| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Appendix to report 4: country reports MEXICO
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
MEXICO
1 General information
Location:
Middle America, bordering the Caribbean Sea and the Gulf of Mexico, between Belize and the US and bordering the North Pacific Ocean, between Guatemala and the US
Area:
1,972,550 sq km
Land boundaries/coastline:
4,353 km/ 9,330 km
Border countries:
Belize 250 km, Guatemala 962 km, US 3,141 km
Population:
109,955,400 (July 2008 est.)
Age structure:
0-14 years: 29.6% (male 16,619,995/female 15,936,154)
15-64 years: 64.3% (male 34,179,440/female 36,530,154)
65 years and over: 6.1% (male 3,023,185/female 3,666,472) (2008 est.)
Administrative divisions:
31 states and 1 federal district
GDP (purchasing power parity):
$1.353 trillion (2007 est.)
GDP (official exchange rate):
$893.4 billion (2007 est.)
GDP- per capita (PPP):
$12,400 (2007 est.)
Drug research
Several individual researchers are active in drug research. There is no developed drug research tradition, supported by governmental funding and an institute in Mexico.
Main drug-related problems
Drug trafficking is by far Mexico’s major problem.
2 Drug problems
2.1 Drug supply
2.1.1 Production
Mexico has no national studies on drug production and trafficking nor does it have a systematic national reservoir of data (expert’s comments).
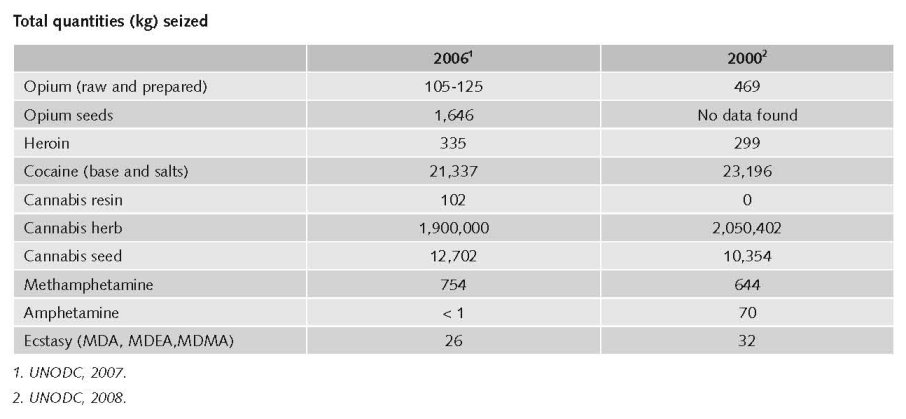
In 2002 Mexico produced an estimated 5,600 kg pure heroin. This is slightly less than its average yearly production of 7,200 over the preceding years. For 2005 the production was around 8,000 kg (Bucardo, 2005).
Marijuana cultivation and production decreased from 56,586,000 kg to 43,663,000 kg in 2004-2006. The production from the cultivated poppy area changed significantly in the same period, from 22,000 to 29,000 and 19,000 kg respectively (OAS/CICAD, 2006).
2.1.2 Trafficking
Mexico has no national studies on drug production and trafficking nor does it have a systematic national reservoir of data (expert’s comments).
2.1.3 Retail/Consumption
No published national data found in English on retail/consumption.
2.2 Drug Demand
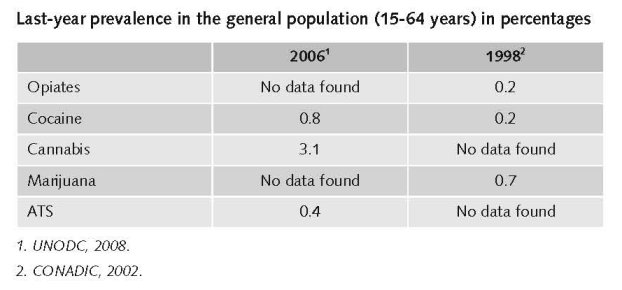
Until now, four household surveys on drug use were conducted in Mexico in 1988, 1993, 1998 and 2002. These were held among 12-65 year old people living in urban areas of more than 2,500 inhabitants (reported to be covering 75% of the country’s population) (Medina-Mora et al., 2003).
2.2.1 Experimental/recreational drug users in the general population
1 $1=€0.681543. Exchange rate 18 December 2008.
Until now, three national surveys on drug use among younger people were conducted in Mexico in 1976, 1986, 1991. These were held among students “at the intermediate and upper intermediate education levels”. The first two were held among students in urban areas, the third one also among students in rural areas, nationwide (Medina-Mora et al., 2003).
No data found on life-time prevalence among young people (15-24 years).
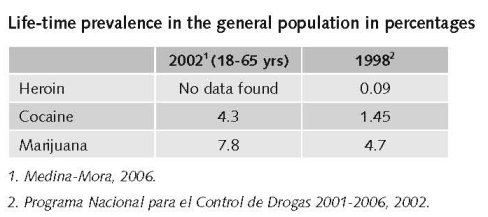
For the younger age group (18-29 years), illegal drug use (lifetime prevalence of marijuana and cocaine) has grown faster than ten years ago and earlier. Cocaine was used rarely and mostly in isolated groups in the 1970’s. Marijuana use may already start at a young age. Cocaine shows the greatest proportion of new onset at later ages (Fleiz et al., 2007).
No data found on last-year prevalence among young people (15-24 years).
2.2.2 Problematic drug users/chronic and frequent drug users
No published national data in English found on problematic drug users/chronic and frequent drug users.
Until now, several qualitative studies on drug use have been conducted among high-risk groups (youngsters working in the street, women) from 1978 to 2002 (Medina-Mora et al., 2003).
No published national data in English found on the number of problematic/chronic-frequent users and injecting drug users in the general population.
This number is estimated at 53,162, but for what year remains unclear (Aceijas et al., 2006; Cook & Kanaef, 2008).
2.3 Drug related Harm
2.3.1 HIV Infections and mortality (drug related deaths)
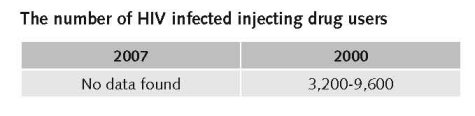
Of the estimated 160,000 people living with HIV, approximately 2-6% are believed to be IDUs, i.e. 3,200 – 9,600 (Bucardo et al., 2005).
Reported AIDS cases attributed to IDUs have been low. Local sentinel surveillance data suggest an increase of HIV prevalence associated with drug use may be manifest in border states with the USA (Magis-Rodriguez et al., 2002).
No published national data found on the number of newly HIV infected injecting drug users. There are a number of local studies in big cities.
The AIDS epidemic was largest in the second half of the eighties. In the early nineties this trend was buffered and curbed from 1994 on (Bucardo et al., 2005).
The number of HIV/AIDS infections due to drug use has probably decreased (INCB, 2007).
HIV infections remain largely concentrated in men who have sex with men, sex workers and injecting drug users. In various studies from 2005 HIV prevalence of 2-4% was found among injecting drug users in Tijuana and Ciudad Juarez (next to the border of the US). More than 85% of these users reported to use non-sterile equipment. Prevalence rates are higher among female sex workers in the same cities mainly due to unprotected sex. Drug using female sex workers showed higher prevalence rates (UNAIDS, 2008).
No published national data found on the number of drug related deaths by overdose.
Mexico has no reliable statistics that allow for estimating the number of drug-related deaths (OAS/CICAD, 2006).
In 2006 drug gangs were responsible for 2,100 drug-related deaths (El Universal).
2.3.2 Drug related crime or (societal) harm
Among 18 Latin American countries, Mexico has the highest subjective probability rate to bribe a police man, a judge or a civil servant. I.e. participants in a study were asked about the likelihood of being able to bribe those public servants (Goehsing, 2006).
The Northern states at the border of the US suffer most from drug related crime and violence caused by rivalry between drug syndicates. Drug-related violence is rising substantially during the past decade (expert’s comments).
The Ministry of Health acknowledged that drug related violence impeded the most recent drug study to fully deploy the polls in five states: Baja California, Sinaloa, QR, Campeche and Tabasco. One explanation is the loss of control over federal, state and local governments by the PRI. The PRI had control over these governments and was able to enforce unwritten arrangements with drug cartels. These informal arrangements do not work anymore. The mediator role of the PRI has weakened now other parties are also in control, which were not in power before (Meyer et al., 2007).
3 Drug policy
3.1 General Information
3.1.1 Policy expenditures
No published national data found in English.
$900,000 (€613.710,31) was allocated in 2006 to the states and municipalities to strengthen activities to control local retail trafficking (OAS/CICAD, 2006).
3.1.2 Other general indicators
No numbers are available on arrest and imprisonment for drug-law related offences. No data were found on use/possession for personal use or the production, trafficking and possession of bigger quantities.
Despite their importance, few studies have been conducted to date on court-initiated referrals. People under arrest or in social rehabilitation institutions should be included in information systems (Medina-Mora et al., 2003).
Mexico does not provide a figure for the number of persons arrested for illicit drug possession for personal use (OAS/CICAD, 2006).
3.2 Supply reduction: Production, trafficking and retail
Priorities of supply reduction covered by policy papers and/or law
No English publications were found.
Drug policy and drug laws are meant to reduce drug-related criminality. Changes in policies and laws point at a more stringent militarisation of the Mexican society in order to improve coping with criminality related to illegal drug trafficking.
The plans and programmes developed, did not lead to substantive reforms of the police force in order to be more effective in counter-drug operations. Calderon submitted a series of constitutional reforms to Mexico’s justice system to address insecurity in the country but this all has to be debated in Congress.
Examples of measures mentioned in the Integral Strategy to Prevent and Combat Crime are: the merging of four federal police forces, professionalization of the federal police force, mechanisms to combat police corruption, penitentiary reform, and active participation of civil society in crime prevention (Meyer et al., 2007).
3.3 Demand reduction: Experimental/recreational drug use + problematic use/chronic-frequent use
Prevention programmes implemented
No data found on the implementation of prevention programmes.
A number of prevention activities have been implemented during the past decade, but there was no continuity. School-based programmes for preventing drug-related crime and drug dependence have been operative from 2004-2006 directed at school children and university students. No specific descriptions are given. Guidelines for Preventing Drug Use in Mexican Schools were presented in 2006. Unclear remains what is done with these (OAS/CICAD, 2006).
An existing Telephone Guidance Centre (COT) is a help line providing information and guidance to people in crisis situations due to drug-related problems. Support is given in referring patients to care facilities. It handles an average of 25,000 – 30,000 calls per month. It is not a national telephone help line directed at the general public for information about drugs and drug use. One campaign in 2002 was more drug specific; it included written information (leaflets etc.). Nowadays these campaigns are more supporting treatment/help seeking. These present data on availability and possibilities for treatment. TV campaigns mainly covered preventive messages, e.g. risks of drug use, of overdose. These campaigns use fear-appeal strategies. There is no information about risks of the use of specific drugs anymore (OAS/CICAD, 2006).
The short life span of activities is for an important part due to government changes. Mexican government changes imply that the whole government is changed which is not supportive for continuity of actions implemented by former governments (expert’s comments).
Treatments available
“Little data exist which describes the extent of drug abuse treatment in Mexico overall.” (Bucardo et al., 2005). Most residential and governmental programs are abstinence-based (Bucardo et al., 2005) and few offer methadone maintenance (Magis-Rodríguez, 2000).
Addiction treatment is mainly abstinence-directed in Mexico and treatment facilities are insufficient. There are treatment farms that are non-professional, using ‘cold turkey’, mainly run by NGOs or community centres and based on experience, not on evidence. There are also private centres that are very expensive for the rich. One treatment commodity is funded by CONADIC and named “Vive sin Drogas” (expert’s comments).
Most residential and governmental treatment programs are abstinence based and one offers methadone maintenance in Ciudad Juarez on the border with the US (Bucardo et al., 2005).
There are substitution programmes available (Cook & Kanaef, 2008).
In 1988 only one treatment program existed in Tijuana, while now there are 20 residential drug treatment programs that for the Unity Network for Treatment of Addictions ‘RUTA’ with a capacity to treat 3,500 persons per year (Bucardo et al., 2005).
The OAS/CICAD publication offers additional information that is partly different from that collected by other sources.
Guidelines and standards of addiction care are available at state and local levels. Quality evaluations of treatment services are held every two years. Nowadays there are 400 recognised residential care facilities, 96 out-patients programmes (including clinics) and six in-patients programmes in Mexico. Both modalities are offered by public programmes, targeting both adults and adolescents. Some 29,306 patients received treatment in 2004, 33,652 in 2005 and 25,403 in 2006. There is no system of treatment system evaluation (OAS/CICAD, 2006).
Priorities of demand reduction covered by policy papers and/or law
Mexico has no laws or regulations at the federal or state level that permit the possession of illegal drugs for personal use. Drug possession is an offense (OAS/CICAD, 2006).
Treatment programs were until recently not sanctioned by the Ministry of Health (MoH), but laws are now enacted to sanction and control these programs. Therefore the MoH created the Municipal Office for Control and Treatment of Addictions (Bucardo et al., 2005).
3.4 Harm reduction
3.4.1 HIV and mortality
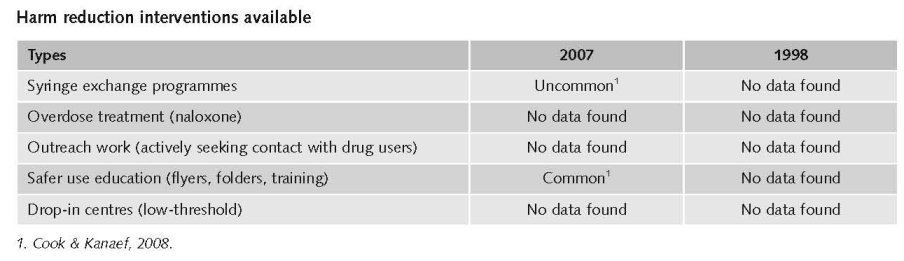
Harm reduction is a relative new concept in Mexico. NGOs are the initiators.
Harm Reduction activities are in general tolerated but rarely promoted (expert’s comments).
There are/were drug consumption rooms in Mexico but most of these have been demolished by police action as part of an anti drug crusade of President Fox from 2000 to 2004 (Bucardo et al., 2005).
In 2004 there was probably only one documented needle exchange program operational in Mexico realised by ‘Program Companeros’ in the state of Chihuahua. This program is community based, and has gained the trust of drug users, and provides users with information on health risks and the importance of cleaning needles and syringes (Bucardo et al., 2005).
Limited targeted programmes are present to increase access and uptake of voluntary HIV counselling and testing and to provide HIV/Sexually Transmitted Infection prevention (Cook & Kanaef, 2008).
“Overall, 48% of participants reported ever being arrested for carrying an unused/sterile syringe, even though syringe purchase and possession is legal in Mexico. (…) More than half of the participants (57%) had been arrested for possessing a used syringe” (Pollini et al., 2007).
Priorities of harm reduction covered by policy papers and/or law
Prevention and treatment of sexually transmittable diseases is explicitly mentioned in a Health Program policy paper. Interventions such as HIV/AIDS counselling programmes, providing chlorine, sterile syringes and condoms for injecting drug users are reported to have reduced HIV infections among this target group.
The Health Program policy paper is covered by nine laws and regulations. In 1996 health services were decentralised to 31 states and the Federal District (principle of cooperative federalism). Separate responsibilities of different institutions are described (National Health Program 2001-2006, no publication year).
Mexico explicitly supports harm reduction in national policy documents (Cook & Kanaef, 2008).
Possession of drugs is illegal in Mexico and this legal provision is actively enforced by the police. Sale of needles and syringes is legal and does not require prescription (Bucardo et al., 2005; Pollini et al., 2007).
From 2000 to 2004 a national crusade against drug trafficking was launched. This for instance led to the closure of 1400 (!) shooting galleries or picaderos in Tijuana (Bucardo et al., 2005).
While not officially sanctioned, the state government of Chihuahua tolerates NEP (Bucardo et al., 2005).
3.4.2 Crime, societal harm, environmental damage
No information found on interventions/measures to reduce harm for society.
References
Consulted experts
R. Blancas, Coordinator, CAM project, Mexico City.
M. del Carmen Serrano Carreto, Research Associate, University Colégio de México, Mexico City.
S. Eichhorn, Project leader, UNODC, Mexico City.
M.E. Medina-Mora, Head of the Psychiatric Institute ‘Ramón de la Fuente’, Mexico City.
M. Tiburcio Sainz, Research assistant, National Institute of Psychiatry ‘Ramón de la Fuente’, Mexico City.
Documents
Bucardo J, Brouwer KC, Magis-Rodriguez C, Ramos R, Fraga M, Perez SG, Patterson TL, Strathdee SA. Historical trends in the production and consumption of illicit drugs in Mexico: Implications for the prevention of blood borne infections. Drug and Alcohol Dependence, 2005, 79: 281-293.
CIA. The World Factbook: Mexico. Available: www.cia.gov/library/publications/the-world-factbook/geos/mx.html, last accessed 12 December 2008.
CONADIC. Encuesta Nacional de Adicciones 2002. Mexico City, Secretaria de Salud/INEGI/Instituto Nacional de Psiquiatría, Epidemiología, CONADIC, 2002. Available: www.conadic.gob.mx, last accessed 12 December 2008.
Consejo Nacional contra las Adicciones etc. Drogas, Encuesta Nacional de Adicciones 1998. Mexico City, Consejo Nacional contra las Adicciones/Juntos pro la Salud/Secretaria de Salud, 1998.
Cook C, Kanaef N. Global state of harm reduction 2008. Mapping the response to drug-related HIV and hepatitis C epidemics. London, International Harm Reduction Association (IHRA), 2008.
Degenhardt L, Chiu WT, Sampson N, Kessler RC, Anthony JC, et al. Toward a global view of alcohol, tobacco, cannabis, and cocaine use : Findings from the WHO World Mental Health Surveys. Plos Medicine, 2008, July, 5(7), e141.
El Universal. El universal January 2nd 2007. Available: (http://www.el-universal.com.mx/notas/397603.html, last accessed on 12 December 2008.
Fleiz C, Borges G, Rojas E, Benjet C, Medina-Mora ME. Uso de alcohol, tabaco y drogas en población Mexicana, un estudio de cohortes. Salud Mental, 2007, 30(5): 63-73.
Goehsing J. A multi-pronged approach to transnational criminal networks: The case of Latin America and the Caribbean. Centro de Estudias y Programas Interamericanos, Instituto Technológico Autonómo de Mexico, 2006. (CEPI Working Paper Series. Paper nr.5).
Magis Rodriguez C, Marques LF, Touzé G. HIV and injecting drug use in Latin America. AIDS, 2002, 16(Suppl. 3): S34-S41.
Medina-Mora ME, Borges G, Fleiz C, Benjet C, Rojas E, Zambrano J, Villatoro J, Aguilar-Gaxiola S. Prevalence and correlates of drug use disorders in Mexico. Rev Panam Salud Publica/Pan Am Journal of Public Health, 2006, 19(4): 265-275.
Medina-Mora ME, Cravioto P, Ortíz A, Kuri P, Villatoro J. Mexico: systems for the epidemiological diagnosis of drug abuse. Bulletin on Narcotics, 2003, 55, ½,: 105-119.
Meyer M, Youngers C, Bewley-Taylor D. At a crossroads : Drug trafficking, violence and the Mexican state. Washington, Washington Office for Latin America (WOLA), 2007.
National Health Program 2001-2006. Program for action on HIV/AIDS and STI Prevention and Control. Mexico City, 2002.
National Health Program 2001-2006. The democratization of health in Mexico : Towards a universal health system. Executive summary.
OAS/CICAD. Mexico. Evaluation of progress in drug control 2005-2006. OAS/CICAD, Multilateral Evaluation Mechanism (MEM). Mexico, Mexico City, 2006 (OEA/Ser. L/XIV.6.2 – MEM/INF. 2006 Add. 22 p15).
Pollini RA, Brouwer KC, Lozada RM, Ramos R, Cruz MF, Magis-Rodriguez C, Case P, Burris S, Pu M, Frost SDW, Palinkas LA, Miller C, Strathdee SA. Syringe possession arrests are associated with receptive syringe sharing in two Mexican-US border cities. Addiction, 2007, 103: 101-108.
Programa Nacional para el Control de Drogas 2001-2006. D.R. Procuraduria General de la República. Primera edición, 2002.
Secretaria de Salud. Drogas. Mexico City, Secretaria de Salud/Sistema Nacional de Encuestas de Salud/Encuesta Nacional de Adiccciones, 1990.
UNDCP (United Nations International Drug Control Programme. World Drug Report 1999. Vienna, 2000.
UNODC (United Nations Office on Drugs and Crime). World Drug Report 2007. Vienna, UNODC, 2007.
UNODC. World Drug Report 2008. Vienna, UNODC, 2008.
| < Prev | Next > |
|---|