| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 201 |
| Yesterday: | 251 |
| This Week: | 201 |
| Last Week: | 2221 |
| This Month: | 4789 |
| Last Month: | 6796 |
| Total: | 129388 |
EXTENT AND PATTERNS OF USE AND ABUSE
 |
|  |
| 
| Reports - Marihuana and Health |
Drug Abuse
EXTENT AND PATTERNS OF USE AND ABUSE
BACKGROUND CONSIDERATION'S
In order to discuss the scope of marihuana use the terms use and abuse should be defined. Use can be fairly easily defined as any consumption of parts or products of the cannabis plant that are believed to contain the active ingredient (s), or consumption of the active ingredients themselves. Use includes the act of smoking marihuana or hashish, the ingesting of marihuana or hashish incorporated into foods, the consumption in any manner of the active tetrahydrocannabinols or the drinking or infusion of marihuana or hashish, which is believed rare in the U.S. at this time.
There is, however, no wide agreement on the meaning of the term abuse. Marihuana abuse has been defined at the most restrictive end of a continuum, as any use of the substance; at the most permissive end, as use that has resulted in serious adverse reactions of the individual. A middle position is that abuse is frequent, regular or chronic use, implying that habituation has occurred. It will be seen elsewhere that reliable figures on adverse reactions are not to be found; thus, it is not possible to give estimates of abuse in that sense. In many studies only the fact that someone has "ever used" marihuana was sought, making it unfortunately impossible even to distinguish frequent, regular or current use from past or present experimentation.
Most estimates of the scope of marihuana use rely on figures representing any use by the individuals in their lifetime; a few have looked at incidence, the use of the substance during a specified time period, usually a year, or the time elapsing from the beginning of the academic year to the survey. Their finer gradations have not been measured or reported in enough studies to enable one to make good estimates of use vs. abuse, regardless of the definition employed. Also, use of hashish has seldom been asked for or categorized separately from marihuana, so it is not known whether it should be included with marihuana or not.
SCOPE OF THE PROBLEM: U.S.A.
The task of simply describing the scope of marihuana use in the U.S. has been and still is difficult. Some of the data needed for estimates simply do not exist. Those that do exist cannot be used with full confidence because they lack validity or reliability (or both).
The only sources of information on use by the Nation as a whole are results of commercial polls (such as Gallup's) that included questions on drug use. Sources like these often are inadequate for reliable estimates of the scope of the problem. Gross measures of use are often the only basis for the figures. Information about methodology often is lacking, so that size of the sample, standards of interviewing, and the like, cannot be judged. Moreover, most surveys and polls of illicit drug use cannot guarantee that all responses to questions are valid. Studies to assess the probability of valid responses on this subject do not exist.
Other than nationwide polls, the sources for estimates consist mainly of one-time studies of high school and college students conducted in scattered locations, with varying quality of sampling techniques' in- struments, and survey methods (3). Recently, however, a handful of studies have been repeated for the second and third years, so that changes in drug use in those locations can now be gauged more reliably (26, 22, 20, 12).
The first nationwide survey of college students by any Federal agency (NIMH grant 16536-01) has just completed the tabulation of preliminary data. This study of 10,000 students at a sample of fifty colleges across the country was conducted by Dr. Peter H. Rossi in the Department of Social Relations at Johns Hopkins University (27).
PROBLEMS IN OBTAINING ACCURATE ESTIMATES
Assessing marihuana abuse has special difficulties beyond the ordinary precautions for assuring, statistical reliability and validity. The reluctance of drug users to admit to illegal behavior in interviews or questionnaires can reduce the estimates below the true figure. On the other hand, in certain situations, young students may use the oppor- tunity to pretend higher use, inflating the estimates. In order to im- prove the probability of valid responses, it is advantageous to offer respondents confidentiality or immunity from prosecution. (In extreme cases, researchers too have been subject to subpoena of their records or of their knowledge of illegal drug use by respondents). Until November 1970 there were few States that protected confidentiality (New York was one) or provided researchers immunity (Massachusetts and New Hampshire were two).
Another difficulty arises in attempting to collect data in classrooms. Many principals and boards of education are opposed to use of the school day for this purpose or do not wish to risk parental disapproval. In many schools parental approval must be obtained for any testing of pupils. Finally, permission to survey .a school population s often dented from fear of the adverse publicity that might result.
ESTIMATES or MARIHUANA USE
In October 1969, Gallup reported results of a poll of a sample of adults 21 years and older in the United States that indicated that 1% of these adults had used marihuana at some time (11). It was estimated that the total number was about 10 million. At about the same time, the Director of the National Institute of Mental Health testified .before a Senate Subcommittee that eight to twelve million persons in the United States had some experience with marihuana (31). The _Gallup Poll indicated that use was more common among younger than older persons: 21-29 years (12%) ; 30-49 years (3%) ; 50 and over (1%). Also, the poll showed that men tended to use it more than women (6% vs. 2%). Those with college background had a higher use rate than those with a high school or grade school background (9% vs. 3% vs. 1%), and the West and East'', regions had higher rates than the South and Midwest (9% West and 5% East vs. 2% South and Midwest).
Preliminary data from a 1970 nationwide survey of college students indicates that 31% of the students have used marihuana at some time; 14% of the students had used it every week or two during the semester in which the sell-administered survey schedules were completed (27 ) . Compared with the Gallup figures for 1969, it indicates a substantial increase among college students; this comparison, however, can only be rough because of possible differences in methods and sample sizes used in the two surveys.
Nationwide surveys of college and high school students now in progress (27, 9) cannot yet show whether student rates of marihuana use differ by region as adult, rates apparently did in 1969 (11). Since the separate studies of schools and colleges vary so much in geographical coverage, sampling, method of administration, and other conditions of data collection, comparison of their rates by region is not warranted. Until 1969, few if any studies were made in the Midwest or South, so knowledge of the problem was heavily influenced by studies made on the West and East coasts.
Nevertheless, the studies that have been done in the Midwest since 1969 hardly indicate that rates are any lower there. A Michigan study of eleven high schools in 1969 showed that rates varied from none to 34% of students in selected schools who had "ever used" marihuana (6). In the same year, the rates were 12% in one Utah study and 23% in a Wisconsin study (13, 30). One college study only, at the University of Michigan in 1969, revealed a rate of 44% who had "ever used" marihuana (10). These rates are at least as large as, and some are larger than, rates found in some studies in other parts of the country.
The fact that marihuana use had been increasing up to 1969 has been indicated by several surveys that were repeated the second and third year in the same location. In all of these surveys, the use of marihuana increased five to twelve percentage points between 1968 and 1969. This increase occurred in the secondary schools in San Mateo County, California (26); at the University of Maryland (20) ; at Carnegie-Mellon University, Pittsburgh (12) ; and among college students nationwide (22). Undoubtedly increases would have been found in almost every school or college during that period.
There is just one study capable of indicating high school trends for 1970, but it shows an interesting change. For three years, San Mateo County in California has conducted a survey of drug use in the junior and senior high school grades (26). In 1970, a total of 35,145 students were surveyed. In both survey years 1968 and 1969 there were steady, large increases in marihuana use. The increase in 1970, however, was decidedly smaller. For boys, instead of the average 7.9 percentage point increase in "any use" between 1968 and 1969, there was an average 1.6 percentage point increase between 1969 and 1970. For girls, the increase was greater, but there was a definite lessening of the former rapid increase. An average increase of 7.2 percentage paints from 1968 to 1969 declined to a 3.4 percentage point increase in 1970.1 The average proportion reporting use within the past year was 42%, a high rate among the schools surveyed.
Even more important than the apparent lessening of the rapid increases in marihuana use in the high schools, the seventh and eighth grade classes in San Mateo actually showed a decrease in marihuana use between 1969 and 1970. In every category of student by age, grade, and sex, the reported use of marihuana had declined slightly from the previous year's figures.
Changes in use of marihuana in one country's schools cannot represent the situation generally in schools across the country, of course. Undoubtedly, in many schools and colleges there will continue to be increases in use, and rapid increases. However, schools on the West Coast were the first to experience the onslaught of drugs, and there is some reason to expect that their experience may presage a stabilization of rates or possible decline in interest among students.
USE BY INDIVIDUALS OTIIER THAN STUDENTS
If there is now the beginning of a lessening in student drug use, it may be outweighed by increased interest in marihuana on the part of. out-of-school young adults. A study of marihuana use (one or more times) by adults 18 years and above in San Francisco in 1969 indicated that almost the same proportions (about 40%) of non-college young adults as college students of the same age groups had used the drug (16). The rate of use by all adults 18 years or older in San Francisco in that study was 13% ( 17).
By way of comparison to student studies and to studies of adults of all ages, the figures below are given for certain other groups which were studied separately (3).
High school dropouts who had ever used marihuana in a study in Utah in 1969 made up 50% of the group. In another study, marihuana users made up 26% of a group of employed youths 16 to 23 years old. Three studies have been made of marihuana use by servicemen, two conducted with soldiers in Vietnam. In the most detailed report, 32% of the servicemen in Vietnam had used marihuana at some time, three fifths of the users had done so twice since coming to Vietnam. In another study, 23% of enlisted men on active duty in 1969 had used marihuana (4). Forty-seven percent of Negro men who had grown up in St. Louis had tried marihuana at least once by the time they were in their early thirties (24). Studies of hippie communities consistently show 95% to 100% who have used marihuana (3).
GRADATIONS OF USE
It is recognized that gross estimates of marihuana use cover a number of gradations on several dimensions. Where frequency has been determined, it has been found that many users have used once, and only a portion have used more than 10 or 20 times. Where current usage (i.e. prevalence) has been determined, it has been found that only a portion who ever used were doing so at the time of the study. Another dimension that has not been measured but undoubtedly varies for many users is the regularity with which the drug is used. In 1969 the Director of the National Institute of Mental Health testified that about 10% of all users of marihuana were chronic 2 users and about 25% occasional users (31). The remainder were "tasters" or one-time users. On the basis of those percentages, it was estimated that there were 800,000 to 1,200,000 chronic users of marihuana in the Nation at the time, and 2 to 3 million occasional users.
Other studies have results that resemble the 10% chronic, 25% occasional, and 65% experimental distribution, but the categories differ. In one high school study and one study of nine campuses, both in 1969 about 40% of those w.ho had ever tried marihuana had ceased using it (21, 1). In a study of over 5000 enlisted men on active duty, about 60% of users had used it ten times or more (4). Among servicemen in Vietnam, 76% of users had experimented or used it twenty times or less (25). In the nine-campus study, there were relatively more experimenters in the older group of students, and more moderate or heavy users in younger groups.
The question of how long a person might use marihuana at the various gradations of use cannot be answered yet. One comment from an observational study of drug using groups of young peers was that most youth even when using marihuana daily tend to pass through the drug scene in about a year (29). After this stint in the subculture; they may still use marihuana occasionally, however.
SOCIO-DEMOGRAPHIC CHARACTERISTICS OF USERS
Some indication of the identity of marihuana users nationwide was found in the Gallup poll results of 1969, mentioned above. In addition, marihuana studies on campuses and in high schools provide a fairly consistent picture of the characteristics of users (5, 6, 28). It should be kept clearly in mind that these characteristics are only associated statistically with marihuana use and do not imply causation. Single males are three times as likely to use marihuana as single females or married persons of either sex. Users tend disproportionately to be from upper income or professional families. Those who are not affiliated with a formal religion are more likely to have used marihuana. They tend to major in arts, humanities, or the social sciences rather than in other fields. More than non-users, they have dropped out of school at some point. They participate less in campus organizations or activities except political ones.
Most of these findings were from studies done in 1968 and 1969. It is a distinct possibility that as more students try marihuana the differentiating characteristics noted in early studies will be less pronounced. This is a phenomenon that occurred with respect to drinking and smoking in past years. The more widespread the practice became the less deviant were the practitioners as a group.
Approximately the same pattern of socio-demographic characteristics is found among high school users of marihuana. In addition, it has been found that they are more likely to date steadily and start dating earlier than non-users. Again, the association is statistical and does not imply that marihuana use leads to earlier dating. Among high school students in one study, marihuana use or interest in use was related to college plans: the college-oriented were also marihuana-oriented (19).
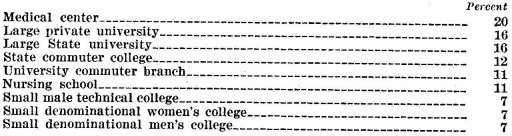
Student marihuana use also varies by type of college or school, along the lines suggested by the nature of users (1). Colleges whose students have higher socio-economic backgrounds, such as private colleges or universities, tend to have higher rates. (Women's colleges are exceptions.) Large public universities also have fairly high rates, as well as liberal arts colleges, except the small denominational schools. Schools with a professional, vocational, or technical program tend to have lower rates. In the nine-campus study in the West in 1969, the following rates of marihuana use were found for the different types of colleges:
High schools follow a similar pattern: Private schools and urban and suburban schools have higher rates of use than small town and rural schools.
THE HANG LOOSE ETHIC
Certain attitudes and interests have been shown to be even more closely related to marihuana use than are the socio-demographic characteristics (28). None of these attitudes was true only of marihuana users, nor true necessarily of all of them. And there is no indication that marihuana use caused them. Characteristics of the hang-loose ethic have been defined as: dissatisfaction with own education and the system; opposition to the Vietnam war and the draft; approval of sexual freedom; feeling a communication gap between self and parents; anticipation of satisfaction from future leisure activities more than from work; participation in "happenings" and mass protests; interest in underground newspapers; and acceptability of possible circumvention of laws (but not necessarily of breaking them).
High school marihuana users' attitudes tend to be similar. In high schools, however, marihuana use appears to be more recreational than symbolic of positions on politics and life (6).
INITIATION AND SOURCE OF SUPPLY
Few detailed data are available on initiation in a group of drug 'users or source of supply of marihuana. In several studies, however, it appears that most users are introduced by a close friend or someone they know well. In one college study, most began use in a friend's apartment with one or two others present (12). In one high school study, students most often obtained the drug in other people's homes, and about half obtained it without spending money (14).
Before the rapid spread of interest and use in marihuana in the 1960's, the sociologist Howard Becker described the process of becoming a marihuana smoker (2). In essence, the initiate seldom experiences any effects of the drug in the beginning without instructions from associates on how to inhale and hold the smoke in the lungs. The individual's interpretation of the experience as euphoric and sociable is aided by the expectations of the group.
MARIHUANA USE IN OTHER COUNTRIES
Cannabis grows in most of the countries of the world, including all those in the Western hemisphere, Africa, the entire continent of Asia, Australia and the Indonesian archipelago. A few scattered varieties may be found in Europe. Although there are botanical affinities between the various subspecies of cannabis sativa, the amount of psychoactive components in the plant varies widely.
The use of the plant for medical and religious purposes probably predates its use as a recreational drug. Cannabis has played a medical role in every country in which it was grown, including the United States, where from colonial times until at least the second decade of the present century, it was used in the treatment of a variety of illnesses. Until 1937, marihuana in some form was a staple in many U.S. patent medicines. It is still used in Arabic and Indian medicine, and in the United Kingdom may be prescribed by doctors in the form of an extract or tincture of cannabis. According to the 1968 report on cannabis by the Advisory Committee on Drug Dependence, medical use by doctors is increasing in Britain (7).
In many countries cannabis has been used for religious purposes, either in conjunction with certain ceremonies ( where use is presumably not continuous) or to aid in meditation and the attainment of certain mystic states (particularly in India) when use would be presumably more constant, and the actual amount of the drug consumed much greater. The Indian Hemp Commission Report examined the use of cannabis in various parts of India, by various religious groups, and two later published reports have expanded on the original material (18). Religious use of cannabis has been noted among certain cult groups in Central and South Africa, Brazil, Mexico and Jamaica.
Despite the thousands of years cannabis has been used for medical, religious and recreational reasons, and in spite of its practically worldwide distribution as a growing plant, there are no accurate figures available on a worldwide basis of the amount of marihuana consumed ( and in what form), how much goes into medical and how much into nonmedical channels, the number and kinds of users, and the modal frequency of use. Moreover, the quantity and quality of reporting in this field varies widely from country to country, depending, as it does, not only on the method of data collection and the sources from which that data is collected, but also on the perceived threat to the society of cannabis use, and the history of its use in discrete and disparate segments of the population.
In 1956, the United Nations Commission on Narcotic Drugs observed that it was clear that the consumers of cannabis, as of opium, numbered over 200 millions in the world, and that geographically it was the most widespread drug of abuse. Actual hard figures as to prevalence and incidence are notoriously lacking, however. Most countries rely on figures of arrest and customs seizures to indicate the extent of the problem, and these figures, of course, depend on the size and training of the enforcement patrols, general public interest in the problem, and a host of other variables. It can certainly be said with confidence that these figures underrepresent the total amount of marihuana consumed, as well as the number of users. In India, government excise records provide the most accurate statistics on the amount of cannabis consumed.
The Wootton Subcommittee of the British Advisory Committee on Drug Dependence received estimates from witnesses concerning the number of people who had tried cannabis and those who used it regularly (7). Estimates of the number of British users ranged between 30,000 and 300,000 and the Commission itself could find no firm basis for issuing an estimate of its own. They did publish a list of convictions for cannabis offenses from 1945 on, and their figures show a steady progression from 4 in 1945 to 2393 in 1967. In 1966 and 1967 there was an annual doubling of convictions but Commission members doubted that these figures represented an actual increase in amount of cannabis consumption and suggested they were possibly due to increased police vigilance.
The type of cannabis offender also changed markedly from the 1950's (when the first use of cannabis was noted among non-white immigrants to England) to 1964 when, for the first time, white persons constituted the majority of offenders. This trend has continued. The Commission concludes that, on the basis of convictions alone, cannabis use is not only widespread geographically, but cuts across class and color lines as well.
Many witnesses felt that it was possible to distinguish various types of marihuana users, for example, college and university students, jazz and pop musicians and artists, people working in the mass media, professionals in a variety of fields, as well as a growing number of workers in unskilled occupations—however, none of these witnesses could give anything but an informed guess as to the actual number of people involved in these various groups.
Although the Wootton Subcommittee Report mentions the fact that an increasing number of doctors are prescribing extract of cannabis and tinctures of cannabis, they give no exact figures as to the number , of prescriptions, the number of doctors prescribing, or the amounts prescribed. At the time the report appeared, there was no requirement that prescription records should be available to the Inspector of Drugs, but Commission members felt that such records should be made available in order to keep a close watch on the prescribing trend within the next few years.
In Ireland, there are no complete studies either from private or official sources relating to drugs and drug abuse. There is, however, a Working Party on brug Abuse established by the Ministry of Health in December of 1968, and they have released some figures on drug abuse in the Dublin area. A press release from this Working Party (June 2, 1970) indicates that there are at least 350 young people who have abused drugs, and the number is increasing. The drugs involved to date have been mainly amphetamines, barbiturates and tranquilizers (usually stolen) and LSD and cannabis smuggled into the country. An outpatient center for drug abusers has been set up in Dublin at the Jervis Street Hospital.
In July 1970, the German Federal Ministry for Youth, Family and Health was given a 1971 budget of approximately $375,000 to carry out a program of intensified efforts to prevent a rise in drug abuse (primarily hashish and marihuana). German authorities state that they did not, until comparatively recently, have a drug abuse problem, and they still do not have much of a problem with the hard narcotics. Illicit use of heroin and opium is virtually unknown.
Part of the funds budgeted for the Federal Ministry will be used to conduct at least two surveys—one survey, to be conducted by the Federal Center for Health Information, will attempt to determine pattern of use and motivation for use in sample of 300 persons aged 15 and over. The second survey will be conducted among 5,000 school children. The Bonn Government has also requested aid from other countries (including the U.S.) to help them in developing effective programs of prevention, education and treatment in the drug abuse field.
In Austria, the growing amount of drug use by juveniles is a major concern of the Federal Ministry of Education and Arts. In the Spring of 1970, the Ministry initiated a survey of school authorities in Austrian schools (excepting elementary schools and those for the mentally retarded) to find out how many cases of drug use had come to their attention. Although the final reports of this survey have not been published, it was apparent that hashish was the drug of choice for most students.
Sweden in 1968-1969 conducted, through its Military Psychological Institute' an extensive study. of 23,305 eighteen year old military conscripts to investigate their use of drugs, including tobacco and alcohol. The study (which guaranteed anonymity to the respondents) was undertaken in four major recruiting areas. Fifty per cent of the boys in the study came from big city areas.
In large city areas about 19-26% of the conscripts had used illicit drugs at least once, and for smaller cities the rate was between 8% and 9%. For drug experienced conscripts (defined as someone who has used a drug at least once) cannabis is by all odds the drug of choice, at least 58-73% of the conscripts have used cannabis from one to ten times, and cannabis is the favorite drug for 74% to 91% of them. The first drug tried, for about 77% to 89% of the users, was cannabis. Between 25% and 60% of those who have not tried illicit drugs have been offered them one or more times.
In Australia, according to a New York Times dispatch, December 20, 1970, the Minister for Customs and Excise states that they have seized twenty times more drugs this year than two years ago. Surveys by the narcotics section of the federal police department have shown that students account for 6 to 8 per cent of defendants charged with drug offenses, members of the armed forces 2.3 per cent. The bulk of the offenses were committed by unskilled and semi-skilled workers in their early twenties. Marihuana was involved in 44% of the drug cases brought to court this year—an increase of almost 13% in such prosecutions since last year.
In New Zealand, a special committee set up in 1968 under the Board of Health, made its first report in February of 1970 on Drug Dependency and Drug Abuse in New Zealand (8). The Committee indicated that they were not in a position to give a full and comprehensive picture of total cannabis use in New Zealand, but that on the basis of evidence obtained during the course of extensive public hearings they were prepared to state that at least four groups of users could be identified. These groups included : Multiple drug users (those who combined cannabis use with the use of other drugs), cannabis only users, spree or occasional users, and experimental users. Since cannabis is only intermittently available in New Zealand, this was not the drug of initiation for many of the drug users whom the committee interviewed. Drug use seems to be concentrated more in North Island than in South Island. Cannabis was introduced to New Zealand early in the 1940's by American servicemen, but did not seem to catch on to any extent until the early 50's, when it was taken up by people in the entertainment industry. In the 1960's other segments of the population became involved and members of the Commission believe that use, while still not extremely extensive, so far as they could determine, is now spread through varying segments of the population.
In Canada the Interim Report of the Commission of Inquiry Into the Non-Medical Use of Drugs (the Le Dain Report) gives the results of high school and college surveys on cannabis use (15). In eleven high school surveys conducted in various parts of the country in 1968 and 1969, admitted cannabis users (defined as those who had used the drug at least once within the past six months) ranged from a low of 5.9 to a high of 24.2%. In the largest of these surveys (N of 11,454) conducted in 1968 in London, Ontario, the usage rate for males was 7.9 and for females 3.6%.
College surveys carried out in 1968 and 1969 at six universities ranged from a low of 19.6% use to a high of 44.5%. In general, surveys carried out in 1969 show a higher use rate (use defined in the same way as in the high school surveys; i.e., use at least once within the past six months) than those conducted n 1968. One survey, is ried out in the fall and spring terms of the same academic year, is of particular interest because it shows a rise in percentage of users from 19.6% to 27.3%.
The Commission, on the basis of these published survey studies, as well as testimony gathered from expert witnesses, and data from government and police records, states that it is reasonable to believe that probably more than 10% of all high school students in Canada have used cannabis, and, of course' some studies in certain parts of the country have found much higher proportions. Data on use from a university level suggest that at least 25% of all university students have at least experimented with marihuana.
The Commission solicited, and received, letters from private citizens on the non-medical use of drugs. A review of these letters, as well as expert testimony from informed observers, indicates that the use of cannabis has spread to groups other than the young in various social classes.
Although the New World has a much greater array of both narcotic and hallucinogenic plants than the Old World, cannabis is not indigenous here. The plants were probably introduced at the time of the Spanish conquest to Mexico, Central and South America: There is a difference of opinion among experts about Brazil, with some persons claiming that cannabis was introduced by the original Portuguese explorers, and others who state that it came in later, with the advent of Negro slaves. In some of the islands of the West Indies (Jamaica, Trinidad) cannabis (ganja) was brought in by East Indian indentured laborers after the emancipation of the Negro slaves. In the United States, most writers feel that cannabis (in the form of the hemp plant) was introduced by the early English colonists.
There are few adequate use figures from any of the Latin American countries, but unpublished reports from the Pan American Health Bureau, as well as other informed sources, agree that the same phenomenon observed in other parts of the world, i.e., the spread from exclusive lower class use to use by at least the younger members of the middle and upper classes is increasing. These reports are particularly interesting in view of the fact that in Latin American countries the difference in life style between members of the lower classes and those of the upper class has always been much greater than that which prevails in more highly industrialized and urbanized countries.
The growing amount of multiple drug use by middle and upper class youth has prompted interest on the part of public health authorities, and they have asked for expert assistance from the United States in the design of survey studies to be used with school populations.
Brazilian scientists have long had an interest in calm abis use, as is evidenced by papers presented at the second Pan American Scientific Congress held in Washington in 1915. Present day research interest spans the physical and the behavioral sciences.
Up until the beginning of rapid industrialization in southern Brazil about two decades ago, use of cannabis tended to be centered in the northeastern coastal states, and in cities with a high concentration of non-whites such as Bahia. Poor immigrants from these regions to Sao Paulo and Rio de Janeiro brought machonha with them when they decided to hunt for jobs in the fast growing industries. Present day reports indicate that use has spread from these impoverished workers to young members of the middle and upper classes.
Reports emanating from Lima indicate that there is a growing use of drugs of all types, primarily by young middle and upper class students. However, there is one interesting footnote which should be appended—in the Lima squatter settlements with inhabitants drawn mainly from the high Andes, there is evidence that coca is being replaced by cannabis as the drug of choice. Such self-medication, i.e., the substitution of cannabis for a stronger drug, has been noted previously in other parts of the world, for example, India, where cannabis has been used n place of opium.
In Mexico, where use of marihuana has long been common among both the rural and the urban poor, authorities indicate that use is now spreading among wealthy youngsters, as is indicated by the growing number of arrests in this group.
Cannabis is an illicit drug in all Latin American countries but most drugs which can be obtained only on prescription in the tinted States (sedatives, amphetamines, tranquilizers) can be bought over the counter in most countries there.
In the Caribbean, marihuana (ganja) was introduced by East Indian laborers after emancipation. An NIMH sponsored study of chronic cannabis users in Jamaica indicates that they are drawn from at least five disparate population groups. Up until about three years ago users were predominantly members of lower class rural and urban groups, but authorities report that middle and upper class youngsters are now incerasingly turning to use of the drug. One group of users in Jamaica, the Rastafaris, are of particular interest, since a good deal of their religious ritual as well as life style revolves around the drug. These people call themselves "the chemists of the divine herb" and use ganja in all forms, from both male and female plants, in foods and for smoking. Ganja is even used in a concoction especially designed for babies with croup.
Cannabis use was widespread in Near Eastern, African and Asian countries for a much longer period of time than in 'Western countries, so the literature is much more extensive from these regions. However, several cautions should be borne in mind when considering these studies. These cautions include : 1. The use of biased samples (study groups frequently drawn from prison populations or exclusively from mem- bers of the lowest economic groups) • 2. The lack of adequate control groups; 3. Frequent failure to consider the implications of the fact that cannabis tends to be mixed with other drugs ( tobacco, dhatura, or more rarely opium) , or the corollary question of the extent to which users of cannabis are also users of other drugs.,
The question of the duration of use of cannabis is probably one of the most important issues from a public health standpoint. Observations of Eastern writers tend to be at odds with those from other parts of the world. Most of the former imply that once the cannabis habit is 'established it is likely to last as a da4 habit for many years. However, actual longitudinal data on representative samples of persons initiated to its use are seldom if ever cited. In other parts of the world there are indications that there may be discontinuation . With some users after adolescence, and with others the establishment of a pattern of intermittent-use.
The government excise records of India afford the most accurate statistics on the amount of cannabis used in that country, but it must be recognized that there is no adequate estimate of the amount of material which enters the country illegally, primarily from 'Nepal. It is estimated that the current number of habitual ganja users is about 240,000 (not including the users of bhang, or of smuggled charas). This is about one half of the number of licit ganja and charas users (excluding bhang) estimated in 1940. Most observers feel that the steady decline in cannabis use in India can be attributed to several factors, including a reduction in the number of acres licensed by the government for production, higher excise duties, increasing competition from other drugs, and a growing belief that cannabis is essentially a low status drug.
Although the decline in cannabis consumption in India is striking, there is some evidence that India is not immune from the rising use of multiple drugs by students, which is characteristic of many other countries.
In Egypt, expert observers estimate that the current number of hashish users is about 180,000, which would include about four to five percent of the male population between 20 and 40.
There are no adequate current use figures from Morocco but most trained observers estimate that about 30 to 35% of the adult male population use cannabis to some degree.
There are no estimates available for -South Africa after 1953. In that year the estimate of users was about 50% of the native male population in some areas, but relatively low in others.
There are no estimates at all available for the number of users in Nepal, the only country in the world where cannabis use is legal.
The foregoing brief summary of cannabis use in countries other than the United States points up the general inadequacy of the data currently available on extent, patterns, and persistence of use, the physical and psychological characteristics of users, as well as the general social climate in which cannabis use is either introduced, expands, or declines.
Research into the relative frequency of the various patterns of cannabis use in differing cultures is badly needed, as well as longitudinal studies with user groups in certain selected countries, and carefully designed small studies which will examine in depth natural history of drug using careers.
1 These changes are not a function of a statistical "ceiling effect" that sometimes results when 'there is little room for figures to change. The proportions having had "any use" during 1970 ranged from 32% to 51%; at these levels, there was sufficient room for large Increases, but they did not occur.
2 In this instance "chronic use Is a loose concept covering all use at the upper levels of frequency, regularity, or both,
REFERENCES
1. Barter, James T., Mizner, G. L., & Werme, P. II. Patterns of drug use among college students. (Unpublished report to Bureau of Narcotics and Dangerous Drugs, U. S. Dept of Justice, 1970).
2. Becker, Howard. Outsiders. Glencoe, Ill., Free Press, 1963.
3. Berg, Dorothy. Illicit use of dangerous drugs in the United States. Bureau of Narcotics and Dangerous Drugs, U. S. Dept. of Justice, Sept. 1970.
4. Black, Samuel, Owens, K, & Wolff. R. P. Patterns of drug use : A study of 5.482 subjects. American Journal of Psychiatry, 127(4) : 420-423, Oct. 1970.
5. Blum, Richard H., & Associates. Students and drugs. (Vol. 2) San Francisco, Jossey-Bass, 1969.
6. Bogg, Richard, Smith, It., & Russell, S. Drugs and Michigan high school students. Final report of a study conducted for the Special Committee on Narcotics, Michigan Legislature, 1968.
7. Cannabis. Report by the Advisory Committee on Drug Dependence. London, Her Majesty's Stationery Office, 1968. (Wootton Committee Report).
8. Drug dependency and drug abuse in New Zealand. 1st Report. Board of Health, Report Series #14, Feb. 16, 1970. Wellington, New Zealand, A. It. Shearer, Government Printer.
9. Elinson, Jack. NIMH grant 17589. A study of teen-age drug behavior. Columbia University, New York, N. Y.
10. Francis, John B., & Patch, D. J. Student attitudes toward drug programs at the University of Michigan. University Committee on Drug Education, Ann Arbor, Michigan, Sept. 1969.
11. Gallup Poll. Washington Post, May 26, 109; October 26, 1969.
12. Goldstein, Joel. The social psychology of student drug use. Dept. of Psychology, Carnegie-Mellon University, Pittsburgh, Pa., 15213, 1970.
13. Governor's Citizen Advisory Committee on Drugs. Drug use among high school students in the State of Utah. In: Advisory Committee report on drug abuse. State of Utah, State Capital Building, Sept. 1969.
14. Grosse Pointe Public School System, Grosse Pointe, Michigan. PSC Coinnrunicator, Jan. 13, 1970.
15. Interim, report of the Commission on Inquiry Into the Non-Medical Use of Drugs. Berger Bldg., Metcalfe Street, Ottawa, Canada) Ottawa, Queen's Printer for Canada, 1970. (LeDain Report)
16. Manheimer, Lean I., Mellinger, G. D., & Baiter, M. B. Use of marihuana in an urban cross-section of adults, in communication and drug abuse (Wittenborn, Smith & Wittenborn, Eds.) Springfield, Ill., Charles C. Thomas, 1970.
17. Manheimer, Dean I., Mellinger, 0. D., & Baiter, M. B. Marihuana use among urban adults. Science, MI :1544-1545, Dec. 19, 1969.
18. Marihuana. Report of the Indian Hemp Drugs Commission, 1893-1894. Silver Spring, Md. The Thomas Jefferson Press 1909. (Introduction & Glossary by John Kaplan.) Reprinted, original published in 1894.
19. Manes, Armand L. Anticipatory socialization toward college as a factor in adolescent marihuana use. Social Problems, 16 :357-364, 969.
20. McKenzie, J. D. Trends in marihuana use among undergraduate students at the University of Maryland. Researhe Report #3-70. Counseling Center, University of Maryland, 1970.
21. Montgomery County, Md., Joint Advisory Committee on Drug Abuse. Final Report, Vol. 2. Montgomery Co. Public Schools, Rockville, Md., 1969.
22. Newsweek Staff. Report of a national college student survey (untitled). Newsweek, Dec. 29, 1969.
23. New York Times, Dec. 20, 1970.
24. Robins, Lee. & Murphy, G. Drug use in a normal population of young Negro men. American Journal of Public Health, 57 (9) :1580-1596, Sept. 1967.
25. Roffman, Roger A., & Sapel, E. Marihuana in Vietnam, International Journal of the Addictions, 5 (1 ) :1-42, March 1970.
26. San Mateo, California Dept. of Public Health and Welfare, Research and Statistics Section. The use of alcoholic beverages, amphetamines, LSD, marihuana, and tobacco reported by high school and junior high school students. San Mateo, Cal. 94403, 1968--GO; and preliminary release of 1970.
27. Study of life styles and campus communities. Preliminary report. Dept. of Social Relations, Johns Hopkins University, Balto., Md. 21218, Dec. 1970.
28. Buchman, Edward A. The "hang-loose" ethic and the spirit of drug use. Journal of Health and Social Behavior, 9 (2) :146-154, June 1968.
29. Speck, Ross V. NIMH grant 14943. Psychosocial networks of young drug users. Hahnemann Medical College, Philadelphia, Pa. Final report, Oct. 1970.
30. Udell, Jon G., & Smith, R. S. Attitudes, usages, and availability of drugs among Madison High School students. University of Wisconsin, Bureau of Business Research & Service, Madison, Wise., July 1969.
31. Yolks, Stanley F. Testimony before the Subcommittee to Investigate Juvenile Delinquency in the United States, of the Senate Committee on the Judiciary, Narcotics Legislation Hearings, Sept. 17, 1909.
| < Prev | Next > |
|---|