| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Appendix to report 4: country reports PORTUGAL
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
PORTUGAL
1 General information
Location:
South-western Europe, bordering the North Atlantic Ocean, west of Spain
Area:
92,391 sq km
Land boundaries/coastline:
1,214 km / 1,793 km
Border countries:
Spain 1,214 km
Population:
10,676,910 (July 2008 est.)
Age structure:
0-14 years: 16.4% (male 912,995/female 835,715)
15-64 years: 66.2% (male 3,514,905/female 3,555,097)
65 years and over: 17.4% (male 764,443/female 1,093,755) (2008 est.)
Administrative divisions:
18 districts and 2 autonomous regions
GDP (purchasing power parity):
$232.3 billion (2007 est.)
GDP (official exchange rate):
$223.3 billion (2007 est.)
GDP- per capita (PPP):
$21,800 (2007 est.) (CIA World Factbook)
Drug research
Drug research is coordinated and funded by the National Focal Point at the Institute for Drug and Drug Addiction (Instituto da Droga e da Toxicodependência - IDT), which is also a major actor in undertaking research, together with university departments. Recently, a national network was set up by a group of researchers for the discussion and dissemination of academic work in this area. The national focal point, through its website and reports, and the national scientific journals are the main dissemination channels for drug-related research findings (Country overview).
Main drug-related problems
The main drug problem in Portugal is consumption and trafficking, in particular transhipment of cocaine from West-Africa to European countries and of cannabis resin from Morocco to other countries in Europe. Production plays no significant role.
2 Drug problems
2.1 Drug supply
2.1.1 Production
No reports found on production of illicit drugs in Portugal.
2.1.2 Trafficking
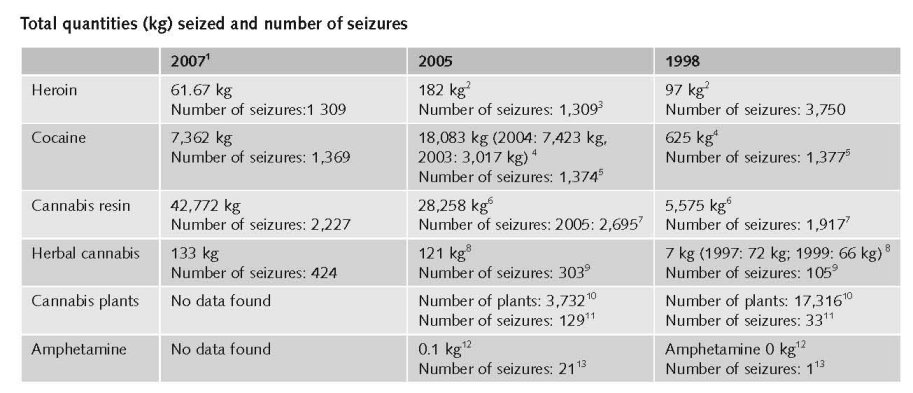
1. Expert’s comments.
2. Quantities (kg) of heroin seized, 1995 to 2005 - EMCDDA Table SZR-8-SEIZURE-HEROIN-QUANTITY.htm
3. Number of heroin seizures, 1995 to 2005 - EMCDDA Table SZR-7-SEIZURE-HEROIN-NUMBER.htm
4. Quantities (kg) of cocaine seized, 1995 to 2005 - EMCDDA Table SZR-10-SEIZURE-COCAINE-QUANTITY.htm
5. Number of cocaine seizures, 1995 to 2005 - EMCDDA Table SZR-9-SEIZURE-COCAINE-NUMBER.htm
6. Quantities (kg) of cannabis resin seized, 1995 to 2005 - EMCDDA Table SZR-2-CANNABIS-QUANTITY.htm
7. Number of Cannabis resin seizures, 1995 to 2005 - EMCDDA Table SZR-1-SEIZURE-CANNABIS-NUMBER.htm
8. Quantities (kg) of herbal cannabis seized, 1995 to 2005 - EMCDDA Table SZR-4-SEIZURE-HERBAL-CANNABIS-QUANTITY.htm
9. Number of herbal cannabis seizures, 1995 to 2005 - EMCDDA Table SZR-3-SEIZURE-HERBAL-CANNABIS-NUMBER.htm
10. Quantities (number of plants) of cannabis plants seized, 1995 to 2005 - EMCDDA Table SZR-6-SEIZURE-CANNABIS-PLANTS-QUANTITY.htm
11. Number of seizures of cannabis plants, 1995 to 2005 - EMCDDA Table SZR-5-SEIZURE-CANNABIS-PLANTS-NUMBER.htm
12. Quantities (kg) of amphetamine seized, 1995 to 2005 - EMCDDA Table SZR-12-SEIZURE-AMPHETAMINES-QUANTITY.htm
13. Number of amphetamine seizures, 1995 to 2005 - EMCDDA Table SZR-11-SEIZURE-AMPHETAMINE-NUMBER.htm
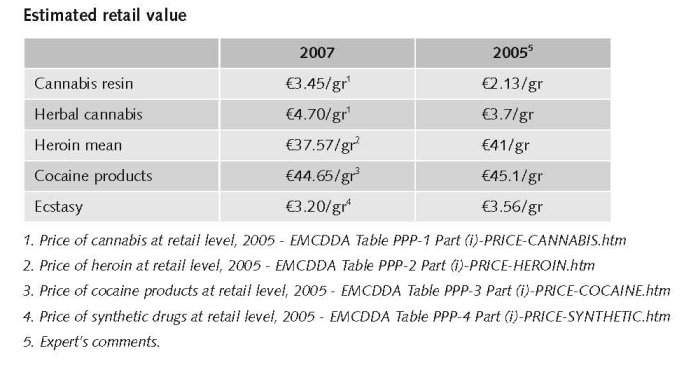
Estimated market value
Regarding the prices of drugs at trafficker and trafficker-user level the mean prices of herbal cannabis and ecstasy were the lowest reported since 2002, contrary to cocaine which registered in 2006 the highest price since 2002 (National Report, 2007).
In comparison to 2006, in 2007 the price of drugs at trafficker and trafficker-user level suffered some variations, with the decrease registered in the average price of heroin and the increase in the average price of hashish and herbal cannabis (liamba).
The mean price of heroin was the lowest reported since 2002, contrary to cocaine which for the third consecutive year was priced higher than heroin. The mean prices of hashish and herbal cannabis (liamba) registered the highest values since 2002. For the first time since 2002, was broken the increase trend of cocaine price and the decrease of ecstasy price (National Report, 2007).
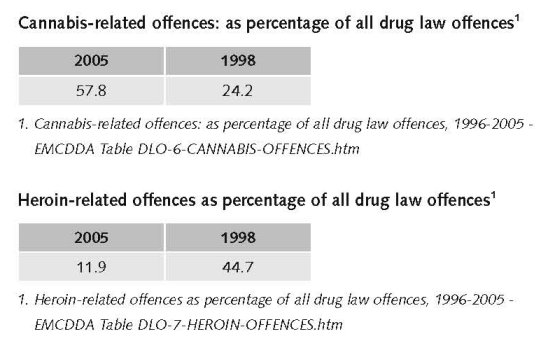
Following the trend, which has been verified since 2000, the number of heroin seizures decreased and now ranks below hashish and cocaine. However, the number of seizures increased for all substances in comparison to previous years. For the fifth time since 1990, the number of hashish seizures again surpassed that of heroin, the substance that always registered the highest number of seizures in Portugal until 2002, and for the second time the number of cocaine seizures also surpassed that of heroin (National Report 2007). Portugal plays an important role in cocaine and cannabis resin transhipment from North-West Africa to European countries (UNODC, 2008).
2.1.3 Retail/Consumption
2.2 Drug Demand
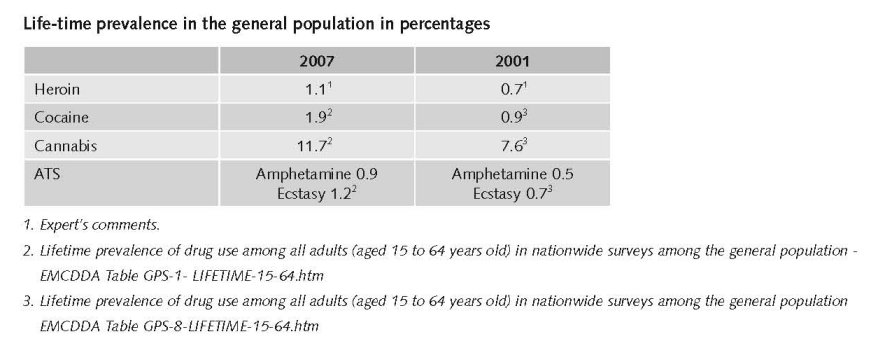
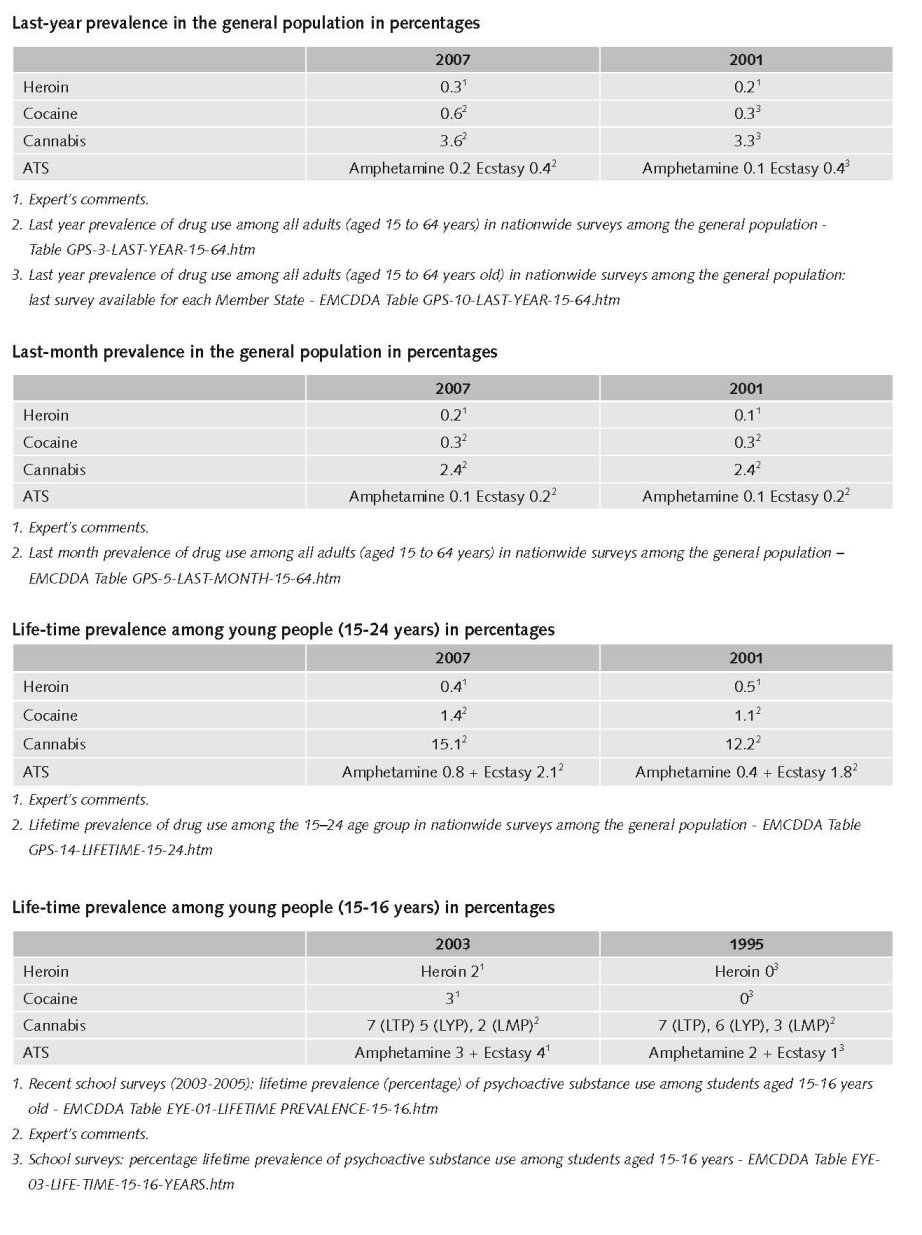
2.2.1 Experimental/recreational drug users in the general population
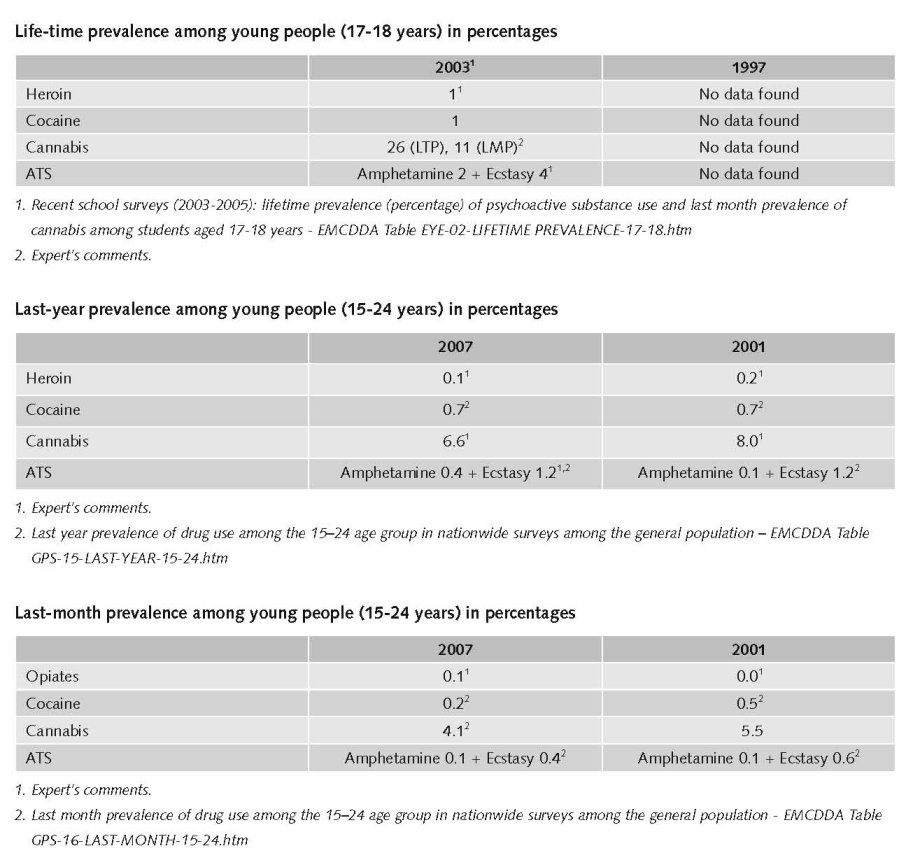
The first general population survey on drug use was conducted in Portugal in 2001. A sample of 15,000 individuals representative of the Portuguese population was surveyed. The results revealed that 7.8% of respondents aged 15 to 64 had used an illegal drug at least once in their lives (lifetime prevalence). The most-reported substance in this context was cannabis (7.6% lifetime prevalence). The use of other illegal substances was less frequently reported. Lifetime prevalence was less than 1% for cocaine, heroin, ecstasy, amphetamines and LSD. The second national survey, carried out among the general population in 2007, indicated 11.7% lifetime prevalence of cannabis use and 1.9% for cocaine use among the age group 15–64. Last year prevalence for cannabis use was reported by 3.6% of the sample, while 0.6% reported cocaine use (Country overview).
Data from the ESPAD surveys suggest an increase in experimentation, as well as in recent and in current use of almost all illicit drugs. The ESPAD survey results of 2003 showed that the lifetime prevalence rate for any illicit drug use increased to 18% (compared to 12% in 1999). As regard individual drugs, the lifetime prevalence rate for marijuana/hashish increased to 15% (9% in 1999). Three percent of the students admitted the use of cocaine at least once in their lives (1.3% in 1999) and 4% reported lifetime use of ecstasy (2.3% in 1999). The lifetime prevalence rate for heroin decreased. However, the question on heroin use was formulated differently in 2003 and therefore it is not possible to attribute the decrease to a real decrease in experimentation or to the change in formulation. Results of the ESPAD 2003 survey are available at the Portuguese focal point website (Country overview).
2.2.2 Problematic drug users/chronic and frequent drug users
In 2001 a series of national problem drug use estimation studies were conducted, providing estimates ranging from 2.3 to 8.6 problem drug users per 1 000 inhabitants aged 15–64 years old in Portugal. The disparities between results were mainly due to the fact that different case definitions and methodologies were used, as well as to limitations in the databases. Three estimations were based on the multiplier benchmark method, and one on the back calculation method. Estimates based on injecting drug users (IDUs) only, suggested a rate between 4.3 to 6.4 users per 1 000 inhabitants aged 15–64 years. Further estimates are necessary to improve methodologies and validate these results (Country overview).
2005 study appealed to different estimation calculation methods (multiplier methods) for three distinct definitions of case: 1) Users of opiates, cocaine and/or amphetamines; 2) Long term/Regular users of opiates, cocaine, and/or amphetamines; 3) Actual/Recent users of drugs by intravenous use.
Due to some discrepancies with definitions of case and methods used for calculation of the estimates donned in 2000, for comparative effects, some readjustments had to be proceed in 20001, estimates continuing however to be necessary to have some cautions reading comparative data2.
1 Namely re-calculation of 2000 estimation adapted to the first definition of case.
2 Namely at the second definition of case, since 2000 method – back-calculation - aimed to determine the estimation of IDUs. This definition of case is more restrict than the one applied in 2005.
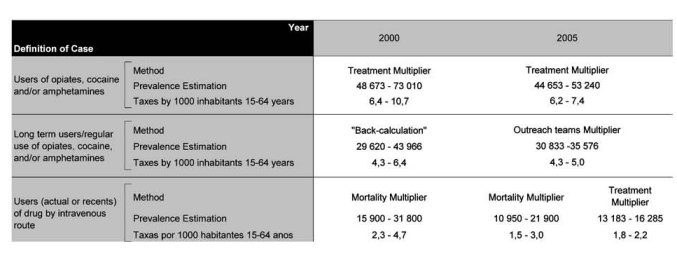
In relation to 2005 estimates, and as foreseen taxes decrease while the definition of case refers to a target-population more and more restricted of problematic drug users, varying the taxes for a thousand inhabitants of 15-64 years between the 6.2-7.4 for the overall definition and between 1.5-3.0 for the definition of problematic drug users more restricted.
Despite some methodological limitations in the comparative reading 2000-2005 data, it is unquestionable the evidence of a decrease on the estimated number of problematic drug users for any of the considered definitions, being the most significant the one that relates to injecting drug users (expert’s comments).
The number of problematic/chronic-frequent users (in the general population)

There is no information on injecting drug users.
2.3 Drug related Harm
2.3.1 HIV infections and mortality (drug related deaths)
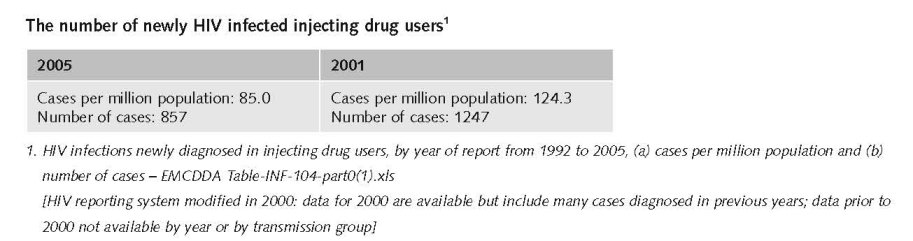
The number of HIV infected injecting drug users

According to 31/03/2007 notification data (from analytical tests) from the Surveillance Centre of Transmissible Diseases (CVEDT), the decreasing trend concerning the percentage of drug users in the total number of notified HIV positive cases since 1993 continues to be reported. From the 31 132 notifications ever received, 45% (46% in 2005 and 48% in 2004) were drug use related. Considering the different stages covered by these notifications, 48% of the AIDS cases, 40% of the AIDS related complex cases and 44% of the asymptomatic carriers cases were drug use associated (National Report, 2007).
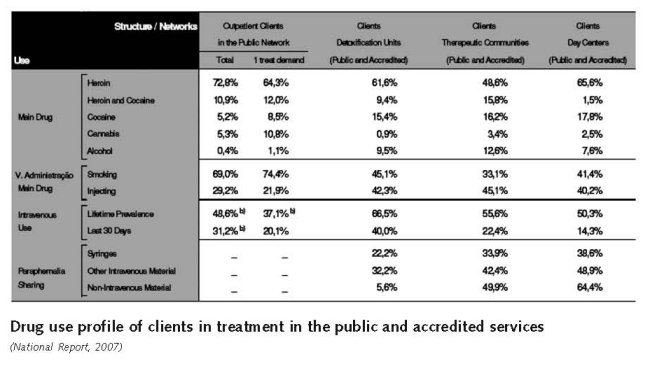
In Portugal, global estimations of the prevalence of infectious diseases among drug users are not available. However, some data concerning clients of some treatment facilities are available, and can provide information on rates among some sub-groups of drug users: (i) those demanding treatment for the first time at the out-patient treatment public network; (ii) those submitted to a detoxification treatment in public or certified private detoxification units; or (iii) those in treatment in public or certified private therapeutic communities (Country overview).
In 2006, rates of HIV infections ranged from 10.9% to 20.2% among voluntarily-tested drug users treated for the first time at public out-patient units (32% of them submitted tests), public or certified private detoxification units (97% submitted tests), and public or certified private therapeutic communities (97.6% submitted tests). For the same sub-groups, in 2006, rates for acute hepatitis B infections ranged between 2.9% and 5.6% (with 28.5%, 89% and 95.5% of the respective total clients being tested) and for hepatitis C between 41.7% and 84.8% (with 32%, 92% and 97% of the respective totals being tested) (Country overview).
In general a decreasing trend in the percentage of drug users in the total number of notifications of AIDS cases continues to be registered (since 1999). Concerning HIV, HCV and HBV in the treatment settings, positive cases remained stable in comparison to previous years (Country overview).
The decreasing trend in the percentage of drug users in the total number of notifications of AIDS cases continues to be registered. Concerning HIV and hepatitis infection in the treatment setting, data on HIV, hepatitis B and hepatitis C positive cases remained stable in comparison to previous years (National Report, 2007).
This stabilisation may be related, amongst other factors, to the implementation of harm reduction measures, which may be leading to a decrease in intravenous drug use (also visible in data concerning administration route in first treatment demands), or to intravenous drug use in better sanitary conditions, as indicated by the number of exchanged syringes in the National Programme “Say no to a second hand syringe” (National Report, 2007).

In 2006, 216 direct drug-related deaths were reported by the Special Register, defined as an individual whose post-mortem toxicological analyses is positive for any illicit drug of abuse. The national DRD definition relates to all positive toxicological results for drugs whatever the cause of death (overdose, traffic accident, etc), and is not in line with the EMCDDA DRD standard. The 2006 figure is close to that registered in 2005 (219 cases) but represents an increase in comparison with previous years (156 in 2004, 152 in 2003, 156 in 2002). In approximately 61.6% of cases, opiates or opiates in combination with other substances (mainly cocaine or alcohol) were the main substance involved in drug-related deaths. In 2005 and 2004, the proportion was 67% and 69% respectively. Data from the General Mortality registry are not comparable with the data from the Special Registry (Country overview).
Expert comments
When interpreting the results of assessments of HIV-infected drug users, it should be taken into consideration that the sample of tested drug users at various services is not always representative of the group. It must also be mentioned that some of the treatment samples included IDUs and non-IDUs, and consequently the rates among IDUs will probably be higher than those presented (Country overview).
3 Drug policy
3.1 General information
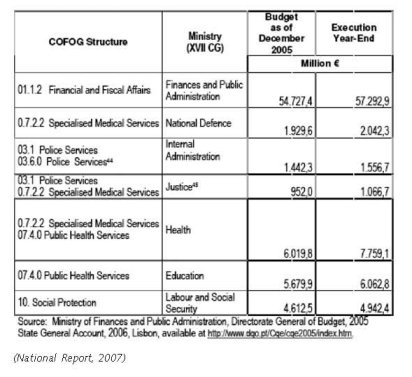
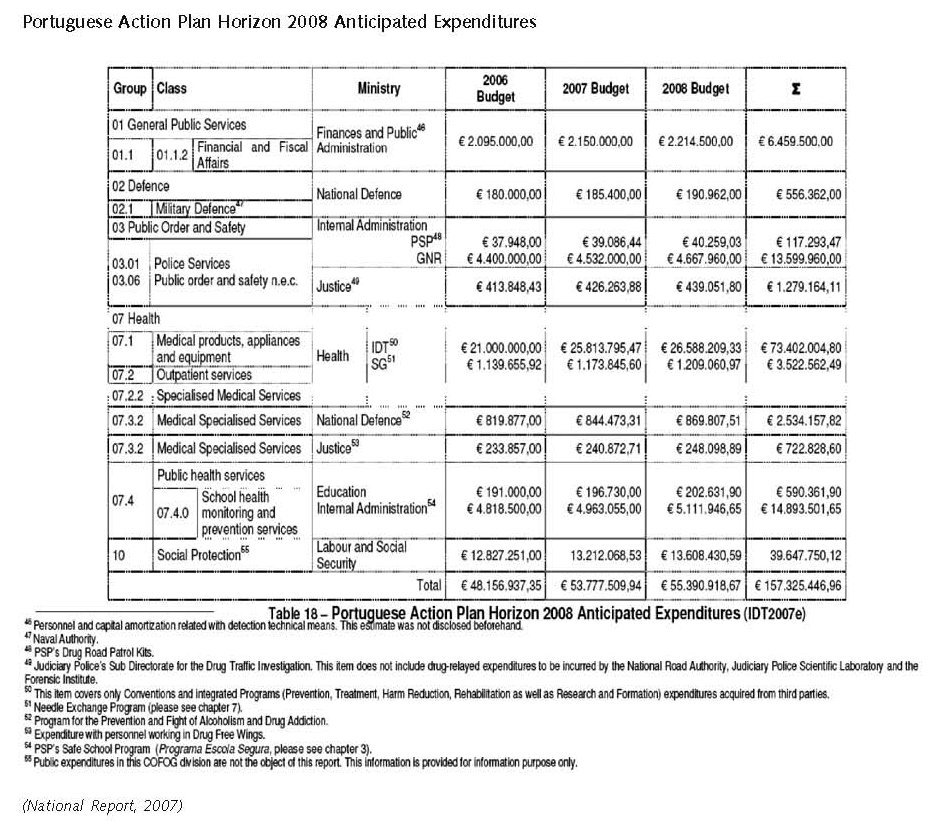
3.1.1 Policy expenditures
According to the Portuguese National Strategy for the Fight against Drugs (NSFAD) (PCM1999), published in 1999, public investment in drug policy measures should double in five years to PTE 32 billion (159.615.327,06 €), to finance the implementation of the national drug strategy, especially in various fields of drug demand reduction. In 1999 public investment in all the areas that encompassed the Portuguese policy against drugs amounted to PTE 16 billion (€79,807,663.53) (National Report, 2007).
However, due to the lack of information, the Instituto Nacional de Administração, which was commissioned with the external evaluation of the National Strategy (INA2004) carried in 2004, reported that it was not possible to compare public expenditures in 1999 and 2003 (National Report, 2007).
In subsequent years the national report presented every year to the National Parliament did not include an overall estimate of drug-related public expenditures, no doubt because of the difficulty of distinguishing direct and indirect drug-related expenditures in budgets and activity reports of institutions that implement the Portuguese National Strategy (INA2004) (National Report, 2007).
3.1.2 Other general indicators
The 1999 Portuguese ‘National strategy for the fight against drugs’ defined the general objectives in the drugs field and is currently being implemented through the ‘National plan against drugs and drug addiction plan 2005–12’, which focuses on four main ideas: geographical proximity, integrated approaches and responses, focus on the citizen, and improving quality and accreditation mechanisms. The objective set for the national plan is to significantly reduce the use of drugs amongst the population and its negative social and health consequences. The national plan is complemented by an ‘Action plan against drugs and drug addiction 2005–08’, which covers the areas of coordination, international cooperation, information/research/training/evaluation, the legal framework, demand reduction and supply reduction, and identifies for each action the party or parties responsible, a timetable and the indicators/assessment instruments to monitor the plan’s implementation (Country overview).
The National Drug Strategy of 1999 meant a major boost of the drug policy efforts in Portugal in all fields. Development, implementation and coordination of drug policy received much attention as can be seen from the investment mentioned above and from the development of the legal basis of drug policy from 2000 onwards (National Reports, 2000 – 2007).
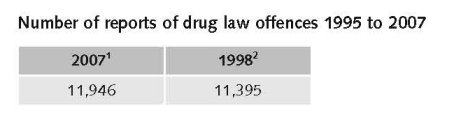
Numbers on arrests and imprisonment for drug-law related offences
1. Expert’s comments.
2. Number of reports of drug law offences 1995 to 2005 - EMCDDA Table DLO-1-OFFENCES-NUMBERS.htm
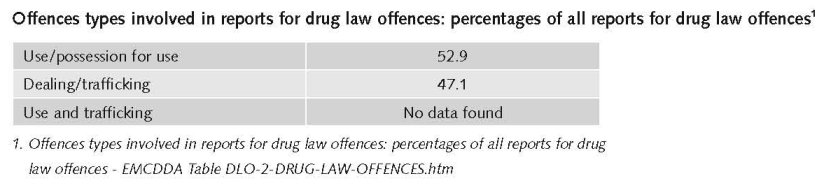
The percentage of individuals in prison for Drug Law offences, in 2006, continues to decrease to reach again the lowest value since 1997 (27% of all individuals in prison). Individuals were mainly imprisoned for traffic offences (90%).
An important reason was the implementation of Law n. º 30/2000, of the 29th of November; it defines the legal framework applicable to the consumption of narcotics and psychotropic substances, together with the medical and social welfare of the consumers of such substances without medical prescription (expert’s comments).
Numbers on arrests and imprisonment for use/possession for personal use
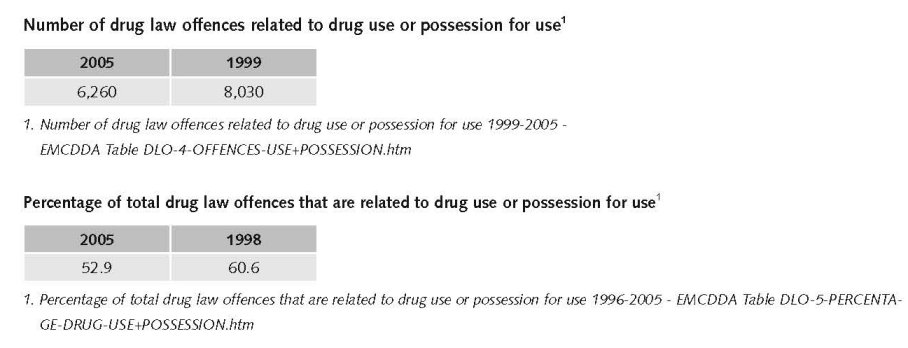
Finally the political guideline to decriminalise the personal use of drugs was implemented through Law 30/2000 of the 29th of November (National Report, 2000).
Court data indicates that, in the past years, decreases were reported in terms of the number of convictions for traffic and for traffic-use. The majority of these individuals possessed only one drug, mainly hashish, for the third time, and not heroin, as in previous years. In comparison to previous years the number of individuals who possessed only cocaine continues to increase. Of the convicted individuals, 96% were convicted for traffic, 1% for use (cultivation) and 3% for traffic-use (National Report, 2007).
3.2 Supply reduction: Production, trafficking and retail
The main focus of supply reduction is on retail and trafficking.
Priorities of supply reduction covered by policy papers and/or law
The legal framework in place since July 2001, although decriminalising illicit drug use, maintains drug use as an illicit behaviour and also maintains the illegal status for all drugs included in the relevant United Nations Conventions. However, a person caught in possession of a quantity of drugs for personal use (established by law), without any suspicion of being involved in drug trafficking, will be evaluated by a local Commission for Drug Addiction Dissuasion composed of a lawyer, a doctor and a social worker. Sanctions can be applied, but the main objective is to explore the need for treatment and to promote healthy recovery (Country overview).
Drug trafficking may be sentenced to one to 12 years imprisonment depending on different criteria, one of them being the nature of the substance supplied. For users who sell drugs to finance their own consumption, the penalty is reduced (Country overview).
The National Drug Strategies 1999-2004 and 2005-2012 both have/had a strong focus on supply reduction, in particular on drug trafficking. In 2006 a decision was reached that one main priority of the Portuguese Presidency of the European Council would be on drug trafficking in western African countries (National Report, 2007).
Laws are focussing especially on measures against trafficking.
In the period from 2000 till 2007 different laws and legal provisions were introduced to increase effectiveness of reduction of drugs trafficking. Law n. º 5/2002 of the 11th of January 2002 – establishes special measures to fight against economic and financial organised crime concerning evidence collection, information confidentiality and confiscation of assets in crimes of drug trafficking, terrorism and terrorist organisation, weapons traffic, passive corruption, money laundering and criminal association, amongst others (National Report, 2002).
Law n.º 30/2000 of the 29th of November 2000 - defines the new legal framework for personal use of illicit substances (cf. last year’s report). Concerning the setting up of the CDTs (Commissions for the Dissuasion of Drug Use), one CDT was implemented in each district to implement Law 30/2000 which decriminalises drug use and places the priority of law enforcement concerning drug use in treatment and social inclusion, rather than in criminal or penal aspects (National Report, 2001).
Resolution of the Council Ministers 39/2001 of 9th the April - approves the National Plan Against Drug and Drug Addiction - Horizonte 2004. The Plan has 30 concrete objectives and a financial support of 32 millions till 2004. The main objective concern the reduction to 1/3 the drug use of heroin, reduce drug related deaths by half and reinforcement of the financial support to primary prevention by 150% (National Report, 2001).
In the 1999-2004 period there was an intensive production of legal documents in this area. The contribution of this area was found to be globally positive but there are still areas were specific regulation is needed (e.g. in the harm reduction area) (National Report, 2005).
3.3 Demand reduction: Experimental/recreational drug use + problematic use/chronic-frequent use
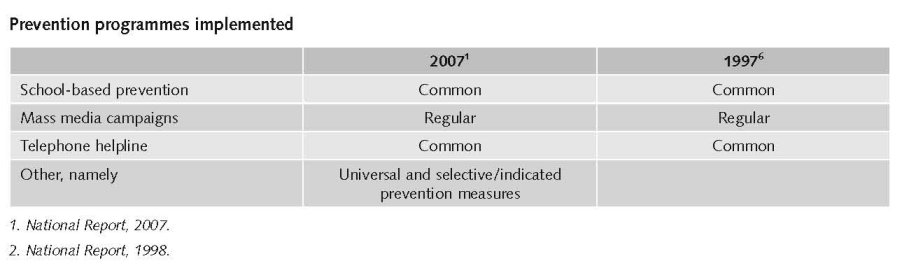
Universal drug prevention is part of the Portuguese school curriculum. Prevention programmes are delivered through training sessions, awareness-raising activities and dissemination of information through printed material. One initiative undertaken since 2006 is the ‘Safe schools’ programme, whereby law enforcement agents patrol the areas surrounding schools to prevent and protect from criminal activities such as drug trafficking in the surrounding area, are also involved in awareness and training activities in teaching establishments (targeting students, parents, school staff and law enforcement agents). This initiative focuses on drug abuse and alcoholism, road safety, self-protection, risk prevention and security in the school community (Country overview).
Selective prevention is mostly targeted at school drop-outs and deprived neighbourhoods, and is given high priority from both a political and practical perspective. Selective prevention in recreational settings is carried out by a few teams and focuses on direct counselling and information (Country overview).
Special characteristics of the prevention culture in Portugal within the European context are the decentralisation of implementation at local level via focused intervention programmes, strong momentum towards better quality control, tight monitoring and increasing interest in selective prevention (Country overview).
Treatments available
In 2006, 32,460 clients were in treatment, and of those 4,745 (20.2%) requested treatment for the first time. The total number of active clients has remained relatively stable in the past few years (maximum 32,064 in 2001, minimum 29,596 individuals in 2003). For the first time since 2001, the percentage of clients in treatment for the first time increased: the previous figures were 27.3% (2001), 19.6% (2002), 17.6% (2003) and 16.6% (2004). Among first-time treatment clients, 76.5% reported opioids as their main substance followed by 10.8% for cannabis and 8.5% for cocaine (Country overview).
Drug treatment in Portugal can be classified into four main categories: (i) out-patient drug treatment; (ii) day care centres; (iii) detoxification units; and (iv) therapeutic communities. All centres provide both psychosocial and substitution treatment. Day centres offering out-patient care are provided by public and non-governmental services. Withdrawal treatment is available in public and private detoxification units. In-patient psychosocial treatment mostly consists in therapeutic communities and is mainly available in private services. There is also short-term and long-term residential psychosocial drug treatment available (Country overview).
Contrary to the decreasing figure that has been registered since 2002, in 2006 the number of registered clients in both public (110 clients, 68 in 2005) and private units (4,118 clients, 4,093 in 2005) increased in comparison to previous years (National Report, 2007).
Data from the public therapeutic communities indicate that 62% of their clients (41% in 2005 and 53% in 2004) in 2006 were admitted for the first time into a TC. 98% of the admissions (93% in 2005 and 96% in 2004) resulted from a therapeutic project (National Report, 2007).
Substitution treatment is widely available in Portugal, through public services such as specialised treatment centres, health centres, hospitals and pharmacies as well as NGOs and non-profit organisations. Methadone has been made available since 1977 and buprenorphine since 1999. Furthermore, Decree Law 183/2001 Article 44.1 and Decree Law 15/93 Article 15.1-3 stipulate that methadone treatment can be initiated by treatment centres whereas buprenorphine treatment can be initiated by any medical doctor, specialised medical doctors and treatment centres. Moreover, the provision of buprenorphine in pharmacies started in 2004. In 2006, 22,922 clients were registered in opioid substitution programmes (21,054 in 2005, 16,877 in 2003). 4 833 cases were new admissions (4 206 in 2005) and 6 087 (5,222) left the programme during the year, 16% of whom with medical release (17% in 2005) (Country overview).
Indicators available continue to suggest effective responses at treatment level (increase in the number of clients involved in both drug free and substitution programmes) and at harm reduction level (levelling off of infectious diseases). The number of active clients in the out-patient public treatment network increased though first treatment demands continue to decrease. Heroin continues to be the main substance associated to health consequences and specifically in the sub-population of drug users that seek access to different treatment structures but references to cocaine and cannabis in this setting are increasing.
The availability of substitution programmes continues to increase and the number of clients continues to increase steadily, though in 2006 the percentage of those who were involved in buprenorphine programmes, slightly decreased in comparison to previous years (National Report, 2007).
Priorities of drug prevention and treatment covered by policy papers and/or law
Both Drug Strategies (National Strategy for the Fight Against Drugs 1999 – 2004 and National Plan Against Drugs and Drug Addiction 2005-2012) underline the importance of a well developed and comprehensive system of drug prevention and drug treatment services.
The National Strategy for the Fight Against Drugs (1999 – 2004) gives special relevance to drug use prevention: “The principle of prevention is implemented through the priority of prevention interventions which aim to reduce drug demand, through training and information programmes in communities or in specific target groups” (National Report, 1999).
The National Plan Against Drugs and Drug Addiction 2005-2012 puts emphasis on the implementation of a wide variety of prevention programmes (1, p 21). It aims to: (i) increase the number of drug prevention programmes based on scientific evidence; (ii) increase the number of selective prevention programmes directed to vulnerable groups; and (iii) improve the process of selection, monitoring and evaluation of prevention programmes (Country overview).
The National Action Plan – Horizon 2008 is prioritizing preventive interventions with local communities based on a national needs assessment, pilot projects in the field of selective prevention interventions (PIF), developing interventions for areas lacking in responses and the development of a website addressing young people (National Report, 2007).
The National Strategy refers that “treatment is a fundamental strategic option”. Treatment is a constitutional right of any citizen and it also may be thought of as a “preventive action, reducing drug use, protecting public health and, in certain cases, protecting the security of people and assets”.
The importance of expanding the drug abuse treatment network is also clearly referred in the Ministry of Health’s strategy for 2002 which determines as intervention guidelines:
• The setting up of new public specialised treatment centres (…);
• A wider availability of treatment in private units to the drug users, through protocols and conventions;
• The expansion of substitution treatment programmes (National Report, 1999).
The publication of the Ministry of Health’s strategy for the years 1998-2002, also stressed the importance of disseminating substitution programmes, with the main objective of “guaranteeing the access to substitution programmes to all heroin addicts who fulfil the admission criteria” (National Report, 1999).
Priorities of demand reduction covered by policy papers and/or law
Regulation nº 17/2004 of the 28th of April – sets up the General-Directorate of Innovation and Curricular Development in the Ministry of Education which, amongst its other responsibilities, will be responsible developing the area of substance abuse prevention in the school setting (National Report, 2005).
With the publication, in 1994 of the regulation for the administration of substitution drugs for heroin, the expansion of the network for the distribution of methadone and the diffusion of substitution programmes was systematically initiated (National Report, 1999).
Methadone maintenance treatment (MMT) was introduced in 1977, high-dosage buprenorphine treatment (HDBT) in 1999 (Year of introduction of methadone maintenance treatment (MMT), high-dosage buprenorphine treatment (HDBT) and heroin-assisted treatment, including trials - EMCDDA Table HSR-8-METHADONE-INTRODUCTION.htm)
3.4 Harm reduction
3.4.1 HIV and mortality
Additional information
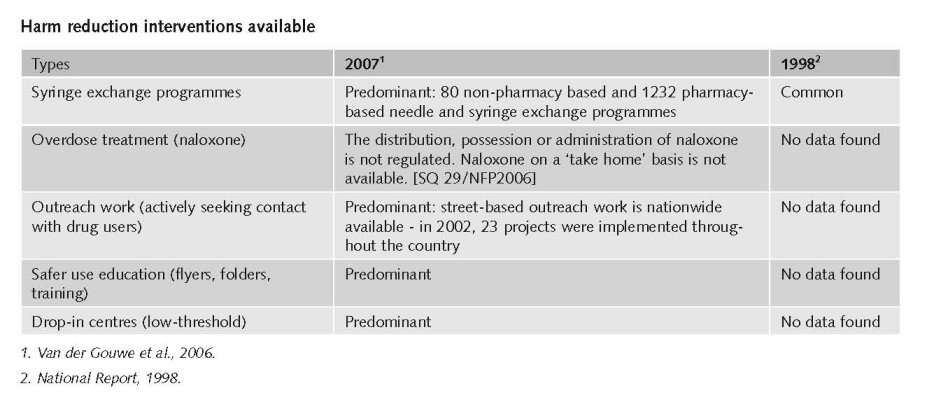
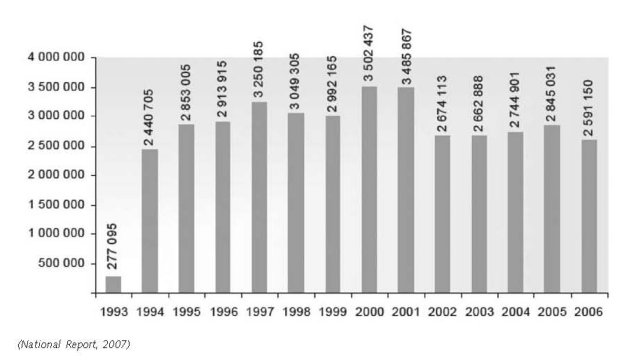
The National Commission for the Fight Against AIDS (Comissão Nacional de Luta Contra a SIDA), in cooperation with the National Association of Pharmacies (Associação Nacional de Farmácias) implements the national syringe exchange programme ‘Say no to a second-hand syringe’ which was set up in October 1993 to prevent HIV spreading amongst IDUs. The programme currently involves pharmacies (approximately 48% of all pharmacies on the Portuguese mainland), several mobile units, and other public and NGO facilities. In 2006, pharmacies were responsible for 52.8% of all syringes exchanged. About 38 million syringes have been exchanged through this programme from its launch in October 1993 until December 2006. In 2006,
2 591 150 syringes were exchanged, which represented an 8.9% decrease in comparison with 2005. This national NSP was externally evaluated in 2002 and it was concluded that it had avoided 7 000 new HIV infections per each 10 000 IDUs during the eight years of existence of the programme. Regions with the highest population density such as the Lisbon, Porto and Setúbal districts are still those with the higher quantity of exchanged syringes, and have been since the beginning of the programme (Country overview).
Syringes exchanged/ Totals of the Country from 1993 to 2006
(Programme “Say no to a second hand syringe” 1993 to 2006 ANF)
Priorities of harm reduction covered by policy papers and/or law
The main priorities established by the national plan for the 2005–12 period in the area of risk and harm reduction are: (i) to set up a global network of integrated and complementary responses in the harm reduction area with public and private partners; and (ii) to target specific groups for risk reduction and harm minimisation programmes. A network of harm reduction programmes (syringe exchange, low threshold substitution programmes, etc.) and structures, including drop-in centres, refuges, shelters, contact units and mobile centres, is being developed throughout the country in critical zones of intensive drug use with the aim to prevent drug-related risks such as infectious diseases and social exclusion and delinquency (Country overview).
The need for harm reduction services like syringe exchange, outreach work and substitution treatment was also emphasised in the National Strategy for the Fight Against Drugs (1999 – 2004) be it in more general terms than in the new Drug Strategy (National Report, 1998).
In 2000 and subsequent years many the legal fundament for harm reduction services developed strongly. In 2001 the general framework of harm reduction policies was established in Decree-Law n.º 183/2001, of the 21st of July 2001 (National Report, 2001). In 2002 different regulations were issued to establish conditions and criteria for different harm reduction services (National Report, 2002).
Law 3/2007 of the 16th of January 2007 - Adopted measures to prevent infectious diseases in the prison setting and sets the legal framework for a syringe exchange programme in that setting, to avoid the contamination and propagation of infectious diseases. Other responses concerning the prevention of infectious diseases and the availability of treatment for drug abuse were also reinforced (National Report, 2007).
Diploma Nº 22 144/2007 of the 21st of September 2007, approved the specific regulation for a syringe exchange pilot project in selected prisons (National Report, 2007).
Diploma n. º 748/2007, of the 25th of June 2007 – Established the criteria for the IDT to authorise the setting up of harm reduction programmes and facilities listed in Decree-Law 183/2001.
Diploma 749/2007, of the 25th of June 2007 – Established the criteria for the IDT to fund harm reduction programmes and facilities listed in Decree-Law 183/2001 (National Report, 2007).
3.4.2 Crime, societal harm, environmental damage
Most important statements of harm reduction covered by policy papers and/or law
• Promote interaction/intervention in Prison Establishments with relevant services of the Ministry of Justice;
• Promote the creation of experimental spaces for intervention in overdose situations;
• Mobilise all specialised units within the IDT in general, and the CATs in particular, as well as all Private Units providing treatment under a protocol with IDT, in order to expand their intervention in the field of risk and harm reduction, according to local needs and resources;
• Promote an effective interaction between all CATs and outreach structures, building integrated responses according to the needs identified (expert’s comments).
References
Consulted experts
A. S. Santos, Coordinator for International Relations Unit, Institute on Drugs and Drug Addiction, Lisbon.
Documents
CIA. The World Factbook: Portugal. Available: www.cia.gov/library/publications/the-world-factbook/geos/po.html, last accessed 10 December 2008.
Country overview: Portugal. Available: www.emcdda.europa.eu/publications/country-overview/pt, last accessed 10 December 2008.
National Report to the EMCDDA, Portugal, 1998.
National Report to the EMCDDA, Portugal, 1999.
National Report to the EMCDDA, Portugal, 2000.
National Report to the EMCDDA, Portugal, 2001.
National Report to the EMCDDA, Portugal, 2002.
National Report to the EMCDDA, Portugal, 2005.
National Report to the EMCDDA, Portugal, 2007.
Van der Gouwe D, Gallà M, Van Gageldonk A, Croes E, Engelhardt J, Van Laar M, Buster M. Prevention and reduction of health-related harm associated with drug dependence: an inventory of policies, evidence and practices in the EU relevant to the implementation of the Council Recommendation of 18 June 2003. Utrecht, Trimbos Institute, 2006.
UNODC (United Nations Office on Drugs and Crime). World Drug Report 2008. Vienna, 2008.
| < Prev | Next > |
|---|