| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Appendix to report 4: country reports TURKEY
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
TURKEY
1 General information
Location:
South-eastern Europe and South-western Asia (that portion of Turkey west of the Bosporus is geographically part of Europe), bordering the Black Sea, between Bulgaria and Georgia, and bordering the Aegean Sea and the Mediterranean Sea, between Greece and Syria
Area:
780,580 sq km
Land boundaries/coastline:
2,648 km / 7,200 km
Border countries:
Armenia 268 km, Azerbaijan 9 km, Bulgaria 240 km, Georgia 252 km, Greece 206 km, Iran 499 km, Iraq 352 km, Syria 822 km.
Population:
71,892,808 (July 2008 est.)
Age structure:
0-14 years: 24.4% (male 8,937,515/female 8,608,375)
15-64 years: 68.6% (male 25,030,793/female 24,253,312)
65 years and over: 7% (male 2,307,236/female 2,755,576) (2008 est.)
Administrative divisions:
81 provinces
GDP (purchasing power parity):
$853.9 billion (2007 est.)
GDP (official exchange rate):
$663.4 billion (2007 est.)
GDP- per capita (PPP):
$12,000 (2007 est.) (CIA The World Factbook)
Drug research
TUBIM is the Turkish national Monitoring Centre for Drugs and Drug Addiction and collects data on these topics. There are no research institutions available in Turkey working specifically on the issue of drugs and drug addiction (Country overview).
Main drug-related problems
Turkey is mainly a transit country (a bridge between continents), an important trafficking route for heroin from the East (Afghanistan/Iran) to Western Europe and the other way around for ecstasy from Europe (the Netherlands, etc.) to the East.
2 Drug problems
2.1 Drug supply
2.1.1 Production
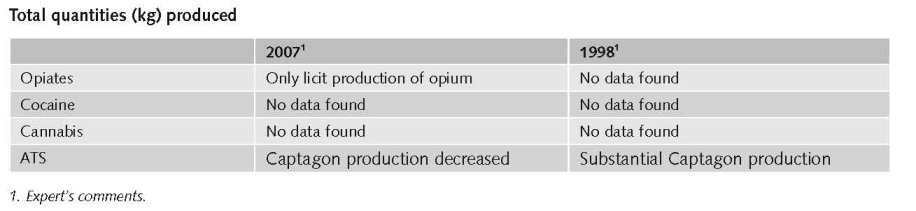
In Turkey amphetamine (Captagon) production and some cannabis production for domestic market can be found.
UNODC reports for seizures of illicit laboratories in Turkey that in 2006 12 Captagon laboratories, and 1 heroin production site were dismantled. Turkey reported the discovery of 12 clandestine amphetamine (Captagon) laboratories in 2006, the largest seizure of laboratories the country has reported to UNODC. The lab types included both manufacturing and tableting operations. In addition, the INCB reported that 197 litres of P-2-P were also seized there in 2006; the largest seizure of its kind by Turkey in recent years. It could be that increased control in Bulgaria has led to a shift in production to Turkey (UNODC, 2008).
Non-specified amphetamines in Europe are more likely to be amphetamine-based than methamphetamine-based. Seizures have declined slightly since their 2004 peak, consistent with reports of shortages in Europe of P-2-P24, its main precursor. This decline may also reflect indications of amphetamine (Captagon) manufacture shifting towards the Near and Middle East, the largest consumer market for Captagon. The discovery of several labs in Turkey, some of which were on the border with Syria, could have necessitated a new source of supply. One of the more interesting trends within Europe has been the continuing shift of production and trafficking in amphetamine to both the new-EU and non-EU States Members. In 1996, the EU-15 countries accounted for 97% of all European amphetamine seizures (UNODC, 2008).
2.1.2 Trafficking
Turkey is affected by three main heroin drug trafficking routes namely: the Balkan route, the northern (Black Sea) route and an eastern Mediterranean route. Cocaine enters Turkey from South America. Cannabis enters Turkey through Lebanon, Albania and Afghanistan. Turkey acts as a transit route for opium originating from Afghanistan en route to Western Europe, and also acts as a transit route for Captagon tablets originating in Eastern Europe en route to countries in the Middle East (Country overview).
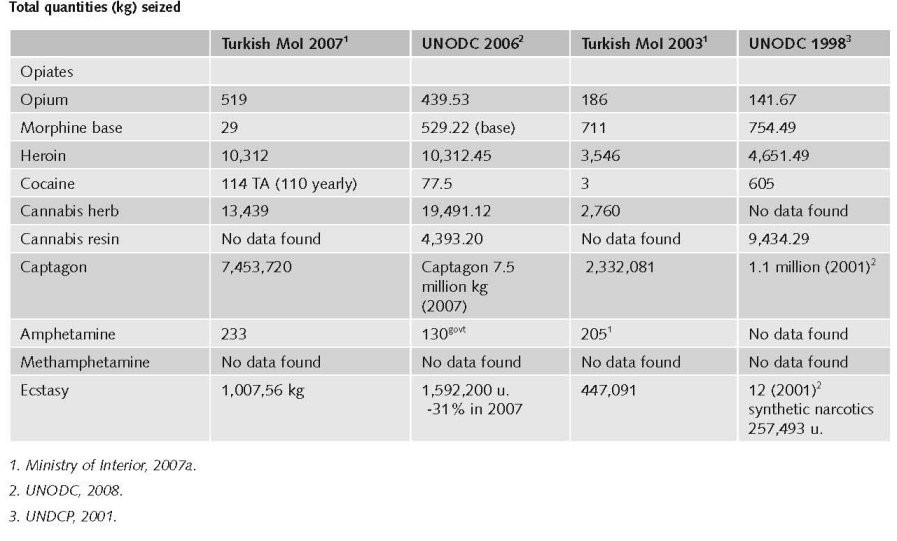
Global heroin seizures amounted to 58 mt, about the same as a year earlier (-1%). The largest heroin seizures in 2006 were reported by Iran (10.7 mt or 19% of global heroin seizures), followed by Turkey (10.3 mt or 18%), China (5.8 m or 10%), Afghanistan (4 mt or 7%), Pakistan (2.8 mt or 5%), the Russian Federation (2.5 mt or 4%) and Tajikistan (2.1% or 4%) (UNODC, 2008).
Most of the opiates from Afghanistan destined for Western Europe continue to be trafficked via Pakistan, Iran, Turkey and the Balkan countries (UNODC, 2008).
Amphetamine tablets for the Near and Middle East have typically been produced in Southeast Europe (Bulgaria and Turkey) and trafficked and marketed as Captagon to near and Middle East countries (UNODC, 2008).
In 2006, the total number of drugs seized amounted to 7,286 kg. 73.6% of these seizures were related to cannabis followed by 12% of ecstasy seizures and 11% heroin seizures. In 2006, a substantial increase was reported in the quantity of drugs seized for cannabis, heroin and captagon tablets, if compared to the previous year. In 2006, the quantity of seized cannabis resin and herbal cannabis amounted to 24,884 kg whereas in 2005, it amounted to 13,719 kg. The quantity of seized heroin in 2006 amounted to 10,312 kg whereas in 2005 the quantity amounted to 8,173 kg. Furthermore, in 2005 a total of 6,404,923 captagon tablets were seized, rising to 19,971,625 tablets in 2006. In March 2006, almost 2 kg of heroin were seized through a courier in the Hakkari Province, with the purity of the seized heroin reported at 95%. This was the first time in Turkey that the seized heroin had such a high level of purity (Country overview).
Regional ATS trafficking (in and through Turkey) has significantly increased in the last years, with seizure totals of amphetamines, methamphetamines and non-specified amphetamines rising from just 33 kg in 2001 to 729 kg in 2006. Amphetamine seizures alone increased from 52 kg in 2005 to 233 kg in 2007 (UNODC, 2008a).
Estimated retail value in 2005
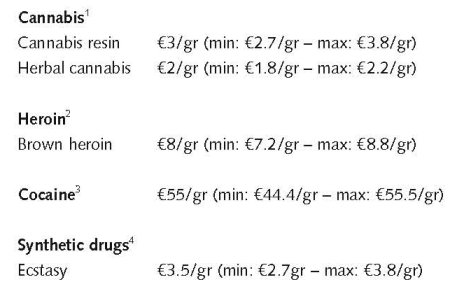
1. Price of cannabis at retail level, 2005 - EMCDDA Table PPP-1 Part (i)-PRICE-CANNABIS.htm
2. Price of heroin at retail level, 2005 - EMCDDA Table PPP-2 Part (i)-PRICE-HEROIN.htm
3. Price of cocaine products at retail level, 2005 - EMCDDA Table PPP-3 Part (i)-PRICE-COCAINE.htm
4. Price of synthetic drugs at retail level, 2005 - EMCDDA Table PPP-4 Part (i)-PRICE-SYNTHETIC.htm
In 2006, a substantial increase can be observed in the average price per gram for the majority of substances, when compared to the previous year. In 2006, the average price for cannabis resin was €6/gram whereas in 2005 the average price was €4/gram. The average price for brown heroin increased from €8/gram in 2005 to €14.5/gram in 2006. Furthermore, the average price for cocaine increase from €50/gram in 2005 to €90/gram, whereas the average price for ecstasy was €3/tablet in 2005 and increased to an average price of €6/tablet in 2006 (Country overview).
2.2 Drug Demand
2.2.1 Experimental/recreational drug users in the general population
The first study covering Turkey was conducted by the public sector and by the Turkish Psychiatrists Association in 2002.
The survey was conducted with 7681 respondents, surveyed at home. Results from this study indicate that 1.2% of participants (n=97) in this study used illicit drugs at least once in their lifetime. Another study on drugs use among the overall population (aged 15–64) in Turkey was realised in coordination with UNODC. Results from his study indicate that 0.05% of participants in this study had used opium poppy derivative drugs and 0.06% had used volatile drugs at least once in their lifetime (Country overview).
In addition to that, an ESPAD survey, covering 6149 samples aged 15-16 has been conducted in 6 metropolitan cities (Adana, Ankara, Diyarbakır, I.stanbul, I.zmir and Samsun). According to the result of this study, 4.2% use inhalants 4.3% use cannabis, 1.8% use ecstasy, 3% use tranquilliser, 1.5% use heroin, and 1.6% use cocaine at least one time in the life time period. Apart from that ESPAD survey, a research study exists which was conducted by the Turkish Grand National Assembly Research Commission to examine behaviour among schoolchildren. The study, conducted among 26 009 students in 261 schools (130 official and 131 private) in 60 provinces selected by TUI.K (Turkish Statistical Institute), indicates that 15.6% of students smoke tobacco, 16.5% have drunk alcohol at least once in the last month, and 2.9% have used drugs/stimulants in the last three months (Country overview).
The rate of opium poppy derivative drugs in Turkey in the overall population between the ages 15-64 is estimated to be 0.05% and the rate of volatile drugs in 0.06% in average (National Report, 2007).
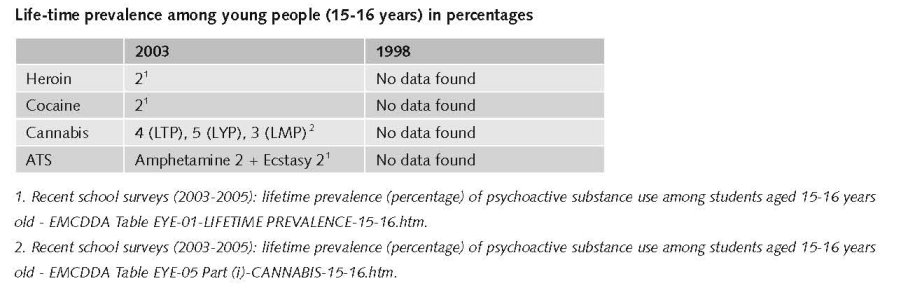
There has been an increase in use of drugs over the years, although heroin use is rather low compared to the use of cannabis and synthetic drugs. There was no XTC use in Turkey 10 years ago, it started to show on the domestic market around 2003; methamphetamine use is still rare. Captagon is produced in Turkey but use in Turkey itself is limited. Cocaine use is also very limited. It can be found in Istanbul and big tourist areas in summer time. The use of Ketamine, GHB, or magic mushrooms is very rare (no seizures of any importance of these drugs so far in Turkey) (expert’s comments).
There is no information available on last-year and last-month prevalence in the general population.
2.2.2 Problematic drug users/chronic and frequent drug users
So far, there is no national problem drug use estimate available in Turkey (Country overview).
Data on number of drug users were collected from 2004 onwards. Only reliable data from persons seeking in-patient treatment are available (expert’s comments). In 2004, 1,427 persons have been treated for drug addiction (Ministry of Interior, 2007a).
There is no detailed information on the exact number of drug addicts in Turkey nor on the routes of administration (Ministry of Interior, 2007a). The estimated number of drug users is 30,000-40,000; the estimated number of problematic users 5,000 (heroin users) (expert’s comments).
2.3 Drug related Harm
2.3.1 HIV infections and mortality (drug related deaths)

According to a 2008 IHRA report on the state of harm reduction in 2008, adult HIV prevalence amongst people who inject drugs is considered 0% in Turkey (Cook et al., 2008).
Regarding HIV, data from the Ministry of Health General Directorate of Essential Health Services, recorded a total of six IDUs declaring being HIV positive in 2006 (Country overview).
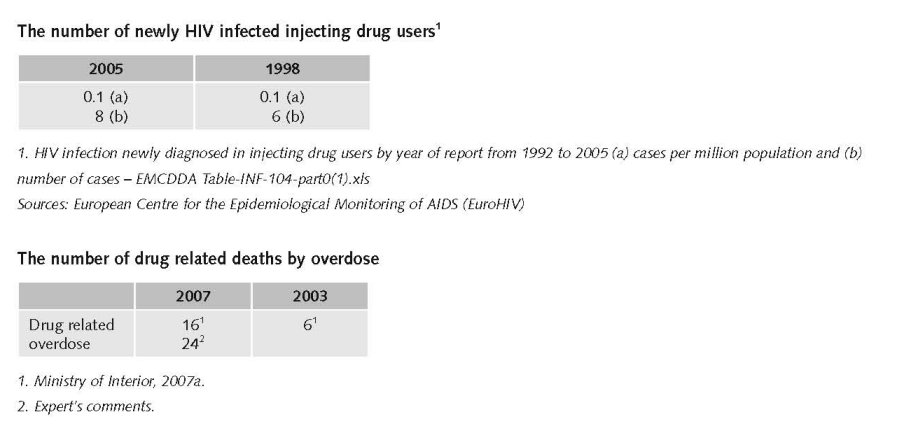
Available figures for drug related deaths by overdose differ substantially.
Until 2005, data on drug-related deaths were collected and accessible through police records. In 2006, within the framework of the Phare project and in direct collaboration with the EMCDDA, a special working group on drug-related deaths data was created. This new working group is composed of three main partners. The Ministry of Justice; the General Directorate of the Security Department of Anti-smuggling and Organised Crime and the General Command of Gendarmerie Department of Anti-smuggling and Organised Crime. The working group, together with several other international experts and the EMCDDA, is currently developing a new and reliable system for data collection on drug-related deaths (Country overview).
There is a study claiming a number of ‘deaths from drug overdose and toxicity’ for the period 1997-2001, i.e. 374 deaths, with a mortality rate of 0.17 per 100,000 population. Highest mortality rates were found in Istanbul (0.83) and Gaziantep (0.71). The mean age was 34.0, and most cases (71.7%) were below the age of 40. The proportion of female cases was 13.6%. Opiates were implicated in 91.5% of deaths and benzodiazepines in 25.9%. Two fifths (38.8%) of the cases involved use of more than 1 drug. In 36.6% of cases, the route of final drug administration was by injection. The most common location of death was at a home (33.7%). In 1998 the number of drug-related death was 58 (Colak, 2006).
In 2006, there were approximately 51 drug-related deaths reported, with 88% being male (n=51) and 12% female; 44 due to opium poppy and derivates; 5 due to amphetamines; 2 due to MDMA. Furthermore, 86% of the drug-related deaths were due to opium poppy drugs and their derivatives, followed by 1% for amphetamines and 4% for ecstasy (Country overview; National Report, 2007).
2.3.2 Drug related crime or (societal) harm
No information found on drug related crime or (societal) harm.
3 Drug policy
3.1 General information
Turkey’s ‘National policy and strategy document on counteracting addictive substance and substance addiction 2006–12’ replaces the former ‘Strategy document on preventing, monitoring and management on drug addiction 1997–2006’. The new strategy is comprehensive, focuses mainly on illegal drugs and covers the same five pillars as in the EU strategy: coordination, supply reduction, demand reduction, international cooperation and information/ research/ evaluation. It also has 12 main objectives, among which are: (1) preventing addictive substance trafficking and abuse, and (2) protecting the whole population and risk groups. The new strategy is complemented by an action plan for the period 2007–09, which was adopted in December 2007 (Country overview).
Besides this strategy an “Action Plan for the Implementation of National Policy and Strategic Document on Counteracting Addictive Substance and Substance Addiction, 2007-2009” (Ministry of Interior, 2007) was produced. Both the National Drug Strategy and First National Drug Action Plan were put in place in 2007.
The Narcotic Coordination Committee has been established recently through the first action plan, and is covering all aspects of the drug phenomenon, not only addiction. This committee consists of all relevant representatives of Ministries. The Turkish Monitoring Centre for Drugs and Drug Addiction (TUBIM) coordinates correspondents all over the country (Country overview).
3.1.1 Policy expenditures
The drug policy expenditures in Turkey increased during the past ten years as the efforts taken by Turkish law enforcement increased substantially. The majority of expenditures target supply reduction (expert’s comments).
Total expenditures on in-patient treatment maybe 3 million TRY (1.5 million)1, for out-patient treatment maybe 2 million TRY (€1 million) (expert’s comments).
3.1.2 Other general indicators
Numbers on arrests and imprisonment for drug-law related offences
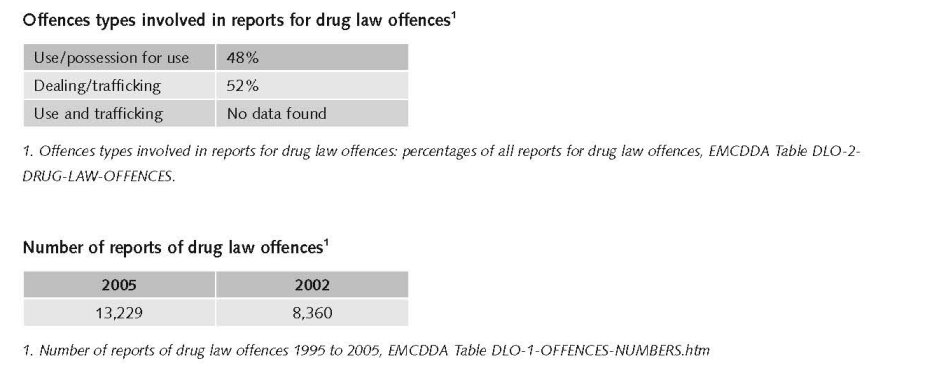
2002 data refer only to police data, while data for the period after 2002 refer to all data reported by the main prosecuting authorities (police, gendarmerie, customs); this change is likely to affect comparability across time (expert’s comments).
1 Exchange rate in December 2008: 1 TRY = €0.5
Numbers on arrests and imprisonment for use/possession for personal use
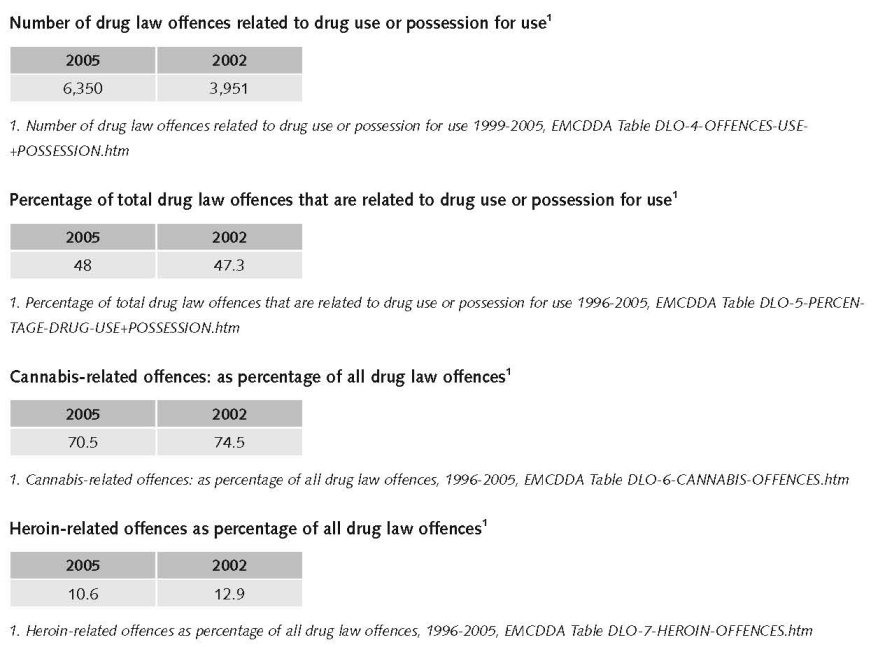
The number of drug related arrests has increased in the past decade; one of the reasons for this increase is the fact that Turkish drug control measures were intensified during this period (expert’s comments).
The Turkish Penal Code outlines prison sentences of one to two years for those who grow, receive or provide drugs for personal use, while someone using drugs may be subjected to treatment and/or probation for up to three years. There is also an option of judicial supervision rather than arrest under the Penal Procedure Code, for any offence with a maximum possible sentence of three years. For any offence committed under the influence of drugs, there is no penalty for an offender who could not comprehend or control his actions (this exemption will not apply if the drugs were taken deliberately). Instead such offenders, and those posing a serious threat to society due to addiction, may be sent to a secure institution for treatment and protection (Country overview).
Since the introduction of the diversion option (June 2005) probation services started, introducing the possibility for judges to divert convicted drug users to treatment. There are 134 branches, and since this date treatment demand increased considerably (expert’s comments).
Production and import or export of drugs are punished by a minimum sentence of 10 years, and sale or supply by a sentence of 5–10 years. However, in this case punishments are linked to drug type, with a specific requirement to increase the above sentences by 50% if the drugs involved are cocaine, heroin, morphine or morphine base; a similar increase is obliged for involvement of organised crime, or individuals in positions linked to legal trade such as doctors, pharmacists, health officers, etc (Country overview).
3.2 Supply reduction: Production, trafficking and retail
The main focus in Turkey is on anti-trafficking measures reflecting Turkey’s geographical position as a transit country.
Both the “National Policy and Strategy Document on Counteracting Addictive Substance and Substance Addiction, 2006-2012” (Ministry of Interior, 2006) and the “Action Plan for the Implementation of National Policy and Strategic Document on Counteracting Addictive Substance and Substance Addiction, 2007-2009” (Ministry of Interior, 2007) have a strong emphasis on supply reduction.
In the National Policy the Republic of Turkey has adopted approaches that:
1. consider crimes related to supply of illicit substances as crimes against humanity and substance addiction as a disease and an important public problem;
2. are based on systematic, holistic, inter-disciplinary, multi-sectoral, mutual communication and interaction in efforts for prevention, protection and rehabilitation aspects of trafficking and abuse of addictive substances under the light of own experiences and practices derived from scientific practices;
3. focus on conducting the activities by means of effective, efficient and dynamic thoughts and in pluralist, multi-dimensional cooperation and coordination within the framework of national and international agreements and new policies and strategies devised in conformity with national legislation; respect the dignity and value of being a human (Ministry of Interior, 2006).
There has been a large increase in supply reduction (anti-trafficking) measures over the past years inside Turkey and at its borders, which might have supported the growth of the Northern Black Sea route (through Ukraine). The number of anti-trafficking operations targeting local drug trafficking organizations increased from 36 in 2005 to 444 in 2007 (National Report, 2007). The number of international operations increased from 12 in 2003 to 47 in 2007 (National Report, 2007). There is also an increase of arrested people and of the amount of drug seizures (expert’s comments).
3.3 Demand reduction: Experimental/recreational drug use + problematic use/chronic-frequent use
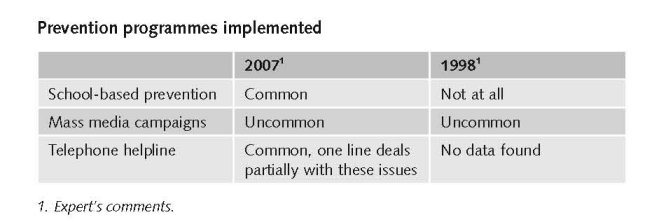
There is a nationwide prevention programme available, but it has so far been fully implemented in 12 provinces only (expert’s comments).
The main prevention programmes undertaken in Turkey focus on a number of areas: increasing awareness of drugs; dissemination of information; increasing individual and social skills; and reinforcing environments that may deter drug-taking (Country overview).
Universal drug prevention in Turkish schools falls under the responsibility of the Ministry of Education. Prevention programmes are mostly targeted at young people through seminars, discussion panels and conferences. Furthermore, training is also provided to teachers and administrators, with the aim of preventing young people from initiating drug use. In 2006, various conferences, seminars, theatre performances and awareness-raising activities were organised around the themes of alcohol, gambling and drug addiction. These were targeted at the general population, non-governmental organisations, public institutions and the private sector (Country overview).
In 2006, a total of 1,013 activities were conducted by 243 personnel, assigned in EGM/KOM/implementation and liaison departments. A total of 178,521 persons were reached, consisting of 7,166 teachers, 15,519 student-guardians, 10,891 NGO members, 5,926 public institutions officers, 6,535 private sector workers and 127,640 primary, high school and university students. In 2006, TUBI.M provincial focal points organised awareness-raising information activities on the prevention of drug use and addiction. These activities were delivered to 10,891 non-governmental organisations, 5,926 public institutions and 6,535 private sector personnel (Country overview).
Drug addiction is considered as an illness, according to regulations (Ministry of Interior 2007a). However, according to the Turkish laws, drug use is defined both as a disease and as criminal act.
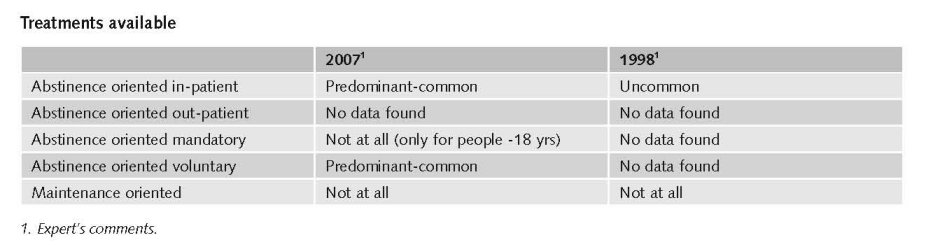
As a result main focus in Turkey is on abstinence oriented drug treatment; substitution treatment (abstinence or maintenance) does not exist (Mathers et al., 2008).
Treatment demand data in Turkey are provided by the Directorate General for Treatment Services of the Ministry of Health.
In 2006, data were gathered from 15 national in-patient treatment centres, out of the 17 in-patient treatment centres (Country overview).
During 2006, a total of 2,853 in-patient clients entered treatment, out of which 1,530 were first-time clients. Data regarding treatment clients suggest that 41.8% of all clients entering treatment reported opioids as the primary drug, followed by 37.2% for cannabis and 3.8% for cocaine and ecstasy respectively. Among first time treatment clients, a slightly different trend was identified, with 50.8% for cannabis, followed by 28.6% for opioids and 4.2% for ecstasy (Country overview).
Furthermore, in 2006, 32% of all clients entering treatment were aged less than 25 years. A higher percentage in age distribution was reported among new treatment clients, with 39.2% under the age of 25 years. As far as gender distribution is concerned 94.6% of all clients were male whereas, a relatively smaller proportion of 5.4% were female. A similar trend in gender distribution was reported among first time treatment clients with 95.4% for male and 4.6% for female (Country overview).
The implementation of drug-related treatment in Turkey falls under the responsibility of the state, where the Science Committee for Methods of Drug Addiction treatment is responsible for the national coordination of drug-related treatment. The main tasks of this committee are to monitor, accredit and evaluate treatment services. Drug-related treatment is provided mainly by public agencies, private entities and NGOs. Funding for drug treatment services is mainly provided by the state and through health insurance funds (Country overview).
The majority of treatment services for problem drug users are aimed at dealing with addiction in general and not specifically for users of illicit drugs. Drug-free treatment aimed at achieving a future drug-free life is the main approach adopted by Turkish treatment programmes. The interventions in drug-free programmes consist of psychotherapeutic methods and supporting methods, with the majority of drug related treatment services taking place within in-patient settings. In Turkey substitution treatment is not yet available (Country overview).
Specific treatment differentiated per substance used exists only in 1 private centre. (There are a few private centres for the treatment of drug addiction in Turkey) (expert’s comments).
The demand for treatment among drug users increased largely after the Probation Act was put in place, in 2006, but the number of users of different substances however, did not increase (expert’s comments).
When the number of people who are in the probation system (diversion) are included, it is obvious that there is a need for more treatment centres and additional expert personnel (National Report, 2007).
There are only data about in-patient treatment available; reliable data for out-patient treatment are not available (National Report, 2007).
Priorities of demand reduction covered by policy papers and/or law
Before 2004, there were no good protocols. Drug treatment services worked according to the hospital rules. There has been no recent change in the laws in last years, but the Turkish penal code has changed, now allowing for diversion (treatment instead of prison sentence).
A change in regulations is needed as the treatment regulations are now still based on a psychiatric concept. Out-patient and long-term in-patient treatment should also be covered (expert’s comments).
A decree concerning certification of doctors, psychiatrists and nurses to be assigned to drug treatment centres dealing with training programmes and examinations has been published. A guide book is prepared for diagnosis and treatment criterion to be used as education curriculum (Ministry of Interior, 2007a). There are now official Regulations for Drug Addiction Treatment Centres and a Drug Addiction Treatment Methods Scientific Commission (Ministry of Interior, 2007a). Drug treatment is also a priority in the “National Policy and Strategy Document on Counteracting Addictive Substance and Substance Addiction, 2006-2012” (Ministry of Interior, 2006) and the “Action Plan for the Implementation of National Policy and Strategic Document on Counteracting Addictive Substance and Substance Addiction, 2007-2009” (Ministry of Interior, 2007).
The most important statements
The main objectives of the National Strategy are as follows:
1. Preventing addictive substance trafficking and abuse;
2. Protecting the whole population and risk groups;
3. Improving the existing organizational network in order for all parties to conduct more effective activities for risk groups;
4. Supporting the structures with specialized and qualified personnel to work professionally in the fields of protection, prevention and training;
5. Completing the institutional structuring and increasing the administrative capacity of the centre as EMCDDA Turkish National Focal Point and provinces, better functioning of the organizations, creating a holistic, multi-organizational and shared database and establishing a working environment based on coordination and cooperation;
6. Considering utmost benefit to the society and individuals in line with prevention of substance abuse and trafficking;
7. Protecting the health of communities and individuals at national and international levels;
8. Raising independent, creative, productive and qualified children and young people who are healthy in physical, emotional and social aspects;
9. Providing children and young people with better opportunities for living, protection, growing, and participation parallel to International Convention on the Rights of Child;
10. Developing programmes and projects that will ensure effective participation of children and young people in social life;
11. Educating young people to make them responsible individuals in every field and level (Principles of International Youth Year - 1985);
12. Providing a safe, qualified life with high level of freedom, justice, safety and welfare through an effective fight against trafficking and abuse of addictive substances in the world and Turkey;
13. Creating a social solidarity which will allow every individual in all segments of the society to be sensitive to each activity encouraging committing crime or using an addictive substance (Ministry of Interior, 2006).
The primary objective of the First National Action Plan: to prevent public use of illicit drugs and drug-related crimes, to reduce harmful effects of drugs on public and public health and to improve treatment facilities (Ministry of Interior, 2007).
Those priorities are covered by law and legal provisions, among which the Turkish Drug Law, the Law Concerning the Protection of Families, Highway Traffic Law, Code of Criminal Procedure, Turkish Civil Code, and the Turkish Penal Code.
3.4 Harm reduction
3.4.1 HIV and mortality
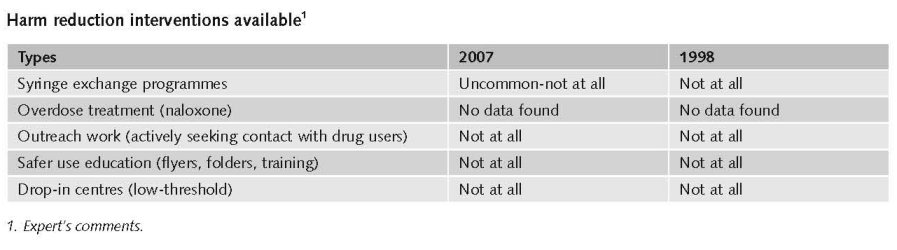
Harm reduction does not exist as such in Turkey. Substitution treatment is not available but pending for approval. Needle and syringe exchange programs are not available (Mathers et al., 2008) except for some harm reduction intervention at a local level. There are mentions of some needle and syringe exchange in Istanbul (expert’s comments).
Harm Reduction is mentioned in the National Drug Strategy and First National Drug Action Plan as well as in treatment protocols. However there are no programmes yet.
The third ‘National strategic AIDS action plan for the years 2007–11’ was adopted in 2006. This action plan includes targets and strategies concerning prevention, diagnosis and increased access to treatment, increased education, and development of legislation, social support, monitoring, and evaluation of activities regarding HIV/AIDS/HBV/HBC. Several activities are planned for 2008, such as increasing the awareness among intravenous drug users of HIV-AIDS, investigating behavioural changes associated with drug use, training field workers, as well as the ‘Turkey HIV/AIDS prevention and support programme’. Currently, neither opioid substitution treatment nor needle and syringe exchange programmes are available in Turkey (Country overview).
3.4.2 Crime, societal harm, environmental damage
No information found on interventions/measures to reduce harm for society.
References
Consulted experts
M. Akilli, Head of Department, Directorate General of customs enforcement.
P. Altan, Head of STIs Department, Program Director, HIV/IDS Prevention and Support Program PIU, Ministry of Health.
T. Aydin, Central counter narcotics division, Superintendent, Department of Anti-smuggling and organized crime.
T. Bora, Superintendent, Forensic chemist expert, Ministry of Interior, General Directorate of Turkish national police department of Ankara criminal police laboratories.
A. Gevenkiris, Turkish Grain Board, Director of poppy and alkaloid affairs department.
A. Hakan, Expert doctor, Chairman of forensic medicine institute. Ankara Office.
K. Kamer Vehbi, Department Head for probation and help centres.
E. Kavasoglu, Ministry of Health, Treatment service.
B. Levent, General Director of Special Education and psychological Counselling, Ministry of Education.
A. Pek, Head of Anti-Smuggling and Organized Crime Department, KOM.
M. Tokac, General manager of pharmaceuticals and pharmacies.
Documents
CIA. The World Factbook: Turkey. Available: www.cia.gov/library/publications/the-world-factbook/geos/tu.html, last accessed 10 December 2008.
Colak B, Baser L, Yayci N, Etiler N; Inanici MA. Deaths from drug overdose and toxicity in Turkey 1997-2001. The American Journal of Forensic Medicine and Pathology 2006; 27(1):50-4.
Cook C, Kanaef N. Global state of harm reduction 2008. Mapping the response to drug-related HIV and hepatitis C epidemics. London, International Harm Reduction Association (IHRA), 2008.
Country overview: Turkey: Available: http://www.emcdda.europa.eu/publications/country-overviews/tr, last accessed 20 December 2008.
Mathers BM, Degenhardt L, Phillips B, Wiessing L, Hickman M, Strathdee SA et al. for the 2007 Reference Group to the UN on HIV and Injecting Drug Use. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review, 2008.
Ministry of Interior. National Policy and Strategy Document on Counteracting Addictive Substance and Substance Addiction, 2006-2012. Ankara, 2006.
Ministry of Interior. Action Plan for the Implementation of National Policy and Strategic Document on Counteracting Addictive Substance and Substance Addiction, 2007-2009. Ankara, 2007.
Ministry of Interior, Turkish National Police, Department of anti-smuggling and organised crime. Turkish Report on Organized Crime and Drugs 2007. Ankara, 2007a.
National Report to the EMCDDA, Turkey, 2007.
UNDCP (United Nations International Drug Control Programme). Studies on Drugs and Crime. Global Illicit Drug Trends 2000. Statistics. Vienna, UNDCP, 2001.
UNODC (United Nations Office on Drugs and Crime). World Drug Report 2008. Vienna, UNODC, 2008.
UNODC. World Drug Report 2008. Global ATS Assessment. Vienna, UNODC, 2008a.
| < Prev | Next > |
|---|