| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Appendix to report 4: country reports BRAZIL
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
BRAZIL
1 General information
Location:
Eastern South America, bordering the Atlantic Ocean
Area:
8,511,965 sq km
Land boundaries/coastline:
16,885 km / 7,491 km
Border countries:
Argentina 1,261 km, Bolivia 3,423 km, Colombia 1,644 km, French Guiana 730 km, Guyana 1,606 km, Paraguay 1,365 km, Peru 2,995 km, Suriname 593 km, Uruguay 1,068 km, Venezuela 2,200 km
Population:
196,342,592 (2008 est.)
Age structure:
0-14 years: 27% (male 26,986,909/female 25,961,947)
15-64 years: 66.8% (male 64,939,225/female 66,157,812)
65 years and over: 6.3% (male 5,182,987/female 7,113,707) (2008 est.)
Administrative divisions:
26 states and 1 federal district
GDP (purchasing power parity):
$1.849 trillion (2007 est.)
GDP (official exchange rate):
$1.314 trillion (2007 est.)
GDP- per capita (PPP):
$9,500 (2007 est.) (CIA World Factbook)
Drug research
Drug research activities: Formerly, drug research was concentrated in a few researchers and universities (e.g. Sao Paulo). Nowadays initiatives have started to stimulate specialised education for university students.
Main drug-related problems
Brazil is not a production country, but a trafficking and consuming country. Brazil is a producer of cannabis, trace amounts of coca cultivation in the Amazon region, used for domestic consumption, thus also a consumer country. It is an important transhipment country for Bolivian, Colombian and Peruvian cocaine heading for Europe.
2 Drug problems
2.1 Drug supply
2.1.1 Production
Brazil is not a drug production country.
There is synthetic heroin of some importance in the Eastern part of Brazil (low prices).
2.1.2 Trafficking
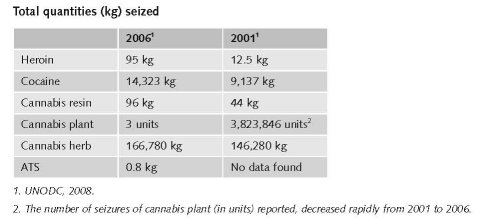
Cocaine seizures remain relatively low, between 7,000 and 16,000 kg annually since 2004 (International Crisis Group, 2008).
1 $1=€0.697488. Exchange rate 17 December 2008.
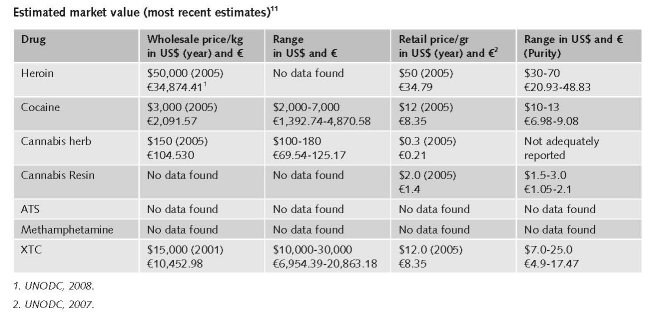
2.1.3 Retail/Consumption
No published national data found in English on retail/consumption
2.2 Drug Demand
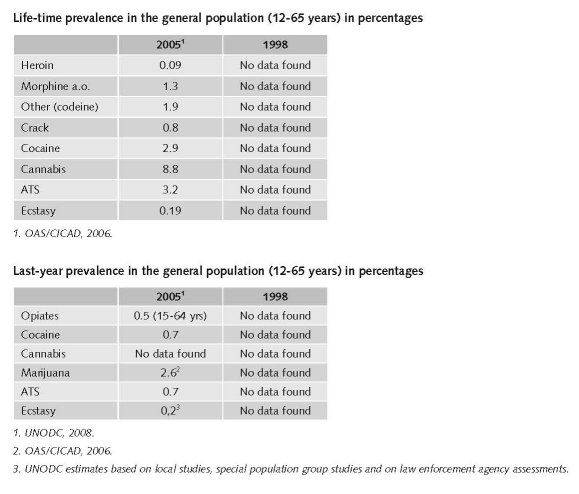
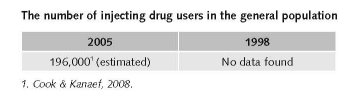
2.2.1 Experimental/recreational drug users in the general population
“Although Brazil is a country of continental dimensions, no striking differences were observed concerning the use of drugs in general in the cities surveyed, which represent the five geographical regions.” (Galduróz et al., 2004). This conclusion is based on data from four surveys conducted in the period 1987 to 1997.
While still relative low, drug use has increased. According to UNODC, Brazil is the largest opiates consumer in South America with 0.5% annual use rate (International Crisis Group, 2008a).
An estimated 50-53 tons of cocaine and “merla” (weed) is annually consumed in Brazil (International Crisis Group, 2008).
It may well be that these differences nowadays are substantial because Brazil has modernised and especially young people are more individualised and adhering to a modern lifestyle, in the big cities and also elsewhere (expert’s comments).
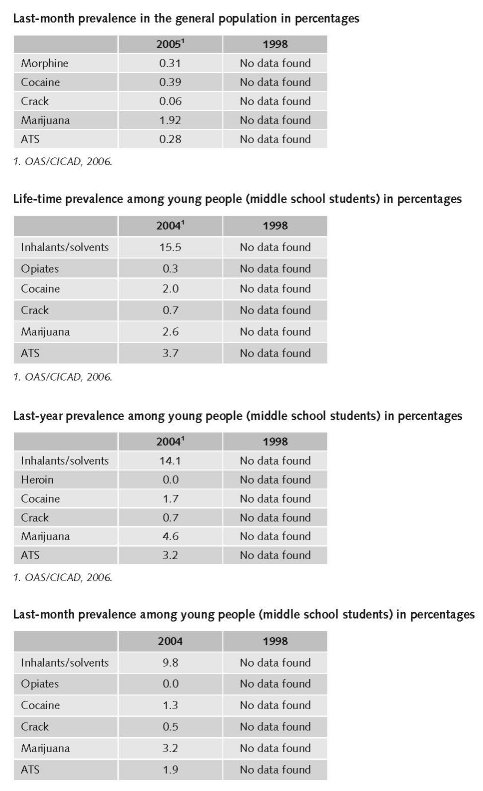
2.2.2 Problematic drug users/chronic and frequent drug users
Brazilian reports use the terms “dependency” or “frequent users” defined as ≥ 6 per month (expert’s comments).
No reliable data about 2007 and 1998 were found on the number of problematic/chronic-frequent users (in the general population).
No data were found on the number of injecting drug users among younger people (< 20 years).
2.3 Drug related Harm
2.3.1 HIV infections and mortality (drug related deaths)
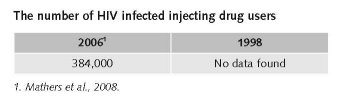
For 2006 this was estimated 48% (18-78) of approximately 800,000 people who inject drugs, thus 384,000 HIV infected IDUs (Mathers et al., 2008).
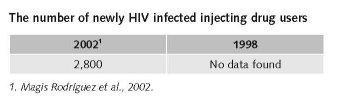
The average incidence rate remained stable at approximately 14.3 per 100,000 inhabitants (Magis Rodriguez et al., 2002).
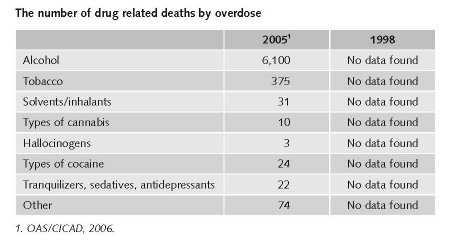
Interpreting numbers of drug related death (DRD) is difficult. The Brazilian registration system for DRD is SIM (= mortality information system). Since 2003 this is modernized. It will take another 2-3 years to be fully operative (expert’s comments).
2.3.2 Drug related crime or (societal) harm
Drug/related crime has increased during the past decade. Especially in the big cities. This is to be understood primarily as drug-related gang violence (expert’s comments).
Differences in harm between regions
Big cities versus other parts. In the favelas of the big cities high-risk situations are predominant. In these areas significantly higher risks exist for becoming involved in violence caused by drug gangs and gang-police violence. Elsewhere community activities are (or may be) organised that reduce harm (expert’s comments).
3 Drug policy
3.1 General information
3.1.1 Policy expenditures
Expert comments suggested that there are no structured national statistics on expenditures on drug policy available.
The Ministry of Health gave indications of the expenditures for specific types of care managed by this ministry. A total sum of expenditures is difficult to give.
a. 72,500,000 Reais (€21,505,810.132) (in 2007 for out-patient treatment in 150 Centres for Psychosocial Care for both alcohol and drug problems.
b. 694,500,000 Reais (in €205,680,084.73) 2007 for 1,200 other centres of out-patient psychosocial care.
c. 460,000,000 Reais (€136,013,479.27) (in 2007 for in-patient care (20-25% of the patients are there for drug problems).
d. Unknown expenditures for medical care for drug related health problems.
e. No estimates available for 26,000 multidisciplinary primary care teams working all over the country. At least some professionals in each of these teams are trained in prevention and treatment of drug problems.
f. Expenditures for drug prevention are unknown because these activities are part of general health promotion activities (see also demand reduction among experimental drug users).
3.1.2 Other general indicators
No data were found on numbers on arrests and imprisonment for drug-law related offences.
Numbers on arrests and imprisonment for use/possession for personal use
Numbers have probably reduced due to the new law that proclaims that possession of small amounts of drugs for personal consumption is not punished anymore by imprisonment. Because it remains unclear how the principles of this new law trickles down to daily practice of police officers and judges, one should not be overoptimistic yet about the net result for drug users in the streets (expert’s comments).
3.2 Supply reduction: Production, trafficking and retail
Priorities of supply reduction covered by policy papers and/or law
No reported data (in English) were found.
Brazil is neighboured by Paraguay (a high-quality cannabis producer), Colombia, Peru and Bolivia (main coca producers).
It has 9000 km. frontier to defend with neighbouring countries (mostly difficult to reach routes with mountains and jungle) and 7000 km coast line. It is unfeasible to do this effectively.
The change in border control (harm reduction) has predominantly been an increased sophistication. But criminality has also increased and became more sophisticated, maybe faster than border control (expert’s comments).
The policy targeting a reduction in criminalisation of drug users is only partly realised in daily reality yet. There are some 440,000 prisoners in Brazil and the annual increase is some 25,000. Approximately half of these are probably due to drug-related criminality (no statistics are available). A formal decriminalisation of possession of small amounts of illegal drugs for personal consumption has been initiated (expert’s comments).
2 BRL=€0.296632. Exchange rate 17 December 2008.
3.3 Demand reduction: Experimental/recreational drug use + problematic use/chronic frequent use
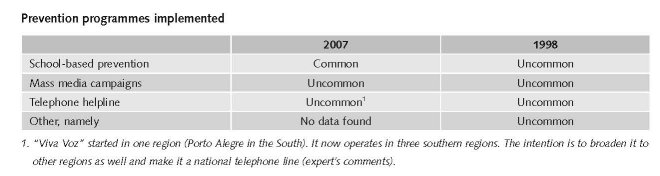
Most important in Brazil are the 27,000 small multidisciplinary primary health care teams that operate on a daily basis all over Brazil. These teams take care of health education and care and nowadays also include prevention of drug-related problems. The mission is enhancing self care and autonomy. An example of their focus is prevention and care of misuse of medical drugs (e.g. benzodiazepines that are primarily used for losing weight but people get dependent on these drugs). The funds for these teams are continuous but small/insufficient. A second example of important preventive activities are those realised by the 240,000 community help workers in this country (expert’s comments).
Five drug prevention programmes are mentioned, i.e. preschool education (< 7 yrs), primary education programme, primary and secondary education, a project focussing on street children and one on at-risk young mothers (OAS/CICAD, 2006).
Treatments available in 2007
Heroin dependence (also synthetic heroin) and cannabis use (although cannabis is regionally popular) is not considered an important health problem in Brazil. Cannabis is a problem from a criminality (supply reduction) perspective. The use of party drugs is increasing among young people. There are increasing health problems due to cocaine use but no specific treatments are available. The same goes for inhalants/solvents among children living on the street.
There exist a multitude of multidisciplinary teams taking care of health prevention/promotion and health care on local levels nationwide. Drug problems are covered as far as possible. Team members are also trained (short refreshment courses) for drug prevention and getting in contact with drug users, mainly of alcohol or over-the-counter (medical) drugs. There are now primary health care groups for women (mostly for dependence on benzodiazepines or stimulants). Brazil lacks an organised treatment network, specifically focussing on drug problems.
In 2006 138 out-patient treatment programmes existed and 36 new ones started.
The hospitals have a role but hospital care happens rarely for drug users. One reason is a lack of capacity (professionals).
This gap is filled by therapeutic communities organised by some 500 charity services in the country. These communities are mainly paid by charity funds and at best for a small part by the Federal Government.
In most cases treatment is abstinence oriented out-patients treatment. There are private clinics for those who can pay this. Maintenance treatment does not exist or is very rare. Heroin is no important problem in Brazil (expert’s comments; OAS/CICAD, 2006).
Priorities of drug prevention and treatment covered by policy papers and/or law
Drug demand reduction policy was a mainly enforcement focussed policy domain. It is now to be transformed into a public health policy domain, i.e. not prison-directed but recovery-directed. The Ministry of Health has a specific drug policy since 2006. Continued effort to implement and control this remains necessary. Funds to support activities were increased but these are still insufficient. In the next years health policy is aiming at a further integration of public health care, mental health care and treatment of drug dependence. Federal laws mention minimum standards of treatment. Legal measures were confirmed to set forth measures for the prevention of drug abuse, treatment and social integration of drug users and addicts and the establishment of norms to control the unauthorized production and illegal trafficking of drugs, defines crime and other matters. The new element concerns the decriminalisation of the possession of small amounts of drugs for personal use (expert’s comments; Presidency of the Republic, 2006; OAS/CICAD, 2006).
3.4 Harm reduction
3.4.1 HIV and mortality
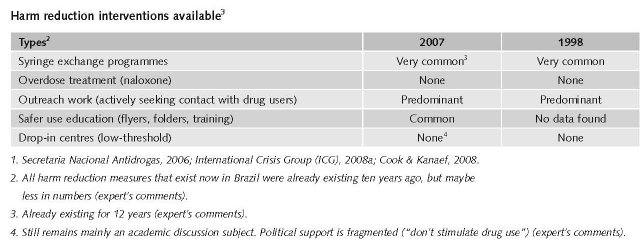
Ten years ago harm reduction policy and activities were exclusively concentrated on HIV/AIDS treatment programmes among the general population. The number of HIV cases remained stable during the past years (an estimated total of 700,000).
The number of illicit drug users decreased by more than 70% and this user population is concentrated in low income families and areas. Harm reduction activities for these people are part of broader focussed public health activities. A small part of these activities are focussed on illicit drug use. Ex-drug users are also participating in these activities as peers. Integrated tool-kits are used for injecting drug users but probably locally, not nationwide.
Priorities of harm reduction covered by policy papers and/or law
Brazil explicitly states supporting harm reduction and needle exchange programmes in national policy documents. It however does not have substitution maintenance programmes operational (Cook & Kanaef, 2008).
3.4.2 Crime, societal harm, environmental damage
Drug-related criminality and societal harm in Brazil is most frequently found in poor neighbourhoods of big cities (favelas). Here armed criminal groups that control drug distribution are the driving force behind street violence, mostly directed against other gangs or against the police (International Crisis Group, 2008a). However, in general, societal harm in these slums is considered to be primarily caused by social inequality and related variables. Drug trafficking may probably be partly caused by this inequality. Young people, particularly unemployed school drop-outs are at highest risk of becoming a drug addict, delinquent or killed (Berman et al., 2008).
3 $1=€0.697488. Exchange rate 17 December 2008.
References
Consulted experts
F. Cordeiro, Psychologist, Ministry of Health, Brasilia.
P. Delgado, Psychiatrist, Ministry of Health, Brasilia.
P. Dreyfus, Research Coordinator of the Small Arms Control Project, Viva Rio (NGO), Rio do Janeiro.
P. do Carmo Arruda Vieira Duarte, Director of Public Policies in Prevention and Treatment, SENAD, Brasilia.
G. Quaglia, UNODC Regional Office, Brasilia.
N. Santos, Research assistant, UNODC Regional Office.
I. Szabó, Coordinator of the Human Security Programme, Viva Rio (NGO), Rio do Janeiro.
P. Uchoa, Director, SENAD, Brasilia.
Documents
Berman EG, Krause K, LeBrun E, McDonald G. Small arms survey 2007. Guns and the city. Geneva, Graduate Institute of International Studies, Cambridge University Press, 2008.
CIA - The World Factbook: Brazil. Available: www.cia.gov/library/publications/the-world-factbook/ge-os/br.html, last accessed 20 December 2008.
Cook C, Kanaef N. Global state of harm reduction 2008. Mapping the response to drug-related HIV and hepatitis C epidemics. London, International Harm Reduction Association (IHRA), 2008.
Galduroz JCF, Noto AR, Nappo SA, Carlini BA. Trends in drug use among students in Brazil: Analysis of four surveys in 1987, 1989, 1993 and 1997. Brazilian Journal of Medical and Biological Research, 2004, 37: 523-531.
INCB (International Narcotics Board). Part III. Analysis of the world drug situation. 2007.
International Crisis Group (ICG). Latin American drugs I: Losing the fight. ICG Latin America Report No. 25, March 2008.
International Crisis Group (ICG). Latin American drugs II: Improving policy and reducing harm. ICG Latin America Report No. 26, March 2008a.
Magis Rodríguez C, Marques LF, Touzé G. HIV and injecting drug use in Latin America. AIDS, 2002, 16 (Suppl. 3), S34-S41.
Mathers BM, Degenhardt L, Phillips B, Wiessing L, Hickman M, Strathdee SA, Wodak A, Panda S, Tyndan M, Toufik A, Mattick RP. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. The Lancet 2008, vol. 372, Sept 24.
Mini Dublin Group. Regional report for South America. Council of the European Union. Brussels, January 2008 (Cordrogue 10).
Naciones Unidas Oficina contr la Droga y el Delito (UNODC). Jóvenes y drogas en paises sudamericanos: un desafío para las políticas públicas. Primer studio comparative sobre uso de drogas en poblacion escolar secundaria de Argentina, Bolivia, Brasil, Colombia, Chile, Equador, Paraguay, Perú y Uruguay. Published by Tetis Graf E.I.R.L., Lima, 2006.
OAS/CICAD (Organisation of American States/Inter-American Drug Abuse Control Commission). Brazil. Evaluation of progress in drug control 2005/2006. OEA/Ser.L/XIV.6.2; MEM/INF, 2006.
PNAD. National Antidrug Policy. Available: www.senad.gov.br, last accessed 19 December 2008.
Presidency of the Republic-Institutional Security Office, National Anti-drug Secretariat. Law No. 11.343 of August 23, 2006. Decree No. 5,912 of September 27, 2006.
Secretaria Nacional Antidrogas. Gabinete de Seguranca Institutional de Governo Federal do Brasil. Innovation and participation. Governmental report on drug demand reduction. 2003/2006. Brasília, SENAD.
SENAD (Secretaria Nacional Antidrogas de la Presidencia de Republica). National Policy on Drugs. Brasília, SENAD, 2005. (CCD-341.555 5).
UNODC (Naciones Unidas Oficina contr la Droga y el Delito. Jóvenes y drogas en paises sudamericanos: un desafío para las políticas públicas. Primer studio comparative sobre uso de drogas en poblacion escolar secundaria de Argentina, Bolivia, Brasil, Colombia, Chile, Equador, Paraguay, Perú y Uruguay. Published by Tetis Graf E.I.R.L., Lima, 2006.
UNODC. World Drug Report 2007 (Statistical Annex). United Nations Publication. Vienna, UNODC, 2008.
| < Prev | Next > |
|---|