| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 187 |
| Yesterday: | 251 |
| This Week: | 187 |
| Last Week: | 2221 |
| This Month: | 4775 |
| Last Month: | 6796 |
| Total: | 129374 |
2 Archetypal Heroin
 |
|  |
| 
| Books - Drugs |
Drug Abuse
2 Archetypal Heroin
The Beginnings of Dependence
Although the number of heroin users in this country is statistically negligible estimates vary between totals of 400 and 2,000, or between 0.8 and 4 per hundred thousand of the population - this is the archetypal drug of addiction, and round it we form our attitudes towards drugs and drug use generally.
Fifteen years ago Britain hardly had a drug problem, and had not had one since the turn of the century and the end of Victorian proprietary medicines that relied on opium for their remarkable cure-all effects. The Interdepartmental Committee on Drug Addiction (the Brain Committee) reported in this sense in 1961 : `. . . on the evidence before us the incidence of addiction to dangerous drugs was very small. .. there seemed no reason to think that any increase was occurring ...'1
At that time, and for many years before, the addict population was a small, self-contained group of between three hundred and four hundred of whom about one in ten used heroin; most of these were elderly people who had contracted the habit through medical treatment. There were also about seventy doctors and nurses who had access to drugs and had probably started using them in some long period of duty when they also felt unusually ill and tired. There were a very small number of non-medical addicts - perhaps only a dozen. Richard H. is an example of ;one who has made an adequate adjustment to life. He is about forty-five, a thin, rather worried-looking man who worked for many years as the head of a design team in an advertising agency. His cuffs and collars are often frayed and sometimes a bit grimy; he is a bachelor and lives with a boyfriend and housekeeper in a neat little house by the river. His job brings him into emotional collision with a variety of people; he does his best to avoid arguments, which cause him almost physical pain. He is worried about his job, about rivals in other firms, about his superiors and his subordinates. He treats everyone with the greatest politeness; yet intrigues incessantly. At lunch time he slips out to place disastrous bets; everyone likes him and sympathizes with the strain he suffers. He criticizes all about him with the most undiplomatic freedom.,
He was young and at art school with several people who now have international reputations; then, just after they had begun their professional lives, he was the most successful. Now he is shy about them. Almost deliberately, it seems, he refuses to adjust to the rapidly changing modes of visual presentation. His work became old-fashioned in 1963 and he left his job. No one would have dreamed of asking him if he were an addict, and he certainly never talked about it.
He, and others like him, used heroin as a private, shameful accessory to their lives, for its pharmacological properties alone: to relieve anxiety, and to prevent withdrawal. That people can use opiates for twenty Years or more without showing intellectual or moral deterioration is a common experience.
We think it must be accepted that a man is mentally or morally normal who graduates in medicine, manies and raises a family of useful children, practises medicine for 30 or 40 years, never becomes involved in questionable transactions, takes a part in the affairs of the community and is looked on as one of its leading citizeni.... Such cases . .., and they are not uncommon, have taken as much as 15 grains of morphine daily for years without losing one day's work because of morphine. Such addicts however are under the necessity of concealing a practice which is disapproved by the public and proscribed by law. To this demoralizing situation is added the shame most of them feel at being the slave of a habit from which most of them would lib to be free. This combination of furtive concealment and shameful regret cannot help but bring about some change for the worse in any personality, but the change produced in mature individuals is usually so slight that it cannot be demonstrated or cannot be classed as 'moral deterioration '?
To these heroin plays niuch the same role as insulin to the diabetic, and they are by no means rare among people dependent on opiates. A more modern example from New England: a doctor 18 who had a wife, a mistress, two children and a busy practice injected about a grain of morphine a day intramuscularly; 'one shot for patients, one for mistress, one for family, one to sleep'. When the mistress broke off the affair he went to a psychiatrist complaining of depression, but as soon as he could organize another mistress felt perfectly happy and went on as before.3 This case also illustrates how drug dependence always accompanies other serious, social and psychological symptoms, and often appears to be the least that is wrong with the addict.
The New Addicts
But before the first report of the Brain Committee had been set up in type, the situation had changed so obviously that it could not be ignored. Instead of being passive, secretive people, addicts became publicists and proselytizers. Something like the American pattern of addiction began to emerge, with new addicts being actively recruited, mainly from adolescents, both working and middle class. Just how this self-perpetuating social pattern began is not at all clear. Looking back, the first sign of it was the arrest of a young professional trafficker in 1951 who had stolen a large amount of heroin and cocaine from a hospital pharmacy. In the three months he was at large in the West End of London he had built up a clientele of fifty customers. All of these, over the years, have emerged as confirmed addicts, who presumably have to some extent carried on their patron's energetic business habits.
An early contribution may have been made by the flight of addicts from Canada's new penal drug code of 1958. The first arrived at the end of 1959, and by the end of 1962 about 70 had come, some with criminal, trafficking backgrounds. By the end of 1965 about half had either died, returned voluntarily or been deported to Canada. We must also take into account the general change in teenage attitudes at the end of the fifties, with the shift of interest away from the crude external power relationships of gangs to rather more private worlds of experience expressed in clothes and music. In this changed atmosphere drug use might well be more readily accepted.3
Bewley gave an analysis of the number of heroin addicts known to the Home Office, and their recruits, deaths, cures and deportations in each year from 1955 to 1964.4 He reported that the number of new addicts each year followed-a smoothly increasing curve, doubling roughly every nineteen months. A follow-up paper by the same author30 carries the study forward to the end of 1966. He found the rate of increase slightly accelerated: the number of new cases reported doubled every sixteen months, and the total was1,272. He predicted that there would be 800 new cases reported in 1967 and 1,200 in 1968. If the more or less stationary pre-1958 total of 60 addicts is subtracted from the yearly tab, it seems that every three 'new pattern' addicts recruited two more each year. But it became apparent that the totals of heroin addicts known to the Home Office (before the introduction of Treatment Centres and the registration of users) fell far short of reality. Just how far short was not apparent until Rathod and de Alarcén published their penetrating study31 of teenage heroin users in Crawley New Town (one of the characterless new communities near London) over the years 1966-7. They found 27.21 known, probable or suspected heroin users per 1,000 among boys from 15 to 20. Their total, which may be incomplete, came to 92: a figure that contrasted strikingly with the eight cases there that had been reported by their doctors to the Home Office.
With a sudden rush of new young addicts, the Brain Committee was reconvened in 1964; its proposals and the chances of effective control of the situation are considered in Chapters 10 and 11. What it ignored, however, was one important aspect of the new wave: the favourable, indeed grasping, attitude to publicity of many young drug users.
This new brand of user makes addiction in itself a way of life, to be seen and commented on. Their drug dependence is an inarticulate but forceful statement about themselves and society; now that the subject of sex is being assimilated, this is perhaps the most shocking statement an adolescent can make. It is difficult to tunderstand the spread of addiction unless one bears this in mind. The mythology and way of life of the heroin user plays as much part in the whole phenomenon as the pharmacology of the drug itself. We examine the myths in Chapter 4; here 20 it is necessary to set out the salient facts about the drug. The vital function of heroin, or any of the opiates whether natural or synthetic, seems to be their capacity for blotting out anxiety, and releasing the counter forces of confidence and euphoria. These drugs are used medically as painkillers, and although they dull the perception of pain, their more important function is to suppress the patient's alarm about the pain he still feels. A set of experiments at Lexington, the American hospital in Kentucky for the investigation and treatment of addiction, shows this rather neatly. Two experiments were set up, in both of which patients were asked to guess whether each of a series of shocks was more or less painful than a control shock. In one situation the experimenter treated the subjects amiably, there was no formality, and they could press the key to give themselves the shocks: most people graded them correctly. In the other set-up things were Made very formal, everything was done in a curt and worrying way, and the actual electrical contact was made out of the patients' sight and without warning. In general these shocks were thought to be more painful than they actually were. Both sets were repeated with the subjects full of morphine. This time, apparently because worry over the second experimental situation was relieved by the drug, the subjects did as well as in the informal set-up.6
A more commonly given reason for addiction, which accords with the generally held mythology of drugs, is the 'kick', the sensuous pleasure on injection, particularly that produced by heroin. Opinions vary enormously about this. In some reports it is a sensation so poignant that no one can resist it. Nyswander says that some staff members at Lexington learned to feel the kick, and experienced it as a sort of orgasm in the stomach. She describes an addict getting his pay-off for helping in an experiment there: he chose to have a quarter grain of morphine injected into a neck vein.
There was a slow flush over his body; he rubbed his neck and his arms in an expression of pu're` joy and said: 'This is why men go to prison, and it's worth it' ... It is possible that the intensity of pleasure exceeds any pleasure known to non-addicts.7
She remarks In another passage that when long-term ex-addict prisoners, after three or four years' confinement, are asked whether they would him a luscious girl or a shot of morphine, they always say they would choose the chug. What are we to make of this evidence? It is possible thiy never particularly liked girls. Drug use often seems to correlate with inability to cope with the opposite sex. Then one must bear in mind that they have presumably been to, or heard about Lexington, where experiments are paid for in drugs. They might, by making contrary statements, hope to provoke an amusing trial of the matter.
Psychiatrists with a Freudian training often report tat opiates are used as sex-substitutes.
Over and over again one hears addicts describe the effects of their injection in sexual terms. One addict said that after a fix he felt as if he were coming from every pore. Another said that he used to inject the solution in a rhythmic fashion until it was all used up, and said that this was akin to masturbation albeit much better.'
Many people feel no more than a warmth in the stomach and a tickling sensation in the crutch; the pleasure of this is often offset by the characteristic vomiting that the first shots of heroin or morphine produce. One ex-addict says that for a while 'it felt as though you had golden fire running through your veins', but this wore off, and towards the end of his self-terminated addiction he found heroin merely stupefying. Dr Goulding, one of the Secretaries of the Brain Committee, found that heroin had no more effect on him than a 'second-rate sleeping pill'. An experiment in which two successive doses of morphine were given to 150 healthy young men, found only three who would willingly allow the injection to be repeated, and none who would have sought it out. The authors conclude:
Opiates are not inherently attractive, euphoric or stimulant. The danger of addiction to opiates resides in the person and not the drug."
From an earlier, classic paper on addiction:
The intensity of pleasure produced by opiates is in direct proportion to the degree of psychopathy of the person who becomes an addict....
The subsequent depression resulting from long continued use of the drug carries him as far below his normal emotional plane as his initial exaltation carried him above it.10
In other words perhaps: if one is emotionally, very screwed up, relaxation feels marvellous, just as women feel positive sensations of pleasure when they take off tight shoes. But if one is relaxed to begin with the drug has no pleasure to offer.
The third important effect, which tends to continue drug use, is in no dispute: withdrawal. It is happily difficult to see this display of symptoms in Britain today, since addicts in prisons and hospitals are generally let down slowly under substitute opiates, tranquillizers and sedatives, but the fear of it is always in the addict's mind. It is indeed a spectacular and well documented medical drama. Dr Robert de Ropp describes it well: ,
'Withdrawal sickness' in one with well-developed physical dependence on opiates is a shattering experience and even a physician accustomed to the sight of suffering finds it an ordeal to watch the agonies of patients in this condition. About twelve hours after the last dose of morphine or heroin the addict begins to grow uneasy. A sense of weakness overcomes him, he yawns, shivers, and sweats all at the same time while a watery discharge pours from the eyes and inside the nose which he compares to 'hot water running up into the mouth'. For a few hours he falls into an abnormal tossing, restless sleep known among addicts as the 'yen sleep'. On awakening, eighteen to twenty-four hours after his last dose of the drug, the addict begins to enter the lower depths of his personal hell. The yawning may be so violent as to dislocate the jaw, watery mucus pours from the nose and copious tears from the eyes. The pupils are widely dilated, the hair on the skin stands up and the skin itself is cold and shows that typical gooseflesh which in the parlance of the addict is called 'cold-turkey', a name also applied to the treatment of addiction by means of abrupt withdrawal.
Now to add further to the addict's miseries his bowels begin to act with fantastic violence; great waves of contraction pass over the walls of the stomach, causing explosive vomiting, the vomit being frequently stained with blood. So extreme are the contractions of the intestines that the surface of the abdomen appears corrugated and knotted as if a tangle of snakes were fighting beneath the skin. The abdominal pain is severe and rapidly increases. Constant purging takes place and as many as sixty large watery stools may be passed in a day.
Thirty-six hours after his last dose of the drug the addict presents a truly dreadful spectacle. In a desperate effort to gain comfort from the chills that rack his body he covers himself with every blanket he can find. His whole body is shaken by twitchings and his feet kick involuntarily, the origin of the addict's term, 'kicking the habit'.
Throughout this period of the withdrawal the unfortunate addict obtains neither sleep nor rest. His painful muscular cramps keep him ceaselessly tossing on his bed. Now he rises and walla about. Now he lies down on the floor. Unless he is an exceptionally stoical individual (few addicts are, for stoics do not normally indulge in opiates) he fills the air with aies of misery. The quantity of water secretion from eyes and nose is enormous, the amount of fluid expelled from stomach and intestines unbelievable. Profuse sweating alone is enough to keep both bedding and mattress soaked. Filthy, unshaven, dishevelled, befouled with his own vomit and faeces, the addict at this stage presents an almost subhuman appearance. As he neither eats nor drinks he rapidly becomes emaciated and may lose as much as ten pounds in twenty-four hours. His weakness may become so great that he literally cannot raise his head. No wonder many physicians fear for the very lives of their patients at this stage and give them an injection of the drug which almost at once removes the dreadful symptoms. `It is a dramatic experience,' writes Dr Harris Isbell, 'to observe a miserably ill person receive an intravenous injection of morphine, and to see him thirty minutes later shaved, clean, laughing and joking.' Rut this holiday from hell is of short duration and unless the drug is administered again all the symptoms start afresh within eight to twelve hours.* If no additional drug isOgiven the symptoms begin to subside of themselves by the sixth or seventh day, but the patient is left desperately weak, nervous, restless, and often suffers from stubborn colitis."
The tender de Ropp does not mention that both men and women suffer constant orgasms during the critical period.
The next effect, once physical dependence has been established, is the hunger of the addict for his drug when the amount of it circulating in his bloodstream falls below a comfortable point.
Just what happens inside the addict's body is uncertain — some lines of research are sketched below — but he feels the anxiety, irritability, discomfort of someone with powerful appetites who badly needs a meal, multiplied a hundred times. This appears to be a self-contained symptom, and not just a conscious attempt to avoid the withdrawal syndrome. The extremities of cunning and self-immolation this forces on addicts are well illustrated in this account:
I once treated a twenty-seven-year-old nurse, who complained of a recurrent cystitis, for which she had previously consulted one of my colleagues whose name she had obtained from a training hospital. She told him that she had had a kidney removed; a large scar on her back bore witness to this fact. She appeared to be in acute distress, with temperature, pallor, tenderness in the lumbar region. The physician did a urinalysis in his office and discovered crenated red blood cells which, together with other findings revealed in a thorough examination, seemed to substantiate her story. She stated that she was working as a nurse, and as she seemed to be quite intelligent, there was no reason for the physician to suspect anything out of the way.
She requested morphine but instead was given a prescription for Demerol, which she said she could administer herself. She phoned the next day to say that she was allergic to Demerol and asked him to leave a prescription for Dilaudid at the drugstore. He did so, and within twenty-four hours he called her to check on the condition. To his surprise, there was no such telephone number as the one she had given. When she again phoned for medication, the physician suggested that she first come in for another examination and mentioned the desirability of hospitalization. She made some excuse and he never heard from her again. He then realized that she was probably an addict, but he was puzzled about the appearance of crenated red blood cells in the urine.
Several months later this woman was arrested for stealing drugs from a hospital. She was sent to a prison-hospital and, by coincidence, I recognized her from my colleague's description of the diagnostic picture and her clever fuses to obtain drugs. A little probing cleared up the mystery of the crenated red blood cells: before she consulted a physician she put a small pencil up into her uretha, causing bleeding into the bladder.
This woman's entire period of hospitalization was characterized by self-inflicted injuries in an effort to obtain drugs while surgical repairs were being made. She swallowed, among other things, a wrist-watch, glass, broken pieces of silverware, stones and safety pins. In a continuous state of anxiety when off drugs, she could not work consistently. One night I was summoned to her room and found her sweating profusely, with dilated pupils and a low-grade temperature. She complained of a severe pain in her lumbar region. Examination of the urine showed crenated red blood cells. Despite the patient's previous history of feigning a kidney condition, she was given the benefit of the doubt and Demerol was prescribed until a medical work-up could be completed.
She continued to complain of severe pain and on the following day a flat plate of the abdomen revealed an opaque area in the region of the left ureter. On a tip from the technician, I examined the patient before she had her next X-ray and found on her back a flat wad of chewing gum mixed with some calcium-like material which would simulate a stone on the X-ray plate. The Demerol was stopped, but she continued to require medication from time to time and, in fact, demanded as much attention as ten other patients.
There was no doubt about this woman's difficult medical history and even in a purely custodial arrangement she could not cope with her problems. As a matter of fact, she hanged herself while doing a short term in a house of detention where she was forcibly and suddenly withdrawn from drugs. In my opinion, this particular patient needed , drugs to handle her emotional and psychic turmoil just as the diabetic needs insulin in order to function well. Fortunately this type of case is a rarity.12
In time the kick weakens, the high vanishes, with good management withdrawal need never be experienced, and all the heroin addict has left is constant drowsiness, constipation, impotence, and the need for a slowly mounting dose.
The Pharmacology of Opiates
A considerable amount of work has been done on the internal action of drugs — much of it, one must admit, unintelligible to the layman — but there is no certainty yet on the mechanisms of their operation. One obvious fact is the power of opiates. The ordinary addict's dose of half a grain is roughly eqpivalent to only four millionths of the body's weight. On injection, heroin is immediately broken down into morphine and by-products. The lungs, liver and kidneys collect morphine readily, and soon after injection they contain a higher concentration than the blood. In fact, it is estimated that only between 2 per cent and 14 per cent is available as molecules free to enter brain tissue. An hour after rats were injected with two millionths of a gramme of morphine per gramme of body weight (equivalent to a dose of 2-4 grains for a well grown man) their brains contained no more than 0-09 millionths of a gramme per gramme of tissue, or 2 per cent of the concentration ope would expect if the drug was distributed evenly through the body. The kidneys, on the other hand, contained 8,000 per cent of their share.'13
This sort of evidence suggests that the effects of opiates may be due not so much to the drug, but to a body chemical released or inhibited by it. But the extreme difficulty of saying anything definite about the pharmacological action of drugs is illustrated by the work of Hill, who found that morphine — classically considered a depressant — could either slow down simple reaction times or speed them up, and that this effect depended solely on whether his subjects were paid for their cooperation before or after the experiment.14
In other experiments it is found that morphine both depresses and excites nervous activity. In cats with severed spinal cords habituation to opiates depresses one set of leg reflexes, and excites another pair; withdrawal spectacularly reverses these effects. One explanation of these phenomena is that morphine is absorbed quickly on the outer layers of nerve cells, giving a short-term stimulant effect, and slowly on the inside, producing habituation and depression. Another explanation points simply to the complex pyramidal nature of nervous organization; because of the function of some nerve cells in both exciting and inhibiting others, a single effect from the drug might be expected to produce widely different effects on the total organism. In the same way one might suppose that the drunkenness ofa general might haveeffects on the behaviour of an army very different to the drunkenness of all the privates.
A more sophisticated idea is that morphine works by filling up keyhole-like positions on nerve cells that are normally occupied by molecules of a chemical called 5-hydroxytryptamine. In reaction to this, the nerve cells develop more sites which are in turn slowly filled up by morphine molecules. While this slow invasion is going on, there is also a rapid metabolization of morphine molecules making it necessary for the addict to keep injecting the drug to keep up the coverage. Thus if there is enough morphine in the bloodstream things are functionally as normal: although there are far more receptor sites on the nerve cells most of them are covered up and no more 5-HT comes in contact with the nerves than necessary. But the growth of new receptor sites is always a jump ahead of the quantity of morphine present so the addict is slowly forced to step up his dose. After the last dose at the beginning of withdrawal the morphine is destroyed and not replaced, leaving the nerve cells over-supplied with receptor sites, and overwhelmed with 5-HT, which produces the well-known effects of withdrawal. In support of this idea, it is noticed that 5-HT is continuously produced in the brain, and that the effect of raising the 5-HT level in dogs closely resembles Withdrawal. However, similar theories involving adrenaline, noradrenaline and other chemicals have been proposed.15
This general type of theory accounts for the interesting fact that withdrawal symptoms are opposite to the effects of the drug. It is suggested that the complex of signs felt during withdrawal - muscular pain, inability to keep still, air hunger, gooseflesh, nausea, bowel urgency, anxiety and the rest - are part of a deep-seated defence reflex which warns the body and prepares it for danger. The addiction-prone person is plagued by unwelcome sensations - which most of us feel only in the dentist's waiting-room - and takes the drug to be free of 'them. The euphoria he feels, and only he feels, is due to the relief of this pressure. On withdrawal he gets back, very literally, the accumulated reflex that he has avoided during addiction.16
Intermediate between the involuntary autonomic nervous effects of opiates and their withdrawal, and the conscious elements of the addict's life, lies the craving for the drug, and the compulsion to obtain it. The plaintiveness and ingenuity of addicts' attempts to get opiates are very characteristic. One example was described on p. 25; every doctor who treats addicts can describe similar cases of this personality aberration. Animals show the same behaviour. In one experiment a group of chimpanzees was trained to solve problems for food rewards. Naturally enough they were then hardly interested by the offer of a syringe of morphine; after addiction their performance for food was low, but for the syringe high.17
An unusually brutal experiment in America shows the importance of the fore-brain in craving. Four patients who were about to have bilateral frontal lobotomies - three for schizophrenia, and one for phantom limb pain - were addicted and withdrawn. Whether this was done with the patients' permission is not stated. Disappointingly the schizophrenics showed all the involuntary signs of withdrawal, but did no make the characteristic faces and demands of the normal addicts. The fourth man responded in the usual way, asking repeatedly and pathetically for a dose of morphine. After one-sided lobotomy had been done on all four the process was repeated with the same result; again the phantom limb man was the only one to show craving. After the second lobotomy none of them showed any but the non-purposive signs of withdrawal - vomiting, gooseflesh, loss of weight and so on.6
This section was intended as no more than a rough guide to the sort of ideas that are being investigated in this difficult field. So far, it is safe to say, theoretical investigations of opiate addiction have thrown some useful light on the working of the nervous system, but hardly contributed yet to solutions of the problems caused by these drugs.
Addiction in Britain
Heroin addiction has now been a social problem in Britain long enough for some research to have been done on it, and for some facts to emerge. A survey of heroin users in some, unnamed, industrial town, taken in 1967 and repeated in 1968,32 found that of fifty heroin users, 84 per cent were male, and their average age was 21 - that of the girls 19, and almost all were single. Social classes I and II were over-represented and Class V underrepresented. Half of them took heroin daily, and their dosage ranged from * of a grain to 5 grains. Among the other half, 36 per cent used the drug irregularly, 4 per cent were in hospitals or prisons, and 12 per cent had given it up.
The national statistics on addiction, as published by the Home Office,33 show a remarkably high turnover, with, recently, a fall in the number of known addicts. Thus, of 2,782 known addicts during 1968, 61 died, and 965 dropped out. In 1969, 64 died, 1,351 dropped out, and 1,135 started, leaving, at the end of the year, 1,466 users of heroin and methadone.
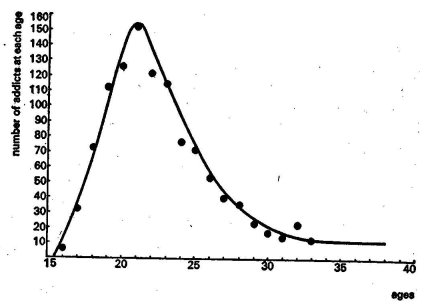
Figure 1. This graph shows the numbers of known British heroin and methadone users plotted against their age. The great majority are in their early twenties. Source, reference 33.
American Addiction
Opiate addiction has, until recently, been such a rarity in Britain that it has hardly been worth investigating it. America, on the other hand, has devoted enormous resOurces to the investigation and treatment of this condition. The material on addiction is therefore largely due to American workers. The dependence of addiction on culture and the expectations of the addict is so important that one can only offer this as suggestive material; but the similarity between Britain and America is enough for us to see the relevance of many American findings to our own problems.
American investigators have the advantage of two State hospitals — Lexington, Kentucky, opened 1935, and Fort Worth, Texas,opened 1938,which treat bothvoluntaryandconvict addicts. There is a Federal Bureau of Narcotics, curiously enough under the control of the Treasury, which keeps records of active addicts, and claims that no one can use drugs illicitly for more than two years without being recorded. Addiction is spread over America in an interesting way. Broadly one can say that it occurs where the opportunity to get drugs co-exists with social and economic squalor. An analysis of the admissions to the two hospitals shows two main patterns.18 The 'southern' pattern, a survival from 1915, is found in Alabama, Georgia, Kentucky. Addicts tend to be 90 per cent white, aged about 43, and usually using the old morphine mixtures: pergoric, Dilaudid, and sometimes morphine itself. The modern pattern of imported heroin use is found in New York, Puerto Rico, the District of Columbia and Chicago. Two thirds of those from the first three States are Negro or Puerto Rican, and their average age is about 27. A narrow belt of heroin use is growing near the borders with Mexico in Arizona, New Mexico and Texas. Both these patterns continue phenomena described in 1928 by Kolb's' and by Terry and Pellens.20 It is also possible to compare Lexington's population now with that in 1937, when the first study of the hospital's intake was made.21 In 1937 the southern type was more common and outweighed admissions from New York and Illinois. During the interruption of world communications during the Second World War heroin was very difficult to come by and addiction rates fell. After the war it rose again to a peak of 1,823 cases in 1950, and is now slowly falling.18 This drop, and the distribution of Lexington and Fort Worth compulsory admissions, correlates well with the Federal Bureau of Narcotics' file, but Ball and Cottrell comment that unfortunately this file is probably not a reliable guide to the total number of addicts, since there is little demographic relationship between the voluntary patients— who make up about a third of the Lexington population, and four fifths of the admissions22 - and the Bureau's records.23 Obviously the underprivileged addict who lives in a criminal, addict society has a far better chance of being picked up than, say, a respectable doctor living in a small town in the centre of the country.
In twenty-five years the mean age of addicts has fallen by eight years to 33.5. In 1937 less than one male patient in five was under 30, in 1962 almost half were. Before the war 10 per cent of the patients were non-white; now one third are Negro, 12 per cent Puerto Rican, 5 per cent Mexican. An examination of young addicts admitted to a New York hospital, ingeniously controlled against their non-addict friends, showed the joint importance of social as well as psychiatric reasons for addiction in this group. The authors comment that urban Negroes and Puerto Ricans have very low status and very high rates of hospitalization for all mental illnesses, especially dementia praecox (schizophrenia). They are particularly susceptible to alcohol psychoses, delinquency and TB. Curiously, the addicts often seemed to come from homes that outwardly seemed better than average, but it often - turned out that the parents had unrealistic attitudes towards life, or simply denied the difficulties of life in the slums. In these homes the parents were more concerned with status - new furniture, a big car outside - than with security or the advancement of their children through education and work. The authors conclude that addicts exceeded the controls in personality malfunction to a statistically significant and clinically impressive extent.., youths ... do not become addicted independent of psycho-pathology '.24
Ball comments that there has been a notable increase in the number of addicts from the minority groups in American society'.25 We in Britain are less likely to be faced with the problems of ghettoes on the Harlem scale, but we should not be complacent about the safety of our own second or third generation coloured immigrant populations. Cultural underprivilege is not something static: advance in one part of society generates deprivation in another. Our own addicts seem to come not from distinct ethnic underprivileged groups, but more from an underprivileged class: the teenagers, who are both exposed to and denied many of the pleasures and opportunities of our own society.
The Myths of Inevitable Addiction and the Pusher
Although it is possible to demonstrate some physical adaptation even to one day's use of heroin, by injecting the antidote nalorphine which precipitates an immediate withdrawal, it takes something like half a grain a day for a fortnight before anyone is even mildly physically dependent on the drug.'* Even then the withdrawal will be nothing worse than a mild dose of flu, lasting a couple of days. The idea of instant addiction after one dose is not substantiated. Addiction must, in fact, be the result of continued, conscious action, with some deterrents to be overcome like vomiting, the unpleasantness of sticking needles into veins, the expense and trouble of buying the drug on the black market. Add to this the later 'sitting round in doctors' waiting rooms, having to 'find somewhere to shoot up, feeling sick before a shot, feeling sick after it and then sleepy'. 'It all became a bore. You have to work at being an addict,' says one who gave it up.
This impression is confirmed by Chein's study for the New York Youth Board of New York adolescent drug users. He and his associates found that ,in the most desolate 15 per cent of the city, where 75 per cent of the addicts live; although narcotics of a sort were available on every street corner, only one boy in ten tried heroin over the four-year study period, and far fewer became addicted. There it is quite common for the kids to joy pop at weekends for years, without ever getting a large enough dose to produce withdrawal symptoms and force dependence on them,
In America before the passage of the Harrison Act in 1914 one could buy opiates either raw or mixed in patent medicines at every pharmacy.* Yet of a population of 100 millions, it is estimated that only 100,000 were addicted. That is one per thousand at the beginning of the century; fifty years of vicious repression has reduced this to one per three thousand.
An extremely interesting contribution to the problem of addict recruitment was unwillingly made by the United States Army out of its experiences in Vietnam. There, no doubt with the energetic help of the Vietcong, some 30 per cent of its soldiers became addicted to heroin. It must be said that only 10 per cent injected it, while the rest smoked the drug, but nonetheless, they had genuine physical habits. As if this were not bad enough - for an addicted soldier is not the most aggressive fighting machine, and the logistic problem of supplying his habit must have been enormous - on return to the U.S.A. many of these men claimed disability pensions on the grounds that heroin addiction is permanent and disqualifies the sufferer from any sort of productive life. Apart from the expense of the pensions, the political repercussions of so many conscripts 'wounded' in such a way, which the American people have been taught to associate with the utmost depravity, would have been most damaging to the Army. So the military authorities were forced to embark on a research programme which followed up returned soldiers and found that - as one might expect - only 1 per cent 35 continued as addicts in the calmer conditions of their native land. One can well understand that the circumstances of fighting the war in Vietnam would in themselves be a very good reason for addiction in the most normal person, and once they were removed there would be no reason to continue.
It is also a fantasy that in a black market under conditions of repression addicts are made by the pressure and organized wiles of pushers and traffickers. An authoritative American handbook says:
The susceptible person does not, as a rule, start out looking for a shot and he is not, as a rule, coaxed into taking one by a 'pusher' for the illegal drug trade. Ordinarily he is introduced to drugs by his associates.'
The practice of handing out free or cheap samples at random in the hope of landing a customer is both uneconomic and dangerous since there is nothing to stop him betraying his supplier. Under these conditions drug initiation is a matter between friends who trust each other,
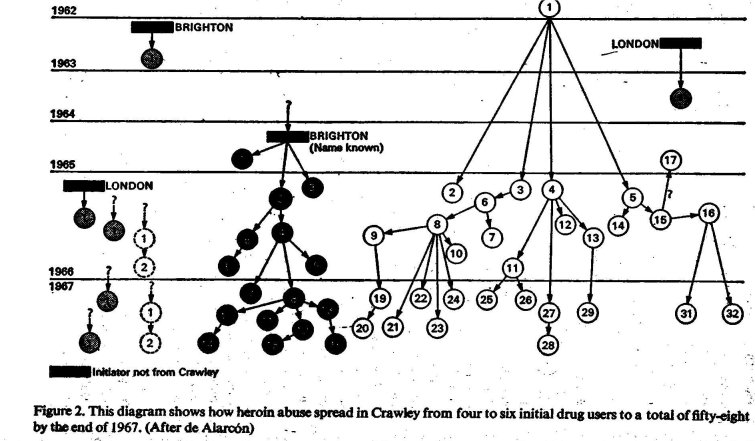
A penetrating piece of work by de Alarc6n34 (see also below p. 139 et seq.) uncovered the way heroin addiction spread among teenagers in Crawley New Town. By asking each newly identified heroin addict who had initiated him, when and where, he was able to describe how between 1962 and 1965 a small number of Crawley teenagers had been initiated in other towns. In the first half of 1966 these few users met each other in Crawley; in the second half of that year and the first half of 1967 the infection rapidly spread from them to teenagers who had not before used drugs. Two major trees of initiations were winkled out: in one, thirty-two users could be traced back to one in the town of Worthing; in the other, sixteen stemmed from an initiation in Brighton. With the control of heroin in 1968 the epidemic seems to have been stemmed, but that may be simply because addicts changed to other drugs — probably amphetamines and barbiturates — and are initiating their new friends into these.
it is unfortunate that our more liberal system of drug control seems to have encouraged the friendly initiator, who after all gets his supplies free from the National Health Service, and whose potential customers are under no great police or social pressures to inform on him.
English addicts, in the words of a prostitute who surveys the scene, 'want to turn the world and its mother on', and as things are at the moment they have every reason, both for self-esteem and self-interest, to keep at it. Until the spring of 1968 it was not difficult to get two or three times the necessary dose from the few doctors who deal with addicts; at El a grain on the London black market a small surplus can provide a comfortable living,
Drug Morbidity
It does not appear that the presence of heroin in the body, even at the rate of 15 grains a day, is intrinsically physically damaging. But most heavy heroin users take grain-for-grain doses of cocaine, a powerful stimulant of the same class as caffeine or amphetamine, to reduce the numbing effect of the opiate. It is possible that much of the harm attributed to heroin is in fact caused by cocaine hydrochloride. In medical practice cocaine, the oldest local anwsthetic, is considered too dangerous for injection, since it is an intense stimulant of the central nervous system. In large doses it causes acute paranoia, and in some cases 'a sudden, rapid and fatal collapse'.23 Because of its powerful anaesthetic properties, the flesh it touches is unusually apt to suffer secondary damage: habitual cocaine sniffers tend to lose the partition between their nostrils. But large doses of heroin seem to produce fewer ill effects than large doses of alcohol, which cause peripheral neuritis — the deterioration of the long nerve cells joining the fingers and toes to the spinal column, producing tingling, insensitive, clumsy hands and feet. The major damage in both cases is done by the way of life that accompanies heavy drug use: irregular meals, insufficient vitamin intake, insanitary living; these overwhelmingly hurt health.
The medical complications donunonly found among addicts at Lexington are: 'Serum hepatitis [a sort of jaundice], venereal diseases, malnutrition, skin infection with residual scars, superficial venous thrombosis [swelling and blocking of the arm veins used for injections], abscess formation both of the skin and internal organs, acute intoxication from accidental overdosage, amenorrhoea, fungus diseases of the skin, respiratory diseases [pneumonia, tuberculosis, bronchial asthma], psychosomatic disorders, peridontal disease and dental caries.'26 This is confirmed among British addicts by Bewley,30 who also finds that 60 per cent of British heroin addicts have some signs of liver damage.
The morbidity of opiate use is equally debatable. On the one hand there are the cases quoted at the beginning of this chapter who go on for decades, on the other adolescents who are dead after a couple of months. Since no one knows accurately either the number of addicts at risk, or the number who die, it is extremely difficult to come to any firm conclusions. O'Donnell followed up a large group of Kentucky addicts: over half had died in the twelve years since their first discharge from Lexington, of murder, suicide, disease, accidents, infections and mental illnesses.28 On the other hand Winick's study of drop-outs from the Federal Bureau of Narcotics' active file showed a considerable number who had been addicted for thirty-five years or more, and one who had kept going for fifty-six years.29
In New York about 350 deaths a year occur among about 35,000 addicts.27 In England, up to the end of 1966, there had been 69 deaths from 2,532 'addict years at risk', giving a mortality rate of 27 per 1,000 per year, nearly three times the New 'York rate and twenty-eight times the rate for non-addicts of similar ages. In 1968 and 1969 the rate fell slightly to 22 per 1,000.33 But the calculation of morbidity depends as much on the numbers of drug users at risk as on the number of deaths. We only know the numbers of heroin and methadone users; there may be ten times as many people involved in the drug world, and equally at risk. The extremely high apparenI death rate may also be because addicts often aren't identified until they die. But it is certain that, on average, addicts die sooner than non-addicts.
Perhaps what kills is not so much the drug as the personality that uses it self-destructively, that gives itself overdoses, that fails to take simple sanitary precautions with injections; that in fact wants to kill itself without having to make the decision to do so. It is not true simply to say that to become addicted is to embarkon a slow, painful suicide.
One distinguished, psychiatrist, who runs a hospital clinic, even sees heroin addiction as a welcome triumph of natural selection over the National Health Service. In his view addiction singles out weak people who would, in earlier times, have died before reaching maturity, and even if it doesn't kill them, it prevents them breeding — to the benefit of the race.
*These symptoms relate to morphine or heroin. It should be emphasized that synthetic drugs having a morphine-like action, such as pethidine, also give rise to addiction. The withdrawal symptoms are somewhat different. Addiction to pethidine is particularly common among doctors and nurses and is, according to Isbell, more harmful in its effects than addiction to morphine.
*The impact of opiates on nineteenth-century Americans is shown by an analysis of 10,000 prescriptions made up by Boston drugstores in 1888: altogether 1,481 contained opiates; so did 25% of those renewed once, 61% of those renewed twice and 78 % of those renewed three times.2
| < Prev | Next > |
|---|