| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Appendix to report 4: country reports SOUTH AFRICA
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
SOUTH AFRICA
1 General information
Location:
Southern Africa, at the southern tip of the continent of Africa
Area:
1,219,912 sq km
Land boundaries/coastline:
4,862 km / 2,798 km
Border countries:
Botswana 1,840 km, Lesotho 909 km, Mozambique 491 km, Namibia 967 km, Swaziland 430 km, Zimbabwe 225 km
Population:
48,782,756
Age structure:
0-14 years: 29.2% (male 7,147,151/female 7,120,183)
15-64 years: 65.5% (male 16,057,340/female 15,889,750)
65 years and over: 5.3% (male 1,050,287/female 1,518,044) (2008 est.)
Administrative divisions:
9 provinces; Eastern Cape, Free State, Gauteng, KwaZulu-Natal, Limpopo, Mpumalanga, Northern Cape, North-West, Western Cape
GDP (purchasing power parity):
$467.8 billion (2007 est.)
GDP (official exchange rate):
$282.6 billion (2007 est.)
GDP- per capita (PPP):
$9,700 (2007 est.) (CIA World Factbook)
Drug research
Much of the available information on substance use come from occasional national surveys and irregularly studies conducted in specific locations (e.g. Capetown and the area of Johannesburg) and from information on police arrests and seizures (Da Rocha Silva, 1998).
• Research on drug use and related harm on national and local level and on an ongoing basis (monitoring) does not exist or has been partially developed in South Africa. This research tends to be initiated sporadically within selected communities. Some communities or populations have been severely neglected, such as rural communities and out-of-school young people (Da Rocha Silva et al., 2007; Peltzer et al., 2008);
• Researchers generally do not specialise in drug research (Da Rocha Silva et al., 2007; Peltzer et al., 2008);
• SACENDU=South African Community Epidemiological Network, an integrated drug information system. SACENDU is a network of researchers, practitioners and policy makers, meeting every six months to discuss about quantitative and qualitative data on drugs (research and other kinds) (UNODC, 2002).
Main drug-related problems
The main problem of South Africa is trafficking and consumption. There is also cannabis herb production and increasing production of synthetic drugs, both for the domestic market.
2 Drug problems
2.1 Drug supply
2.1.1 Production
There was large scale cannabis cultivation in small remote and mountainous or otherwise inaccessible spots. There is no evidence for plantation style cultivation in South Africa in 1998-2001.
Data come from aerial surveys initiated by the South African Police Service’s Aerial Application Unit or subcontractors. Crop eradication efforts have been undertaken. Estimates on the amount of hectares fluctuate significantly over the years and some apparent inconsistencies in reporting have been discovered (UNODC, 2002).
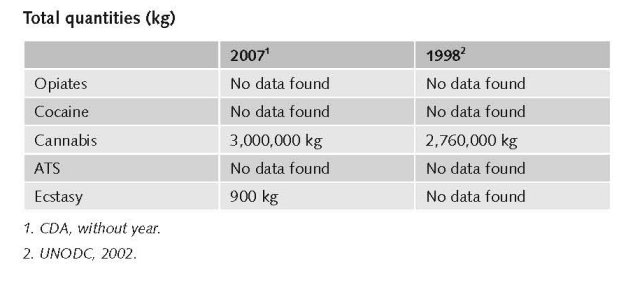
Estimated production area for cannabis in 1998 is 1,300 hectares. The standard yield is reported to be 2,120 kg/ha, resulting in 2,760,000 kg cannabis in 1998. This is equivalent to around 830,000 kg marijuana. Most consumed cannabis during 1998-2001 comes from South Africa (UNODC, 2002).
Cannabis plant production is reported to be 3,000,000 kg (the measuring year is not reported but probably 2006), half of which is use in South Africa. Estimates of cannabis production areas have been controversial in recent years, with some unrealistically high figures put forward by the authorities. Current estimates put the amount of land under drug cultivation at 1,000-1,200 hectares (UNODC, 2003).
The production of ecstasy is estimated 900 kg (CDA).
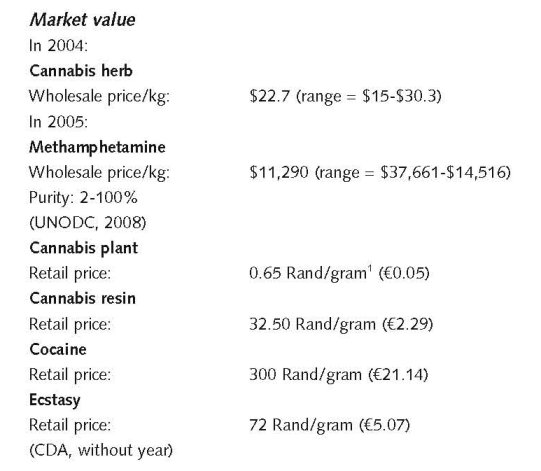
Market value of these drugs/price per gram
No data found on market value of these drugs/price per gram.
2.1.2 Trafficking
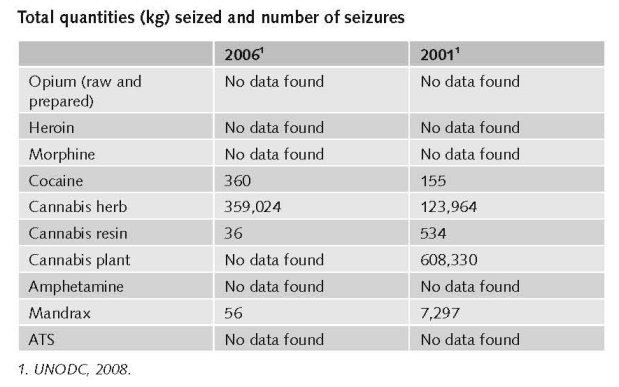
UNODC mentions statistics from the South African Narcotics Bureau (SANAB) indicating that a total of 495,928 kg of cannabis plant was seized in 2001 which is reported to be a considerable decline of the number of seizures since 1994 (700,000 kg) (UNODC, 2003).
The 2002 UNODC Country Profiles on Drugs (mentions different statistics and partly for other years. Seizures of cannabis have been subject to major annual fluctuations during the 1990s. In 2000 718,000 kg of cannabis herb was seized, ranking second behind the weight of the Mexican seizures (2,050,000 kg). Mandrax is a popular drug (downer) in South Africa (imported from India and China) of which 5,436 kg was seized in 2001. In 2001, 284 kg cocaine was seized. The numbers are on average increasing between 1998 and 2001 (UNODC, 2002).
Seizure reports of amphetamine should be treated with caution because what is seized as amphetamine or “speed” in the South African context is often ephedrine.
South Africa plays an important role in trans-shipment of heroin, hashish, and cocaine. The geographical position, porous borders and international trade links with Asia, Latin America, Western Europe and North America have made it an attractive drug transit country (UNODC, 2002).
1 1 ZAR = €0.0704823. Exchange rate 18 December 2008.
2.2 Drug Demand
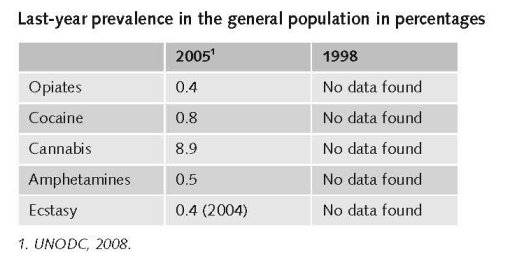
2.2.1 Experimental/recreational drug users in the general population
General picture around 1998
Reliable national statistical data on drug use prevalence are absent in South Africa. Studies are local or regional, predominantly in densely populated regions e.g. Capetown, Gauteng (Johannesburg and Pretoria), and Durban. Statistics used for 1990-2001 were mainly based on drug-related arrests and treatment seekers (UNODC, 2002).
In 1998 cannabis was probably the most frequently used illicit drug, followed by Mandrax that is mostly used combined with cannabis (‘white pipe’). Depressants (benzo’s etc.) and inhalants are third and fourth. Cocaine (crack) is the fifth most popular drug. ATS is sixth and heroin and other opiates seventh.
This sequence in popularity has not changed substantially (Department of Social Development, 2007).
2 $1 = €0.690578. Exchange rate 17 December 2008.
General picture around 2006/2007
Sophisticated, methodologically comparable national surveys, and especially general population surveys, on drug use are rare in South Africa, particularly with regard to young people (Da Rocha Silva & Malaka, 2007).
Accurate, up-to-date statistical data on drug use in South Africa are difficult to obtain. Instead deductions are made from recent research, departmental reports and information from international sources (Department of Social Development, 2007).
During the years before 2005 there has been an increase in drug use among younger people (under 20 years) in the Western Cape, namely from 5% in 1996 to 25% in the first half of 2004 (Parry, 2006).
“A new trend is the movement of drug consumption from traditional white urban areas to black communities, schools and universities” (Department of Social Development, 2007).
Life-time prevalence in the general population in percentages
There are no official prevalence figures. Results of repeated local surveys suggest that cannabis is most prevalent and Mandrax (primarily imported from India and China) is second most commonly used. Mandrax is frequently smoked with cannabis (‘white pipe’). Although heroin, cocaine and ecstasy are less commonly used, since mid-1990s sentinel surveillances point at significantly increased use of these drugs. In urban areas cocaine is particularly associated with crack from 1998 on. Glue and solvent sniffing is a common problem among street children and youth (UNODC, 2002).
Last-month prevalence in the general population in percentages
The only school-based Youth Risk and Behaviour Survey (YRBS) conducted in 2002 in South Africa found that current (past month) use of cannabis was 9% among students. In a national household survey in 2005 cannabis prevalence was 2% in the past 3 months among 15-19 year-olds and 1.7% in persons 15 years and above (Peltzer et al., 2008).
Higher current cannabis use rates were found in urban (2.3%) than in rural (1%) areas in 2005. These rates were not found to be related to education level (Peltzer et al., 2008).
Past three months use appears to be well under 1% for most other illicit drugs in general population samples studied in 1994 (Human Science and Research Council (HSRC) African Blacks, 10-21 yrs.), 2002 (YRBS, 13-19 yrs.), and 2005 (SABSSM II, 15-19 vs. > 20). These drugs were inhalants, mandrax, cocaine, opiates, club drugs, hallucinogens, and over-the-counter prescription drugs. Thus, the past month prevalence is smaller (Peltzer et al., 2008).
Current drug use is lower compared with the USA and Australia, though it is difficult to compare different surveys and different populations (Peltzer et al., 2008).
No data found on life-time, last-year or last month prevalence among young people 15-24.
Sophisticated, methodologically comparable national surveys, and especially general population surveys, on drug use are rare in South Africa, particularly with regard to young people (Da Rocha Silva & Malaka, 2007).
2.2.2 Problematic drug users/chronic and frequent drug users
No data found on the number of problematic/chronic-frequent users of opiates, cocaine, cannabis and ATS in the general population in 2007 and before (1998).
The number of injecting drug users in the general population
“Injecting drug use: IDU is not common, but information on drug abuse is not complete and the real situation may be more problematic than it currently appears.” (UNODC, 2002).
An extrapolation of figures from Shisana et al. (2005) result in 16,145 injecting drug users of 15 years and older, having injected recently (last three months) or longer ago (not specified) (expert’s comments).
No data found on the number of injecting drug users among younger people (< 20 years).
2.3 Drug related Harm
2.3.1 HIV infections and mortality (drug related deaths)
The number of HIV infected injecting drug users
There is no good information on HIV prevalence among injecting drug users (Parry et al., 1999).
Few studies are done and these are mainly focussing on HIV prevalence rates among samples of arrestees in Capetown, Durban and Johannesburg or on the association between drug use and HIV prevalence. Only 1.3% reported injecting drug use and 0.8% needle sharing. Still, IDUs had higher rates of HIV infection than non-IDUs (Parry & Pithey, 2006).
No data found on the number of newly HIV infected injecting drug users in 2007 and the ten years before and on the number of drug related deaths by overdose in 2007 and the ten years before.
2.3.2 Drug related crime or (societal) harm
Criminality has increased and partly changed in origin during the past ten years. Criminal syndicates from Nigeria and other Central African countries have intruded the drug market now. And South Africa has become a transhipment point for illegal drugs coming from South America and largely going to Europe (Shaw, 2002).
It is also hypothesised that the large influx of people from other African countries (Zimbabwe and other areas) to what is perceived as a more wealthy and stable country (South Africa) has resulted in a dramatic increase of both legal and illegal immigrants, in greater unemployment, thus also in a need to escape to illegal income-creating activities. Drugs provide an easy way of achieving this. Coupled to a suspected involvement of some members of the security personnel (police and customs) in the drug trade, this has led to the exploitation of both the needy and the infrastructure in the drug trade (expert’s comments).
3 Drug policy
3.1 General information
“The basis for the national drug control framework is the National Drug Master Plan (Master Plan), adopted by parliament in February 1999.” Before that plan the response of government was “disjointed, fragmented and uncoordinated” (UNODC, 2002). The National Master Plan, created a quasi-governmental Central Drug Authority (CDA) to monitor its implementation. Its role has been limited substantially due to insufficient financial resources (UNODC, 2002).
Ten years ago the priorities of the master plan were: crime, youth, community health welfare, research and information dissemination, and international involvement (Drug Advisory Board, 1999). In 2007 other priorities (vulnerable groups) were added to these: e.g. children, people with disabilities, elderly, HIV/AIDS infected people), communication (cross-cutting area), capacity building, and occupational groups at risk. In both the annual reports of 2006/7 and 2007/8 (p. 32), the Central Drug Authority advocated and recommended the adoption of an integrated strategy to combat the drug problem, with the elements being supply, demand and harm reduction (CDA, 2008). There are also critical remarks made on the fact that harm reduction still does not have high priority in South Africa (Leggett, 2008).
3.1.1 Policy expenditures
Ten years ago it was considered impossible to determine accurately the amount of Government spending on drug supply and demand reduction activities. However, the money spent on demand reduction is generally considered low, when compared to supply reduction (UNODC, 2002). Detailed data were and are not available. Government subsidies are paid to registered treatment centres and other organisations. The amounts of money are based on requirements defined in agreed business plans produced by these centres and organisations (expert’s comments). Funding for treatment (demand reduction) was very limited (1998-2001), thus the main activities were done by NGOs. Still there was a relatively wide network of public and private substance abuse treatment facilities including some 300 organisations for support and after care, largely in urban areas (the former townships are not covered): 67 community treatment facilities, 147 provincial and private hospitals and psychiatric hospitals, 12 detoxification facilities and 25 specialist in-patient units/half-way houses (UNODC, 2002).
3.1.2 Other general indicators
Numbers available on arrests and imprisonment for drug-law related offences
Based on data from local studies (in Capetown, Durban and Gauteng) it has been concluded that compared with cocaine, since 1999 a larger percentage of all drug-related arrests have been related to ecstasy. The absolute number of heroin-related arrests is however still relatively low.
The national number of cannabis-related arrest (for both possession and sales) in 1998 was estimated to be around 6,000, for mandrax this number was some 1,100 and for heroin it was 60. These numbers were on average increasing until 2001 (UNODC, 2002).
“Drug-related arrests had declined from a peak of over 47,000 in 1994 to 40,000 in 1998. In 2001, 49,323 such cases were made.” (UNODC, 2003). No data were found for more recent years.
No data found on numbers on arrests and imprisonment for use/possession for personal use.
3.2 Supply reduction: Production, trafficking and retail
Priorities of supply reduction covered by policy papers and/or law
In 1998-2001, law enforcement activities were mainly focussed on reducing drug production and drug trafficking (UNODC, 2002). In a more recent publication it was concluded that South African drug enforcement was primarily directed against large scale distributors and trafficking syndicates. Local police seldom focus upon retail level distributors (Peltzer et al., 2008).
The most important statement in the National Master Plan, approved in 1999, is to ensure that the law is effectively enforced, especially against those involved in the supply and trafficking of illegal drugs. Drug policy statements (objectives) on this subject have not been substantially changed during the past ten years (Drug Advisory Board, 1999; Central Drug Authority, 2007).
There have been changes from a purely supply reduction approach towards a combination of supply and demand reduction in the period ending in 2006. There is also a shift towards including a culturally-acceptable form of harm reduction since 2006, i.e. an integrated approach (expert’s comments). Harm reduction (i.e. needle exchange programmes) is still culturally unacceptable, but “some” maintenance treatments exist.
The Medicines and Related Substances Control Act (101/1965): provides a definitional and conceptual basis for drug control policy. The South African Drugs and Drug Trafficking Act (140/1992) forbids the trafficking of drugs or precursors. Drug dealing is punishable up to 25 years imprisonment. Drug possession up to 15 years (UNODC, 2002). Pending change in legislation governing the Central Drug Authority (presently the Substance Abuse Act: Act 20 of 1992) and prevention and treatment of substance abuse, to enable the Central Drug Authority (CDA) to execute its mandate more effectively and to enable the national Department of Social Development to set and enforce norms and standards for the committal, treatment and aftercare of ‘service users’ (usually ‘addicts’ or ‘substance dependents’) both voluntary and involuntary (UNODC, 2002). Legal changes were designed to provide the Central Drug Authority with an implementing structure nation-wide to work on department and province-specific (mini) drug master plans. This concerns both supply and demand reduction (expert’s comments).
3.3 Demand reduction: Experimental/recreational drug use + problematic use/chronic-frequent use
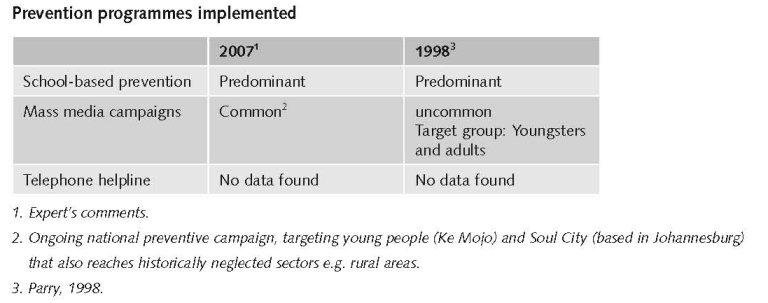
In 1998-2001 no national programme for primary drug prevention was available in South Africa (UNODC, 2002).
Nowadays, maintenance treatment units for opiate users are absent, treatment is abstinence oriented. Both in-patient and out-patient treatment are available (expert’s comments). Substitution therapy is available “(…) for detoxification. Methadone is available as high alcohol-content syrup (Physeptone) while buprenorphine is available at a few private facilities.” (Weich et al., 2008; also cited by: Carney & Parry, 2008).
Still there is a relatively wide network of public and private substance abuse treatment facilities including some 300 organisations for support and after care, largely in urban areas (the former townships are uncovered!): 67 community treatment facilities, 147 provincial and private hospitals and psychiatric hospitals, 12 detoxification facilities and 25 specialist in-patient units/half-way houses (UNODC, 2002). Some authors estimates the number of treatment sites at 72-120 (Carney & Parry, 2008).
“South Africa has few state-funded facilities dedicated to substance-abuse treatment, thus drug-treatment services are provided primarily by private facilities (Myers, 2004, 2005). In recent years state funding to state-subsidized specialist treatment facilities has been decreased significantly.” (Dewing et al., 2006). There are currently five state-funded specialist treatment centres. The capacity is insufficient for the treatment demand in the country. Additionally, there is a proliferation of private treatment centres over the past decade. Few addicted people can afford this (expert’s comments).
Priorities of demand reduction covered by policy papers and/or law
The following priorities were formulated in 1999:
• Motivate youth to refrain from drug abuse;
• Ensure that schools offer effective programmes on drug education, giving pupils the facts, warning them against the risks, and helping them to develop the skills and attitudes to resist drug misuse;
• Develop effective national and local public education strategies focusing particularly on young people;
• Ensure that individual drug abusers have access to a range of advice, counselling, treatment, rehabilitation and after-care services (Drug Advisory Board, 1999).
Some issues were at a later date added e.g. training young people as peer educators (Central Drug Authority, 2007).
Published national drug policy papers from 1999 and 2007 have not significantly been changed in the past ten years. The master plans (Drug Advisory Board, 1999; CDA, without year) are mainly descriptions of what should be done, not what has been done (CDA, without year). The implementation of the National Drug Master Plan is guided by Act 20 of 1992. It is presently under review and is scheduled to be enacted in 2009 (expert’s comments).
3.4 Harm reduction
3.4.1 HIV and mortality
Harm reduction in the South African context has been associated primarily with ‘needle exchange programmes’, a concept that is culturally unacceptable (expert’s comments). There is no legal restriction to setting up syringe exchange programmes (Leggett, 2008).
South Africa currently has targeted programmes for IDUs, as information and awareness programmes run by government and civil society that address the link between drug use and HIV (Carney & Parry, 2008). In an effort to enable a shift to be made from the present limited perception of harm reduction to a more culturally acceptable one, the Central Drug Authority has tentatively defined harm reduction in the South African context as including: detoxification and rehabilitation; aftercare and re-integration; medical treatment of problems related to drug use and abuse; education and communication related to long-term recovery; substitution therapy and controlled drug use; control of legal distribution and access to illicit drugs; programmes for limiting the spread of HIV/AIDS and TB etc through intravenous drug use (Central Drug Authority, 2007).
3.4.2 Crime, societal harm, environmental damage
No information found on interventions/measures to reduce harm for society.
References
Consulted experts
R. Eberlein, Member of the Executive Committee of the Central Drug Authority.
T. Leggett, Research Officer, Vienna-based UN Office on Drugs and Crime.
D. Malaka, Associate Professor, Department of Social work, University of the North.
C. Parry, Director, Alcohol and Drug Abuse Research Group, Medical Research Council (MRC).
L. Da Rocha Silva, Director Centre for Alcohol/Drug-related Research (CADRe).
Documents
Carney T, Parry CDH. Harm reduction in Southern Africa: Strategies used to address drug-related HIV (and Hepatitis C). Brief report prepared for the IHRA on which information exists around drug use, injecting drug use, HIV and harm reduction in 10 Southern African countries. July 3rd, 2008.
CDA. National Drug Master Plan 2006-2011. Pretoria, Central Drug Authority, (without year).
Central Drug Authority. Annual Report 2005/6. Pretoria, 2007.
Central Drug Authority. Annual Report 2006/7. Pretoria, 2008.
CIA World Factbook: South-Africa. Available: www.cia.gov/library/publications/the-world-factbook/geos/sf.html, last accessed on 10 December 2008.
Da Rocha Silva L. Alcohol. tobacco and other drug use: Young South Africans (10-24 years). Paper presented at the XIth International Conference on Alcohol, Liverpool, UK, April 1998.
Da Rocha Silva L, Malaka D. An analysis of South African drug-related research and future directions. The Social Work Practitioner-Researcher, 2007, 19(3): 1-21.
Department of Social Development. National Drug Master Plan 2006-2011. Pretoria, Department of Social Development, 2007.
Dewing S, Plüddemann A, Myers BJ, Parry CDH. Review of injecting drug use in six African countries: Egypt, Kenya, Mauritius, Nigeria, South Africa and Tanzania. Drugs: education, prevention and policy, 2006, 13(2): 121-137.
Drug Advisory Board. National Drug Master Plan. Pretoria, Drug Advisory Board, 1999.
Leggett T. Intravenous drug use in South Africa. In: Karim SSA, Karim QA. (eds.). HIV/AIDS in South Africa. Cambridge, Cambridge University Press, 2005, 2008 (2nd): 217-225.
Parry CDH. Substance abuse in South Africa: Country report focussing on young persons. Prepared for the WHO/UNODC Regional Consultation – Global initiative on primary prevention of substance abuse among young people. Harare, Zimbabwe, February 24-26th 1998.
Parry CDH, Karim QA. Country report: Substance abuse and HIV/AIDS in South Africa. Atlanta (Georgia), Global Research Network on HIV prevention in drug-using populations. 2nd Annual Meeting Report, August 26-28, 1999.
Parry CDH, Pithey AL. Risk behaviour and HIV among drug using populations in South Africa. African Journal of Drug and Alcohol Studies, 2006, 5(2): 140-157.
Peltzer K, Ramlagan S, Johnsons BD, Phaswana-Mafuya N. Illicit drug use and treatment in South Africa: a review. (Substance Use & Misuse, in print).
Shaw M. West African criminal networks in South and Southern Africa. African Affairs, 2002, 101: 291-316.
Shisana O, Rehle T, Simbayi LC, Parker W, Zuma K, Bhana A, Connolly C, Pillay JS, et al. South African National HIV prevalence,
HIV incidence, behaviour and communication survey, 2005. Cape Town, Human Sciences and Research Council (HSRC), HSRC-Press, 2005.
UNODC (United Nations Office on Drugs and Crime). Country profile on drugs and crime. UNODC, Regional Office for Southern Africa, 2002.
UNODC. Strategic programme framework on crime and drugs for
Southern Africa 2003. UNODC Regional Office for Southern Africa, 2003.
UNODC. World Drug Report 2008. Vienna, UNODC, 2008.
Weich L, Perkel C, van Zyl N, Rataemane ST, Naidoo L. Medical management of opioid dependence in South Africa.
South African Medical Journal, 2008, 98(4): 280-283.
| < Prev | Next > |
|---|