| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
6 The Need for Meaningful Community Engagement1
 |
|  |
| 
| Reports - Redefining AIDS in Asia |
Drug Abuse
Communities comprise the glue that holds people together. The key to achieving health in the community is based not only on getting services to the community, but also engaging and empowering them to be the catalysts of change and bearers of success.
—The Global Health Council
Who decides about HIV priorities and who sets the agenda? This question was among the main concerns of the 'new' health promotion principles embodied in the 1996 Ottawa
Charter on Health Promotion, and the subsequent Jakarta Declaration. Rather than regarding communities as passive beneficiaries of services, these principles recognise that 'people are able to think and act constructively in identifying and solving their own problems'.2
RESPONSES OFTEN BEGIN AT THE COMMUNITY LEVEL
In many countries, organized responses to AIDS have begun at the community level, and have been driven by the efforts of people living with AIDS, their loved ones and caregivers, and activists. This has also been true in Asia. Crusading journalists in southern India challenged mandatory HIV testing and the detention of sex workers. In Manila, gay men began early peer education and condom distribution projects. Families in China demanded care services for people infected by transfusions of contaminated blood products.
It is now generally accepted that community engagement is an essential part of HIV programme implementation and service delivery. This reflects more than merely a demonstration of an ethical commitment to involve communities in decisions that affect them. This approach acknowledges that the experiences of individuals and communities, especially people living with HIV, are essential in crafting, implementing, and evaluating an effective response.
In the context of Asia's HIV epidemics, the word 'community' usually refers to those people who are infected or affected by HIV, rather than to people living in specific places. This is the usage adopted in this Report. Such communities would include people living with HIV, sex workers, injecting drug users, transgendered people, and men who have sex with men.
In discussing how to involve and support communities, it is important to recognize that not all these people necessarily regard themselves as belonging to a particular 'community'. Some, such as brothel-based sex workers or men who have sex with men, may readily self-identify as sex workers or as gay. But others, such as rural women who occasionally exchange sex for money or food, or men who have sex with men while imprisoned, are unlikely to see themselves as part of such 'communities'.
COMMUNITIES AND COMMUNITY ORGANIZATIONS: HOW THEY DIFFER
In some parts of Asia, the word 'community' is used inter-changeably with community-based organizations and/or non-governmental
organizations. It is also used to refer to members of mass organizations (such as national women's leagues) or activists in social movements (such as HIV treatment activists, or participants in social renewal efforts such as Sri Lanka's Sarvodya Shramadana Movement). In India, the most decentralized governmental structures (the Panchayati Raj Institutions) were explicitly designed to serve the interests of 'communities'.
Although there is no single 'correct' typology of community organizations, it is useful to differentiate people or community members from community-oriented entities. Some institutions are set up and led by a particular community, and they can range from small self-help groups to large trade unions. Others are organized by 'outsiders' to serve, mobilize or even foster a community. They may include community-oriented local Government structures or professional non-governmental organizations involved in public health or development work.
ENGAGING COMMUNITIES IS ESSENTIAL TO STRONG RESPONSES
By signing onto the UN General Assembly Special Session (UNGASS) Declaration on HIV/AIDS, Governments declared a commitment to the participation of civil society in their response to HIV. Unfortunately, involvement of key populations in national HIV responses in Asia remains uneven and in many places is merely tokenistic. Yet the benefits of strong community participation are well-documented.
Community leaders foster trust: Given that HIV is usually transmitted by risky sex or drug injecting practices, it is not surprising that most successful HIV prevention interventions feature strong participation by community members. At its most basic, community participation in the context of HIV programmes is essential for reaching people involved in risky behaviour with information they are likely to trust. Studies in Asia have shown that more than 80 per cent of drug users could be reached within six months with cleaning kits and condoms through the involvement of peer outreach workers. Approaches relying on other types of interventions, such as police, local community leaders, social workers, and medical staff, reached only about one quarter of the drug users.3
Changes in community norms are critical to sustained behaviour change: Community participation is also crucial to understanding and influencing the norms of groups at risk in order to encourage safer practices. Examples include sex workers' efforts to enforce safe sex norms in commercial settings. Community participation of people living with HIV is also important for the provision and use of care and support programmes, reducing stigma, promoting adequate nutrition and palliative care and supporting continuity of treatment.
There is a growing body of empirical evidence showing the benefits of community participation. In a study of over 6,000 female sex workers in the Indian state of Andhra Pradesh, it was found that sex workers who did not participate in a sex worker support group were four times more likely to Report only occasional or inconsistent condom use, compared with colleagues who did belong to such groups. Women who were less able to count on the social support of peers for financial and medical emergencies had a two to three times higher risk of bejng infected with HIV. Similar, though less dramatic, patterns were observed in the same state in a linked study of over 6,000 men who had sex with men.4
It is important to note that stigma, discrimination, gender inequality, violence against sexual minorities, and other social inequities that undermine HIV programmes are also very localized. This underlines the need to engage local communities directly through advocacy, and indirectly through influential institutions such as religious organizations.
Community involvement can open space for discussion about controversial issues: Thereby helping to promote greater understanding of HIV among political and social leaders. Although sex (especially paid sex and sex between men) and drug use are typically treated as taboo subjects, non-governmental and community-based organizations are often willing to broach these sensitive issues publicly. An excellent example has been the advocacy work of the Sonagachi Project of Kolkata, India, which has been important in persuading elected representatives, ministers and party officials to acknowledge the rights of sex workers and to support efforts to improve their working conditions.
Community engagement helps build more realistic and sustainable programmes: Partnerships and community engagement can foster a sense of 'ownership' of the response that is typically absent when projects are externally run. This kind of trust can help ensure that the interventions are more viable, acceptable, and suited to the needs of communities.
Community knowledge can accelerate effective responses: Communities can also contribute to research into HIV risk behaviour and transmission trends. For example, if a narcotic suddenly becomes more expensive due to a reduction in supply, drug users may switch from smoking to injecting the drug, thus increasing the risk of HIV transmission. This information will be known immediately at the community level, but may take time to reach researchers and planners. A study in Southeast Asia cites an example where molecular epidemiology studies and satellite imaging were used by researchers to plot the spread of HIV among injecting drugs users. The same evidence was also available from the drug users themselves who had already described the geographical patterns of drug routes and resultant HIV spread between Myanmar and India.5,6 The sooner new information can be gathered, the sooner programmes can be developed or adapted to address new trends and thémore cost-effective they are likely to be.
Communities and their organizations can quickly adopt new approaches and advocate for them: Community-based organizations are often less bureaucratic than their Government counterparts. Being smaller can give them the flexibility to respond quickly to new situations and adopt new lessons. They can identify important issues that reqiiire swift action, and help muster the activism that might be needed to achieve the desired results. In this way, the AIDS ACCESS Foundation of Thailand, worked with other partners to increase the availability of an important HIV drug, iddr.8 lb do so, they formed alliances, built networks, and drew together a range of expertise in the non-governmental sector.
Communities can help Governments respond effectively: When programmes piloted by community-based organizations prove successful at the local level, Governments can consider scaling them up to the national level. For example, in China, gay and other men who have sex with men set up community hotlines to provide support and information on HIV and other issues. By 2007, the Government had recognized the importance of working with men who have sex with men and was funding programmes aimed at supporting them.
Community-based organizations are often more efficient in service delivery: The involvement of community-based organizations also increases operational efficiency in the delivery of services, since it is in the community's interest to ensure that work is carried out responsibly and effectively. This could be one of the reasons why, according to some studies, Global Fund projects in which the Principal Recipient was not a Government organization tend to show better results than Government-led projects. A study of 148 Global Fund grants found that the grant process for Government Principal Recipients lagged behind that of nongovernmental Principal Recipients by more than three months.9 These findings are supported by evaluations of World Bank HIV programmes, where the efficiency of governmental and non-governmental sub-grant programmes have been compared.19
By involving the affected communities, both Governments and the communities benefit. However, for such involvement to occur, Governments must recognize that effective, sustainable, and appropriate responses to HIV are a shared responsibility. This can only happen if communities are involved in the design of policy, development of strategic and operational plans, and mid-course correction.
Throughout the world, treatment centres collaborate with community-based organizations to enlist people living with HIV as outreach workers, counsellors, adherence support workers, and home-based care providers. In many cases, people living with HIV fill a gap in health care delivery where there are shortages of 'professional' workers. However, it is not unusual for people living with HIV who perform essential services either to work for nothing or to receive a nominal stipend in acknowledgement of their work. Community organizations typically receive minimal funding when they participate in these partnerships. This state of affairs is unsustainable. Formal programmes that actively recruit people living with HIV as employees in relevant areas should be established, and wages reflect the nature of the work performed.
ACCOUNTABILITY IS ESSENTIAL FOR BOTH GOVERNMENT AND COMMUNITIES
Accountability and transparency can be improved by involving community organizations in monitoring and evaluating HIV programmes. Skills training and resources should be available to community organizations in order to facilitate these tasks. Monitoring and evaluation should also gauge the extent and quality of civil society participation and community engagement in national HIV responses. The Coalition of Asia-Pacific Regional HIV/AIDS Networks (The Seven Sisters) has produced a toolkit for carrying out such an evaluation in relation to Universal Access processes, known as The Minimum Standards of Participation of Civil Society in Universal Access'.12
Regional monitoring of national responses can be useful for tracking countries' progress in meeting their various commitments. For example, the International Treatment Preparedness Coalition has released its 4th Missing the 722rget Report, a donor-funded exercise in which community organizations and representatives researched and identified gaps in the provision of treatment at country level.
Accountability is vital; even when priority areas are funded, the programmes need to be effective and well-monitored. The Commission, therefore, sees a need for impartial 'AIDSWATCH' bodies to monitor and objectively assess HIV responses. Such bodies should exist at both regional and national levels to ensure accountability for monitoring all actors in the AIDS response: Governments, communities, and donors.
One option would be for people living with HIV and representatives of key populations to Report to regional community HIV networks, which in turn would Report to UNAIDS with the aim of integrating findings into UNGASS and Universal Access reporting processes. But accountability should be a two-way process. However important it is for communities to monitor Governments, it is civil society and community organizations that are responsible for a growing share of HIV programmes. These organizations should also be accountable—both to their constituencies and to Government—for the commitments they make and the responsibilities they assume.
Three factors should be taken into account in assessing the contributions from various community groups and representatives:
• their accountability to people who are affected by the deliberations;
• their relevant experience; and,
• their knowledge of the issues at hand.
A good point of departure is for civil society and non-governmental organizations to adhere to the principles contained in the Code of Good Practice for Nongovernmental Organisations Responding to HIV/AIDS,13 which identifies guiding, organizational, and programming principles that have been endorsed by over 160 international and national organizations. Regional and national networks have the responsibility to ensure this happens.
More broadly, Governments and community-based organizations should recognize the importance of mutual accountability, especially with respect to:
• transparency of information;
• open and equitable governance (structures and processes); and
• authentic consultation (planning and execution of advocacy and programmes).
There is much room for improvement in these areas. Many Governments and inter-governmental agencies are reluctant to share information or to involve community-based organizations in decision-making processes. At the same time, some community-based organizations are inclined to be more accountable to their funders than to their constituencies.
STRONGER PARTNERSHIPS BETWEEN GOVERNMENT AND COMMUNITIES CAN BUILD COMMITMENT AND MUTUAL TRUST
Gaining the confidence and co-operation of the groups who are most at risk is critical to the success of HIV responses. Government staff may be uncomfortable working with community-based organizations, which sometimes are seen as being donor-driven, opportunistic, unaccountable or representing narrow interests rather than the wider public. Governments may feel that community groups are unduly negative, exaggerate social problems, and promote the interests or concerns of marginal communities.
For their part, community-based organizations may be frustrated by what they perceive as the inflexibility of Government bureaucracy. They may fear that Governments want to maintain control over decision-making processes and avoid sharing resources and power and strategic information, or else their previous experiences of working with Governments may have been disempowering and demoralizing.
Creating more effective collaboration between Governments and communities depends on the degree to which Governments are open to input from the communities, and what communities gain in working more closely with Governments. In Indonesia, for example, the Working Group on AIDS of the Faculty of Medicine of the University of Indonesia has successfully worked with people living with HIV, and built partnerships with the Government and the local pharmaceutical manufacturing industry to provide over 1,000 people with antiretroviral therapy since 1999.
A tangible way to build commitment and trust is to institutionalize community involvement, rather than to rely on good will alone. Stronger partnership would address complaints by Governments about a lack of genuine community engagement. Institutionalizing community involvement means creating formal, salaried positions in relevant Government and other structures (National AIDS Commissions, HIV research bodies, decision-making or consultation bodies, etc.); such a step would greatly strengthen the relationship between Governments and communities.
The regional coordinating mechanism of the Global Fund to Fight AIDS, TB, and Malaria for the Pacific Islands provides an example of how to ensure meaningful community representation and involvement. Many of the Fund's Country Coordinating Mechanisms have been struggling to ensure community involvement. But the Pacific Islands Country Coordinating Mechanisms is exceptional; it has achieved equal participation of Government and community representatives. Each of the 11 participating countries nominates a Government and a civil society representative, and the Country Coordinating Mechanisms also includes room for representation from a regional organization of people living with HIV.
STIGMA AND DISCRIMINATION BLOCK COMMUNITY PARTICIPATION IN POLICYMAKING
The stigma attached to sex work, drug use or sex between men is reflected in many countries by national legislation that makes such behaviour illegal. In certain countries, community activists have helped overcome some of these barriers, even where there is little likelihood in the short term of effecting legal reforms or changes in social attitudes. Often, progress has been achieved through participation in national AIDS governance structures such as Global Fund Country Coordinating Mechanisms and National AIDS Commissions. There are also many local-level examples where communities have managed fruitful negotiations with local police to allow outreach, participation and harm reduction activities to occur unimpeded.14
Meanwhile, stronger efforts are needed to reduce discrimination by means of effecting legal reform and strengthening the human rights frameworks, as well as by supporting community organizations in monitoring discrimination and developing advocacy strategies. Legal working parties could be established to review current legislation and laws, in order to recommend concrete actions for Governments.
At a more basic level, it may also be necessary to help to mobilize and to organize affected communities. This implies, among other things, providing training in skills and network-building. It is not that communities lack skills and assets, but rather that those attributes may need to be adapted so that communities can engage more effectively with Governments.
BUILD A TRADITION OF COMMUNITY INVOLVEMENT IN COUNTRIES WITH LIMITED CIVIL SOCIETY PRESENCE
What about countries where civil society hardly exists? While some countries in Asia have well-developed civil society sectors that include non-governmental and community organizations, others lack a tradition of civil society mobilization and organization. Indeed, some Governments seem to be uncomfortable with the mere notion of autonomous community mobilization and engagement, and a few openly discourage or proscribe such activities. In some places, support groups of people with AIDS are classified as self-help groups rather than non-governmental organizations or community organizations, and independent local organizations do not exist In a few countries, civil society engagement is currently impossible.
In such situations, rather than recite mantras about the importance of community partnerships, practical strategies must be devised to support the emergence of independent community organizations, and to encourage a more tolerant attitude on the part of Governments. The Global Fund and UNAIDS, including UNDP with its focus on governance and human rights, should take the lead in supporting and ensuring that community organizations have the space and capacity to be involved in the AIDS response.
PUBLIC—PRIVATE PARTNERSHIPS ENSURE FAST DISBURSEMENT OF FUNDS FOR COMMUNITY PROGRAMMES
Community organizations cannot participate in national processes if they lack human resources, finance, information, and preparation time.
Often, they are expected to take part in processes or provide services on a volunteer basis, while covering their own transport and opportunity costs. This is unfair and ultimately counterproductive. Resources for community engagement need to be a part of overall budgets for even the simplest HIV projects.
In Asia, such organizations of people living with HIV that do exist tend to be fragile, under-resourced and reliant on a small number of dedicated individuals. It is important to devise ways of supporting these organizations and enhancing their work, so that they can strengthen community engagement. One way of doing this is to make sure that resources are allocated in national AIDS plans and budgets to support capacity building for community organizations.
When drawing up budgets, adequate funds should be earmarked for building capacity and for management infrastructure of community-based organizations. Funding agencies should also help to fund the core activities of community-based organizations. The responsibility for disbursing funds efficiently could be assigned to designated structures in Government. Another option would be to set up a small grants fund that specifically addresses these resource needs.
The Commission proposes the creation of public-private partnership structures that would be responsible for the funding and oversight of community-run HIV projects and programmes. Government and non-governmental entities would be equally represented in these stpuctures, which should include strong representation from community groups. Funding would come from national AIDS budgets, as well as from bilateral donors. The same structure could serve as 'principal recipient' of Global Fund grants. Funds would then be disbursed to those projects or organizations that provide services to most-at-risk populations, people living with HW and their families. The Commission recommends that the World Bank and the Global Fund should take the initiative to develop a quality model of public-private partnerships along these lines.
GOVERNMENT HAS THE PRINCIPAL RESPONSIBILITY TO MAKE COMMUNITY INVOLVEMENT 'MEANINGFUL'
Governments may engage with communities, but often the process is formalistic and lacks substance. Consultation outcomes are not reflected in Government decisions, or community representatives do not have the power to negotiate issues, or they are coerced into adopting or supporting particular positions. Governments sometimes 'cherry-pick' those community representatives who are most compliant and sideline others.
Governments should promote the authentic involvement of community organizations. Building direct relationships with key individuals and organizations may assist in this process. It may also be useful to support interest-based coalitions that can consult with their constituencies, develop a consensus, and coordinate their inputs with those of Government.15 Many such entities exist in Asia, ranging from networks of people living with HIV, sex worker organizations, women's coalitions, national bodies such as the Malaysian AIDS Council, regional networks (such as the Coalition of Asia Pacific Regional HIV/AIDS Networks), and international networks that work in Asia (such as the International Treatment Preparedness Coalition).
Strengthening community engagement presupposes knowing where they are located and what work they do. An assessment or mapping of community organizations and representatives is needed to identify who is working on HW. Further assessments can then identify which of those actors is most appropriate to work with, and what their skills, experiences, resources, and needs are.
A further step in strengthening community involvement is to develop a broad action plan with a time-frame for implementation and measurable indicators. Such a plan will include the terms of reference for involving communities in national plans, monitoring and evaluation, and programme implementation. It could also include analysis of the support and resources that are needed in order to facilitate stronger community involvement.
While community representatives can play a role in advocating in favour of community engagement, and advising on how to best to do this, it is ultimately national Governments who are responsible for making it happen.
But representation on national bodies like National AIDS Commissions or Country Coordinating Mechanisms should involve a process in which communities nominate their representatives. Ad hoc representation by individuals 'cherry-picked' by Governments should be done away with.
COMMUNITY ORGANIZATIONS NEED SUPPORT TO BUILD THEIR CAPACITY FOR ENGAGEMENT
Although community organizations have a vital role to play in building an effective and sustainable HIV response, many are disorganized and lack capacity. In much of Asia, they lack the administrative and managerial capacity to organize, manage, and implement interventions without technical and financial support. They often lack legal status, are not registered, and therefore are ineligible to receive donor funds, and are unable to act as representatives in official forums and structures. It is important that they receive the support they require to meet these logistical requirements.
Community-based organizations often require partnerships with established non-governmental organizations and academic bodies to earn credibility, develop capacity, and articulate their needs. In this sense, there is a clear scope for other non-governmental organizations and academic institutions to become involved in the community-level response by strengthening community-based organizations.
Many mainstream non-governmental organizations in Asia do not participate in the HIV response because it involves dealing with unfamiliar groups of people. Without an understanding of the lifestyles and hardships faced by people affected by the epidemic, it is difficult to iiriplement effective interventions.
Some international non-governmental organizations act as AIDS service providers, mainly by disbursing funds to local non-governmental organizations, with or without community involvement. Sometimes successful implementation occurs, but communities are treated as passive beneficiaries. Devolution of power to the community organization is seen as an optional feature, rather than an intrinsic aspect of the project. Once funding dries up, some of these organizations move onto other work, leaving their community 'partners with little or no support. The involvement of non-governmental organizations as intermediary actors therefore must address the issue of sustainability of the programme (see Box 6.4).
Non-governmental initiatives can be more costly than community-run programmes. A comparison of Thai and Cambodian responses illustrates this. The latter programme was mainly funded by donors and cost four to five times more than the Thai response, which was almost exclusively nationally funded. This may be justifiable where an emergency response is required to an epidemic such as HIV. However, there is no excuse for ignoring the need to strengthen the human and organizational capacity of community groups.
Large international or national non-governmental organizations can play a valuable role in providing services where community organizations have not yet developed the necessary technical and management capacity to do so. But the ultimate objective must be to hand the programme over to the community. Ideally, the role of such NGOs should be temporary, laying the groundwork for community-led programmes.
A few organizations (HOPE in the Philippines and KHANA in Cambodia) have been very successful in building capacity and supporting community initiatives. AVAHAN, a Bill and Melinda Gates Foundation initiative for India, which has received the largest grant of its kind for most-at-risk groups, has committed itself to transferring ownership to the community in its programme statement.
1 'The ideas and discussions presented in this Chapter were initiated and developed through an on-line consultation, collecting the perspectives of civil society throughout the region to strengthen the quality of the Commission's recommendations. The 'Asia regional stakeholder perception and priority survey' took in the views of over 600 participants from the community of people living with HIV (PLHIV); local and national NGOs, international NG05, community-based organizations (CB0s), media and journalist groups, academic and education institutions, and private sector companies, through an online survey and key informant interviews. This open and independent civil society online consultation was one of the first of its kind in Asia, and it has provided valuable inputs to inform this chapter and the recommendations of this Report.
2 WHO (1983), New approaches to health education in primary health care: Rchnical Report Series, 690, World Health Organization.
3 C. Hangzo, et al. (1997), 'Reaching out beyond the hills: HIV prevention among injecting drug users in Manipur, India', Addiction 92 (7), pp. 813-20.
4 Prontier Prevention Project: Participatory Site Assessments: Cambodia, Ecuador, Andhra Pradesh State in India (2003). International AIDS Alliance, available at http:// w-ww.aidsalliance.org/custom asp/publications/view.asp?publication id = 87
5 C. Beyrer, et al. (2000), 'Overland heroin trafficking routes and HIV-1 spread in south and Southeast Asia', AIDS 14, pp. 75-83.
6 K. Sarkar, et al. (1997), 'Relationship of national highway with injecting drug abuse and HIV in rural Manipur, India', Indian Journal of Public Health, 41(2), pp. 49-51.
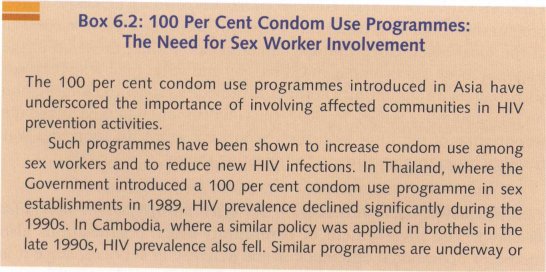
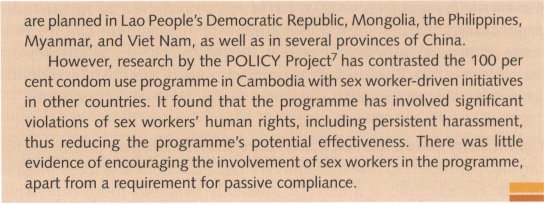
7 David Lowe (2003), Documenting the experiences of sex workers, unpublished draft report to the Policy Project, David Lowe Consulting, Asia.
8 N. Ford, et al. (2004), 'The role of civil society in protecting public health over commercial interests: lessons from Thailand', Lancet, 363, pp. 560-3.
9 S. Radelet (2004), 'The Global Fund to Fight AIDS, Tuberculosis, and Malaria: Progress, Potential and Challenges for the Future', report available at: http:// www.cgdev.org/content/opinion/detail/2992/
10 Martha Ainsworth, et al. (2005), 'Committing to results: improving the effectiveness of HIV/AIDS assistance: an OED evaluation of the World Bank's assistance for HIV/ AIDS control', full report and supporting documents available at X59Z9LKY00
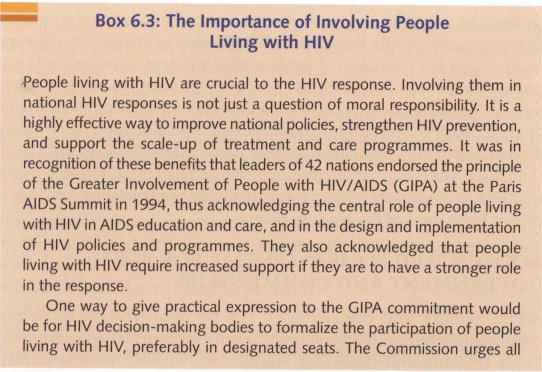
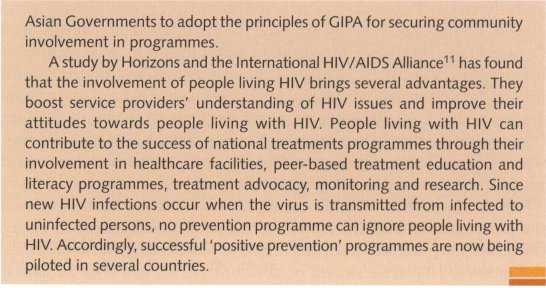
11 Meaningful involvement of people living with HIV/AIDS' at www.aidsalliance.org under 'documents'.
12 The Seven Sisters: The Coalition of Asia-Pacific Regional Networks on HIV/AIDS (2007), Minimum Standards for Civil Society Participation in the Universal Access Initiative available at:
13 International Federation of Red Cross (2005), available at: health/hivaids/code/.
14 C. Jenkins and S. Sarkar (2007), Creating environments that care: interventions for HIV prevention and support for vulnerable populations: focus on Asia and the Pacific, Bangkok: Alternate Visions.
15 In general, it is desirable for Governments to work with organizations rather than individuals. National HIV/AIDS non-Government organizations such as the Malaysian AIDS Council, the HIV/AIDS Coordinating Council (Cambodia) or the Thai National Coalition of AIDS organizations have legitimacy and accountability based on their representation of many groups, and would likely have built up strong organizational experience.
| < Prev | Next > |
|---|