| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
3. Methods
 |
|  |
| 
| Reports - Rapid Situation and Response Assessment South Asia |
Drug Abuse
3. Methods
3.1 Location of the study
The study was conducted in various locations of the following countries by RSRA teams formed in each of the assessment sites.
Bangladesh
Mentor Agency: International Centre for Diarrhoeal Disease Research
Partner Agency
Light House, Bogra Dhaka Ahsania Mission, Dhaka
Community Health Rehabilitation Education Awareness (CREA), Dhaka
Ashokti Punorbashon Nibash (APON), Dhaka
Addiction Life Overcome (AL0)1, Chittagong
Bhutan
Mentor Agency: Youth Development Fund Partner Agency2:
Youth Development Fund (YDF), Thimpu REWA, Thimpu
India
Mentor Agency: RRTC NORTH-Society for Promotion of Youth and Masses (SPYM)
Partner Agency:
J & K SPYM, Jammu SAHARA, Delhi
NIRVAAN, Barabanki
Mentor Agency: RRTC EAST I-Vivekananda Education Society
Partner Agency:
Vivekananda Education Society, Kolkata Vishwa leevan Seva Sangha, Bhubaneshwar
Human Development and Research Institute (HDRI), Kolkata
Mentor Agency: RRTC EAST II-Calcutta Samaritans
Partner Agency:
Alpasankhyak Avam Harijan Samaj Kalyan Kendra, Muzaffarpur
Kripa Foundation, Darjeeling
Young Mens Christian Association, Jamshedpur Mentor Agency: RRTC WEST-Muktangan Mitra Partner Agency:
Kripa Foundation, Mumbai Muktangan De-Addiction Centre, Pune
Gandhi Bhavan Trust (Navjeevan De-Addiction Centre), Bhopal
Mentor Agency: RRTC SOUTH-TT Ranganathan Clinical Research Foundation
Partner Agency:
TT Ranganathan Clinical Research Foundation, Chennai
Trivandrum Social Service Society, Trivandrum
Women's Organization in Rural Development, Namakkal
Mentor Agency: RRTC NORTHEAST-I Galaxy Club
Partner Agency:
Integrated Children and Women Development Centre, Imphal
Kripa Foundation, Imphal
SHALOM, Churachandpur
Mentor Agency: RRTC NORTHEAST II Kripa Foundation, Nagaland
Partner Agency:
Kripa Foundation, Kohima
Bethesda Youth Welfare Centre, Dimapur New Hope Centre, Shillong
Mentor Agency: RRTC NORTHEAST-III Mizoram Social Defence & Rehabilitation Board
Partner Agency:
Care Project, World Vision, Kolasib
Agape Moral Reformation Organization, Aizawl New Life Home Society, Aizawl
Nepal
Mentor Agency: Drug Control Programme, Ministry of Home Affairs
Partner Agency:
NAMUNA Integrated Development Council, Rupendahi
Nagarjun Development Community, Rupendahi
Drug Abuse Prevention Association Nepal, Kathmandu
Nepal Youth Rehabilitation, Kathmandu
Community Awareness Against HIV/AIDS & Drug Addiction (CAADA), Kathmandu
Prerana, Kathmandu
Sri Lanka
Mentor Agency: Sri Lanka Federation of Non Government Organizations Against Drug Abuse
Partner Agency:
Alcohol and Drug Information Centre, Colombo Mithuru Mithuro Movement, Colombo
Sri Lanka Anti Narcotics Association, Colombo Apekedella, Polonnaruwa
3.2 Organising the rapid situation and response assessment
Planning is critical for effective implementation of rapid situation and response assessments. The following steps were taken for implementing RSRA:
1. Identifying priorities for action.
2. Establishing a core rapid assessment team, which included a team leader, peer outreach coordinators and peer outreach workers, both male and female.
3. Conducting an initial community consultation.
4. Identifying the parameters of rapid assessment.
5. Building and training the RSRA team.
6. Establishing a community consultation process.
7. Undertaking field work.
8. Carrying out data analysis.
9. Translating the findings into action plans.
3.3 Recruitment strategy
3.3.1 Mentor agencies and NGO partners
The first step was identifying and reaching out to drug users and their female sex partners. Mentor agencies were identified in the five countries and they were given the responsibility of identifying and coordinating with the partner NG0s. Overall, there were eight mentor agencies for India (one each for the South, West, North region; two for the eastern region; three agencies for the north-eastern region) and one mentor agency each for the countries of Bangladesh, Bhutan, Nepal and Sri Lanka. The partner agencies have been working with the drug users in their respective localities and they were given the task of carrying out the RSRAs in their areas. Forty NGO partners were involved in the RSRA in these five countries (India: 24; Nepal: 6; Bangladesh: 5; Sri Lanka: 4; and Bhutan: 1).
3.3.2 RSFtA team
In each assessment site, the RSRA team consisted of a team leader who was responsible for overall coordination; three peer outreach coordinators who had the responsibility of monitoring, supporting and supervising the team of outreach workers; five outreach workers to carry out the field level activities; and site-specific peer volunteers who assisted in identifying and engaging the drug users and their sex partners. To ensure that female regular sex partners could be reached for assessment, the project ensured that at least one of the peer outreach coordinators was a woman with experience of having worked in the drug use/HIV field. Similarly, it was emphasized that at least two of the five outreach workers should be females with either a drug use background or should be a spouse of a drug user. The peer volunteers and the outreach team were engaged in the field work and they were responsible for recruiting the required number of drug users and their regular sex partners for the assessment.
3.3.3 Training for the rapid assessment team
A tool-kit on rapid situation and response assessment' as well as a facilitators training manual on RSRA were developed by UNODC ROSA. With the help of these, international/ national experts in the field provided rigorous training to all the assessment team members on research methodology, assessment procedures, report writing, and use of research findings for intervention development. Mentor agencies were asked to identify master trainers who would be responsible for ongoing support to the team members and they were guided and assisted by the experts during the training sessions. The master trainers remained in touch the implementing partner NGOs throughout the period of assessment and provided ongoing supervision during the data collection.
3.4 Data collection strategies
3.4.1 Sampling plan for the quantitative survey
The strategy consisted of the following steps:
1. Initial mapping of indicators of drug use/injection drug use.
2. Ethnographic mapping of certain neighbourhoods and geographical locations identified to have high prevalence of drug use and drug injecting.
3. Development of a recruitment plan for each site.
After recruitment, the respondents were interviewed using a structured interview schedule. The NGO partners were responsible for the recruitment of drug users and their sex partners for assessment and data collection. The recruitment was always confined to specified geographical locations identified by the NGO partners in consultation with the mentor agencies. The geographical areas included for assessment are areas with high prevalence of drug use and in each country there was a good geographical spread covering the areas with high prevalence of drug use. The project emphasized the recruitment of opioid users (both injecting and non-injecting) for the assessment.
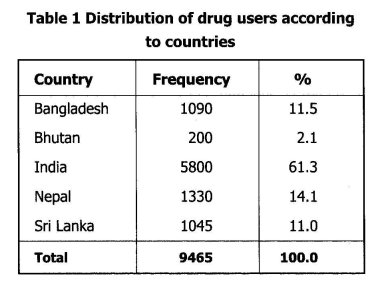
The aim was to recruit around 250 male drug users / IDUs and about 150 female regular sex partners in each of the assessment sites. Using the snow-ball technique, drug using clusters were identified and drug users recruited for assessment by the peer volunteers and assisted by peer outreach workers who were familiar with the drug use scenario in their locality. The drug users recruited were requested to bring their female regular sex partner for the assessment. The identified female sex partners were interviewed by the women outreach workers. The outreach team and the peer volunteers continued to remain in touch with the drug users and their partners following assessment for the purpose of providing peer-led HIV interventions and other services. The total number of drug users recruited from each of the countries is shown in Table 1.
3.4.2 Measures
The data for the study was collected by the peer outreach coordinators (the male coordinator collecting the data from drug users and the woman coordinator collecting data from regular sex partners) over a three-month period (June—August 2005) in four countries, namely, Bangladesh, India, Nepal and Sri Lanka. The RSRA in Bhutan was carried out in May 2006. Information from the drug users and their regular sex partners was collected through separate structured interview schedules that were specially developed for this project. Data from the drug users and female regular sex partners was collected on demographic characteristics; drug use; sexual practices and behaviours; self reported symptoms during the past year; risk perception and HIV/AIDS knowledge. Overall, the RSRA reached 9,465 current drug users and 4,612 of their female regular sex partners (4,612/9,465; 48.7°/0) for the assessment.
3.5 Data Analysis
The findings of the rapid assessment survey were summarized using descriptive statistics to illustrate the demographic characteristics, drug use status, sexual behaviours, health status, risk perception and HIV/AIDS knowledge of the female regular sexual partners of drug users by country. The data was analysed using software package Epi Info (version 6.4b, Centres for Disease Control, Atlanta, GA, in collaboration with World Health Organization, Geneva, Switzerland) for frequency distribution and univariate analyses.
3.6 Ethics
The data was collected after obtaining informed consent. All participants were assured that a refusal to be part of assessment will not lead to denial of any of the services offered by the implementing NGO partner. The interviews were held in the drop-in-centres (DICs) of the NGO partners or at times in the field at a convenient and secure place.
3.7 Problems and barriers during assessment
• Drug users from all socio-economic groups were not represented in the study; the sample may not be representative of the drug users as the recruitment was done through snow-balling technique.
• The field researchers in some sites were exposed to unsafe conditions.
• The existing facilities for drug users are inadequate in most places and it was difficult to refer the clients requesting help to appropriate services.
Despite these difficulties, the researchers managed to gather necessary and relevant information crucial for intervention development.
1. RSRA was carried out by ALO, but due to technical reasons is not included in this analysis
2 YDF and REWA together carried out the RSRA in Thimpu
3
| < Prev | Next > |
|---|