| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 194 |
| Yesterday: | 251 |
| This Week: | 194 |
| Last Week: | 2221 |
| This Month: | 4782 |
| Last Month: | 6796 |
| Total: | 129381 |
1. 2 Three contexts
 |
|  |
| 
| Books - A Society with or without drugs? |
Drug Abuse
1. 2 Three contexts
One contextual factor is the international control system of drugs. The influence of the international control system on national drug policies has often been omitted in studies. In this study, the impact of the international problem definition on the national drug policy is included.
In sociological theory on social problems, the drug problem is viewed as essentially socially constructed. In the centre of this construction stands the problem definition. The problem definition as proposed by the government and adopted by politicians on the national level supposedly determines the nature of a drug policy and the goals for the action programme and its implementation.
The third arena is a set of institutions that implement the drug policy on a central and local level, for example, departmental officials, the judicial system, physicians, and social workers.
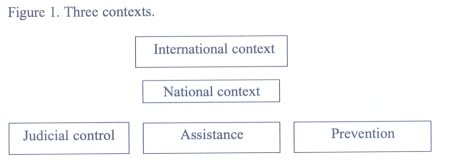
In the following section, these three levels will be discussed in more detail.
The international context
From the beginning of the twentieth century, an increasing number of nations have joined an international control system that today is under the aegis of the United Nations. The fact that the first global control system concerned production of and trade in narcotic drugs and eventually their use illustrates the importance of controlling drugs.(1)
Due to the nature of international treaties as a compromise between a wide range of vested national interests and cultural values, the treaties do not regulate national drug policies in detail (Chatterjee 1989). However, they do outline an international mainstream definition of the drug problem (Hartnoll 1989). This means that a national drug policy has to take obligations in international treaties and conventions into account and cannot deviate from the mainstream definition without isolating itself from the international community. Consequently, a national drug policy is influenced and circumscribed by international conventions which has to be included in an analysis of national drug policies. This is especially important because it means that at the time drug use was defined as a domestic problem in Sweden and the Netherlands, the frame for the national drug policy was already in place. However, due to differences in juridical and social/political traditions a certain freedom for national control systems on drugs was left within the framework of the conventions. This means that policymakers understood and accepted that social/cultural contexts are important factors in shaping and implementing a policy on drugs.
The drug problem as a social problem
At the national level, the drug problem has to be defined in order to set the course for the drug policy. The process of defining a problem is part of the policymaking process and the outcome is the result of a collective process of defining a phenomenon as a social problem. The question why one social phenomenon becomes a problem that needs to be addressed by society while others do not achieve such status has been a research subject for many scholars. This is not to deny that a (relatively small) part of the population uses illegal drugs and some of those experience serious troubles caused by drug use. That is an established fact. The crux is why such use is perceived as problematic.
Herbert Blumer (1971) developed a model in which he discerned different stages in a process by which a putative bad social condition receives the status of a social problem. He described the framing of an official programme of actions as a product of bargains in which different points of view and interests are accommodated.
This is a defining and redefining process in a concentrated form - the forming, the re-working and the recasting of a collective picture of the social problem, so that what emerges may be a far cry from how the problem was viewed in the earlier stage of its career. The official plan that is enacted constitutes in itself, the official definition of the problem; it represents how the society through its official apparatus perceives the problem and intends to act towards the problem (Ibid. 304).
The basic presumption is that actions against a problem not only reflect objectively existing conditions but also are determined by the causal explanation of the problem as adopted in the problem definition. The crucial phase in this process is when politicians decide on an action programme and thus legitimise a certain definition.
Blumer's model of a social problem, aims at stages of the process in which a certain condition is defined as a matter for society to address. Marc Peyrot (1984) on the other hand, analysed the cyclic character of the development of a problem. The first cycle of a social problem (first generation) comprises three periods:
1 mobilising agitation, parties claim that there is a problem that needs to be dealt with
2 policy formation, an official policymaking body formulates a plan of action
3 policy implementation, responsibility for dealing with the problem is delegated to one or more agencies that carry out official programmes.
These stages constitute the first generation of a problem. If the action programme for various reasons fails to solve or exaggerates the problem, a next cycle (second generation) can start:
4 program modification, new or alternative programmes can be established or old programmes can be reinforced (more of the same) and changes occur only in the techniques of intervention.
5 agitation for reform parallels stage 1. Alternative definitions and their remedies are proposed and lobbied for (Ibid. 86).
Peyrot made a note that is crucial for this study:
A second (or subsequent) cycle is influenced by the one(s) preceding it. Remedial approaches instituted in earlier eras may be abandoned and replaced by later ones or they may survive and coexist with newer remedies. In either case, the earlier approach shapes the context in which later efforts take place, although to a different extent. The degree to which an earlier remedial approach is institutionalised is the crucial historical variable. The more deeply ingrained the prior approach, the more difficult it is for a new approach to supersede it, being superimposed on the earlier foundation (Ibid. 86).
In both "career" models, the processes of legitimising a problem definition and the implementation of an action programme are central parts. Hilgartner and Bosk (1988), however, rejected the idea of an orderly succession of stages in the career model because it hinders an analysis of the interactions among problems and the competition between them. They pointed out two critical features of the social problem definition process:
• social problems exist in relation to other social problems.
• they are embedded within a complex institutionalised system of problem formulation and dissemination (lbid. 55).
As an alternative research strategy, they proposed the "arena" model. Instead of focusing on the stages of a social problem's development the arena model examines "the effect of those arenas on both the evolution of social problems and the actors who make claims about them" (Ibid. 55). There is a range of arenas, in which the collective definition process takes place: executive and legislative branches of government, the courts, the cinema, the news media, political campaign organisations, social action groups, books, the research community, religious organisations, professional societies, etc. The arena model focuses on the competition between actors that attempt to get their problem on the political agenda as a matter of high priority. Besides competition for (the limited) space in arenas, actors compete about definitions as well, i.e. between alternative ways of framing the problem. Which problem definition that manages to achieve master status is crucial for the future of the problem, the interest groups, the policy, and its implementation.
A sloppy process
In this thesis, the models as described above are used to examine the process by which the government and parliament officially adopt a definition of the problem. In other words, the arena where decisions are made on a drug policy, new legislation is adopted, responsibility for its implementation is allocated, and resources are distributed. It is at the political level that a competition between different models of causality, definitions of the problem and motives for the choice of actions, can be discerned.
The policymaking process is complicated and sloppy (Bosso 1994: 201). According to Marcel de Kort (1995: 16), an analytic framework that considers drug policies as based on rational decision making and scientific knowledge is inadequate. Instead, the researcher encounters diverging approaches, based in ideological settings with strong political, ethical, juridical and medical connotations. To cope with the diverging points of view, ideological backgrounds, theories and interests that are inconsistent or even exclude each other in the policymaking process, another approach is required. Policymaking aims at meeting the different views of involved interest groups. Policymakers concentrate on compromises and their goal is to keep the inevitable inconsistencies as limited as possible. According to Rochefort and Cobb (1994), hard-pressed policymakers often adopt a holistic approach that spreads resources among the leading interest groups. In addition, the distribution of resources may reflect which problem definition prevails.
Policy domains and interest groups
The process of policymaking and defining the problem does not occur in a vacuum but is framed by a context of historical developments and cultural values. The process of problem definition is contextual (national and international). The policy elite, interest groups, and even the mass media are not completely free to act in any way they want. They play key roles in defining problems and setting agendas, but none of this takes place in a vacuum:
The process of problem definition is part of the political `stream' [process of policy making]. As such, it is not only affected by culture, societal values, and prevailing norms, but also by the formal structure of governing institutions and procedures within which politics take place (Bosso 1994: 192).
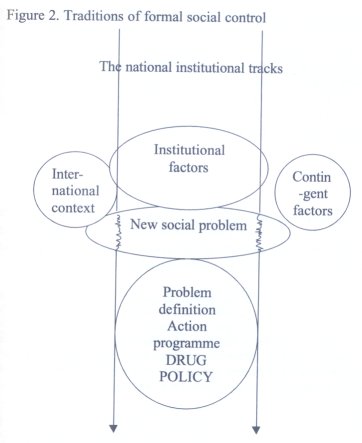
This leads us to the level where we find the actors that influence the definition of the drug problem. As shown in figure 2, at least three sections of the central and local governments have a voice in the problem definition process, the legal control system, the assistance system and institutes for prevention, e.g. the education system. They constitute a policy domain, i.e. a set of actors with major concerns, whose preferences other domain participants must take into account. Connected to the drug policy domain, is a policy network that comprises institutionalised interest groups such as politicians, authorities, professions, etc. In addition, issue pressure groups in civil society, i.e. outside the state and city administration, have an interest in influencing the government on the drug policy issue. Such issue pressure groups are, for example, parents of drug users, self-help groups, and the media. If the relationship between the state, interest groups, and issue pressure groups is fundamentally different in Sweden and the Netherlands, it could contribute to an explanation of the different outputs of the policymaking processes.
To identify the most prominent actors in the policy domain in which the process of problem definition is located, some questions can help to guide, based on the suggestion of the Swedish sociologist Sven Ake Lindgren (1993: 54):
• Which actors agitated to draw attention to the (drug) problem and how?
• Which actors were involved in the process of legitimising the problem definitions?
• Which actors proposed the action programme?
• Which authorities or organisations were made responsible for the implementation of actions?
• Which agencies for formal social control should implement the programme? 2
• Which actors agitated for a modification of the problem definition, the drug policy, and action programme?
It is important to emphasise that a policy on drugs undergoes change. When a programme fails to achieve expected results, other actions may be often proposed instead (programme modification). Both structural and contingent factors influence the elaboration of the policy. A contingent factor is, for example, changes in patterns of drug abuse, introduction of new drugs, new groups of users or prevalence rates. Structural factor are, for example, the institutional framework in which the drug policy is developed, the way governance is executed, and its openness to issue pressure groups. Structural factors are not immutable to changes but they change slowly. The historian Charles Tilly (1998: 31) has studied how states, in spite of converging into one type of national state, retain some features - for example, the character of their representative institutions - that clearly reflected their earlier historical experiences. It seems reasonable to me to expect that this also will be the case with historically grown practices of formal social control. The ways in which the action programmes have been organised and implemented are related to and reflect basic values concerning the order of society. For an analysis of the implementation of action programmes, this means that we must consider the traditions of institutions (law, medicine, and assistance) and the way they influenced and practised political directives. The Norwegian scholar on social policy Ivar Lodemel (1997) has called this "policy inheritance". In his study on poverty regimes in Norway and Britain, he concluded that when governmental bills to reform previous policies on poverty were presented to the parliaments, the existing structures for implementing the measures remained unchanged. The point is that they did not just inherit a policy but were also involved in elaborating the proposals.
Institutions
After having described the sources of theoretical inspiration to the thesis, it is time to outline its research design. Susanne MacGregor has in a proposal for the cross-cultural comparative study of drug policy regimes pointed out a guiding principle that suits my thesis:
Comparative analyses need to pay attention to the varying political strength of the institution of medicine and the historical origins of the policies in each society. The policy framework that developed began on the basis of the problem of a definition of the problem that was present at that time, including which substances were seen as of central concern initially. While the problem may change or the perception of the problem may change, the weight of interest bound up with the established institutional arrangements is a powerful force for conservatism (1999: 121).
In my opinion, a drug policy can be regarded as a function of institutionalised arrangements of formal social control and new social problems. Institutional factors are for example, the political system, the judicial system, the assistance system, traditions of formal social control, and the relation between the central state and civil society. The international control system on drugs is an institutional factor too. I regard social problems as contingent factors; i.e. they arise beyond the scope of the institutionalised tracks. If such phenomena have been defined as social problems, they constitute arenas for interventions. Which actors are permitted to the policy domain that is set to intervene is largely determined by institutional factors, such as traditions of formal social control. In addition, the action programme that is designed to counteract the problem will follow the structures that have historically developed because its design must having meaning to the people it is aimed at. This theoretical presumption can be illustrated by figure 2.
| < Prev | Next > |
|---|