| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4.1% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 180 |
| Yesterday: | 251 |
| This Week: | 180 |
| Last Week: | 2221 |
| This Month: | 4768 |
| Last Month: | 6796 |
| Total: | 129367 |
DRUG USE AS A SOCIAL RITUAL
 |
|  |
| 
| Books - Drug Use as a Social Ritual |
Drug Abuse
DRUG USE AS A SOCIAL RITUAL
Social Drug Use and Social Structure
With other humans, users of heroin and cocaine share an overriding need for warmth, contact, interaction, (group) identity and social solidarity (1, 2). In that respect they do not differ much from users of other drugs, such as tobacco, alcoholic beverages and cannabis products. Group use of drugs (legal or not) is a universal practice (3) to initiate and potentiate situations that satisfy the above needs by engendering feelings of togetherness, identity and solidarity. Social drug use serves as a social lubricant and thus as a ritual binding mechanism (4, 5). An important difference can be found in the status of the drugs and the legally sanctioned opportunities offered for their use. Some drug use is integrated in culturally defined and legally sanctioned social structures, built on a history of experience with use and misuse. Tobacco can be used in almost every social group or gathering (although there is a recent trend to limit smoking in public places, e.g. by forbidding smoking in administrative office buildings and creating smoke free zones in restaurants and trains). Group use of alcohol is an important feature of many human interaction, in particular at festivities, receptions, and in leisure time. Moreover, there are many designated places for alcohol use, e.g. cafes, bars and dancings. A well defined set of social controls has been developed surrounding the use of these two substances (6). In The Netherlands such provisions are even created for the use of the relatively new drug cannabis in the form of so called coffee shops that offer the opportunity to buy and use this drug. In an increasing number of cafes and dance clubs the use of cannabis is nowadays normalized.
For the use of illegal drugs, such as cocaine and heroin such venues do not exist. Society at large does not know how to deal with the use of these drugs and, as a consequence, does not provide its users with guidelines and models for socially accepted and controlled use of these drugs (7). Likewise, legally sanctioned or tolerated social structures for the use of these drugs are absent. This does, however, not mean that such controls do not exist. Nor does it mean that a social structure for the use of heroin and cocaine is absent.
The Social Structure of Illegal Drug Use
In addition to the processes described in chapter two (2.3.3, 2.3.4) the notion of social structure is also of importance for this study. A social structure can be defined as an ordered series of social relationships (being defined as existing between two or more individuals if there is some harmony in their individual interests) or a system of values (8). Undoubtedly, there is some harmony in the individual interests of users of illegal drugs and therefore each individual drug user has a value for the others. This will result in a community with similar interests or "an agreement upon certain recognized values" (8). In the drug using community these values include a positive attitude towards drugs and the associated patterns of use. But because of the illegal status, survival and secrecy will be equally important and these can sometimes conflict with the former two. The drug subculture can further be described as an adaptive mechanism which enables drug users to live an ordered social life in the environment given by the conditions of drug prohibition (9). Malinowski described this adaptive mechanism as two-fold:
"Firstly, there is the primary or external adaptation which consists in man's adjustment to his geographical environment and is motivated by his basic biological and physiological needs --the instrumental imperative. Secondly, there is the secondary or internal adaptation which is motivated by the integrative imperatives --that is, the necessity for harmonizing the conflicting needs and aspirations of man." "The former type of adaptation is evidenced in all the various economic, political, educational and legal activities of human beings. The latter type of adaptation is in fact the integration into normatively regulated social behavior of all such activities of man which his instrumental imperatives urge him to perform." "It must be emphasized that this adaptive mechanism (culture) is always end-oriented, the end being the satisfaction of man's primary and secondary needs; and furthermore, that each and every constituent of it has a definite form and function as determined and defined by the cultural context which in its turn is to be understood with reference to the social configuration to which it (the culture) belongs."
When this functionalistic perspective is applied to illegal drug use the instrumental imperative becomes clear --drugs. This basic need of drug users is thus the driving force of the subculture. As an adaptive response to a hostile environment --represented by mainstream society's drug laws and their enforcement-- drug users have developed their own specific channels to secure the relatively undisturbed use and acquisition of drugs. Moreover, the stigma (10) or deviant label (11) attached to the use of these drugs, thwarts participation of its users in conventional social structures, leading to increasing active involvement in the social structure formed around this stigmatized and deviant activity --the subculture. The universal need for interaction, solidarity and harmony --the integrative imperatives-- will then lead to the integration of drug use in a subcultural set of rules and rituals ultimately aimed at the maintenance of this social structure that is essential for the satisfaction of drug users' needs.
Social Rituals and Rules Surrounding Group Drug Use
And in fact, the preceding theoretical deduction is supported by the data as explicit rituals and rules have evolved around the most apparent need of drug users, in particular around use and acquisition of the preferred substances. Most of these rituals and rules are normally not explicitly defined. Seldom are they discussed by the research participants. When discussed, it is mostly when they are broken, in initiations, or in other special situations. They are part of the stock of knowledge that the experienced user utilizes in his everyday dealing with the social space he is living in. "The values [or rules] that prompt or sanction the performance of ritual are also ... the same values that motivate people in their everyday life" (12). Rituals and rules are often closely intertwined (13) expressing the same cultural elements, each one amplifying the other (14). For these reasons radical separations between the two can, in most cases, not be made (13).
Ritual Places --The House Address
Social drug use rituals are performed at places where drugs are sold, where people hang out, use drugs and socialize. Such places are important locales of the subculture. In Rotterdam most drug sales occur at house addresses, and at these addresses it is generally allowed to use the purchased drugs. Besides at house addresses people use at home, their friends homes, abandoned buildings and other public places. These places are also frequented to meet friends and socialize. Figure 9.1 shows where the observed drug administrations were recorded.
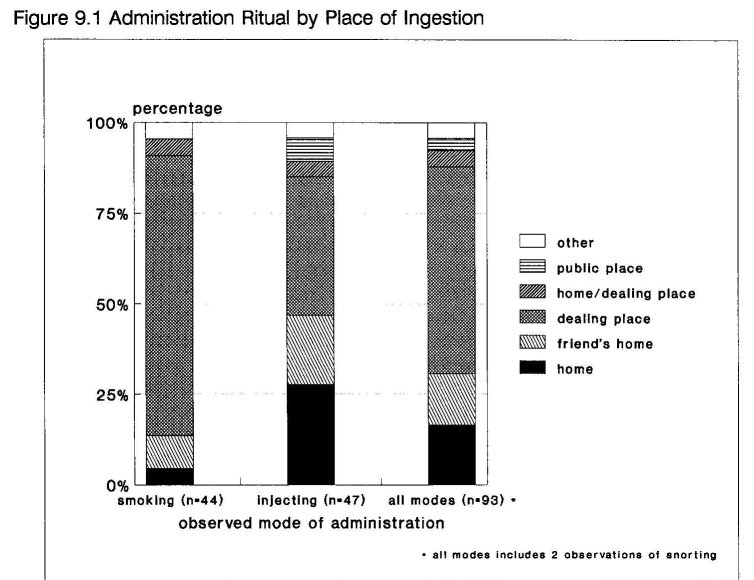
Although IDUs use their drugs much less frequent at house addresses (frequently they are not allowed) than smokers and more at home, a friends home, or in public places, it can be ascertained that house addresses in particular serve an important function in the social structure, as they combine two important elements --purchasing drugs and socializing with other drug users. The average house address is located in a rented house, or a squat waiting for renovation. The resident allows a dealer to sell at his place and in exchange he gets free drugs and sometimes some money. House addresses often move around. One user, who was involved in dealing, alternately as the dealer and as the one providing the place, called this a spreading of the risk to prevent police detections and busts.
The Rotterdam Police Policy Towards House Addresses
In Rotterdam many of the house addresses are actually known by the police. The places are sometimes visited by police officers, who come to look for a certain person, or to see what is going on:
Doug and Harrie report about a visit yesterday of two police detectives from the narcotic squad. Doug tells "They didn't do nothing, they made a nice chat. They saw Harrie busy with making a package for a customer. He was taking out cocaine from the bag with a knife and put it on a paper. They saw it and didn't do anything. They told Harrie to keep things quiet around here. And they were happy for me that I could make my dope by doing this. They said they had noticed, they hadn't seen me on the streets for some time, making my money. "It's better you stay here"; they told me". He continues: "What do you think what a difference it makes to me, socially and financially. I'm staying out of the hands of the police. Keep more money in my pocket, don't have to hustle all day, be out on the street constantly, etc". Harrie confirms that he feels the same way. He hasn't been dealing always, just a couple of months now. He says: "Now I can stay out of the criminal circuit through this dealing".
Apparently not only drug users make a distinction between consumption level dealing and the criminal circuit. It is evident that the house addresses can only exist by the grace of this pragmatic policy of the Rotterdam Police. This policy is based upon the Dutch national drug policy, that is not aimed at eradication of the drug problem, but at it's containment and management of drug-related problems (15, 16). At the local level this resulted in a policy that tolerates the use and sales of heroin and cocaine within certain, rather vague, limits. House addresses where these drugs are sold and used are often condoned as long as there is no trafficking in stolen goods, no sales of large quantities or too many customers and, related to that, above all, no unacceptable nuisance for the surrounding residents. This policy is also communicated to the users. In the following fieldnote the researcher witnessed a visit of a uniformed police officer to a house address, that was busted for dealing the week before. That morning, the residents of the place were released out of custody. While one of the residents prepares an injection of heroin, the policeman explains why the place was busted:
"It was because the neighbors had complained and it is the police policy to shut down dealing places when they cause to much nuisance." He warns Karel not to let another dealer start dealing again. "It is a question of our credibility to the neighborhood", he says. "Send addicts who want to buy drugs to Curly's place (which is a few blocks across the street). Let their neighbors have the trouble for a while. If it starts here again, we will crack it down immediately."
The explanation of this police officer reveals a core of the Rotterdam drug policy --reduction of drug related nuisance. It furthermore shows the awareness of the police of other dealing places --in this case at Curly's house.
The Organization of the House Address
A house address is normally ran by a dealer and his staff. The staff exists at least of a doorman and a guard to prevent robberies. Sometimes there are two guards, another person behind the weigher or a go for --someone who does shopping and delivers messages. In general, they are paid in drugs. Often the resident fills one of the positions. There are a few different types of house addresses. At the most common type drugs are sold and smoking the purchased drugs is allowed. At these places, smoking paraphernalia, such as aluminum foil, ammonia or baking soda and spoons (to prepare cocaine for smoking), toilet paper or tissues and water are supplied as a service to the customers. At a minority of house addresses injecting is allowed, generally, when either the dealer and/or the resident are IDUs. Often a separate room is designated for that purpose. At some places where injecting is permitted, injection paraphernalia and chemicals were available for common use, such as spoons, water, acid (lemon juice or ascorbic powder) and sometimes clean syringes and needles, which were supplied by a nearby outreach and needle exchange program (see chapter fourteen). Sometimes one can only use drugs bought elsewhere, because drugs are not sold at the place. There are no clear cut borders between these types and the situation can change from the one into the other, often depending on the people who run the place. There are no explicit charges, such as entrance fees or for the use of paraphernalia, which are normal in comparable American shooting galleries (17, 18, 19).
Most house addresses have a clear layout with the intended purpose to separate the dealing from the using so that the dealer can easily survey the situation (Figure 9.2).
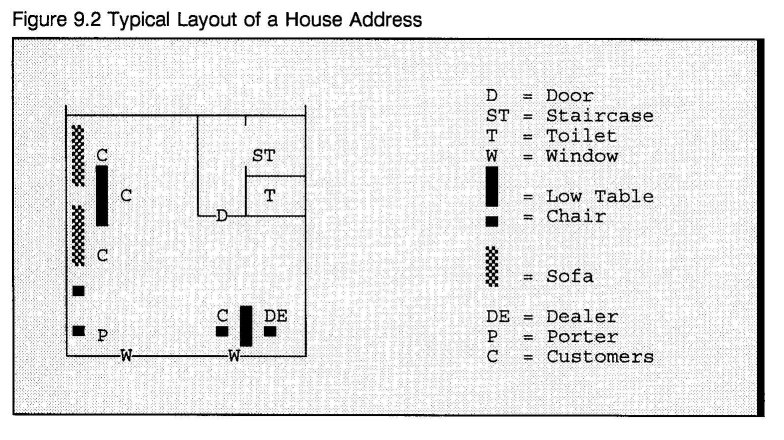
When the dealing and using happens in the same room, the table of the dealer typically stands in a corner, separated from the table or couch designated for using:
The dealing is taking place in the back room. At this moment Lottie, a Surinamese woman is selling. She sits on a couch that's standing against the window side. In front of here a low, square, white table. On the other side of the room stands another couch, in front of it a little wooden table with two more chairs around it. This 'corner' is used by the customers to smoke their dope.
Sometimes different rooms or even different floors are used.
Rules and Ritual Interaction at House Addresses
As a rule, only one or two customers are allowed to enter the dealing room or take place at the dealer's table at the time. When the transaction is completed the customer must leave this room or table. He can then either leave (IDUs often do) or take a seat at the for smoking designated area:
Someone is coming up the stairs. The guard asks the boy on the couch to leave. " 4 people up here is too much, we allow 2 customers at the same time in the attic room. The others have to wait downstairs. Normally you also can't use here, you have to do that downstairs."
From the guard's explanation not only the rule becomes clear, but also that it is not always equally applied. Friends, (very) steady customers and other high status users are often invited for a chat and a smoke at the dealers table:
Jack has just brought in a new client, who orders a quarter gram heroin. ... Lottie empties the scale by putting the heroin into a paper. ... She tells the new client that if he wants to smoke he has to go to the use corner on the other end of the room. ... In contrast, Jack is allowed to smoke at her table.
A further rule allows only for a certain number of people using their drugs at the place. This limit can vary by place and time. Most dealers are stern innkeepers. Unless he has a distinctive relationship with the dealer or the resident, the person that came in first is summoned to leave by the doorman or dealer (after a reasonable period of time) when the maximum number of people is reached. During the observations it was not observed that people disputed the basic premise of these two rules:
After a while Boris asks a customer to leave. The man says that he will after his chineesje is finished and so he does.
By limiting the number of people present, the dealer and his staff can not only survey and control the place to a greater extend, it also preserves a good atmosphere by preventing tension originating from hectic bustle. This is especially important when large amounts of cocaine are consumed. While drug use at house addresses is frequently characterized by a sociable pub-like atmosphere, when heavy cocaine use dominates the place communication often ceases and there is an imposed silence, as a consequence of the in chapter five described increased sensitivity for sound. Sometimes even the light is dimmed. As one experienced user explained a novice: "When shooting up cocaine, there has to be some rest and quietness for some time." Whether the drug is shot or smoked does not seem to make much difference. The next fieldnote was recorded at a dealing place where cocaine was smoked:
It's extremely quiet in the room. The doorman is the only one standing and walking around. The two windows at the street side have lace curtains. The low table stands on the left side of the room. Around it 10 users are sitting, one of them is the dealer who sits in the middle of the long end with his back against the wall. Everybody seems to be turned into themselves. No one talks with one another. All are smoking or have been smoking cocaine. They are all looking straight ahead into nowhere.
It is not unusual for the doorkeeper to point entering customers at a cocaine dominated atmosphere and ask for silence:
The door is opened by a girl, she's the porter and helps cleaning the place. She lets Nadir in, asking him to be relaxed because the people inside are smoking cocaine. In the room there is hardly a word spoken, everybody stays very calm and speaks with a low voice. If there is any conversation it's about the works on the table: "Can you give me the knife, can I have your lighter for a moment, is there some clean water", etc.
Such warnings are certainly not pointless. When disturbed in their rush cocaine users can get irritated:
Doug sits relaxed in an armchair and enjoys the cocaine rush. A few moments later two other users enter the room. They are noisy and uptight because the dealer has already closed business and left. The expression on Doug's face (who is still in his rush) hardens: "They're screwing up my 'flash'," he says, "Why must they be so noisy?"
Such a situation can be compared with rambunctiously entering a football canteen crammed with supporters who are all highly concentrated watching a cup finale on television. Then suddenly turning off the tv, while the star player of their national team is taking the decisive penalty. Such a loaded atmosphere can escalate into a sudden outburst of violence:
There is suddenly rumor coming out of the living room. For some time two Dutch users and a Moroccan are using there. One of the people that are waiting knows that they have been smoking cocaine the whole afternoon. That's why they're in that room, it's too crowded in here. Suddenly the sound of breaking glass. The waiting room floats empty, most of them go on to the street. The Moroccan boy jumped through the window. He was chased by one of the Dutch guys armed with a stick. The other Dutch tells: "He is 'para' from the cocaine, he wanted him (the Moroccan) to be quiet but he kept on waffling."
House rules are thus primarily directed at the smooth functioning of the house address --both internally and as part of the non-using community. The main objective is to secure the safe and undisturbed intake and purchase/selling of drugs. It can be determined that safety in this context has a double meaning --safe use, directly related to the intake of drugs and safety in relation to the outside. Examples of the former, such as smoking only (smoking is a safer mode with a very low chance of overdose), limited number of people present and silence when cocaine is smoked can equally be applied to the latter. For example, limiting the number of people present not only has a positive influence on the mutual interactions, it also makes the situation more controllable for the dealer and it limits the nuisance in the neighborhood, which limits the chance of detection and busts.
Ritual interaction around the actual purchase of drugs at house addresses is limited. There may be some ritual deliberations over the volume of drugs one receives for the money paid, the position of the balance on the scale or the respect one has to pay the dealer. In contrast, American research indicated elaborate ritual interaction in drug sales, aimed at the detection of undercover narcotics officers --often a customer has to shoot up in the dealer's presence to assuage (necessary) suspicion (20).
The most explicit social ritual revolves around the sharing of drugs. Both smoking and injecting are commonly done with other people present. The mean number of people present at the observed smoking rituals was 5.4, for injecting this was 3.3. In 50% of the observed drug administration rituals drugs were shared. The drug sharing ritual can be witnessed in many forms. Some approach the formal Durkheimian format (13), others resemble more the daily encounters or interaction rituals (21) Goffman referred to and Collins called natural rituals. (2) In the following examples the different forms can be observed.
The first example was recorded at the madhouse, a squat named so by its regular visitors. Until short for it's demolition, the place was inhabited by a transient group of older IDUs without regular housing. Harrie was one of the few people who lived on a permanent basis in the place and served as a manager:
When Ronald and Frits entered the room they had just bought drugs at another address. They wanted to shoot up fast. Frits took his spoon and lemon and put the spoon on the table. He then dribbled some lemon on the spoon. Ronald took two little paper packets out of his wallet. One contained two stripes of heroin the other contained one stripe of cocaine, as Ronald said later. Meanwhile Frits got a fresh syringe. In the house there mostly is a box of syringes and a sharpsafe container available. Frits went to a jerrican with water and with the syringe (without the needle) he pulled up some water. Then he poured a bit on the spoon. Ronald had already opened up the packets and put ± half of the heroin in the spoon. Frits heated the spoon with a disposable cigarette lighter. After the heroin had dissolved he stirred the solution with the safety cap of the needle. Then Ronald threw all of the cocaine into the heroin solution and stirred again. After removing the needle, Frits drew up the mixture with his syringe through a piece of kleenex. He put the needle back on and gave it to Ronald. Ronald fetched another syringe, took off the needle, redrew the piston and put the needle of the loaded syringe through the hub of the empty one. He then squirted about 1/4 of the solution into the reservoir. After putting the needle back on he gave the syringe to Harrie who offers them and other people facilities for shooting up and dealing. Ronald then repeated his action, using again a new syringe, but now he divided the remaining 3/4 into two even portions. One for Frits and the other for himself. Then they all took the fix.
As usual, Ronald and Frits share their jointly bought drugs. They inject a mixture of heroin and cocaine. Preparing a heroin/cocaine cocktail is a multi-stage and highly determined sequence, which requires a sufficient level of concentration and skills. One clumsy move and a shot can be spilled. Many users do not want to be disturbed while preparing a shot. Ronald and Frits conversely, prepare the shot together. Frits does the actual cooking, but Ronald determines how much heroin and cocaine is put in the shot and divides the solution. Frits carries the cooker and the lemon and Ronald carries the drugs. Moreover, Not only in the way they prepare and use them, but also in the way they buy drugs Ronald and Frits have a stereotypical pattern. Four weeks after the above observation one of the researchers was on a dealing address, observing the drug sales and use. There he ran into Ronald and Frits again:
Frits and Ronald came in. They came to score but Ronald started to talk to the researcher. After a few minutes, Frits, impatiently, took Ronald's wallet out of his hands. Then Ronald (a little agitated) said to Frits "As long as you know that it is my wallet." On asking, Frits replied that Ronald always buys the dope and he himself prepares the shots.
Ronald and Frits must be very confident about each other's actions. They perform the preceding preparation sequence with an explicit labor division as can be seen in the schematic breakdown of the sequence.

During this sequence there was hardly any conversation, no waiting or commands. They were both completely focussed on the task at hand. There was absolutely no ambiguity about the roles and tasks and both were well aware and certain about their own and their partner's role and focus. During the sequence they share one predominant goal --getting high. They can be said to share a common mood or emotion. Such a strong mutual focus of attention, without ambiguity or uncertainty about each other's role, combined with a common emotion are thought to be key ingredients of ritual, having a strong binding effect. (2)
And, in fact, Ronald and Frits have a strong and enduring relationship. They are a typical dyad or running mates --"a partnership of two best buddies or lovers, in which both participants implicitly understand the common benefits of the partnership". (22 23) Ronald described his relationship with Frits as follows:
"Frits and I are almost always using together, we do everything together. We are like brothers to each other, he is my half brother you know." "He is 41 now and I am 37; my father had a bit on the side then." "We don't share needles but I don't mind using the same spoon cause I'm sure that he won't share with someone else." "We're always together except when one of us is in jail."
Their common activities and the synchronicity of intense emotional experiences, such as drug induced euphoria and withdrawal secures their strong positive relationship. (19)
In the next fieldnote drug sharing takes a much more casual shape. The observation is recorded on a dealing address where a group of chasers was sitting around a table in a relaxed and sociable atmosphere:
Around the table are sitting three Moroccan males and the dealer. They are chasing some heroin. On the table are a role of aluminum foil, several lighters and a teaspoon with a white residuum on the edge. It is used to prepare cocaine for smoking, but currently only heroin is smoked. Then two other Moroccans enter the room. They greet the other present Moroccans and start a conversation in Arabic. One of them buys heroin ... and starts preparing for chasing. He does not have a knife and borrows one. With the knife he takes some heroin from the pack and puts it on his friend's aluminum foil. He also gives a little to the other men at the table.
At first hand this may seem an everyday and casual situation, but it has some definite ritual aspects. The ritual interaction in this fieldnote centers around two behavioral sequences directed at regulating the group interaction--the greeting and the sharing of drugs. The greeting ritual is a formal communicative procedure (24) and opens "a channel for communication and interaction" and it "defin[es] role and status", (25) in this case at an equal level. A conversation is started --a controlled and regular social situation (24) -- and one of the newcomers buys some heroin. He not only shares his heroin with his friend that came in with him but also with the others at the table. By sharing with the men at the table, the generous donor consolidates the good atmosphere, and shows that he respects them and in turn is worthy of respect. (21) The situation equals that of the familiar situation of giving a round in a cafe. As in any group, among drug users rituals are also directed at the regulation of normal day-to-day interaction under the given circumstances. (21)
Instrumental Functions of Drug Sharing
As in solitary drug taking rituals, much of the drug sharing ritual is also aimed at controlling the drug experience. The maximizing the drug effect function is expressed in pooling money and buying drugs in groups of two or more people. This is a regular practice among dyads and other friendship groups but sometimes this is also done by strangers who hook up temporarily for this purpose. In the following fieldnote a man ringed at a house where he thought to find a dealer. Jack, who squatted the place to sleep in tells him that the dealer has moved. Jack continues:
"But I know an other address. What do you want to buy ?", he asks the man. "I want to buy some heroin for ¦25.-" the man replies. Jack says "I've got some foreign bank notes, pounds, dollars. When I bring you to the address can you buy a 'kwart' (quarter gram) for ¦35.-? Then I'll give you the bank notes. The man agrees to buy a quarter and they leave together. ... At the address the man buys a quarter gram of heroin and divides the package in about 1/3 for Jack and 2/3 for himself.
In the Netherlands the illegal market in heroin and cocaine is not only dominated by the market mechanism at the higher levels of trafficking, but also at the street level. Therefore, pooling money results in more drugs for the same amount of money.
The drug sharing ritual is frequently aimed at preventing withdrawal. This is a common practice and users refer to it as helping one another.
Achmed tells he's sick and asks Nadir if he got something for him. Nadir says he's sick too and wants to use: "I'm not really sick yet, but it's pulling me. If you know a good address we can go there together and I will help you".
One helps a fellow user who is in need of a dose with a betermakertje (a little straight maker - -a small dose to ameliorate withdrawal). The term betermakertje is mostly used when asking a favor from a dealer. Helping does not only refer to preventing or ameliorating withdrawal, it can be extended to maintaining the desired level of intoxication. During the entire period of fieldwork the research team met few users in a clear state of withdrawal and it was observed that helping also referred to sharing cocaine.
The young man prepares the cocaine and shares it with his mate. One of the other men at the table who just finished his cocaine, asks him "Kun je een puntje voor me missen?" (Could you spare me a knife tip) The young one excuses himself for being not able to help him. But one minute later he grabs a knife from the table and takes a little bit of cocaine base of his foil to put it on the foil of the guy who had asked for it, saying: "Sorry, I can't miss more, we already have to smoke from it both".
Analysis of the observed drug sharing rituals shows that drugs were shared for several reasons, inherent to life in the drug subculture. Drug sharing is not only a ritual but also the rule among the research participants. The rule regulating the sharing of drugs can be broken down to the following subset of sharing rules:
1. Share drugs with your partner(s), friends and acquaintances.
The drug users that shared drugs were in most cases in some way related to each other, but the ties relating them often varied in strength and content. In 68% of the observed drug sharing events, they were mainly related through participation in the regular drug taking activities, as for example buying and using at the same dealing addresses (N = 93). At dealing places users meet friends and make new contacts. Moreover, the relations were often much more intense and multiplex, that is, drug users did not only frequent the same places to use and buy drugs, but were in more aspects related to each other. For example as sexual partners (9%), family (9%), or they lived in the same, sometimes squatted, house (5%). 23% of the sharing IDUs were involved in a dyadic relationship.
2. Share drugs with sick users; help them with a betermakertje
Although mostly practiced among friends and acquaintances, this rule takes drug sharing beyond the group of known users. It shows that knowing each other is not a condition per sé for drug sharing as the next gloss indicates:
"I met Karel last week at the Salvation Army. I didn't know him. But I was sick (in withdrawal) and he helped me out with some 'bruin'. That never happened to me before, a perfect stranger that's willing to help me."
Helping is a very strong rule. Even when one is not very eager to help a certain person, as the following excerpt depicts:
Jack starts to prepare a shot. When he is almost ready, Cor asks him for a little bit of the dope. first J. does not respond, but Cor persists: "Ah, Come on J. just give me a few drops" Jack does not seem pleased with the situation, but when he draws his shot through the cotton he does not take all the solution from the spoon and pushes the spoon to Cor.
The strength of this rule is demonstrated by the observation that some users actually procure the main part of their drugs by asking favors of fellow users, appealing again and again to the internalized rule that one helps a sick addict. However, only few of them are able to maintain the delicate balance. Sooner or later it will become obvious to their donors that they break rule three.
3. I help you now, later you will help me
Users help each other, expecting to get the same treatment when they need help themselves. A user who regularly shares some drugs with others has a larger chance of being helped than a user who is stingy with drugs. The reach of rule two is limited by the expectancy of reciprocity. Former reciprocity is often used as an argument when asking for a favor.
4. Share drugs in exchange for services
In the first situation presented above, besides splitting the drugs they bought together, Ronald and Frits share with Harrie, who offers them the facility to inject and gave them new syringes. They do not pay an admission fee for using his facility, nor do they pay for the syringes. However, they give Harrie a taste of their jointly bought drugs and doing so they follow rule four. Frequently users provide each other with small services in exchange for drugs or other services. Permitting other users to use in ones house is a frequently observed example. In general, these exchanges go without negotiations or explicit agreements. Providing services to others is for some users an important source of drugs, necessary to support their habit. Likewise, many users find ways to make some drugs working in various positions for a dealer --as doorman, security or go-for.
5. pleasing the dealer
When purchased drugs are consumed at the place of purchase, smoking users often share a little with the dealer. They put a knife tip of heroin or some cocaine base on the dealer's smoking foil. The aim of this gesture is to maintain a good relationship with the dealer in the hope that he will be considerate in times of short finances by giving a betermakertje. Some users, however, object strongly to this practice, such as Arie, an older IDU:
Arie says he would never beg a dealer for a little more dope. "[T]hat's against my feeling of self-respect, ... you got to take care for yourself. Some people will do almost everything to get the sympathy from the dealer, hoping they will get some privileges out of it, like buying on credit, getting good bags, some extra dope for free, etc. Some dealers exploit their position, they act like if they were God himself."
6. If you share, do it well
When drugs are shared, the donor must share in a way so that the recipient gets the impression that he is taken serious, as can be witnessed in the next fieldnote:
Before he goes on, he takes a little cocaine base out of the package he made, and puts it in another paper to give it to Lottie. When Lottie sees the little bit in the paper her eyes seems to shoot fire. Lottie: "You want to give me that. You insult me with that. If you can't miss anything today then say it to me, but don't give me this." The man says he is sorry and he will make it up with here next time.
Sometimes, appeals to share drugs are made when the user, who is being asked, feels he can not possibly help, as he does not have enough drugs or money. Then elaborate explanations are given why one is unable to help:
Numa asks Paco for his opinion, "What do you think Paco, last time I met him (he's pointing at a Moluccan user of ±35 years who is walking towards them.) I had Coke and enough money. He asked me to help him, which I did. Now he's asking again. I've got some Coke left but I'm out of money. So do you think it's strange I can't help him now." Paco first answers he does not want to interfere, but then he says "it's your business if you want to help someone or not, you know what you've got and what you can do with it." Numa turns to the Moluccan user and says "you see, he understands why I can't help you today. You know yourself, when I can, I will help you, you saw that last time. So don't be angry with me, you make me feel guilty." The Moluccan user answers "yeah, yeah, I understand ..."
That unanswerable appeals to share elicit feelings of guilt is a strong indication of the power of the sharing rule. However, the sharing rule is, at times, broken, as are other rules and behavioral codes. Many drug users at times engage in behavior in which they not only violate the rules and laws of the dominant culture, but also of their own subculture. But it is insufficient to simply remark that drug users engage in such rule breaking behavior as they are not the only group in the population in which this phenomenon occurs. "Situational exceptions to idealized cultural standards can frequently be observed throughout various sectors of the population ... and [t]hese moral dynamics are not, of course, limited to the experience of drug users." (26) Such moral division of labor is also observed in the legal and medical professions where, because of the relative differences in status, some lawyers and physicians do the dirty work while others of higher status do not and may even condemn such activities. (27) "The credibility of the system of ethics embraced by street drug users cannot be measured by absolute behavioral conformity any more than the credibility of business ethics can be assessed in terms of the absolute absence of fraud." (26) "The concept of norm ... does not require a correspondence between what persons say and what they do; discrepancies are to be expected. ... [B]ecause norms identify behavior that ought or ought not to occur, behavior may (and often does) depart from norms. ... The more relevant consideration includes the conditions under which this potential for deviance is realized and the conditions under which norms guide specific conduct." (28) Therefore, the circumstances under which the embraced rules are violated and the judgments drug users themselves hold regarding these violations are of equal importance.
As the last example showed, a refusal to share is acceptable if one is unable to share (i.c. one has a low availability of drugs and money). When one is perceived as being able to share, however, a refusal is condemned and may put pressure on a relationship:
About a week or 3 ago I was here with Harrie. He had one stripe of heroin left, his last one. He wanted to share it with me. Then, last week, I was a little bit sick and I asked him a 'betermakertje'. Meanwhile Harrie had started dealing. Then he says to me, "Sorry Arie, I can't do it now, I only have seven grams left."
Harrie's position and with that his relation with Arie has, however, changed when he started dealing. Dealing is not an easy occupation. Not only must a dealing user stay out of the hands of the police and hire a doorman and (body)guard to prevent rip-offs, he also has to manage the very frequent demands of customers for credit, betermakertjes and other favors. Dealers are often wangled by customers who are short of money. But they must control their financial balance and anticipate the financial credibility of their customers. Otherwise they are quickly out of business. At the other hand, they want to stay on good terms with their peers. This makes dealing a stressful activity and only few users manage to stay in business for extended periods of time.
The ability to conform to the rule of sharing is to a great degree dependent on drug availability. (26) Drug availability is, however, a relative notion, dependent on ones position in relation to the drugs and the perception of this position by the persons involved.
Symbolic Functions of Drug Sharing: Effects on the Social Consciousness
These drug sharing rules are all expressions of the almost universal subcultural code of share what you have. (29) And indeed, the data provide a broad pattern of sharing behaviors. The stereotype of drug users is that of ripping each other off as predatory individuals. While this behavior does indeed occur, a more prevalent pattern seems to be sharing. The drug users in this research shared many valued items such as housing, food, clothing and money. Often they helped one another with daily problems associated with drug user life. For instance, homelessness is not uncommon and in some of the places visited for this research several homeless drug users were given shelter for a shorter or longer period. One other such problem is that many IDUs suffer from collapsed veins and abscesses due to insufficient hygiene. Some insist on injecting themselves, others are happy to get help from another, often experienced injector, such as the following fieldnote shows:
A woman and her partner have just bought drugs and are shooting up. Both don't have an easy job. The man is trying several spots to shoot up. She also tries more than one spot and finally she asks Ria to do it. Ria takes the syringe, looks carefully at the females arm and sticks in the needle. Then she redraws the piston a little and blood runs in the syringe. She has hit a vein. After seeing the blood she presses the piston, takes out the syringe and hands it to the woman. Shooting up the woman took her very little time and she looked like a professional nurse doing her daily work.
In contrast with similar American examples involving house doctors or professional hitters in shooting galleries, there is no commercial trade off in this service. (18 19 30 31) Sometimes, users ingest more drugs than their usual dose and slip into a deep nod which can end in overdose. They then depend on the safeguarding of a fellow user, like in the next situation:
In Gus' house are Ria Vis and Jerry, Gus just left to do some shopping. Ria is asleep in an armchair. "She has swallowed pills", Jerry says, "she is 'out' now." A Little later Ria Wakes up a little. "It's alright Ria just go nicely asleep." Jerry says to her. Jerry is staying with her to take care if anything should happen.
It is clear that the sharing of drugs is an important element of a broader pattern of social interaction in the drug subculture. Besides the instrumental functions, described above, drug sharing is a way to socialize and to (re)establish relations in the drug scene. In the next example, Harrie was just ejected from the crisis center, after a stay of three and a half weeks. He drew some money out of the bank, bought drugs and went to Karel's place, where he lived before he went into the crisis center:
"I left for Karel's place to take a shot and to surprise Karel with a little cocktail as well. He was still a sleep when I came in and was happily surprised to be wakened up for a cocktail."
By sharing drugs with Karel, Harrie expresses not only that he is back, but also that he is a generous and trustful member of the community, who is aware of his obligations to his friends and fellow users; their common bond is renewed and their group sentiments are reinforced. (32)
Drug sharing plays a crucial role in the social organization of the drug subculture. This observation is not unique as it was also found in other research. (33 34) For example, Sandoval found sharing of resources, such as cars, food and drugs to be a common practice among a group of "heavy polydrug users": "Customarily when one user had a large supply, he would share with his friends as an investment for the times when he had none available. Even the dealers who made their livelihood selling drugs were not rigid. They often gave their friends free drugs." (34)
The important part drugs play in ritual is not limited to users of illegal drugs in modern western society, as in some studies of non-western, not primarily drug-driven, cultures, the sharing of drugs is also a main feature of social ritual. (35 36) What these traditional cultures and the drug subculture have in common is that they all live under harsh and demanding circumstances in which valued items are often scarce. (5 33 35 36) The lives of the members characteristically "oscillate between states of extreme mental dejection and extreme mental joy. Crises, calamities and disappointments of numerous sorts which are ever occurring ..., tend to disrupt the normal functioning of life and create a veritable condition of social dysphoria. Rituals on such occasions serve to counterbalance the disturbing actions of these adverse circumstances and restore social euphoria." (32)
The regular performance of the drug sharing ritual ensures continuity and smothers social conflicts that are often based on controversies of material origin (money, drugs or other valuables). (32 37) The elemental interaction pattern which is reflected in the drug sharing ritual is the reciprocal exchange of valued items among members of the same group. (36) This leads to the transformation of a multitude of individuals into an effective, relatively stable and cohesive social structure.
According to Collins "sharing a common mood or emotion" is a basic ingredient of ritual. (2) This means that sharing the drug high by sharing drugs is a fundamental condition for "drug use as a ritual event" as sharing is a requirement for the development of just that characteristic behavioral sequence which all definitions have in common --mechanical, stereotyped, repetitive, stylized actions. Sharing drugs results in sharing the common mood of the drug high, "an experience or knowledge which cannot be shared or transmitted during the course of ordinary social interaction. Sharing drugs has created a special bond similar to the bond created in the ritual context". (5) "Drugs also give the users a feeling of identity and a common bond ... and [this bond] acts as a strong supportive system for its members." (34) Because drugs are shared and ritualized, they have become a potent binding force. (35) Drug sharing not only helps to maintain the psychopharmacological balance, but serves an essential purpose in defining the social space drug users live their daily lives in --it separates the in-group from the out-group. (38) Labeled as structural outsiders and ostracized by mainstream society drug users have become mutually dependant for fulfilling basic human needs. As one of the research participants expressively phrased it:
"We help everybody here, black, white, red, yellow, we don't have apartheid here. What would become of us if we don't help each other, no one else does".
Of course, not all users at all times behave conform these community positive rules and rituals. Often they are broken. Users cheat each other, rip off their dealing peers or steal money and drugs. These community negative behaviors are often the subject of savage gossip. As Faupel explained, lack of conformity to subcultural norms is most evident in users with limited structuring of daily life and a reduced drug availability. (26) Such situational ethics are, however, not unique and have been documented in several other areas and social groups. (39 40 41 42) But the failure of drug users to "consistently maintain ethical integrity is commonly understood to be evidence for a lack of any normative sensitivity whatsoever". (26) As a result, some clinical psychiatrists termed drug users "extremely egoistic cannibals" whose "negative, undesirable, destructive, learned behavior" is caused by a junkie-syndrome that overrules all other behavior. (43 44 45) However, similar to Fiddle's observations of law enforcement personnel, (46) clinicians generally see drug users at their worst. Their observations are confined to drug users in clinical settings, users who applied for treatment because they could no longer manage their drug use. Furthermore, and this also applies to the negative opinions of drug users regarding their peer's behavior, norm conforming behavior is usually taken for granted, while it is the deviations from or breaches of the norms that leave the strongest impressions. The findings of this study underline the limitations of such observations. Junkie behavior is certainly an integral part of the daily experiences and behaviors of drug users and many experience a feeling of mistrust, but a subculture cannot revolve around merely negative relationships. Positive relationships and interpersonal trust are essential for its maintenance. (19) These are generally ritually confirmed and reinforced by shared use of drugs --the instrumental imperative of the subculture. (9)
This balance between positive and negative behavior is dependent on the perceived drug availability. With a sufficient availability positive relationships can be maintained with a considerable number of other drug users. When availability decreases this number will shrink to a small core around the individual and users will less often share the drugs they crave.
Craving for altered states of consciousness has been termed a universal human condition comparable to the other primary drives. (47) Just as with food, drink and sex, the acquisition and use of drugs is thus of essential importance in the fulfillment of this primary drive. Likewise, food, drink, sex and drugs have all served a major role in social ritual throughout history. Sharing these items brings people together and strengthens mutual ties. It can therefore be argued that drugs have intrinsic or primary ritual value for biological and social reasons. When drugs are shared, this generally fulfills the requirements for ritual (prescribed psychomotor sequence, special meaning). The from drug sharing resulting common mood -- the drug high-- satisfies desires for intimacy, social solidarity and harmony. As a result, drug sharing is a reinforcement of group identity and group cohesion, resulting in the maintenance of the drug using network, and ultimately, the drug subculture. As the survival of the tribe is an intrinsic goal of all forms of human organization, use and sharing of drugs is a fundamental (and normal) human behavioral expression.
- Durkheim E: The division of labor in society. New York: The Free Press, 1964.
- Collins R: Towards a neo-Meadian sociology of mind. Symbolic Interaction 1989, 12(1):1- 32.
- Bourguignon E: Altered states of consciousness, myths and rituals. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 7-24.
- Guanon R: Introduction to the study of Hindu doctrines. London: Luzac and Co., 1945.
- Cleckner PJ: Cognitive and ritual aspects of drug use among young black urban males. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 149-168.
- Zinberg NE: Drug, set, and setting: The basis for controlled intoxicant use. New Haven: Yale University Press, 1984.
- Harding WM, Zinberg NE: The effectiveness of the subculture in developing rituals and social sanctions for controlled drug use. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 111-134.
- Radcliffe-Brown AR: Structure and function in primitive society. London: Cohen and West Ltd, 1952.
- Malinowski B: A scientific theory of culture and other essays. New York: Oxford University Press, 1960.
- Goffman E: Stigma: Notes on the management of spoiled identity. New York: Simon and Schuster, Inc., 1963.
- Becker HS: Outsiders: Studies in the sociology of deviance. New York: The Free Press, 1973.
- Wallace AFC: Religion: An anthropological view. New York: Random House, 1966.
- Durkheim E: The elementary forms of the religious life. London: George Allen & Unwin LTD, 1971.
- La Fontaine JS: The interpretation of ritual. Introduction. London: Tavistock, 1972.
- Engelsman EL: Dutch policy on the management of drug related problems. British Journal of Addiction 1989; 84:211-218.
- Engelsman EL: Drug misuse and the Dutch: A matter of social wellbeing and not primarily a problem for the police and the courts. BMJ 1991; 302:484-485.
- Chitwood DD, McCoy CB, Inciardi JA et al.: HIV seropositivity of Needles from Shooting Galleries in South Florida. Am J Public Health 1990; 80:150-152.
- Murphy S, Waldorf D: Kickin' down to the street doc: Shooting galleries in the San Francisco Bay Area. Contemporary Drug Problems 1991; 18(1): 9-29.
- Des Jarlais DC, Friedman SR, Strug D: AIDS and needle sharing within the IV-drug use subculture. In Feldman DA, Johnson TM (eds.): The social dimensions of AIDS. New York: Praeger Publishers, 1986: 111-125.
- Carlson KA: Identifying the stranger: An analysis of behavioral rules for sales of heroin. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 191-206.
- Goffman E: Interaction ritual: Essays on face to face behavior. New York, Pantheon Books, 1967.
- Feldman HW, Biernacki P: The ethnography of needle sharing among intravenous drug users and implications for public policies and intervention strategies. In: Battjes RJ, Pickins RW (eds.): Needle sharing among intravenous drug abusers: National and international perspectives. Rockville: NIDA, 1988: 28-39.
- Preble E, Casey JJ: Taking care of business - the heroin user's life on the street. Int J Addict 1969, 1: 1-24.
- Firth R: Verbal and bodily rituals of greeting and parting. In: La Fontaine JS (ed.): The interpretation of ritual. London: Tavistock, 1972.
- Goody E: Greeting, begging and the presentation of respect. In: La Fontaine JS (ed.): The interpretation of ritual. London: Tavistock, 1972.
- Faupel CE: Drug availability, life structure and situational ethics of heroin addicts. Urban Life 1987; 15(3,4): 395-419.
- Hughes EC: The sociological eye: selected papers. Chicago: Aldine- Atherton, 1971.
- Meier RF: Norms and the study of deviance: a proposed research strategy. Deviant Behavior 1981; 3:1-25.
- Wieder DL: Telling the code. In: Turner R (ed): Ethnomethodology: selected readings. Middlesex, England: Penguin Education, 1974, pp 144-172.
- Stern LS: Self-injection education for street-level sexworkers, In: O'Hare, P., Newcombe, R., Buning, E., Drucker, E., Matthews, A. (Eds.) Reducing the Harm from Drug Use. London: Routledge, 1992: 122-127.
- Sterk CE: Living the life: Prostitutes and their health. Ph.D dissertation Rotterdam: Universiteitsdrukkerij 1989.
- Nagendra SP: The concept of ritual in modern sociological theory. New Delhi: The academic journals of India, 1971.
- Agar MH: Into that whole ritual thing: Ritualistic drug use among urban American heroin addicts. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 137-148.
- Sandoval MC: Patterns of drug abuse among the Spanish-speaking gay bar crowd. In: Du Toit BM (Ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 169-187.
- Carter WE: The Aymara, and the role of alcohol in human society. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 101-110.
- Partridge WL: Transformation and redundancy in ritual: a case from Colombia. In: Du Toit BM (ed.): Drugs, rituals and altered states of consciousness. Rotterdam: Balkema, 1977: 59-74.
- Turner VW: Dramas, fields and metaphors. London: Cornell University Press, 1974.
- Becker HS: Outsiders: Studies in the sociology of deviance. New York: The Free Press, 1973.
- Deutscher I: Words and deeds: social science and social policy. Social Problems 1966; 13: 235-254.
- LaPierre RT: Attitudes vs. actions. Social Forces 1934; 13: 230-237.
- Warriner CK: The nature and functions of official morality. American Journal of Sociology 1958; 64: 165-168.
- Becker HS, Geer B: The fate of idealism in medical school. American Sociological Review 1958; 23: 50-56.
- Epen JH van: Wat doen mensen met mensen? In: Heroïneverstrekking als alternatief voor behandeling: Verslag van een tweedaagse conferentie. Amsterdam: SKS, 1977; pp 4-8.
- Epen JH van: Drugverslaving en alcoholisme: diagnostiek en behandeling. Amsterdam: Elsevier, 1983.
- Noorlander EA: De doelgroep van P3. In: Mol A, Majoor B, Malinowski H (eds.): Junkies little helpers. Rotterdam: STOP, 1982.
- Fiddle S: Portraits from a Shooting Gallery. New York: Harper and Row, 1967.
- Siegel RK: Intoxication:life in pursuit of artificial paradise. New York: Pocket books, 1990.
| < Prev |
|---|