| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4.1% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 180 |
| Yesterday: | 251 |
| This Week: | 180 |
| Last Week: | 2221 |
| This Month: | 4768 |
| Last Month: | 6796 |
| Total: | 129367 |
SOCIAL DETERMINANTS OF SELF-REGULATION IN PSYCHOACTIVE DRUG USE: TOWARDS AN EXPLANATORY MODEL
 |
|  |
| 
| Books - Drug Use as a Social Ritual |
Drug Abuse
SOCIAL DETERMINANTS OF SELF-REGULATION IN PSYCHOACTIVE DRUG USE: TOWARDS AN EXPLANATORY MODEL
Part one of this dissertation analyzed the rituals and rules that have developed in the subculture of regular users of heroin and cocaine. The presented data showed that both on individual and group level the functions and meanings of drug use rituals are multifold and intertwined, serving instrumental as well as symbolic goals. The analysis linked these rituals with other ritualistic behavior patterns, which serve several intrinsically human --individual and social-- needs. Part two presented studies on the health consequences of the observed administration, and sharing and exchange rituals, their relationship with policy and an intervention which utilized and reinforced common ritualized behaviors.
A prominent feature of the studied rituals and rules is that they aim to control or regulate the drug taking experience. This is most apparent in the stereotypical behavioral sequences surrounding self-administration of drugs by the individual drug user, but it also plays a distinct role in many observed (ritualized) interactions, for example in the recurrent sharing of drugs. Thus, the data offer strong support for Zinberg's theory, that the control of drugs is largely established by (sub)culturally based social controls --rituals and rules (as Zinberg called them, social sanctions) which pattern the way a drug is used. Ultimately, users themselves regulate their use of intoxicants through a peer based social learning process, in which specific rituals and rules are developed as adaptations to the effects of the interaction between drug, set and setting. (1 2)
However, it has also become clear that the ability to self-regulate drug use is not evenly spread over all users. Some users seem able to use large amounts of cocaine (and heroin) without or with little of the characteristic problems described in chapter five, whereas others --typically the down and out users hanging around the Central Station-- actually use very little of these (expensive) drugs, but seem most susceptible to their related (psychological) problems.
This paradoxical observation leads to two suppositions: 1) As was already contended in chapter 7, self-regulation or control is more than limiting ones intake. It equally refers to the prevention and management of drug related problems and should, therefore, be perceived as a multidimensional process. 2) The effectivity of rituals and rules in exercising control over drug use is apparently moderated by additional factors, which impact on the individual's ability to comply with these social regulatory processes.
Recapitulating, it is thus clear that, conforming to Zinberg's theory, rituals and rules are key determinants of drug use self-regulation processes. However, Zinberg's theory does not explain the intra-group variation in the ability to effectively utilize these social controls, found in this study. Nor does it account for the multidimensional nature of self-regulation processes. Besides rituals and rules, the theory does not explicitly address other potential factors which may impact upon the effectivity of these social controls. In that respect, Zinberg's theory is rather static. This does not make it invalid, but does, indeed, signify a need for revision. The theory requires certain adaptations and elaborations that will make it possible to explain the dissonant findings of this study.
In this chapter an attempt is made to revise Zinberg's theory. The chapter will introduce and discuss two distinct (clusters of) factors that, in addition to the concept of rituals and rules, are thought to be essential determinants of the self-regulation processes that control drug use. These factors are Drug Availability and Life Structure. (3) The chapter will explore the nature of, and interactions between Drug Availability, Rituals and Rules, and Life Structure. The chapter's ultimate purpose is to present a hypothetical model which explains controlled use of drugs in terms of a dynamic interaction between these three distinct factors. Evidently, this model builds on the work of Zinberg as it seeks to specify and detail the variables that constitute the social setting, in which self-regulation processes take shape.
To demonstrate the model, a secondary analysis of the 1989 treatment admission data of the Rotterdam methadone programs (RODIS) is presented. This secondary analysis was stimulated by some peculiar results in the 1989 RODIS report regarding the prevalence of cocaine use in different ethnic groups, which, apparently, resembled the two cocaine/heroin patterns found in the field study (see chapter 5.4.3). The 1989 RODIS report contains separate chapters on cocaine use and ethnicity, in which cocaine use (and whether or not this was experienced as problematic); life time prevalence of overdose, psychotic episodes, unconsciousness and seizures; the level of heroin use; and their mutual associations are considered. (4) These chapters provide the basic material for the present secondary analysis.
First, these RODIS data are presented and discussed in light of the analyses in chapters five and seven. Ensuing, the issue will be further investigated in the secondary analysis. In the next step the findings of this analysis will be discussed in terms of the three determinants of the proposed model, whereafter a general explanation of the model will be presented.
The Secondary Analysis of the RODIS Data
Distribution of cocaine use and problems associated with its use
RODIS classified treatment applicants' cocaine use in three categories --non-user (32%), user (62%) and problematic user of cocaine (6%) (N = 1095). (4) Not surprisingly, the reported prevalence of overdose, psychotic episodes, unconsciousness and seizures increased from non- users to cocaine users to problematic cocaine users. The prevalence of these problems was also analyzed for differences between the following (aggregated) ethnic groups: Dutch, Surinamese/Antilleans, Moroccans and foreigners. The Surinamese/Antillean group scored lowest on all four indicators, while the Dutch had the highest scores on three out of four.
The ethnic composition of the cocaine use groups showed a highly compatible picture. The Dutch users were over-represented among non-users and, more dramatically, among problematic users. 36% of the Dutch users abstained from cocaine use, 55% used cocaine without perceiving it as a problem and 9% labeled their cocaine use as problematic. In contrast, among the Surinamese/Antillean users the prevalence of cocaine use was significantly higher (77%), but seemingly this resulted in fewer problems (3%). Problematic cocaine use was apparently absent among Turkish and Moroccan clients, while the foreign clients resembled the total population.
Comparison of these data suggests that the bulk of the problems in the cocaine using groups is presented by the Dutch, whereas the Surinamese/Antillean contribution is negligible. Thus, while they use less frequently, Dutch heroin users more often experience problems with cocaine use and score highest on three out of four of the RODIS indicators of problems. A completely opposite picture is presented by the Surinamese/Antillean heroin users. They score lowest on all problems indicators, using cocaine significantly more often with considerably less problems.
Distribution of cocaine/heroin patterns
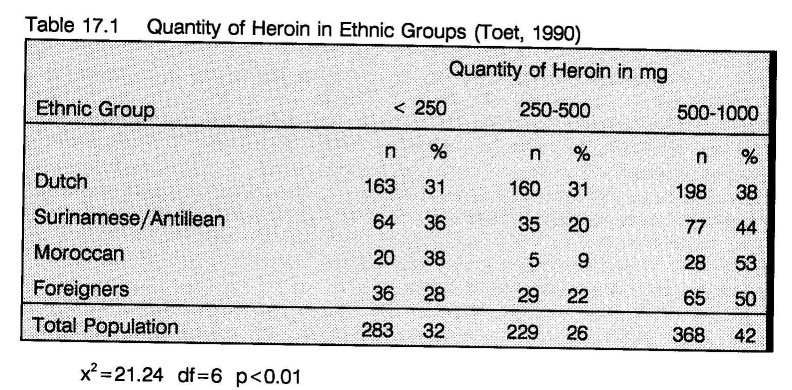
As was established in chapters five and seven, heroin use is positively correlated with cocaine use --heroin is employed to control the negative side effects of cocaine. This general trend was also clear in the RODIS data (see table 7.1 in chapter 7.2.2). However, the ethnographic analysis also suggested the existence of two different cocaine/heroin patterns (see chapter 5.4.3). The ethnic breakdown of the quantity of heroin use of the treatment applicants in RODIS showed differences between the ethnic groups, which might confirm these patterns. Dutch users were rather evenly spread over the three categories, while the Surinamese/Antillean and other groups were more often using little or much heroin. (table 17.1). (4) To further explore these differences, the RODIS data has been broken down to the genuine ethnic groups/nationalities. The resulting database consisted of 651 Dutch, 175 Surinamese, 67 Moroccan, 34 German, 29 Antillean and 20 Turkish users. 17 users came from Belgium and Luxembourg, 38 from other EC-countries and 9 were non EC European residents. 9 users came from other Mediterranean countries and 34 from non European countries.
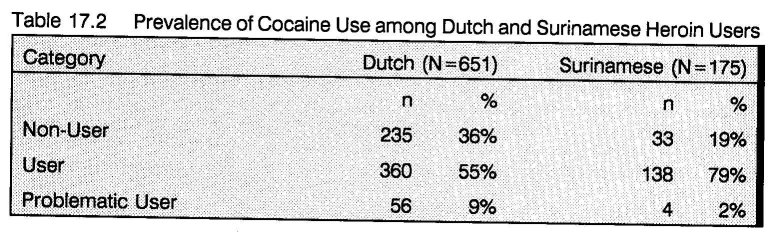
The analysis of their cocaine use showed an increased difference between the Dutch and the Surinamese, while the cocaine use patterns of the Antilleans fell somewhat in between. The Moroccan and Turkish patterns did not change and the Germans more or less resembled the Dutch. Apart from the Surinamese and the Dutch, all other groups were either too small or too heterogeneous for further inclusion in the analysis. Table 17.2 shows the large difference in cocaine use prevalence between the Dutch and the Surinamese heroin users, applying for treatment in Rotterdam.
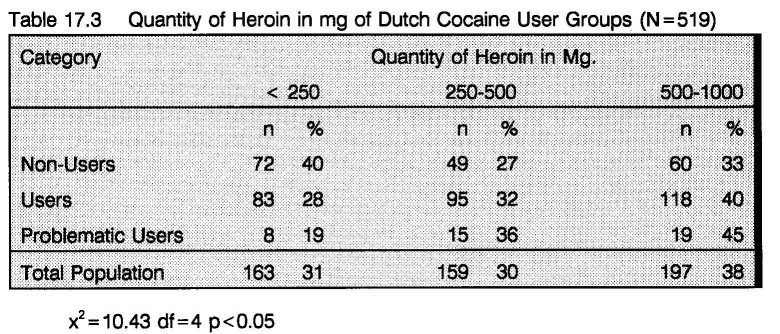
To assess the relationship between cocaine use and level of heroin use in the two groups, these variables were cross-tabulated for the Dutch and Surinamese heroin users separately. Tables 17.3 and 17.4 present the results of this procedure. Comparison of these tables first of all supports the suggestion that differences in heroin use are related to cocaine use. The patterns of heroin use of the Dutch and the Surinamese non cocaine users follow a rather similar distribution, corresponding with that of the total group of non-users (see table 7.1 in chapter 7.2.2). In both groups, almost 3/4 of the people use either less than 250 mg (low level) or between 500 mg and 1 g (high level), with the Dutch displaying a somewhat higher prevalence of low level use. About 1/4 uses 250-500 mg (middle level).
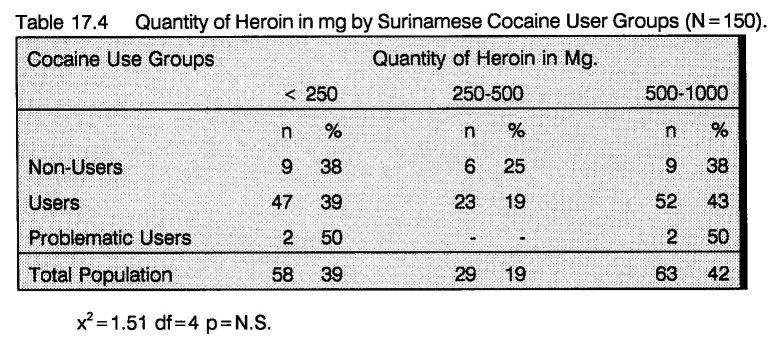
These results also seem to confirm the cocaine/heroin patterns observed in the field study. Among Dutch cocaine users a gradual increase in heroin use can be observed --the middle and to a greater extent the high level increase, while the low level group decreases (pattern I). When Dutch users take cocaine, they counter the negative side effects of this stimulant with increasing doses of heroin. In the Surinamese group the high level increases considerably and the low level slightly, while the size of the middle group strongly decreases. When taking cocaine, Surinamese users either use much (pattern I) or little heroin (pattern II). Thus, a large number of cocaine taking Surinamese heroin users can do so without increasing their use of heroin as well.
Recapitulating, the results of this comparison suggest that Surinamese users more often use cocaine, but experience less problems with the use of this drug, even without employing the typical subcultural self-medication procedures, involving increased heroin use.
The results of these secondary analyses correspond largely with the analysis of the fieldwork data. The results presented in chapter five suggested that users, who are successfully involved in dealing are in a better position to exercise control over their drug use (and have strong incentives to do so), suffer less from cocaine related problems and depend less on the heroin controls cocaine ritual as they use much more cocaine than heroin (pattern II). Indeed, this correspondence can be understood by the relatively high involvement of the Surinamese users in consumer level drug transactions. Although all ethnic groups in this study were, to some extent, involved in consumption level dealing, the Surinamese dominated retail dealing, occupied the key positions in multi-ethnic crews, and had the best connections with the middle level suppliers, as these positions were often held by Surinamese also. Suppliers contacted during the field work were all Surinamese males, who abstained from heroin use. Several recent studies confirm the relatively higher involvement of the Surinamese in dealing. (5 6 7 8 9 10 11) For example, in the study by Grapendaal and colleagues 55% of the dealers were Surinamese, whereas these only comprised 19% of their sample. (5)
The suggestion that it is their higher involvement in dealing which enables the Surinamese users to exercise control more efficiently is examined in the following section in terms of availability, life structure, and rituals and rules.
Determinants of Drug Use Self-Regulation
Drug Availability
Maintenance of the high use levels typical in the population under study requires a sufficient availability of drugs and the necessary funds to finance this. Legal income is normally insufficient to cover high drug use levels. In general, the resources required can therefore only be generated through prostitution (which is not illegal in The Netherlands) or illegal activities, such as acquisition crime or (mostly consumption level) drug dealing. Success in one of these hustles is thus an important condition for maintaining high use levels. In the Dutch context the most lucrative hustle is dealing. Consumption level drug transactions are tolerated to a large degree. In contrast, stealing has become more difficult over the years, partly due to increased property protection. The heroin using population in The Netherlands is furthermore aging and criminal careers become too demanding for long-term and older users. (5) Not only are they fed up with the stressful daily pursuit of money, their skills (in terms of e.g. physical condition and appearance) have also deteriorated.
Similar factors may influence the earnings of users involved in (street) sex work. The number of johns and the price for the sexual service may vary with daily fluctuations in weather, physical condition (e.g. signs of withdrawal), genital infections, periods and pregnancies (women only), and seasonal and event specific influences, such as Christmas or football matches. (12) Deterioration of appearance as a result of aging, poorly managed drug use and lifestyle is of major economic concern for sex workers. A successful hustle in crime or prostitution is therefore reserved for only a minority of users. Given the Dutch conditions, successful users --in terms of being able to consume (high quantities of) drugs without experiencing the, often axiomatically with drug use associated problems-- will thus most likely be involved in dealing.
Drug Availability Influences the Nature of Rituals and Rules
Drug availability has thus a pivotal impact on the daily lives of regular drug users. Artificially limiting the availability of drugs may limit their intake of drugs to a certain degree, but at considerable (psycho-social) expense. Apart from creating a strong economic incentive for the sale of drugs in unregulated entrepreneurial circuits, restricting availability induces and fuels a psycho-social process, which greatly multiplies the ritual value of drugs --ushering in a narrowing of focus in the user. Fixation on the drug will lead to strong limitation of behavioral expressions when the drug is craved and difficult to obtain, and to impulsive indulgence when a dose becomes available. As a result, rituals and rules around the drug become less directed at self-regulation and safety in the sense of health, but more at safeguarding, covering and facilitating drug use and the related activities (e.g. drug transactions) itself. (13) In contrast, the absence of uncertainty as to the whereabouts of the next dose liberates the user from the recurrent obsessive worries with (obtaining) the drugs and the necessity to chase them. Sufficient availability thus creates a situation in which rituals and rules can develop which restrain drug use and induce stable use patterns. As the results indicate, this does not necessarily mean lower levels of drug use. When the drugs are sufficiently available, the studied users can seemingly sustain high consumption levels, without developing typical drug related problems.
A sufficient drug availability can therefore be understood as a precondition for the development and effectivity of rituals and rules that regulate the patterns and levels of use.
Life Structure
An equally important condition is that the availability of drugs is stable. This requires that the hustles users engage in to generate drug money are successful on a stable basis. Recently Faupel constructed a typology of heroin users, based on a cross-classification of drug availability and life structure --which refers to "the regularly occurring patterns of domestic, recreational, work, and criminal activity that shape and constrain the daily life of heroin users". (3)
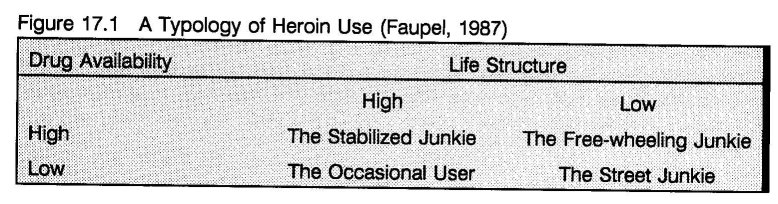
Faupel used this typology to explain the maintenance and breaching of the ethical standards of the heroin subculture by individual heroin users. An important finding of his research was that the careers of users who were able to uphold their ethical standards were not only characterized by a high availability of drugs, but also by a high degree of life structure. (3)
Faupel emphasized the regular activities (both conventional and drug use related) that structure daily patterns as key determinants of life structure. (3) It seems logical to include people's connections, commitments, obligations, responsibilities, goals, expectancies, etc.. Relationships and aspirations that are demanding, and simultaneously have value in social (e.g. affection) or economical (e.g. income) ways are equally important determinants of life structure. Regular contacts with controlled and non-users are therefore of considerable importance, as is participation in structures and activities not (primarily) driven by drug related incentives.
Life Structure and the Stability of Drug Availability
Faupel's findings suggest that, although a high drug availability is essential for the development of social controls, without a stable life structure it only offers them limited support. The importance of life structure is most clearly demonstrated by its absence as represented by the free-wheeling junkie (Figure 17.1). A sudden rise in availability of drugs or money --a big sting-- interferes with or undermines the daily, and largely fixed pattern of (both conventional and drug) activities, and may result in a sharp escalation of drug use. When then drugs and money are finished, the user very often finds himself in a worse position --habituated to a higher consumption level, while the connections required for a steady generation of income have been neglected. (3) The account of Assad in chapter 5.5 offers a perfect illustration.
Several recent Dutch studies documented a differentiated image of the heroin user that is only poorly compatible with the stereotype of the uncontrolled junkie. These studies indicate that the life structure of an increasing number of heroin users bears a considerable resemblance with that of their non drug using unemployed neighbor in terms of time allocation and social activities. (14 15 16 17) Many heroin users maintain a considerable number of non drug-related connections. Apart from family ties, one third to 40% share their housing with non-users (including partners), while one third to 40% of friends and acquaintances are non-users. (6 17) The typical (if one can speak in such terms) heroin user is ± 30 years old and spends more time on watching TV, than on chasing drugs, while the main income source is the social security system. (5 6 14 18) Methadone forms the basis of the drug menu and the amount of drugs he uses is more determined by the available resources than vice versa. (6 15) When involved in criminal activities he tries to uphold relatively high ethical standards characterized by a dislike of violence. (5) This depiction seems to represent the most common end phase of a long (> 10 years) heroin career and is significant for the aging population.
Using the concept of deviant career, Grapendaal et al. used the term normalized user for this type of user. In their study they furthermore distinguished the dealing user and the criminal user. Both these types used more cocaine and heroin than the normalized user. Their study suggest that the dealing user is a rather persistent type, while the criminal type is more often a phase preceding the normalized user -- at some point in the career this lifestyle becomes too demanding and the user calms down. (5) Another outcome may lead to a fourth type: the marginalized or down and out user, who lost the skills to make money, is often homeless, cut off from most former contacts, and troubled by intensive psychological problems begs other users for a mazzeltje (a taste) or searches the street for crumbs.
This picture is largely in line with the conclusion of 17.3.1. Maintaining the demanding life structure of the successful criminal is only reserved for a limited number of users, during a limited period of time. When the necessary skills and resources are exhausted, the user either retires or marginalizes. In the first case, self-regulation strategies increasingly depend on activities that help the user to abstain from or, minimize use of illicit drugs, supported by regular use of methadone. In the latter case, the conditions to do so are absent. The durability of the dealer type, at the other hand, signifies a comparably stable pattern of relatively controlled use of heroin and cocaine, as part of a highly structured entrepreneurial career.
Consumption level dealing can, indeed, be compared with any other small retail business, in particular with a small street or market vendor. Successful dealing is primarily a matter of good shopkeeping and obeys similar economic demands and rules. At the end of each day the small retailer must have earned the money to pay for his stock for the next day, the wages of employees, other business costs and the costs of living. When it was a good day or week, the surplus income can be invested or spent on luxury goods. This little entrepreneur must have a good sense of his financial position. So must the small dealer:
He counts the money and studies a list with numbers. Then he says, "Well, we made a small profit after all now."
Such simple bookkeeping has been observed several times. Just as his fellow marginal, but less criminalized colleague the small dealer does not normally have large (financial) reserves and therefore small mistakes can have major consequences:
Harrie complains that business is going bad last days. "Yesterday we lost ¦400.- on the dealing. We forgot the scale so that I had to do the weighing without."
A few more mistakes and the dealer is out of business. A successful dealer works often on fixed hours, with a stable team of employees and keeps precise track of the financial balance. He can, for example, not afford himself to show up at the dealing place at random times, unless he has monopoly power. But this is not the case in Rotterdam. The Rotterdam consumption level market for heroin and cocaine is in essence an open market with considerable, but generally peaceful competition. Besides a certain degree of commercial skills, a product of reasonable quality and the will to sell on tick and give betermakertjes and mazzeltjes (tastes) to regular customers in need, successful entrepreneurship requires stability and continuity. Such stipulations substantially structure the time allocation of those successfully involved in dealing.
Rituals and Rules
Maintaining scheduled activities and fulfilling social obligations, etc. --thus maintaining a stable, high degree of life structure-- requires rather careful management of drug consumption and related activities. Such management is dependent on the development of, and compliance with, rituals and rules. (1) In The Netherlands, heroin users have developed rituals and rules to control the use of this drug in the course of twenty years of collective experience. Compared with the situation abroad, heroin users in The Netherlands experience relatively minimal repression. This, and the easy accessibility of the heroin substitute methadone, have been indispensable facilitators of the social learning processes that facilitate controlled drug use. Of course, this process has not been complete. A majority of the users in this study still experience problems with heroin. One reason is that heroin remains a very expensive drug, inducing availability problems. Likewise, there are almost no models of controlled heroin use available. Furthermore, people are socialized into heroin use in the context of a subculture that was formed under more repressive and unstable conditions. The addition of other drugs to the daily use patterns also complicated self-regulation processes.
In particular, the nesting of cocaine in these heroin rituals disrupted the process to a considerable degree. But cocaine did not stop the pursuit for control. Adaptation to the changed pharmacological factor in Zinberg's concept (from heroin to cocaine) is a prominent feature of the current cocaine/heroin patterns. However, the combination of cocaine's pharmacology, high use frequencies and rapid delivery systems, results in subjective availability problems, which considerably burdens the adaptation process. It is therefore expected that the first signs of adaptation to cocaine will be found among users who have comparably easy access to cocaine and heroin, and a high degree of life structure.
Again, this points in the direction of users involved in dealing. Not only their position provides the conditions required for their development and maintenance (sufficient level of drug availability and the degree of life structure to maintain it on a steady basis), dealing also provides the incentive to comply with regulatory rituals and rules. Controlling ones drug use during working hours is a prerequisite for successful participation in the drug trade. Leisure time drug use may likewise not interfere with occupational stipulations and it must thus also be contained by similar social controls.
Of course, not only their privileged dealing position enabled the Surinamese users to better regulate their drug use. Several, partly related, factors further supported stability. For example, Surinamese users often exert rather intense social pressure on each other to remain in control. (10 19) To a certain extent, social control is also exercised by non-using partners and family. (20) The Winti folk religion may add further restrains. (20) Thus, in particular in the domains of life structure and ritual and rules, Surinamese users experience additional controlling factors.
A Feedback Model of Drug Use Self-Regulation
The DARRLS-Trinity: Drug Availability, Rituals and Rules, Life Structure
The dealers' higher level of self-control can now be explained as an example of the interaction between drug availability, rituals and rules, and life structure. The high drug availability of dealers is evident. Regular involvement in drug selling also provides the necessary degree of life structure. Successful consumption level dealing is subject to similar economic demands and rules as any other small retail business. It provides the structured activity, while relating with customers, crew and wholesale suppliers engender demanding connections, commitments, obligations, responsibilities and expectancies. Thus, the stipulations of successful entrepreneurship structure the time allocation of those involved in dealing to a large extent. To maintain dealing activities successfully, the dealing user must regulate his personal use, so that it does not interfere with (the schedules and demands that contribute to) taking care of business. Such rituals and rules can only develop under the condition of sufficient drug availability.
Drug availability, rituals and rules, and life structure must thus be considered in coherence. The continuity of drug availability is dependent on the stability of life structure which results from rather strict compliance to the rituals and rules regulating patterns of drug use. Because availability is a precondition for the development and maintenance of regulating rituals and rules, the following hypothetical model can now be formulated:
Drug Availability, Rituals and Rules, and Life Structure are a trinity --interactive factors in an internally coherent circular process, in which these factors are themselves modulated (modified, corrected, strengthened, etc.) by their outcomes. It is thus a 'feedback circuit' that determines the strength of self-regulation processes controlling drug use.
This model --the DARRLS-Trinity-- is graphically represented in figure 17.2.
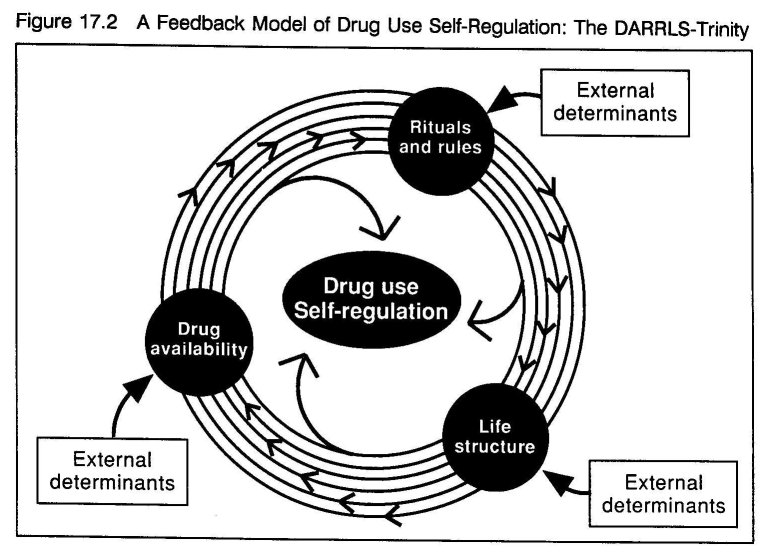
Rituals and rules determine and constrain the patterns of drug use, preventing an erosion of life structure. A high degree of life structure enables the user to maintain a stable drug availability, which is essential for the formation and maintenance of efficient rules and rituals. Self-regulation of drug consumption and its (unintended) effects is thus a matter of a (precarious) balance of a circularly reinforcement chain.
External Determinants of the DARRLS-Trinity: Effects of Drug Policy
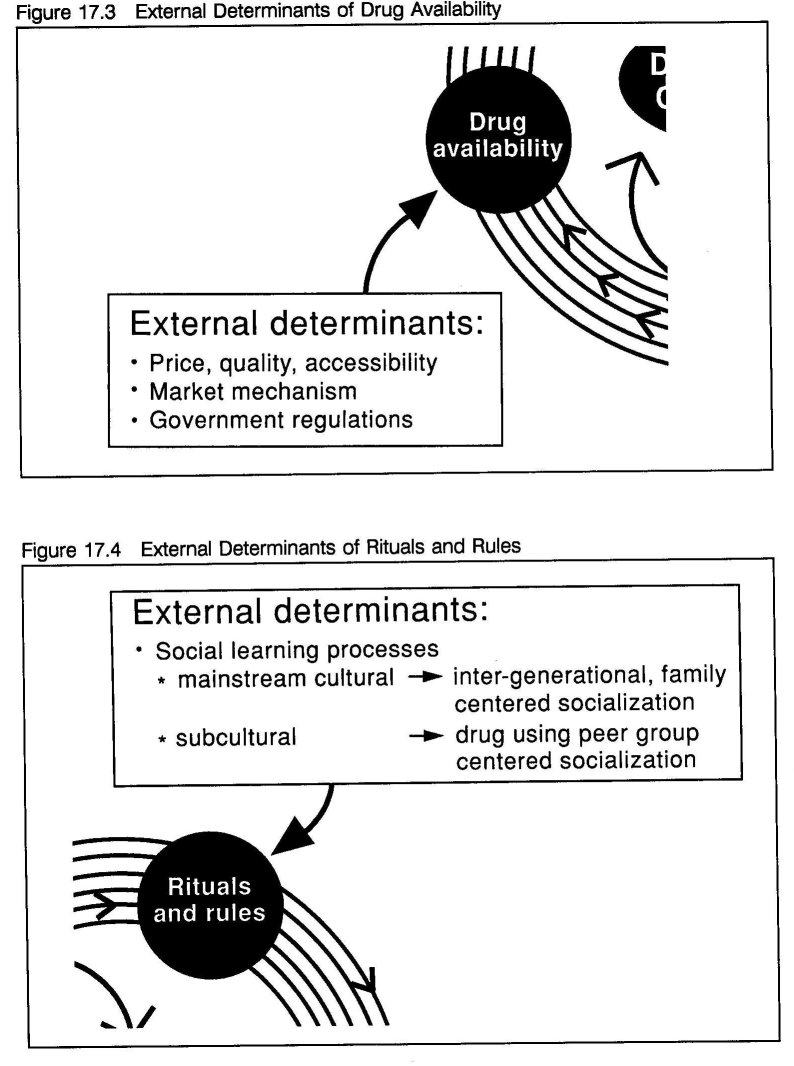
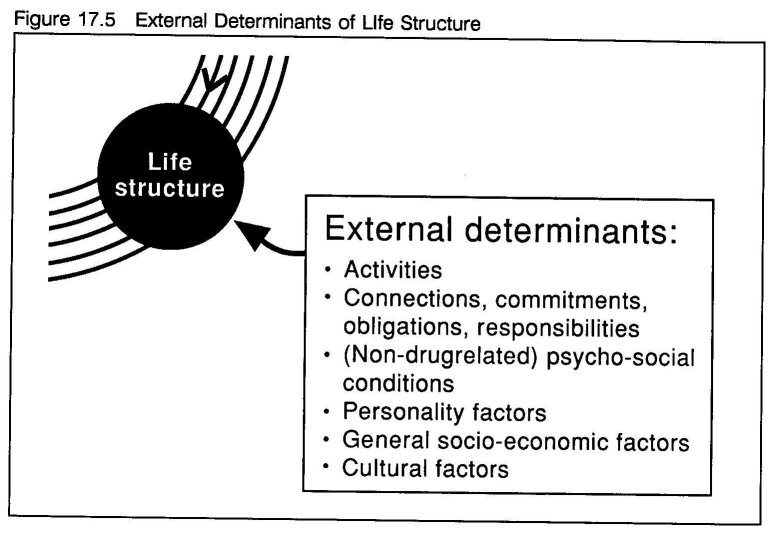
Although this feedback model is circular, it is not a closed and independent circuit. The three cornerstones of the feedback model are each the result of distinctive variables and processes. Drug availability is determined by price, purity and accessibility, which are mediated by market factors and governmental regulations. (figure 17.3) Rituals and rules are the product of culturally defined social learning processes. (figure 17.4)
The shape and degree of life structure are the product of the regular activities, relationships and ambitions which may be drug related or not. General socio-economic factors and actual living conditions, personality structure and the prevalence of (non drug related) psycho-social problems, and cultural factors may further determine life structure. (figure 17.5) Clearly, external stimuli can impact on the feedback system, in particular on its ability to support controlled and adjust uncontrolled use.
The social definition of drugs and their users, embodied in drug policy, can be seen to affect the model at all three cornerstones. Excluding alcohol and tobacco, most, if not all current drug policies are based on some degree of prohibition, rooted in criminal law. (21) Legalization is a term that is often used to represent the opposite of prohibition or the situation this term refers to. What is actually meant with the words prohibition and, especially legalization is not always evident. The words are often used in quite a holistic sense --not infrequently functioning as a smoke screen. The latter is then lumped together with related but distinct concepts such as decriminalization and normalization, whereas the former gets equated with the war on drugs. (21)
According to Webster's New World Dictionary (22) the word prohibition originates from the Latin word prohibitio and refers, besides to the 1920-1933 U.S. federal ban on beverage alcohol, to 1. "a prohibiting or being prohibited" and 2. "an order or law forbidding something to be done". The word is a derivative from the verb to prohibit, which Webster's describes as 1. "to refuse to permit; forbid by law or by an order" and 2. "to prevent; hinder". Prohibition forbids, or commands individuals to refrain from, certain action or behavior. Drug prohibition commands people to refrain from the use of drugs, based on the premise that use of these substances is unacceptable. It is, however, obvious that a considerable number of people disagree with this point of view and consequently disobey such commands. In that respect it is clear that only the weaker connotation (to hinder) of the second meaning of the verb is applicable, as drug prohibition does not prevent drug use. Note that, although often implicitly assumed, prohibition is more a process than an unequivocal phenomenon, as both historically and geographically considerable variations can be found.
Legalization, or the L-word as it nowadays is often euphemistically referred to in American discussions on drug policy, also refers to a process: According to Webster's the term means "to make legal or lawful". The word is derived from the adjective legal which originates from the latin word legalis, meaning 1. "of, created by, based upon, or authorized by law" and 2. "in conformity with the positive rules of law; permitted by law". Legalization is thus a process that reacts upon and seeks to abolish the prohibition of drugs, which is perceived as a failing and counter-productive process. (23) Legalization is not the alternative or opposite of prohibition, but merely paves the way for alternative drug control policies, outside of criminal law, which are expected to be more successful. Beyond this, the term does not entail any information on the nature of such policies.
Clearly, both terms give rise to confusion and various interpretations. Drug prohibition does not necessarily mean a total war on drugs and legalization is not a synonym for free, uncontrolled availability of drugs --the terms do not represent a factual dichotomy and may, indeed, be merely expressions of the academic argot of the advocates of the competing perspectives in the drug debate. (21) Despite the preceding linguistic discussion, prohibition has come to symbolize the (variably enforced) illegal status of drugs, while legalization denotes the opposite state, in which drugs are legal. While this imposed dichotomy bears some obvious risks, it can serve the present investigation of the effects of drug policy on the DARRLS- Trinity, when its limitations are kept in mind. Therefore, figures 17.6 to 17.9 present such dichotimized representations of the continuum from prohibition to legalization.
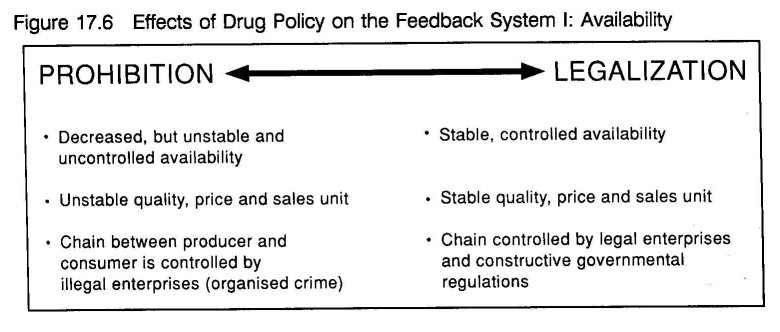
Given the socio-political conditions of drug prohibition it is evident that availability is the weakest link in the chain as prohibition artificially limits drug availability. (figure 17.6) Prohibition may obstruct the possibilities for drug use to a certain degree, thereby limiting general prevalence. It has, however, been argued that this, so called, deterrence effect of prohibition primarily reinforces already existing anti-drug attitudes. (21) But prohibition induces a broad spectrum of reactions from users, aimed at circumventing its effects and provides the economic incentive for unregulated entrepreneurial ventures --prohibition turned drugs into a highly profitable commodity. While its aim is to make drugs unavailable, it has only created an uncontrolled availability. Overall the availability of drugs may be lower, but in situations, specific neighborhoods and sub-populations which are more susceptible drug availability is actually much higher. This may well be a main factor in the spread of drug use. (24 25)
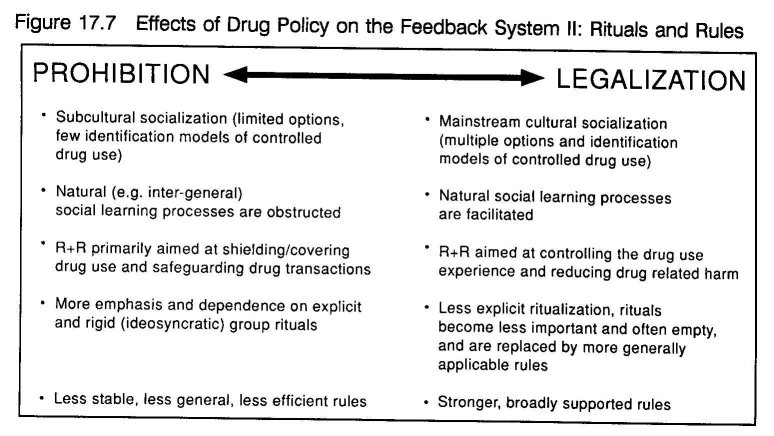
Prohibition affects the formation of rituals and rules as it obstructs and interferes with natural social learning processes by which most aspects of social (appropriate) behavior are conveyed. (figure 17.7) The social controls that regulate substance use can be rooted in mainstream culture, as is for example the case with alcohol. The rituals and rules that sanction controlled alcohol use are mainly determined by general family centered (inter-generational) socialization processes, which offer socially acceptable models of alcohol use and reinforce moderate use. In the case of illicit drugs the efficiency of these primary socialization processes is severely damaged. As a result, rituals and rules surrounding illegal drug use largely depend on subcultural or peer group socialization, characterized by a larger emphasis and dependence on idiosyncratic and rigid rituals and only limited applicable rules. These rules and rituals will primarily reinforce those behaviors which constitute the raison d'être of the subculture.
Prohibition likewise impairs the life structure of drug users. (figure 17.8) The user must participate in criminalized drug-driven networks to secure a steady supply of drugs. In these social networks he will relate with uncontrolled drug users. An increasing part of the activities will be centered around the acquisition of drugs. Meanwhile, secret drug users must manage to live double lives, as prohibition fuels stigmatization and ostracism when users are recognized as such. (26) Once labeled a junkie (all drug users are junkies), other undesirable traits are automatically attributed --criminal, unreliable, dishonest, pitiful, violent, etc.-- and this prevents and overrules the identification of more positively valued labels. (27)
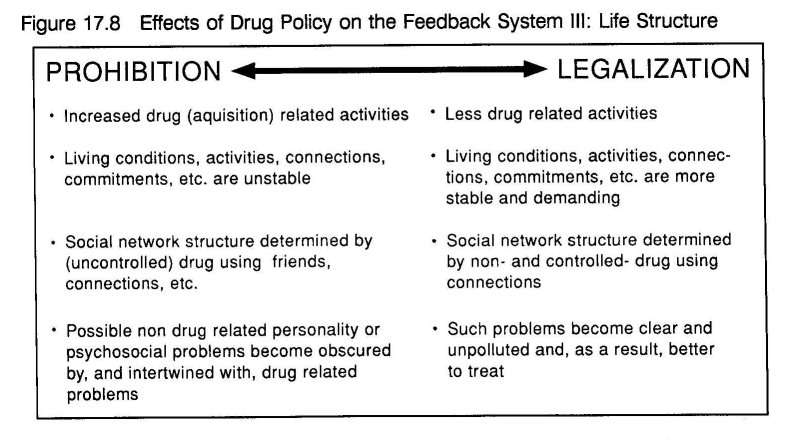
This results in the reduction of connections with non drug users, as both parties experience stress in interacting. It also obstructs contacts between controlled users, as they all fear disclosure. (26) Public knowledge of drug use may even lead to disproportional sanctions -- loosing a job or expulsion from school, denial of general (mental) health care and relegation to specialized care systems which are often combined with intense social control, eviction from ones housing, confiscation of possessions, imprisonment, etc.. The stigmatized junkie identity impedes participation in conventional roles and groups and progressively changes the lay out of day-to-day activities and the nature of relations.
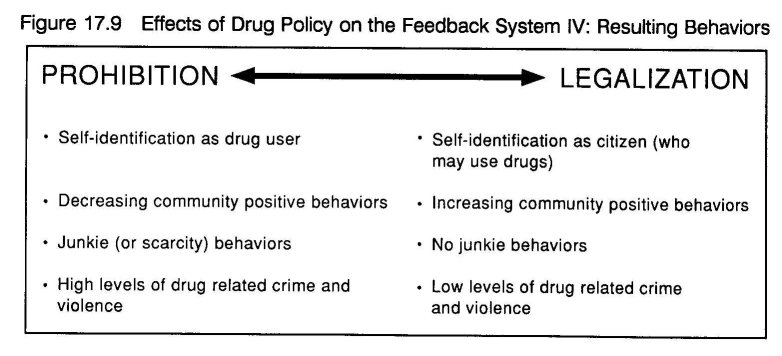
It can thus be concluded that prohibition interferes with the natural processes underlying self- regulation. It generates and reinforces the stereotypical negative image (junkie, criminal, violent) and related behaviors, which are generally related to drug use per se. (figure 17.9)
It is evident that the use of intoxicants, even of those often referred to as hard drugs, does not inevitably lead to uncontrolled or harmful patterns of use. Just as with many other intensely pleasurable experiences, the use of intoxicants may become the predominating activity. Drug use is, however, rarely an isolated activity. Intertwined with many other aspects of life, it is normally a social activity. Drug use patterns --which drugs people use and how they use them- - are subject to a multitude of social determinants, such as availability, trends and cultural patterning. Therefore drug use cannot be isolated from its social context. As Zinberg argued, control over the use of drugs is mainly determined by social variables. The presented feedback model of drug use self-regulation provides an interesting framework for the future study of the interactions between drug use behaviors and the factors that determine its social context.
- Zinberg NE: Drug, set, and setting: The basis for controlled intoxicant use. New Haven: Yale University Press, 1984.
- Harding WM, Zinberg NE: The effectiveness of the subculture in developing rituals and social sanctions for controlled drug use. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 111-133.
- Faupel CE: Drug availability, life structure and situational ethics of heroin addicts. Urban Life 1987; 15(3,4): 395-419.
- Toet J: Het RODIS nader bekeken: Cocainegebruikers, Marokkanen en nieuwkomers in de Rotterdamse drugshulpverlening rapport 87. Rotterdam: GGD-Rotterdam e.o., Afdeling Epidemiologie, 1990.
- Grapendaal M, Leuw E, Nelen JM: De economie van het drugsbestaan: Criminaliteit als expressie van levensstijl en loopbaan. Arnhem: Gouda Quint, 1991.
- Korf DJ, Hogenhout HPH: Zoden aan de dijk: Heroinegebruikers en hun ervaringen met en waardering van de Amsterdamse drughulpverlening. Amsterdam: Instituut voor Sociale Geografie, Universiteit van Amsterdam, 1990.
- Hoekstra JC: Handelen van heroïnegebruikers. Effecten van beleidsmaatregelen. Groningen: RUG, 1987.
- Korf DJ, Kort M de: Drugshandel en drugsbestrijding. Amsterdam: Criminologisch Instituut Bonger, UVA, 1990.
- Gemert F van: Mazen en Netwerken: De invloed van beleid op de drugshandel in twee straten in de Amsterdamse binnenstad. Amsterdam: ISG, 1988.
- Janssen O, Swierstra K: Heroinegebruikers in Nederland: een typologie van levensstijlen. Groningen: Kriminologisch Instituut, 1982.
- Swierstra K, Janssen O, Jansen JH: Heroinegebruikers in Nederland deel II: De reproductie van het heroinegebruik onder nieuwe lichtingen. Groningen: Criminologisch Instituut, Rijksuniversiteit Groningen, 1986.
- Gelder PJ, Kaplan CD: The finishing moment: Temporal and spatial features of sexual interactions between streetwalkers and car clients. Human Organization 1992; 51(3): 253-263.
- Carlson KA: Identifying the stranger: An analysis of behavioral rules for sales of heroin. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 191-206.
- Kaplan CD, Vries M de, Grund J-PC, Adriaans NFP: Protective Factors: Dutch intervention, health determinants and the reorganization of addict life. In: Ghodse H, Kaplan CD, Mann RD. (eds.): Drug misuse and dependence. London: Parthenon, 1990: 165-176.
- Swierstra K: Drugscarrières, van crimineel tot conventioneel. Groningen: Rijksuniversiteit Groningen, 1990.
- Korf DJ, Mann R, Aalderen H van: Drugs op het platteland. Assen/Maastricht: Van Gorcum, 1989.
- Korf DJ, Aalderen H van, Hogenhout HPH, Sandwijk JP: Gooise Geneugten: Legaal en illegaal drugsgebruik (in de regio). Amsterdam: SPCP Amsterdam, 1990.
- Korf DJ: Jatten alle Junkies? Tijdschrift voor Criminology 1990; 32(2): 105-123.
- Grund J-PC, Blanken P: From 'Chasing the Dragon' to 'Chinezen': the Diffusion of Heroin Smoking in the Netherlands. Final Report. Rotterdam: Instituut voor Verslavingsonderzoek (IVO), 1993.
- Gelder PJ van, Sijtsma JH: Horse, coke en kansen: Sociale risico's en kansen onder Surinaamse en Marokkaanse harddruggebruikers in Amsterdam. I Surinaamse harddruggebruikers. Amsterdam: Instituut voor Sociale Geografie, UvA, 1988.
- Wijngaart GF: Competing perspectives on drug use: The Dutch experience. Amsterdam/Lisse: Swets and Seitlinger, 1991.
- Guralnik DB et al.: Webster's New World Dictionary of the American Language, second college edition. Cleveland/ New York: William Collins + World Publishing Co., Inc., 1974.
- Nadelmann E: Impasse in drug policy: What are the options? Keynote address at the third International Conference on the Reduction of Drug Related Harm, Melbourne, Australia, 23- 27 March, 1992.
- Hughes PH: Behind the wall of respect: Community experiments in heroin addiction control. Chicago: University of Chicago Press, 1977.
- Hughes PH, Crawford GA: A contagious disease model for researching and intervening in heroin approach. Addictive diseases 1972; 2: 149-155.
- Goffman E: Stigma: Notes on the management of spoiled identity. New York: Simon and Schuster, Inc., 1963.
- Becker HS: Outsiders: Studies in the sociology of deviance. New York: The Free Press, 1973.
| < Prev | Next > |
|---|