| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 194 |
| Yesterday: | 251 |
| This Week: | 194 |
| Last Week: | 2221 |
| This Month: | 4782 |
| Last Month: | 6796 |
| Total: | 129381 |
8. 1 Epidemic vs. Symptom
 |
|  |
| 
| Books - A Society with or without drugs? |
Drug Abuse
8. 1 Epidemic vs. Symptom
As was the case in the bill from 1968, the government did not use
epidemic as a metaphor to describe the spread of drug abuse. On the
contrary, Lidbom pointed several times to the impropriety of the
metaphor. However, in the Riksdag debates, right-wing MPs in
particular frequently used the epidemic metaphor, referring to theories
of Bejerot. Proponents of the epidemic theory opposed all definitions in
which negative social and psychological disturbances are a cause of
drug abuse, which they denoted the "symptom theory". A statement
from the government on assistance may illustrate the "symptom"
theory:
The underlying idea for assistance is that abuse of drugs and other addictive
substances can be regarded as primarily a social and social psychological problem
triggered by a dysfunction of the individual's interaction with other people and
phenomena in the person's regular milieu (Prop. 1972: 67:24).
According to the epidemic theory, however, people without such
symptoms, e.g. members of the medical profession, had also succumbed
to drug addiction. There must therefore be another primary cause,
namely, the substance itself: "We can speak of an epidemic that hits
blindly and independently of social and psychological preconditions"
(Rd, 1972: 87: 35). One consequence of the epidemic theory is the
necessity to isolate the drug addict after detoxification to prevent
contacts with drugs and other drug abusers and subsequently a relapse
into drug abuse. Some conservative MPs tabled a reservation, urging
the standing committee to state that drug abuse was not only a symptom
of social problems but a epidemiological problem as well (SoU 1972:
21).
While most Social Democratic MPs described the problem in
moderate terms, members of the Conservative and the Liberal parties
but also several Social Democrats described the problem in terms of
crisis. Rune Gustavsson, of the Centre Party (in 1977 Minister of Social
Affairs) spoke of the drug trade as: "a business that break down large
parts of a whole people" (Ibid. 31). Yngve Persson (Social Democrat),
an influential union leader and member of the RNS, stated: "the only
possible goal for the drug policy is to free our people from this misery"
(Ibid. 78). However, despite the controversies about the origin of the
drug problem and parts of the action programme, and the most suitable
countermeasures, there was no disagreement on the seriousness of the
problem. The Riksdag overruled the reservations from non-socialist
MPs and a MP from the Communist Party and approved the decisions
of the standing committees (Rd 1972 no. 87: 92).
The Dutch threat
From the beginning of the first problem definition process, international
co-operation was regarded as crucial in the struggle against drug abuse.
Sweden worked hard in the international context to bring amphetamines
under international control. Against this background, it is
understandable that the Dutch decision not to sign and ratify the
Convention on Psychotropic Substances established in Vienna in 1971
provoked strong reactions in Sweden.75 This was particularly
provocative to because a major part of smuggled amphetamines was
alleged to come from the Netherlands. MPs, the Minister of Justice
(Lidbom), and the National Police Commissioner had unsuccessfully
tried to induce the Dutch to view the international trade in drugs more
realistically and to adjust their drug legislation. However, there was
more than the position of the Netherlands in amphetamine trafficking to
Sweden. The whole Dutch drug policy was a thorn in the flesh for many
MPs. Svensson (Social Democrat), for example, stated that:
From Holland a figure of 140,000 cannabis-dependent persons was reported. In
some cases, this did not cause serious problems, in other cases it was a prelude to an
abuse that certainly can become tremendously annoying for this country. What is it
one can discover there and I would like to bring up? Well, that the use [of cannabis]
is so widespread that it had become a political factor. The case is, if I am right, that
for political reasons there was no power to interfere. It would be terrible if we got
into the same situation, i.e. if milder drugs were so widespread that one would not
dare to interfere for fear of getting on the wrong side of large groups of youth (Ibid.
65).
Apart from the wrong interpretation of the survey, referred to in the
Baan Committee's report (lifetime prevalence was estimated at
140,000, not dependency), the observation of Svensson was not wholly
beside the point. The Dutch government indeed had to consider the
opinions of large sections of the population, not just groups of youth. In
addition, it was against the tradition of governance to act when large
dissent existed in society on a particular issue. Besides, repressive
interventions had failed to stop the dissemination of cannabis among
Dutch youth.
According to a Liberal MP, Hamrin, the difficulties in achieving a
united front against smuggling could be exemplified by the
Netherlands. The failure in making the Dutch understand what was at
stake and co-operate in halting the big dealers put Sweden in a
distressing position (Ibid. 76).
Against the backdrop of the negative results of these efforts, ten MPs
representing all parties in the Riksdag had sent a letter to the Dutch
government on 15 March 1972. It said:
We, personal members of the Swedish Riksdag, have noticed that statements made
by the Swedish government and the National Swedish Police Board to the Dutch
government to take measures in order to facilitate smuggling of drugs from Holland
have failed to receive sufficient positive reaction. Public opinion in Sweden finds it
inconceivable that Holland, with its strong legal traditions, does not consider itself
able to co-operate in measures that are more effective. We appeal to the Dutch
government to rapidly undertake actions that can facilitate interference in the
outrageous trade in drugs (Ibid. 76).
In order to keep the heat on the Dutch government, MPs should at
regular intervals and by appropriate methods call attention to the fact
that Sweden and other countries were worried and waiting for results
(Ibid. 77).
Minister Lidbom answered that nothing indicated that the Dutch in
the near future would radically change their attitude. There was no
other way than continuing to persuade the Netherlands to change course
by its own political institutions (Ibid. 31). How to persuade them was a
difficult question. Ultimately it was a matter of influencing (Dutch)
public opinion, and in this field voluntary good forces could co-operate:
organisations, newspapers, television, etc. Likewise opinion moulding
on a political level was important and an exchange of MPs and experts
from both countries would be desirable. The Swedish ambassador in
The Hague had been requested to investigate this possibility (Ibid. 81).
This episode illustrates that the Dutch drug policy was seen as a major
problem for the Swedish drug situation.
In the meetings of the BRÅ Narcotics Group, the Netherlands was
regularly discussed. In 1973, the country was still mentioned as the
main source of the trafficking of amphetamines to Sweden. In 1974, the
Dutch governmental plan to decriminalise cannabis had come to the
attention of the group (Meeting 3 May 1974). In 1975, Amsterdam was
pointed out as the centre for heroin distribution (Meeting 12 September
1974. However, the NPB emphasised the good co-operation with Dutch
police authorities (Meeting 1 November 1973).
Prelude
In the second half of the 1970s, some developments occurred that
eventually ended in a revision of the first problem definition. As in
1968/1969, one may speak of a hectic period in the history of the
Swedish drug policy.
In autumn 1975, the situation had not changed much since the
description by Lidbom in 1972. The Minister of Social Affairs reported
that no important changes had occurred during the last year. Severe
drug abuse was still confined to big city regions and cannabis more
spread out. Surveys indicated that the number of young people who had
tested drugs was decreasing (Prop. 1975/76: 100: 7: 164).
In the next budget bill, the situation was depicted somewhat
differently.76 While drug abuse was still a quantitatively limited
problem compared to alcohol abuse, it was a serious symptom of
psychosocial problems. The most widespread drug during the seventies
had been cannabis but, as the minister said: "the majority of those who
have tested cannabis cease after one or few occasions." Furthermore,
surveys indicated that the number of youngsters that tried drugs had
decreased (Prop. 1976/77: 100: 8: 171). Data on the prevalence of
severe drug abuse were not available, and to fill this gap a case-finding
study would start in March 1977. Data from other sources, however,
indicated that abuse of central stimulants was still dominating among
established addicts, but a shift to abuse of opiates was also noted.
Abuse of morphine base had disseminated on a small scale in the
Stockholm and Malmö regions since the beginning of the seventies. In
1974, police and assistance agencies had reported intravenous abuse of
heroin. For the NPB, this was reason to increase the number of police
officers and in 1977, special drug brigades were established in all
counties.
In summary, developments of prevalence and incidence of drug
abuse during the seventies so far was described in both positive and
negative terms. The most common drug was cannabis, but many
youngsters tried this only once or twice. Surveys among pupils in
primary school showed a descending trend in the prevalence rate of
those who had ever used drugs, especially during the first half of the
seventies. Intravenous abuse of amphetamines was confined to the
metropolitan regions. The increase in abuse of opiates and in particular
heroin was most worrying.
Directors-General once again
Against the background of the increase of heroin abuse in particular, the
minister appointed a Leading Group in March 1977. This group was to
recommend actions against drug abuse and to co-ordinate actions,
especially in the field of assistance. The body comprised the under-
secretaries of state of social affairs (chairman) and justice and a number
of directors-general of central authorities.77The Leading Group
appointed 15 regional working groups that were to map the local
situation.
In its final report, February 1978, the Leading Group reported that
the situation concerning treatment was still distressing, especially the
insufficient expansion of treatment homes. Another conclusion was that
shortcomings in assistance to drug abusers constituted the weak link of
the action programme. It was heavily undersized and, as emphasised by
police and customs, actions in other fields of the action programme had
therefore lost in effect (Ds S 1978: 2: 12). A major expansion of
treatment homes was necessary but also ambulatory care needed
reinforcement. The involvement of popular movements, unions, and
voluntary organisations in aftercare needed more attention. Many
municipalities called for family care as an alternative to intramural
care.78
Furthermore, the Leading Group concluded that abuse of alcohol was
by far the biggest abuse problem in the country. Drug abuse was most
pronounced in big city regions, but drug problems had been noted in
smaller cities too. Multiple drug use was common. The situation was
judged as serious and the need for actions on a broad front was stressed.
However, according to the Leading Group no innovative methods or
additional resources were needed but intensified co-ordination between
actors in the action programme (Ds S 1978: 2: 20).
The report from the Leading Group was followed by the first drug
policy bill presented by a non-socialist government in March 1978. As
always in Swedish drug policy bills, the dissemination of drugs was
described extensively. Surveys indicated that the number of young
people testing cannabis had decreased. As regarding severe abuse the
picture was more blurred. According to estimates by authorities, the
number of intravenous abusers in the country was between 10,000 and
15,000. Abuse of central stimulants had stabilised but was still
dominating. Abuse of heroin had gained ground quickly, especially
since 1976. The number of heroin abusers in Stockholm was estimated
at 1000 and another 1000 in the rest of the country (Prop. 1977/78:105:
17). Cocaine was quite rare but could be expected to spread.
According to the Minister of Social Affairs, Gustavsson, the situation
was very serious. As in previous governments, the starting point for a
drug policy was that society could not accept use of drugs for other than
medical and scientific purposes, all other use was abuse. However, a
new feature was introduced in this bill; drug abuse was also rejected as
a phenomenon that did not belong in Swedish culture. It was something
un-Swedish:
The struggle against drug abuse may not be confined to just limiting its presence
but must be directed at eliminating drug abuse. Drug abuse can never be accepted as
part of our culture (Ibid. 30).79
The statement was unanimously accepted by the standing committee on
social affairs, even if the committee and (the government) reckoned that
the measures as proposed in the bill would not ultimately solve the
problem (SoU 1977/78: 36: 4).
The minister described the drug problem in terms of the "symptom"
theory:
Concerning the origins of drug (and alcohol) abuse these can be an expression of
psychological and social difficulties whose causes often can be found in society's
own imperfections. In the struggle against abuse, which to the highest degree is a
matter of preventing its emergence and dissemination, these causes must be
combated (Ibid. 30).
Some examples of social causes were unemployment, deficiencies in
the work environment and unsatisfactory living and leisure conditions.
As before, it was emphasised that the struggle against abuse was a
matter for all sections of society.
The epidemic theory was not referred to in the bill or in the report
from the Leading Group. On the other hand, it would show up in the
Riksdag debate in May 1978. Several MPs could not understand why
the epidemic of drug abuse did not come under the Law on Contagious
Diseases, which would entail an obligation to apply for treatment.
Bejerot and his organisation the RNS were frequently mentioned. The
issue of compulsory care was not on the agenda because discussions
had to wait until a state committee had completed its report on this
subject. Nevertheless, some MPs referred to the Hassela treatment
homes community which had stressed the need for extending the
maximum age for compulsory care according to the Care of Young
Persons Act to 23 years (Rd 1978 no. 160: 60). The lack of knowledge
on the results of treatment methods was also mentioned as a problem.
The pessimism about treatment results for heroin abusers was
unjustified, according to the minister, who referred to American
research (Ibid. 73).
It is striking that no particular international developments were
discussed in the bill, the Riksdag, and the standing committee on Social
Affairs (SoU 1977/78: 36). The Netherlands was not mentioned as a
problem.
The bill passed the Riksdag but not without voting on reservations
from social democratic MPs and motions of the Communist Party (Ibid.
80).
New guidelines
In 1977, complaints from police officers in the Stockholm region
reached the local prosecutors. Experiences had shown that the generous
practice of dismissal of prosecution stood in the way of actions against
street-level dealing. Dealers simply did not carry with them drugs for
more than a week's use, and police officers experienced actions against
drug dealing as meaningless. The prosecutors in Stockholm were
receptive to the complaints and decided that possession of heroin and
cocaine should be excluded from the possibility of dismissing
prosecution (Solarz 1987: 93).
In 1980, the national guidelines were reviewed. Dismissal of
prosecution should moreover only be used for quantities of one smoke
of cannabis (0.751 g) or one dose of central stimulants (0.10.2 g),
(cocaine excluded). When in doubt about the quantity, prosecution was
recommended. Furthermore, dismissal should be restricted to first-time
offenders. The Prosecutor-General pointed out that the adjustment of
guidelines this time was not caused by new legislation. Apart from
developments in the field of legislation, the prosecutors also had to
keep themselves informed on developments in medicines and social
conditions (RÅC I: 94). Up till then, a basic standpoint for prosecution
had been to prioritise actions against professional illegal trade and
distribution of drugs. Now the Prosecutor-General stated that also
actions against illegal retail sale were important. By actions on this
level, trade would become more risky and less profitable for those that
benefit from organised crime, which in turn would diminish interests in
further distribution. Moreover, it would lead to greater difficulties in
getting access to drugs, which in its turn facilitated rehabilitation of the
addict, and decreased the risks of disseminating drug abuse. However,
combating small-scale dealing was not enough. It would be necessary to
interfere on the level of abusers as well by taking measures against
possession of drugs.
The guidelines contained a reconsideration of the harm caused by
cannabis. New scientific documentation of the damage done by
cannabis contradicted opinions that cannabis was harmless. For
example, continued use could trigger psychosis and cause changes in
the personality. Another reason was that the use of cannabis had spread
to socially established persons. This development could partly be
counteracted by a more restrictive policy on dismissals and a fine could
have individual and general preventive effects for this category (Ibid.
7).
Compulsory care
When the State Committee on Social Welfare published an interim
report with principles for a new Social Welfare Act, compulsory care of
abusers was part of the new organisation of social services (SOU 1974:
39). However, the committee was divided on this point and in the
referral round, many organisations were critical as well. They perceived
the proposal as a preservation of the Temperance Act. The criticism
came from a new generation of social workers that believed that social
work should be based on voluntariness and assisting clients, not
controlling or suppressing them. Critical voices could also be heard
from politicians from left-wing parties. They denoted the act as a law
aimed at fostering the working class (Holgersson 1988: 253).
In February 1975, the Minister of Social Affairs, Aspling, instructed
the committee to investigate the possibilities for compulsory care of
substance abusers (drug and alcohol abusers) outside the realm of social
welfare. However, when the non-socialist government came into office
in autumn 1976 the Minister of Social Affairs, Gustavsson, instructed
the committee to investigate the former proposal on compulsory care
within social welfare as well (Ibid. 266). This created a situation in
which the committee had to consider two directives simultaneously.
In 1977, the State Committee on Social Welfare published its final
report (SOU 1977: 40). The committee proposed a new Social Welfare
Act in which the goals and obligations of municipal social service were
outlined. Compulsory care of adult drug and alcohol abusers was not
part of the act. However also this time the committee was divided on
this subject. A (conservative) minority supported the directive from
Minister Gustavsson. A committee of officials was appointed to work
out a compromise. The next year the committee proposed that a special
provision would be added to the LSPV act that enabled compulsory
care of substance abusers in a mental hospital for a maximum period of
four weeks in situations of emergency (Ds S 1978: 8). In the bill for the
Social Welfare Act, compulsory care of adult abusers was also
proposed to be a matter for psychiatry. Those who were dependent on
alcohol or drugs and in need of detoxification and other psychiatric care
related to dependency could be admitted compulsorily if absence of
care implied serious danger to their health or life or someone else's
personal security or health (Prop. 1979/80:1). However, this was not the
end of the story. In June 1980, the Riksdag approved a new Social
Welfare Act but without a law on compulsory care on which there was
still was large disagreement. The Minister of Social Affairs appointed a
working group to review the issue of compulsory care on the basis of
discussion in the Riksdag on this matter. In January the next year the
working group delivered a draft for an "Act on the Care of Adult
Abusers in Certain Cases" (LVM). The bill passed the parliament in
December and came into force in 1981. The LVM Act (SFS 1981:
1243) enabled compulsory care of adult abusers of alcohol and drug
abusers for a period of two months with a possible prolongation of
another two months. The decision to prolong compulsory care was to be
taken be the social services not the court. Furthermore, responsibility
for compulsory care was allocated to counties and municipalities. The
main difference from the Temperance Act is that the LVM Act
primarily aims at improving abusers' condition and increasing their
motivation for voluntary treatment. In other words, while the
Temperance Act primarily was to protect society, in the LVM Act the
condition of abusers was in focus.
New threats
The next governmental drug policy bill came in February 1982 and was
called "Actions against Alcohol and Drug Abuse" (Prop. 1981/82:143).
Besides the fact that alcohol and drugs were discussed in one single bill,
another striking fact is that very little attention was paid to assistance.
Control measures and information seemed to be more important.
In the bill, the situation concerning drug abuse was depicted in detail.
The case-finding study that started in 1977 and was published in 1980
was referred to. For the first time, prevalence of severe drug abuse
could be discussed based on a study.
Table 1: Severe drug abuse in the big cities 1979.80
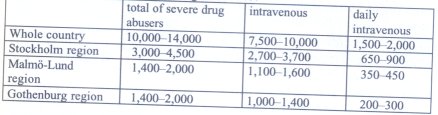
Opiate abusers, including heroin, comprised half of the category daily
(7501000) and 30% (25003300) of all intravenous drug abuse.
Further, a high number of multiple drug users were reported (Ds S
1980: 5: 92).
According to the BRÅ Narcotics Group, access to drugs had
increased slightly since 1979. Other data on developments in the drug
market came from police sources. The number of seizures had increased
sharply from 3359 in 1978 to 6992 in 1981. According to the minister,
the increase could be explained by increased policing against street-
level dealing and the changed guidelines for prosecutors in 1980.
However, custom had not changed its practice and recorded an increase
in seizures, which indicated increased availability of drugs in the
country, especially of amphetamines and heroin, and according the
police cocaine also was for sale in the streets (Prop. 1981/82: 143: 6).81
Furthermore, severe drug abuse was not confined to big city regions
any longer but manifest throughout the country. The drug problem was
described as a serious social and medical problem whose character had
recently become more serious. However, this development was similar
to that in most countries where drug abuse had become a threat to social
welfare (Ibid. 20).
Cannabis
Abuse of cannabis was substantial according to a report from the BRÅ
Narcotics Group (Ds S 1982: 1). However, annual surveys conducted
during the seventies showed a decline in lifetime prevalence among
youth (aged 15/16) that experimented with drugs, mainly cannabis. The
latest survey in 1981, however, showed a slight increase from 8 to 9%.
However, according to a household survey (age 1224), lifetime
prevalence of cannabis use had increased during the same period, from
9% in 1971 to 15% in 1980 (Ibid. 9). In spite of the fact that this was a
minor increase and opinions were divided on how to interpret the
surveys, the minister stated that a new wave of cannabis smoking had
started around 1979, as in other Western countries (Rd 1982 no. 153:
155). The image of a new wave of cannabis was also conveyed by a
report from the inquiry on the extent of drug abuse (UNO) (Ds S
1981:11). The overall conclusion by the UNO was that the drug
situation among young people had not worsened during the 1970s (Ibid.
79). The question is then: which data supported the assertions that a
new wave of cannabis was on its way? Part of the UNO inquiry was a
qualitative study among 19 youngsters (1216 years) from different
social backgrounds. Especially worrying was the use of cannabis
among upper-class youth that did not use cannabis to escape from
problems but as a symbol of freedom. Often they had learned to smoke
marijuana during visits to the US. Youth in this social category would
presumably not encounter serious problems when they wanted to quit
abuse of cannabis. However, it was a well-known fact that new patterns
of abuse usually start in upper-class groups and then disseminate to
groups with different social backgrounds. Youngsters with less
favourable conditions often have less potential to end abuse (Ibid. 50).
This line of reasoning is strikingly similar to the conclusions by the
Baan Committee some ten years previously; however, countermeasures
were of a completely different character.
It is likely that the government referred to the UNO report when it
stated that:
Abuse of cannabis has disseminated to groups that traditionally are not regarded as
categories of abusers. Among them, a tolerant attitude towards cannabis abuse
prevails. The drug is part of their lifestyle and they defend its abuse with false
assertions that it does not entail any social or medical harm. This message has also
been mediated by parts of the commercial culture. Behind this message are
economic forces that are risking the social and economic well-being and health of
the people for their own gain (Prop. 1981/82:143: 42).
This statement shows some new aspects of the drug problem. Cannabis
was used in other groups than the traditional, already deviant youth.
These new users were not aware of or ignored the basic facts about
cannabis-related harm. Furthermore, the dark forces were not just the
big dealers but also parts of commercial culture.82 Information that
aimed at changing people's attitude was considered an important and
effectual instrument to counteract this development. However, a
precondition for the efficiency of information was that society acted
consistently so that concord would be achieved between the message
and the actions (Ibid. 43).
Controlling the streets
During 1981, the police increased actions against street-level dealing.
Nationwide actions against drug criminality and in particular against
street-level dealers were pursued in autumn 1981 and spring 1982.
Round-ups of apartments and other places where drug abusers and
dealers hung out were parts of the action. Special attention was paid to
drug problems in schools and police officers were active in providing
information on drugs in schools and organisations (Prop. 1981/82: 143:
23). In the standing committee on justice, a motion was tabled
demanding a criminalisation of use of drugs. The committee held the
view that there was reason to change the Drug Act in this respect (JuU
1981/82: 47).
In July 1982, some changes in the Drug Act came into force. The
maximum penalty for simple drug offences was increased from two to
three years' imprisonment. The minimum penalty for serious drug
crime was increased from one to two years' imprisonment. A novelty
was the motivation for changing the Drug Act; it was aimed at
accentuating society's repudiation of drug abuse (Hoflund 1987: 26).
While previous provisions of the Drug Act sought to combat certain
aspects of the trade in drugs, from this period on, law provisions would
also be a symbol that conveyed a message to the population.
Assistance
The establishment of treatment homes was still a weak link in the
"chain of care". In spite of generous state subsidies for establishing and
running treatment homes, the speed of opening new homes was still
disappointing. In July 1981, the number of beds in state-subsidised
homes was 352, with an additional number of 100 beds that were
funded in other ways. The reasons for this slow pace, according to the
minister, could be found in administrative and practical difficulties in
starting a treatment home.
Concerning ambulatory care, the number of specialised centres for
drug abusers was 26 in January 1982. The major activities of these
centres were outreach work, different kinds of treatment and aftercare.
Detoxification and motivational work was done at special wards of
psychiatric hospitals (200 beds). An experiment with conditional
treatment instead of imprisonment had started in 1979 and would be
evaluated (Prop. 1981/82:143: 16).
Opinion formation
Information on drugs to the public followed the path set out by the SBN
in 1969, i.e. producing basic facts by central state authorities. In 1977
"Facts on Drugs and Drug Abusers", approved by the BRÅ Narcotics
Group, was published by the National Board of Health and Welfare. In
1980, the Ministry of Social Affairs and the BRÅ Narcotics Group
published a brochure "Facts on Hash and Marijuana". The brochure was
produced because of the worrying developments concerning cannabis
abuse and sent to all pupils aged 1319 (800,000 copies).83 A
complementary guide to teachers was distributed in 70,000 copies. In
spring 1981, two television programmes on the subject of hash were
broadcast and a leaflet printed. The RFHL started a nationwide action
called "Strike Back against Hash". In 1979 a committee for opinion
moulding against the drug culture was installed by the government
(SoU 1981/82:43). In 1981 a nationwide campaign against alcohol was
launched by the Ministry of Social Affairs and carried out by authorities
and organisations. In 1982, a similar action against drugs was pursued.
The target groups were youth and their parents (Prop. 1981/82:143: 8).
A novelty in the 1982 bill concerns the role of information. A new
concept was introduced, "opinion formation". Information was no
longer aimed at warning the people against the dangers of drugs (and
alcohol) or obtaining support for the government's struggle against
drugs. It also aimed at creating opinion against drug abuse (and
alcohol). Opinion against drugs had become a weapon in the struggle
against drugs, and cannabis was the main target.
Drug culture
Another new feature in policy documents was the introduction of the
concept of "drug culture". Information on drugs and influencing
attitudes would militate against the drug culture. What is this drug
culture? The Minister of Social Affairs had suggested that commercial
interests lay behind. The Minister of Education stated that many
youngsters had difficulties in defending themselves against the special
"youth culture" that was often associated with a naively positive
attitude to alcohol and drugs (Rd 1982, no. 153: 119). By information
on drug-related harm and by influencing norms, schools could make
pupils take a stand against the glorification of drugs.
In the plenary debate on the bill in May 1982, the Minister of Social
Affairs expressed her satisfaction with the national actions. The goal for
actions was to initiate a debate and to make young people reject drugs
(and alcohol). Actions had been fruitful so far. Thanks to the assistance
of almost all organisations in Sweden, meetings with parents had been
organised throughout the country. Young people demonstrated against
drug dealing (and alcohol dealing). Drug-free rock concerts, music, and
dance parties have been a great success in many places. Several MPs
also concluded that a new attitude was growing among the people, for
example, among parents concerning the purchase of alcoholic
beverages for their children (Ibid. 153).84
The Riksdag also discussed the cannabis-glorifying youth culture.
Sigurdsen (s) (Minister of Social Affairs in the next Social Democratic
government) was rather specific in defining the drug culture:
Pop music glorifies hash, and the culture that follows in its track is characterised by
the hallucinatory effects caused by the drug. We just can look at the covers of
albums in record shops. I think one can say that the drug-arousing community
develops its own culture (Ibid. 181).
Sigurdsen was also afraid that if the dimension of what was going on
remained undisclosed, a generation would run the risk of going under. It
was a shame to a rich welfare society that drugs had achieved such a
strong foothold. No more investigations were needed, but actions. An
alternative had to be created to the drug culture. At the same time,
Sigurdsen had declared in a newspaper article that she and the party
now had dissociated themselves from the former "blather" of drug
liberalism (Svenska Dagbladet 29 October 1982). A MP from the
Conservative Party supported her. He too pointed out the covers of
records as the source of drug-inspired lifestyles. According to him
freedom of speech would be respected but:
We can in each and every context and we shall do that forcefully point out
individuals and groups that have drugs as part of their message. In that case, they
will constantly be pushed into a position of defence that will become increasingly
intolerable. We must stop the "blather" culture (Ibid. 185).
The term "blather" (flum in Swedish) deserves a brief comment. In the
Swedish context of the drug problem "blather" usually denotes
opinions, people, a phenomenon or culture that do not express a firm
attitude against drugs. It is often used as a synonym of another
pejorative, "drug liberal".
75 The Netherlands was not the only country that did not sign. It was not until 1976
that the required number of signatories (40) was reached and the Convention came
into force.
76 In October 1976, after 44 years of Social Democratic governments, a non-
socialist coalition came into office.
77 Five members had also been members of the SBN in 1968. This time a reference
group of MPs informed the parliament about the Leading Group's activities.
78 Family care means that socially stable families take care of one or more
youngsters as an extra member of the family with financial compensation from the
social services.
79 For alcohol policy, the overall goal was to limit total consumption.
80 Data were obtained from authorities and registers. The definition of severe abuse
was all intravenous abuse, regardless of the frequency, and all daily or almost daily
abuse, regardless of the mode of intake (Ds S 1980:5).
81 The increase of amphetamines was explained by a reorganisation of Dutch crime
syndicates and increased domestic manufacture (Prop. 1981/82: 143: 6).
82 In the UNO report, musicals like Hair and Quadrophenia and rock concerts were
mentioned as examples.
83 The brochure was translated into seven immigrant languages.
84 The minimum age in Sweden to buy beverages in the state System Company is 20.
| < Prev | Next > |
|---|