| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 211 |
| Yesterday: | 251 |
| This Week: | 211 |
| Last Week: | 2221 |
| This Month: | 4799 |
| Last Month: | 6796 |
| Total: | 129398 |
Chapter 13 Young people, recreational drug use and harm reduction
 |
|  |
| 
| Reports - EMCDDA Harm Reduction |
Drug Abuse
Chapter 13 Young people, recreational drug use and harm reduction
Adam Fletcher, Amador Calafat, Alessandro Pirona and Deborah Olszewski
Abstract
This chapter begins by reviewing the prevalence of recreational drug use and related
adverse health outcomes among young people in European countries. It then employs a
typological approach to review and discuss the current range of responses that aim to reduce
the harms associated with young people’s recreational drug use in Europe. These responses
include: individually focused and group-based interventions (school-based drugs education
and prevention, mass media campaigns, motivational interviewing, and youth development
programmes) and ‘settings-based approaches’, which make changes to recreational settings,
such as nightclubs, or institutional settings, such as schools, to address the social and
environmental background of young people’s drug use.
Keywords: young people, drug use, prevalence, harm, intervention, Europe.
Introduction
This chapter focuses primarily on young people’s use of illegal drugs (rather than alcohol and
tobacco use). However, the potential for harm is likely to be greatest when young people use
both drugs and alcohol, and many of the interventions reviewed in this chapter are
considered to be appropriate for reducing the harms associated with both drug and alcohol
use. The chapter will begin by reviewing the prevalence of drug use among young people in
Europe and the related adverse health and other harms. The appropriateness and likely
effectiveness of different types of interventions that aim to reduce the harms associated with
young people’s recreational drug are then discussed. Harm reduction has traditionally
focused on adult ‘problem’ drug users, particularly injecting drug users (see, for example,
Ball, 2007, and Kimber et al., 2010), and neglected not only the harms associated with young
people’s recreational drug use but also how to reduce these harms.
This chapter considers young people’s recreational drug use to be drug use that occurs for
pleasure, typically with friends, in either formal recreational settings, such as nightclubs, and/
or informal settings, such as on the streets and in the home. This is thus a broader definition
than the one applied in other EMCDDA publications, which often focus specifically on young
people’s drug use within a ‘nightlife context’ (e.g. EMCDDA, 2002). This chapter is primarily
focused on young people aged 14–19, although some studies report on other age ranges
(e.g. 14–24) and therefore at times it has been necessary to define ‘young people’ more
broadly. Furthermore, data on prevalence and trends of drug use among young people often
aim to provide an indication of overall levels of use and therefore do not always distinguish
between recreational drug use and more problematic patterns of use.
Trends in young people’s recreational drug use in Europe
The European School Survey Project on Alcohol and Other Drugs (ESPAD) and recent
general population surveys have revealed lower prevalence of use of cannabis and other
illicit drugs for European youth compared to youth in the United States (Hibell et al., 2004;
Hibell et al., 2009; EMCDDA, 2009). However, these overall European-level data mask
diversity within the EU in terms of young people’s use of cannabis, ‘club drugs’, such as
ecstasy and amphetamines, and cocaine.
Cannabis
The 2007 ESPAD data revealed that the highest lifetime prevalence of cannabis use among
15- to 16-year-old school students is in the Czech Republic (45 %), while Estonia, France, the
Netherlands, Slovakia and the United Kingdom reported prevalence levels ranging from
26 % to 32 % (Hibell et al., 2009). Lifetime prevalence levels of cannabis use of between 13 %
and 25 % are reported in 15 other countries. Less than 10 % of 15- to 16-year-old school
students report cannabis use in Greece, Cyprus, Romania, Finland, Sweden and Norway.
Early onset of cannabis use has been associated with the development of more intensive and
problematic forms of drug consumption later in life. In most of the 10 EU countries with
relatively high prevalence of frequent use, between 5 % and 9 % of school students had
initiated cannabis use at age 13 or younger. In addition, compared to the general population
of students, cannabis users are more likely to use alcohol, tobacco and other illicit drugs
(EMCDDA, 2009).
National survey data reported to the EMCDDA shows that in almost all EU countries
cannabis use increased markedly during the 1990s, in particular among school students. By
2003, between 30–40 % of 15- to 34-year-olds reported ‘lifetime use’ of cannabis in seven
countries, and more than 40 % of this age group reported ever having used cannabis in two
other countries. However, data from the 2007 ESPAD surveys suggests that cannabis use is
stabilising — and in some cases declining — among young people in Europe: of the 11 EU
countries for which it is possible to analyse trends between 2002 and 2007, four countries
showed overall decreases of 15 % or more in the proportion of 15- to 16-year-olds reporting
cannabis use in the last year, and in four other countries the situation appears stable (Hibell
et al., 2009; EMCDDA, 2009).
Ecstasy and amphetamines
It is estimated that 7.5 million young Europeans aged 15 to 34 (5.6 %) have ever tried
ecstasy, with around 2 million (1.6 %) using it during the last year (EMCDDA, 2009).
Estimates of prevalence are generally even higher among the subgroup of 15- to 24-yearolds,
for whom lifetime prevalence ranges between 0.4–18.7 % in European countries
(estimates fall between 2.1 % and 6.8 % in most European countries). Among 15- to 16-yearold
students lifetime prevalence of ecstasy use ranges between 1 % and 7 % in countries
surveyed in 2007 (EMCDDA, 2009).
Studies of recreational settings that are associated with drug use, such as dance events or
music festivals, provide further evidence regarding young people’s ecstasy and
amphetamine use. Estimates of young people’s drug use in these settings are typically high.
However, comparisons between surveys can only be made with the utmost caution, as the
age and gender distribution of survey respondents as well as variations in the setting may
lead to observed differences. Studies conducted in recreational settings in 2007 in five EU
countries (Belgium, Czech Republic, Latvia, Lithuania, Austria) reveal lifetime prevalence
estimates of 15–71 % for ecstasy use and 17–68 % for amphetamines (EMCDDA, 2009).
Much of party-going young people’s drug use occurs on weekends and during holiday
periods (EMCDDA, 2006b).
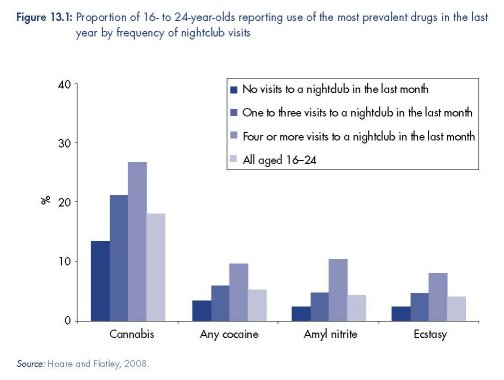
A further indication of the extent to which the use of these drugs may be concentrated
among the young, club-going population can found in the 2007/8 British Crime Survey
(Hoare and Flatley, 2008). The study found that those 16- to 24-year-olds who reported
visiting a nightclub four or more times in the last month were more than three times as
likely to have used ecstasy in the last year than those not attending nightclubs (2 % vs.
8 %) (Figure 13.1). In a French study that was carried out in 2004 and 2005 among 1 496
young people at ‘electronic’ music venues, 32 % of respondents reported ecstasy use and
13 % reported amphetamine use in the past month (Reynaud-Maurupt et al., 2007).
Among specific sub-populations that self-identified as ‘alternative’, prevalence estimates
for ecstasy and amphetamines were as high as 54 % and 29 %, respectively (Reynaud-
Maurupt, 2007).
Cocaine
Although cocaine is the second most commonly used illicit drug in Europe after cannabis
(EMCDDA, 2007), estimates of the prevalence of cocaine use among school students are very
low. Lifetime prevalence of cocaine use among 15- to 16-year-old students in the ESPAD
survey is between 1 % and 2 % in half of the 28 reporting countries, and in the rest it ranges
between 3 % and 5 % (Hibell et al., 2009; EMCDDA, 2009).
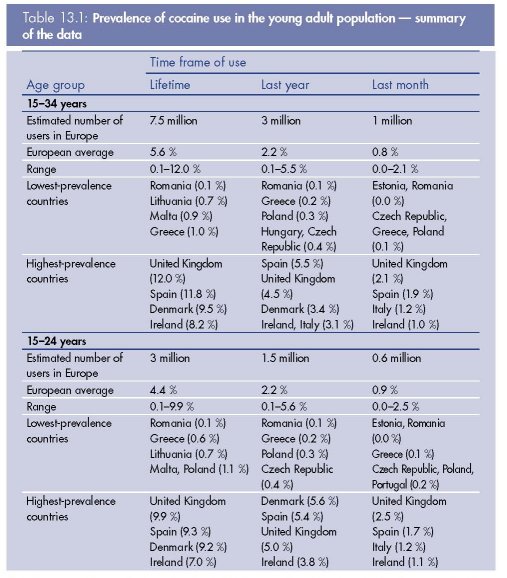
Note: European prevalence estimates are based on weighted averages from the most recent national surveys conducted
from 2001 to 2008 (mainly 2004–08), therefore they cannot be attached to a single year. The average prevalence for
Europe was computed by a weighted average according to the population of the relevant age group in each country. In
countries for which no information was available, the average EU prevalence was imputed. Population base is 133 million.
The data summarised here are available under ‘General population surveys’ in the EMCDDA 2009 statistical bulletin.
Source: EMCDDA, 2009.
Of the 4 million Europeans who used cocaine in the past year, around 3 million were young
people and young adults (EMCDDA, 2009). The prevalence of past-year cocaine use among
15- to 24-year-olds is estimated to be 2.2 %, which translates to about 1.5 million cocaine
users. In contrast to the prevalence estimates for cannabis or ecstasy use, which are highest
among the 15 to 24 age group, measures of more recent cocaine use (last year and last
month) are similar among the 15 to 24 and 25 to 34 age groups (see Table 13.1). Of the 11
countries for which it is possible to analyse trends in cocaine use between 2002 and 2007,
the proportion of 15- to 34-year-olds reporting cocaine use in the last year increased by
15 % or more in five countries (Ireland, Italy, Latvia, Portugal, United Kingdom), remained
stable in four (Germany, Spain, Slovakia, Finland) and only decreased in two countries
(Hungary, Poland).
Cocaine use is also strongly associated with alcohol use. For example, the British Crime
Survey 2007–08 found that among 16- to 24-year-olds who made nine or more visits to a
pub in the last month, 13.5 % reported using cocaine in the last year, compared to 1.7 %
among those who had not visited a pub (Hoare and Flatley, 2008). Visiting nightclubs was
also associated with higher cocaine use, as nearly 10 % of the 16- to 24-year-olds who
visited a club on four or more occasions during the last month reported using cocaine in the
last year, compared to 3.3 % among those who had not visited a club (Hoare and Flatley,
2008). Studies conducted in nightlife settings also report higher prevalence of cocaine use
among club-goers than among the general population (EMCDDA, 2007).
It is worth noting that alcohol is almost always the first drug with strong psychoactive and
mind-altering effects used by young people, and its widespread availability makes it the
main drug connected to poly-drug use among young adults, particularly in recreational
settings. Other psychoactive substances commonly referred to as ‘legal highs’ are
increasingly sold as alternatives to controlled drugs. In 2009, a snapshot study of 115
online shops located in 17 European countries showed that a range of herbal smoking
products and ‘party pills’ containing legal alternatives to controlled drugs were being sold
(EMCDDA, 2009).
Health and other harms
It is now widely acknowledged that recreational drug use can be an important source of
status and recreation for young people (Henderson et al., 2007); it can not only facilitate a
shared sense of group belonging and security (Fletcher et al., 2009a), but also a sense of
being different from other groups of young people (Shildrick, 2002). However, as
recreational drug use has increased among different sections of the youth population, so has
evidence of drug-related harm and concerns about the consequences of adolescent drug use.
Although the vast majority of this increase in drug use among young people has been
attributed to the use of ‘soft’ drugs (e.g. cannabis and ecstasy), these substances still have
health risks, especially for frequent users who are most at risk of harm.
Cannabis can cause short- and long-term health problems, such as nausea, anxiety, memory
deficits, depression and respiratory problems (Hall and Solowij, 1998; MacLeod et al., 2004;
Solowij and Battisti, 2008; Hall and Fischer, 2010). Although more research is needed on the
long-term effects of adolescent cannabis use on mental health, cannabis use is also thought
to increase the risk of mental health problems, particularly among frequent users (Hall, 2006;
Moore et al., 2007) and those with a predisposition for psychosis (Henquet et al., 2005).
Regular cannabis users can also become dependent (Melrose et al., 2007).
The true extent of future mental health problems due to adolescent ecstasy use is unclear, but
young ecstasy users may be at risk of depression in later life and there is evidence that
ecstasy use may also impair cognitive functions relevant to learning (Parrott et al., 1998;
Schilt et al., 2007). Dehydration, a more immediate risk for ecstasy users, can cause loss of
consciousness, coma and even death. Furthermore, evidence from cohort studies suggests
that early initiation and frequent use of ‘soft’ drugs may be a potential pathway to more
problematic drug use in later life (Yamaguchi and Kandel, 1984; Lynskey et al., 2003;
Ferguson et al., 2006).
Cocaine use can result in dependence and/or serious mental and physical health problems,
such as depression, paranoia, and heart and respiratory problems (Emmett and Nice, 2006).
Hence, although only a small minority of young people use cocaine (NatCen and NFER,
2007; Hibell et al., 2009), their numbers are increasing in some countries in Europe, posing
an increasing public health issue.
In addition to presenting direct health risks, adolescent drug use is also associated with
accidental injury, self-harm, suicide (Charlton et al., 1993; Beautrais et al., 1999; Thomas et
al., 2007) and other ‘problem’ behaviours, such as unprotected sex, youth offending and
traffic risk behaviours (Jessor et al., 1991; Home Office, 2002; Jayakody et al., 2005; Calafat
et al., 2009). For example, a recent report by the United Kingdom Independent Advisory
Group on Sexual Health and HIV (2007) has suggested that there are strong links between
drug use, ‘binge’ drinking and sexual health risk, with similar trends in these risk behaviours.
Furthermore, although the links between crime and heroin or cocaine dependence are well
known, there is increasing evidence of links between teenage cannabis use and youth
offending (e.g. Boreham et al., 2006). This is not to say that there is necessarily a direct
causal relationship between adolescent drug use and social problems, but there is clear
evidence that they cluster together among certain groups of young people.
A typology of interventions
There have been surprisingly few attempts to synthesise the evidence relating to interventions
in European countries addressing young people’s recreational drug use. Here we adopt a
typological approach to describe and discuss responses that aim to reduce the harms
associated with young people’s recreational drug use. These include: (1) individually focused
and group-based interventions — school-based drugs education and prevention, mass
media campaigns, motivational interviewing and youth development programmes — and (2)
‘settings-based approaches’ which make changes to recreational settings, such as nightclubs,
or institutional settings, such as schools, to address the social and environmental background
of young people’s drug use.
This is not an exhaustive list of interventions in Europe that target young people’s recreational
drug use. For example, we do not discuss interventions that are directed primarily at young
people’s parents rather than young people themselves (see Petrie et al., 2007 for a review of
the evidence relating to current parenting programmes). Social policies that may impact on
macro-social — or ‘structural’ — factors, such as youth cultures, poverty or social exclusion,
that are also associated with young people’s drug use, are also not discussed, because they
rarely aim to specifically reduce the harms associated with recreational drug use. The
decriminalisation of drugs, drug classification policies, and policies and enforcement to
reduce the supply of illicit drugs and illicit sales of prescription drugs are also beyond the
scope of this chapter.
Individual and group-based approaches
School-based drugs education and prevention
In Europe, schools provide universal access to young people under 16 and are widely
recognised as a key site for drugs education and prevention interventions that aim to prevent
or delay drug use and reduce the frequency of drug use during adolescence (Evans-Whipp
et al., 2004). However, evidence from randomised controlled trials (RCTs) of classroom-based
drugs education interventions aiming to improve knowledge, develop skills and modify peer
norms suggest that the effect of these interventions on young people’s drug-use behaviour are
limited: a recent systematic review found that they can have positive effects but concluded
that these are small, inconsistent and generally not sustained (Faggiano et al., 2005). In other
words, drugs education may promote students’ ‘health literacy’ but is not sufficient on its own
for changing young people’s behaviour or reducing drug-related harms.
Faggiano and colleagues (2005) found that school-based drugs education programmes
based on a ‘comprehensive social influence approach’ and those that are delivered by other
students (rather than teachers) appear to have the most positive effects — programme
characteristics that were also associated with more positive effects in systematic reviews of
alcohol education and smoking prevention interventions in schools (Foxcroft et al., 2002;
Thomas and Perera, 2006). However, in reviewing the evidence for drug education
programmes in schools, Cahill (2007) has highlighted the difficulties of implementing
complex interventions such as peer-led programmes in school settings and suggested that
caution is also required with normative education to ensure that adolescents receive
appropriate messages.
A key challenge in Europe and elsewhere is therefore to pilot and further evaluate evidencebased
school-based drugs education and prevention interventions (Faggiano and Vigna-
Taglianti, 2008; Ringwalt et al., 2008). ‘Unplugged’ is an example of a European schoolbased
programme that employs a comprehensive social influence model. It aims to reduce
young people’s substance use via 12 interactive sessions addressing topics such as decisionmaking,
‘creative thinking’, effective communication, relationship skills, self-awareness,
empathy, coping skills and the risks associated with specific drugs (Van Der Kreeft et al.,
2009). A recent cluster RCT of the ‘Unplugged’ programme in 170 schools across seven
European countries suggested that curricula based on such a comprehensive social-influence
model are not only feasible to implement in schools in Europe, they may also reduce regular
cannabis use and delay progression to daily smoking and episodes of drunkenness
(Faggiano et al., 2008).
The ASSIST (A Stop Smoking in Schools Trial) programme in the United Kingdom provides an
example of an effective peer-led health promotion intervention that is feasible to deliver in
schools: a cluster RCT of the ASSIST programme involving 59 schools in Wales found a
significant reduction in smoking among the intervention group, including among the most
‘high risk’ groups of students (Campbell et al., 2008). The programme uses network analysis
to identify influential students and train them as peer supporters to ‘diffuse’ positive health
messages throughout the school. Researchers at the Centre for Drug Misuse Research in
Glasgow have recently piloted a peer-led drugs prevention programme based on the ASSIST
programme in two secondary schools in Scotland; this study suggested that it is feasible to
deliver cannabis and smoking education (CASE) together using this approach (Professor Mick
Bloor, personal communication). However, further research is needed to examine the effects
of this intervention on students’ drug use and drug-related harms.
Mass media campaigns
Mass media campaigns have become a popular tool among health promoters seeking to
inform young people about the risks associated with recreational drug use and/or seeking to
encourage current users to reduce their use and minimise the risk of harm. These
interventions, such as the recent United Kingdom FRANK advertising campaigns on the
mental health problems associated with recreational cannabis use (http://www.talktofrank.
com/cannabis.aspx), aim to increase the information available to young people and reframe
issues relating to young people’s recreational drug use on public health terms. These mass
media campaigns to raise awareness about the effects of drug use in the United Kingdom
have also been integrated with a ‘credible, non-judgemental and reliable’ online and
telephone drugs advice and information service for young people and their parents (Home
Office et al., 2006).
However, mass media campaigns that aim to reduce the harms associated with young
people’s recreational drug have rarely been evaluated to examine their effects on young
people’s behaviour, attitudes or intention to use drugs — and where they have, the findings
have not always been positive. A national survey to evaluate the United States Anti-Drug
Media Campaign suggested that mass media campaigns have little or no effect on changing
attitudes once young people have initiated drug use (Orwin et al., 2006), and may even
have harmful effects as those young people who were exposed to the adverts were more
likely to report cannabis use or an intention to use cannabis (Hornik et al., 2008). Similar
negative outcomes were reported in another large-scale evaluation of the Scottish cocaine
campaign ‘Know the score’: two-fifths (41 %) of respondents said that the campaign made
them more likely to find out more about cocaine and 12 % felt that the campaign had made
them more likely to experiment with cocaine (Phillips and Kinver, 2007). A meta-analysis of
evaluations of mass media campaigns to reduce smoking, drinking or drug use by Derzon
and Lipsey (2002) found that campaigns featuring messages about resistance skills appeared
to have the most harmful effects and were associated with significantly higher extent of
substance use than observed in control communities.
Flay and colleagues (1980) have suggested that the key factors to change behaviour via
mass media health promotion campaigns include: repetition of information over long time
periods, via multiple sources and at different times (including ‘prime’ or high-exposure times).
Mass media interventions also provide the opportunity to reach specific target groups within
a short timeframe (HDA, 2004). However, population-level mass media campaigns require a
significant financial investment (Hornik, 2002) and are competing in an increasingly crowded
market with a range of other information available to young people (Randolph and
Viswanath, 2004).
Brief interventions
Approaches based on early screening of young people’s drug use and brief behaviour change
interventions, such as motivational interviewing, have been rigorously evaluated in the United
Kingdom and elsewhere (Tait and Hulse, 2003; Tevyaw and Monti, 2004). Developed by Miller
and Rollnick, motivational interviewing has been defined as a ‘client-centred, directive method
for enhancing intrinsic motivation to change by exploring and resolving ambivalence’ (Miller
and Rollnick, 2002). Evidence suggests that it is feasible to deliver brief one-to-one interventions
such as motivational interviewing to young drug-users in a wide range of settings, such as
youth centres, further education colleges, general practitioners’ surgeries and ‘emergency
rooms’ (Gray et al., 2005; Martin et al., 2005; McCambridge et al., 2008), and where brief
interventions employ motivational interviewing principles they have been found to be effective
in reducing young people’s drug use (Tait and Hulse, 2003; McCambridge and Strang, 2004;
Tevyaw and Monti, 2004; Grenard et al., 2006).
Reviewing the evidence from trials of brief motivational interviewing interventions, Tevyaw
and Monti (2004) found consistent evidence that this approach can ‘result in decreases in
substance-related negative consequences and problems, decrements in substance use and
increased treatment engagement’, and these effects appear to be greatest among young
people who report the heaviest patterns of drug use and the least motivation to change prior
to intervention. Researchers have also found evidence that as little as a ‘single session’ of
motivational interviewing can significantly reduce cannabis use among heavy users and
among those young people considered to be at ‘high risk’ of progressing to more
problematic drug use (McCambridge and Strang, 2004).
However, the existing evidence suggests that, although brief interventions based on
motivational interviewing can encourage young people to moderate their drug use in the
short term, this approach is unlikely to have long-term effects on its own (McCambridge and
Strang, 2005) and may therefore need to form part of a more holistic approach to harm
reduction. Further research is also needed to examine the essential elements of motivational
interviewing interventions and their effects on developmental transitions during adolescence
(McCambridge and Strang, 2004; McCambridge et al., 2008). Furthermore, motivational
interviewing is complex and requires practitioners to develop skills and experiences over time
in order to deliver it proficiently. As such, it is likely to be difficult to replicate and evaluate
existing intervention more widely across Europe at present while is there is limited capacity to
deliver such interventions.
Youth development
Youth development programmes work with groups of teenagers and aim to promote their
personal development, self-esteem, positive aspirations and good relationships with adults in
order to reduce potentially harmful behaviours, such as drug use (Quinn, 1999). As well as
enhancing young people’s interests, skills and abilities, youth projects also have the potential
to divert young people away from drug use through engaging them in more positive sources
of recreation, and youth workers can provide credible health messages and signpost health
services. There has been considerable interest from policymakers in youth development
interventions as an alternative means of reducing young people’s drug use. For example, in
the United Kingdom youth work programmes targeted at socially disadvantaged and
‘excluded’ young people and other ‘at-risk’ groups have been supported by the Government,
including new community-based youth development projects such as the Positive Futures
initiative and the Young People’s Development Programme (Department for Education and
Skills, 2005).
Evaluations of youth development interventions targeted at vulnerable young people have
shown mixed results: although some studies report that youth development interventions have
had positive effects (Philliber et al., 2001; Michelsen et al., 2002), others suggest these
interventions may be ineffective (Grossman and Sipe, 1992) or even harmful (Palinkas et al.,
1996; Cho et al., 2005; Wiggins et al., 2009). It appears that involvement in such programmes
may result in an increase in drug use where: young people are stigmatised (or ‘labelled’) via
targeting, which further reduces their self-esteem and aspirations; and/or harmful social
network effects arise through aggregating ‘high risk’ young people together, thus introducing
young people to new drug-using peers (Bonell and Fletcher, 2008). For example, in a study
examining an intervention for high-risk high school students (Cho et al., 2005), greater
exposure to the programme predicted greater ‘high-risk peer bonding’ and more negative
outcomes, including higher prevalence of cannabis and alcohol use (Sanchez et al., 2007).
Youth development approaches are therefore likely to be most appropriate and effective where
they are delivered in universal settings to avoid the harmful ‘labelling’ and social network
effects associated with targeting ‘high risk’ youth. In the United States, after-school and
community-based youth development programmes promoting civic engagement and learning
through the principle of ‘serve and learn’ — which involves voluntary service, reflection on this
voluntary service though discussion groups, social development classes and learning support
— have been found to be effective in reducing a wide range of risky behaviours including
involvement with drugs and teenage pregnancy (Michelsen et al., 2002; Harden et al., 2009).
Where youth workers aim to target ‘high risk’ groups of young people, ‘detached’, street-based
services may be more appropriate in order to avoid the potentially harmful social network
effects associated with aggregating these young people together in youth centres, although this
needs further evaluation (Fletcher and Bonell, 2008). Examples of street-based youth projects
include the Conversas de Rua programme in Lisbon (http://www.conversasderua.org/) and the
‘Off the Streets’ community youth initiative in Derry, Northern Ireland.
Settings-based approaches
Settings-based approaches to health promotion have their roots in the World Health
Organization’s (WHO) Health for All initiative and the Ottawa Charter for Health Promotion
(WHO, 1986). The Ottawa Charter argued that health is influenced by where people ‘learn,
work, play and love’, integrated new thinking about health promotion, and heralded the start
of this new approach (Young, 2005). Key principles regarded as necessary to achieve the
status of a ‘health promoting setting’ are the creation of a healthy environment and the
integration of health promotion into the routine activities of the setting (Baric, 1993). Since the
late 1980s, health promotion interventions have been widely established, which make
changes to recreational ‘settings’, such as nightclubs, or institutional ‘settings’, such as schools,
to address the social and environmental determinants of harmful drug use.
Interventions in recreational settings
Studies of young people in Europe who attend dance music events consistently report much
higher prevalence of drug use than found in surveys of the general population (EMCDDA,
2006a). A ‘Hegemonic Recreational Nightlife Model’ has been used to understand how
recreational drug use and the settings where this takes place now govern many young people’s
weekend entertainment and social networks, and can give ‘meaning’ to their lives through
intensive participation (Calafat et al., 2003). The recreation industry thus not only supplies
services but also contributes to defining entertainment and creating the conditions in which
recreational drug use takes place. In turn, there is a wide range of risk behaviours associated
with recreational drug use in this context (e.g. violence, sexual risk, traffic risk), and these have
been found to be influenced by factors such as a ‘permissive atmosphere’ (Homel and Clark,
1994; Graham et al., 2006), overcrowding (Macintyre and Homel, 1997), overt sexual activity
(Homel et al., 2004; Graham et al., 2006) and transport habits (Calafat et al., 2009).
A wide range of interventions now aim to change the physical context and/or the social and
cultural norms of recreational settings to address the conditions and influences associated
with the most ‘habitual’ contexts for young people’s recreational drug use, such as nightlife
settings and music festivals, and the potential harms arising from use in such contexts. For
example, several organisations in Europe have launched safer nightlife guidelines. ‘Safer
dancing’ guidelines, developed in the United Kingdom, have now become an important tool
in this field. Other examples are the Safe Nightlife initiative in Holstebro, Denmark, and the
London Drug Policy Forum’s ‘Dance Till Dawn Safely’ initiative.
Safe-clubbing guidelines aim to reduce opportunities for drug-related problems to occur in
these settings and include promoting the accessibility of free water, the immediate availability
of first aid and outreach prevention work with young clubbers. Reports on the availability of
such measures, in nightclubs with sufficiently large target populations for the intervention to
be implemented, were collated by the EMCDDA in 2008 (EMCDDA, 2009). These reports
highlighted the limited availability of simple measures to prevent or reduce health risks and
drug use in European nightlife settings. For example, it was found that outreach prevention
work was provided in the majority of dance clubs in only two out of 20 European countries
(Slovenia and Lithuania), while free water was still not routinely available in nine of the 20
countries. Furthermore, while 12 countries now report having developed guidelines for
nightlife venues, only the Netherlands, Slovenia, Sweden and the United Kingdom report that
they are monitored and implemented.
The most widely implemented intervention in recreational settings is the responsible beverage
service (RBS) guidelines to support staff and managers in harm reduction strategies. A recent
systematic review, however, concluded that there is no reliable evidence that these interventions
are effective in preventing injuries or other harms (Ker and Chinnock, 2008; see also Herring et
al., 2010). Community-based approaches to responsible service may produce the largest and
most significant effects. For example, Stockholm Prevents Alcohol and Drug Problems (STAD) is
a community-based prevention programme that started in 1996 in Stockholm to promote
community mobilisation, the training of bar staff in RBS and stricter enforcement of existing
alcohol licensing and drug laws: an evaluation found a decrease in alcohol-related problems,
increased refusal to serve minors and a 29 % reduction in assaults (Wallin and Andréasson,
2005). However, large-scale community-based interventions are likely to be expensive and
need political commitment. Other factors may also limit compliance to responsible service, such
as low pay, high staff turnover and a stressful working environment, and the efficacy of such
interventions is therefore likely be greater when enforced as a statutory intervention (Ker and
Chinnok, 2008; Wallin and Andréasson, 2005).
Promising interventions that need further evaluation are glassware bans in recreational
settings (Forsyth, 2008) and the creation of collaborating guidelines between licensed
premises and accident and emergency services (Wood et al., 2008). Some nightclubs in
Europe have now incorporated a first aid service inside the premises, but we are not aware
of any evaluations of their effectiveness. Further research and effective collaboration between
health promoters, nightlife settings and the alcohol industry are likely to be crucial in
reducing the harms associated with young people’s recreational drug use. However, building
relationships across these sectors is not straightforward. ‘Codes of practice’ with the potential
of enforcement may be the most appropriate means to facilitate engagement across the
sectors (Graham, 2000). At present, there seems to be a reluctance to enforce greater
accountability through law enforcement. The Tackling Alcohol Related Street Crime (TASC)
intervention in Cardiff provides an example of a broad and multifaceted intervention
implemented largely by the police that produced reductions in violence at the relevant
premises, although further research is needed to examine the feasibility of introducing policeled
approaches in nightlife settings more generally (Maguire et al., 2003).
Finally, on-site pill testing in recreational settings has been a controversial issue for several
years and appears to be steadily less common in Europe. The main arguments against pill
testing are the limited capacity of on-site tests to accurately detect harmful substances and
that, by permitting on-site pill testing, contradictory messages are being sent out about the
risks related to both use and possession of controlled substances (EMCDDA, 2006b).
Whole-school interventions
Following the emergence of ‘settings-based approaches’ to health promotion, traditional
classroom-based drugs education programmes have gradually been accompanied by
additional strategies in schools that address more ‘upstream’ environmental, social and
cultural determinants of young people’s drug use, such as student disengagement and
truancy. The origin of this new ‘settings’ approach to health promotion in schools is attributed
to a WHO conference in 1989 which led to the publication of The Healthy School (Young
and Williams, 1989). Following this report, ‘whole-school’ approaches have received
continued support from international networks, such as the WHO, the European Network of
Health Promoting Schools (ENHPS) and the International School Health Network (ISHN)
(WHO, 1998; McCall et al., 2005).
Using cross-sectional survey data from 10 European countries, Canada and Australia,
Nutbeam and colleagues (1993) found a consistent relationship between ‘alienation’ at
secondary school and ‘abusive behaviours’, such as smoking, drinking and drug use, and
warned that ‘schools can damage your health’. Further analysis of this data suggested that
students’ perceptions of being treated fairly, school safety and teacher support were related
to substance use (Samdal et al., 1998). Three recent systematic reviews of experimental
studies of ‘whole-school health promotion interventions’, which make changes to schools’
physical environment, governance and management, policies, and/or educational and
pastoral practices, have found that these approaches appear to be ‘promising’ for reducing
a wide range of ‘risky’ health behaviours among young people (Lister-Sharpe et al., 1999;
Mukoma and Flisher, 2004; Fletcher et al., 2008). The review by Fletcher and colleagues
found that changes to the school social environment that increase student participation,
improve teacher–student relationships, promote a positive school ethos and reduce
disengagement are associated with reduced drug use. The Gatehouse Project in Australia is
one of the best-known examples (http://www.rch.org.au/gatehouseproject/).
Although various pathways may plausibly underlie school effects on drug use and drugrelated
harms, three potential pathways via which school effects on drug use may occur have
been identified: peer-group sorting and drug use as a source of identity and bonding among
students who are disconnected from the main institutional markers of status; students’ desire
to ‘fit in’ at schools perceived to be unsafe, and drug use facilitating this; and/or drug use as
a strategy to manage anxieties about schoolwork and escape unhappiness at schools lacking
effective social support systems (Fletcher et al., 2009b). This evidence further supports ‘wholeschool’
interventions to reduce drug use through: recognising students’ varied achievements
and promoting a sense of belonging; reducing bullying and aggression; and providing
additional social support for students.
Discussion
There is considerable data on the prevalence of recreational drug use among young people
in European countries, and the related adverse health and other harms. However, much of
this evidence regarding overall prevalence of young people’s drug use is gained through
school-based surveys and we cannot assume that patterns of drug use among young people
who have low school attendance and young people who have been excluded from school
will therefore be accurately captured in these surveys; there are also practical problems with
collecting reliable self-report data about students’ use of drugs in school-based surveys
(McCambridge and Strang, 2006). Street-based surveys of young people, such as the
Vancouver Youth Drug Reporting System (VCH, 2007), could therefore complement existing
monitoring systems in Europe. Nonetheless, current European surveys that monitor
prevalence and trends are well established and allow cross-national comparisons to be made
regarding young people’s drug use.
In response to public and political concerns about the harmful consequences of young people’s
drug use, a wide range of interventions have been implemented throughout Europe and
elsewhere. There is no ‘magic bullet’, and harm reduction strategies in this context will need to
encompass both universal and targeted strategies that seek to prevent or delay drug use,
reduce the frequency of drug use during adolescence, and make changes to risk environments.
Mass media campaigns may be politically important but appear to be largely ineffective (and
occasionally counter-productive). If they are to continue to play a role in informing young
people about the risks associated with recreational drug use, health promoters should design
mass media campaigns in conjunction with young people and — although it is difficult to
attribute changes in behaviour to mass media interventions — these campaigns should be
subjected to pilot trials prior to ‘roll-out’. Future mass media campaigns should also pay close
attention to providing easy access to information via the Internet and telephone advice lines.
Based on the current evidence, school-based programmes show greater promise for
preventing young people initiating drug use at a young age than mass media interventions.
Comprehensive social influence models and peer-led programmes based on the ‘diffusion of
innovations’ approach are the most promising approaches for drugs education and
prevention in schools, and thus should be piloted and evaluated more widely in Europe.
Interventions that promote a positive school ethos and reduce student disaffection and
truancy are likely to be an effective complement to these drugs education and prevention
interventions in schools. These school-level ‘settings’ interventions focusing on the more
‘upstream’ determinants of risk should also now be piloted and evaluated in Europe to
examine their potential for harm reduction.
Motivational interviewing shows considerable promise in a wide range of settings, including
among those young people with the heaviest patterns of drug use. However, motivational
interviewing is resource-intensive and where there is insufficient investment this will impact on
its potential for harm reduction. New training programmes in motivational interviewing
should therefore be considered a priority in European countries, initially to build capacity for
greater intervention in recreational contexts and among professionals working with high-risk
young people.
Youth development approaches appear to be most appropriate and effective in addition to,
rather than as an alternative to, school, such as after-school and school-holiday programmes
promoting self-esteem, positive aspirations, supportive relationships and learning through the
principle of ‘serve and learn’, which is based on volunteering in the local community. In
addition, because of its focus on working with existing peer groups (and thus its ability to avoid
the potentially harmful effects associated with centre-based youth projects), as well as its
greater reach and flexibility, detached, street-based youth work may be the most appropriate
and effective approach for targeting those young people deemed at ‘high risk’ of harm. These
approaches should be the subject of further evaluation in Europe with high-risk groups.
Perhaps of greatest concern at present is the lack of agreement and guidance about what to
do in recreational settings in Europe to reduce drug-related harm. There are few statutory
policies governing the most ‘habitual’ contexts for young people’s recreational drug use, such
as nightlife settings and music festivals, or rigorous evaluations of interventions in such
settings in Europe. Guidelines promoting the accessibility of free water, immediate availability
of first aid and outreach services have been implemented with promising effects in some (but
by no means all) European countries. These should be enforced through changing them into
laws where possible and be accompanied by additional efforts to encourage responsible
alcohol service and reduce other risky behaviours.
References
Ball, A. (2007), ‘HIV, injecting drug use and harm reduction: a public health response’, Addiction 102, pp. 684–90.
Baric, L. (1993), ‘The settings approach: implications for policy and strategy’, Journal of the Institute of Health
Education 31, pp. 17–24.
Beautrais, A. L., Joyce, P. R. and Mulder, R. T. (1999), ‘Cannabis abuse and serious suicide attempts’, Addiction,
94, pp. 1155–64.
Bonell, C. and Fletcher, A. (2008), ‘Addressing the wider determinants of problematic drug use: advantages of
whole-population over targeted interventions’, International Journal of Drug Policy 19, pp. 267–9.
Boreham, R., Fuller, E., Hills, A. and Pudney, S. (2006), The arrestee survey annual report: Oct. 2003–Sept. 2004,
England and Wales, Home Office, London.
Cahill, H. W. (2007), ‘Challenges in adopting evidence-based school drug education programmes’, Drug and
Alcohol Review 26, pp. 673–9.
Calafat, A., Fernandez, C., Juan, M., et al. (2003), Enjoying nightlife in Europe: the role of moderation, Irefrea,
Palma de Mallorca.
Calafat, A., Blay, N., Juan, M., et al. (2009), ‘Traffic risk behaviors at nightlife: drinking, taking drugs, driving,
and use of public transport by young people’, Traffic Injury Prevention 10, pp. 162–9.
Campbell, R., Starkey, F., Holliday, J., et al. (2008), ‘An informal school-based peer-led intervention for smoking
prevention in adolescence (ASSIST): a cluster randomised trial’, Lancet 371, pp. 1595–602.
Charlton, J., Kelly, S. and Dunnell, K. (1993), ‘Suicide deaths in England and Wales: trends in factors associated
with suicide deaths’, Population Trends 7, pp. 34–42.
Cho, H., Hallfors, D. D. and Sanchez, V. (2005), ‘Evaluation of a high school peer group intervention for at-risk
youth’, Journal of Abnormal Child Psychology 33, pp. 363–74.
Department for Education and Skills (2005), Every child matters: change for children, young people and drugs, Her
Majesty’s Stationery Office, London.
Derzon, J. H. and Lipsey, M. W. (2002), ‘A meta-analysis of the effectiveness of mass-communication for changing
substance-use knowledge, attitudes and behaviour’, in Crano, W. D. and Burgoon, M. (eds), Mass media and drug
prevention: classic and contemporary theories and research, Lawrence Erlbaum Associates, Matwah.
Emmett, D. and Nice, G. (2006), Understanding street drugs, Jessica Kingsley Publishers, London.
EMCDDA (European Monitoring Centre for Drugs and Drug Addiction) (2002), Recreational drug use: a key EU
challenge, Drugs in focus, European Monitoring Centre for Drugs and Drug Addiction, Lisbon.
EMCDDA (2006a), Annual report 2006: the state of the drugs problem in Europe, European Monitoring Centre for
Drugs and Drug Addiction, Lisbon.
EMCDDA (2006b), Developments in drug use within recreational settings, European Monitoring Centre for Drugs
and Drug Addiction, Lisbon.
EMCDDA (2007), Cocaine and crack cocaine: a growing public health issue, European Monitoring Centre for
Drugs and Drug Addiction, Lisbon.
EMCDDA (2009), Annual report 2009: the state of the drugs problem in Europe, European Monitoring Centre for
Drugs and Drug Addiction, Lisbon.
Evans-Whipp, T., Beyers, J. M., Lloyd, S., et al. (2004), ‘A review of school drug polices and their impact on
youth substance use’, Health Promotion International 19, pp. 227–34.
Faggiano, F. and Vigna-Taglianti, F. D. (2008), ‘Drugs, illicit — primary prevention strategies’, International
Encyclopaedia of Public Health 2, pp. 249–65.
Faggiano, F., Vigna-Taglianti, F. D., Versino, E., et al. (2005), ‘School-based prevention for illegal drugs use’,
Cochrane Database of Systematic Reviews 2, Art. No. CD003020.
Faggiano, F., Galanti, M. R., Bohrn, K., et al. (2008), ‘The effectiveness of a school-based substance abuse
prevention program: EU–Dap cluster randomised controlled trial’, Preventive Medicine 47, pp. 537–43.
Ferguson, D. M., Boden, J. M. and Horwood, L. J. (2006), ‘Cannabis use and other illicit drug use: testing the
cannabis gateway hypothesis’, Addiction 101, pp. 556–69.
Flay, B. R., DiTecco, D. and Schlegel, R. P. (1980), ‘Mass media in health promotion: an analysis extended
information-processing model’, Health Education and Behavior 7, pp. 127–47.
Fletcher, A. and Bonell, C. (2008), ‘Detaching youth work to reduce drug and alcohol-related harm’, Public Policy
Research 15, pp. 217–23.
Fletcher, A., Bonell, C. and Hargreaves, J. (2008), ‘School effects on young people’s drug use: a systematic
review of intervention and observational studies’, Journal of Adolescent Health 42, pp. 209–20.
Fletcher, A., Bonell, C., Sorhaindo, A. and Rhodes, T. (2009a), ‘Cannabis use and “safe” identities in an innercity
school risk environment’, International Journal of Drug Policy 20, pp. 244–50.
Fletcher, A., Bonell, C., Sorhaindo, A. and Strange, V. (2009b), ‘How might schools influence young people’s drug
use? Development of theory from qualitative case-study research’, Journal of Adolescent Health 45, pp. 126–32.
Forsyth, A. J. M. (2008), ‘Banning glassware from nightclubs in Glasgow (Scotland): observed impacts,
compliance and patrons views’, Alcohol and Alcoholism 43, pp. 111–17.
Foxcroft, D. R., Ireland, D., Lowe, G. and Breen, R. (2002), ‘Primary prevention for alcohol misuse in young
people’, Cochrane Database of Systematic Reviews 3, Art. No. CD003024.
Graham, K. (2000), ‘Preventive interventions for on-premise drinking: a promising but under researched area of
prevention’, Contemporary Drug Problems 27, pp. 593–668.
Graham, K., Bernards, S., Osgood, D. W. and Wells, S. (2006), ‘Bad nights or bad bars? Multi-level analysis of
environmental predictors of aggression in late-night large-capacity bars and clubs’, Addiction 101, pp. 1569–80.
Gray, E., McCambridge, J. and Strang, J. (2005), ‘The effectiveness of motivational interviewing delivered by
youth workers in reducing drinking, cigarette and cannabis smoking among young people: quasi-experimental
pilot study’, Alcohol and Alcoholism 40, pp. 535–9.
Grenard, J. L., Ames, S. L., Pentz, M. A. and Sussman, S. (2006), ‘Motivational interviewing with adolescents and
young adults for drug-related problems’, International Journal of Adolescent Medicine and Health 18, pp. 53–67.
Grossman, J. B. and Sipe, C. L. (1992), Report on the long-term impacts (STEP program), Public/Private Ventures,
Philadelphia.
Hall, W. (2006), ‘The mental health risks of adolescent cannabis use’, PLoS Medicine 3, p. e39.
Hall, W. and Fischer, B. (2010), ‘Harm reduction policies for cannabis’, in European Monitoring Centre for Drugs
and Drug Addiction (EMCDDA), Harm reduction: evidence, impacts and challenges, Rhodes, T. and Hedrich, D.
(eds), Scientific Monograph Series No. 10, Publications Office of the European Union, Luxembourg.
Hall, W. and Solowij, N. (1998), ‘Adverse effects of cannabis’, Lancet 352, pp. 1611–16.
Harden, A., Brunton, G., Fletcher, A. and Oakley, A. (2009), ‘Teenage pregnancy and social disadvantage:
systematic review integrating controlled trials and qualitative studies’, BMJ 339, b4254.
HDA (Health Development Agency) (2004), The effectiveness of public health campaigns, Health Development
Agency, London.
Henderson, S., Holland, J., McGrellis, S., Sharpe, S. and Thompson, R. (2007), Inventing adulthoods: a
biographical approach to youth transitions, SAGE, London.
Henquet, C., Krabbendam, L., Spauwen, J., et al. (2005), ‘Prospective cohort study of cannabis use,
predisposition for psychosis, and psychotic symptoms in young people’, BMJ 330, pp. 11–16.
Herring, R., Thom, B., Beccaria, F., Kolind, T. and Moskalewicz, J. (2010), ‘Alcohol harm reduction in Europe’, in
European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), Harm reduction: evidence, impacts and
challenges, Rhodes, T. and Hedrich, D. (eds), Scientific Monograph Series No. 10, Publications Office of the
European Union, Luxembourg.
Hibell, B., Anderson, B., Bjarnsson, T., et al. (2004), The ESPAD report 2003: alcohol and other drug use among
students in 35 countries, The Swedish Council for Information on Alcohol and Other Drugs, Stockholm.
Hibell, B., Guttormsson, U., Ahlström, S., et al. (2009), The 2007 ESPAD report: substance use among students in 35
European countries, The Swedish Council for Information on Alcohol and Other Drugs, Stockholm.
Hoare, J. and Flatley, J. (2008), Drug misuse declared: findings from the 2007/08 British Crime Survey, Her
Majesty’s Stationery Office, London.
Home Office (2002), Updated national drugs strategy, Her Majesty’s Stationery Office, London.
Home Office, Department of Health, Department for Education and Skills (2006), FRANK review, Her Majesty’s
Stationery Office, London.
Homel, R. and Clark, J. (1994), ‘The prediction and prevention of violence in pubs and clubs’, Crime Prevention
Studies 3, pp. 1–46.
Homel, R., Carvolth, R., Hauritz, M., McIlwain, G. and Teague, R. (2004), ‘Making licensed venues safer for
patrons: what environmental factors should be the focus of interventions?’, Drug and Alcohol Review 23, pp. 19–29.
Hornik, R. (2002), ‘Public health communication: making sense of contradictory evidence’, in Hornik, R., Public
health communication: evidence for behavior change, Erlbaum, Mahwah.
Hornik, R., Jacobsohn, L., Orwin, R., Piesse, A., and Kalton, G. (2008), ‘Effects of the National Youth Anti-Drug
Media Campaign on youths’, American Journal of Public Health 98, pp. 2229–36.
Independent Advisory Group on Sexual Health and HIV (2007), Sex, drugs, alcohol and young people: a review of
the impact drugs and alcohol has on the sexual behaviour of young people, Department of Health, London.
Jayakody, A., Sinha, S., Curtis, K., et al. (2005), Smoking, drinking, drug use, mental health and sexual behaviour
in young people in East London, Department of Health/Teenage Pregnancy Unit, London.
Jessor, R., Donovan, J. E. and Costa, F. M. (1991), Beyond adolescence: problem behaviour and young adult
development, Cambridge University Press, Cambridge.
Ker, K. and Chinnock, P. (2008), ‘Interventions in the alcohol server setting for preventing injuries’, Cochrane
Database of Systematic Reviews 3, Art. No. CD005244.
Kimber, J., Palmateer, N., Hutchinson, S., et al. (2010), ‘Harm reduction among injecting drug users: evidence of
effectiveness’, in European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), Harm reduction:
evidence, impacts and challenges, Rhodes, T. and Hedrich, D. (eds), Scientific Monograph Series No. 10,
Publications Office of the European Union, Luxembourg.
Lister-Sharp, D., Chapman, S., Stewart-Brown, S. and Sowden, A. (1999), ‘Health promoting schools and health
promotion in schools: two systematic reviews’, Health Technology Assessment 3 (22), pp. 1–207.
Lynskey, M. T., Heath, A. C., Bucholz, K. K., et al. (2003), ‘Escalation of drug use in early onset cannabis users vs
co-twin controls’, JAMA 289, pp. 427–33.
McCall, D. S., Rootman, I. and Bayley, D. (2005), ‘International school health network: an informal network for
advocacy and knowledge exchange’, Promotion and Exchange 12, pp. 173–7.
McCambridge, J. and Strang, J. (2004), ‘The efficacy of single-session motivational interviewing in reducing drug
consumption and perceptions of drug-related risk and harm among young people’, Addiction 99, pp. 39–52.
McCambridge, J. and Strang, J. (2005), ‘Deterioration over time in effect of motivational interviewing in reducing
drug consumption and related risk among young people’, Addiction 100, pp. 470–8.
McCambridge, J. and Strang, J. (2006), ‘The reliability of drug use collected in the classroom: what is the
problem, why does it matter and how should it be approached?’, Drug and Alcohol Review 25, pp. 413–18.
McCambridge, J., Slym, R. L. and Strang, J. (2008), ‘Randomized controlled trial of motivational interviewing
compared with drug information and advice for early information among young cannabis users’, Addiction 103,
pp. 1819–20.
Macintyre, S. and Homel, R. (1997), ‘Danger on the dance floor: a study of interior design, crowding and
aggression in nightclubs’, in Homel, R. (ed.) Policing for prevention: reducing crime, public intoxication and injury,
Criminal Justice Press, New York.
MacLeod, J., Oakes, R., Oppenkowski, T., et al. (2004), ‘How strong is the evidence that illicit drug use by young
people is an important cause of psychological or social harm? Methodological and policy implications of a
systematic review of longitudinal, general population studies’, Lancet 363, pp. 1579–88.
Maguire, M., Morgan, R. and Nettleton, H. (2003), Reducing alcohol-related violence and disorder: an evaluation
of the ‘TASC’ project, Home Office, London.
Martin, G., Copeland, J. and Swift, W. (2005), ‘The adolescent cannabis check-up: feasibility of a brief
intervention for cannabis users’, Journal of Substance Abuse Treatment 29, pp. 207–13.
Melrose, M., Turner, P., Pitts, J. and Barrett, D. (2007), The impact of heavy cannabis use on young people:
vulnerability and youth transitions, Joseph Rowntree Foundation, York.
Michelsen, E., Zaff, J. F. and Hair, E. C. (2002), A civic engagement program and youth development: a synthesis,
Child Trends, Edna McConnell Clark Foundation, New York.
Miller, W. R. and Rollnick, S. (2002), Motivational interviewing: preparing people for change, Guildford Press, London.
Moore, T. H. M., Zammit, S., Lingford-Hughes, A., et al. (2007), ‘Cannabis use and risk of psychotic or affective
mental health outcomes: a systematic review’, Lancet 370, pp. 319–28.
Mukoma, W. and Flisher, A. J. (2004), ‘Evaluations of health promoting schools: a review of nine studies’, Health
Promotion International 19, pp. 357–68.
NatCen and NFER (2007), Smoking, drinking and drug use among young people in England in 2006: headline
figure, NHS Information Centre, London.
Nutbeam, D., Smith, C., Moore, L. and Bauman, A. (1993), ‘Warning! Schools can damage your health: alienation
from school and its impact on health behaviour’, Journal of Paediatric and Child Health 29, pp. S25–S30.
Orwin, R., Cadell, D., Chu, A., et al. (2006), Evaluation of the National Youth Anti-Drug Media Campaign, NIDA,
Rockville.
Palinkas, L. A., Atkins, C. J., Miller, C. and Ferreira, D. (1996), ‘Social skills training for drug prevention in highrisk
female adolescents’, Preventive Medicine 25, pp. 692–701.
Parrott, A. C., Lees, A., Garnham, N. J., Jones, M. and Wesnes, K. (1998), ‘Cognitive performance in
recreational users of MDMA or “ecstasy”: evidence for memory deficits’, Journal of Psychopharmacology 12, pp.
79–83.
Petrie, J., Bunn, F. and Byrne, G. (2007), ‘Parenting programmes for preventing tobacco, alcohol or drugs misuse
in children <18: a systematic review’, Health Education Research 22, pp. 177–91.
Philliber, S., Williams, K., Herrling, S. and West, E. (2001), ‘Preventing pregnancy and improving health care
access among teenagers: an evaluation of the Children’s Aid Society-Carrera Program’, Perspectives on Sexual
and Reproductive Health 34, pp. 244–51.
Phillips, R. and Kinver, A. (2007), Know the score: cocaine wave 4 — 2006/07 post-campaign evaluation, Scottish
Executive Research Group, Edinburgh.
Quinn, J. (1999), ‘Where need meets opportunity: youth development programs for early teens’, The Future of
Children 9, pp. 96–116.
Randolph, W. and Viswanath, K. (2004), ‘Lessons learned from public health mass media campaigns: marketing
health in a crowded media world’, Annual Review of Public Health 25, pp. 419–37.
Reynaud-Maurupt, C., Chaker, S., Claverie, O., et al. (2007), A Pratiques et opinions liées aux usages des
substances psychoactives dans l’espace festif «musiques électroniques», TRENDS, Observatoire Français des Drogues
et des Toxicodependences.
Ringwalt, C., Vincus, A. A., Hanley, S., et al. (2008), ‘The prevalence of evidence-based drug use prevention
curricula in U.S. middle schools in 2005’, Prevention Science 9, pp. 276–87.
Samdal, O., Nutbeam, D., Wold, B. and Kannas, L. (1998), ‘Achieving health and educational goals through
school: a study of the importance of the school climate and the student’s satisfaction with school’, Health
Education Research: Theory and Practice 13, pp. 383–97.
Sánchez, V., Steckler, A., Nitirat, P., et al. (2007), ‘Fidelity of implementation in a treatment effectiveness trial of
Reconnecting Youth’, Health Education Research 22, pp. 95–107.
Schilt, T., Maartje, M., de Win, M. L., et al. (2007), ‘Cognition in novice ecstasy users with minimal exposure to
other dugs: a prospective cohort study’, Archives of General Psychiatry 64, pp. 728–36.
Shildrick, T. (2002), ‘Young people, illicit drug use and the question of normalization’, Journal of Youth Studies 5,
pp. 35–48.
Solowij, N. and Battisti, R. (2008), ‘The chronic effects of cannabis on memory in human: a review’, Current Drug
Abuse Reviews 1, pp. 81–98.
Tait, R. J. and Hulse, G. K. (2003), ‘A systematic review of the effectiveness of brief interventions with substance
using adolescents by type of drug’, Drug and Alcohol Review 22, pp. 337–46.
Tevyaw, T. O. and Monti, P. M. (2004), ‘Motivational enhancement and other brief interventions for adolescent
substance use: foundations, applications and evaluations’, Addiction 99, pp. 63–75.
Thomas, J., Kavanagh, J., Tucker, H., et al. (2007), Accidental injury, risk-taking behaviour and the social
circumstances in which young people (aged 12–24) live: a systematic review, EPPI-Centre, London.
Thomas, R. E. and Perera, R. (2006), ‘School-based programmes for preventing smoking’, Cochrane Database of
Systematic Reviews 3, Art. No. CD001293.
Van Der Kreeft, P., Wiborg, G., Galanti, M. R., et al. (2009), ‘“Unplugged”: a new European school programme
against substance abuse’, Drugs: education, prevention and policy 16, pp. 167–81.
VCH (Vancouver Coastal Health) (2007), 2006 Vancouver youth drug reporting system: first results, Vancouver
Coastal Health Authority, Vancouver.
Wallin, E. and Andréasson, S. (2005), ‘Effects of a community action program on problems related to alcohol
consumption at licensed premises’, in Stockwell, T., Gruenewald, P. J., Toumbourou, J. W. and Loxley, W. (eds)
Preventing harmful substance use: the evidence base for policy and practice, John Wiley, West Sussex.
Wiggins, M., Bonell, C., Sawtell, M., et al. (2009), ‘Health outcomes of a youth-development programme in
England: prospective matched comparison study’, British Medical Journal 339, pp. 2534–43.
Wood, D. W., Greene, S. L., Alldus, G., et al. (2008), ‘Improvement in the pre-hospital care of recreational drug
users through the development of club specific ambulance referral guidelines’, Substance Abuse Treatment,
Prevention and Policy 3, p. 14.
WHO (World Health Organization) (1986), The Ottawa Charter for Health Promotion, World Health Organization,
Copenhagen.
WHO (1998), HEALTH21: an introduction to the Health For All policy framework for the WHO European Region
(European Health for All Series No. 5), World Health Organization, Copenhagen.
Yamaguchi, K. and Kandel, D. B. (1984), ‘Patterns of drug use from adolescence to young adulthood: predictors
of progression’, American Journal of Public Health 74, pp. 673–81.
Young, I. (2005), ‘Health promotion in schools: a historical perspective’, Promotion and Education 12, pp. 112–17.
Young, I. and Williams, T. (1989), The healthy school, Scottish Health Education Group, Edinburgh.
| < Prev | Next > |
|---|