Drug AbuseChapter 4 The Relationship Between Heroin Use Onset Date and Current Injecting Drug Use in the Netherlands: Changes over Time From ± 1970 to 1990.
4.1 Introduction
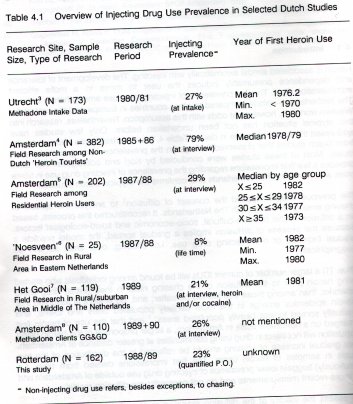
Heroin is associated almost axiomatically with injecting. The development of tolerance and dependence presumably induces the user to move to a more efficient administration ritual. The low prevalence of injecting drug use among heroin users in The Netherlands --unique compared to other countries in Europe and the rest of the Western world-is, however, at odds with this assumption. Nevertheless, research into this atypical situation has not been undertaken before. Only few studies have addressed the issue, but none in depth. Table 4.1 summarizes some relevant results from Dutch studies that presented findings on the prevalence of drug administration rituals. Most of these studies were conducted by Korf and colleagues. The table provides a few first impressions regarding the prevalence of injecting drug use in some cities and towns in The Netherlands and confirms the atypical Dutch situation.
The previous chapter applied the concept of diffusion' to analyze the spread of chasing among heroin users in The Netherlands. It reconstructed this process, based on a diffusion model of sociocultural, socioeconomic and socioecological factors. Because the process of diffusion implies a gradual spread, the model predicts a gradual increase of non-injecting drug use, i.c. chasing, over time, as well as geographically.
Thus, (1) a larger number of current IDUs will be found among individuals who started using heroin prior to the diffusion of the chasing ritual in their (initial) drug using networks, than among those that started hereafter; and, (2) when it is assumed that "heroin epidemics emerge in the most densely populated cities and towns, and gradually spread to less heavily populated areas", and that the use of heroin first emerged on a noticeable scale in Amsterdam, a larger proportion of the heroin using population will not inject in drug using communities at greater distance of Amsterdam. This gradual increase of chasing should be reflected in the distribution of the two rituals in samples of heroin users. The first impressions derived from table 4.1 (cautiously) suggest lower prevalence of injecting drug use outside of Amsterdam and at more recent measurements and do not contradict the diffusion model.
To assess the validity of the diffusion model, a review of existing databases was undertaken to examine their suitability for secondary analysis for the two above distinguished diffusion patterns. Testing for geographical diffusion turned out to be impossible. Comparable data sets were not only unavailable, it was also felt that the research question was too sensitive and complex to test on data sets, that were not explicitly developed for this purpose. For example, certain border towns (at relatively great distance from Amsterdam) may well be subject to, what in this case can be called 'reversed diffusion', that is diffusion of injecting from across the border. Testing for changes over time seemed more promising, as, in that case, the analysis could be limited to comparisons within the selected data sets.
Two data sets containing the two crucial variables (year of onset heroin career and current administration ritual) became available. These were cordially supplied by the following organizations:
P. Boumanhuis Centrum Verslavingszorg Zuid-Holland-Zuid (Center for Addiction Services) in Rotterdam. The data were collected from January 1989 until December 1990 during the intake procedure for methadone (maintenance) treatment.
Gemeentelijke Geneeskundige & Gezondheidsdienst, afdeling Volksgezondheid en Milieu (GG&GD - Municipal Health Service, Department of Public Health and Environment) in Amsterdam. The data result from the AIDS-cohort study and were collected during 1989 and 1990.*
On both these datasets the following, from the diffusion model derived, hypothesis has been tested: The year of heroin career onset is associated with the current selfadministration ritual: Current injecting is related with earlier onset dates.
4.2 Methods
4.2.1 Matching the Samples: Dilemmas and Choices
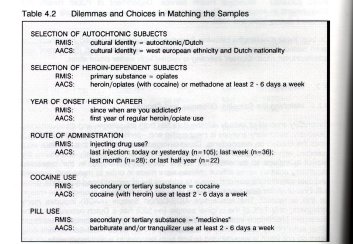
Secondary analysis of already existing data has both advantages and disadvantages. Obviously, secondary analysis is inexpensive and --perhaps even more important-- it limits the burden on respondents. Disadvantageous is, however, that the data were collected with some specific aim, thereby often not, or only partially addressing the explicit questions to be answered in the secondary analysis. In the presented secondary analysis some difficult choices were made in order to make both samples and data-sets comparable and usable to address the aforementioned questions. (table 4.2) First of all the data-sets have been reduced to autochtonic subjects. The reason for this is twofold. The Amsterdam AIDS-Cohort Sample (AACS) includes many foreigners; only 71% of the original sample (n=520) has a Dutch nationality. In the Rotterdam Methadone- Intake Sample (RIVIIS) the majority of the clients (n = 1123) are either autochtonic Dutch (64%) or Surinamese (17%). Since most Surinamese drug users do not inject, it was decided to limit both samples to autochtonic, white, Dutch subjects. Secondly, since the RMIS consists of subjects seeking methadone treatment it should be of no surprise that 99% report opiates to be their drug of first choice. Again for the sake of comparability and clarity, both samples have been restricted to opiate using subjects. For the AACS this implies that heroin, methadone or other opiate use at least two days a week was taken as an inclusion criterion. The combined inclusion criteria resulted in matched samples of Autochtonic, White, Dutch Opiate Dependent Subjects, with a sample-size for the RMIS of 711 subjects and for the AACS of 282 subjects.
Regarding the route of administration, the following points must be stressed. Both the AACS and the RMIS are selfreported data and therefore subject to the usual limitations. While in Amsterdam specific questions about (first) injection practices were asked, in Rotterdam subjects were merely asked if they injected their drugs. The Rotterdam data are therefore more likely a representation of the subjects self-definition as either an IDU or a chaser --they contain no information on life-time prevalence of injecting or (single) exceptions. In the AACS current injecting has been defined as 'having injected at least once during the half year prior to interview. However, of the total sample 87.2% has ever injected, while 60% of the subjects defined as current non-IDUs have injected at least once in their career.
* Four cases were collected in 1991.
4.2.2 Statistical Analyses
In analyzing the data and testing the hypothesis both univariate and multivariate statistical techniques have been applied, using SPSS/PC. First, current administration ritual (CAR) has been related to several relevant variables. For dichotomous variables, e.g., sex and cocaine use, Ch i2 -statistics have been computed, while for interval variables, such as the year of heroin career onset, t-tests were performed. Although the relative number of current IDUs in the RMIS and the AACS differed, the factors correlating with injecting were identical. Therefore, the univariate correlates of injecting are presented for both samples combined. Second, all tested variables which related to CAR were consequently entered into a multivariate discriminant analysis. To test the hypothesis, a hierarchical procedure was selected in which - after forced entry of all other variables - the year of onset of the heroin career was entered last, thereby testing whether this variable contributed significantly to the discriminant function (i.c., in terms of reducing Wilks's Lambda, which is "a statistic which takes into consideration both the differences between groups and the cohesiveness or homogeneity within groups`) after the discriminative value of the other variables had been assessed. Results of the discriminant analyses, presented separately for the RMIS and AACS, are summarized in terms of (1) standardized canonical discriminant function coefficients (which give a measure of the relative and standardized contribution of the specific variable with respect to the discriminant function - and thus, in this case, the discriminative value of that variable in discriminating current IDUs from current non-IDUs), and (2) the classification results (i.e., by comparing the classification as IDU or non-IDU based on the discriminant function with the actual CAR). Unless otherwise indicated, in the following (non-)IDU refers to current (non-) IDU.
4.2.3 Sample Description and Comparison
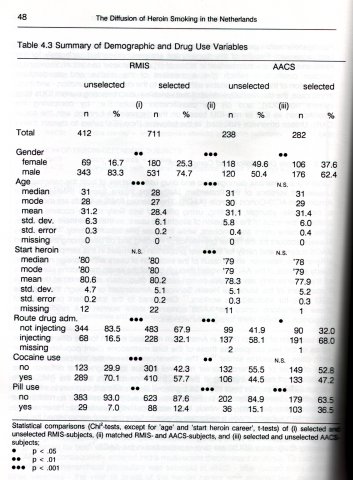
Table 4.3 summarizes demographic and drug use variables of both the selected and unselected versions of the Rotterdam Methadone Intake Sample (RMIS) and the Amsterdam AIDS-Cohort Sample (AACS). The selected RMIS subjects are more likely to be female, younger, injecting, using pills and less likely to use cocaine. This is probably the result of the exclusion of allochtonic users, as these are more often male, older, cocaine users and smokers, while they use pills less frequently." 5 This may likewise account for the higher prevalence of injecting and pill use among the selected AACS subjects and partly for the lower proportion of females in this sample. The latter difference is, however, also a result of the exclusion of users with a foreign nationality. Study subjects of the AACS enrolled through one of the seven methadone clinics (one of these takes only sex workers or non-resident drug users as clients) of the Drugs Department of the Municipal Health Service in Amsterdam or through the separate STD clinic for addicted sex workers." Compared to the total client population of these methadone clinics the AACS contained more women. 12 A relatively large proportion of these were foreign sex workers.
The exclusion of foreign users in Amsterdam may also explain for the different gender ratios of the two samples, as those of the total methadone client populations are in both cities remarkable similar.` 12 The differences between the samples in age and year of onset of the heroin career may well be due to geographical diffusion. The prevalence of current injecting in the AACS is twice as high as in the RMIS (68% versus 32%). This difference might be explained by the different contexts in which the data have been gathered. In Rotterdam the subjects entered a methadone (maintenance) program, for which they were routinely questioned. However, the Amsterdam subjects made a deliberate choice to have themselves screened for HIVinfection. Since the possibility to become HIV infected is significantly related to injecting drugs (as opposed to non-injecting modes of drug administration), it is not odd that injecting drug users (IDUs) are over-represented in the AACS.13
4.3 Results
4.3.1 Year of Onset of the Heroin Career and Current Injecting
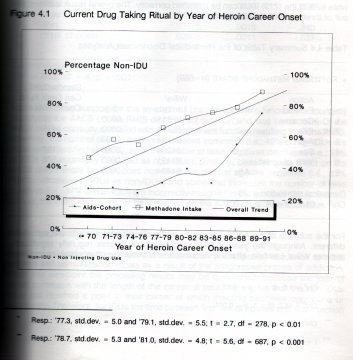
In both samples a relationship has been found between, the year in which the heroin career commenced and whether or not injecting was the current self-administration ritual. Amsterdam IDUs on the average started using heroin on a regular basis in the beginning of 1977, while non-IDUs used opiates regularly two years later.* Similarly, Rotterdam IDUs are addicted since the middle of 1978 as compared to non-IDUs who became addicted in the early 1980s. **This relationship is presented graphically in figure 4.1. It can be seen that opiate users, that started their drug career as early as 1970 or before, are in minority non-IDUs (45% for RMIS and 26% for AACS). This percentage rises steadily -via 71% and 39% for those starting in the early 1980s--- to 88% and 75% for (respectively, RMIS and AACS) subjects starting their drug career as late as 1989 to 1991.
Univariate analysis for both samples combined, showed that injecting is more prevalent among men (43%) than among women (40%), although this difference is not significant;' among subjects who used cocaine in the six months prior to interview (48% vs. 36%);- and among subjects who used pills in that period (64% vs. 37%). *** Finally, IDUs were about two years older than non-IDUs; 30.4 versus 28.4 years respectively. ---'Because of these multiple univariate relations, the discriminative value with respect to the administration ritual of all these variables has been assessed in a multivariate discriminant analysis.
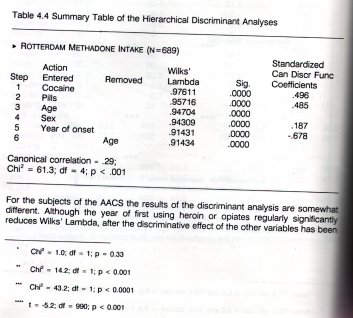
For the RMIS the year of onset of opiate addiction has the highest discriminative value with regard to the prevalent mode of drug administration; it has the largest standardized canonical discriminant function coefficient of all variables entered in the discriminant equation. (table 4.4). Moreover, even in a hierarchical discriminant procedure the year of onset significantly reduces Wilks' Lambda. By means of the canonical discriminant function 66% of the (470) nonIDUs can be classified correctly, while 62% of the (219) IDUs can be classified correctly. The overall result is almost two out of three correct classifications (65%).
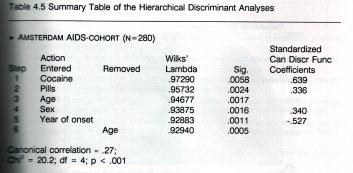
For the subjects of the AACS the results of the discriminant analysis are somewt different. Although the year of first using heroin or opiates regularly significan reduces Wilks' Lambda, after the discriminative effect of the other variables has be assessed, the strongest discriminative variable in respect to IDU is whether or not the subjects used cocaine in addition to opiates. (table 4.5). The classification results of the canonical discriminant function for the AACS are almost an exact replication of the RIMS classification. 66% Correct classifications of (90) non-IDUs, 62% correct classifications of (190) IDUs and an overall result approaching two out of three correct classifications (63%).
Some additional support for the strength of both discriminant functions is found by classifying the AACS on the RMIS discriminant function and vice versa. 64% Of the AACS can be correctly classified with the discriminant function resulting from the RMIS. However, the number of false positives increases somewhat (i.e., 42% of non-IDUs are incorrectly classified as IDUs), while the number of false negatives decreases (i.e., 33% of IDUs are incorrectly classified as non-IDUs). Similarly, classifying the RMIS on the AACS discriminant function does not affect the number of false negatives (i.e., 37% misclassifications of IDUs as non-IDUs) and somewhat increases the number of false positives (i.e., 37% of non-IDUs are incorrectly assigned to the group of IDUs). Overall, 63% of the RMIS can correctly be classified on the AACS discriminant function.
4.3.2 Progression into Injecting Drug Use
The conventional view on heroin use assumes an (inescapable) sequence to more efficient self-administration rituals as a result of the progressive proces of addiction. From this viewpoint the preceding results may be questioned, because the year of onset correlates with the length of the career. It could be argued that the non-IDUs have not reached a point in their career at which injecting becomes opportune or necessary. Therefore, for IDUs the time between first use of opiates and first injection
was calculated, and compared to the length of the heroin career of non-IDUs.* As the data on first injection was not available for the RMIS, this analysis was limited to the AACS.
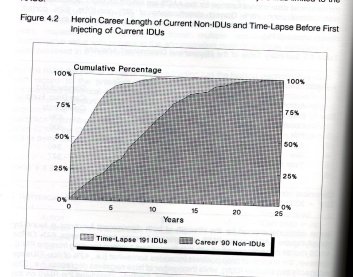
Although IDUs report a longer heroin use career than non-IDUs,*' most non-IDUs have a career of regular heroin consumption long enough to have made the transition to injecting. As can be seen from figure 4.2, 43% of current IDUs first injected in the year (or the years before---*) they used heroin regularly. 52% made the transition. Again, it must be emphasized that this does not imply that these current non-IDUs never injected.
--- Resp.: 10.5 years, std.dev. - 5.1 and 8.8 years, std.dev. = 5.3; t - -2.6, cif - 278, p < .05 ... In 35 cases first injecting supposedly preceded regular use of heroin (or other opiates). Some of these individuals may have injected heroin on an occasional basis prior to regularly using the drug. Others probably injected other drugs, such as amphetamine or opium, before heroin use. Some discrepancy may have resulted from errors of interviewee's memory or interpretation, the interviewer, and/or further data processing (recording, entry, or coding). Given these explanations, it was decided to equate these cases with subjects, who reported first injection and first heroin/opiate use in the same year (time lapse - 0 year). Excluding these cases did not really influence the results of the analysis.
within two and 77% within four years (mean= 2.1, median= 1, mode= 0). In contrast, four out of five non-IDUs have been using opiates for at least tour years and half of them have a career length of more than eight years. Thus, comparing the length of the heroin using career of non-IDUs to the transition time of IDUs, it can be concluded that non-IDUs have been long enough at risk to initiate a regular injection pattern.
4.4 References
1. Katz E, Levin ML, Hamilton H: Traditions of research on the diffusions of innovation. American
Sociological Review 1963; 28: 237-252.
2. Parker H, Newcombe R, Bakx K: The new heroin users: prevalence and characteristics in Wirral,
Merseyside. British Journal of Addiction 1987, 82: 147-157,
3. Bindels P, Steinbusch M, Tiggelman A, Vernooy R: Onderzoeksverslag 1 Methadonteam Utrecht.
Utrecht: Consultatiebureau Alcohol en Drugs Utrecht, 1981.
4. Korf DJ: Heroinetoerisme 11: Resultaten van een veldonderzoek onder 382 buitenlandse dage
lijkse opiaatgebruikers in Amsterdam. Amsterdam: ISG, Universiteit van Amsterdam, 1987.
5. Korf DJ, Hoogenhout HPH: Zoden aan de dijk: Heroinegebruikers en hun ervaringen met en
waardering van de Amsterdamse drugshulpverlening. Amsterdam: Instituut voor Sociale Geografie, Universiteit van Amsterdam, 1990.
6. Korf DJ, Mann 1, Aalderen H van: Drugs op het platteland. Assen/Maastricht: Van Gorcum,
1989.
7. Korf DJ, Aalderen H van, Hogenhout HPH, Sandwijk JP: Gooise Geneugten: Legaal en illegaal
drugsgebruik (in de regio). Amsterdam: SPCP Amsterdam, 1990.
8. Hes J, Korf DJ, Buning E, Elorche M: Bekijk het Een follow-up onderzoek naar audiovisuele
en andere AIDS-voorlichting bij drugskliënten van de Amsterdamse GG&GD. Amsterdam: Amsterdamse Werkgroep Aids en Drugs, 1991.
9. Klecka WR: Discriminant analysis. Beverly Hilis/London: Sage University Paper, # 19, 1980: 54. 10, Toet J: Het RODIS nader bekeken: Cocainegebruikers, Marokkanen en nieuwkomers in de
Rotterdamse drugshulpverlening rapport 87. Rotterdam: GGID-Rotterdam e.o., Aldeling Epidemiology, 1990.
11. Hartgers C, Hoek JAR van den, Krijnen P, Brussei GHA, Coutinho RA: Changes over time in
heroin and cocaine use among injecting drug users in Amsterdam, The Netherlands, 1985-1989. British Journal of Addiction 1991; 86: 1091-1097.
12. Reijneveld SA: Methadonverstrekking in Amsterdam in 1990: Jaaroverzicht van de Centrale
Methadon Registratie. Amsterdam: GG&GID Amsterdam, Stafbureau Epidemiologie en Documentatie, 1991.
13. Hartgers C, Santen GW van, Haastrecht HJA van, Hoek JAR van den, Akker R van den,
Coutinho RA: De HIV-preva)entie onder druggebruikers die methadon verstrekt krijgen bij de drugsafdeling van de GG&GD te Amsterdam. T Soc Gezondheicisz 1992; 70: 275-279.










 |
|  |
| 