| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 207 |
| Yesterday: | 251 |
| This Week: | 207 |
| Last Week: | 2221 |
| This Month: | 4795 |
| Last Month: | 6796 |
| Total: | 129394 |
Report 3 Difficulties in constructing a global estimate: the need for further refinement
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
4 Difficulties in constructing a global estimate: the need for further refinement
The viability and utility of the construct just developed is now considered through an attempt to generate our own prevalence-based, bottom-up estimate of the economic burden of drug use for a limited number of consuming nations. What becomes immediately apparent is that even using this simplified conceptualization of the burden of drug use, it is impossible to implement a consistent and comprehensive assessment of these few costs across most countries. Further reductions in both the number of countries considered and the elements actually included must be made due to the lack of systematic data collection efforts across most countries. These reductions are due to factors that could change in the future if data systems improve, so they are viewed as refinements made out of practical necessity rather than conceptual preference.
4.1 Limiting the number of countries considered
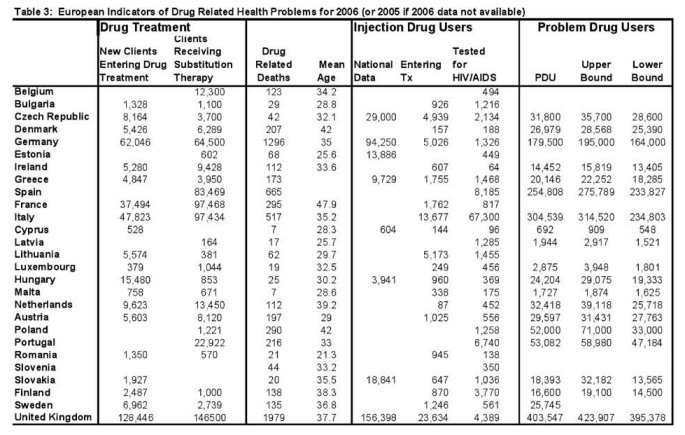
Originally this construct was to be broadly applied to a large set of developed and developing countries, but it quickly became evident that reliable data on even a small subset of drug-related harms is sorely lacking for most countries. This can be best illustrated by simply taking a closer look at a region of the world that has relatively good drug-related outcome measures, the 27 member states of the European Union. Unlike any other region, the EU has for the past several years dedicated significant resources to the compilation and standardization of measures of drug harm across its member states through a coordinated effort led by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). The task of harmonizing indicators across the member states has been a slow and difficult process because the member states started with very different data collection efforts in existence and it takes time to agree on a common definition and develop and harmonize processes for collecting data elements employing that common definition. Thus, the data reported to the EMCDDA today remains incomplete and highly variable in a few domains despite the significant progress that has been made. Table 3 summarizes data on just a few health indicators reported in the 2007 National Focal Point (REITOX) reports and compiled by the EMCDDA in the 2008 Statistical Bulletin. 7 Although our goal was to obtain data for each health indicator across all EU member countries for the year 2006, several countries do not yet report annual updates for all of the health indicators we are hoping to use. So, what is included in Table 3 are estimates reported in the REITOX reports for either 2005 or 2006 (EMCDDA, 2008b). Data from previous years were not included although they are available in the EMCDDA data tables so that we could demonstrate the point that consistent estimates are not available across all indicators for a particular year. When data are not reported for either 2005 or 2006 in the EMCDDA Statistical Bulletin, the indicators are left blank in Table 3.
For some health indicators, there is fairly comprehensive reporting of health issues evidence of the success that EMCDDA has had in coordinating these data across countries. In particular data on new clients entering treatment, those receiving substitution therapy and drug-related deaths are fairly comprehensive in that estimates are provided by most Member States. However, even for these indicators, the EMCDDA provides extensive notes and cautions to users explaining that simple comparison of the levels of these indicators across all EU countries is still not possible due to some remaining differences in reporting, data methods, and definitions (which they are continually improving upon). Indeed, the EMCDDA writes in the methods section for drug-related deaths the following:
“National statistics are improving in most countries and their definitions are becoming the same, or with small differences, to the common EMCDDA definition (called “Selection B” for the General Mortality Registration and “Selection D” for the Special Registries). A few countries still include cases due to psychoactive medicines or non-overdose deaths, generally as a limited proportion of the total. In addition, there are still differences between countries in procedures of recording cases, and in the frequency of post-mortem investigation (including autopsy rates). In some countries information exchange between General Mortality Registries and Special Registries (forensic or police) is insufficient or lacking, which compromise the quality of information. However considerable progress has been obtained during the last years in quality and reliability of information on many Member States. Direct comparisons between countries in the number or rates of drug-related deaths should be made with caution; but if methods are maintained consistently within a country, the trends observed can give valuable insight and interpreted together with other drug indicators.” (EMCDDA, 2008b).
Then there are indicators for which there is less consistent reporting even within the EU. In particular relatively few countries are able to provide national estimates of injection drug users even though this number provides the basis for measuring problem drug use, as defined by the EMCDDA. Indeed, as indicated by the second column under “Injection Drug Users” there are several countries who do not even report estimates of the fraction of clients entering treatment who inject drugs. Given the uncertainty regarding the actual number of injection drug users within each country, it seems difficult to understand how countries such as Poland can report the total number of problem drug users (final column). The EMCDDA requests that all member states provide information on the number of problem drug users, which they define as “injection drug use or long duration/regular use of opioids, cocaine and/or amphetamines. This definition specifically includes regular or long-term use of prescribed opioids such as methadone, but neither includes their rare nor irregular use, nor the use of ecstasy or cannabis. Existing estimates of problem drug use are often limited to opioids and polydrug use” (EMCDDA, 2007a). While, Poland does report information on individuals receiving substitution therapy, this number (1,221 individuals) alone provides little understanding to someone not intimately familiar with the data collection efforts inside of Poland of how the 52,000 problem drug users were determined. Similarly, it is not clear how Italy can report having 304,539 problem drug users, but only 97,434 clients receiving substitution therapy and again no national estimates of IDU use. The low correlation among these three variables (problem drug use, injection drug use and substitution therapy clients) that, by definition of problem drug user should be highly correlated, is perplexing and raises questions regarding the variability of methods each country employed to generate these results to even a casual user of these data.
The fact that the EU has not completely harmonized all of their harm indicators already is not by any means surprising or an indication that the current efforts are futile. Instead, it is indicative of the fact that this is a very difficult task and when done with great care and consideration, as being done by the EMCDDA, takes time. Furthermore, the attention that the EMCDDA is giving to the consistent collection of these data within its Member States raises general awareness of how different even similarly-named indicators can be across countries and how cautious one must be in simply drawing comparisons. The inconsistencies in data indicators across countries outside the EU are certainly far greater than that within the EU because of the coordination that has been undertaken in the EU.
Given the difficulties in interpreting numbers reported from different countries demonstrated by the EMCDDA, it was decided that the current effort would be greatly improved by focusing on a narrow set of countries for which the data are believed to be of reasonably high quality and information regarding their collection was readily available. Specifically, we attempt to construct consistent indicators of harm from existing data sources for the United States, Canada, Australia, the UK, Spain, France, Italy, Germany and the Netherlands. These countries are selected for because (a) they each represent a major consuming country, (b) the European countries selected are the largest consuming countries of the original 15 EU nations and hence represent important markets, and (c) these countries are believed to have the most reliable data in light of significant national efforts to collect meaningful data within each of them.
4.2 A further reduction in the cost elements considered
Some of the cost elements included as part of the conceptual framework in Figure 1 cannot be assessed even for a narrow set of countries with relatively rich data. In particular, there is no systematic reporting of reliable and consistent estimates across countries on the non-mortality based lost productivity (e.g. absenteeism) and drug-induced crime. Significant conceptual differences exist across countries regarding what should be included in these costs and how to measure them (Godfrey et al., 2002; ONDCP, 2004; Rehm et al., 2007; Collins & Lapsley, 2008). Many of these inconsistencies stem from scientific literatures that are far less conclusive regarding the extent to which drug use causally influences each of these outcomes. The findings from the literature are sensitive to which drugs are being considered, the age of the individuals involved, as well as the environment.
4.2.1 The literature on the association between drug use an non-fatal productivity losses
Substance use is believed to diminish productivity and lead to poor labour market outcomes for several reasons. First, it may delay initiation into the work force, thereby reducing experience and human capital accumulation associated with on-the-job training (Johnson & Herring, 1989). Second, it may decrease the probability of being employed which, again, may interfere with human capital accumulation (Gill & Michaels, 1992; Register & Williams, 1992). Third, it may increase absenteeism which directly influences the productivity of not only the drug user, but also those individuals who work with him (French et al., 1998; Zarkin et al., 1992). Finally, substance abuse may reduce an individual’s productivity at the job, which should translate directly into lower wages if wages are indeed a good indicator of marginal productivity (Hoyt, 1992).
Empirical studies that analyze the direct effect of substance use and abuse on earnings, which is presumed to be the strongest indicator of an individual’s productivity, have generated very mixed findings, however. Even after accounting for the endogeneity of substance use, earnings of substance users are found to be higher by some researchers (Kaestner, 1991; 1994a; Gill and Michaels, 1992; Register & Williams, 1992; French & Zarkin, 1995), lower by others (Burgess & Propper, 1998; Hoyt, 1992), and either statistically insignificant or not determinable by others (Kaestner, 1994b; Zarkin et al., 1998). The lack of a robust finding has led many economists to focus on other measures of productivity, such as the probability of being employed or unemployed (Bray et al, 1997; Register and Williams, 1992; Kandel & Davies, 1990) or absenteeism (French et al., 1998). Here, too, the evidence is mixed. Given the uncertainty regarding a causal association, some researchers have attempted to capture the time spent away from work dealing with drug-related problems, such as treatment (Collins & Lapsley, 2002; ONDCP 2004; Rehm et al., 2007). But research remains inconsistent across countries in the consideration and treatment of these costs.
It is clear that the relationship between substance use / abuse and labour market outcomes is dynamic and can be potentially influenced by the relationship between early substance use and human capital production. The potential for reverse causality, however, is also real. Just as substance use and abuse can lead to job separations and other poor labour market outcomes, job separations may lead to increased substance use and abuse. In light of the potential for feedback loops, it is important to use appropriate statistical methods that can isolate the true nature of the relationship. Much research in this area remains to be done examining associations within countries before aggregate level measures of lost productivity due to substance use can be reasonably constructed.
4.2.2 The literature on drugs and crime
Findings from surveys of prison populations over the past five years for European Member countries and the U.S. show that, compared to the general population, drug users are overrepresented in the prison population (EMCDDA, 2006; National Institute of Justice, 2000). Information pertaining to lifetime use rates among prison populations, however, provide no real information as to whether the individuals’ drug use caused the crime to occur (with the exception of those crimes which are by definition caused by use or sale of a drug). The mere fact that a person uses an illicit substance does not mean that it was that substance that caused the individual to engage in crime in the first place (i.e. causal attribution). Moreover, a positive drug test does at the time of arrest does not necessarily imply that the individual was under the influence at the time the crime was committed. It merely implies there is a strong positive association between drug use and crime, which may be driven by a true causal mechanism (for some crimes and some drugs) or by some other factor (observable or unobservable) that is correlated with both the decision to engage in crime and the decision to use drugs.
When considering the economic burden of drug use, one wants to capture all those resources that are lost because of the use of drugs – not because the same people who use drugs also engage in criminal behaviour. Thus it is necessary to include only those criminal costs that are clearly attributable to drug use. The scientific literature most often refers to three categories of drug related crime based on Goldstein’s tripartite model: psychopharmacological, economic compulsive and systemic crime (Goldstein, 1985). Psychopharmacological crime refers to crime committed by individuals under the influence of an illegal substance. In other words, the chemical properties of the drug alter the individual’s thinking, perceptions or mood and induces the individual to engage in the crime. Crimes that typically fall into this category include assaults and sexual offenses. Economic compulsive crime refers to crimes committed by drug users who are in need of income to fund their drug habit. These crimes generally include broad property crimes (theft, larceny, burglary, identity theft, motor vehicle theft), robbery, prostitution, and possibly drug selling that might generate income for the individual engaging in the crime. The third category of crime, systemic crime, refers to crime generated by efforts to maintain a black market or territory by illegal participants in the black market. Typical crimes included in this category are homicide, manslaughter, aggravated assault, and money laundering. A fourth category of drug-related crime is slowly gaining in recognition, victimization (MacCoun et al., 2003).
While much has been written on each of these types of crimes and recent estimates of the cost of drug abuse attempt to consider their impact (e.g., Collins & Lapsley, 2008), the scientific evidence providing definitive proof of a causal association between drug use and particular crimes is rare in population data. Evidence from treatment populations appears to be far more convincing of a strong association (Zarkin et al., 2005; McCollister et al., 2003; Aos et al., 2001), but that evidence has yet to be broadly construed as evidence of a causal relationship.
Without any clear guidance regarding what types of crime can and should be considered drug-related, independent investigators construct their own estimates of these relationships based on information they have available to them. Given the significant differences in data availability, this translates into estimates that are not naturally comparable across countries. For example, as part of their National Focal Point reporting, several EU countries report the extent to which either police agencies or the reporting agency attribute specific crimes to drugs. Other countries, including the U.S., use information on the number of arrestees or prisoners who report being under the influence of drugs or in need of drugs at the time of their crime as a way of estimating the number of drug-induced crimes. Both measures have limitations in that they both only represent crimes that generate an arrest and hence underestimate the extent to which these activities actually happen. However, they are not exactly comparable as the police reports reflect the police’s interpretation of weather a crime was conducted to get drugs, whereas the arrestee or prison population data give information based on the perpetrator’s own self-report.
4.3 Examination of a few indicators for countries with good data collection systems
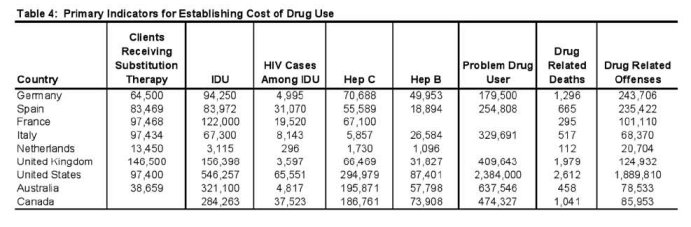
Table 4 presents a small set of indicators that might be used to construct an estimate of cost using the framework described above for a few countries that are generally believed to have good data available. However, careful examination of each of the indicators presented here raises doubts as to whether even such a simple comparison is truly meaningful. In this section we discuss issues regarding the comparability of the actual indicators that might be considered. In the next section we discuss the difficulties in trying to cost some of these measures.
4.3.1 Drug treatment
In the first column of Table 4 information on the number of clients receiving substitution therapy is reported circa 2006. 8 While data are generally available for many developed countries on the number of new treatment admissions and those receiving substitution therapies (as indicated in Table 3), countries do not consistently report information regarding the fraction of treatment episodes that take place in particular treatment settings or under specific therapies within those settings. That makes it extremely difficult to know how to compare treatment as well as the cost of the treatment, as costs are intrinsically tied to the type of treatment received (and for some countries, where it is given). Although substitution therapy is not the only form of drug treatment used across countries, and for some countries it is not even the most common form of drug treatment, it is a somewhat more standardized form of treatment that can be generally understood across countries and reported in such a way as to reflect a similar construct. There remains considerable variability in the types of substitution therapies that are available within countries, so direct comparisons across countries in any particular type of substitution therapy (e.g., methadone maintenance, bupenorphine, or prescription heroin) would not do adequate justice for demonstrating the extent to which substitution therapies are used in general. However, summary measures of the number of people receiving any type of substitution therapy should provide some measure of the availability of treatment generally.
4.3.2 Injection drug use
In order to estimate the number of individuals impacted by HIV/AIDS, Hepatitis C and Hepatitis B due to illicit drugs in specific countries one must first have a good estimate of the number of injection drug users, as most countries only report rates of infection for these diseases among injection drug users. As shown earlier in Table 3, very few European countries provide national estimates of the number of IDUs. In fact, only 9 of the 27 member states of the European Union provide national estimates of the number of injection drug users for 2005/2006.9 But in order to obtain national estimates of these infectious diseases of interest, one must start with national estimates of IDU rates, so attempts are typically taken to fill in the holes for non-reporting countries.
A common strategy used by researchers when current data are not available is to look for previous national estimates of the same indicator. Indeed, the EMCDDA reports in Table PDU-102 of the 2008 Statistical Bulletin all the individual studies that have been conducted providing national estimates of the population of injection drug users in Member States. Careful examination of this information shows that earlier national estimates for many of the non-reporting countries are available. For example, there is an estimate for Italy from 1996, Spain from 1998, France from 1999 and the Netherlands from 2001. These national estimates are inserted into Table 4 for these countries and are used for developing estimates of HIV/AIDS, Hep B and Hep C. However, some of these national estimates are more than 5 years old, and considerable changes in the number of injection drug use may have occurred in these countries. Thus, relying on such old estimates for generating good estimates of the incidence of these diseases for 2005/2006 would not be recommended.
While it is possible to construct current estimates for non-European countries, the methods for doing so necessarily differ across countries which should immediately raise concerns regarding their comparability. For the United States, a national estimate of injection drug users can be constructed by combining information from the 2006 National Survey on Drug Use or Health (NSDUH) on the number of dependent users (cocaine, heroin and stimulant) with information on the fraction of dependent individuals entering treatment who are likely to inject their drug of choice (TEDS, 2006). Such an estimate, while feasible, is hardly ideal as the household population is known to under represent or completely miss relevant populations who engage in use of harder substances, and hence injection drug use, and the Treatment Episode Data Set (TEDS) data only capture individuals in treatment. However, no national estimate of injection drug use for all drugs is available for the U.S., and so any construction would necessarily rely on inadequate data. For Australia, the 2004 Australian Household Survey inquires about injection drug use more generally in the survey. Approximately 1.9% of the population report ever injecting drugs in their lifetime, thus this estimate can be multiplied by the fraction of the Australian population that is 15 years of age or older to generate an estimate of national IDU.10 For Canada, a similar approach to that of Australia may be used, as the 2004 Canadian Addiction Survey includes a question regarding lifetime injection drug use within the survey (1.1% of the respondents report yes). Again, given this is a nationally representative household survey capturing individuals age 15 years and older, this estimate of injection drug rate can be multiplied by the population of Canada. Approaches for Canada and Australia, while possible, again are likely to underestimate the true number of injection drug users due to the fact that household surveys miss these often marginalized populations.
The true consistency and reasonableness of these IDU estimates for various countries is something that needs to be seriously considered. Although it is possible to obtain estimates for most countries, as indicated by the fact that we were able to “fill in” the IDU column in Table 4, some estimates are highly dated and others are based on general household surveys which are likely to significantly under-represent the very population we are trying to capture with this indicator. A simple examination of the values for particular countries raises serious questions. While the United States clearly comes out as the country with the highest number of IDU’s, this translates to only 18.2 per 10,000 people, far lower than the UK, Australia and even Canada and much closer to per capita rates from Spain and France. Given the substantially different injection culture in Spain, France and the United States, comparability in the number of IDUs per capita seems a bit implausible. And the rate for Canada, which is a country neighbouring the United States and suffering from many of the same drugs of abuse, seems implausibly high when compared to the U.S. Thus, it seems unlikely that indicators constructed in this disparate manner truly do a good job representing the real variability in injection drug use that is likely to exist across countries (2005/2006). Such an observation is important because these estimates of the number of injection drug users form the basis for estimating the rates of drug-related HIV/AIDS, Hep C and Hep B, as is discussed next.
4.3.3 HIV/AIDS
HIV prevalence rates among injection drug users are consistently tracked by most developed countries in an effort to monitor the global AIDS crisis. For example, the EMCDDA reports in their Statistical Bulletin each year the percent of a sample of injection drug users who test positive for HIV.11 The samples used to generate these estimates are in some cases nationally representative (e.g. Germany, Spain and Italy) and in other cases they are based on sub-national populations (France, the Netherlands and the UK). And again, in many cases estimates are not available for the most recent year, so earlier studies from previous years are employed (e.g. the Netherlands and France).
Similar estimates are available from national health statistics agencies for the other Western countries considered here. Information on the fraction of IDU-related new HIV cases in the U.S. comes from the U.S. Centres for Disease Control (CDC)12, which is then multiplied by the estimated number of injection drug users in the United States to get at the number of IDU-related HIV cases. Information on drug related HIV outcomes in Australia come from Australian Institute of Health and Welfare NCHECR annual surveillance report of IDU users participating in a needle and syringe exchange programs. Table 4.2.1 (2006) shows that the percent of IDU users testing positive with the HIV antibody across all 8 locations is 1.5%. Again, prevalence estimates of IDU-related HIV are then multiplied by the total number of IDU users estimated for Australia. Data on IDU-related HIV for Canada come from the 2006 report on I-TRACK: Enhanced Surveillance of Risk Behaviours among Injection Drug users in Canada Phase I Report (Public Health Agency of Canada, 2006). As in Australia, this surveillance system monitors known IDUs who participate in needle and syringe exchange programs throughout Canada. Thus, the method from which prevalence rates of HIV/AIDS among IDU users varies considerably across countries as do the population based from which they are drawn.13
HIV incidence rates among injection drug users from various national health departments are multiplied by the number of injection drug users reported in the second column of Table 4 to generate the number of drug-related HIV/AIDS cases for each country, as shown in Column 3 of Table 4. Estimates of the number of drug-related HIV cases reported in the Netherlands and the UK seem implausibly low, especially when compared to the other developed countries. In the case of the Netherlands, the low HIV number is driven by the fact that we have a small number of IDU users on which to get this total. In the case of the UK, it is actually that the estimated rate of HIV/AIDS among IDU users (range of 0.6 – 4.0, so midpoint is used) is significantly smaller than that of other European countries. This could be due to measurement error, as the UK estimate is drawn from sub-national studies. These examples demonstrate again why one should be cautious drawing comparisons from these numbers even though they appear to be tracking the same phenomena, as the lower number of HIV cases reported for some countries are not necessarily reflective of lower incidence rates but rather less comprehensive estimates of the components that make up these numbers.
4.3.4 Hepatitis C
As is similar to the case for HIV, most Western countries report the prevalence of injection drug users testing positive for HCV antibody. However, there remains substantial variation in the samples from which these prevalence estimates are obtained as well as the reliability of national estimates of IDU users for that country. Information among EU Member States regarding the prevalence of Hep C among IDU users is again systematically collected by the EMCDDA and reported in Table INF-2 of the annual Statistical Bulletin, but again countries may use national samples or sub-national samples to generate estimates of these rates. In Australia and Canada, the same systems used to report HIV/AIDS are used to monitor Hep C among injection drug users, using sub-national sample of IDU’s who choose to participate in needle and syringe exchange programs. In Australia, the rate for 2006 is 61% and that for a Canada is 65.7%. For the U.S., there is no similar monitoring system to track rates of Hep C among IDU users. Instead, information on the fraction of new Hep C cases occurring among IDU users is used as a method for estimating total IDU-related Hep C. Thus, the denominator for which the estimate from the U.S. is being built is fundamentally different than that for Australia, Canada or even the EU Member States. Thus, it should not be surprising then that the attributable fraction for the U.S. looks somewhat different (that for the U.S. is 54%). These differences in approaches across countries again highlight the problems in trying to draw comparisons of indicators.
4.3.5 Hepatitis B
Hepatitis B is again approached the exact same way as HIV/AIDS and Hepatitis C, although with slightly different data sources.14 First, an estimate of the prevalence of hepatitis B among IDUs is obtained from either a national sample or subsample. Then this fraction is multiplied by the number of IDUs estimated for each country, with the exception of the United States where the fraction represents only new cases of hepatitis B rather than all cases. Note that prevalence estimates are generally based on results from patients showing hepatitis B surface antigen (HBsAg (1)), which is considered the best marker for acute and chronic HBV infection. However, when countries do not report results for this marker, information on surface antibody (aHBs) or core antibody (aHBc) is used instead.
4.3.6 Problem drug use
A measure of the number of individuals suffering from problem drug use (PDU) is necessary to estimate the intangible cost of living with addiction. As noted in Table 3, even countries that are required to report this information have difficulty systematically constructing estimates of the number of PDUs. The EMCDDA asks EU Member States to report in the National REITOX reports estimates of the number of PDUs. In the case of Germany, Spain, Italy and the UK, the prevalence of PDU employing the standardized definition is reported in Table PDU-1. Unfortunately, data on PDU are not reported for either France of the Netherlands in the summary table, suggesting that either estimates were not created or could not be constructed in a manner that is consistent with measurement in the other Member States. The concept of PDU has not been widely adopted outside the EU. So for the United States, Australia or Canada an alternative approach for estimating these problem users has to be taken, immediately indicating that comparability across these countries as well as with the EU Member States is a problem. In the United States, information from the 2006 National Survey on Drug Use or Health (NSDUH) is used to identify the number of people meeting DSM-IV criteria for cocaine, heroin, other opiates, methamphetamine, and other stimulants. Thus problem drug use is operationalized as those experiencing clinically diagnosable abuse or dependence. Similarly in Australia, information from the 2007 NDSDUH is used to get number of dependent or IDU users for cocaine, heroin, or amphetamines and this number is multiplied by the 2007 population (AIHW, 2008). In Canada, information from the 2004 Canadian Addiction Survey (CAS) is used to identify fraction of Canadian population who report past year use of cocaine, speed and ecstasy. This total is then multiplied by 0.4, as the CAS study shows that between 36.7% and 42.1% of recent illicit drug users (excluding cannabis) are problem users (Aldif et al, 2005).
Estimates of the total number of PDUs for each country using the methods just described are reported in Column 6 of Table 4. Again, differences in these numbers across countries cannot be viewed as indicative of real differences in light of differences in how these numbers are defined and measured, particularly when looking at the non-European countries as compared to the European countries. In the case of the U.S., Canada and Australia, considerable scepticism is likely as estimates are based again on general household populations. Furthermore, because different drugs are of concern in these countries, it may be the case that the drugs considered in non-European countries are broader than that applied by countries constructing estimates within the EU.
4.3.7 Drug related deaths
The definition of drug related death adopted here is identical to that employed by the EMCDDA, which is “those deaths that are caused directly by the consumption of drugs of abuse. These deaths occur generally shortly after the consumption of the substance(s)”. By construction therefore, homicides, suicides or motor vehicle fatalities involving illicit substances are not necessarily reflected in these numbers unless a medical examiner identified in the ICD-9 codes that consumption of illicit drugs was the cause of the death.15 While it is possible to construct a similar estimate of drug-related deaths for the United States, data from other countries are not as readily available. Thus for Canada and Australia, existing estimates of the number of drug-related deaths based off of slightly different definitions are included in the table so as to capture some deaths, even if they are not measured the same. Given the inability to collect information for all countries using the same specific definition, caution should be taken in making comparisons across countries.
4.3.8 Drug related offences
This indicator is intended to capture country-specific information on the number of arrests related to the possession, sale and/or trafficking of illicit drugs. Thus, these represent the crimes associated with engaging in drug trade or use, not crimes committed under the influence of a substance. However, given that possession of a drug is not a criminal offense in all countries, these numbers will also reflect a slightly different approach across countries to managing drug markets. Information on drug related offences for European countries comes from the Statistical Bulletin’s Table DLO-2, DLO-4, and DLO-5, which attempts to reconcile country differences in regarding the treatment of offenders caught in possession of a drug. Indeed, in their data the EMCDDA has countries report administrative as well as criminal offences to improve comparability across the EU Member States. We add to these numbers information from the Federal Bureau of Investigation’s Crime in the United States for the U.S., Canadian Crime Statistics for Canada, and estimates from the Australian Illicit Drug Data Report for Australia. Not surprisingly, it can be seen in the final column of Table 4, that the United States has the greatest number of drug related offenses in total. The U.S. also has the highest rate per capita (63.1 per 10,000 people versus 29.5 for Germany and 27.9 for Australia). However, the data would also suggest that Spain had more drug related offences in 2006 in total and per capita (54.7 per 10,000 population) than the UK and France (who had per capita rates of 26.3 and 16.1, respectively). This is inconsistent with our intuition for these countries given that Spain, unlike the other countries, has decriminalized possession of all illicit substances. However, the difference is likely due to the inclusion of administrative offences in the E.U. measures. Unfortunately, offence estimates from non-EU countries, like Australia, that also retain administrative offences for some drug possession offences (e.g. cannabis) are not likely to be reflected in their numbers.
As the previous discussion highlights, efforts to obtain country-specific measures for all the indicators presented in Table 4 raises numerous questions and issues regarding the probable comparability and reliability of these indicator data even for countries with relatively good data collection systems. And these questions and concerns arise even before further issues related to the measurement of unit cost estimates are considered. When additional issues related to the inconsistency in quantifying the cost of each outcome are also considered, as outlined in the next section, the reasonableness of comparing estimates of the burden of drug use by combining these indicators of harm with measures of costs becomes even more questionable.
7 The data presented in Table 3 come from various tables presented in the EMCDDA’s Statistical Bulletin for 2008 (EMCDDA, 2008b).
8 Information for European countries comes from the EMCDDA Statistical Bulletin (2008), Table HSR-3 (“Estimated number of clients in methadone treatment and of clients receiving any opioids substitution”, Column 4 “All substitution clients, 2006”). Information for the United States comes from the 2006 Treatment Episode Data Set (TEDS). Information for Australia comes from the 2007 National Opioid Pharmacotherapy Statistics Annual Data Statistics, which reports numbers for 2006. Information on the number of individuals receiving substitution therapies in Canada are not available.
9 For these 9 member states, comparisons in the prevalence of drug-related HIV/AIDS rates can be reasonably done.
10 Precise information on the 2006 Australian population by age could not be accessed, so we used the readily available 2007 estimates for generating our total population estimate. According to official records, the total Australian population grew by only 317,200, so we should not have introduced to large of an error using this method.
11 Prevalence rates of HIV infection among IDU are reported for all EU countries in Table INF-1, which represents the primary source of our numbers.
12 U.S. Centers for Disease Control (CDC). Available: www.cdc.gov/Features/dsWorldAidsDay/, accessed December 2008.
13 It should be recognized that not all HIV cases among IDU’s are necessarily caused by injecting drugs. Studies evaluating the fraction that can be attributed to IDU, however, suggest it is a high proportion. Given the lack of systematic information on the fraction of non-IDU drug users who might also spread or contract HIV/AIDS due to risky sexual behavior, it is not possible to include this population in the estimate here. Non injection drug use can contribute to HIV infection as well as other sexually transmitted disease in at least three ways: (1) by facilitating sexual risk behavior (e.g., through reducing inhibition, reducing the probability of condom use); (2) by motivating sexual risk behavior (e.g., engaging in prostitution or hustling in order to get drugs); and (3) through physiological effects that make infection more likely if sexual contact occurs. For example, smoking cocaine in a pipe can cause lesions on the lip or the mouth, which may increase the likelihood of HIV transmission via oral sex. Similarly, use of crystal meth can prolong erection, enabling men to engage in intercourse for much longer periods, causing abrasions that facilitate HIV transmission. While it is known that these things can and do happen, there is no good population-level data that can assist in the estimation of the attribution factor of drug to HIV through STDs.
14 Prevalence rates of hepatitis B are again obtained from information reported by the EMCDDA in the Statistical Bulletin (2008) (Table INF-3). For the United States, information on hepatitis B comes from the Centers for Disease Control (MMWR, 2008), but represents fraction of new hepatitis B cases that are due to IDU. Data on rates of hepatitis B among IDU for Australia again come from Australian Institute of Health and Welfare (AIHW, 2007), but do not necessarily represent new cases. We could not identify a reasonably recent source of information on hepatitis B in Canada, so we used the attribution factor published by Popova et al., 2007.
15 Information on European countries comes from Table DRD-1 of the Statistical Bulletin. Information for the United States comes from authors own analysis of CDC’s WONDER data system. Data for Australia are from Collins and Lapsley (2008). Finally, information from Canada is based on Popova et al. (2007)’s estimate for 2002, as more recent data were not available.
| < Prev | Next > |
|---|