reduced about twenty to twenty-five per cent in the first hour after injection of morphin in doses of one and two centigrams. Repeated doses were attended by very rapid disappearance of this diminished metabolism and by a return to the initial level. At the same time the acidosis previously described (section 1) as following morphin, also disappears. From its behavior during addiction, which at this early stage gives no evidence of affecting the respiration and the pupils, the conclusion is reached that the acidosis resulting from morphin is caused by the increase of acid products of metabolism consequent on reduced basal metabolism. A warrant for this is the failure of the reaction regulating function of the paralyzed respiratory centre."
B. Legewie-1924.57
This author reports a detailed history of a case of delirium in morphinism, which although rarely observed is caused, he believes, by morphin abstinence and not by the primary disease. He states:
"The case represents a peculiar type of man in whose family history morphin played an important role, who showed a personal and family tendency to delirium and who for many years has been a marked gastrointestinal hypochondriac. When he was 58 years old he became ill with cancer of the rectum and on account of great pain was given morphin. It is certain that he himself never took morphin publicly or privately and that his dose was increased very gradually until it reached (before the delirium) 0.06-0.08 g. daily. From the beginning he showed an oversensitiveness to the morphin with symptoms such as muscular spasms, marked trembling of the whole body and chills. Psychically at first he experienced a phase of productive euphoria lasting for a month and followed by a like period of lethargy. Three months after the administration of the first dose of morphin and three months before death the first signs of a progressive derangement appeared. At first there were hallucinations which in the beginning he corrected himself and later others easily handled. The symptoms gradually increased, he became more restless, disoriented, thought himself followed, failed to recognize his surroundings, suffered from frequent and especially optical hallucinations, and showed great motor excitation. But there were no symptoms of circulatory weakness or other changes in his physical state. At the height of delirium he showed marked stupefaction. Upon a relatively large dose of morphin the delirium ceased abruptly. Until death, which took place eight days later, the patient remained under the influence of large doses of morphin, showing symptoms of intoxication such as nausea, salty taste, etc., but psychically he was self-possessed and normal. On the day before death the first symptoms of circulatory weakness showed, and then followed sudden death in spite of a relative state of well-being."
Speaking of the origin of the delirium, the author states:
"If from a differential-diagnostic point of view we were to enumerate the causes involved, we should have to consider only the possibility of origin in exhaustion or inanition, in the organic or toxic action of the carcinoma, in an autointoxication from constipation or in the action of the morphin."
Legewie disposes of the first four possibilities and explains his
hypothesis that the action of the morphin accounts for the delirium as follows:
"There are two other reasons for attributing the origin of the delirium to the morphin. In the first place undoubtedly with the beginning of the morphin administration there appeared also a change in the patient's psychic state. At first we observed a euphoric overproduction, which could be distinguished from the usual euphoria of chronic morphinism by its nature and intensity. The patient showed none of the general high spirits of complete comfort. On the contrary from the earliest injection of morphin there appeared such unpleasant symptoms that after a short time he feared injections. Also he himself was unaware of his high spirits. For this reason if they faded he could show no desire to renew them with a further dose of morphin. But in fact he was in high spirits. For, apart from his inclination to joke, which postulates a general feeling of comfort, how else could such functional increase be explained? This picture represents a slightly hypomanic state rather than the usual euphoria of morphinism. Yet there could be no doubt as to the existence of some relationship to the morphin administration.- I prefer to consider it a positive effect of morphin analogous to the usual euphoria, but corresponding to the other unusual reactivity of our patient to morphin.
"The same applies to the subsequent state of loss of interest and increased depression—at this time also there was a positive action of the morphin on the cerebrum.
"Following upon this state there began gradually a psychotic alteration which seemed to have no connection with the previous state and which slowly increased to the point of delirium. Now we come to the second cause which touches upon the relationship of the morphin administration, namely, the prompt control of the delirium by morphin upon the administration of a dose considerably larger than that previously administered. It is not likely that a delirium produced either directly or indirectly by the primary disease shortly before death and therefore at the height of the exhaustion, constipation, or cachexia, could cease upon a relatively small dose of morphin. This became the more obvious to me when I myself at first thought of an autointoxication psychosis. This is supported further by the fact that there must have been an under-supply of morphin. Also the patient when the dose was withdrawn again reverted to physical and mental discomfort. Upon repeatedly high doses the patient remained quiet. In our case therefore the morphin at first showed a marked alteration in the whole psyche, a change which doubtless may be caused by morphin intoxication but which varies from that usually formed in morphinists by reason of the peculiar constitution of our patient. On the other hand under-dosing for a long period was sufficient to produce a delirium which promptly was controlled by a corresponding increase in the dose. In both cases, there was a marked action of the morphin on the cerebrum. It is certain, however, that both series of symptoms did not run simultaneously. Probably they followed each other but they were antithetical. If we consider the one as a positive action such as chronic intoxication, we must consider the other a negative one such as the effect of abstinence. It cannot be a positive morphin injury through chronic abuse because otherwise under the prevailing conditions there could be no stopping of the delirium with an increase in the dose. This applies also, if we agree wtih Chotzen as to the psychotic symptoms being an indirect effect of the morphin, in relation to the general prostration brought about by the morphin intoxication. It is not possible to see why the symptoms of poisoning of a psychical nature appear so often after the withdrawal of the drug as was the case in two of his four patients who were `pure' morphinists, except on the basis that the prostration must have progressed upon the further administration of the morphin and led to a delirium at the same time during the abuse of morphin. The lack of a desire for the drug in our patient was striking. There must have been involved at one time influences affecting the personality of the patient upon which the morphin history showed little light; but then also the secondary symptoms were so great that they created a natural resistance. I do not think that a true morphinist, a person morbidly desiring morphin, with an opportunity to obtain a further supply would have run blindly into a delirium. Still I do not think that from this lack of desire we should conclude that there was any different reaction from that of pure morphinism in our patient during abstinence.
"Therefore for me it is beyond doubt that the morphin produced the delirium. The lack of morphin led to the delirium or, in other words, we have here in a delirium susceptible psychopath during the pure use of morphin an abstinence delirium. Therefore this case offers an exception to the view held by Bonhoeffer cited above."
Torald Solmann-1924-1926.58 58'
In a report of experiments dealing with the effect on the growth of white rats of chronic poisoning by certain drugs, the author, 1924,58 gives the following conclusions as to the effect of the morphin group:
"Morphine, codeine and heroin increase body weight materially above the normal control animals; with codeine, the increase continued throughout the twenty-seven weeks, even with daily doses rising to 870 mgm. per kilogram. With morphine, the increase of body weight turned into a sharp and steady decline, after 11 weeks, even when the daily dosage had reached only 2.5 mgm. per kilogram. With heroin different groups of rats gave discordant results."
"The rats often showed a marked preference for the drugged food; but this occurred also with non-addiction drugs, and was probably not due to `craving,' but to other, accidental causes. No `abstinence symptoms' were noted on temporary withdrawal."
As to the late mental and physical effects of opium addiction in human beings,6e' Sollmann says:
"The life of the addict is doniinated by the abstinence symptoms that start when the effect of the dosage begins to wear off; by the consequent need of obtaining the drug at any cost; and often by the fear of detection. If the supply is regular, the addicts may appear quite normal; so much so that the addiction may be kept secret for many years, and the addict may occupy responsible positions. Close observation, however, would generally reveal signs of the addiction; especially variability of moods, depressed or stimulated, according to the interval since the last dose.
"Opiate debauches doubtless accentuate the weaknesses of moral character from which they originate. They tend to make their victims slothful, apathetic and unreliable. They do not lead to the more active crimes, as cocaine may; except in so far as crime may be necessary for obtaining the drug.
"The addicts of inherently good character, if they take the drug solely to ward off the intolerable depression, are not so seriously affected. Their will-power and self-reliance is weakened, as by any other enslaving self-indulgence, and the agony of drug-deprivation drives them to deception and more serious crimes when their supply is threatened; but outside of this, their character and mental faculties are said to remain practically normal. A large part of the traditional depravity of the addicts exists. in the minds of the public, rather than in life. This pariah-attitude makes it more difficult for the addicts to lead a normal life, and thus tends to drive them into the very vices of which they are accused. (Bishop).
"Physicians should look upon drug addicts as patients with a nervous disease. Like other nervous patients, they must be treated with firmness, but also with sympathy and kindness.
"The moderate use of opiates may not produce any definite physical deteriorations. Animals, at least, may even gain in weight, presumably by being less active. With more severe addiction, the digestion becomes seriously disturbed, obstinate constipation alternating later with equally obstinate diarrhea, loss of appetite alternating with voracious hunger and thirst and polyuria. The patient loses weight rapidly, and suffers from marasmus and cachexia.
"The skin becomes hard, pale, dry and rough; sometimes, of a peculiar waxy appearance. The nails, teeth and hair are also diseased. The condition of the integument is rendered worse by the local effects of the injections when the drug is used hypodermically. The whole skin may be mottled with scars and marks of recent or older injections, and abscesses are often produced through want of cleanliness.
"The pupils are usually contracted. The pupillary and accommodation movements. are affected. The heart may become irregular. Albuminuria, glycosuria and amenorrhea are frequent. The sexual functions are lessened (functional impotence, sterility), but usually return on withdrawal. (Wholey, 1912.) Fevers resembling simplex, intermittent, and typhoid are seen. The motor-nervous system shows considerable change: nervous tremors, increased reflex irritability, etc. These conditions sooner or later weaken the resisting powers of the patient, so that he falls an easy prey to some other ailment, and thus rarely reaches old age. However the habit may persist for over thirty years (McIver and Price)."
L. Stern-Piper-1925.59
This author studied the rate of sedimentation of the blood of ten cases of chronic morphinism and six of eukodalism, both during addiction and during withdrawal, according to the technique used in an earlier study in relation to post-encephalitic disturbances analogous to that used in expressing the different degrees of fixation in the Wassermann reaction.
He found that in nine of the ten cases of morphinism tested during addiction the rate was accelerated, while in one it was retarded. During withdrawal, however, the rate gradually lessened, reaching normal in four and one-half to five months. Practically the same results were obtained in the cases of eukodalism, although they were found to be much less definite.
On the basis of his experiments the author speculates as follows:
"From the theoretical point of view, in analogy with the concept of Linzenmeier of the processes of sedimentation acceleration as a defensive reaction of the plasma to the introduction of foreign proteins, with the attendant increase in the globulin fraction at the expense of the albumins, the same phenomena might be conceived to take place as a defense mechanism against the morphin in the circulating blood in chronic cases, or against certain decomposition products which may be produced. Possibly the formation of these latter substances may be associated with a chronic stimulation of the parasympathetic system by the poison, in accord with the theory of Wuth that assumes an increase in tonus of the parasympathetic during habituation and during abstinence a tonic change in the sympathetic. That in in vitro experiments, as I have found, morphin does not cause an acceleration, but rather a transitory retardation of the sedimentation velocity, cannot be adduced as evidence on this point. In the test tube morphin is also weakly hemolytic. But for the formation of the defensive substances a chronic stimulation by the poisons must require a comparatively long time, such as can only be evidenced in. vivo. During the process of deprivation it must be assumed that with the suppression of the poison or with the lack of the decomposition products caused by its stimulation, the sedimentation velocity gradually diminishes. That, as Wuth assumes, endocrine principles, possibly associated with an hyperfunction of the thyroid, are to be found in the blood during the period of withdrawal of the drug, does not directly oppose the fact of the loss in acceleration during abstinence, since it must be assumed that these substances, as native to the body, exert no accelerating effect upon the sedimentation velocity."
• • • • •
"My studies should stimulate further work upon the question of the relations of sedimentation velocity in morphinism. If my observations can be confirmed by tests on a larger number of cases, the sedimentation velocity rate should prove of diagnostic value in cases where there is a chronic morphinism due to injection of the drug. The method should also serve to distinguish whether a patient has relapsed again or whether he is still in the chronic stage of addiction.
"As for the question of the duration of the process of breaking away from the use of the drug the test may be of the greatest clinical importance. If my experience affords an index, cases—with an initial, very strongly positive reaction which gradually becomes reduced during the period of deprivation—should always be kept under control up to the time that the sedimentation rate is restored to normal, that is, for at least four to five months.
"Further, it must never be forgotten that the value of the method is limited, in that other disturbances, particularly the infectious diseases, must be excluded.
"As for the value of the method in eukodalism no definite statement can be made, although in this condition also changes in the rate of sedimentation have been observed. Further studies are here necessary. For the diagnosis of eukodalism, as well as for a means to determining the duration of the period of deprivation in this condition the validity of the sedimentation velocity determination cannot at present be considered."
Lawrence Kolb-1925°°
The author distinguishes between the pleasure and relaxation of relief from pain, and the mental pleasure derived by certain individuals from the use of opium. The former of these states is a negative pleasure, the latter, a positive one. Individuals, he states, who receive positive pleasure from opium continue its use until it becomes a physical necessity, increasing the dose as more of the drug becomes necessary to produce the effect. As tolerance is established, positive pleasure is decreased and practically the only pleasure then received from the drug is that arising from the relief of withdrawal symptoms. After the first stage of addiction, when supplies of opium are irregular, the addicted individual passes through periods of comfort and discomfort to which is added the anxiety arising from police activities and the fear that the next dose will not be available. He is restless, discontented and unhappy, and more and more of the drug is necessary to maintain comfort, until a point is reached where pleasure is overshadowed completely by pain. At this point frequently addicts seek treatment and when, after this, their health improves, the fundamental psychic distresses for the relief of which the drug originally was taken again assert themselves and with the memory association of the pleasure opium once gave relapse is almost certain, with a recurrence of the former cycle of events.
The author finds from his studies that the intensity of pleasure produced by opiates is in direct proportion to the degree of psychopathy of the individual in question, and that the subsequent repression from long-continued use carries him as far below his normal emotional plane as the first exaltation carried him above it. The author continues:
"The unhappy state into which addicts oT long standing finally descend is such that a superficial examination of a group of them with low native intelligence or lack of education might lead one to believe that only a small proportion of them ever received pleasure from opium apart from that involved in its power to relieve withdrawal symptoms.
"With few exceptions they say: `It only makes me comfortable.' This explanation is apparently true for most, if not for all, nervously normal people who become addicted, but it is not true of the abnormal type who make up the bulk of addicts of the present time--and it is probable that no person who deliberately addicts himself fails to derive pleasure of some kind from the drug. When the addiction history of a group of addicts is studied carefully, it is found that practically all of the psychopaths and neurotics among them have for a longer or shorter period experienced some sort of mental pleasure from the use of opiates. But most of the cases are seen by physicians long after the memory of the short period of pleasure has been beclouded by the distress that later ensued. This distress causes them to seek relief, and it is uppermost in their minds. They are, therefore, honest when they claim to take the drug only to prevent suffering.
"The examination of intelligent people able to give expression to their feelings is more satisfactory, and it is mostly from these that we discover the secret of how the pleasure that opium induces in psychopaths allures them into addiction in the first place and causes them to relapse time after time.
"Whether opium causes pleasure to absolutely stable individuals is difficult to decide. Fourteen per cent of the addicts in the series of cases (230 in number) with which this paper deals were classified as having been normal before they became addicted, and a few of these received pleasure from the drug that did not seem to be a mere contrast with the discomfort that it relieved. The examination of these apparently normal cases that received unusual satisfaction from the drug was not, however, as thorough in all of its phases as was desirable, and it is possible that a more extended study of the cases would have disclosed traits of personality or abnormal trends that would have justified placing them definitely among one of the nervously abnormal classes referred to in an earlier paper."'
The author then cites a case in illustration of the fact that normal individuals sometimes derive pleasure from taking an opiate. He continues:
"Against apparently stable persons of this kind who receive pleasure from opium are the thousands of persons who have taken an opiate prescribed by physicians without feeling anything but drowsiness and relief from actual pain. It would appear from this that those individuals who are made happy by opium must have some special mental conflict that the drug relieves, even though they are not nervously abnormal in the ordinary sense.
"In one series of twelve professional men among these cases who admitted receiving pleasure from opium, ten had either been drunkards or were neurotic individuals before they became addicted. The father of one of the others had migraine; a sister, epilepsy; and a brother, aged twenty-eight, died of apoplexy. The addict himself had apparently been normal, but was always timid and somewhat shrinking in his contact with other people.
"Another professional man who derived pleasure from cocaine felt none whatever when he later became addicted to morphine.
"The more nearly normal of the abnormal cases referred to above had been addicted twenty-two years. His father was neurotic and had a strong tendency to despondency; a sister died of apoplexy. The patient himself had a normal, open make-up as a boy in so far as outward appearances and social activities were concerned, but with it there was a feeling of bashfulness and a disposition to be easily discouraged. Like a brother of his, he always shrank from pain and his attitude may be best indicated by his description of what to him were the horrors of treatment for drug addiction. His body, he said, felt as if it were being placed alternately in fire, scalding water, and acid. He was successful in his profession, a respected citizen, and took an active part in politics, but always felt ill at ease when required to take a leading part in any gathering. He found that opium gave him confidence and enabled him to meet people without inwardly shrinking and without feelings of restraint. This was not interpreted by him as pleasure, but he described what he called a condition of ecstasy which once came over him, after a hard day's work, while he was riding to the barn on a load of hay. This was before he started to use the drug, but he has experienced a similar feeling a few times since, following hypodermic injections. It is probable that the feeling he described is akin to that aroused sometimes in normal people by the pleasurable relaxation and satisfaction that supervenes upon the completion of a difficult task.
"It frequently happens that the first experience with opium produces more pleasure than any subsequent indulgence arouses. When the first dose is taken for illness, the added factor of relief from physical pain furnishes a ready explanation for this—and the rheumatic physician who struggled to stay awake never again experienced the same intensity of feeling. In other cases the explanation probably is that its newness is an added charm."
"The expressions that addicts make use of in describing their sensations illustrate better than anything else the mental pleasure that opium gives abnormal persons. At the same time they show the neurotic basis of addiction by indicating emotional conflicts or feelings of inadequacy, the relief from which is expressed as pleasure. The following are some of the common statements made:
" `It makes my troubles roll off my mind.'
" `I do not have a care in the world.'
" `It is exhilarating and soothing.'
"You do not care for anything and you feel happy.'
" `You have a contented feeling and nothing worries you.'
" `It stimulates you and makes you forget, so you don't care about anything.'
"'It makes you drowsy and feel normal.'
"'It causes exhilaration and a feeling of comfort.' "'A deadening, pleasurable effect.'
"A clear inference from the foregoing expressions is that opium produces in these cases a feeling of mental peace and calm to which they are not accustomed and which they can not normally achieve."
"A better description of the pleasurable effect of opiates than the average untutored addict gives might be expected from highly educated persons. One of these, typical of others, said it caused a buoyancy of spirits, increased imagination, temporarily enlarged the brain power, and made him think of things he otherwise would not have thought of.
"In addition to the mental pleasure produced by opium, some addicts receive a pleasurable physical thrill of short duration and varying intensity immediately following an injection of morphine or heroin. As the intensity of this thrill wanes with increasing tolerance, sonic resort to injections directly into the veins in order to bring it out in full force again. It is largely this thrill which addicts have in mind when they speak of the 'kick' that the 'shot' gives them. Most of them describe it as a feeling of warmth that quickly spreads through the abdomen following an injection. The description suggests vasomotor relaxation with increased blood to the parts. In some cases the thrill spreads throughout the entire body and then gives intense pleasure. Striving for a repetition of it naturally leads to larger doses.
"The physical thrill apparently sometimes takes a sensuous character. An addict with an intelligence quotient of 110, who described the mental effect as 'a feeling of comfort so that nothing worries you,' said, in regard to the physical thrill, that it was a pleasurable, tingling sensation that passed over the entire body. He linked this sensation with sexual feeling and mentioned that some of his associates gave it the same coloring. Another psychopath, with an intelligence quotient of 88, described the sensation as a thrill through the body lasting seven or eight minutes and resembling the sexual orgasm. The brother of this patient derived intense pleasure from the thrill, but said that it did not in any way resemble sexual feeling.
"None of the thirty-one nervously stable addicts in this series of cases had experienced anything but a slight feeling of warmth in the abdomen following injections of morphine or heroin. This was considered pleasurable except in so far as it was a part of the general feeling of comfort and relief that is brought on in all addicts when a needed dose wards off oncoming withdrawal symptoms. The apparent immunity to the thrill of normal persons who become addicts may be explained in part by the fact that such addicts do not take 60 grains of morphine daily nor do they inject the drug directly into the veins, but in the psychopaths the degree of pleasure seems to depend upon the degree of psychopathy, and it is possible that the sympathetic nervous system of these abnormal cases may be so constituted as to be more susceptible to the influence of narcotics."
He then proceeds with a discussion of the use of cocain and the sensations arising therefrom, after which he states:
"As would be expected, cocaine and an opiate combined give more intense pleasure than either of these drugs alone...."
Under the heading of "Deterioration," the author continues:
"The production of pleasure by such unnatural means as the introduction into the organism of substances that distort body functions and change the flow of emotions, so that for the time being there is a different outlook on the world, may be expected to bring about a gradual change in character, mentality, and physical condition that in most cases would be harmful. This expectation is in part realized in the majority of cases. In fact, the continued use of opium or cocaine is always harmful physically, but in studying the effects of these drugs on the mental and moral characteristics of addicts it is important to consider the type of persons from whom they are recruited and judge each individual addict according to what he was before he became addicted. An influence that injures a normal individual by perverting his normal body functions may improve an unstable individual by changing his perverted functions. In an earlier paper the writer has indicated how that property of opium which produces lethargy and idleness in normal persons may express itself as a temporary stabilizing influence in criminal psychopaths by blotting out the underlying stresses that give rise to the irritability, discontent, and unrest that result in the commission of crime. The soothing effect of the drug causes in one case the loss of ambition for useful work, and in the other an abatement or suppression of abnormal or antisocial impulses.
"In evaluating the effect that narcotics may have produced in any given case, it is necessary to have clearly in mind, and to consider collectively, the original character of the person, the physical harm that the drugs have done to him, the mental and moral consequences of the physical difficulties, the stabilizing influence, if any, that may have been exerted by the drugs, and the demoralizing effect upon the addict of being looked upon as an outcast or criminal.
"There is a widespread belief that addiction to opium leads rapidly and inevitably to moral deterioration. This belief has arisen through a failure to appreciate that the psychopath who was originally a murderer, thief, drunkard, or social offender of one kind or another is more susceptible to addiction than stable people—and during the past thirty years the public psychology with regard to drug addiction has been such that normal addicts have concealed their addiction whereas the delinquency of the psychopathic addict has kept him in the public eye. The consequence has been that practically all addicts with whom the public has been acquainted have been deservedly despised, and the inference that the addiction was solely responsible for their antisocial behavior a,nd useless lives was inevitable.
"When addicts are carefully studied, it is found that some of them have not been injured morally or mentally. A larger proportion have deteriorated morally, and a few, chiefly former drunkards, have been helped by opium.
Intellectual deterioration is apparently never due to the use of an opiate alone. Morphine and heroin have not been found to differ in so far as the degree or kind of deterioration produced by them is concerned. Cocaine is a much more injurious drug, and it seems that most of those who have deteriorated have used both an opiate and cocaine.
Degree of Deterioration: Different Types
"That individuals may take morphine or some other opiate for twenty years or more without showing intellectual or moral deterioration is a common experience of every physician who has studied the subject, and years ago, when addiction was much more common than it is today, many practitioners had one or two such cases among their patients. In this series most of the normal cases, and many of the neurotics, have not suffered any demonstrable moral or mental deterioration.
"The statement that certain addicts have not deteriorated does not mean that they are of the highest type of citizen. The highest type of citizen is a moral individual with superior intellect balanced by a normal flow of emotions and with a personality undisturbed by nervous instability of any kind. Very few persons answering to this description ever become addicted except through the necessities of unusual stresses, and their addiction is usually quickly cured when the stress is relieved. What is meant is that these addicts started off with a varying degree of mental and moral equipment that has not been demonstrably changed by opium.
"The criterion for lack of deterioration in individuals originally useful and in good standing in the community has been continued employment in useful occupations, the respect of associates, living in conformity with accepted social customs, avoidance of legal prosecution except those brought about by violations of narcotic laws, undiminished mental activity, and unchanged personality, or, when this could not be determined, the possession of a personality that would be considered by psychiatrists to be within the range presented by nervously normal individuals or mild psychoneurotics.
"We think it must be accepted that a man is morally and mentally normal who graduates in medicine, marries and raises a family of useful children, practices medicine for thirty or forty years, never becomes involved in questionable transactions, takes a part in the affairs of the community, and is looked upon as one of its leading citizens. The same applies to a lawyer who worked himself up from a poor boy to one of the leading attorneys in his county, who became addicted to morphine following a severe abdominal disease with recurrence and two operations, and who continued to practice his profession with undiminished vigor in spite of his physical malady and the addiction."
* * * * *
"In one group of twenty-five professional men who were carefully studied from the standpoint of deterioration, seventeen had suffered no apparent mental or moral deterioration. Four of these had always been shrinking, fearful neurotics. One had been a drunkard who had apparently been lifted out of the gutter into respectable citizenship by his shift from alcohol to morphine.
Two were apparently above the average in mental and moral stability, and the remaining ten were evenly divided between average normal individuals and persons who in early life, before they began to use opium, had brought more or less discredit upon themselves by indulgence in alcohol, but who had always been socially useful.
"Of the eight deteriorated cases, two had been extreme drunkards before becoming addicted to opium. One of these had been cured of his addiction. only to relapse into whiskey. He was seldom sober. One, now off the drug for nine months, was a respected citizen who had spent much time and money in treatments that were not permanently beneficial. Another highly neurotic individual whose mother was insane is also off the drug. He had suffered several relapses. One, a former drunkard, was suffering from cerebrospinal syphilis and morphine addiction. One, now practicing medicine, once gave up his practice for ten years in order not to tempt himself with opiates. He resumed practice only to relapse, but has now been cured for eight months. Of the two remaining cases, one had delirium and hallucinations of hearing before he became addicted, during and for several months following attacks of malaria. `Voices' also bothered him several times in the course of and for a short time after cures for addiction. The other case, a cocaine-morphine addict with poor heredity, had definitely deteriorated.
"Barring the addict who had hallucinations of hearing before becoming addicted, only two of the eight had deteriorated mentally—and with the possible exception of the syphilitic patient, none had deteriorated in the intellectual sphere.
"The relative amount of harm chargeable to narcotics and to other factors in these eight cases is difficult to determine with certainty. It is believed that opium and cocaine have contributed materially to the ruin of the two that deteriorated mentally, and have lowered the moral tone and decreased the social efficiency of all of the others. The moral slump was slowed up, but not arrested, in the two drunkards by the change from whiskey to opium. but both of them might have been respectable and much more useful citizens had they avoided both of these poisons."
The author speaks of the mechanism of deterioration in what follows:
"The greatest degree of deterioration occurs in the group of addicts recruited from among carefree, pleasure-seeking young persons who are mildly neurotic or whose personalities deviate somewhat from the normal. The stability of more nearly normal addicts enables them to carry on efficiently in spite of their addiction, and the criminal psychopaths are already so devoid of moral sense that but little more deterioration is possible with them, while in many of the inebriate addicts, where the narcotic is substituted for excessive doses of a more destructive poison, deterioration is sometimes arrested or retarded by the change from alcohol to opium.
"The mental and moral deterioration due to opium is traceable to the physiological effect of the drug and the social consequences of a life of addiction.
There is no destruction of protoplasm such as follows prolonged excessive use of alcohol. Neither nerve cells nor fibers degenerate; consequently the drug cannot produce diseases analogous to Karsakoff's psychosis, acute hallucinosis, or alcoholic multiple-neuritis, and hospitals for the insane have remarkably few cases diagnosed as drug psychosis. Such psychoses are so rare that one is led to suspect that Case 72 is typical of most of those that do occur.
"Morphine and heroin, when taken in large doses, sap the physical and mental energy; lethargy is produced, ambition is lessened, and the pleasurable feeling already described—that all is well—makes the addicts contented. These various effects cause them to pay less attention to work than formerly; consequently, they tend to become idlers and dependents, but only a small proportion are made idlers by this means alone. Those who depend upon the illegitimate traffic are sometimes unable to work because of discomfort and weakness due to insufficient narcotics, and at other times they stay away from their work in order to look for the drug. There are cases in this series who have gone to distant cities regularly to get an ounce of heroin or morphine, and others who have lost as many as a dozen jobs through neglecting work to meet their peddlers or through lying in bed in the morning instead of going to work because the dose that would have put energy into them was not available. Often, when these cases secure a supply, after their short periods of deprivation, they take more than is actually necessary to keep them comfortable. The result is that they alternate between physical and mental irritability and physical and mental lethargy. Both extremes make for emaciation, physical inefficiency, and unusual mental reactions.
"The dreamy satisfaction and the pleasurable physical thrill produced by opium in many addicts in their early experiences with it are of themselves forms of dissipation that tend to cause moral deterioration. Addicts as a rule are compelled to associate with persons of low moral character in order to continue their addiction. Financial embarrassment resulting from idleness or the high price of peddled narcotics impels them to beg money from their friends, obtain it from members of their families by subterfuge, or steal, in order to supply themselves with drugs; they suffer in manliness through feeling what they often consider the just contempt of the public; they suffer more through their constant fear of arrest or because of a term in the penitentiary served for having narcotics in their possession.
"The whole train of events above described brings about unfavorable character changes and gradual moral deterioration, and converts what might have been fairly useful citizens into outcasts, idlers, or dependents.
"It has been difficult in some of the cases to determine whether the moral deterioration has been wholly or partly due to drugs or whether it would have occurred in the natural evolution of their personalities. When a boy is so incorrigible that it is necessary to train him in a reformatory, not much is expected of him. The same is true to a less degree of the neurotic child who has been petted, pampered, and spoiled by his parents. The deteriorated cases comprise some whose early life histories conform to the above and who may have been useless in any event, but the study of their life histories seems to show that narcotics added a handicap which made them worse than they otherwise would have been."
Of the effect of addiction on industrial efficiency, Dr. Kolb states:
"In connection with the deterioration caused by addiction, the industrial records of 172 of these cases have been surveyed. The records were considered to be good or fair in 88, and irregular or unsatisfactory in 84 cases.
"The criterion for a good or fair record was continued employment and satisfactory work. Housewives who performed their household duties with average efficiency for the social class to which they belonged were classified with those having good records. A sojourn in the penitentiary for violation of narcotic laws has, in this classification, not been allowed to vitiate an otherwise good industrial record. Some cases who were self-sustaining, but who worked in inferior positions because of their addiction, have been classified as having poor records. The percentage who have good records is probably surprising to those who accept the general view that addicts are almost invariably useless characters. The percentage might have been higher but for the inconvenience caused in some of these cases by necessary narcotic laws.
"Of the entire number, 512 per cent had good industrial records, but if the professional men and colored people are excluded from the reckoning, only 42 per cent had good records. The records were good or fair in 18 of 24 of the professional men, and in 18 of 24 colored persons. The reason for the percentage of good records shown by the colored addicts is that most of them were recruited from normal individuals. The professional men maintained themselves on a higher plane of industrial efficiency because of their superior intelligence, higher average of nervous normality, and more advantageous position from a financial standpoint. Three of the six professional men rated as irregular or poor owed their industrial inefficiency to excessive drinking before they became addicted to drugs. Two, one of whom is rated as very poor, were harmed by morphine and cocaine, but the probabilities are that both of these cases would have made an unsatisfactory showing in any event. The other one has always been self-sustaining, but is rated irregular because his struggle with narcotics impelled him to accept for a time a position financially and socially less satisfactory than his education and training should have afforded.
"No case classed as nervously normal in this entire series showed a poor industrial record, but in some abnormal cases the record was good. The psychopathic nature of some of these cases was such that even without narcotics nothing but an idle, aimless life could have been expected. Some of the inebriates had good industrial records, and the history presented by a few of them seemed to indicate that had they not changed from alcohol to opium, they would have been useless drunkards.”
The author summarizes as follows:
"Opiates apparently do not produce mental pleasure in stable persons, except a slight pleasure brought about in some cases by the reflex from relief of acute pain.
"In most unstable persons opiates produce mental pleasure during the early period of addiction. The degree of pleasure seems to depend upon the degree of instability.
"A large number of addicts experience a pleasurable physical thrill following injection of morphine or heroin. Normal addicts experience this thrill in only a very slight degree, if at all.
"Cocaine may produce pleasurable stimulation in both the normal and abnormal, but the pleasurable effect is slight in nervously normal individuals.
"Nervously normal opium addicts apparently do not undergo appreciable mental or moral deterioration, but this class of addicts constitutes only a small proportion of the total number in the United States.
"Much of the moral deterioration attributed to narcotics in the past was not deterioration, but an original nervous instability and moral obliquity.
"Mildly psychopathic individuals deteriorate more because of their addiction than any other class of addicts.
"No preparation of opium produces any appreciable intellectual deterioration. "If there is any difference in the deteriorating effect of morphine and heroin on addicts, it is too slight to be demonstrated clinically.
"Cocaine is much more harmful than opiates and long-continued use of addiction doses of cocaine is destructive both to the physical and mental well-being of any type of person."
K. H. Collins and A. L. Tatum-1925.82
These authors report observing in dogs, during the course of certain experiments in chronic morphinism, a conditioned salivary reflex, as follows:
"Dogs were given subcutaneous administrations of morphine sulphate daily. A:small amount of morphine (30 to 80 mgm. per animal) produces in the dog salivation and usually emesis and defecation. After seven or eight daily administrations of morphine these dogs salivated profusely and even in a few instances vomited before the morphine had been given. The entrance into the dog room of the person conducting the experiment was in most cases sufficient to precipitate this copious salivation. The sight of a hypodermic syringe never failed to produce a secretion of saliva, which continued for a variable length of time, occasionally for several hours providing distractions, such as feeding, did not occur, or the reaction stopped by the narcosis produced by the subsequent administration of morphine.
"If this salivation is secondary to nausea, it might be suspected that in this condition the ability to swallow was impaired. That this cannot be the case is evidenced by the fact that the dogs were observed to drink and on a few occasions to eat during this period of salivation.
"Pain cannot be a factor since morphine itself is the most powerful of analgesic agents. Furthermore, fear was never at any time evident in these animals.
"Eight dogs have been observed in this study of chronic morphinism and all have developed this phenomenon after seven or eight days. One cat has developed a similar condition after fourteen days, differing from the dog only in the ease with which the reflex is established. Three of these dogs have been receiving morphine daily for a period of four months and at the time of the present writing still salivate at the sight of a hypodermic syringe."
N. Sysak-1925.63
The author gives in detail the postmortem findings and clinical history of two cases of poisoning from morphin; one a case of acute poisoning and the other of chronic poisoning following six years' use of the drug. He sums up these findings and discusses them as follows:
"We have before us, therefore, two cases of death from morphin poisoning—one from acute and the other from chronic poisoning. The first case concerns a young patient, who took a rather large quantity of morphin 11/2 days before death and succumbed to this poisoning. The autopsy revealed in addition to old cirrhotic tuberculosis of the lungs: central necroses in the liver; moderate fatty degeneration, fairly abundant glycogen as well as infiltrates in the periportal connective tissue; also fatty degeneration and moderate hyperemia of the kidneys; adrenals rich in lipoid; fatty degeneration of the heart as well as hemorrhages and ecchymoses in the leptomeninx, pleura, epicardium, and spleen. The case displayed, therefore, two processes alongside each other: an old tubercular pulmonary process, which had almost healed and a new process consequent upon the poisoning. The second case concerned an older man, who had been giving himself morphin injections for six years, finally developed skin abscesses and general oedema, and died of marasmus. The findings at the autopsy were: indurated dermatitis in connection with abscess scars of various ages along with abscesses of the skin; general anemia and oedema of the lower extremities; amyloidosis of the kidneys, liver, and spleen; glycogen in the liver and kidneys; hemosiderosis of the parenchymatous organs and spermato-angitis fibrosa. The man died of marasmus following a skin infection, connected with the chronic morphinism.
"The alterations in the first case agree completely with those seen in acute yellow liver atrophy and in poisoning with phosphorus, chloroform, and mushrooms. The fatty degeneration of the liver as well as of other organs, such as the kidney, the heart, is distinct evidence that in morphin poisoning we have an alteration of the total metabolism in the sense of a lipemia, the morphological expression of which manifests itself in the fatty degeneration of the Kupffer's stellate cells. The fatty degeneration of the liver in my case was not extreme, yet moderately abundant; in particular, the regions about the periportal connective tissues showed infiltrates of only a few small marginal drops of fat. In this connection we must remember that the fatty degeneration of the liver was considerably advanced by the cirrhotic pulmonary tuberculosis, which, as is known, always induces fatty degeneration of the liver. For this reason the extreme fatty degeneration of the liver which, according to the statement of many authors, is supposed to be a characteristic diagnostic symptom of acute yellow atrophy of the liver, cannot be adduced as shown by the findings in this case, as the differential diagnosis of poisonings as against acute yellow atrophy of the liver. We may leave undecided the question as to whether the fatty degeneration in connection with poisoning is to be referred to diminished resorption of nutriment (Salvioli and Sachetto) or to the hindering of the synthetic function of the hepatic cells through disturbances of the oxidation process in particular, or to the activation of lipolytic ferments which, having been thrown into the circulation, bring about the mobilization of fat in the tissues. In my case the lipoids in the adrenals were also augmented, a condition observed also by Landau in acute yellow atrophy of the liver. I might mention, as a noteworthy finding, the fairly abundant glycogen in the hepatic cells which were still well preserved. This finding contradicts the generally prevailing view that liver glycogen is strongly affected and, in fact, diminished by poisons, such as phosphorus, arsenic, sublimate, morphin, and others. This diminution is supposed to be the result of irritation of the sympathetic system either by the poisons directly or by asphyctic action, and either from the central sugar center or from its peripheral nerves and those situated in the liver. The fatty degeneration of the liver associated with poisoning has also been connected with the alleged diminution of glycogen, and many investigators—Rosenfeld among others—have spoken of an antagonism between fat and the storing of glycogen. But Lubarsch has shown that the theory of antagonism is scarcely applicable to the liver. Gierke, on the contrary, has spoken of the parallelism in the deposition of both substances. The findings in this case as well as my investigations among children show that we may not speak of antagonism between fat and the deposition of glycogen, and that glycogen may be found in abundance also in connection with poisoning. There is nothing astonishing in the fact that other investigators came upon different findings if we remember that even under physiological conditions the glycogen content of the liver may vary considerably with the nutrition and previous activity. The picture becomes still more diversified when post-mortem and other circumstances are added. This glycogen finding agrees also with the facts established in animal experiments by Seegen, according to which the formation of sugar in the liver is not affected by the morphin narcosis.
"The necrosis of the hepatic cells was still in an early stage in my case: there were, moreover, no signs of regeneration or reparation. This finding shows clearly that with morphin just as with other kinds of poisoning the necrosis—i.e., increased decomposition of the cellular albumin—occurs during life. Krontowski and Jacobi succeeded in demonstrating this increased decomposition of albumin under the influence of various poisons in vitro, while Freund observed in animal experiments a very considerable increase in the excretion of nitrogen under the influence of large doses of morphin. It seems worthy of note that the necrosis was already present 1% days after the poison had been taken, whereas in poisoning with phosphorus it generally does not appear until later—after 4-7 days, according to Cornil and Brault—and that its location was centro-acinous. From the last comprehensive work by Herxheimer on acute yellow atrophy of the liver and related lesions, we know that necrosis in the liver characterizes not only acute yellow atrophy of the liver, but also poisoning with chloroform, phosphorus. Amanita phalloides; its location, however, is not the same for all diseases. In poisoning with phosphorus it may vary. Renz, Ranvier, Cornil and Brault, among others, have seen it in the periphery; d'Amore Falcone, Krönig, in the center. In poisoning with chloroform as well as with Amanita phalloides the centro-acinous region is favored. In acute yellow atrophy of the liver there is no typical seat of the beginning in the acinus, and it varies greatly in individual cases. Zenker, Hirschberg, Kretz, Paltauf, among others, consider the centro-acinous location typical, while Eppinger, MacCallum, Hlava, Kimura, Marchand, among others, give the peripheral as the typical location.
"In general, therefore, the necroses seem to have a certain preference for the center of the acini. According to Herxheimer, the location in the acinus is determined by the initial form of the process—i.e., whether it begins with fatty degeneration or with cell destruction; also, by the quantity of the noxious substance. For this reason he warns against considering the location in the acinus a diagnostic differentiation between poisonings and genuine liver atrophy, as many investigators have done.
"In the characteristic picture of my case are to be included also the hemorrhages of varying degree in the pleura, endocardium, leptomeninx, and spleen, which are probably to be attributed to the vascular lesion caused by the poison, like those found in connection with many kinds of poisoning, as phosphorus, chloroform, as well as in connection with acute yellow atrophy of the liver.
"The second case, which concerns a chronic morphinist, also displays serious somatic lesions resulting from the chronic use of morphin and the abscesses caused by the injections. Four facts give evidence of this: 1) the amyloidosis of the spleen, liver, kidneys, and adrenals; 2) the iron pigment found in abundance in the liver, spleen, and testicles, and, less abundantly, in the kidneys and adrenals; 3) the atrophy of the testicles with constriction of the seminal tubules and thickening of their wall; 4) the finding of glycogen granules in the liver and kidneys. As for the amyloidosis, we know that this finding indicates extensive decomposition of albumen. Lubarsch and Czerny see the essential cause of amyloidosis in nuclear decay conditioned by the primary disease, as a result of which certain albuminous bodies come into the circulation. According to investigations made by Leupold, amyloid is formed in connection with extreme cellular decay, comes later into the blood, and is then supposedly thrown out in the organs through the sulphuric acid, which has not been got rid of because the tissues suffering from amyloid degeneration are incapable of acting. The hemosiderosis in this case is also characteristic of the metabolic disturbances going on in the organism. As is well known, iron pigment is deposited in the organs in many cases when there is intense albumen decay, as Lubarsch has shown in connection with nutritive disturbances in infants and hunger oedemas. Besides, Huebschmann, Stefani, and I have seen such findings mostly in connection with chronic nutritive disturbances in children who were dying of atrophy. Intense atrophy of the panniculus adiposus and diminution of the physiological fat in the parenchymatous organs of this case give further support to the aforementioned assumption of a serious metabolic disturbance.
"The finding of glycogen in the nuclei of the hepatic cells as well as of the renal epithelia is interesting. According to Huebschmann, the cause of the appearance of glycogen granules must be sought in the failure of the protoplasm to do its part in relation to the carbohydrate metabolism. In the course of the disease intense degeneration of the liver has developed in places; in my case this manifested itself in inflated nuclei, containing almost no chromatin, as well as in atrophy of the cells. More, therefore, must have been demanded of the other cells, and since the noxious cause continued its activity, they lost their power of storing glycogen. This deficiency was partly compensated for by storage in the nuclei. For in the opinion of many investigators, it seems possible for part of the metabolic processes, normally consummated in the protoplasm, to be accomplished in the nucleus, when the protoplasm fails.
"Hildebrandt's experiments on rats have shown that chronic administration of morphin interrupts the mechanism of metabolism in some form or another. The experiments established the following: chronic morphin doses produce at the beginning of the experiment a retardation of metabolism in the animal organism; in the final stage, however—after about four weeks—there always occurred suddenly a rapid loss of weight: the animals became cachectic and at the same time the metabolism rose quite considerably above normal. Schuebel's experiments on dogs likewise have shown that the addiction of animals to morphin causes increased excretion of phosphoric acid, purin bases, and fat, and these facts justify the assumption that continued incorporation of morphin produces increased decay of nuclein substances as well as of the fat cells, manifested in the decrease of the body weight. There is not the slightest doubt, however, that not only the chronic morphin poisoning, but also the abscesses which the injections had been causing for a long time, and the chronic inflammation of the skin must be held responsible for the metabolic disturbances which were among the findings of this case; the amyloidosis, in particular, must be ascribed chiefly to the latter process, as its occurrence in connection with morphinism is not known in the literature, whereas it has been observed very frequently in connection with long-continued abscess formation in the skin.
"Likewise, the finding of spermato-angitis obliterans which explains the clinical observation of impotence in morphinists, gives clear evidence that mor thin poisoning acts injuriously not only on the brain centers, but also on the sexual organs, as happens also in poisoning with alcohol, iodide of potassium (Adler). in tuberculosis and lues (Kaufmann), and in X-ray irradiation (Herxheimer-Hoffmann). According to Herxheimer and Adler, the poisons produce in the first place vacuolar segmentation, caryolysis of the spermatids and spermatocytes, and finally, the desquamation of the epithelium into the lumen, which results in the thickening of the basal membrane, constriction of the tubules, and proliferation of the connective tissue.
"Thus we see that morphin acts injuriously on many organs, and that this injury manifests itself not only in clinical symptoms but also in pathologic-anatomic alterations. It is difficult to say whether this effect is to be ascribed, as Rost conjectures, to the phenol hydroxyl group in morphin, since the nature of chronic morphinism has not yet been explained. It is also difficult to determine in what way the lesion of the individual organs is produced. The poison might act directly on the cells—and the state of the organs in this case would speak for that—or it might act by way of the nerves—a view vigorously supported by many investigators (Freund, Laubender), especially with regard to the metabolic disturbances in connection with morphin poisoning—or again, through injury of the endocrine organs acid the disturbance of their endocrine activity.
"There has been as yet but little investigation of the pathologic-anatomic alterations in connection with acute morphin poisoning. The findings are mostly macroscopic with but little regard for histology. For this reason we find in manuals of toxicology, of legal medicine, etc., only generally accepted statements, mostly to the effect that there is nothing especially distinctive in the findings for acute morphin poisoning. The best description of the pathological alterations as yet was given by Falck in 1855; according to him, the cerebral meninges and sinuses are extremely plethoric; occasionally there are hemorrhages in the ventricles and here or there in the brain or under the arachnoid membrane; the pulmonary vessels are overfilled with blood; sometimes there are hemorrhages in the pulmonary tissue, intense plethora of the liver, the kidneys, and other glandular organs. Binz extracted the brains of rabbits, treated them with morphin solution under incubation temperature, and found granulation of the nuclei, whereas the nuclei of the preparations kept in salt remained clear. Saratschow, in experiments on dogs, observed in cases of acute morphin poisoning `swelling, loss of branches, and vacuolization of the cells in the central nervous system.' Klestadt described in a case of morphin poisoning, which showed marked sugar excretion, a remarkable deposition of glycogen in the epithelia of the convoluted urinary tubules. According to Jaksch. beyond the hyperemia of the brain, the cerebral meninges, and sinuses, there is nothing characteristic. Hoffman, Troeger, and Dittrich make the same assertion.
"For chronic morphinism also there are for the most part only general statements, which refer only to symptoms of marasmus. According to Jaksch, the anatomical findings are marasmus praecox with atrophic disturbances in the hair and teeth, emaciation, and anemia of the organs. According to Robert, there are observable symptoms of irritation in the intestine, extreme atrophy of the panniculus adiposus and the muscles, cirrhotic alterations of the skin, anemia of all organs, abscesses under the skin, and oedema of the brain. Saratschow found in cases of chronic morphinism in dogs granular degeneration of the cells in the central nervous system. Leuser, on the basis of a case of morphinism which displayed the clinical symptoms of polioencephalitis haemorrhagica inferior, arrived at the assumption that the morphin had caused a lesion of the liver and that this had in turn caused the polioencephalitis.
"The scant statements with regard to the pathologic-anatomic alterations in connection with morphin poisoning are no doubt due to the fact that investigators contented themselves with the macroscopic findings alone, and that for the most part no histological investigation was made. Careful investigation, however, might help to clarify much that is still obscure with regard to the nature of morphinism."
Eleanor M. Scarborough-1926 a"
In view of the claims of certain observers that thyroid feeding increases the susceptibility of animals to acute morphin poisoning, and the alleged resemblances between chronic morphin poisoning and hypothyroidism, the author reports the findings of certain experiments with rats to which were administered morphin, thyroid, and morphin combined with thyroid. The objects of the experiments and the method, are described in what follows:
"Object of Experiments
"To combine thyroid feeding with chronic morphine poisoning in rats, and to compare the susceptibility of these rats to morphine with that of rats under the saine doses of morphine without thyroid feeding, by observing, during life, the influence of morphine, with and without thyroid feeding, on the behavior, body weight and temperature of the rats, and on the condition of the coat. Also, postmortem, to compare the weights of certain organs, and the structure of the thyroid glands.
"Method
"Albino rats at the age of ten to eleven weeks were used for the experiments. The animals were kept on a uniform diet, the appetite being gauged by noting the amount of food left.
"Experiments, five to nine weeks in duration, were carried out on 48 rats (32 males, 16 females), arranged in 12 groups of 4. A group was taken from animals of the same sex, and wherever possible, of the same litter, and consisted of :
"A. A control rat.
"B. A. rat receiving a daily hypodermic injection of morphine sulphate in initial doses of 1 mgm., increasing to 8 to 12 mgm. The initial dose was that found by Macht and Mora to produce a definite effect on behavior, sometimes with after-effects on the day following administration, but always with subsequent complete recovery.
"C. A rat receiving thyroid daily by the mouth. G. W. Carnwick and Company dessicated thyroid was used in doses of 0.025 grams. This dose was approximately 1/5000 of the body weight, a dose which was found by Cameron and Carmichael to diminish the rate of increase of body weight.
"D. A rat receiving both morphine and thyroid in the same doses as B and C. "During the experiments a record was kept of body weights and of rectal temperatures, and the condition of the coat was noted.
"In the fifth to ninth week of the experiments the animals were killed (one rat, under morphine and thyroid, died during the third week of treatment). Postmortem, the thyroid gland was removed for histological examination; the heart, liver, kidneys and suprarenals were removed, washed free from blood, and weighed: the amount of abdominal and subcutaneous fat was noted."
The results in the different groups of animals are given in what follows:
"Effect of drugs on behavior. Of the 12 rats which received thyroid only, 9 were more active than the controls. Of the 12 rats receiving morphine only, 5 were quiet, and 7 were sometimes quiet and sometimes nervous and jerky. In the latter condition the animal would cower in the corner of the box, and make sudden, rather purposeless, darting movements, when attempts were made to handle it. Observations were made about a quarter of an hour after the drug injection. In most cases there was a persistent after effect the next morning, similar to the immediate effect but less marked. The nervous animals became tamer again as the drug effect wore off. The effect of an increase in dose was generally most marked on the day of the change, and decreased slightly on subsequent days, indicating the development of tolerance.
"The incidence of nervous and jerky symptoms was accentuated by combining thyroid with morphine administration. Thus of the 11 rats which received thyroid and morphine, 2 were always nervous and jerky, and 9 were sometimes nervous and jerky and sometimes quiet. (The animal which died in the third week of an experiment is omitted from these and the following results.)
"The incidence of a positive Straub sign (i.e., a peculiar stiffening and curling of the tail, the so-called biological test for morphine) was somewhat greater when morphine was given with thyroid. Thus the sign was sometimes present in 11 of the rats under morphine only, and always present in 1. In 3 of the rats under thyroid and morphine the sign was always present, and sometimes present in 8.
"Condition of coat. The coats of the control rats were sleek and thick. Under thyroid the coats of 4 rats remained normal, while 8 became rougher (i.e., less sleek). The coats of all the rats under morphine tended to become rough and thin, but this was only well-marked in 2 animals receiving morphine alone, whereas, when thyroid was given with morphine, the coats of 10 rats showed well-marked changes, with loose hair and bald patches in some cases.
"The appetite, as compared with the controls, was very slightly impaired in the thyroid fed rats, although these animals appeared to be the most eager for food. The impairment was somewhat more marked in the case of animals receiving morphine, but the amount of food taken by most of the animals seemed ample, even when they were losing weight.
"The amount of fat. Large deposits of abdominal and subcutaneous fat were found in 11 control rats, 4 thyroid fed rats and 1 rat under morphine only. This amount was reduced in 1 control, in 8 thyroid fed rats (3 very marked) and in 11 rats under morphine only (3 very marked). Emaciation was most pronounced, however, in the rats under thyroid and morphine in all of which the amount of fat was reduced (10 very markedly).
"Changes in body weight. The modification of growth produced by drug administration is indicated by the following average weights throughout the series:
| Controls | Morphine | Thyroid |
Thyroid and morphine |
|
| grams | grams | grams | grams | |
| At commencement | 109 | 107 | 111 | 116 |
| At end | 163 | 137 | 135 | 126 |
| Difference | +54 | +30 | +24 | +10 |
"The rate of increase in body weight was diminished in all the treated animals most markedly in the case of the rats under thyroid and morphine. An actual loss of weight occurred in 3 thyroid fed rats, and in 5 rats under thyroid and morphine, but never in an animal under morphine only.
... During the five weeks recorded the morphine treated animals in each group were receiving the same doses.
"Changes in temperature. The modifications in temperature following drug administration are indicated by the following figures, which give the average temperature throughout in the fourth week of each experiment.
Controls 98.8
Morphine 100.1
Thyroid 100.3
Thyroid and morphine 102.5
"The temperature was higher than normal in all the treated animals (with the exception of 2 rats under morphine, and 1 under thyroid). The rise in temperature was more marked in every case under the combined drug treatment.
"Weights of organs removed post-mortem. The following table gives the average weights of the heart, liver, kidneys and suprarenals throughout the 12 groups, compared without reference to body weight:
| Heart | Liver | Kidneys | Suprarenals | |
| Control | 0.59 | 7.41 | 1.48 | 0.0307 |
| Morphine | 0.54 | 6.64 | 1.31 | 0.0346 |
| Thyroid |
0.64 | 8.48 | 1.70 | 0.04 |
| Thyroid and morphine | 0.62 | 6.93 | 1.65 | 0.043 |
"The weights of the suprarenals vary widely even in the control animals. In ~+
the case of the other organs the average weight in the morphine rats is low. ~I
in the thyroid rats high, and in the thyroid and morphine rats intermediate, being below the control average in the case of the liver only.
"Changes in the thyroid gland. Upon macroscopic examination, post-mortem, the glands of those rats which had received thyroid, with or without morphine, appeared smaller and paler pink.
"Microscopic examination of sections, stained with haematoxylin and Biebriech scarlet, showed a condition of diminished activity in the glands of those rats which had received thyroid, with or without morphine, as compared with the glands of control or morphine rats.
"The sections thus formed two groups: (a) the normally active glands from control and morphine rats, and (b) the less active glands from rats which had received thyroid, or thyroid and morphine. The difference in activity was determined with reference to the size and number of vesicles, the type of epithelium, the occurrence of vacuoles in the colloid, etc.
"Summary
"1. Chronic morphine poisoning, when associated with thyroid feeding, is not accompanied by any accentuation of the depressant action of morphine on the central nervous system.
"2. The metabolic effects, produced by combined chronic morphine poisoning and thyroid feeding, are more marked than those produced by either drug alone, and resemble the effects of pronounced hyperthyroidism.
"3. The weights of organs concerned in metabolism are low in chronic morphine poisoning. The combination of chronic morphine poisoning with thyroid feeding tends to check the hypertrophy of these organs which otherwise accompanies thyroid feeding.
"4. Chronic morphine poisoning is not associated with any change in the structure of the thyroid gland."
Eugène Gelma and Max Aron-1926.°5
The authors state their objectives to be the determination of the influence of substances capable of selective absorption by the nervous system exercised on the evolution of anura with the idea of obtaining indications of the stages of the functional development of the neuraxis. The account of their experiments follows:
"Malonyl urea employed in the form of somniferin in watery solution (20 to 25 drops of somniferin in 100 cc. of water) did not affect in any way the first evolutionary stages of the fecundated eggs of rana temporaria placed in such solution. Segmentation blastolysis and gastrulation proceeded normally. But when the embryos attained a length of 6mm. to 61/2 mm. the development stopped. If the embryos are quickly enough placed in plain water they are able to continue their evolution. If not, they die rapidly without passing the stage which we have just mentioned.
"This fact appears to signify that the acquisition, by the elements of the embryonic nervous system of anura, of their definite physicochemical characteristics occurs at the period marked by the narcosis of the tadpoles. Further, it is at the stage where histologic examination of the neural tube shows the first signs of the differentiation of the neuron. Spontaneous movements appear at the saine stage. All evidence indicates that the physicochemical evolution of the nerve cells, which makes them sensitive to the action of somniferin, is dependent on their morphologic and functional evolution.
"We wondered if morphin, by reason of the affinity for the nervous system which is attributed to it at least in the higher vertebrates, would show in anura effects comparable to those of malonyl urea. This is not the case. In weak solutions of morphin (1/z cgr. per 100 cc. of water) development remains normal for the great majority of experimental embryos, also during the first stages of ontogenesis, until after the appearance of movements. In more concentrated solutions (1 to 10 cgr. to 100 cc. of water) death of the very young embryos takes place more or less quickly. Tadpoles further advanced in evolution sometimes suffer the same fate, but their resistance seems to increase with age. Variations, however, are noted, for the same concentration of morphin in the length of survival of different lots of embryos. However, these findings warrant the hypothesis that morphin acts as a general poison on the embryos of anura without any specific effect upon nerve tissue.
"It will be remembered that Overton, with a different object from ours, studied the influence of morphin on tadpoles, making no note, however, of the stages which preceded the differentiation of neurons. He concluded, as have we, that morphin penetrates these animals slowly and that they resist its action even in very strong concentrations. The same author, on the other hand, administered strychnin to embryos of all ages and noted results which agreed in some measure with those which somniferin gave us; harmless in the first stages of ontogenesis, strychnin did not give evidence of its action until the embryos had reached a length of about 9 mm. It then caused paralysis comparable, Overton says, to that caused by curare. It seems well to point out that the manifestations of the elective influence of strychnin show themselves definitely later than do those of malonyl urea and we are thus shown through pharmacological methods a means of obtaining definite indications on the development of the functional stages in anura of different elements of the neuromuscular system."
S. Nishigishi-1926.6°
After a study of the basal metabolism of fourteen morphinists, five
opium addicts, and two pantoponscopolaminists, the author arrives at the following conclusions:
"1. The basal metabolism of normal Japanese and Chinese varies about ten per cent from the average value of Aub and DuBois.
"2. The basal metabolism of morphinists, opium addicts, and pantoponscopolaminists generally shows a normal value during the period of addiction.
"3. This basal metabolism is not influenced by either the length of time of addiction or the amount of the customary dose, but depends on the condition of the addict in regard to nutrition, that is, it behaves as in normal subjects.
"4. The basal metabolism of these morbid individuals rises considerably during the period of abstinence.
"5. The condition of nutrition is influenced in these morbid individuals by dietetic conditions and mode of life and increase of metabolism during the period of abstinence, but not by the length of the time of addiction and the amount of the customary dose.
"6. Increase of basal metabolism during the period of abstinence directs suspicion, besides the disturbance of the smooth muscles, for instance those of the digestive canal, to the question of functional anomaly in the organs of internal secretion."
In the same volume of the Journal of Oriental Medicine, Nishigishi reports in a second paper on certain studies of the blood chemistry of morphinists, his object being a further study of the pathogenesis of the condition. Six cases were included, one Chinese and five Koreans. His conclusions follow:
"1. During the period of abstinence the residual nitrogen and urea nitrogen in the blood was normal in amount, the carbonic acid in the blood plasma slightly diminished, and the acetone bodies in the blood greatly increased but within normal limits: the lactic acid of the blood was in excess.
"2. The increase of lactic acid in the blood during the abstinence period is certainly due to the defective combustion of carbohydrates originating in a systemic deficiency of oxygen from the sudden increase of metabolism caused by abstinence.
"3. These anomalies of carbohydrate metabolism inevitably lead to insufficient oxidation of fat and consequent increase of acetone bodies.
"4. The increase of lactic acid and of acetone bodies is manifestly the cause of the diminution of carbonic acid in the blood plasma.
"5. A review of the experimental studies of animals of various investigators regarding functional increase of the thyroid gland and of the facts established by the writer respecting increased metabolism during the period of abstinence renders it highly probable that the increase of lactic acid and acetone bodies during the period of abstinence is referable to an enormous increase in thyroid function.
"6. During the period of addiction the carbonic acid increases slightly in comparison with the period of abstinence, and the lactic acid and acetone bodies fall to their normal amount, while the quantities of residual nitrogen and urea nitrogen remain normal.
"7. The amount of serum albumen remains unchanged during both periods."
Ernst Joel and Fritz Frankel-1926 67
In this, the second of a series of three articles dealing with the pathology of addiction, the authors seek to distinguish between habit and habituation from both the somatic and psychic points of view. In the preceding article they discussed the mechanism of acquired immunity to poisons and emphasized the fact that without exception habituation to poison implies not complete but only partial increase of tolerance, which explains why the process of habituation, which in itself seems purposeful, is nevertheless something morbid bringing a disharmony to the organism; while some organs are less harmfully affected, others are affected to a great degree, often in an increasing degree.
If the poisons are of the euphoric or narcotic order, e.g., those which supply a decided increase of pleasure acting principally on the central nervous system, it is difficult to draw conclusions as to the reaction. The authors point out that in the case of cocain, habituation in the sense of a gradually acquired tolerance does not exist. This is substantiated by clinical observations with regard to the pharmacological habituation to cocain and also by animal experimentation. For this reason cocainism differs essentially from morphinism. In both cases there is an intensive desire for the drug, a tenacious clinging to the poison, danger of relapse, a habit deeply rooted in the personality. In contrast to morphin there is lacking in the chronic use of cocain an acquired tolerance of the organism which requires increasing doses; equal doses always produce the same physical effects; there is no physical habituation and hence no true weaning, i.e., a sensitization of the organism after an interval in the administration, physical hunger for the poison, and finally real abstinence symptoms when the body reacts with symptoms which are the negative of the effect of the drug.
Whatever new symptoms appear in the picture of cocain poisoning during abstinence can be easily explained as a consequence of the abuse and very often as a return of the status quo ante.
The authors continue as follows:
"Numerous new experiments with cocain users, which we have since assembled, enable us to confirm completely our earlier views. Moreover, we have not found in the literature any facts which would gainsay our conception. On the other hand, we have been enabled to grasp even more clearly the significance of a factor to which we did not before call special attention—namely, that when we consider the manner in which poisons which beget a sense of well-being produce their effect, we must take into account not only passionate habits, but also habituation, and particularly, psychic habituation, i.e., increased psychic tolerance.
"Agreement with regard to these matters is made more difficult by language usage which applies the same word synonymously to two concepts. Just as the word `Arbeit' (work) expresses the activity as well as the product of this activity of habituating (disregarding the fact that at times it is altogether efforts as well as the condition which these systematic efforts beget as result, so habituation denotes, on the one hand, the union between a single stimulus and its single effect and, on the other hand, the condition thus brought about of diminished response to the single stimulus. For example, a dog becomes accustomed to morphin (activity of habituation) and as a consequence of this single act of habituation there appears the condition of habituation: he is habituated. In the psychic domain there now appears the complicating factor that the activity, of habituating (disregarding the fact that at times it is altogether ineffective) may have as its consequence not only habituation but also habit. We may define habit as a condition in which stimuli which were originally single and occasional experiences, become a necessity of life. That they are really necessities is not always self-evident; the fact, however, may be quite clearly established in negative fashion through the 'disclination to give them up. By way of illustration, the necessary character of going a certain way can become apparent only on the occasion of a disturbance which comes from the outside and which is in itself quite unimportant. The essential difference between habituation and habit lies in the fact that the concept of habituation implies diminution of the effect of initially effective stimuli and the necessity of increasing the stimulus, whereas habit does not raise the threshold of the stimulus, but may even be compatible with the efficacy of weaker stimuli. The two concepts have so little interconnection, that passionate habit may occur without habituation, and on the other hand, habituation need not presuppose a habit. Furthermore, it is more likely that habituation may lead to the giving up of habits than to the fixing or maintaining of them.
"Consequently, we should not do as Heilbronner does—i.e., we should not apply the word habituation to the fact that weaker stimuli become effective, but we should rather regard this as a typical effect of habit, `a driving in' (Einfahren), a consequence of practice.
"It is precisely in the cravings for poison that we find a justification for a sharp distinction between somatic and psychic habituation.
"The individual who craves them longs for some sort of sensation: euphoria, comfort, reverie, cheering up, excitement, excess, psychic adventure, mysterious happenings. We know that the poison gives him everything he desires, and even much more. The stage of euphoria may be followed—as in the case of cocain and hashish—by a stage of delirium with persecutory and terrifying hallucinations, so that one is constantly amazed at the willingness of the toxicomaniac to accept the risk of the latter stage into the bargain. We find in such an enjoyment of intoxicants an association of pleasurable and painful experiences, occurring together, in succession, and intermingled. There exists, therefore, the possibility that in the course of time the joy will not be sufficiently exhilarating, while the horrors grow less and less terrifying. And such is actually the case. We have known cocainists who would not take the drug after the first persecutory hallucinations. When the recollection paled a little, they took to the drug again; soon the visions no longer seemed so `awful'; in fact, the thing began to assume a new attraction for them, just as in the case of other things, too, something which at first causes disgust may, after the disgust has vanished, become attractive, until finally a third stage is reached, in which the attraction likewise palls. If a cocainist, after being at first cautious in his dosing, grows bolder—if, in fact, he is now on the scent for every possible experience, painful or pleasurable, we should speak not of habituation merely, but of psychic habituation. The hallucinations have not ceased, but the cocainist has become dulled against their terrors.
"Manifestly, then, increased dosage arising from psychic habituation without preceding somatic habituation is quite understandable. What is termed habituation in the pharmacological sense is somatic habituation.
"We can now distinguish between somatic and psychic habituation to a drug. And that allows for the possibility that psychic habituation may arise from general psychological conditions.
"The delimitation of somatic from psychic increase in tolerance for a drug can be demonstrated with especial clearness by comparing the craving for morphin with the craving for cocain. In the case of morphin it can be shown how a certain psychic need at the beginning can be so satisfied by the administration of the drug that equilibrium, satisfaction, contentment result. If the need remains the same and the dose also, the quantity of the available drug becomes less effective by reason of the somatic habituation (destruction, increased excretion, decreasing sensitivity). And so, when the need remains the same, the quantity administred may have to be increased to make up for the quota claimed by habituation and thereby to restore the balance between demand and supply.
"In cocain a different situation exists. Here, too, there is an initial need which is satisfied by an adequate dose. The body does nothing to diminish the effectiveness of the dose. It may even become more sensitive. If despite that fact, a dulling against initially effective doses does occur, the cause is not in a change of the efficacy of the supply but in a change of the demands, and furthermore—and this alone is the criterion for a true condition of habituation—this change is due not to external influences but to the misuse of the drug itself.
"The somatic or pharmacological habituation in the narrower sense is, therefore, an habituation associated with a need which remains the same. Psychic habituation is habituation through an increasing need.
"From the above relations it becomes evident, likewise, why almost all drug users no longer find satisfaction, after a time, in a single drug. If a morphinist takes to cocain, the fact can be easily understood from the condition of somatic habituation—i.e., he would like to get to something positive over and above the mere abolition of abstinence symptoms. But we have seen often enough that cocainists, despite the euphoria and mental excitement, took to other euphoria-supplying drugs, not because they dreaded the hallucination, but because the entire intoxication-experience and with it the hallucination no longer made any impression, inasmuch as they had become dulled to it.
"This dulling may be as much a symptom of somatic as of psychic habituation. We should call it somatic dulling if a drug—e.g., mescalin—could not, after a time, stir the mind to visions. Should such illusions in another case be associated with psychic effects of the drug, anxiety-effects, for example, and should these grow weaker as the craving develops so that they no longer cause hallucinations, then we should assume psychic habituation.
"Psychic and somatic habituation may, of course, exist alongside each other.
"The compulsive demand for more, the hunger for the drug, has at times been regarded as the sign of a somatic, cellular habituation. But here, too, we must refrain from the assumption of somatic processes so long as an explanation is possible along psychic lines.
"For example, when a doctor finds a therapeutic substance less effective, he increases the dose. A laxative, for example, has to be taken in greater quantity to induce evacuation. The efficacy or lack of efficacy of this remedy, whose point of attack is extracerebral, is recognized by doctor and patient in about the same way, i.e., by its external result alone. The patient himself is a spectator, so to say, except that he is more closely concerned. But when the drug affects the brain, as the intoxicants do, the patient recognizes the effect not indirectly—by a mechanical, peripheral process, so to say—but quite directly. His entire person becomes identified with the effect or lack of effect. The participation of the whole personality explains why 'increase in tolerance is followed by a direct desire for more, by an increase of the dose. That which, in the case of peripherally-acting drugs, leads to resolution and a definite course of action, becomes in this case, where the personality is at the center of the action, a hunger, a drive, a craving.
"Again, we may explain in what sense the concepts which we have been discussing—somatic habituation, psychic habituation, and habit—are intended to be taken by following the origin and course of a craving for a drug. A morphinist will be strongly attached to his drug in the first period of his abuse (misuse) of it—i.e., so long as he has immediate profit from it. But this attachment is much less an habituation than a habit, since at this time a euphoric effect is still possible without an increase in the dose. This habit will continue to become more passionate ; it will lead to an extension of the field of action, in which the slightest impulse provokes the act of intoxication, and the ardent desire for obtaining toxic enjoyment generates a readiness for activity or, as Bleuler calls it, an `opportune apparatus' (Gelegenheitsapparat). Thus, through the might of his habit, the morphinist gradually loses all power of choice as to occasion, and at the same time he becomes more closely attached to his particular drug because as a consequence of the increase of the dose habituation sets in. And with that the original habit loses its significance as regards the craving; by now the evermounting consumption springs from the increasing tolerance and the abstinence-symptoms--the craving for the poison must now be explained as purely physical. And through that the psychic sphere becomes more and more impoverished. If there still exist active tendencies there, then the patient longs for a positive gain, e.g., through cocain, over and above the mere removal of abstinence symptoms. This new poison, to be sure, affords him no somatic tolerance; but, with the return of habit a psychic habituation may perhaps develop, as a result of which the intoxication-experience grows weaker and weaker, existence becomes unendurable, and the drug user is driven to suicide."
Ernst Joel and Alice Ettinger-1926.°8
In the third article on the pathology of addiction the authors realized that the theories as to the nature of habit, habituation, tolerance, etc., propounded in the preceding article, needed further corroboration, and selected the following as the chief points to be demonstrated:—the dissociation of habituation—not all parts of the body are dulled against the effects of chronically administered poison; many remain positive, e.g., myosis even in the advanced addict to morphin, bradycardia in the addict highly habituated to morphin. This permanence of sensitivity may induce sensitivity, though there may be a partial reversal of the effect. In a morphinist the poison is no longer a sedative, but a stimulant. The excitement caused by morphin in the non-addict has become the chief effect in the addict. The question is, to what extent does this excitement attack extra-psychic points; how far are the withdrawal symptoms the expression of psychic discomfort; how far are they manifestations of physical need; is the fact that the withdrawal is accomplished more slowly than the habituation due to the conditioning of the habituation by euphoria while the withdrawal is checked by dysphoria. Finally, the substitution of other soporific drugs for morphin is difficult in the case of an addict, as has been shown in the case of somnif en. Is there an increased tolerance for these remedies, or is morphin addiction specific and the abstinence symptoms so specific that even large doses of other drugs. affect them but slightly?
To demonstrate these matters the authors employed tame white rats weighing about 100 g. These animals were on a mixed diet. The drugs employed were morphin, dicodid and dilaudid, injected under the skin of the back. Approximately 300 rats were used. They described, first, reactions of normal rats to certain stimuli—vocal reaction on pinching, the defense reaction, the flight reaction, the posture reaction, the jump reaction, forced movements, convulsions, the corneal reflex, and total behavior. They then studied these same reactions in acute morphin poisoning with medium doses-5 to 10 mg. —and described the resulting narcotic condition which lasted from two to three days. First the vocal reaction vanishes, then the defense reaction, while the flight reaction is extinguished only by a high degree of narcosis. Exophthalmus develops, the corneal reflex generally becoming negative somewhat later. There is motor deficiency, general repression. They assume a semi-lateral or a flat position not that of normal sleep. The gait becomes uncoordinated, wiry-legged, slinking, mincing.
Then follows the stage of excitation with automatic movements, the narcosis and excitation overlapping. Gradually the corneal and defense reactions reappear and the stupor disappears. The excitation manifests itself chiefly in a noisy, heedless, and apparently forced gnawing of the sides of the box while food is avoided. Animals even gnaw at their own paws and other animals until bleeding occurs. This is followed by a particularly energetic defense against painful irritations. This stage lasts from two to three hours and is followed by a third stage, when the animal shows all the signs of ordinary sleep. Twenty-four hours after the beginning of the experiment the animals are tired but react normally.
In the case of large doses-25 to 50 mg.,—the first period lasts longer and may result in convulsions. Doses above 60 mg. are generally fatal. With small doses-1 to 5 mg.—narcosis predominates.
In the following the reactions observed in rats habituated to morphin and morphin derivatives are given in full.
"The fact that in an acute test fatal doses do not have this effect on the habituated organism is regarded as the clearest proof that habituation has been attained. Consequently, the aim of the experiment would have to be to stupefy animals against fatal doses. But the fact that habituation has been accomplished may be recognized not only by the fact that previously unendurable doses have become endurable, but just as much by the fact that previously effective doses have become ineffective. It is just this ineffectiveness that causes the patient to use a larger quantity. The mode of experimental procedure would, therefore, have to be: administration of the drug until, as compared with the initial effect, the drug has lost or diminished its power. The advantage of the first method lies in the distinctness of the issue of the experiment. Nevertheless, the second way seems to have some advantages, too. First, so far as concerns the sharpness of the decision, the disappearance of characteristic symptoms is just as conspicuous as, and at the same time more capable of gradation than, the failure to die. Then, we avoid here two possibilities of error, which are inherent in the first-named method. First, in all experiments for the purpose of habituation, part of the animals die before they have attained the desired immunity. If now the survivors exhibit a slighter degree of mortality or none at all as compared with the controls the result may be due to the fact that during the habituation process there had occurred a natural selection of animals which were originally especially resistant to the drug. This is all the more likely as the individual animals vary from the start in their sensitiveness to morphin. Second, in the course of the experiment, particularly when the higher doses are reached, the animals become sickly, thin, and cachectic. . Furthermore, this general debilitation brings factors into the picture of habituation which are hard to appraise. We, therefore, prefer to habituate the animals slowly and only up to medium doses, or we do not attempt any increase in the dose at all, contenting ourselves with determining whether and just how an equal dose causes the original picture of the poisoning to change from day to day.
"Without holding rigidly to a schedule, we generally proceeded in such manner that within 10-12 days we had increased the dose of morphin from 5 mg. to 30 mg. In other experimental series, e.g., with dicodid, we treated individual series with a daily dose of 5 mg. for 2-3 weeks. The difference in the reaction of the non-addicted and the addicted animal is extraordinary. Compare the table on the next page.
"While, therefore, we find in the non-addicted animal disappearance of the voice and defense reactions, lasting for hours, and narcotic symptoms as displayed in the suspension position, cataleptic postures, and the like, the addicted animal begins but a few minutes after the injection to exhibit tic movements, forced gnawing, and other signs of motor unrest, which appear in the non-addicted animal only after a number of hours. It is also at once evident that the total duration of the poisoning is shorter after addiction, and that the addicted animal exhibits again at the end of the experiment his initial behavior, whereas the non-addicted animal is after eight hours still in the second stage. The narcotic stage, therefore, disappears, and there remains the excitation stage. The symptoms of excitation, which originally followed the stupor symptoms as second phase, have been pushed forward to the beginning. In this alteration of the organism there has noticeably come to pass a distinct, but not a complete, dulling against the analgesic effect of morphin. Exophthalmus generally no longer appears.
"When morphin, dicodid, or the like, is administered daily in the same quantity, the habituation process may be directly traced as a curve, as the excitation symptoms set in a little sooner every day, until finally they appear after a few minutes or almost immediately after the injection. Apart from this, they have become, in the course of the chronic poisoning, more violent, even though the dose remains the same. Where they did not occur at all in the non-addicted animal or where there was only a suggestion of them, they now appear in extremely violent form, or can be induced by means of liminal (as to effect) for
the normal animal. We, therefore, have here not alone the case of a dissociated habituation, but in addition to this, the case of an increase in the symptoms of resistance to the drug. We append tabular form.
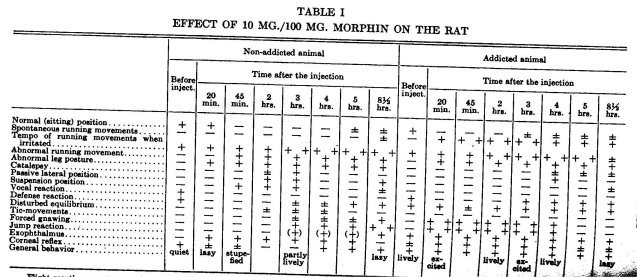
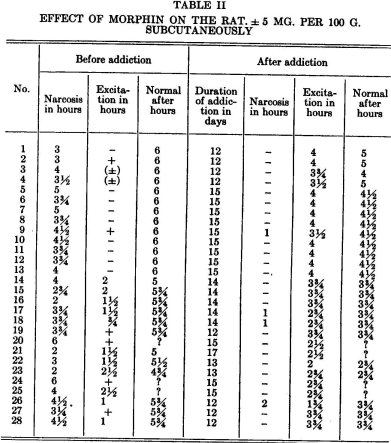
"In view of these conditions, the question arises as to how habituated animals behave with reference to normally fatal doses of morphin. In the ease of moderately habituated animals, in accord with what we have just related, we generally encounter a situation which at first surprises us—namely, that they succumb, amid convulsions, sooner than the controls. Along with the excitation, which is unretarded by a preliminary narcotic stage, there is induced a greater readiness to go into convulsions. But when the animals have reached a relatively high degree or long period of addiction, they finally also acquire resistance to fatal doses. It is noteworthy in this connection that the motor unrest, the tic movements, and the like, cannot be eliminated, but that in such cases rather, they are occasionally to be seen even 24 hours after the injection. Absolute freedom from symptoms is never attained, not even after a very lengthy preliminary treatment.
The Specificity of Habituation
"The results of the habituation experiments paved the way for the investigation of the specificity of morphin habituation in rats. The resistance to the narcotic action led us to ask whether other narcotics or hypnotics would still be effective; the susceptibility, the acquired sensitiveness to the stimulating effect might perhaps be referable also to other stimulants. The third thing to be investigated was whether the morphin-habituated animal behaved exactly the same or quite differently with reference to chemically related substances of the morphin group—first the effect of the drugs to be investigated was determined through preliminary experiments.
a. Hypnotics
"Chloral hydrate. 15 mg./100 g. rat causes a narcotic condition, in which a passive dorsal position is not corrected.
"It appeared that five morphin-habituated animals reacted in the same way as normal animals. They fell asleep just as quickly; the soundness of their sleep (measured by acoustic or tactile rousing stimuli) and the duration were about the same as in the case of the controls. The following is an example:
Normal animal
White rat, weight 130 g., 15 mg./100 g. Chloral hydrate
11:03 Injection
11:15 Passive dorsal position +. Respiration jerky. In response to a slight irritation, correction and normal (sitting) position. Vocal reaction +. Motions hesitant.
11:22 Remains for a long time in passive dorsal position.
11:45 Passive lateral position +. Pinching the tail brings vocal reaction and upright position.
12:25 When irritated, wakes up, runs about.
1:15 Normal (sitting) position, slow motions. Passive dorsal position —. Vocal reaction + . Defense posture + .
Morphinized animal
White rat, weight 145 g., 15 mg./100 g. Chloral hydrate
11:02 Injection
11:12 Spontaneous lateral position. When irritated, moves with utmost difficulty and much vacillation.
11:22 Spontaneous lateral position.
11:39 Completely atonic. Passive lateral position +. Vocal reaction —. 12:28 When irritated, wakes up. Runs with much staggering.
1:15 Lively defense. Passive dorsal position —. Vocal reaction +.
"Amylene hydrate. Four experiments with amylene hydrate gave similar results. In the case of this drug, too, the dose chosen was such that there was but small claim for any original resistance to sleep. With 50 mg./100 g. of amylene hydrate, the main symptoms of narcosis are over in normal animals in about 3 hours.
"The result was that the morphinized anima's passed into a narcotic stage just as the normal animals, but the severity of the disturbances as well as their duration were rather greater in the morphinized animals.
"Luminal. For lumina! sodium we used a dose of 12 mg./100 g. The effect begins to show itself after 20 minutes; the maximum soundness of sleep is over after about 3-4 hours, but even after 6 hours disturbances of equilibrium are still discernible.
"Four morphinized animals were compared with three controls. Both groups fell asleep at the same time, suffered the same disturbances of coordination; the soundness of the sleep was about the same in all animals. Six hours after the injection the poisoning was practically over. Here, too, the controls now displayed lighter disturbances of equilibrium and a greater inclination for running than the morphinized animais. It follows, therefore, that the latter, too, are at the very least just as ready for narcosis as the controls.
"The results of our investigations with three differently constituted hypnotics showed that the morphin-habituated organism is, on the whole, not at all resistant to central narcosis, but that it has lost the narcotic reaction to the drug to which it is habituated.
b. Stimulants
"For the following experiments the respective drugs were used in doses not large enough to induce convulsions, because in the morphinized rats there might be a greater readiness for excitation. The drugs employed differed as to point of attack and species.
"Picrotoxin, administered in a dose of 02 mg./100 g., produced no convulsions in the normal animal. The chief symptom during the first hour is a heavily pulsating tremor, which, if it is not visible without further ceremony, manifests itself when the animals are forced to balance themselves on the edge of a box.
"Three morphinized rats, after a dose of 02 mg. of picrotoxin, showed exactly the same behavior as the control animals.
"Strychnin, 0.1 mg./100 g. causes in the normal rat a distinct augmentation of the reflexes. Excitability in response to sound or shock is increased. Since the results were at first not quite uniform, 15 animals, habituated to morphin, dicodid, or dilaudid, were experimented upon altogether. Result: here too, there was agreement in the behavior of the habituated and the unhabituated animals; in no case was there a sensitization of the morphinized rats to the effects of strychnin.
"Another stimulant investigated was cocain. To a dose of 5-10 mg./100 g. the normal animal reacts after about 30-45 minutes with general restlessness, sexual excitation symptoms, pugnacity lasting for hours—in short, with an excitation state of quite a different sort from that produced by morphin. Observation of six animals habituated to morphin and seven to dicodid proved that they, too, exhibited the typical cocain excitation; the morphin excitation, therefore, can be produced only by this alkaloid itself. There were no differences as regards the commencement and duration of the effect.
c. Morphin derivatives
"If then, the experiments made so far indicate specificity of morphin habituation, the degree of specificity had now to be determined more precisely. If the degree was very high, one might expect that preliminary treatment with morphin produced dulling against morphin alone; therefore the morphin derivatives which were to be tested presented something new and hence, efficacious. The drugs used were eukodal, dilaudid, dicodid, and codein.
"Eukodal. If we disregard questions as to dose, we find in regard to eukodal an almost complete agreement with the diphasic picture of morphin poisoning. The dose was 2 mg./100 g. The average reaction to the dose is presented in tabular form.
TABLE III BEHAVIOR OF FIVE RATS UNDER THE FIRST DOSE OF 2 MG. EUKODAL /100 G.
| No | weight of rat in g. |
Duration of Narcosis in hours |
Duration of Excitation in hours |
Remarks |
| 1 | 90 | 3¼ | ? | Not observed to the end |
| 2 | 95 | 3 | + | |
| 3 | 120 | 3 | - | |
| 4 | 90 | 4 | - | |
| 5 | 80 | 2 | 2 |
"For the five morphinized animals 2 mg. of eukodal had lost their narcotizing effect. The animals presented only an excitation stage of about 2-4 hours, which was quite similar to the picture of morphin excitation in a morphin-habituated animal. A difference was displayed in the fact that in the case of a dose of eukodal which was equivalent to a dose of morphin with regard to the duration of the narcosis, the animals, in antithesis to their behavior under morphin, gave no vocal reaction and repeatedly assumed a spontaneous lateral position.
"Dilaudid (Dihydromorphinon). The picture of acute poisoning with dilaudid was likewise almost identical with that presented by morphin poisoning. As a rule, 2 mg./100 g. have a 2-4 hour narcotic effect. Generally, even with this dose, there followed a stage of excitation. In the morphinized animals (six experiments) in antithesis to the control animals, this dose did not produce narcosis, but did produce a condition of excitation for about four hours with forced motions and attacks of gnawing. During the excitation three animals exhibited in the intervals a certain stupor, which did not occur under morphin.
"Dicodid (Hydrocodeinon). To a dose of 5-10 mg./100 g. dicodid, which in its acute effect corresponds to about 2 mg. dilaudid, five morphinized rats reacted with excitation only, and in such manner that their condition was exactly similar to that after morphin.
"The similarity of the effect of dicodid and morphin on morphin-habituated animals was so complete that even with the most careful observation it would have been impossible to decide what the animals had received.
"Tests with codein passed off in the same way. 15 mg /100 g. usually results in a distinct, but frequently also only in an abortive development of narcosis for about 11/2 hours. This is again followed by a stage of excitation analogous to that after morphin. The morphinized animals (four tests) displayed in response to this dose no symptoms of narcosis whatsoever, but only excitation symptoms, as after morphin, even though briefer and weaker.
"Tests with. substances chemically related to morphin show, therefore, that these drugs are interchangeable with morphin. The reaction of the habituated rat discloses no differences, or no essential ones; the rat is fortified or sensitized in the manner characterized above also against eukodal, codein, dilaudid, and dicodid. In the case of dilaudid and dicodid, for which according to our conclusions habituation is possible within exactly the same limits as for morphin, we made the further investigation as to whether these relations could be reversed. As a matter of fact, rats habituated to dicodid and dilaudid react to morphin as if the preliminary treatment had been made with morphin.
"The results of the tests as to the specificity of habituation are summarized in the following table.
TABLE IV
| No. | Drug | Test dose per 100 g. in mg. | Normal animal | Morphinized animal |
| 1 | Chloral hydrate | 15 | Narcosis (2-3 hrs.) |
Narcosis (2-3 hrs.) |
| 2 | Amylene hydrate | 50 | " (3 hrs.) | " (3 hrs.) |
| 3 | Luminal | 12 | " (4 hrs.) | " (4 hrs.) |
| 4 | Picrotoxin | 0.2 | Tremor (1 hr.) | Tremor (1 hr.) |
| 5 | Strychnin | 0.1 | Augmented reflex- excitability | Augmented reflex- excitability |
| 6 | Cocain | 5-10 | Pugnacity, states of excitation, restlessness | Pugnacity, states of excitation, restlessness |
| 7 | Eukodal | 2 |
Narcosis (2-4 hrs.) Excitation (2 hrs.) |
No narcosis Excitation (2-3 hrs.) |
| 8 | Dilaudid | 2 |
Narcosis (2½ hr.) Excitation |
No narcosis Excitation (3-4 hrs.) |
| 9 | Dicodid |
5 |
Narcosis (1½ hr.) Excitation (2 hrs.) |
No narcosis Excitation (2-3 hrs.) |
| 10 | Codein | 15 |
Narcosis (1½-2 hrs.) Excitation |
No narcosis Excitation (2-3 hrs.) |
Withdrawal and Withdrawal Symptoms
"If habituation means increasing dulling through continuous use • of a drug, then withdrawal means the re-sensitizing of an organism to the original effect of the drug. We can, therefore, test how long it takes, after the stopping of the regular administration of the drug, for the animal to react to the test dose in exactly the same manner as the first time. The results showed that the withdrawal took a longer time than the habituation. The alteration, which the organism has suffered through the drug, endures for a surprisingly long time. Even weeks after the withholding of morphin, there was no narcosis after renewed administration, but only excitation, though in weakened form. Table V shows this quite clearly.
TABLE V 12 MG. DICODID. REACTION OF A DICODID-HABITUATED RAT, WHICH HAS NOT HAD ANY FOR 3 WEEKS, AND OF A NORMAL RAT
|
After the Injection |
Habituated | but | now | drug | free | animal | Normal | animal | |||
| Hrs. | Min. | DR | VR |
Motor unrest |
SP | CR | DR | VR |
Motor unrest |
SP | CR |
| 5 | + | - | - | _ | + | + | + | - | + | + | |
| 20 | - | - | + | + | - | _ | - | - | + | - | |
| 1 | 45 | + | - | + | + | + | _ | - | - | + | - |
| 2 | 20 | + | - | + + | - | + | _ | - | - | - | + |
| 3 | 00 | + | + | + + | - | + | _ | - | + | - | + |
| 3 | 45 | + | + | + + | - | + | _ | - | + | + | + |
DR—Defense reaction. VR—vocal reaction. SP—Suspension position. CR—Corneal reflex.
"Even after 30 days of abstinence, animals formerly habituated differ distinctly from those who have had no previous treatment. This fact is all the more remarkable when one considers the fact that the habituation process in rats is recognizable after 3-4 days.
"By abstinence symptoms (withdrawal symptoms) we mean such symptoms as distinguish the chronically drugged animal from the normal one, when it. is no longer in the stage of acute poisoning. The behavior of the morphinized animals is now altogether different from that of the normal ones. They are much more lively than the normal animals, often even highly excited and wild, are difficult to get hold of, and are generally irritable; the last is recognizable in, e.g., a greater spontaneous inclination to jump, augmented jump reflex, a more furious defense, and more extended vocal reaction. They are frequently in fighting attitude, and appear to be under greater sexual excitement. We were able, by means of control tests, to exclude the possibility that this condition of increased irritability results from the daily injections as such. Animals which receive daily injections of a physiological salt solution are not so tame, to be sure, as rats which have never been experimented upon; yet they do not exhibit the irritability of morphinized animals; furthermore, this condition can also be induced in rats through a continuous internal administration of opiates. If we define abstinence symptoms as those symptoms which can be banished by means of the very drug, the want of which produced them, then this, too, will hold good for the morphinized rats. To be sure, they become excited upon the renewal of the dosing; but this excitement is altogether different from the irritable excitement of abstinence. Fighting attitude, augmented defense reaction, and vocal reaction disappear; the animals pay much less attention to the world about them, disregard the food which is offered them, and are completely absorbed in their own peculiar movements.
Results
"The rat reacts to morphin and its derivatives with a diphasic picture of poisoning. The narcotic stage is followed by a stage of excitation.
"After habituation this diphasic character disappears. The narcosis is excluded. The excitation now conies about at once; dissociation of habituation. This excitation is more violent than at the beginning; augmentation of the excitation effect.
"The hypnotics chloral hydrate, amylene hydrate, luminal, are no less effective on the chronically morphinized animal than on the normal animal.
"The drugs which induce convulsions or excitement—picrotoxin, strychnin, cocain—do not have a stronger effect on the chronically morphinized animal than on the normal animal.
"The morphin derivatives eukodal, dicodid, dilaudid, and partly also codein, act on the morphin-habituated animal essentially like morphin itself, and are interchangeable with due regard as to dose.
"The rat may be habituated to dicodid and dilaudid.
"Habituation to morphin and its derivatives is achieved considerably more quickly than the withdrawal.
"During abstinence the rat presents typical symptoms, which may be banished by means of morphin (or its derivatives).
Discussion of the results
''These results afford an answer for many of the questions raised in the beginning. Thus the somatic factors in the development and general picture of morphinism can be more sharply distinguished from the psychic factors. If the question is as to how far abstinence symptoms are to be explained as preponderatingly psychic, how far the reversal of the effect in the addict arises from an abnormal craving for stimulation, then we see from our experiments with animals, in which we expressly disregard psychic symptoms, that corresponding alterations make their appearance. Here there has developed an augmentation of the stimulating effect along with a simultaneous resistance to the narcosis. This situation exceeds even that of a dissociation of habituation, as discovered by van Egmond in the chronic morphinizing of the dog, or by Langer in habituation to heroin. Langer emphasizes the fact that the stimulating effect of heroin is induced in the addicted dog by the same dose as in the non-addicted one. Naturally, sensitization may be assumed only when the same dose produces an increase in the stimulation symptoms. Biberfeld's experiments, which were made without regard to this caution, are not convincing. Also, we deem it important that it can be securely established that the withdrawal requires a disproportionately longer time than the habituation. The organism surrenders comparatively slowly an alteration in reaction which it acquired very quickly. Thus, too, the morphinist yields to his original poison even after months of abstinence more easily than before; and probably not merely because he knows or values its effects, not merely because he has made a deliberate decision, but as much because of an extrapsychic biological reaction of the mechanism of which we as yet have no idea whatever.—If Cloetta's rats, after two days' abstinence, died of lethal doses which they tolerated before, the fact does not at all contradict our discoveries, but only confirms what we have already said concerning the relatively easy habituation to convulsant morphin doses. For the clinic of morphinism there is greater practical significance in what we have established as valid for the compass of medium doses.
"The picture of acute poisoning and the alteration of its diphasic course through habituation can be linked with the views put forth by McGuigan and Ross and Tamura. According to these authors, in the process of metabolism a stimulating oxidation product is developed from the paralyzing morphin; only the dissimilarity of the metabolism is responsible for the fact that the mammal reacts with convulsions for large doses only, whereas the frog always presents two stages: narcosis and excitation. As we (in agreement with Rubsamen) have seen, the rat reacts essentially exactly like the frog; the principal difference between the two classes of animals does not hold at all. Yet it might be asked whether the disappearance of the narcotic stage in the morphinized rat and the exclusive appearance of the excitation stage were to be connected with an accelerated oxidation of the morphin in the course of habituation. If the fact that the excitation commences immediately after the injection already contradicts this —even if not forcibly, we furthermore believe that according to more recent experiments made by Joel and Arndts, another interpretation is more likely. The latter showed that the rabbit, which when intact reacts to morphin with paralysis and only after large doses with convulsions, displays excitement and a tendency to convulsions after much smaller doses than were required for the intact animal, when the cerebrum has been removed. They concluded from that and from further tests that the point of attack of the stimulating effect of morphin lies in the midbrain, and that normally the cerebrum has an inhibitory effect on the excitation apparatus. Assuming next that not all nervous systems have an equally great capacity for habituation—we refer to the quite different behavior of the respiratory center and the vagal center under chronic morphin poisoning—van Egmond and van Dongen—it would be quite understandable that only the systems which may be narcotized are capable of habituation°A and that the excitable systems are incapable; furthermore, that in the non-addicted animal the excitation can break through only after the narcosis has passed off, but that in the addicted animal, in which the point of attack of the narcosis has been functionally excluded, the excitation manifests itself immediately and exclusively. The omission of the narcosis in itself makes apparent an increased stimulation. Moreover, in the normal animal part of the drug is dissipated during the narcotic phase, but with the omission of that phase the entire injection is at the disposal of the excitable systems.
"After the experimental demonstration that chronic administration of dicodid and dilaudid likewise causes an alteration in the reaction, the corresponding clinical cases of morbid habituations may, without further' ceremony, be compared with the conditions existing under morphinism.
"The specificity of morphin habituation, as expressed in the unaltered sensitiveness to hypnotics, appears incompatible with clinical observations. (Compare also Biberfeld's corresponding results with dogs.) Here it must be noted that the resistance of morphin addicts to comparatively high doses of hypnotics, as revealed in the clinic, is observed during the withdrawal—that is, at a time when the patient is generally in a condition of serious psychic alteration. The higher degree of toleration with reference to narcotics, which springs from a condition of increased excitability (cf. the experiments on animals by Gensler) should, naturally, not be confused with a non-specific habituation, which then extends itself also to hypnotics. Decisive experimental conclusions are not yet at hand. Furthermore, it is doubtful whether animal experiments can here contribute to the understanding of clinical phenomena."
S. D. Ludlum and Ellice McDonald-1926.7°
These authors adopted the "smooth muscle reaction" of the intestinal tract as a means of estimating vagus-sympathetic balance of the vegetative nervous system. The action of morphin was studied in
addicted individuals. Their report of findings is included in the following:
if ... It was found that morphine hunger was a state of increased sympathetic tonus, or sympathetic preponderance with corresponding decrease in the smooth muscle reaction. The method was the twenty-hour roentgen-ray study of the vegetative innervation of the colon and the immediate fluoroscopic observation of the barium meal in the stomach in the absence of other drugs and purgatives. By means of the haustral arrangement and postural tone of the stomach and large intestine, it was possible to determine the effect of morphine and its withdrawal on the vegetative nerve balance.
"This is a method that lends itself readily to the study of drugs, endocrines and salts. The vagus division causes contraction of the haustra and diminished amplitude of the smooth muscle of the gastro-intestinal tract, and the sympathetic division causes increase in the amplitude and enlargement of the haustra. This is well seen in a study of the effects of atropine and physostigmine (eserine) on the intestinal smooth muscle. Atropine, as is well known, is a sympathetic stimulant (or paralyzes the vagus producing sympathetic preponderance), and roentgenograms before and after injection of atropine showed that a dilatation of the large intestine with obliteration of the haustra was produced by atropine. Physostigmine, on the contrary, produces vagus preponderance and it was found by means of roentgenograms before and after injections of physostigmine that contraction of the haustra and diminution of the caliber of the large intestine was produced by it. It was obvious, therefore, that the alterations in the haustral arrangement and postural tone of the smooth muscle of the intestine (which we call the smooth muscle reaction) were nerve (and not local) effects, and that the rhythm, rate and amplitude of the gastro-intestinal tract, as viewed by the roentgen rays, could be taken as an index or criterion of the vagus-sympathetic balance of the vegetative nervous system.
"In the habitué, morphine hunger was marked by dilatation and haustral relaxation of the colon and dilatation of the pupil—a decreased smooth muscae reaction (Figs. 1, 2 and 3)." n
*
"Morphine increases the vagus preponderance of the vegetative nervous system as we have found magnesium and calcium salts to do. It is not surprising, therefore, that Gwathmey has found that there is a synergism between morphine and magnesium sulphate. Both of these substances are in the class of anesthetics that decrease permeability of the cell, as we believe most, if not all, of the vagus stimulants do.
"The necessity of the morphine habitué may, therefore, be spoken of as an alteration of the vegetative nerve balance with sympathetic preponderance which morphine relieves by producing vagus stimulation. The condition is dependent on chemical changes of a colloid character in the bodily equilibrium, and morphine hunger is evidence of a deep physiologic need. The hope of the treatment of the habitué must be, therefore, in the correction of this physiologic or bodily unbalance by means of such substances as will produce the vagus preponderance or correction of the sympathetic preponderance and not produce the anesthetic or pain relieving effects of morphine."
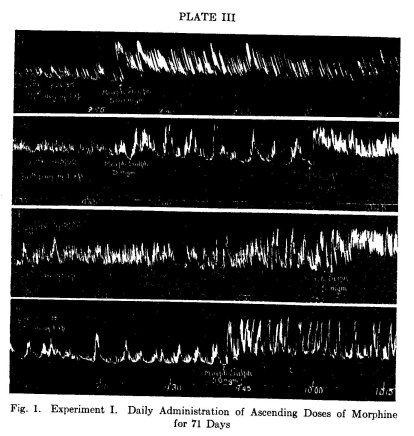
"Dog IA6, weight 20 kgm. Tracings from Thiry-Vella fistula of ileum, with rubber balloon and bellows recorder. Very slow kymograph.
"Tracing A, shows the effect of 50 mgm. morphine sulphate on the 10th day of the experiment.
"Tracing B, shows the effect of 3 mgm. morphine sulphate followed by 75 mgm. on the 29th day of the experiment.
"Tracing C, shows the effect of 3 mgm. morphine sulphate, followed by 250 mgm. on the 50th day of the experiment.
"Tracing D, shows the effect of 500 mgm. morphine sulphate on the 71st day of the experiment.
Eaton M. MacKay and Lois L. MacKay-1926.72
These authors first report the existence of a marked increased tolerance to morphin in uremic rats after double nephrectomy. They suggest a relationship between the increased morphin tolerance and the adrenal cortex hypertrophy in uremic rats. Further findings are given in what follows:
" ... Many findings point to a connection between non-specific resistance and the adrenal cortex. In so far as morphine is concerned, we have been able to confirm the observations of Lewis and Scott that tolerance to morphine is decreased following double adrenalectomy. In addition, we have found that the adrenal cortex hypertrophies when a rat is given increasing doses of morphine. The hypertrophy is greater the larger the tolerance attained."
G. H. Miller and O. H. Plant-1926.73
In a previous paper these authors reported "that injections of morphin and other opium alkaloids in unanesthetized dogs produced a marked increase in tone of the intestinal muscles together with an increase in frequency and amplitude of the large tone waves." Their objective in the present study was the determination of the effect of tolerance and withdrawal on the action of morphin as noted in normal dogs. Their experiments and findings are given in the following:
"Two experiments were carried out on dogs with Thiry-Vella fistulae of ileum. In one, a small dose was repeated daily for six weeks, in the other ascending doses were administered daily for a period of ten weeks. Graphic records of intestinal contractions were made by the technique reported in a previous paper by means of a sausage-shaped rubber balloon filled with water, inserted into the fistula and connected with a bellows recorder. In this way records were obtained without anesthesia or operative procedure at the time of the experiment.
"Experiment I. Ascending doses of morphine sulphate. Dog IA6, a large female collie, weighing 21 kgm. was used. The dog had recovered completely from the operation at which the fistula was made. It was in excellent condition and of quiet, friendly disposition. Daily hypodermic injections of morphine sulphate were administered for seventy-one days and during this time the dose was increased from 21 mgm. (1 mgm. per kilogram) to 500 mgm. (25 mgm. per kilogram). The dog remained in excellent condition throughout the experiment and lost only 1 kgm. in weight. There was some loss of appetite during the first two weeks, when the dog would refuse food at the regular feeding time, but usually ate most of the food offered before the next injection. There was never any diarrhea; the stools remained hard as they had been before the experiment was started. The stool interval lengthened somewhat as the experiment progressed, but was seldom longer than two days. In the earlier stages, the period of pronounced narcosis lasted four or five hours, but this became shorter as the experiment progressed and eventually the dog did not go to sleep immediately after the injection, although she kept very quiet and moved but little for several hours. Her disposition underwent a marked change after a few weeks—instead of being friendly and demonstrative she became shy and cowering and four to six hours after the injection became nervous, restless and spent much of the time wandering aimlessly about the kennel. Vomiting did not occur until the dose had reached 50 mgm. (2.5 mgm. per kilogram) and ceased at 75 mgm. Salivation was marked from the beginning; when the dose was increased to 150 mgm. the salivation became very marked, great strings of heavy, viscid mucus hanging from her jaws for several hours after the injection. This continued to the end of the experiment.
"Records of the intestinal contractions were made at intervals of two to three days throughout the experiment. Figure 1 shows the reaction that followed the injection at various stages, on the 10th, 29th, 50th and 71st days of the experiment.
"These tracings $how that the typical reaction to morphine remained throughout the entire period—marked increase in tone and in amplitude and frequency of the peristaltic waves.
"From time to time small doses (0.15 mgm. per kilogram) were injected before the daily dose was given. This amount is near the minimum for producing a distinct reaction and it invariably produced the usual effect, regardless of the size of the daily dose that was then being administered. Such effects are shown in tracings B and C of figure 1.
"During the withdrawal period there were quite marked changes in the character of the tracing obtained. The amplitude and frequency of the waves was increased, particularly the large tone waves (peristalsis). This is seen in figure 2, where tracings taken on the 1st, 2nd and 6th days of the withdrawal period are shown. All of the tracings were taken at the same time of day and therefore bear the same relationship to food and digestion; all were made with the same balloon and bellows-recorder so that the amplification of the contractions is the same in all:
"On the first day of the withdrawal period, the tracing was taken five hours after the time for the daily injection of morphine and comparison of this tracing (fig. 2, A) with the normal period in tracing D of figure 1, which was made on the day previous at the time of the injection, shows that there is a marked increase in the activity of the gut, even at this early stage of the withdrawal period. The increase in activity is even more pronounced on the second day of withdrawal and here the large tone waves are strikingly increased both in frequency and in amplitude (tracing B, fig. 2). A similar increase in muscular activity is evident as late as the sixth day of the withdrawal period (tracing D, fig. 2). After the sixth day, the tracings obtained from the fistula rapidly returned to normal. During the first three or four days of this period the stools were very soft or fluid.
"The general behavior of the animal also changed during the withdrawal period. The first day she slept almost continuously even while the tracing was being made and was difficult to arouse. Later she became restless and hard to control while on the table; there was marked twitching and jerking of the leg muscles, and during the periods of sleep she barked as though dreaming. After about a week her behavior was normal.
"Experiment II. Repetition of the same small dose of morphine sulphate. Dog IAS, a large female collie, weight 23 kgm. The dog had been operated for the formation of a Thiry-Vella fistula of ileum, sixteen weeks before the experiment was begun, and was in excellent condition. The animal had a lively and demonstrative disposition, but was easily trained to lie quietly on the table while tracings were made of the contractions of the ileum.
"Daily injections of 2.3 mgm. morphine sulphate were made for 42 days. Tracings were made from the Thiry-Vella fistula showing the effect of the injection every second or third day during the experiment.
"There was no decrease in the effect of this small dose during the six weeks it was administered. Each injection produced a prompt increase in the muscular activity of the gut, which was as great on the last day of the experiment as at the beginning. In figure 3, are shown the tracings obtained on the 7th, 14th, 23rd and 30th days of the experiment.
Fig. 2. Experiment I. Intestinal Contractions during Withdrawal of Morphine,
after Administration of Daily Ascending Doses for 71 Days.
"Dog IA6. Tracings from Thiry-Vella fistula of ileum with rubber balloon and bellows recorder on slowly moving drum. All the tracings were made at the same time of day and with the same balloon and bellows recorder.
"Tracing A, shows the character of contractions on the 1st day of the withdrawal period (72nd day of the experiment) about 5 hours after the usual hour for injection of the daily dose.
"Tracing B, shows the character of the contractions on the 2nd day of the withdrawal period.
"Tracing C, shows the character of the contractions on the 6th day of the withdrawal period.
Fig. 3. Experiment II. Daily Repetition of the Same Small Dose (0.1 Mgm. per Kgm.) of Morphine Sulphate for 42 Days
"Dog IA5, weight 23 kgm. Tracings from Thiry-Vella fistula of ileum with rubber balloon and bellows recorder. Very slow kymograph.
"Tracing A, shows the effect of the injection on the 7th day of the experiment; tracing B, on the 14th day; tracing C on the 23rd day and tracing D on the 30th day of the experiment.
"During the first twelve days of the experiment the dog showed some general reactions from the injection; nausea, salivation and on three occasions vomiting; slight narcosis, in that the dog was more quiet and somewhat less responsive for a few_.hours but did not go to sleep. There was no change in the character or frequency of the stool and the dog ate regularly. There was a moderate loss in weight, amounting to 2.5 kgm. at the end of the experiment. After the 12th day the injections had no apparent effect on the behavior of the animal, all evidences of nausea and of narcosis disappeared.
"When the administration of the drug was stopped there were no obvious changes in the tracing of the intestinal contractions or in the dog's behavior, except that she slept rather more than usual for a few days.
"It has been repeatedly demonstrated that many of the reactions produced by morphine in dogs disappear or are greatly diminished when the dose is repeated over a long period of time—narcosis, vomiting, respiratory effects, etc. Until the work of van Egmond, 1911, was published, it was supposed that tolerance extended to all tissues which show a reaction to the drug. This author showed that the cardiac vagus center does not become tolerant to morphine. In his experiment on a dog the pulse was markedly slowed by the injections even when they had been continued for a period of several months and the dose had been increased to 230 mgm. per kilogram. At this time the vagus center still showed a distinct reaction to much smaller amounts, e.g., 1 mgm. per kilogram.
"Van Egmond also tested the emptying-time of the stomach in his tolerant dog by means of the fluoroscope and bismuth meal and found that while there was some delay in the passage of the food into the duodenum, it was not nearly so great as described by Magnus 1908 in non-tolerant dogs. He concludes, therefore, that the alimentary canal develops only partial tolerance to this drug. These observations were confirmed by Reach, 1914.
"Van Dongen, 1915, studied the development of tolerance by the respiratory center, pupil, vomiting center and cerebrum in two dogs, and found that these organs eventually show complete tolerance, although the time and dosage necessary to produce it varied considerably for the different functions.
"The results of our experiments, which show that tolerance is not developed by the intestinal muscles to the stimulating effect of morphine, parallel the observations of van Egmond on the cardiac vagus center and furnish added evidence that tolerance to this drug is not developed equally by all tissues which react to it.
"In this connection, it is of interest to point out that there can be no direct relationship between these two observations—the failure of the cardiac vagus center and of the intestinal muscles to develop tolerance to morphine—for while the intestines receive motor fibers that run in the trunk of the vagus, we have shown that section and degeneration of the nerve fibers in the mesentery of a loop of intestine increases rather than diminishes its reaction to morphine, and this eliminates any central action of morphine as the source of the intestinal effect.
"Further, these results have a bearing on the cause of morphine tolerance; particularly on the theory advanced by Faust, 1900. He showed that in dogs the amount of morphine in the feces diminishes rapidly and eventually disappears as tolerance develops, and he holds that tolerance is due to increased destruction of the drug in the tissues. The fact that the intestinal reaction to small doses does not diminish after weeks of administration and that very small amounts of the drug are still effective at a time when other structures like the vomiting center and cerebrum fail to react to very large doses, indicate that other factors than increased destruction of the drug by the tissues play an important part in the development of tolerance to it.
SUMMARY
"1. The stimulation of the intestinal muscles by morphine does not disappear when the drug is administered continuously for several weeks. Very small doses continue to produce the reaction after daily administration during six weeks. Small amounts still produce a distinct reaction when ascending doses have been administered for ten weeks.
"2. These results indicate that other factors than increased destruction of the drug by the tissues play an important part in the development of morphine tolerance."
W. Weimann-1926.74
The author's findings in three human cases and numerous animal
cases of acute and chronic morphin poisoning are given in detail in the following:
"Organic alterations in connection with poisoning through alkaloids generally are very slight, and if present at all, quite unspecific. This holds also for poisoning by morphin and its derivatives, which, along with cocain and strychnin, undoubtedly have the greatest forensic significance of all alkaloids. For morphin poisoning a whole array of repeatedly occurring autopsy findings have been alleged. Yet these are in no way characteristic and, most important, may be altogether wanting.
"In acute morphin poisoning the most constant finding is hyperemia of the brain and its integuments (Manuals of legal medicine and poisoning). The sinuses of the brain also often display abnormal plethora. There may be an increase of fluid. Brain hemorrhages are comparatively rare (Kobert, Trdger). F. Strassman saw a typical purpura cerebri in a case of acute poisoning; Sysak saw extensive meningeal hemorrhages in a person who died two days after being poisoned. The hyperemia of the brain may also be missing. There was even a case in which a remarkably pale and anemic brain was found (Trdger, Auerbach). Usually the pupils no longer are contracted in the cadaver, but more or less enlarged and abnormal after death. The lungs generally are congested, and frequently oedematous. According to Trdger, there are lung hemorrhages, especially if there were convulsions before death. Generally, dark fluid blood is found in the heart. The abdominal organs are also generally hyperemic. The ecchymoses of the mucous membrane of the stomach, frequently present, are almost always attributable, according to Trdger, to the effect of emetics and stomach-rinsing. Only rarely do the contents of the stomach have a characteristic opium odor. Urinary bladder and lower sections of the intestines are well-filled generally because of the atony of their musculature.
"In chronic morphin poisoning, besides the skin abscesses caused by non-sterile injections and their consequences, the most frequent findings are marasmus praecox, general atrophy, and anemia. Often there is also oedema of the brain, lungs, and integuments, rarely symptoms of irritation in the intestine (Manuals of legal medicine and poisoning, Trdger). In addition Trdger mentions thickening of the bronchial or intestinal mucous membrane along with stasis in the lesser circulation (hypertrophy of the right heart, dilatation of the pulmonary artery) ; Weber—premature arteriosclerosis; Sysak—amyloid liver and kidneys, sago spleen, cardiac callosity.
"All these findings are not at all characteristic of morphin poisoning. They may be missing in pronounced cases of poisoning. In acute poisoning they correspond, in general, to the findings for asphyxia, as frequently encountered in the most varied morbid processes. In chronic poisoning they are to be attributed to cachexy, skin infections, or secondary diseases (tuberculosis).
"Thus far histological findings in the organs have been but scantily reported for morphin poisoning. From the beginning, special interest has been accorded in animal experiments to brain alterations only. As regards the work in question I have gone into detail elsewhere; I shall limit myself here to a brief summary.
"The investigations all belong to the period around 1900, when interest was limited to the various diseases of the ganglion cells, which were held to be specific for the individual forms of poisoning. As for other alkaloids, so for morphin, there were found very serious alterations of the ganglion cells which, to a certain degree, at any rate, always followed a definite course:—in acute poisoning, tigrolysis, swelling, and homogenization; in sub-acute and chronic poisoning, in part, serious liquefaction processes, vacuolization or contraction of the cells up to complete destruction. Abnormal fatty degeneration of the cells was also observed. Often the cell alterations were very slight, even for prolonged poisoning. In addition, there were mentioned rather frequently hyperemia of the brain-vessels and capillary hemorrhages; for prolonged poisoning, homogenization and thickening of the capillary walls, fatty degeneration of the capillary endothelia, and cellular or liquid exudations in the perivascular lymph spaces. Degeneration of the fibers of the posterior strands of the spinal cord, similar to that in chronic alcoholism (Nonne) was observed by Alt and Schütz.
"It is evident that the investigations made at that time were by no means without result. Nevertheless, the brain alterations figuring prominently in morphia poisoning were not characteristic. They occurred in precisely the sane form and intensity in connection with other alkaloids and poisons (lead, Hg, phosphorus, etc.) and since the hope of finding specific ganglion cell alterations for the various kinds of intoxications has been destroyed by Nissl's work, research of this sort has been abandoned completely. It is strange that, with a few exceptions, no investigations of the brain of chronic morphinists from modern points of view have been made as yet, with reference to the general histological process and its extension.
"Ewing is the only one who reported, some time ago, brain findings in 3 morphinists, where fatty degeneration, sclerosis, and tigrolysis of the ganglion cells were actually present. Weber, too, observed serious fatty degeneration of the ganglion cells and thickening of the walls of the cortical vessels; and recently Creutzfeldt reported a case of chronic morphinism of several months' duration, terminating in suicide with morphin (and probably veronal), in which in addition to the acute alterations there was present a diffuse fatty degeneration of the cortical cells and brain vessels with distinct cell degeneration in the cortex and increased storing of iron in the striatum.
"Histological findings in the remaining organs of the body have hardly been reported as yet.
"Pilliet mentions fatty degeneration of the liver in dogs. Horiuchi observed in animals already seriously cachectic enlargement and hypertrophy of the suprarenal cortex as well as enlargement of the medullary cells. Sysak, in a case of acute poisoning complicated with tuberculosis, observed, first of all, acute yellow liver atrophy with necrosis of the lobular centers, fatty degeneration of the lobular surface, and periportal infiltration, fatty degeneration of the kidneys and the myocardium along with hemorrhages of the spleen; in a case of chronic poisoning, likewise complicated by many secondary morbid processes, an atrophic amyloid liver, amyloidosis with moderate fatty degeneration of the kidneys, fatty degeneration of the adrenals, pancreas, seminal vesicle, a sago spleen with fatty degeneration of the trabeculae, and hemosiderosis of the parenchymatous organs.
"My investigations have concerned themselves principally with the central nervous. system, which quite automatically attracts special attention in animal experiments; also because the morbid findings in it for all forms of morphin poisoning dominate the picture, completely overshadowing those in the other organs. A case of acute poisoning, which, through the kindness of Professor Spielmeyer I was permitted to investigate at the Forschungsanstalt /fir Psychiatrie in Munich, is the starting point of my investigations.
"A shopkeeper, 26 years old, an unstable and hysterical psychopath, takes about 10 tablets of morphin at 7-8 P.M. At 8 P.M. he vomits; at 8:30 P.M. he becomes dizzy and light-headed. At midnight he was brought unconscious to the Munich Psychiatrical Clinic. Respiration shallow, pin-point pupils; vomiting. After a stomach wash, temporarily regains consciousness. Rapidly grows worse again; increasing loss of consciousness; Cheyne-Stokes respiration; extreme cyanosis. Death ensues 10 hours after poisoning.
"The autopsy (2 hours postmortem) revealed distinct brain hyperemia along with older adhesions and clouding of the meninges. In addition there were dilatation and brown atrophy of the heart, recent tracheobronchitis, old pleurisy, and cicatrised apical tuberculosis. All internal organs were highly plethoric; the urinary bladder was well filled. The brain alone was examined microscopically.
"The second case, which I owe to the kindness of Dr. Bratz, Director of the Asylum for the Insane, Berlin-Wittenau, involved chronic poisoning with laudanum.
"An editor, 42 years old, administered to himself injections of laudanum in large doses for about s/} year for chronic intestinal trouble of long standing. During a visit to Berlin, being unable to obtain laudanum he took 10 tablets of adalin. He was brought to the hospital in a state of sound sleep. Here a pronounced condition of psychic deficiency, in addition to uncharacteristic neurological symptoms, was established. Four days after admission the patient suddenly collapsed and died.
"The autopsy. (22 hours postmortem) revealed as the cause of death a perforated ulcer of the stomach, on account of which the patient had been having hemorrhages for some time, oedema of the lungs, incipient bronchopneumonia, slight atrophy of the spleen, dilatation of the heart, cloudy swelling of the kidneys, increase of lipoids in the suprarenal cortex. The brain was hypere iic and very moist. Ventricle slightly dilated. Microscopic examination of the brain only.
"Another case of chronic ntorphinism I owe to the kindness of Dr. Dyrenfurth, who conducted the legal postmortem.
"Shopkeeper, 26 years old; charity case; heavy morphin abuse for 7 years, after operation for gall-stones. Numerous unsuccessful withdrawal cures in hospitals and asylums for the insane. 15-20 injections daily, according to his mother's statement. One afternoon he came home completely exhausted and slept till next morning. He was found unconscious in bed at 3 o'clock, and died an hour later Hidden in the armpit was a bottle of morphin solution. The mother assumed suicide with morphin.
"Thé autopsy (4 days postmortem) revealed distinct hyperemia of the brain, lungs, liver, and kidneys, a few infarct-like areas in the lungs. Suprarenal cortex very rich in fat. Intestines very much inflated. Old scarred adhesions in place of the gall-bladder. Arms and legs showing numerous abscess scars and fresh points of injection.
"In addition, numerous rabbits, guinea pigs, and mice were given subcutaneous or intravenous injections of maximal doses of morphin several times each day. Some of the animals were given superlethal doses from which they died in 1-3 hours; others were kept longer under morphin until they either died of themselves or were put to death after 1-16 days of poisoning. The sensitiveness of the animals to the poison varies greatly. Habituation appears even after comparatively brief intoxication. The rabbits under poison for the longest period received altogether up to 525 g., the guinea pigs up to 2.04 g., the mice up to 0.1 g. morphin.
Central Nervous System
"The brain findings in the human cases of poisoning show wide agreement despite the fact that in the one there was acute intoxication and in the other chronic. It is a question of a severe and purely degenerative morbid process, widely spread through the entire brain and most highly pronounced in the cortex. Abnormal fatty degeneration, shrivelling, and honeycomb degeneration of the ganglion cells are most prominent ; these have led to the destruction of numerous elements, especially in the third and fifth cortical layers. There is considerable fatty degeneration of the glia cells also and, most important, the walls and especially the endothelia of the brain-vessels contain unusual quantities of lipoid. Along with these there are, in the acute case especially, more acute alterations of the ganglion cells in the form of tigrolysis and swelling of the elements. Most severe are the cell alterations in the forebrain, especially in the cornu Ammonia, while those in the occipital lobe are comparatively slight. Of the deeper brain centers, the striatum is especially affected, but not so intensively by far as the cortex. Further down, the process rapidly decreases, so that the alterations, in the medulla oblongata and spinal cord especially, are comparatively slight. The pia shows slight fibrotic thickening and, especially in the acute case, it is traversed by hemorrhages. Separation of nerve fibres is very slight. The difference in the cases rests chiefly on the differing intensity of the alterations in the ganglion cells. In the chronic cases they are generally more severe and have led partly to a liquefaction of the ganglion elements with extended cell destruction in certain cortical layers. Also, the fatty degeneration of the vessels is here much more intensive than in the acute case. Furthermore, in one of the chronic cases there is a fibrotic degeneration of the cortical vessels, which has also led to the development of infarct-like atrophic areas corresponding to the arteriosclerotic areas. In the acute case there has come about a decided ameboidosis of the glia in the medulla of the hemispheres, which is not found in the chronic cases.
"In the animals the brain lesions vary with the duration of the drugging. In addition, there are certain differences as regards their localization between individual animal species. Here, too, the alterations of the ganglion cells are everywhere in the foreground. In animals subjected to acute poisoning with superlethal doses, which generally died suffering dyspnoea, convulsions, and urine discharge, they are likewise already distinctly pronounced. Essentially it is a case of tigrolysis and swelling of the elements. The brain vessels are regularly richly filled with blood. In animals under poison for a longer period —up to 8 days—the alterations assume very severe forms. The ganglion cells perish under conditions of most severe liquefaction, decomposition of plasma, and disintegration of nuclei. In animals which have been kept still longer under morphin, the cell alterations are not so intensive, but have a more chronic character, so that shrivelling and honeycomb degeneration of the elements are more frequently encountered, the latter perishing in great numbers under these conditions also. In animals, fatty degeneration of the cells and blood vessels plays no part. In the rabbit it is still clearly demonstrable; in the guinea pig it is already very slight; in mice it does not appear at all. All alterations of ganglion cells are accompanied by corresponding glia reactions. The vessels in animals longest under poison are somewhat thickened and generally copiously filled with blood, so that, when dissected, the brain appears highly hyperemic. Extensive hemorrhages in the meninges and the cortex are seen frequently even after a short period of poisoning. Separation of medullary fibres is entirely absent. The different localization of cell alterations in human beings and animals is very important. In the rabbit they show a decided preference for the cortex, the third and fifth layers in the forebrain being most seriously affected. Here, too, the cornu Ammonis is generally most seriously altered. The deeper parts of the brain, preeminently the striatum, are more severely affected in the rabbit than in man. In the guinea pig the alterations in the cortex and striatum are about equal; in fact, the cortex is quite often less diseased than the striatum, and there are even quite severe alterations in the deeper centers way down to the nuclei of the cranial nerves. In mice the cortex is only slightly altered. On the other hand, the ganglion cells in the striatum and the deeper centers of the brain, down to the spinal cord, are most highly diseased. In accord with this, the clinical symptoms of poisoning in animals are essentially different from those in man. Striatal symptoms are preeminent; muscular rigidity in body and neck (opisthotonus), pathologically intensified retention of a certain position, stiffness, trembling. Likewise, the typical manner of holding the tail observed in mice and important for the biological demonstration of morphin is no doubt to be referred to the general muscular rigidity and striatal causes. In animals longest under poison the striatal symptoms are less prominent, making place for certain changes in demeanor, above all, anxiety and timidity.
Lungs.
"The lungs regularly appear congested in animals. Subpleural hemorrhages, inspissations, pneumonia of the inferior lobe, are frequently seen. Microscopically, too, the hyperemia of the lungs is very distinctly apparent. Frequently there is a discharge of dropsical fluid or erythrocytes into the alveoli. Hemorrhages of this sort were very extensive in some animals, especially in mice, so that even larger bronchi were filled with blood. Frequently alveolar epithelium, which had undergone fatty degeneration and desquamation, is mixed in with the dropsical fluid. Bronchopneumonia and severe bronchitis are seen rather often, especially in guinea pigs.
"In the human case of which histological examination was made, there was found unexpectedly a fat-embolism, which, originating from some unidentified trauma (?) caused swift death through pulmonary oedema, quite independently of the morphin poisoning, no doubt.
Heart.
"In the human case there is present a severe and diffuse fatty degeneration of the heart muscle which, in part, has reached an exceedingly high degree. In animals the heart is generally filled with fluid blood. Microscopically there is evident in acute poisoning only a certain indistinctness of the transverse striation. After a longer period of poisoning fatty degeneration of the heart muscle is found in rabbits, but not regularly. Thus, in animals longest under poison, which stood the morphin very well, there was only a suggestion of it; it was most severe—to the point of fatty disintegration of the muscle fibres—in one which had been under poison for 10 days; but this animal displayed serious organic alterations in other respects also. In the guinea pigs there was incipient fatty degeneration of the heart, but only rarely and never to such a high degree as in the rabbit. The heart muscle may here be thoroughly normal even after prolonged poisoning. Fresh myocardial hemorrhages were strikingly frequent in guinea pigs. In mice, even after prolonged poisoning, there were no heart alterations whatever.
Liver.
"In the chronic morphinists the liver showed a high degree of atrophy due to congestion along with severe fatty degeneration and contraction of the central trabeculae of the hepatic cells, in addition to cirrhotic proliferation and infiltration of the periportal connective tissue.
"In the rabbits the liver was extremely plethoric, and the outline of its lobules generally indistinct. In animals subjected to acute poisoning or kept under poison up to 2 days, only hyperemia and slight increase of fat in the central hepatic cells are seen microscopically. Likewise, in animals under poison for a longer period this abnormal plethora of the liver is usually present and frequently leads to contraction and rather severe fatty degeneration of the central trabeculae of the hepatic cells, in connection with which there is also an increase of fat, though not so distinct, in the hepatic cells of the periphery. In addition, the animals often show increased fatty degeneration of the stellate cells on the lobular surface. In an animal under poison for 5 days there was even incipient central lobular necrosis. The hepatic cells and their nuclei were here included in the decay; the intralobular capillaries were highly dilated. In several animals there were small hemorrhages in the liver. In a rabbit under poison for 10 days these dominated the picture completely, having wrought utter confusion in the hepatic tissue; the hepatic cells, dissociated by them, had suffered fatty decay. A little iron was found a few times in the peripheral hepatic cells.
"In the guinea pigs the liver was usually not hyperemic; rather often, on the contrary, after a period of poisoning of some duration, it was pale, grayish-yellow, brittle. Only in animals under poison for some time could fairly severe congestion be determined microscopically; in one case this had led to the contraction of the trabeculae of the hepatic cells. The chief alteration in the guinea pig was fat deposit, and, in fact, this fatty degeneration of the liver generally increases in severity the longer the animals are kept under poison. It is then no longer possible, as in the normal animal, to distinguish in the lobular surface the hepatic cells that have undergone considerable fatty degeneration from those which have no fat at all or only small quantities of fine droplets; but all the hepatic cells contain more or less abundantly finely-granulated as well as larger drops of fat, so that there is presented the picture of a diffuse fatty degeneration of the liver without distinct degeneration of the cells. The stellate cells, too, have generally undergone considerable fatty degeneration. This, however, is not a regular finding. In the animal longest under poison the hepatic cells contained no fat at all beyond a few insignificant droplets. But as evidence of rather severe degeneration, they displayed a peculiar flaky disintegration of their plasma. Only in a guinea pig under poison for 10 days was there present considerable hemosiderin deposit in the lobular surface. Otherwise, the liver was always free of iron. In an animal kept longer under morphin, there had resulted small hemorrhages in the hepatic parenchyma.
"In mice the liver is usually hyperemic after acute poisoning. After prolonged poisoning this hyperemia is usually not so distinct. In isolated cases there were hemorrhages in the hepatic tissue. After poisoning of short duration, there is an increase of the fat content of the liver, already fairly abundant in the normal animal. Hepatic cells which have undergone complete fatty degeneration, encountered in the normal animal only singly, are here seen in groups. After prolonged poisoning, from about 7-9 days on, the fat content of the liver decreases rapidly, so that finally the liver is almost completely free of fat, and cells with drops of fat are met only here and there in the plasma. This loss of fat in the liver is very distinct in animals longest under poison. In addition, the hepatic cells then display flaky decomposition and vacuolar degeneration of their plasma. Their nuclei, however, remain well preserved. There is no deposit of hemosiderin.
Kidneys.
"The human case shows considerable fatty degeneration of the kidneys, which affects not only the collecting tubules but also all the canal systems, and especially, Henle's loop and the intercalary tubules.
"In the rabbit, the kidneys appear hyperemic macroscopically and microscopically. The epithelium of the tubuli contorti (convoluted tubules) is cloudy. In addition, after prolonged poisoning, there is generally found much more severe fatty degeneration of the intercalary tubules and Henle's loop than in the normal animal. These showed most severe degeneration, being filled with large drops of fat, in a rabbit 14 days under poison. In the tubuli contorti also there appears usually, but not regularly, degeneration to fine droplets of fat after a prolonged poisoning. There was no evidence of hemosiderin in the kidney.
"In the guinea pigs the increase of fat, especially in the intercalary tubules and Henle's loop, is still more striking. After prolonged poisoning, these may contain fat in large drops and may even suffer fatty decomposition. There is also an increase of finely granulated fat in the tubuli contorti and in the collecting tubules, which in the normal animal contain only isolated drops of fat. But this, too, is not a regular finding. For in the guinea pig longest under poison, it was strikingly slight.
"In mice the kidney displays only a varying degree of hyperemia, but never fatty degeneration. In one animal there was interstitial nephritis, which was probably independent of the poisoning.
Spleen.
"In the chronic morphinist this shows no essential alterations; in animals, too, it is usually only abnormally plethoric. In the rabbit hemorrhages are often found in the pulp. The cells of the pulp quite often contain increased fat after prolonged poisoning. There was never any evidence of increased hemosiderin.
Testicles.
"In rabbits and mice these show no change. In guinea pigs, after prolonged poisoning, the seminal cells generally show considerable fatty degeneration, but not the interstitial cells. In the chronic morphinists the seminal cells likewise contained finely granulated lipoid in great abundance, and the interstitial cells, too, here showed a high degree of fatty degeneration.
Urinary bladder, digestive tract.
"Their fulness varied in the rabbits. In an animal which had been subjected to acute poisoning and had had a discharge of urine before death, it was empty; likewise in some animals which had undergone prolonged poisoning. In the rest it contained 10-20 cc., in one even 60 cc., of urine. The digestive tract was always well filled, in some cases even to excess. In the guinea pigs and mice, neither bladder nor intestine generally showed unusual fulness.
"The central nervous system is the most severely affected in morphin poisoning. The alterations in this, because of their intensity and regular occurrence, are in the foreground of the pathologico-anatomic picture of poisoning. In agreement with this, the cerebral symptoms usually predominate completely among the clinical symptoms of poisoning. Death in morphin poisoning is a brain death. In the most acute form of poisoning, distinct brain alterations are already apparent which sufficiently explain its swift issue in death before other organic alterations have had a chance to develop, and this fact is confirmed by the experiments on animals. The findings in the central nervous system in the human cases of poisoning have far-reaching similarity. In the acute case they cannot be referred solely to the morphin poisoning, which proved fatal within 12 hours. There it is rather a matter of a chronic brain process, which had been going on for some time, overlaid by acute alterations (acute cellular disease, amoeboidosis of the glia, irritation of the endothelium, hemorrhages). Only the latter may be attributed to the acute poisoning, and show striking correspondence to the alterations displayed by animals subjected to acute poisoning. What caused the chronic brain process in this case cannot be stated with certainty. The poisoned man may have been a chronic morphinist—it is well known that chronic morphinists use morphin for suicide very frequently—and the chronic brain process is to be attributed to the morphin abuse of longer standing.
"The brain alterations, as present in the human cases, occur in association with a great variety of troubles. They occur physiologically in old age, in the most varied forms of infection and intoxication accompanied by cachexia and anemia (tuberculosis, carcinoma, pernicious anemia), and in psychoses, especially in dementia praecox and melancholia. They are, therefore, not at all characteristic of morphin poisoning. They have recently been described by Maier in quite similar form for chronic cocainism. According to Bonhoeffer, they are also found very frequently in chronic alcoholism. Very little is as yet known as to their connection with psychic disturbances. The connection is probably very slight, however. For brain processes of this sort are often seen in individuals who have never in their lives had a psychic disturbance. On the other hand, they occur in pictures of the most severe psychotic states (Dem. prec.). In morphinism they are undoubtedly especially marked principally through their combination with vascularly conditioned atrophy of the cortex. They may suffice to explain the psychic disturbances, which so often appear here—often too, in highly pronounced form, and they are the anatomic expression of the serious brain lesion which also results in the psychic disturbances, though they may not be regarded as the anatomic substratum for the latter.
"Moreover, the brain alterations in acute poisoning are not specific and correspond closely to those observed in the most varied infections: (typhus, sepsis, scarlet fever, dysentery), and intoxications (CO, phosgene, phosphorus, veronal, etc.). In subacute poisoning they assume extremely serious forms and may then lead to extended liquefaction, decomposition, and destruction of the ganglion cells. Recently I saw a lesion of this sort through the entire central nervous system in a case of acute poisoning with arsenic which proved fatal within 6 days.
"The lipoid degeneration of the ganglion cells prominent in the human being is inconspicuous in animals. In the rabbit it is still to be found, in the guinea pig but little, in mice not at all. Probably the reason for this lies in the very different fat metabolism in the brain of these animals, which is very poor in lipoid even normally. In addition, a part is played, no doubt, by the very different poisoning tempo in the animals, their different way of reacting to the poison, and the especial severity of the brain alterations in them, the latter perhaps no longer permitting the appearance of such fatty degeneration.
"Of great importance is the different localization of the brain process in the human being and in animals, and above all, the penetration of the process in animals into the striatum and the deeper brain centers, while the cortex, especially in mice, remains notably exempt. Undoubtedly we must take into consideration here the fact that the intoxication in animals is much stronger and permits the appearance of alterations in brain regions which would otherwise be spared by the process. In addition, however, there is evidently a different sensitiveness of the individual brain centers in human beings and in animals. The further down we go in the animal scale, the more sensitive is the striatum to poison, while the cortex, in accord with its defective development, shows less and less change. Similar differences in the localization of the brain alterations in different animals are known also for other poisons, e.g., phosphorus (Kirschbaum, Lewy).
"The effect of morphin on the brain is in the main direct, as the poison directly injures the various constituents cif the neural parenchyma, especially the ganglion cells. In chronic poisoning, a secondary lesion of the central nervous system also plays a part—through the general cachexia and anemia—to which the poisoning finally leads, and which combines with the morphin effect. Morphin has no special point of attack in certain brain centers, such as is observed for other poisons (nicotin, methyl alcohol—retina; botulism—medulla; stovaine—anterior cornu). It does by far the greatest damage to the cerebral cortex (in animals, the striatum), which is in general the favorite point of attack for the majority of the diffuse, toxic, and infectious brain processes. But morphin also exerts a secondary .effect on the neural tissue through lesions which come in a roundabout way through disturbances in the circulation. Evidence of this is found first of all in the hyperemia of the brain, which is frequently very severe; also in the frequent occurrence of diapedetic hemorrhages in acute poisoning, which may frequently lead, as with other poisons (veronal, phosgene, CO), to real brain purpura (F. Strassmann) ; in the especially severe affection of the hippocampal regions; and, most important, in the chronic degeneration of the walls of the brain vessels, as seen in man and animals after prolonged intoxication.
"The alterations of the remaining organs become inconspicuous in comparison with those of the central nervous system. As is generally the case in alkaloid poisoning, it is not a matter of specific and regularly occurring morbid processes.
"In acute poisoning there appears only severe hyperemia of the internal organs, which is no doubt to be referred chiefly to the paralysis of respiration and to asphyxia. However, the paralyzing effect of morphin on the nerves of the vessels probably also plays a part. Besides the brain, the lungs also display congestive hemorrhages and oedemas, for which an increased permeability of the vessel-walls, consequent upon the action of the morphin, is perhaps to be held responsible. Hemorrhages of this sort have been found with comparative frequency in acute poisoning (Strassmann, Sysak). In addition to the hyperemia and the hemorrhages, other alterations appear only after several days' poisoning, as shown by the animal experiments. In antithesis to this, Sysak—to date alone —found severe central necrosis of the liver and fatty degeneration of the parenchymatous organs in a case of acute poisoning, which proved fatal within 11h days. He emphasizes the similarity of these findings to those for poisoning with phosphorus, chloroform, and mushrooms, and he thinks that in morphin poisoning also there result disturbances of metabolism and lipemia, in connection with which it might be asked whether the fatty degeneration is due to diminished nutritive resorption, disturbances of the function of the liver in the sense of defective oxidation, or the activating of lipolytic ferments together with the mobilization of the fat depots. Intensive fatty degeneration of this sort in connection with the internal organs has not yet been observed in acute morphin poisoning, not even in animal experiments. The fatty degeneration of the organs which finally sets in here after prolonged poisoning has a different significance. Moreover, central necrosis of the liver, as in Sysak's case, within 1% days after the poisoning would be very remarkable. To be sure, among other alkaloids, cocain manifestly can produce very quickly such necrosis of the liver and fatty degeneration of the parenchyma. Thus, Erzer observed for cocain poisoning a finely-granulated fatty degeneration in the human liver within 30 minutes, and severe necrosis of the liver in poisoned animals, especially in mice, within a half day. With cocain, however, we have manifestly an entirely selective action of the poison on the liver similar to that produced by poisoning with phenylhydrazine, amylene hydrate, paraffin oil, and such as cannot be assumed for morphin according to our experience to date with human beings and our experiments on animals. Sysak's case was complicated by pulmonary tuberculosis, lobular pneumonia, exudative pleuritis, and solitary tubercles in the liver. It seems to me that, as Sysak also suggests, the organic alterations must be referred chiefly to the severe tuberculosis, and that at most the acute morphin poisoning served only to promote this as well as the necrosis of the liver. In acute and chronic poisoning there appear then, as shown by the human cases and the animal experiments, organic alterations which in part are quite considerable. In the foreground is the lesion of the parenchymatous organs, which finds expression principally in an increasing fatty degeneration. This is most pronounced in the liver, generally finely granulated and accompanied irregularly by a degeneration of the stellate cells also. Next in order is the fatty degeneration of the kidneys and the heart. The heart lesion is particularly important. It explains the extremely bad condition of the heart frequently encountered among morphinists. But even in chronic poisoning there never occurs the fatty infiltration of the large parenchyma such as is found in poisoning with phosphorus or alcohol. The organic fatty degeneration in connection with the morphin poisoning induces, as seen repeatedly in human beings, a pronounced cachexie. In animals also, even after a comparatively short period of poisoning, there occur extraordinary losses in weight and extreme emaciation, because the resorption of nutriment is more or less checked by the intestinal atony, the fat reserves are reabsorbed, and the processes of oxidation, as shown by Schuebel's experiments in metabolism, are greatly reduced. These defective oxidation processes are probably the chief cause, along with the disturbed nutritive resorption and the direct injury to cells caused by the morphin, of the fatty degeneration of the organs. Disturbances of the circulation, especially in the form of passive hyperemia in the liver, must undoubtedly be considered along with these. Thus, through the combined action of these lesions generally, there develops after prolonged poisoning the fatty degeneration of the liver, kidneys, and heart musculature. The loss of fat and the degenerative cell alterations in the liver, which finally occur in guinea pigs and mice, are evidently to be explained by the fact that after the resorption of their fat reserves the animals are in a state of hunger and the hepatic cells suffer especially intensive injury from the severe poisoning. We then see a disappearance of fat from the cells resembling that which occurs in grave disorders due to under-nutrition and metabolism. (Lubarsch). The fatty degeneration of the organs in connection with chronic morphin poisoning would correspond, therefore, in general to those frequently occurring in connection with chronic infections and intoxications, anemia and cachexia, also e.g. in connection with prolonged chloral action or CO-poisoning (Jacksch, Roos), as the manifestation of lowered oxidation processes and disturbed cellular metabolism. The lipuria observed by Schuebel in morphinized dogs is sufficiently explained by the fatty degeneration of the kidneys.
"The passive hyperemia of the liver may lead to a congestive atrophy, as is evident from the animal experiments and one of the cases of chronic poisoning. In one rabbit there had even developed central lobular necrosis. Morphin, therefore, may bring about—but only after prolonged action—a necrosis of the liver, consequent upon severe circulatory disturbances in combination with direct cell injufy. Still, this rarely happens. These hepatic lesions play a more important part and appear more regularly in connection with poisoning through other soporifics. In experimental poisoning with dial and veronal, Samejuma regularly observed, in addition to the fatty degeneration of the heart, hemosiderosis and atrophy of the spleen, nephrosis, and pronounced pulmonary lesions, similar to those observed in connection with morphin, a severe hepatic lesion, not in the form of fatty degeneration, but of necrosis and vacuolization of the hepatic cells, similar to those observed in connection with cocain (Erzer). After prolonged morphin poisoning the vascular lesions may become so intensive, that extensive hemorrhages may occur also in the myocardium and the liver in addition to those in the brain and the lungs. Nevertheless, according to the results of my animal experiments, augmented decomposition of the blood plays no essential part. For hemosiderosis of the liver was present in a few animals only. Nevertheless, it is possible that hem osiderin deposits in the internal organs might have been more conspicuous, if the poisoning had been continued for a longer period.
"The pulmonary lesions in animals are quite important. We regularly find here more or less severe hyperemia and, consequent upon capillary lesion, congestive hemorrhages and oedemas, which lead to bronchitis and bronchopneumonia, to which the animals are, of course, especially liable by reason of the defective ventilation of their lungs, the lowered oxidation processes, emaciation, and lack of exercise.
"The hemosiderosis, general amyloidosis, and testicular atrophy, observed by Sysak in a case of chronic morphin poisoning, are probably likewise not attributable to the morphinism alone. It is manifestly a matter of the effects of chronic sepsis resulting from recurring skin abscesses, enterocolitis, cholelithiasis, pulmonary lesions, and anemia, which were already present in the patient and now combined with the action of the morphin.
"The retention of urine in connection with morphin poisoning is frequently regarded as especially significant with reference to diagnosis. Morphin causes atony of the urinary bladder as well as of the intestine, so that the former is generally pretty well filled in animals, there being no essential disturbance of the urinary secretion. Nevertheless, this is not a regular finding. For frequently it was also found normally filled or else, especially when the animals had had an involuntary discharge of urine before death, empty, so that the diagnostic significance of the abnormal bladder fullness must be designated as very slight.
Addendum.
"At the close of the foregoing investigations another case of acute morphin poisoning came under my observation through the kindness of Dr. Kipper.
"The case concerns a 5-year-old boy, who was poisoned by his father with morphin, or in all likelihood, pantopon. The father also took the poison and died shortly after. The contents of his stomach revealed considerable morphin. The child was brought to the Charité in a condition of deep coma, with pinpoint pupils almost without reaction, and poor respiration and heart action. In the next two days respiration and heart action improved a little. He also became semi-conscious. Now, however, tonoclonic convulsions, particularly in the region of the facial and the hypoglossal nerves, made their appearance in quick response to noises and touch; also, fibrillar muscle twitchings, states of excitement resembling delirium along with rising and sitting upright, impulsive crawling about, loud screaming, and highly pronounced variations in cerebral temperature. At the end of the 2nd day, abatement of these symptoms; on the other hand, paralysis of respiration and heart, incipient bronchopneumonia, and finally death, about 2', days after the poisoning.
"The autopsy (Prof. Wiitjen, Pathol. Inst., Berlin) disclosed extreme venous hyperemia and swelling of the brain with flattening of the gyri, hyperemia of the pectoral and abdominal organs, bronchopneumonia and pulmonary emphysema, status lymphaticus, swelling of the splenic pulp, anemic spots in the liver, and heavily-filled urinary bladder.
"Histologically it is, a case of extremely severe degeneration in the central nervous system, which becomes very intense in the cortex and the cornu Ammonis. The ganglion cells in the 3rd cortical layer show the most serious alterations—principally acute disease or liquefaction. In the frontal lobe the process has in part advanced so far that the cells are here almost all necrotic (cellular "ischemia") and this has caused laminar degeneration in the 3rd layer. Cell destruction of similar intensity has occurred in the pyramidal band of the cornu Ammonis, which on that account also appears considerably atrophied. The alterations in the ganglion cells in the remaining cerebral regions are not so intensive. Still, even here there are seen, in places, quite serious processes of liquefaction and degeneration, which have produced intensive glia reactions in some basal ganglia regions. A slight fatty degeneration of the ganglion cells is in fact present in the 3rd cortical layer and the cornu Ammonis, but it is quite insignificant. The venous cerebral vessels, in particular, are heavily filled with blood. In the cortex and cornu Ammonis, the cells of their walls do not contain, in view of the child's age, pathologically augmented lipoid matter. In the pia, and here and there in the brain itself, there are diapedetic hemorrhages, which are occasionally extensive.
"Of the remaining organic alterations the most striking is an extremely intensive, diffuse fatty degeneration of the heart, which has caused here and there the fatty decay of muscle fibers.
"The liver also shows principally central fatty degeneration, though symptoms of decay in the hepatic cells are not perceptible. The stellate cells, too, contain considerable lipoid. In the periportal connective tissue are infiltrations of round cells.
"In the highly plethoric kidney there is likewise a severe, partly coarsely granulated fatty degeneration of Henle's loop and the intercalary tubules. In the tubuli contorti also there are here and there fine fat droplets. Moreover, they contain everywhere hyaline and granular casts.
"The splenic pulp contains a little hemosiderin. The germinal centers of the lymph follicles are strongly developed. The lungs appear very plethoric; there is considerable fatty degeneration and desquamation of the alveolar epithelium. Bronchitis and localized pneumonia have developed.
"Of great interest in connection with this ease of morphin poisoning, which proved fatal within 21 days, is the exceedingly severe, purely degenerative brain process, in comparison with which the alterations in the other organs are quite insignificant. Here, too, it is undoubtedly a matter of brain death, just as the clinical picture of the poisoning was purely cerebral. Incidentally, the convulsions, very similar to those occurring in connection with strychnin poisoning, are quite remarkable and indicate the action of pantopon. The brain alterations correspond to those which I was able to produce in animals by poisoning them for several days with large doses of morphin, and also to those observed in connection with other toxic processes (sepsis, gas-gangrene, whooping-cough, etc.). In the remaining organs it is essentially a matter of passive hyperemia and fatty degeneration of the parenchyma, which is quite considerable in the heart muscle, but not as yet highly pronounced elsewhere. The case thus confirms the foregoing conclusions to the effect that in morphin poisoning we are not dealing with a fermentative mobilization of the fat reserves, lipemia, and fatty degeneration of the large parenchyma, such as are found in poisoning with chloroform, phosphorus, and agaricus phalloides, but that we are dealing essentially with a general lowering of oxidation processes and with toxic cell lesion, which finally and, on the whole rather rapidly, lead to organic fatty degeneration in addition to the circulatory disturbances, as shown by this case. Particularly noteworthy also are the serious pulmonary lesions, which correspond to my observations in the other human cases and the animal experiments; and likewise, the cast formations in the kidney. These suggest a more serious nephritic lesion than has apparently been observed to date in connection with morphin poisoning."
Hans Gerhard Creutzfeldt-1926?s
After commenting on the infrequency with which pure cases of chronic morphin poisoning come to autopsy, and citing the neuropathologie findings of Spielmeyer, Weimann, and Husemann, the author reports in detail the histologic changes observed in a case of morphinism dying from acute morphin and veronal poisoning, in which he considers the effect of the veronal taken to have been slight if any.
The case was that of a woman of twenty-six, a morphinist for about two years who took with suicidal intent unknown quantities of morphin and veronal about two hours before admission to the hospital, when she presented the symptoms of morphin poisoning. The condition of the patient while in the hospital and the author's reasons for concluding that death was due to morphin rather than veronal poisoning, are given in the following quotation:
". . . At the time of her admission to the hospital she was in deep stupor and without any sign of mental reaction. The pupils were constricted and fixed, the complexion pink; Achilles and patellar reflexes normal; no pyramidal symptoms; pulse and respiration normal; in 553 cc. of stomach contents there were 0.05 g. of morphin and less than 0.5 g. of veronal. The next day cyanosis appeared, but, with good pulse. The first symptoms of stasis pneumonia were noticed. In 1,160 cc. of catheterized urine (retention of urine) 0.0974 g. of morphin and 1.015 g. of veronal were found. Treatment without any effect. The condition grew worse, the paralysis of respiration increased; temperature rose to 39.9, pulse tense and frequent. On January 22, at 1:45 p.m., about 60 hours after the poisons had been taken, death occurred. We see the case of a morphin-addicted woman poisoned with a considerable quantity of morphin and a small—apparently not fatal—quantity of veronal, taken with the intention of suicide. This may be assumed not only in consequence of the quantitative proof of the poisons in the gastric juice and in the urine, for in both secretions fatal quantities of morphin, but not fatal quantities of veronal, were found; but also because, as will be remembered, morphin, as has often been stated, appears only in very minute quantities in the urine, and much less in the gastric juice of morphin-addicted persons than in that of normal persons, while it is well-known that veronal is extensively eliminated by the kidneys. Also the clinical report is characteristic of poisoning by morphin: skin lightly hyperaemic, absence of any reaction, myosis, good heart activity of long duration with increasing paralysis of respiration. Veronal, on the other hand, usually affects the action of the heart, produces cyanosis, nystagmus and spasmodic tendency. Therefore it seems justified to disregard the veronal poisoning in the present case and to make a diagnosis of `acute morphin poisoning in chronic morphin addiction'."
The autopsy findings are given in full in the following:
"Marked passive congestion and oedema of the brain; passive congestion of liver, spleen, and kidneys; old calcified mesenteric lymphatic glands; marked passive congestion and oedema of the lungs, congestive catarrhal haemorrhagic inflammation of the bronchi; marked parenchymatous tumefaction of the spleen; extensive centres of regeneration in the bone marrow; vermiform appendix absent after operation; peritoneal growths around the cecum and lower ileum; perihepatic growths on the diaphragm; in the gall bladder a stone about the size of a cherry stone.
"The cerebral meninges and the brain itself were in general very congested and showed an increase in their fluid contents; this acted as an oedematous infiltration of the meninges, and in the brain, as its soft consistency indicated by the obliteration of the convolutions and its increased weight. The weight was 1,580 g.
"The microscopic examination was made according to the methods of Nissl, Alzheimer, and Spielmeyer, with alcohol-formalin specimens.
"In the Nissl preparation distinct changes of the nerve cells were seen in the cortex of the frontal and temporal lobes; less in the central region and in the occipital lobes, mostly however in the hippocampus major. Especially changed were the medium-sized pyramidals of the third and the deep fifth, not so completely those of the sixth Brodmann stratum. The prevailing characteristics of this disease of the cells were chiefly inflation of the cell body and granular degeneration of that portion stained by Nissl's method (Nissl bodies). The protoplasm around the nucleus was lighter than the marginal protoplasm, the nucleus pale and swollen; the nucleolus peripherally situated, vacuolated and metachromatic. The loss of color of the cells seemed to spread peripherally. In some elements a fine honeycomb structure was seen; also small annular structures and a fibro-granular degeneration. From this, various intermediate forms progressed to pale, shrunken, shadowy structures, still showing traces of granulation. The apophyses—especially of the extremities—were frequently swollen in the enlarged cells, the unstained tracts more or less stained. Thus they seemed to degenerate quickly. Sometimes they looked as if torn front the cell body. The pericellular neuroglial cells had nuclei which stained well, and some partly enlarged protoplasmic bodies of fine reticular structure, containing metachromatic granules. Figures of segmentation were not found. The process in the nervous elements seemed to have exercised only slight irritation upon the forms of glia cells undergoing decomposition. Also the degeneration of nerve cells, causing formation of small empty spaces, could produce marked substitution—proliferation of the glia. There were centres of degeneration already formed or in process of formation (see Ill. 1)» It seemed, indeed, that in the hilum of the hippocampus major, as appeared in the Cajal preparation, an increase of the protoplasm-infiltrated astrocytes occurred, for numerous forms of quadriga and very large elements with many apophyses were found there. Further, a thickening and condensation of the marginal fibrous tissue in the cortex and in the hippocampus major was noted. In the striatum (C. and O. Vogt), especially in the ventromedial parts of the caudate nucleus, the small nerve cells were slightly swollen, and almost all had faded. The cell body was of reticular, granular structure, the apophyses almost invisible, the unstained tracts still unstained. Numerous elements were apparent only as shadows. .The pericellular cells contained fine and large granules of bluish green and golden yellow color, although in the ganglion cells belonging to them no vacuolization, or fatty degeneration, or deposit of pigment could be found. There were Hortega cells, partly filled with pigment. With the iron dye (Turnbull's method) these grains or layers of pigment were slightly blue in color, their margin was more deeply colored, sometimes the nucleus was of dark blue. Also in the cells of the vessel walls of this region siderophile pigments were accumulated. They stained only partly with scarlet. The oligodendroglia cells contained one or several siderophile globules. Numerous concretions of pseudo-calcium were found in the region of the whole striatum. The cells of the nucleus dentatus in the cerebellum were much enlarged; they were pale and contained rather abundant pigment of greenish blue color. In some glia cells of the Hortega type a great accumulation of coarser grains of pigment was seen. In the neighboring vessels the adventitia cells had likewise stored considerable pigment, but this did not give the reaction to iron. The cells of the pallidum, the substantia nigra, the locus coeruleus, the nucleus of the pons Varolii, and the cortex cerebelli, however, had changed but little. But concretions of pseudo-calcium, large and small grains of pigment, seemed to have increased in the glia and in the vessels. Signs of marked degeneration were seen in the ganglia about the third ventricle (nucleus para-ventricularis, nuclei tuberis, ganglion supraopticum) in which enlargement of cells, and further shadowy forms, were found. In the more ventral parts on both sides of the nuclei dorsales vagi no visible changes could be noted, but the cell accumulations nearer to the floor of the fourth ventricle contained remaining faded elements, shadowy, or broken into fragments. Contrary to the above described marked transformations, the motor and sensory nuclei of cerebral nerves were almost intact. Their cells had good chromatin marks and were of regular form and size. The nerve cells of the spinal cord were also in good condition; unfortunately only portions of the cervical spinal cord could be examined. An exception must be made for the oculomotor nucleus, which showed numerous greatly enlarged elements.
"In the vessels, evidence of a thickening of their walls was generally lacking. Only in the inter- and midbrain two veins thickly surrounded by lymphocytes were found. Moreover, the endothelium nuclei were slightly vesicular, the protoplasm of the endothelial cells was finely reticular in structure. But in many subependymal cortical vessels, and in those vessels passing the plexus (pre-capillaries and veins) some adventitia cells showed large vacuoles.
"The most marked changes were seen in Herxheimer preparations. Here a marked fatty degeneration of all cortical elements was noted, both of the nerve, glia, and mesodermal cells. The ganglion cells were filled with little fat globules, spread over the whole body of the cell, or limited to its lateral parts, its base and its end apophysis. In the hippocampus major (Ill. 2) " where the fatty degeneration was extreme, there were also large fat globules in the nerve cells; and the cell apophyses, especially the end apophyses, were noted as wide bands filled with fat. The pericellular cells likewise contained fat globules. They were thickly clustered in the whole cell body, and diminished only very slightly towards the margin of the cell. In the glia elements with large and pale nuclei, however, the distribution of the fat was seen in fine rays, or in the form of garlands, free, and beginning only at a certain distance from the nucleus. In the epithelial glia cells, the oligodendroglia—so-called by Hortega—generally a single fat globule of medium size was found.
"In the cells of the walls of the vessels we must distinguish two forms of fat accumulation. First, they were filled with a fine, powder-like fat in the protoplasm of the endothelium, so that the walls of the vessels appeared in the preparation as fine red lines; then an accumulation of fine and coarse fat droplets in the adventitia cells, partly transformed into granular cells. While both were found in the gray matter, the greater fatty accumulation was found in the medulla, where, moreover, fatty layers of pigment appeared near the bright red fat globules. The fatty degeneration was most marked in the hippocampus major, in all its portions, also in the small cells. Often there were only globules of fat, without nuclei, where nerve elements would be expected. In the frontal and temporal lobes likewise a diffuse, although in general not so marked, fatty degeneration could be noted, while in the central region only the small and medium-sized elements showed an accumulation of fat, and the Betz cells contained only a few small droplets. In the most infiltrated elements it sometimes happened that the nucleus was displaced and granular cells were formed.
"Special attention was paid to the plexus choroideus. In the Nissl preparation fine ependymal cells showed a marked enlargement, chromophilia of the outer region of the cell body, with the margin of the cell separating into fibres, infiltration of basophile, metachromatic grains and fragments, vacuolization and shrinking, and hypergliomatosis of the nucleus. In the preparation numerous, mostly large, fat drops were seen. Often all ependymal cells contained a villus of fat (Ill. 3) 4°
"Examining the foregoing, we see different kinds of histopathological changes, three of which are to be emphasized. The whole process is to be looked at as non-inflammatory. This opinion cannot be influenced by the few infiltrated vessels in the midbrain and interbrain. The simplest explanation is to attribute them to the terminal pneumonia. Weimann likewise has noted a slight infiltration of lymphocytes in cases of morphin poisoning. The question, whether they may have a closer relation to the intoxication, cannot be definitely denied for the present; therefore I content myself with mentioning it, refraining from more or less poorly grounded assumptions.
"Among the changes of the nervous parenchyma the most astonishing and remarkable one is the marked fatty degeneration, found especially in the elements of the third cortical layer and in all cells of the hippocampus major. It is not limited to the nervous elements, but exists also in the glia and in the endothelium of the vessels. It is distributed in fine droplets in the protoplasm. Larger drops are found in Hortega cells and in some nerve cells. In the astrocytes less frequently slightly larger globules of fat are seen. There are, however, large globules and strata of fat in the adventitia cells of the vessels.
"The question whether we have here a case of acute fatty degeneration or a chronic fat accumulation is not easy to answer. The slight reaction on the part of the Hortega cells perhaps may be assumed to indicate a very recent process. But there seems to be no valid proof that this reaction had not enough time for development in the two days following the acute poisoning. We see on the one hand that the Hortega cells can proliferate exceedingly early, if there are severe morbid transformations in the nerve cells; and on the other, they are not so much affected by the fatty degeneration of the nerve cells as they are by processes, in which a proteoid decay of the protoplasm prevails. But that in this case there was already a removal of fat, is undoubted. Not only the accumulation of large fat globules in the adventitia cells of the vessels, but especially the fatty, ferruginous pigments in Hortega cells and elements of the walls of the vessels found in the cortex, in the striatum, and in the dentatum, point to the fact that decomposition products have been deposited for a long time. The observations of other authors should not be considered as direct contradictions to this assumption. Unfortunately they are not typical enough, being taken from mixed cases (Husemann). I had, however, an opportunity to discuss more carefully the findings of the Spielmeyer case of acute morphin poisoning with Dr. Weimann. Compared with my case, there was undoubtedly a slighter degree of fatty degeneration. On the other hand, Dr. Weimann told me of a case of more severe morphin addiction, that did not die from an acute poisoning with morphin or other poisons; in this case the fatty degeneration was still more marked than in the one here described, Dr. Weimann said. In view of this report—Dr. Weimann has seen my preparations—I think that the case under consideration can be classified between the two cases cited, and I should like to say—with all reservations necessary in all single observations—that in this case the fatty degeneration is the result of the chronic poisoning. That these are chronic changes is apparent also from the older losses of nervous tissue in places. Besides this, the ferruginous pigments, appearing abundantly especially in the striatum, are a distinct sign of an injury—although not too severe—of this nuclear region, which has existed for a long time.
"As acute changes I would first regard the atrophy of the nerve cells in the cortex and in the dorsal vagus nucleus. They seem to be a consequence of the fatal morphia poisoning. This agrees with the results of Nissl, who, in his animal experiments, saw no fatty degeneration after maximal acute poisoning, but only proteoid degeneration of the nerve cells.
"In the treatment of morphin addiction the findings in the case of K. seem to be of significance showing remarkable morphologic injuries of the nervous system. At first we see that neither the nuclear regions nor the lower centres of coordination, but only the younger portions of the brain, and in them especially the gray regions, are most affected, i.e., the cortex, the striatum, and the dentatum. Within the cortex the third layer seems to be most affected. Its elements show a fatty degeneration, and we see the degeneration of nerve cells, which can lead and has led to strictly localized loss of functioning tissue. In the striatum likewise we see the proof of a remarkable disturbance of metabolism. It would be rather hazardous to evaluate these findings locally. But this much can be said, with due caution, that certain symptoms of morphin abuse indicate the existence of severe affective disturbances; such as the loss of will, the weakened resistance, the depravation. Furthermore, we see even in the case of the withdrawn morphin addict a weakness of judgment in the face of his desire and its consequences. Lastly, we know from Weimann's reports that severe dementia with paralytic-like symptoms may be observed in the case of morphin addicts. But as I said before, we will not go too far. As to my opinion, it is sufficient to state that chronic morphin abuse causes injuries to the nervous system, which can be proved, and in part cannot be cured. These injuries affect just the striatum in its interior parts and the third cortical layer of the frontal and temporal regions of the brain, while the lower parts of the brain seem to be less attacked and become affected only in the case of severe acute poisoning.
"That the hippocampus major shows marked changes may be considered, to a certain extent, as a local symptom, because its place is on the margin of the large liquor filter, the plexus choroideus, and on the bottom of the lateral ventricle, in a `dead corner', as I should say, where the possibility of concentrated action of harmful materials contained in the fluid of tissues and ventricles is especially great.
"The fattening of the plexus endothelium seems to be of importance, considering the observations of Mesbrezal, F. K. Walter, and Hauptmann on the permeability of the limiting membranes between blood vessels and surrounding spaces. Unfortunately I have not, for obvious reasons, had experience in permeability in morphin addicts.
"Once more let it be emphasized that the above case seems to be especially clear, because both the clinical picture and the anatomical findings do not point to any noticeable effect of the veronal taken by the patient, as indicated by the absence of annular bleeding—I refer to Weimann's report dealing in detail with annular bleedings in cases of veronal poisoning.
"Summarizing our findings in the case described above, we can make the following statements:
"1. In eases of morphin abuse the central nervous system is injured, as can be morphologically shown.
"2. The cortex is affected with a fatty degeneration, leading to the loss of nervous tissue.
"3. In the striatum ferruginous decomposition pigment appears in increased quantity.
"4. The plexus choroideus shows a fatty degeneration of its ependymal coating.
"5. The part of the brain most affected by chronic poisoning is the telencephalon.
"6. Acute morphin poisoning chiefly causes pure degenerative changes in the small and medium elements of the cortex, in the nerve cells of the periventricular regions, especially of the vegetative vagus nucleus."
M. Cloetta and E. Brauchli-1926.8°
These authors studied the physicochemical changes in the blood in relation to the calcium and potassium concentrations caused by the administration of narcotics. Their observations in relation to these changes in chronic morphin poisoning in dogs are the following:
"Dog No. 12, which had reacted normally with a diminution in calcium of about eight per cent and a rise in potassium of about twenty-one per cent to a single injection of morphin, received small quantities of morphin subcutaneously every day from the 27th of December, 1924, on, beginning with five milligrams per kilogram. On the 16th day of January, 1925, it had received a total of 1.725 grams of morphin hydrochlorate. On the 17th, twenty-four hours after the last injection of morphin, it was given subcutaneously three centigrams per kilogram (after a preliminary estimation of calcium and potassium) and reacted with a mild restful sleep (experiment 12a). After this the dog was treated up to the 31st of March with small doses of morphin and on that day, again twenty-four injected, following which the blood was tested in the same way as before (experihours after the last injection of morphin, three centigrams per kilogram were ment 12b). During the next three days the dog received no more morphin, in order that its calcium and potassium content might be tested during this period of abstinence also (experiment 12e). The values obtained are collected in Table II.
TABLE II
| Experiment number | Dose per kilogram | Percentage changes of | calcium and potassium | Remarks | ||||
| Ca | K | |||||||
| 12 | Morphin 0.03 gm. | -8 | +21 | Normal | ||||
| 12a | Morphin 0.03 gm. | -5 | -31 | First morphin period | ||||
| 12b | Morphin 0.03 gm. | -4 | -9 | Second morphin period | ||||
| 12c | ..... | 0 | 0 | Abstinence |
"In the same way a tolerance test was carried out with the dog that in Table I, Nos. 17 and 17a, is shown to have reacted normally to somnif en and in a reverse manner to morphin. First the animal was treated for five weeks with small daily doses of morphin up to one centigram per kilogram. The plasma was examined twenty-four hours after the last injection and then the same dose as before was injected, that is two centigrams per kilogram. The animal responded with a quiet restful sleep, whereupon the second blood test was made (experiment 17b). Then the morphin administration was continued three weeks longer, reaching twelve milligrams per kilogram, and at that time another test was made in the same way as before (experiment 17e). Now a period of seven weeks passed by, during which sixteen milligrams per kilogram were injected, and then the test with two centigrams per kilogram was carried out. This no longer caused a condition of distinct somnolence and the animal remained awake, but the sensitiveness to pain was perceptibly diminished (experiment 17d). Then administration of morphin was stopped entirely and three days later, during the abstinence period, a blood test was made once more (experiment 17e). The results are collected in Table III.
TABLE III
| Experiment number | Dose per kilogram | Percentage changes of |
|
Remarks | ||
| Ca | K | |||||
| 17a | Morphin 0.02 gm. | +9 | -33 | Normal | ||
| 17b | Morphin 0.02 gm. | -7 | -11 | First morphin period | ||
| 17c | Morphin 0.02 gm. | -5 | +11 | Second morphin period | ||
| 17d | Morphin 0.02 gm. | -5 | +16 | Third morphine period | ||
| 17e | .... |
+5 | -18 | Abstinence |
"The tests indicated that in dog No. 12 chronic use of morphin did not affect the customary reaction of calcium to a fresh injection, a reduction in calcium always resulting as in a fresh animal. On the contrary, the derangement of potassium relation underwent an alteration on morphinization. The fresh animal had reacted with an increase of about twenty-one per cent to the first morphin injection, while habituation caused the first time a decrease of thirty-one per cent, the second time of nine per cent to an injection of three centigrams per kilogram. The second dog originally reacted to injection of morphin by a calcium increase and a potassium diminution. During morphinization each renewed injection of morphin caused a reduction of calcium, while the reduction of potassium was small at first and then became reversed. During periods of abstinence, too, the animals display different behavior. Dog No. 12 shows in both tests scarcely any change since the time of the last injection, and dog No. 17 an increase of calcium and an increase of potassium.
"On considering the alterations taking place in the two animals during habituation and abstinence as to absolute amounts in comparison with the normal, the following figures represent the calcium and potassium in a cubic centimetre of blood expressed in milligrams per cubic centimetre of plasma.
TABLE IV
Dog Normal Conclusion of Abstinence
number habituation
Ca K Ca K Ca K
12 0.093 0.812 0.099 0.73 0.105 0.800
17 0.081 1.120 0.086 0.73 0.095 0.526
"Both animals display a tendency to a higher calcium content and a lower potassium content because of habitual use of morphin, so that dog No. 17 only reached half the original amount of potassium during the period of abstinence. But here again the alterations are quite dissimilar in the two animals, so that the irregularity observed on a single injection in different animals is repeated in morphin habituation.
"SUMMARY
"Administration of hypnotics of the aliphatic series always produces in dogs, in addition to somnolence, a diminution of calcium and an increase of potassium in the blood plasma, while the amount of sodium remains unchanged: there occurs besides a wholly unimportant reduction in surface tension.
"This regularity of occurrence ceases when morphin is injected, since in about half the animals an increase of calcium and a diminution of potassium took place, while in the other half the changes resembled the action of the hypnotic. Only in two cases were both the calcium and the potassium diminished. The sodium underwent no alteration in amount. The surface tension was depressed to a very small extent only, as with hypnotics.
"In chronic users of morphin as well there was no regularity in the derangement of calcium and potassium.
"These results demonstrate that in regard to the effects of hypnotics we are dealing with a very uniform influence of the organic ions, clue to the invariable effect of these substances in partially paralyzing the brain, while morphin produces a very complex effect, variable in different individuals, which combines paralysis and excitation and central as well as peripheral action, and the alterations in the ions are correspondingly totally irregular and individually variable. In consequence, the chief differences in the pharmacological action of the two groups are very clearly defined. We perceive, therefore, in the regular ionic changes produced by hypnotics an organic reaction which has a genetic connection with the causation of sleep."
Kyusaburo Sato-1927.81
The author abstracts the results of studies on the metabolism of animals during chronic morphin intoxication as follows:
"In chronic human morphinism the body metabolism is increased only at the period of morphin hunger. In the opinion of a number of authors this is probably due to hyperfunction of the thyroid.
"As an addendum to studies of chronic morphinism in human beings, the author made experiments to determine the catalase content of the blood of chronic morphinists and of experimentally intoxicated animals.
"The results are as follows:
"(1) The catalase content of the blood of healthy individuals amounts on an average to 8.8 in males, 7.6 in females. The hemoglobin catalase index is 88 in males and 86 in females, according to Nakanishi.
"(2) The catalase content of the blood in chronic morphinism shows no striking difference between the action time and the hunger time of morphin. However, the values are on the whole somewhat lower than in healthy individuals.
"(3) In experimental chronic intoxication of rabbits, the catalase content as well as the hemoglobin index of the blood is always lowered.
"(4) But in acute intoxication this value is, on the contrary, somewhat increased."
Yutaka Teruuchi and Sotaro Kai-1927.82
These authors sought to determine the fate of morphin in the body in both acute and chronic poisoning. They decided, after reviewing the work of others, that the fate of morphin injected into an animal suffering from morphinism only can be explained by determining the amounts of morphin stored in the tissues and the total amounts excreted from the body taken in connection with the total amount of
morphin injected during the entire period of immunization. They state:
"By investigating all the above-mentioned factors, we have learned that in morphinism the rabbit has, unlike the normal animal, a remarkably strong power to destroy morphin and also the fact that the rabbit in morphinism has a marked power to retain and absorb by 'far a larger amount of morphin in its muscle tissues."
They administered to a rabbit, during a period of 32 days in increasing doses, a total of 4.7 gm. of morphin hydrochloride. The following table gives the materials examined, the amounts of drug recorded and the percentages of drug administered found:
TABLE VIII
Materials Found morphin, Percent of mor- Total percent
pure phin administered recoveries
found
Whole urine 0.3014 8.34
Whole feces 0.1124 3.11
Blood 70 cc 0.0050 0.13
Intestinal contents 0.0200 0.55
Intestines
Stomach contents 0.0220 0.60
Stomach 16.36
Whole muscles 0.1300 3.59
Liver
Kidneys
Lungs 0.0015 0.004
Heart
Whole
"From Table VIII it will be seen that morphin in acute intoxication was recovered up to 90 per cent, but in the chronic morphinism, only 16.36 per cent of the total amount of the injected morphin could be recovered. Thus it will be seen that the largest portion of morphin had disappeared, which could not, we believe, be due to the experimental error or loss. If the percentage of the recovered morphin had amounted to 70-80 per cent, the difference might be explained as due either to experimental loss or to error, arising from the fact that the experiment covered a long period of time, but only 16.36 per cent of the total amount was too small for that, but might rather be considered to be the results of the destruction in vivo."
Their résumé and conclusions derived from their findings in the morphinized animal are as follows:
"10. In chronic morphinism, morphin is gradually destroyed in the body, and therefore the animal body gradually acquires a tolerance to it.
"11. In chronic morphinism, the muscle contents of morphin increase markedly while on the other hand the viscera become almost free from it.
"12. In chronic morphinism the morphin content of the blood is found to be larger than that of an equal volume of blood in acute cases.
"13. In chronic morphinism the estimation of the percentage of the morphin contents of the whole body against the amount injected for the last time is meaningless, because we have reason to believe that some of the amount injected before the last might be present in the contents of the stomach and intestine, and the muscle tissues.
"14. In chronic morphinism, the excretion of morphin which has been taking place during the process of time until the development of the chronic intoxication phenomena, chiefly has occurred through the kidneys, and we found that the morphin contents of the urine were by far higher than those of the feces.
"15. In chronic morphinism the protection of the living organism against that poison consisted in the fact that a large amount of morphin which had been introduced once into the body is reserved in the muscles, while on the other hand the destruction takes place in the body and also excretion occurs through the kidneys and stomach.
"16. From the above résumé, we venture to conclude that morphinism is due to the acquired power of the living organism to destroy morphin and to excrete it., besides the augmented power to reserve it in large amount by the muscles, so that even though a large amount of it should be introduced into the body all at once, it can be prevented from immediately attacking the central nervous system."
I. H. Pierce and O. H. Plant-1928.83 84
In the second of a series of articles dealing with studies in chronic morphin poisoning in dogs, the authors report findings resulting from studies of blood cells and hemoglobin in dogs during addiction to morphin and during withdrawal. They state:
"It seemed worth while to study the blood cells and hemoglobin in dogs during chronic morphine poisoning and withdrawal for two reasons: (a) the pathology of chronic morphine poisoning is not understood and therefore data on any demonstrable pathologic change is of value and may ultimately aid in finding the fundamental alterations that make it a disease; in spite of the fact that a large majority of those who have worked on the morphine problem believe that morphine addiction is a true disease, the question will always be raised as to its being such, until the fundamental changes that underlie it are thoroughly understood. (b) Since dogs seem to be very suitable test objects for studying experimentally many phases of chronic morphine poisoning, comparison of data obtained on them with similar data from human subjects adds to the value of all observations made on these animals.
"We have made counts of red and white cells and have estimated hemoglobin content throughout addiction and during withdrawal in 16 experiments on 12 dogs (12 first addictions and 4 second addictions). In addition to the above, similar studies were made on three dogs that died, two during addiction and one on the third day of withdrawal. Differential leucocyte counts were made throughout 8 of the above experiments. The general treatment of these animals and data concerning weight, food, dosage, behavior and symptoms are given in the paper which precedes this one."
The observations were begun from two to four weeks before addiction started and examinations of blood were made once a week during this period and during addiction. During withdrawal daily examinations were made and as withdrawal progressed from two to seven days elapsed between examinations. Blood samples were taken in the morning before the administration of morphin. The usual counting chamber for red and white cells was used, and the Dare hemoglobinometer for estimating hemoglobin. Wright's stain was used in making differential leucocyte counts. Cases in which intercurrent infections occurred were eliminated.
The following figure shows dosage, weight, hemoglobin and red and white cells during addiction, and withdrawal in dog 8, a typical case. The authors summarize as follow:
"Studies of red and white cells and hemoglobin were made on sixteen dogs during addiction to morphine and after sudden withdrawal; differential counts of white cells were made on 8 dogs.
"Red blood cells are normally more numerous in dog's blood than in human blood; during addiction to morphine the number of red cells is not materially altered; following abrupt withdrawal the number is decreased.
"White blood cells are normally more numerous in dog's blood than in human blood; during addiction neither the number nor the relative amounts of the various forms of white cells show any consistent change; during withdrawal there is a marked leucocytosis and during the leucocytosis the percentage of polynuclear neutrophiles is increased.
"The hemoglobin content of dog's blood is not altered during addiction to morphine; during withdrawal the hemoglobin is usually decreased, the fall being parallel to the decrease in red cells."
In the third article, dealing with their studies of morphin intoxication and withdrawal in dogs, the authors give the following as their objects:
"(a) It was shown by Ross, 1918, that single doses of morphine produce hyperglycemia in dogs, and Luzzato, 1905, demonstrated that the acute effects of morphine are accompanied by glycosuria. Because of the well established relationship between liver function and blood sugar, we hoped to obtain at least presumptive evidence as to whether or not the liver developed tolerance to morphine, by following the variations in blood sugar throughout continued administration of the drug and during withdrawal. That some functions affected by morphine do not develop tolerance during prolonged administration was shown by van
FI Quet . T.
Egmond, 1911, with regard to the vagus control of the heart and by Plant and Miller, 1926, in connection with the effects on muscular activity of the small intestine.
"(b) The second object was to determine whether or not a condition of hypoglycemia exists during withdrawal. Some of the withdrawal symptoms in man suggest this possibility. Also, in an experiment on a dog in this laboratory, in which a moderate degree of tolerance was developed, some of the symptoms during withdrawal, especially the marked muscular weakness and tremor, seemed to indicate that hypoglycemia might be a factor in producing them.
"Our animals were all females, of many different breeds, and varied in weight from 5.5 to 18 kgm. They were fed on a uniform diet of raw pig hearts and dog biscuit, with liver and bone meal once a week. The animals were kept in clean, well ventilated kennels, with a daily period of exercise in an outside runway. Each dog received a weekly bath with cresol soap and before the experiment started was given powdered areca nut to get rid of intestinal parasites.
"Several normal animals were kept in the same environment and received the same general treatment as the addicted dogs. Regular blood sugar estimations on these animals served as general controls.
"All of the addicted dogs were kept in the environment and under conditions that prevailed during the experiment for periods of 3 to 6 weeks before the administration of the drug was begun. Blood sugar estimations during this period served as controls for the individual animals. Most of our animals were addicted slowly and administration of the drug was continued over a long period... . The initial dose was 5 or 10 mgm. of morphine sulphate per kgm. This dose was continued until vomiting no longer occurred after the injection and the animal was again taking enough food either to maintain its weight or to regain some of the initial loss; this required from 2 to 4 weeks. Subsequent increments in dosage were governed largely by the dog's general condition as indicated by the weight curve. If the animal was maintaining its weight the dose wits increased at intervals of one to three weeks, if losing weight the intervals were longer-3 to 5 weeks, and if the loss in weight continued the dose was reduced. By following this plan we were able to maintain the animals in good condition throughout the experiments and thus avoid marked changes in blood sugar due to poor nutrition. Figures giving the average weight of each animal during control period and during the first and second halves of addiction are shown in tables I and II, and a typical weight curve is shown in figure I."
The authors continue:
"Two types of blood sugar curves were studied during addiction: (a) the general blood sugar level as shown by weekly examinations throughout the period of continued administration; these estimations were invariably made just before the dose was injected and represent, therefore, the low point in the blood sugar in so far as the effect of morphine is concerned. (b) At frequent intervals during addiction the immediate rise in blood sugar following the injection was studied in detail by taking samples of blood at intervals of 1% to 2 hours during the day. The purpose of making these detailed studies of the rise in blood sugar that follows immediately after the injection was to ascertain whether this rise continued as tolerance developed, that is, whether the liver, or whatever mechanism is responsible for the rise, develops tolerance to morphine.
"During withdrawal the general level of blood sugar was determined at first by daily examinations; as the animal recovered from the immediate effects of withdrawal, blood sugar estimations were made at longer intervals. (3 to 7 days). Withdrawal was abrupt."
After recording in detail their observations during different periods of addiction and withdrawal, the authors comment and summarize as follows:
"COMMENT
"We believe that the rise in the general level of blood sugar during the first half of a long addiction is a direct effect of morphine and is not dependent on the effect of diminished food intake as evidenced by the loss in weight during this period, because (a) it has been shown that during starvation the blood sugar falls steadily until a greater percentage of the body weight is lost than ever occurred in our dogs, and (b) this rise in blood sugar lasted longer than the period during which the animals were losing weight. The resumption of a normal and in sonic cases a lower blood sugar level during the second half of a long addiction is therefore an evidence of the development of more complete tolerance by the sugar regulating mechanism.
"The results of our experiments indicate that the hyperglycemia which occurs immediately after the injection of morphine in a non-tolerant dog is not dependent upon the fall in body temperature, because it disappears during addiction at a time when the fall in temperature still occurs after each dose. It is not due to the narcosis and the consequent decrease in muscular activity because it disappears at a time when the animals still remain very quiet after the injection even though they do not sleep soundly.
"We believe that the disappearance during addiction of the hyperglycemia which occurs immediately after the injection is presumptive evidence of the development of tolerance by the liver, because (a) of all the factors concerned in blood sugar regulation the liver is the most important, cf., Macleod, and as addiction proceeds the blood sugar approaches more and more closely a constant level; (b) there is no question but that the narcosis is dependent on the action of morphine on the central nervous system, and the experiments of Gottlieb furnish strong evidence that the fall in temperature is due to the effect of the drug on the central heat controlling mechanism. The hyperglycemia disappears during tolerance much more rapidly than either the narcosis or the fall in temperature, and further, it reappears more rapidly than either of these effects when the drug is withheld temporarily during addiction.
"SUMMARY
"During the first half of a long addiction to morphine the general level of blood sugar, as shown by estimations made before the injection of the daily dose, is somewhat higher than during the control period before addiction started. During the second half of a long addiction the general level of blood sugar is lower than during the first half and either approaches or is slightly below the normal level.
"The hyperglycemia that occurs immediately after the injection of morphine in a normal dog, rapidly disappears during addiction. The fall in temperature that occurs simultaneously with the hyperglycemia decreases very slowly and does not entirely disappear during addiction.
"When the drug is withheld for two to four days during addiction, the hyperglycemia recurs to approximately the same degree as after the first dose, when administration is resumed ; the fall in temperature is not as great proportionately as the hyperglycemia.
"The blood sugar curve shows a distinct increase during the first week of withdrawal. Later in withdrawal, after withdrawal symptoms have subsided, the blood sugar curve falls somewhat below normal, in some cases."
1 Calkins, A.—Opium and the Opium Appetite. 1871.
2 Kane, H. H.—Opium Smoking in America and China. 1882.
3 Jouet, Daniel—Etude stir le morphinisme chronique. These de Paris. 1883.
4 von Tschisch, W.—Ueber Veriinderungen des Riickenmarkes bei Vergiftung mit Morphium, Atropin, Silbernitrat and Kaliumbromid. Virchow's Archiv. 1885. Vol. 100. pp. 147-176.
5 Ball, B.—Des lesions de la morphinomanie, et de la presence de la morphine dans les visceres. Encephale. 1887.
6 We are led to speculate here as to whether such storage of the drug may not explain the recurrence of certain symptoms which are produced both by the abuse of morphin and abstinence. If these findings are correct and morphin is still stored in the liver for days or weeks after withdrawal, one may question the completeness of so-called "cures" that release their patients after a few days' treatment. Herein may possibly rest the explanation of some of the early relapses following certain routine institutional treatments. The relationship of such possible storage of morphin to the mode of treatment pursued, the length of intoxication, the activity of elimination, the general status of the patient, and to what Sollier calls the "eliminatory crises" are all problems in need of solution, which quite conceivably may have an important bearing on treatment, prognosis, and the prevention of relapse.
7 Pilliet—Note sur les Lesions histologiques de 'Intoxication morphinique subaigue. Comp. rend. Soc. de Biol. 1887. 8s. IV. p. 566-588.
8 Saratschow—Ueber die Veranderungen in den Nervenelementen des Centralnervensystems bei der Morphiumvergiftung. Abstract from Neurol. Centralbl. 1895. Vol. 14. pp. 366-367.
9 Wilson, J. C. and A. A. Eshner—American Textbook of Applied Therapeutics. 1896.
10 Nissl, F.—Die Hypothese der specifischen Nervenzellenfunction. Allg. Ztschr. f. Psychiatrie. 1897-1898. Vol. 54. pp. 1-29. Also Beitriige zur Anatomie and Histopathologie der Nervenzellen mit besonderer Berficksichtigung der pathologischen Zellveriinderungen nach experimentell erzeugten Vergiftungen. All. Ztschr. f. Psychiat., 1897-1898. Vol. 54. pp. 29-107.
11 " Ewing, J.—Studies on ganglion cells. Arch. of Neurology and Psychopath. 1898. Vol. I. No. 3. pp. 263-440.
12" Jacottet, G.—Etude sur les alterations des cellules nerveuses de la moelle et des ganglions spinaux dans quelques intoxications experirnentales. Ziegler's Beitr. 1898. Vol. 22, Part 3.
13" Barbacci, Ottone.—Die Nervenzelle in ihren anatomischen, physiologischen and pathologischen Beziehungen nach den neuesten Untersuchungen. Centralbl. f. alig. Path. u. Path. Anat.., 1899. Vol. 10. pp. 757-823; 865-936.
14 Fuller, S. C.—A Phenomenon Observed in the Blood of Morphinomaniacs. New Eng. Med. Gaz. 1899. Vol. XXXIV. No. 6. p. 241-250.
15 Lancelin, L. E. R.—Morphinisme et Infections. Role des Leucocytes. These de Bordeaux. 1902.
16 In 1898 Cantacuzene in attempting to demonstrate that cholera vibrios were destroyed by the white cells rather than by the serum, narcotized laboratory animals with tincture of opium in order to eliminate the action of the white cells. In these experiments, he showed that the narcotic had a distinctly paralyzing effect upon the white cells, which lasted about 5 hours.
17 In Lancelin's experiments it is assumed that an animal which has been given morphin for one month is typical in his reactions to an average case of chronic morphin using, but this would appear to be open to question. The author does not state the degree of tolerance attained by the animals he uses, but one would scarcely expect a, high degree of tolerance to be established in four weeks, certainly not such as is witnessed in human beings after years of administration. It is quite conceivable, therefore, that his "chronically intoxicated" animals were not typical in their reactions and that in their apparent lack of resistance to infections they did not represent fairly the chronic user in whom years of administration have induced possibly a different "balance" to the drug.
18 Krafft-Ebing, R.--Textbook on Insanity. 1904.
19 Luzzato, R.—Uber die Natur und die Ursachen der Morphinglykosurie Arch. f. exper. Path. u. Pharmakol. Leipz. 1905. LII. 95-106.
20 Paton, S.—Psychiatry. 1905.
21 Allbutt, T. C.—A System of Medicine. 1905.
22 Chotzen, F.—Zur Kenntnis der Psychosen der Morphitimabstinenz. Allg. Zeitschr. f. Psychiatrie. u. psych: gerichtl. Med. 63. 1906. p. 786-803.
23 Schutz, Otto—Anatomische Befunde an Rfickenmark and Nerven bei einer Morphinistin. Neurol. Centralbl. 1908. Vol. 27. pp. 157-159.
24 Shoemaker, J. V.—Materia Medica and Therapeutics. 1908.
25 Achard, Benard and Gagncux—Action de la morphine sur les proprietes leucocytaires. Bull. et Mem. Soc. med. Hopitaux de Paris. 1909. Vol. 28. Ser. 3.
26 Jennings, 0.—The Morphia Habit. 1909.
27 Chartier et D. Morat.—Les Variations de la Formule sanguine chez les Morphinomanes et les Héroinomanes au cours de la désintoxication rapide par la Méthod de Sollier. Compt. rend. de la Soc. de Biologie. June 25, 1909.
28 Case, C. L.—The Pathology and Treatment of the Morphine Habit. Med. Council. 1910, XV, 307-311.
29Krlipelin, E.—Psychiatrie: Ein Lehrbuch für Studierende und Ârzte. 8th ed. 1909-1915. Vol. 2. Klinische Psychiatrie. p. 206-228.
30 Morat, D.—Le sang et les sécrétions au cours de la morphinomanie et de la désintoxication. Thèse de Paris. 1911.
31 Vaquez, H.—Des methodes propres a evaluer la resistance des globules du sang. Comptes rendus de la Societe de Biologie, 5 fevrier, 1898, p. 159. Semaine Medicate, 1898, p. 611.
32 Ch. Achard et Ramond—Recherche de la resistance leucocytaire. Comptes rendus de la Soc. de biologie. 16 janvier, 1909, p. 110, et Semaine medicale, 1909, p. 47.
33 As a digression it is interesting to point out that this is suggestive possibly of incomplete elimination, i.e., morphin storage, and may account for the so-called "post-withdrawal" symptoms mentioned by some authors, who claim that mild withdrawal symptoms persist for weeks or months after stoppage of the drug and eventually lead to relapse. In this connection it would be of interest to determine the leukocytic changes under different methods of treatment and detoxication.
34 Feullié. Leucopathies, métastases, albuminurie et ictères leucopathiques. Thèse de Paris. 1909.
35 Loc. cit.
36 We would point out here that if Morat's explanations of the functional and organic changes he describes are correct, they would clarify certain reported phenomena and stimulate very interesting speculations as to others. The return of the leukocytes to normal and the eliminatory crises he describes should be valuable in guiding treatment and in determining when the patient may be expected to be released from constant observation. All of Morat's work might be profitably repeated and in some directions amplified. If his observations are correct, they would indicate the inadequacy of too brief treatments and of certain other commonly employed therapeutic procedures.
37 Bell, F. McK.—Morphinism and morphinomania. N.Y. M.J. 1911. XCIII. pp. 680-682.
38 Van Egmond, A. A.—über die Wirkung des Morphine auf das Herz (zugleich ein Beitrag zur Frage der Morphingewôhnung). Arch. f. exp. Path. u. Pharm. 1911. Vol. 65. pp. 197-213.
39 Schneider, K.—Zur Frage der chronischen Morphinpsychose und des Zusammenhangs von Sinnestauschungen und Wahnideen. Ztschr. f. d. ges. Neurol. u. Psychiat. Originalen. 19, 1913. p. 25-42.
40 "Pettey, G. E.—Narcotic drug diseases and allied ailments. Tenn. J. A. Davis Co. 1913.
41 "Reach, F.—Zur Kenntnis der chronischen Morphinwirkung. Ztschr. f. exper. Path. u. Therap. 1914. Vol. 16. p. 321-326.
42 Dominick, H.—Uber Morphiumentziehung und die ihrem Verlauf vorkommenden Psychosen. Inaug. Dissert. Kiel, 1914. (We were unable to secure the original dissertation. The above quotation is a translation of an abstract by K. Boas in Neur. Centralblatt. 1915. Vol. 34. p. 943.)
43 Van Dongen, K.—Beitrage zur Frage der Morphingewühnung. Arch. f. Physiologie. 1915. Vol. 162. p. 54-66.
44 Biberfeld, J.—Liber die Mengenverhaitnisse der Hirnlipoide morphingewôhnter Hunde. Biochem. Ztschr. 1915. Vol. 70. pp. 158-163.
45 Beates, Henry, Jr.—A brief Consideration of some mental characteristics of the Narcotic Habitué and a Suggestion for a Feature in Management. Interstate Med. Jour. 1916. 23. pp. 437-444.
46 Dana, C. L.—Problems of Drug Addiction. Med. Rec. Feb. 2, 1918.
47 "White, W. Hale—Materia Medica; Pharmacy; Pharmacology and Therapeutics. London. 1918.
48 Mackin, M. C.—Morphine addiction. Bull. Iowa Inst. 1919. XXI. pp. 171-176.
49 Buckley, A. C.—Basis of Psychiatry. 1920.
50 Anders, J. M. and J. H. Musser—Practice of Medicine. 1920.
51 " Bishop, E. S.—The Narcotic Drug Problem. 1920.
52 Kogerer, H.—Erfahrungen uber die Hechtsche allergische Reaktion bei Morphinisten. Wien. Med. Wchnschr. 1920. LXX. 1045.
53 " Sandoz, C. E.—Report on Morphinism to the Municipal Court of Boston. Jour. Crim. Law and Criminol. May 1922.
54 Sollier, P.—Récherches sur la viscosité sanguine dans l'intoxication morphinique. Bull de l'Acad. de Med. April 24, 1922. pp. 428-431.
55 Sollier, P. and D. Morat—de l'Épreuve de l'Hémoclasie Digestive chez les Morphinomanes au cours de l'Intoxication et de la Désintoxication. Presse Med. January 10, 1923.
56 A review of the preceding material leads us to speculate as to the advisability of withdrawing morphin from a chronic user during the course of an acute infectious malady, just prior to a surgical procedure or at any time when the individual is likely to be in need of all his ability to resist toxemias or shock. It has been claimed by some that influenza, pneumonia, and certain other infections are not so well withstood by chronic users of opium when the drug has been recently withdrawn as when these cases are permitted to remain on a "balanced ration" until recovery from the intercurrent infection is complete. It is also claimed that for the same reason it is advisable to clear up surgical conditions before the withdrawal of the drug. To do so at least would lessen the psychic tendency to relapse from the pain and depression consequent upon operations or illnesses which may closely follow withdrawal. These would appear to be practical points in the handling of these cases which, because of their possible importance in treatment and prognosis as well as in the prevention of relapse, require further observation and study.
57 Loc. cit.
58 Horiuchi, M.—Ueber die Befunde der Nebenniere ber experimenteller Morphiumvergiftung. Trans. Japan Path. Soc. Tokyo. 1923. Vol. 13, p. 47.
59 Hecht, Adolf F.—Pharmakodynamische Untersuchungen an der lebenden Haut. V. Die Allergie der menschlichen Haut gegeniiber primüren taiften und die Morphinempfindlichkeit nach Morphingebrauch. Ztschr. f. g. exp. Med. 1923. Vol. 38. pp. 123-130.
60 David, E.—Uber Morphinismus. Ztschr. f. d. g. Neurol. u. Psychiat. 1924. Vol. 89. pp. 613-617.
61 Wholey, C. C.—The Mental and Nervous Side of Addiction to Narcotic Drugs. J. A. M. A. Aug. 2, 1924. Vol. 83. pp. 321-324.
62 Schoen, R.—Zur Kennt.nis der Morphinwirkung beim Menschen. II. Mitteilung: Die Verhnderungen des Grundumsatzes und der Einfluss massiger Gew•iihnung auf Grundumsatz, Blutreaktion und Atmung. Arch. f. exp. Path. u. Pharm. 1924. Vol. 102. pp. 205-216.
63 Schoen, R.—Zur Kenntnis der Morphinwirkung beim Menschen. I. Die Veranderungen der Blutreaktion und ihre Beg]eiterseheinungen. Arch. f. exp. Path. u. Pharm. 1924. Vol. 101. pp. 365-382.
64 Legewie, B.—Delirium bein Morphinismus. Zugleich ein Beitrag zur Frage der Morphingewiihnung. Ztschr. f. d. gee. Neurol. u. Psychiat. 1924. Vol. 89 pp. 558-578.
65 Soliman, T.—Studies of chronic intoxications on albino rats. VII. Local anesthetics; morphine group; chloral. Journal of pharm.. and exper. therapeutics. July 1924. Vol. XXIII. No. 6. pp. 449-459.
66 Sollmann, Torald—A manual of pharmacology. 3d ed. 1926.
67 Stern-Piper, L.—Die Senkungsgeschwindigkeit des Blutes bei chronischem Morphinismus und Eukodalismus. Berl. Klin. Wchnschr. 1925. Vol. 4. p. 548.
68 Kolb, Lawrence.—Pleasure and deterioration from narcotic addiction. Journal of Mental Hygiene. Vol. IX. No. 4. Oct., 1925. pp. 699-724.
69 Drug Addiction in Its Relation to Crime, by Lawrence Kolb, M.D. Mental Hygiene. Vol. 4, pp. 74-89, January, 1925.
70 Collins, K. H. and A. L. Tatum.—A conditioned salivary reflex established by chronic morphine pois ming. Amer. Jour. of Phys. Sep. 1925. Vol. 74. No. 1. pp. 14-15.
71 Sysak, N.—Zur Frage der pathologisch-anatomischen Veriinderungen bei akuter und chronischer Morphiumvergiftung. Virchow's Archiv. f. pathol. Anatomie u. Physiologie. 1925. Vol. 254. pp. 163-73.
72 Scarborough, Eleanor M.—The Influence of Thyroid Feeding on Chronic Morphine Poisoning. Journal of Pharmacology and Experimental Therapeutics. Vol. 27. Nos. 5 and 6. June, 1926.
73 Gelma, Eugène and Max Aron—Action comparée de la morphine et de la malonylurée sur le développement des larves d'anoures. Compt. rend. d. séances de la Soc. de biol. July 9, 1926. Vol. 95. p. 696.
74 Nishigishi, S.—Studien liber das Morphinismus. I. Mitteilung. Grtmdumsatz der Morphinisten, Opiumisten und Pantoponscopolaministen. Jour. Oriental Med. 1926. Vol. 5. p. 64. Also Studien über den Morphinismus. 2. Mitteilung. Blutchemie der Morphinisten. Jour. Oriental Med. 1926. Vol. 5. p. 69.
75 Joël, Ernst and Fritz Friinkel —Zur Pathologie der Gewfihnung. II. Mitteilung. aber Gewiihnheit and psychische Geweihnung. Therapie der Gegenwart. February 1926.
76 Joël, Ernst and Ettinger, Alice.—Zur Pathologie der Gewahnung. III. Mitt.eilung. Experimentelle Studien über Morphingewahnung. Archiv. für experimentelle Pathologie und Pharmakologie, 1926, Vol. 115, Nos. 5-6, pp. 334-350.
77 Flury (Flury, Arch. f. experiment. Path. u. Pharmakol. 1914. Bd. 64, p. 105) has pointed out, in connection with his investigations of harmalin, that habituation to convulsant drugs in the narrower sense is much rarer than to narcotics.
78 Ludlum, S.D. and Ellice McDonald—Morphine hunger and the smooth muscle reaction. A study of the habitué. J.A.M.A. March 20, 1926. Vol. 86. p. 835.
79 Figures contained in the original article have not been reproduced here.
80 MacKay, Eaton M. and Lois L. MacKay—Resistance to Morphine in Experimental Uremia. Reprinted from the Proceedings of the Society for Experimental Biology and Medicine. 1926. Vol. 24. p. 129.
81 Miller, G.H. and O.H. Plant—Effect of morphine and some other opium alkaloids on the muscular activity of the alimentary canal. II. Influence of continued administration of morphine and of withdrawal on the contractions of small intestines of dogs. J. of Pharm. and Exp. Therapeutics. Aug. 1926. Vol. 28, No. 2. pp. 241-249.
82 Weimann, W.—Zur pathologischen Anatomie der akuten und chronischen Morphiumvergiftung. Deutsche Ztschr. f.d.ges. gerichtl. Medizin. 1926. Vol. 8. pp. 205-220.
83 The brain alterations in the human cases and in the animals have been presented by me in detail and critically discussed in the Zeitschr.f.d. ges. Neurol.u. Psychiatrie. Here they will, therefore, be only briefly reported and discussed.
84 Creutzfeldt, Hans Gerhard.—Histologischer Befund bei Morphinismus mit Morphium-und Veronalvergiftung. Ztschr. f.d. g. Neurologie u. Psychiatrie. Vol. 101. 1926. pp. 97-108.
85 Cloetta, M., and Brauchli, E.—Der Einfluss des Morphins auf den Ionengehalt des Blutplasmas. Arch. f. exp. Path. u. Pharm. 1926. Vol. 3. pp. 254-262.
86 ' Sato, Kyusaburo.—Ueber den Katalasengehalt des Blutes bei chronischer Morphinvergiftung. J. Orient Med. April, 1927. Vol. 6. p. 50.
87' Teruuchi, Yutaka, and Sotaro Kai.—Fate of morphin in animal body. J. Pharmacol. and Exper. Ther. 1927. Vol. 31. pp. 177-199.
88 Pierce, I. H., and Plant, O. H.—Studies in chronic morphin poisoning in dogs.