| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 204 |
| Yesterday: | 251 |
| This Week: | 204 |
| Last Week: | 2221 |
| This Month: | 4792 |
| Last Month: | 6796 |
| Total: | 129391 |
3 CHALLENGES AND CHOICES FOR VICTORIA
 |
|  |
| 
| Reports - Drugs and our Community |
Drug Abuse
3 CHALLENGES AND CHOICES FOR VICTORIA
3.1 Introduction
The significant information and facts about illicit drugs that have informed Council's investigations are outlined in chapter 2.
Council's terms of reference required it to provide the State Government with recommendations regarding the response that should be made to illicit drug use in the community. Council has reached conclusions about the most appropriate strategy, and this chapter outlines the major issues considered and the rationale for Council's recommendations.
As a result of its investigations, Council has many significant concerns about illicit drug use in Victoria. These concerns focus on the harmful effects that drugs can have on the users, their families, friends and the community. More broadly, the Council is concerned that as a community we have a poor understanding of the impact that drugs have on society and the mixed consequences that their legal status generate.
The drugs under consideration in this inquiry are illegal. Licit drugs are available but are subject to varying levels of regulation and restriction. The differing legal response to drugs is a result of complex social and political forces not a statement about the intrinsic status of these drugs. The community is increasingly aware of the risks of misuse of drugs and has accepted greater regulation when dangers are clear. The section of this chapter on the law outlines and assesses a range of legal options.
Reducing drug use and misuse is critical in the light of Council's concerns about the impact of drugs. Prohibition can contribute by containing supply and reducing demand. A wide range of other strategies also prevent use and misuse and deserve attention. Important among these options are education and information strategies. In this area, Victoria is well placed because of its successful health promotion and education strategies, particularly in relation to alcohol and tobacco.
Providing support and treatment to people with serious drug use problems may prevent the development of further problems and will, in some instances, reduce use. Effective support and treatment must be flexible to respond to the diverse needs and situations of drug users. Treatment services need to focus on those with serious problems, and to respond to the harms produced and the context in which misuse occurs.
Since 1985, and particularly since effective responses were developed to HIV/AIDS, Australia has pursued a drug policy goal of harm minimisation. Council believes available evidence lends strong support to current Victorian and Australian approaches. None of the evidence received by Council has argued that there is a set of policies or strategies capable of eliminating drug use from our society in the foreseeable future. On the contrary, considerable concern has been expressed about the social causes of drug use and the likelihood that trends will be towards increased rather than decreased use.
Victoria's response to illicit drugs requires clear objectives that enable evaluation of existing activity and assessment of the likely impact of alternative approaches. The objectives need to be framed in the knowledge that the health consequences of misuse are substantial and that any law enforcement, prevention and treatment approach can have positive and unintended negative consequences.
Council believes the objectives for Victoria's response to drugs should be:
• Minimising the harms caused by the misuse of psychoactive drugs.
• Minimising the use of psychoactive drugs.
Chapter 2 provided a brief description of what is meant by harm minimisation (2.4). The overall objectives through which minimisation of drug-related harms are to be achieved have been spelt out by the National Campaign Against Drug Abuse (NCADA—now the National Drug Strategy) as:
• Promoting greater awareness and participation by the Australian community in confronting the problems of drug abuse.
• Achieving conditions and promoting attitudes whereby the use of illegal drugs is less attractive and a more responsible attitude exists toward those drugs and substances which are both legal and readily available.
• Improving both the quantity and quality of service provided for the casualties of drug abuse.
• Directing firm and effective law enforcement efforts at combating drug trafficking, with particular attention to those who control, direct and finance such activities.
• Supporting international efforts to control the production and distribution of illegal drugs.
• Seeking to maintain, as far as possible, a common approach throughout Australia to the control of drug use and abuse.
The Council had eleven weeks to conduct its inquiries. It has had the benefit of input from written submissions, public hearings, specialist hearings and discussions with experts from Australia and overseas. Approaches that will improve Victoria's approach to illicit drugs have been distilled from these extensive and generous contributions.
Material presented in this report raises a wide range of policy and operational issues. While Council has developed a strategy that underpins its recommendations, it acknowledges that many matters require further consideration, informed public debate and careful reform.
Council has attempted to develop an approach to Victoria's drug problems that, above all else, minimises the harm caused by misuse. This chapter provides the building blocks that give substance to Council's aspirations.
3.2 Current Knowledge
Council heard many inaccurate, false, and misleading assertions during its investigations. Illicit drugs and their effect on the community, and especially on the young, seem to promote views that are not always well grounded in factual information. This tendency is not confined to the general public as many people claiming to be expert in the area of illicit drugs are not always well-informed.
It is likely that the lack of well-informed public debate about illicit drugs is in part due to the fear they inspire in the community, their low prevalence relative to other drugs such as alcohol and tobacco and a lack of concerted public education.
Community understanding of the consequences of alcohol and tobacco misuse is relatively high. This level of understanding probably results from the extensive public education efforts made in recent years. The same does not exist for illicit drugs. While it is fortunate that use of illicit drugs, other than cannabis, is not widespread, efforts to provide the community with information have been limited, partly because of their illegal status. Prohibition has not helped to engage the community in efforts to reduce the harms of illicit drugs or reduce overall usage.
There are many important gaps in the data required to confidently formulate policy, design programs, and monitor service effectiveness. This has affected the shape of proposals put by Council. Qualifications have been placed on much of the data included in chapter 2. Examples of problems are:
• Information on the level of use, particularly dependent and problematic use, is limited and almost certainly understates the position. The data is collected through small-scale household surveys (National and Victorian Household Surveys). Such surveys, because of the nature of the sample, are likely to underestimate the numbers using illicit drugs (Sutton et al, 1995).
- Very few of the preventive and educational initiatives that have been undertaken have been subject to critical evaluation. Some of the completed evaluations were not available to Council as they were regarded as confidential by the organisations that commissioned the work. Evaluations that can be used to predict future behaviours are difficult and costly to conduct. Results are sometimes not available for years, by which time most programs have already changed. This limits the applicability of the results.
• There are gaps and inadequacies in the international data that limit comparisons and analysis (Reuband, 1995). This includes any systematic analysis of the impact of various legislative regimes.
- Few evaluations of treatment services address illicit drug use in any substantive or authoritative manner. Those that exist are equivocal about the effectiveness of various service types or lack of consideration of costs (Pead, 1996).
• Treatment data to describe the patterns of use of services, and the clients of these services, have been inconsistent and unreliable.
- Data gathered by police, the courts and corrections systems are often not comparable, nor is it easy to integrate the data for purposes of evaluation or research. There is virtually no way to track a person's movement through the systems or to assess the impact of the process. Counting methods and definitions constrain comparisons and reliance on longitudinal data.
• Information sharing is not common across services and systems, with data often collected for different purposes and in different formats.
• Researching behaviours that are illegal is difficult. Users are understandably reticent about participating in research and providing reliable answers. Information which includes admissions of illegal activity poses ethical and possible legal impediments to the conduct of useful research since there can be no guarantee of confidentiality.
In this context, advice about reform options should be cautious. Council has heard on several occasions about the risk of 'unintended consequences' of action in this area (Wardlaw, oral submission 1995; Sutton, oral submission, 1996). This is an area where the consequences of action are significant, and where public support and understanding are important. Uncertainty about the consequences of reform and the level of support for any policy option indicates that an incremental and carefully monitored approach is required. Specific action will be required to engage and inform the community, and to better inform policy and program design and operational practice.
Confident policy making and program implementation in this area will require:
• A broadly based research agenda involving collaboration between the Commonwealth, states, academic and service organisations. Research on the impact of various policy initiatives and comparisons across jurisdictions is a potentially significant source of data for monitoring and future planning. It is important that research is initiated and co-coordinated in a national context although there are matters which require research support directly at state level. Commonwealth Government support for drug and alcohol research through two national research centres and an annual grant program has generated important information. Similarly, the State Government has supported some research and has established Turning Point Alcohol and Drug Centre. It has been funded to undertake research and provide clinical services and training. There remain large areas where research could have rapid and direct benefit. Council wants to encourage further research and, to this end, urges ongoing and enhanced support from the National Research Into Drug Abuse program. While integrated funding through bodies such as the National Health and Medical Research Council should also be encouraged, current specific targeted funding remains appropriate.
• Consistent databases across the State Government agencies that have responsibilities in this area. As noted earlier, some data systems within police, courts and correctional services are incompatible. A project to remedy these problems is underway. The Department of Health and Community Services is developing a new database designed to monitor the performance of treatment services. The Coroner maintains a database that is also likely to undergo development as part of a national initiative. Agreement to common definitions, core data and system compatibility is a prerequisite to improving the certainty and confidence of future decision making. Council believes that poor program design and management difficulties often result from inconsistency and gaps in data systems.
• Introduction of local early warning/monitoring systems. Many effective responses to illicit drug use need to operate at the local or street level. A particular need is early warning about changes in the types of drugs and patterns of use in different parts of Victoria. At this stage there are no structures designed to support and coordinate action in local areas, communicate with users, and develop relevant local strategies that minimise harms. A local early warning information system would also provide baseline data that could be linked to broader data systems and then reported back to local areas for comparative purposes. This matter is discussed further in sections on support and treatment and infrastructure.
• Evaluation of the effectiveness of programs. Victoria spends some $100 million annually in law enforcement, education and treatment resulting from illicit drug use. The investigation conducted by Council demonstrates that, in most areas, these funds are applied without the benefit of a strategic framework based on current knowledge about what works in varying situations. The introduction of clear outcome indicators and integrated evaluation processes would provide significant improvements to the current situation. There is a strong reason to believe that targeted evaluations could pay significant dividends in better focused and more effective service provision.
3.3 Demand and Supply Trends
Assessment of the existing and projected scale and patterns of drug supply and demand was an important baseline for Council's deliberations. A wide range of data and perspectives was provided through submissions, consultations and expert hearings.
Key issues raised relating to demand were as follows:
• Our community accepts, and in some cases values, drug use. Alcohol is a central part of many people’s lives. Medicinal drugs are widely used and vital to the health of our community. They are sometimes misused. Illicit drugs are currently used for their psychoactive properties, but potentially some could be used for medicinal purposes (for example, cannabis and heroin).
• Defining some drugs as ‘illegal’ and ‘demonising’ the users has not eliminated their use. Illegal drugs are used by tens of thousands of Victorians. In excess of 30 per cent of our community has used an illicit drug at some time (see chapter 2). These people come from all walks of life and all parts of our State. Some users suffer serious health or other problems as a result of their drug use.
• There is some evidence that problematic and harmful drug use most often occurs where people are vulnerable or lack self-esteem (McAllister et al., 1991). The illegal status of the drugs and the stigma attached to users further entrenches their marginalisation. Provision of information, support and treatment is made more difficult in these circumstances.
• There are potentially serious health consequences that arise from misuse of illicit drugs (table 10). The level and nature of the consequences varies between drugs and is, to some degree, dependent upon the circumstances of their use.
• Use of the major illicit drugs has a direct effect on a very small percentage of the population. However, compared to other countries, the rate of intravenous use of heroin and amphetamines in Australia and Victoria is high and consequently is a problem for users and their associates (see section 2.1.5).
• Data from the National Drug Household Surveys and the Victorian Drug Household Surveys does not indicate that there has been a significant increase in the proportion of people acknowledging use of illicit drugs between 1991 and 1995. The data does, however, suggest that the overall proportion of 18–24 year olds admitting to using illicit drugs has increased slightly from 1993 to 1995. In terms of specific drugs, increases have been recorded for marijuana, amphetamines, hallucinogens and cocaine. Usage rates for other illicit drugs have remained stable or declined.
• The difficulty with extrapolating from this information is that household surveys, due to their nature, are less reliable in obtaining information on highly stigmatised patterns of drug use, such as dependence or intravenous drug use. In particular, they often under-represent high-risk groups such as marginal populations (Pompidou Group, 1994).
• Estimates from the recent review of methadone treatment suggest that there has been a significant increase in number of regular and irregular heroin users in Australia. This review suggests that between 1986 and 1990 there was a 73 per cent increase in the number of regular users, and a 51 per cent increase in the number of irregular users (section 2.1.4). Increasing deaths that appear to be related to using a mix of substances, including alcohol and benzodiazepines, do indicate greater misuse and are a sign of a growing problem.
• Variations in reported prevalence rates make it difficult to estimate the impact increased availability of illicit drugs would have in Victoria. Notwithstanding the difficulties associated with interpreting the available data, a number of comments can be made:
– Males are more likely to use illicit drugs than females, although evidence put to Council suggests that amphetamine use is becoming popular among young women.
– Young males in particular form a large proportion of the drug using population.
– There appear to be lower rates of illicit drug use among employed and married people.
– Prison populations show a high rate of drug use.
Designer drugs, including Ecstasy, appear to be increasingly available. While these are currently at low levels and used among small sub-groups, it is possible that this class of drugs will be increasingly available in the future. It is difficult for Council to predict the future demand for these drugs and it is impossible to predict the harms of barely known substances. It was suggested to Council that increasing interest in quite specific psychoactive effects might contribute to increased demand for this group of drugs.
Key issues raised with Council relating to supply were:
• Global production in illicit drugs appears to be increasing and, despite significant international cooperation, international supply of illicit drugs will continue to grow, possibly at an increasing rate.
• Although not certain, it seems inevitable that some of the increased supply will reach Australia. It is, however, unclear whether increased supply will contribute directly to overall demand. Increased supply can, and almost certainly will, lower the price of some drugs but the consequences of this are hard to predict.
• The Australian Bureau of Criminal Intelligence suggests that increased supply may not have a significant impact in Australia. Heroin is currently widely available throughout Australia at high purity levels and reduced prices, suggesting that sufficient quantities are being supplied to the market.
• Law enforcement agencies throughout Australia have reported that the harder illicit drugs and cannabis were generally readily available throughout 1994.
• Occasional price fluctuations and temporary shortages may indicate either a disruption in the supply or an increase in demand for specific drugs (ABCI, 1995).
• In the case of shortages, when supplies of one drug are limited, there is often a shift to other drugs. There is some evidence to suggest that increased seizures and intensified enforcement efforts can temporarily interrupt established patterns of drug use and sources of supply. This may have the effect of moving users to substitutes or to poly-drug use.
• It is difficult to argue that the quantities of drugs seized are directly proportional to the supply of drugs. Seizure rates are estimated to be low, between 3 to 10 per cent, and seem to exert little influence on heroin price, purity or availability (Weatherburn and Lind, 1995).
During its deliberations the Council was alerted to the problem of inadequate data on illicit drug production.
The United Nations Economic and Social Council comments in its 1995 interim report, Economic and Social Consequences of Drug Abuse and Illicit Trafficking, that:
‘Assessing the economic and social consequences of illicit drug abuse and trafficking implies, first that some measure of the magnitude of the problem is available, and secondly, that there is some conceptual clarity about the nature of the consequences themselves. Estimates of the extent of illicit drug production, distribution and consumption vary enormously, and are often contingent upon the methodology and political orientation of the observer’.
The UN report, while acknowledging that there are no universally accepted figures, supports the view that on the global aggregate, illicit drug production is expanding. This is consistent with advice received by Council from a number of national and international experts (Wardlaw, oral submission, 1995).
The overall relationship between price and escalating demand is not clear. There is a question as to whether the consumption of illicit drugs, like other goods and services, decreases in response to rising prices and increases in response to falling prices. A number of studies suggest that, although small, price elasticities do exist. However, the addition of another variable, such as a successful preventive education campaign, may reduce demand and thereby cause prices to fall, without the falling prices
resulting in more consumption (UN Economic and Social Council, 1995).
On the basis of evidence available to it, Council has concluded that greater emphasis should now be placed on measures to reduce demand for drugs (such as education and health promotion) while maintaining law enforcement as an important control on supply.
Council does not condone drug taking. Nevertheless, it recognises that there will be those who, through ignorance, or other reasons, will misuse drugs whatever the consequences. The major goal of drug policy must be to ensure that people do not take drugs or if they do, that it occurs in ways that minimises the harms caused.
For people who use drugs, information and services aimed at reducing risks should be provided because this may save lives. Information provision should include unambiguous messages that abstinence from drugs is the only totally risk-free option.
Council does not believe that focusing on prevention of use and misuse represents an easy or soft option. Prevention requires multiple approaches and difficult decisions regarding targeting, and the integration of effort across the agencies involved. Minimising unintended consequences requires careful planning and implementation.
Harm reduction as a policy accepts that people use drugs on occasions. The challenge for services which come into contact with drug users is to minimise the harms associated with misuse.
Council’s framework to deal with drug availability, drug use and associated problems includes the following elements:
• Commitment to reducing harm caused by drugs.
• Greater attention to harms and patterns of use of specific drugs.
• Effective control mechanisms that emphasise prevention and variation between drugs and client groups.
• Innovative and up-to-date demand management strategies.
• Emphasis on drug use as a public health problem rather than a crime problem.
• Focus on the drug user as a prime target with intervention designed to reduce emotional, social and physical harm and stigma associated with misuse.
• Collaborative efforts between police, health and other relevant agencies.
• Legislation and law enforcement that is consistent with harm minimisation principles.
• Strong and effective responses to illicit drug trafficking, including heavy penalties.
Council’s approach incorporates a variety of strategies to reduce demand including:
• Information that is accurate, up-to-date and widely disseminated.
• Education that strengthens people’s capacity to make reasonable decisions about drug use.
• Drug treatments that recognise different treatments will work for different people and that most drug dependent people will experience difficulty in stopping use.
• Community action that helps maintain drug users’ links with supportive networks of families and friends.
• Advertising and sponsorship standards that ensure drugs are not seen as fashionable.
• Treatment targeted to high risk adolescents and adult offenders.
• Education, training and work opportunities targeted to young people at significant risk of drug abuse.
3.4 Different Responses To Different Drugs
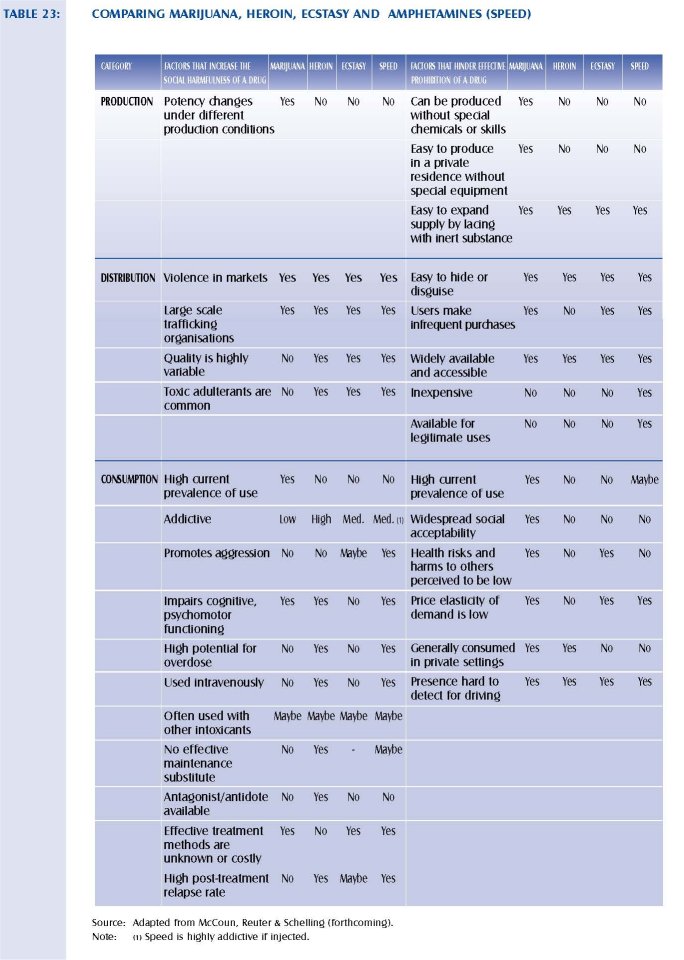
Drugs share many characteristics, in particular risk associated with misuse. However, there are important differences between individual substances. In some cases, these differences appear significant enough to justify varied responses (McCoun et al., in press). Table 23 summarises some of the characteristics that affect response options considered by Council. Analysis and debate revolve around how the production, distribution and consumption of a drug relates to its social harmfulness, and the likelihood of effective control under existing laws.
Use, prevalence and health risks associated with the use and misuse of individual drugs were outlined in chapter 2. Council also considered a range of other information about the most commonly used drugs in Victoria (marijuana, amphetamines and heroin) to assess whether different responses are appropriate for different drugs. Although cocaine is certainly available in Victoria, it was not considered in any detail by Council. Few submissions identified it as an issue and there are almost no problem users presenting at drug treatment services.
3.4.1 HEROIN
In the minds of most Victorians, heroin represents the drug problem at its worst. The prohibition of other, demonstrably less harmful drugs was justified in many submissions on the grounds that their use might lead to heroin. In terms of social cost, heroin dependence under current law is a significant contributing cause of crime, and closely associated with the serious risks of hepatitis B and C and HIV infection.
However, heroin also illustrates the central paradox of drug prohibition: use of criminal law and law enforcement for the protection of public health and morals results in an increase in associated crime and costs to the criminal justice system. Council's discussion with heroin users highlighted the fact that current heroin prices mean most users face the choice of prostitution, theft or trafficking to finance their habit. A constructive linkage between law enforcement goals and treatment is demonstrated by the methadone maintenance program that achieves a measurable reduction in crime and reduced health risks (Goldstein & Smith, 1995).
While many submissions advocated legalisation of heroin, the case for prohibition remains strong. However, Council also acknowledged the costs of prohibition, including increased misery of those who become dependent. To these are added community costs such as the spread of disease, user crime, and the expenditure of scarce law enforcement resources.
A practical response to heroin hinges on maximising the contribution of various programs designed to:
• Discourage initiation into heroin use.
• Control predatory drug trafficking.
• Contain the spread of disease among heroin users.
• Provide easy access to a range of programs that enable dependent users to manage the dependency with a reduced reliance on heroin, or to stop using.
Practical responses also involve the provision of support and treatment to drug dependent people willing to use such services. These are discussed in more detail in other parts of this chapter.
Special attention needs to be given to well-targeted action to prevent initiation. Available evidence suggests general anti-drug messages are of limited value in preventing heroin dependence because those at greatest risk of trying heroin and of becoming dependent are least likely to pay attention to messages from schools or the mass media. Special problems for anti-heroin messages are that only a tiny fraction of any identified population is likely to start using heroin. Thus, if messages have any 'advertising' effect, the number of new users inadvertently attracted could outnumber the number of new or potential users deterred. Consequently, anti-heroin messages need to be targeted very carefully. Current heavy users are likely to be enormously resistant to messages. The prospects of telling them something they do not already know are small and negative messages sometimes contradict their own experiences. To the extent that recently recruited heroin users can be identified by health workers or police, there seems some benefit in making them targets of 'secondary prevention' efforts designed to prevent progression to heavy and dependent use (Kleiman, 1992).
3.4.2 AMPHETAMINES
After cannabis, amphetamines are the most widely used illicit drugs in Victoria. Advice from Victoria's Drug Squad suggests that there is a risk of substantial growth in use of these drugs. Local production continues to provide a readily available supply, despite police success in detecting and closing an average of one amphetamine laboratory a month.
While data remain patchy, there are indications from research studies and official statistics that amphetamine use increased among young Australian adults during the mid 1980s. This was probably because of their widespread availability, their lower cost by comparison with heroin and cocaine, and their relatively benign reputation. Amphetamines appear to be primarily used for recreational purposes in social settings where young people gather to 'party' and have a good time (Hando & Hall, 1995).
Concerns about growth in amphetamine use focus on several issues:
• Australian amphetamine users are more likely to inject the drug than users in other parts of the world. Reasons are unclear, but the apparent increase in the prevalence of injecting amphetamines generates a number of public health concerns. Large individual doses can be fatal. Chronic heavy use can lead to dependence and paranoid psychosis. There is also a high risk that following treatment some users may relapse. In addition, users can become aggressive and violent (Hall & Hando, 1993).
• There are increased risks of motor vehicle and other accidents arising as a result of intoxication from amphetamines and alcohol (Hall, 1993), both of which may lead to aggressive and dangerous driving.
• Many young people do not consider amphetamines to be dangerous. These young people often frequent nightclubs or 'rave' parties and take the drug for the extra energy that allows all night dancing.
• Better organised criminal groups are moving into amphetamine production as a growth market without the inherent risks associated with importation (ABC!, 1995).
• Much production is relatively primitive and there are significant risks of impurities and contaminants in products, adding to health risks for users.
• Withdrawal from amphetamines appears to be more difficult than, for example, heroin.
Practical responses to amphetamines include:
• Legislation to restrict the supply of chemicals necessary for manufacture, law enforcement, and improved national intelligence exchange concerning clandestine laboratories. While significant progress has been made, particularly in developing national legislation relating to precursor chemicals, supply and availability of drugs has not been reduced except for short periods.
• Reducing risks associated with injecting, by improving access to needle exchanges and discouraging unsafe sexual practices among amphetamine injectors.
• Improving information for health professionals about the range of amphetamine related health problems for which young people may seek medical care. In accident and emergency contexts, amphetamines mixed with alcohol contribute to accidental injury and assault.
In psychiatric settings, amphetamine psychoses may be present in young adults with acute psychotic symptoms that remit with minimal treatment over several days (Hall and Hando, 1993). In general practice, concern should be aroused by young adults who come seeking medication to deal with insomnia or who show features resembling a depressive illness.
• A comprehensive training package (From Go to Whoa) has been developed in Victoria for the Commonwealth Department of Human Services and Health and Council urges its promulgation and use.
• Development of effective amphetamine-specific treatment. While replacement programs are now being tested, numbers of dependent users involved are very small. Alternative approaches also need to be explored.
Council's attention was also drawn to a number of initiatives in the Netherlands to minimise harm associated with amphetamine use. These included publication of guidelines for safe organisation and conduct of 'raves' or dances and special facilities to identify, via rapid chemical analysis, the likely content of substances purchased by young people. Both initiatives appear practical approaches to reducing the risks young people face in consuming these drugs.
Ecstasy is a widely used derivative of amphetamines. Ecstasy is probably the best known of a range of so called 'designer drugs'. These drugs can be manufactured to produce a range of different effects on the brain. Council has been advised that the range of such drugs may expand in the next few years. The appearance of such drugs on the market raises new, largely unknown risks to users and uncertainty for health services.
As with amphetamines, usage is likely to occur primarily at 'rave' parties or similar. However, it is possible that as the range of drugs expands, usage patterns may also change. The early warning information service proposed by Council will be vital in monitoring the extent and pattern of use of these drugs.
Although there is evidence of an increase in the use of drugs such as amphetamines and Ecstasy , users of these drugs are only now beginning to appear for treatment. Careful monitoring of new and emerging drugs should be accompanied by development and trialing of appropriate responses which may be similar to existing programs, or new and different interventions.
3.4.3 MARIJUANA
Marijuana is the most widely used illicit drug. Twelve per cent of Victorians have used marijuana in the past year, and this is considerably more than all other illicit drugs combined. Evidence provided to Council regarding a rural police district indicated that more than 90 per cent of police work was drug related. Of this, around 65 per cent related to cannabis, and most of this to use and possession. Use and possession charges also constitute a significant proportion of all charges heard in the Magistrates' Court. Yet marijuana does not loom large among drug problems in terms of observable and measurable harm done to users or to others. It is undoubtedly a powerful intoxicant and can generate a number of serious problems if abused. To decide how large a problem marijuana poses requires judgement of fact and value.
Even if marijuana posed few health risks itself, it would still represent a problem if it tended to lead to the use of other more dangerous substances. Dutch experience indicates that marijuana is not a 'gateway' to heroin. While marijuana is available throughout Dutch cities, there are very low rates of heroin initiation. The most careful study to date, conducted during the 1970s in the United States, explored the marijuana-heroin link among the largely minority-group adolescent population of Manhattan (Clayton & Voss, 1981). Its findings confirmed a relationship between heroin and marijuana, but with an unexpected twist. Heavy marijuana smokers did appear at greater risk of becoming heroin users, but the mechanism did not seem to involve the drug experience itself. Rather, heavy marijuana use appeared to generate involvement in drug selling, either as a way of paying for the marijuana consumed or simply by association with drug sellers. Drug selling, in turn, gave adolescents access to heroin and the money to buy it. This suggests marijuana was a gateway for these adolescents because it was illicit (Kleiman, 1992).
A number of cross-national reviews indicate that response to cannabis would be more effective if it was clearly distinguished from more dangerous drugs. In particular, current levels of marijuana use are more likely to be reduced through education and persuasion than appears likely for other illicit drugs. Marijuana is already widely used and therefore less exotic than other drugs. Therefore there is less risk that discussion in school will create an awareness and curiosity that would otherwise have been absent. By the same token, the target efficiency of the messages—the probability that any given recipient would have seriously considered using the drug now or in the future—is higher for marijuana than any other illicit substance. Benefits of carefully developed education to discourage marijuana misuse seem to outweigh risks (Kleiman, 1992).
During its investigations, Council was made aware that some Victorians may experience significant problems as a consequence of cannabis abuse. Development of a trial treatment service for cannabis users is recommended in chapter 4. Provision of information and support for parents responding to their children's marijuana use was also raised as a significant issue. This is discussed further in the next section. Law enforcement and legislative responses to marijuana are also discussed later in this chapter.
3.5 Information and Health Education
Lack of information and inaccurate information are disturbing features of the Victorian community's knowledge about illicit drugs. While these shortcomings are widely acknowledged, there is less agreement about how information, health promotion and education become active and effective components of Victoria's response to illicit drugs. There has been little planning for a comprehensive, coherent and coordinated information and education approach to illicit drugs in Victoria.
Council believes that prevention must be one of the foundations of Victoria's long-term drug strategy. Dissemination of accurate information, and providing education about drugs within a health promotion framework, is a major component of the Council's proposed strategy.
Health education and information dissemination should always occur within supportive environments. Passive provision of information, even if accurate and well done, will have little or no impact. Information provision in the form of pamphlets, telephone services or curriculum should also take account of relationships between young people's mental status and attitudes to authority—two factors strongly related to drug use.
For legal drugs, primarily alcohol and tobacco, strategies to prevent misuse occur in a health promotion framework. There is now considerable experience in Australia and elsewhere about the effectiveness of health promotion that includes information and education about alcohol and tobacco.
A health promotion approach is likely to make a significant, long-term contribution to reducing use and misuse of illicit drugs. However, the combination and significance of strategies and settings for communicating health messages will be different from those used for legal drugs.
Total population approaches are likely to be more appropriate for drugs that are used by a large segment of the population. The increased prevalence of marijuana use suggests that a health promotion strategy similar to that used with alcohol and tobacco deserves attention.
Focussed strategies regarding the more dangerous drugs are required. Greater attention will need to be paid to ensuring that messages and support services are targeted to user populations and their networks, rather than the general public.
Detailed development of Council's strategy will require considerable community and expert input. An effective framework will require identification of:
• Groups that are the targets of the information.
• Drug(s) to be addressed.
• Behaviours to be targeted (for example, 'safe' use—injecting practices, sharing needles and equipment).
• Means to disseminate the information.
• Desired outcomes (these might include attitudes, knowledge and skills, intended behaviour and actual behaviour with regard to illicit drugs).
3.5.1 COMMUNITY INFORMATION SERVICES
Given that the community receives most of its drug information from mainstream media sources, it is important to facilitate accurate and appropriate reporting as far as possible. The media liaison service that the Australian Drug Foundation offers is an important resource. The media should be encouraged to include information about other targeted services as part of its reporting, such as telephone numbers for further information or advice. The use of community announcements to advertise services might have a role.
The most important specific vehicles for disseminating accurate information to the general community are telephone information and printed materials. However, information provision without other reinforcing activity is unlikely to increase young people's capacity to resist drugs.
Existing specialist alcohol and drug telephone services provide different kinds of information. DIRECT Line provides specific information about the nature and effects of drugs. This information is targeted to those who are contemplating using drugs and their families, and is provided where counselling and referral to specific services is possible. DRUG Info provides a broad base for general information about drugs to the community, and back-up written materials on request. The two services are able to automatically transfer calls where a person's needs can best be met by the other service. Both receive calls from throughout Victoria, but calls from regional and rural Victoria are fewer than expected based on population figures.
Joint promotion of these two services should be encouraged, and opportunities for increased integration explored. Improved data regarding the use of these services is also required for future planning purposes.
Specific strategies are required to address the needs of people from diverse cultural and language groups, and regional and rural communities. Ethnic communities may be better informed through linkages with existing 24-hour interpreter services, recorded messages in languages other than English, recruitment of bilingual staff, and by using ethnic radio and press. Joint promotional efforts would increase the effective use of DIRECT Line and DRUG Info by people from these communities.
The National Drug Strategy has funded development of much printed material over the past ten years. While there have been repeated calls for coordination, printed material continues to be developed in isolation. Pamphlets and other printed materials are most useful when used in conjunction with other broad-based or specific information strategies. Information about illicit drugs, in particular, is likely to be of little or no value on its own.
Council believes that printed materials should be reviewed, and where appropriate for use in conjunction with other information dissemination activities, be translated into languages other than English.
Libraries are an important source of detailed information for the general public. Council has not explored the issue of drug information in general libraries, but notes the value of the comprehensive, specialist alcohol and drug library and information services at the Australian Drug Foundation.
3.5.2 YOUNG PEOPLE, SCHOOLS AND BEYOND
Young people often experiment with drug use, licit and illicit. For a small number, use is chaotic and at problematic levels. Many young people's interest in information is high, particularly where it relates to the functioning of their bodies. Young people are one of the major audiences of mainstream media (particularly television and radio) where they receive information about drugs and lifestyle issues. A range of strategies is required in terms of information provision and education depending upon their developmental stage and social situation and cultural background. Public information is particularly important to assist parents to discuss these issues with their children.
Council believes that efforts to prevent young people using and misusing illicit drugs should be given a high priority.
A hierarchy of approaches exists for responding to young people's drug use. These include broad-based prevention strategies, closely linked to personal and mental health promotion, that aim to prevent the use of drugs when most young people are considering experimentation. This type of program, delivered as an integrated part of the school curriculum, will be all that most young people will need.
Some young people are at a particularly high risk of illicit drug use. It is important to note that these same young people are vulnerable to other health risks, including psychiatric illness, self-damage or mutilation, youth suicide, nutritional disorders, and the broad cluster of problems that are often associated with social disadvantage such as homelessness, family disruption and unemployment. Youth unemployment is strongly correlated with substance misuse (Ray and Ksir, 1990).
To prevent these marginalising circumstances, efforts to support young people are important. Efforts to reintegrate or provide resources and opportunities, such as training programs are likely to be very important drug prevention activities, although detailed consideration of these is beyond the scope of Council.
Council was particularly concerned about the suggestion that there is a lost generation of young people who are using illicit drugs in a destructive way and who, as a consequence, are alienated from mainstream society and are beyond help. This pessimistic view, and variants of it, were put to Council at community and expert forums and in written submissions. Others who spoke to Council had significantly more hope that more could be achieved, first in preventing young people from commencing problematic drug use and second, in intervening to reduce the harms associated with some young people's drug use. This latter view has informed Council's thinking. Council believes very strongly that no young person should be abandoned by the community, no matter how difficult or seemingly intractable many of their problems may be.
Opportunities to provide information exist at youth-specific venues, but it is inappropriate that materials relating specifically to illicit drugs should generally be placed in such venues because of the potential `advertising' effect for non-users. An exception might be where those at high risk of hazardous and harmful drug use congregate, and the use of peer education approaches to reach those especially marginalised. Case management services provide important links for this group.
Response to, and support for, this group of young people are included in later discussions of community involvement, and support and treatment services.
Schools have a critical role to play in informing and educating young people about the role of drugs and their use and misuse in our society. Submissions strongly supported greater priority in this area. Views about when and how this education should be provided were more diverse.
Council heard about efforts of all school systems (government, independent and catholic), individual schools and community bodies to provide school-based drug education. These efforts have primarily concentrated on legal drugs and have produced a number of resources and materials addressing alcohol and tobacco use issues. Much of this effort is positive and deserves support.
However, Council is concerned that some current, widely supported activity does not accord with sound educational principles. Council is aware of the international literature that shows that drug education which is intensive and 'one off' can be ineffective or, in some cases, counterproductive, in fact increasing the likelihood of use. Recent Victorian research confirms these findings (Hawthorne, 1995). Council believes that drug education must be built into the normal structures of education.
Problems arise because the State has had no systematic and formal structure into which drug education fits, and has not equipped schools with the skills and resources to educate students effectively. The absence of a framework has allowed a range of ad hoc initiatives to develop (Hawthorne et al., 1994).
Recent activity has been directed at the development of resources including curriculum guidelines and materials. The principal outcome is the Get Real package developed by the Directorate of School Education (DSE), in consultation with a wide range of relevant organisations. These products are of high quality and deserve support.
Principles to guide school drug education should include:
• Education policy and programs should be consistent across the school environment and developed in conjunction with broader school policy about drugs, and student welfare. School ownership of policy and programs is vital.
• Objectives should be linked to the overall goal of harm minimisation.
• Programs should have sequence, progression and continuity over time throughout schooling and provide consistent and coherent messages.
• Drug education is best included within the health strand of the curriculum, but may also be appropriate to include in other areas such as science.
• Drug education should be delivered by teachers of the subject in which it is included. The teacher should retain responsibility for materials and any other resources used including outside programs.
• Programs should take account of research-based evidence supporting what is effective, and
recognising that what seems like common sense can sometimes be counterproductive.
Success at school levels will also need to ensure that the following issues are addressed:
• Policy development: Schools must develop policies that deal directly and appropriately with the full range of issues about legal and illegal drugs.
• Curriculum space: While Council has not been able to assess the impact on existing curriculum, it believes drug education, incorporating licit and illicit drugs, should be part of core curriculum. While endorsing the need to commence drug education in primary school, Council believes that material relating to illicit drugs should be introduced in the late primary or early secondary curriculum.
• Curriculum content and materials: Further work is required to develop curriculum materials dealing with illicit drugs, particularly cannabis.
• Trained teachers: Council was advised consistently of the importance of ensuring that teachers are pivotal to drug education. Teachers must select and deliver the curriculum and materials appropriate to young people's level, needs and context using the principles outlined above. To deliver this, teachers need to be confident of their competence regarding drug education. This is not currently the case.
Teachers will require enhanced professional development and in-service training opportunities and resources if comprehensive drug education initiatives are to be successful.
Council received some evidence suggesting the presence of illicit drugs in Victorian schools. Given the reported use of drugs by school-age adolescents, this is hardly surprising. Council received no evidence, however, of illicit drug use within school hours.
Schools confront illicit drug use in many ways; drug education within the curriculum, policies relating to drugs and the possible use of drugs at school, and pupil welfare that can involve liaison with parents and community services. The preparedness, capacity, resources and responsiveness to these issues varies widely.
Council heard that some schools had moved to develop strong welfare responses and links to community services, especially those dealing with young people. Other evidence suggested that some schools actively discouraged young people with problems or, at best, provided little support. This leads to an apparent differentiation of schools into what is informally known as 'good' schools (those less likely to retain troubled youth) and 'bad schools' (those schools which worked to retain young people in schools). Further work is required to assess and minimise the long-term damage caused by such differentiation.
Within the school community, there is a small group of young people who are vulnerable to developing serious and lifelong substance use problems. It is important that strenuous efforts be made to retain this group within the school system to enhance their skills, knowledge and preparation for the workplace, and to prevent or delay their labelling and experience of unemployment. Additional resources are needed for this to be effective.
In instances where young people are using drugs, it is important to involve parents where possible, and community-based services in the provision of early intervention or treatment to address drug use issues. This collaboration could be arranged by school pupil welfare coordinators or other appropriate persons.
If the young person leaves school, careful case management into the community and linkage with other facilities and resources could reduce the impact of the sudden lack of support and connectedness to the general community, which makes young people particularly vulnerable to increased and harmful drug use.
3.5.3 TRAINING AND PROFESSIONAL DEVELOPMENT
'While alcohol and other drug problems are relatively common, the majority of human service providers do not receive education and training on how to effectively respond. Consequently, many staff and organisations do not perceive that they have the knowledge, skills, confidence or legitimacy to respond to alcohol and drug related harm. However, a substantial literature has demonstrated that a broad range of human service providers such as general practitioners, nurses and police can have a significant impact on the reduction of alcohol and drug related harm at an individual and societal level.' (Allsop, S., 1996, p.2)
Submissions, expert witnesses and commissioned work brought Council's attention to the role of a wide range of people whose jobs bring them into contact with current and potential drug users. Many of these are professionals in contact with drug users at a time when they may be motivated to change their behaviour.
While specialist services are important to drug users, treatment can be an unnecessary or inappropriate response for some people. Young people and adults are unlikely to seek help or support from specialists until dependency is established and social problems arise. Information, education and practical support can be effectively provided by generalist workers in a range of contexts.
These workers have a potentially critical impact on the provision of information and education about drug use and related issues as part of their principal role. They also have the potential to develop sustainable linkages across the range of health and welfare, law enforcement, and other support services and organisations within the community. This would assist communities to pool their resources and efforts, and provide an integrated response to drug issues.
Incorporating alcohol and drug training in undergraduate courses, and providing ongoing skill development in drug-related issues, has been given relatively little attention, at least partly because of the legal status of many drugs. Making harm minimisation principles relevant to the practice of many professionals can significantly enhance the preparedness and effectiveness of general health and welfare service providers who have an opportunity to intervene with drug users.
An effective strategy to reduce drug use and misuse will, in part, be dependent upon enhancing the knowledge and skills of people like police, doctors, teachers, nurses, welfare staff and youth workers about drugs and a harm minimisation approach. For some of these groups, integrating these matters into existing professional development and training structures is required, and in others, innovative action is needed. Planning in these areas will need to take into account opportunities to make this training part of, or consistent with, accredited educational courses so that participants can gain some professional recognition.
Although there is some shared training between Victorian programs and the National Centre for Education and Training in Addictions in Adelaide, Council believes this is not adequate to address the extent of the need.
There are currently three specific drug-related postgraduate courses available in Victoria. There are also some in other states, including at least one that can be accessed through distance education.
Providing enhanced educational and training opportunities at all levels is important. Council received submissions indicating that there was only a small pool of expert alcohol and drug personnel in Victoria currently and that staff recruitment to specialist programs was difficult. Career opportunities were limited in this relatively small specialist field which indicates that educational opportunities might best be located within broader based undergraduate and postgraduate programs. Council did not examine the current courses with regard to the illicit drug curriculum specifically but believes there are insufficient drug and alcohol educational programs at tertiary levels.
Consistent training for all workers in direct contact with drug users, or people at risk of drug use, would enable better linkages to be made across service systems. Extensive work on development of protocols between specialist drug and alcohol services and other general and specialist services has commenced in some areas, such as child protection and psychiatric services. Some of these are still in their infancy and are currently underutilised. Some remain at draft stage and may lack commitment and resources to implement them.
Council agrees that there is a need to build a core of people from a variety of disciplines who have specialist expertise in substance abuse issues. Building and diversifying the expertise base will also require a long-term investment in higher degrees and research. This is particularly relevant in the professions involved in public health.
Council believes that a strategy for providing education and training is urgently required. This strategy should enable the development of an integrated approach to the provision of drug education across services and organisations.
3.5.4 COMMUNITY INVOLVEMENT
Local government bodies and local communities presented to Council either through submissions, specialist forums or at public hearings. They described initiatives to address specific alcohol and drug issues in their communities. Some of these have been in place for a sustained period, but there has been little attempt at a coordinated local government effort in Victoria.
Advice from groups meeting with Council highlighted the impact of drug use. Advice also highlighted the fact that communities can play a positive role in reducing the harm caused by drugs. Council accepts that there is neither an easy nor consistent way to engage communities whether they be local communities or communities of interest. Fostering positive 'health-oriented' community involvement is likely to be an important ingredient in prevention, education, and reducing the harm caused by drugs.
Communities vary in their level of concern. All share a hope that drugs will not cause problems either directly through use, or indirectly through disruptive behaviour and illegal activity, such as the theft and burglary associated with illicit drug use. Some communities experience heightened concern from time to time that is related to an apparent increase in drug problems or drug-related incidents. The media plays an important part in influencing this level of concern.
The absence of readily available guidelines and well-publicised resources contributes to considerable duplication of effort and frustration. Systematic and reliable information about patterns of drug use and associated harms is usually not readily available at a local level and makes planned responses difficult. This needs to be addressed in an overall effort at enhancing data collection and dissemination.
The involvement and collaboration of major service sectors at the local level are also vital. Council noted examples where this was working well, and others where the different orientation of some sectors contributed to confusion and inconsistent approaches. Intersectoral linkages might occur through a variety of existing structures, such as local government, or sector-specific consultative mechanisms such as Police Community Consultative Committees. Council is not confident that any one of these is necessarily appropriate or working well across all communities.
Current efforts to bring together, document and evaluate these efforts and the subsequent production of guidelines for local action should be supported.
Council noted that the involvement and collaboration of major local service sectors is particularly crucial in establishing strategies and initiatives that address the issues of drug use and misuse among young people. Such strategies and initiatives may include:
• The development of stronger linkages between local services and organisations including schools, youth services, police, sporting and service clubs.
• The establishment of a range of local activities for young people. Young people should be involved in the development of these activities.
• Improving the local public transport service where required to allow young people access and safer travel to entertainment venues within and outside the local area.
• Providing information about drugs and their effects that are appropriately targeted to reach young people where they congregate, or through other appropriate media such as radio and television programs.
Strategies to provide additional support to young people who are particularly 'at risk' and those who have an established drug use problem, may include:
• Providing information about drugs in settings where they congregate, and through appropriate media such as radio and television programs.
• Ensuring access to stable housing.
• Providing assistance in seeking and obtaining employment.
• Re-establishing linkages with their families.
• Providing access to a range of relevant support and treatment services if and as required.
3.5.5 PARENTS
Parents are a critical influence on drug use by young people. This occurs through general care, welfare and provision of guidance and resources, as well as through their own drug use, and their values and opinions on drugs. Parents and peers act as role models and provide information about drugs. A major concern is that misinformation can often take the place of facts.
Parents have stronger influence on younger age groups. While peers become more influential during adolescence, parents remain important and can provide vital stability.
While there were general calls for the provision of information about drugs to parents, there was no clear evidence that parents actively seeking this information had not been able to obtain it.
Many parents of those already using drugs expressed frustration at the lack of information about drug use and related services. Parents with a child who is actively using drugs and sometimes already experiencing severe problems need targeted help. Council heard many distressing stories from parents of drug users. These people were consistently seeking compassion and support and none sought controls or penalties. Many sought assistance for themselves and spoke of the inconsistent advice they received from a range of sources. Some of this advice suggested they 'reject' their child, which they found unacceptable. These parents told stories describing their role in supporting their children that suggested they experienced considerable fear, anger, distress and a sense of impotence. These parents came from all strata of the community.
This group needs specific assistance to deal with their own reactions and to support their child. Where possible counselling should involve interaction between the child, parents and those able to provide support. Council recognises the often complex family relationships associated with drug use and believes that this group might benefit from self-help and other peer support and information initiatives. This was not explored further by Council.
Parents should be encouraged to utilise those whom they ordinarily turn to for support and assistance in their community. This might be a friend, community member, or someone located in a specific service. For those who feel they do not have these resources available, the DIRECT Line telephone service can provide advice, counselling and referral. DRUG Info can assist with information about the drugs that their children are using and printed materials.
Council received advice that in many communities, including ethnic communities, parents often approach religious or community leaders as a first port of call to request information and assistance on drug issues. These parents or religious and community leaders may not be fully aware of resources available. The development of strategies to ameliorate the situation, including those outlined in section 3.5.1, need further consideration. Council's attention has been drawn to the recent seminars organised by the Ethnic liaison Unit of Victoria Police and involving the Centre for Adolescent Health and Odyssey House on 'Drugs in the Greek Community. These seminars aimed to disseminate relevant information to Greek-speaking parents on drugs from the medical, legal treatment, and policing perspective. Further such initiatives should be encouraged and supported.
Improved knowledge and skills relating to drugs and their use could be acquired by parents through increased involvement in schools and promotion of community information services. Information about drugs could also be included in courses or workshops provided for parents (such as parenting skills workshops) by local community organisations. The training of generalist health and welfare workers (including general practitioners, nurses and other health and welfare workers) would increase their ability to provide parents with information and to direct them to appropriate services as required. Schools may also contribute to the knowledge and skills of parents by involving them in issues and activities relating to the provision of drug education within the school.
3.5.6 DRUG USERS
Council was made aware that the provision of prevention and information services to drug users or potential drug users is difficult to achieve, primarily because the illegality of drug use and their mistrust of authorities make them a difficult group to contact. Education targeted to users must therefore be non-judgemental and aimed at harm reduction and safe use. Any insistence on abstinence may impede efforts to disseminate information. Referral to treatment services should be offered on request by the user.
The limited resources or strategies currently addressing the prevention and education needs of drug users concerns Council. Information is currently provided by DIRECT Line, VIVAIDS and at needle syringe exchange outlets.
Drug users are at high risk of suffering the harmful acute and chronic effects of drug use, including HIV/AIDS, hepatitis B and C, as well as the risk of overdose and death. Peer education is likely to be one of the most effective ways of reducing these harms. Drug users who met with Council supported the use of peer-based education. However, Council has also been informed that conventional peer education has not been effective for certain ethnic user groups, and that for these groups outreach services are more effective.
It is clear that hepatitis C is more readily transferred than HIV within the intravenous drug using population. There is a need for further research to determine why this is the case. There is a need to develop targeted education programs aimed at intravenous drug users if the success in controlling HIV spread in the Australian intravenous drug using population is to be replicated for hepatitis C.
3.5.7MEDIA CAMPAIGNS
Council received many written and oral submissions requesting a major media campaign to address the issue of illicit drugs in Victoria. Evaluations of such campaigns conducted nationally and internationally indicate that while they are useful in preparing the community for proposed changes to policy and drug control strategies they have not been successful in convincing users to change their using behaviour. They have also not been successful in stopping use once established. Evidence for their effectiveness in preventing drug use is missing. More dangerously, such campaigns if not very carefully developed, as part of a comprehensive strategy, have the potential to attract some people to illicit drug use.
Major media campaigns are only likely to be used effectively when advertisements are one component of a broader strategy. Evaluation of Victoria's successful campaign to reduce alcohol-related road fatalities has clearly demonstrated the importance of police activity (including speed cameras, booze buses, targeted sponsorships and education) in delivering the impact of key messages in television advertisements.
Council believes that media campaigns should only be used to communicate major changes to policy and arrangements in Victoria: where appropriate, this should be in cooperation with the Commonwealth Government.
Illicit drugs differ from other issues commonly dealt with in media campaigns because they effect a small percentage of the community. Messages targeted at this group run the risk of communicating unintended messages to non-users. They would also have a poor cost benefit return.
Council urges ongoing liaison between journalists and those in the drug and alcohol sector, particularly those involved in information provision. While various efforts could be made to develop appropriate codes of conduct, Council recognises the difficulty of consistently implementing these. This is an area that may warrant future attention.
3.6 Support and Treatment Services
A wide range of problems and issues confront many people who use drugs. The services available to assist them range from the informal through to highly specialised drug and medical services. During its deliberations, Council received wide-ranging input about support and treatment for drug misuse. At times, the same information was used to draw widely divergent conclusions about support services for drug users. The same services were highly praised by some submissions and heavily criticised by others.
Council has not endeavoured to be comprehensive but has examined identified problems and searched for achievable solutions. Council believes that the problems of youth deserve special attention and it has accordingly considered these issues in a separate part of this section. Similarly, the issues for drug users who come into contact with the criminal justice system warrant increased attention and a specific discussion of these issues is included.
Council is aware that there are other vulnerable groups who use illicit drugs; for example, opiate-dependent women with young babies. Many of the issues surrounding this group relate to the absence of adequate family support and general welfare services. Shortages of these services work against these often fragile families gaining the necessary skills to meet the developmental and survival needs of vulnerable young babies and children. This, in turn, may lead either to tragedy, or the precipitous and repeated engagement of child protection services. Solutions to these problems do not lie in the expansion of specific drug and alcohol services but rather a stronger and more able generalist health and welfare sector capable of responding without prejudice to the medical, dental and other care and support needs of opiate or other drug dependent women and their families.
Homeless people are another vulnerable group who experience difficulties in accessing services in the general health and welfare system. Such people are often living on the fringes of society and this increases their chances of having a range of problems, including illicit drug misuse.
Chronic pain sufferers constitute a special group of opiate-dependent people. Issues surrounding this group are, however, not discussed in detail.
Council believes that proposals developed in respect of treatment and support services, although not directly addressing the needs of these groups in detail, will benefit them.
The community and professionals working in all support, treatment and related sectors need to be aware of the importance of illness prevention approaches with illicit drug users. These may include provision of information and education as well as counselling and, for some, substitute drug therapies.
Information and advice about the prevention of spread of blood-borne infections, improvements in nutrition, and sexual health are especially important. Council notes that the needs of injecting drug users require special attention. It may be appropriate that injecting drug users be encouraged to use in less harmful ways, such as inhaling, smoking or snorting.
The provision of secondary consultation by the Drug and Alcohol Clinical Advisory Service is an important means by which the capabilities of generalist health and welfare professional are strengthened to deal effectively with clients who have substance use problems.
It should also be noted that people who take illicit drugs usually take more than one drug simultaneously, although they might have a drug of preference. This phenomenon is described as poly-drug abuse and commonly increases the harms associated with drug use.
3.6.1 SUPPORT SERVICES
PEER SUPPORT AND SELF-HELP GROUPS
Many drug users have had negative experiences that have resulted in an enduring sense that they are alienated from the community and not able to access services. In this context, they have found the support and advocacy offered by peer support groups invaluable. Council has also formed the view that these organisations are vital. Their potential as a link into other services and legal systems is currently underdeveloped. For example, organisations offering peer-based support are successful in delivering family and other support services that have credibility and relevance to users, but also take account of the needs of user's children (McGregor, 1994).
Council urges that these services should be consulted extensively about their role with a view to developing more sophisticated use of the expertise.
NEEDLE SYRINGE EXCHANGE PROGRAMS (NSEP)
Needle exchange programs (NSEP) playa critical role in reducing rates of infection and safer injecting practices, be they provided by outreach services or at fixed locations usually in health centres. Council also acknowledges the important role NSEPs play in providing education to users and, where requested, referral to treatment agencies. Many pharmacies also provide needles, syringes and, where appropriate, advice to users.
Growth in the number of needles/syringes distributed in recent years is evidence both of the demand and support for these programs. Council heard several descriptions of positive and collaborative efforts to maintain individual services. One example involved police and local health services in St Kilda.
The NSEP program remains contentious for some people and examples of local community reluctance to accept these services was apparent. There are important planning decisions that need to be considered, including the harms that result to users and others from unsafe injecting practices. Long delays in establishing NSEPs have hidden and potentially significant costs for the community that must be actively balanced with local issues.
Council was advised that injecting drug use continues in Victoria's prisons despite vigorous attempts to eliminate drugs. In the absence of provision of clean injecting equipment, intravenous drug use in this environment is likely to be high risk. Council accepts that management of this situation requires careful consideration.
3.6.2 ACUTE SERVICES
Individuals experiencing problems with illicit drug use may develop problems that require emergency care. Currently, help may be sought in the emergency rooms, the psychiatric care system, from general medical practitioners and the ambulance service. These services are an important link in the acute care system that supports and treats people with drug problems.
Council was advised that the ambulance service plays a vital role in responding to drug use, particularly in the case of overdose or suspected overdose. Ambulance officers are able to provide general health care and, in the case of a heroin overdose, administer a drug (Narcan) which rapidly counteracts the effect of heroin.
Council was advised that some young drug users believe that the ambulance service will notify either their parents or the police if called. As a result the ambulance service is not called to some overdose situations, dramatically increasing the risk of death. Council believes this issue should be addressed through policy and practice guidelines and protocols.
3.6.3 SPECIALIST DRUG TREATMENT SERVICES
SERVICE REDEVELOPMENT
Victoria has been a leader in the development of many drug and alcohol services over the past thirty years. Council noted, for example, the respect that a number of experts from elsewhere in Australia and from overseas have for the Victorian Methadone Program. This program is delivered largely through general practitioners and community pharmacies rather than specialist clinics.
While most drug users access general health and welfare services when they need assistance for problems, they will often seek specialist support for issues directly associated with their drug use. In addition, they also seek support from specialist agencies to change their drug using or to reduce the harms of drug use. Similarly, general service providers often refer such people to specialist services.
The Victorian drug and alcohol service system is being redeveloped with a view to encouraging general service providers to retain overall management of such clients while the drug and alcohol sector provides specialist backup and treatment (see 2.3.2).
The range of specialist treatments includes thorough assessment, withdrawal programs, counselling and therapy, support or self-help services, and substitute pharmacotherapies such as methadone. Some of these services can be residential, although most are now provided as outpatient services. Some services offer highly specialist long-term residential therapy. Research evidence suggests that this is likely to be appropriate for a quite small number of people and the cost per client is high, relative to other treatment options although more economic than imprisonment.
Council believes that the rationale underpinning the program redevelopment is sound. Council accepts that it is important to develop services which are based on research evidence on what works and to ensure that there is a fair distribution of services across the State. Council does have concerns about a number of transition issues and about the capacity of the service system to deal with the existing level of demand.
Council heard many concerns expressed by current drug service providers, drug users, providers of community services and members of the community about the current provision of specialist drug treatment services in Victoria. Key issues were associated with the transition toward a service system in which drug and alcohol services back up generalist services. Views expressed included challenges to the conceptual basis of this program shift, suggestions of apparent gaps in services and claims that the funding provided for new services is insufficient to provide a professional service.
Council understands that a number of services approved by Government as part of the redevelopment have not commenced operation. The State Government gave approval for the establishment of a range of services following a formal tender process in early 1995. Most of these services are now operating, some on an interim basis. Several others have not commenced and urgent action is required to ensure that these services are established.
A range of other concerns have been raised regarding the still new withdrawal services, residential and home-based. Council accepts that these are relatively new services and that further discussion with service providers and interest groups is required to assess whether the concerns result from the newness of the services or service specifications. An issue requiring consideration in this process is the capacity of the withdrawal services to meet the needs of particular groups (for example, women with children and the homeless).
Redevelopment is not yet completed and elements of both the former and new system exist. This appears to be causing some difficulties for service providers and clients. It is difficult for Council to assess the longer term impact of changes, but current disquiet suggests that ongoing review and evaluation are essential.
There has been considerable input to Council suggesting that there are not enough specialist services to meet the needs of people with serious drug problems. Service providers persistently claimed that clients approaching the specialist drug and alcohol sector are increasingly complex and difficult to manage and include many with psychiatric illness and severe social problems. The data available did not enable Council to assess these claims. It is clear that if the claims are accurate and reflect a sustained shift in demand, the field will be dealing with a more demanding and resource intensive group of clients. A review of client trends and consequent funding requirements may be justified.
Data provided to Council indicates that Victoria, relative to other states, underinvests in specialist drug treatment services (Alcohol and Other Drugs Council of Australia (ADCA), written submission, 1996). ADCA undertook a national survey in 1995. The survey gathered data on:
• Revenue raised through taxes on drugs.
• Outlays in specialist drug and alcohol services by State and Commonwealth Governments.
- The views of people working in the drug and alcohol field about the overall performance of the service system in their State.
Figures for both revenue and expenditures were provided to ADCA by the relevant authority. The performance assessment was based upon responses to a questionnaire.
The report indicates that Victoria spent $4.94 per head of population at the time of the data collection (December 1993). The national average was $8.93. Council believes that the survey figures should only be used as a guide to the general magnitude of expenditures made by all governments.
Various groups have argued that there is a serious lack of post-withdrawal support and counselling services across the State. The need for residential and non-residential post-withdrawal support has been expressed, with an emphasis placed on the need for residential services.
The current approach of the Victorian Government is to provide outpatient, rather than inpatient, rehabilitation services. The Government's approach is based on research that indicates that it is likely that well-designed non-residential services, backed-up by accessible acute services linked with other primary care services, can provide better and more affordable treatment for drug problems and allow greater needs to be met (Pead, 1996). It may be that at this stage of the redevelopment, insufficient linkages have been made and that this is exacerbating concerns. While Council has been unable to conduct a detailed assessment of need, there do appear to be insufficient post-withdrawal services available in Victoria.
SUBSTITUTE PHARMACOTHERAPIES
There is a range of substitute medications available internationally that are used to assist withdrawal, and for ongoing supportive management in the treatment of drug dependence. These are appropriate where the person has a long-standing and entrenched dependence on particular drugs.
There are good reasons to offer such therapies to dependent drug users early in their regular use as a harm reduction strategy. The benefits of early commencement on substitute pharmacotherapies include reducing the chances of severe illness to the user and reducing the spread of infectious diseases within the community.
In Victoria methadone is the only currently available substitute maintenance program that is safe, reliable and enables people to maintain normal lifestyles.
METHADONE SERVICES
Current evidence suggests that the methadone program removes a substantial number of heroin users from crime, trafficking and prostitution to support their dependency. Participation in the program is associated with improvements in nutritional status and a significant lessening of the hazards of intravenous drug use.
Council is persuaded, on the basis of empirical evidence, that methadone is regarded by many users and their doctors as a desirable and appropriate service. Council also heard considerable comment about the problems that some people face and acknowledges that methadone will not attract and retain all heroin users.
Methadone is a restricted and potentially dangerous substance. There are risks both to the person on the program and others if methadone were to be easily accessible in the community. Council supports an ongoing regulatory regime to minimise the risks of misuse. Victoria has made significant innovations surrounding methadone maintenance programs and careful monitoring remains important for the individuals on the program and the broader community.
People continue to have difficulty gaining access to the methadone program in some rural areas. In part, these problems have arisen because of difficulties in recruiting and retaining medical practitioners and pharmacists in rural areas. Council supports further action by the Commonwealth Government and the Royal Australian College of General Practitioners to encourage general practitioners to work in rural areas to undertake public health functions such as methadone prescribing. The Department of Health and Community Services should continue to work with the Pharmacy Guild of Victoria to expand pharmacy coverage.
Council accepts that some groups with special needs (such as young people, persons from minority groups and opiate-dependant persons in prisons) are under-represented in the methadone program. Council is concerned that efforts to develop specialist methadone programs have been delayed and believes that efforts should be made to expedite service development and include unrepresented groups.
Council is also of the view that many opiate-dependent persons on methadone programs benefit from counselling on a non-compulsory basis.
Victoria has led Australia in the training of prescribers of methadone. The Victorian Methadone Program guidelines for providers are a significant advance in the training of prescribers and have been developed in consultation with clinicians, trainers and researchers. In Council's view providers, recipients and regulators of methadone would benefit from the establishment of a peer review group to supply advice to the Department of Health and Community Services, to comment on the results of the monitoring process, and to guide the introduction of best practice innovation in this field.
Current and former users of the methadone program complained about the cost and indicated that for some people the cost is an impediment to involvement. Methadone users are required to meet the prescribing costs incurred in the community pharmacy. Council did not address the matter in any detail.
Council believes continuing improvement can be made in this important program, and that it should be subject to rigorous ongoing evaluation.
OTHER DRUGS FOR USE IN TREATMENT
A range of other substitute and antagonist drugs has been tried internationally in the treatment of opiate dependence. The drugs available include LAAM, Buprenorphine and Naltrexone. The roles these drugs perform differ but they all act to substitute for, replace the effects of, or reduce the craving for, opiates.
Council has not been able to ascertain in detail the cost and benefit of these drugs. Discussion with international experts (Strang, oral submission, 1996) confirms the potential benefit of one or more of these drugs.
Careful assessment is required of these drugs, and others that may be available. Intergovernmental discussions as well as liaison with the pharmaceutical companies is required to ensure trials can proceed expeditiously.
Council is of the view that Victoria has established itself as a leader in setting standards in the methadone therapy. It has the clinical and research capabilities to lead Australia in the development of programs utilising alternatives to methadone such as LAAM and Buphrenorphine, and in establishing the place of Naltrexone in treatment programs during drug withdrawal.
Careful assessment will be required to determine which of these drugs has the greatest potential to supplement methadone in providing a range of treatment options for dependent drug users. The reason to broaden options is that some drug users are not attracted to methadone or find it unacceptable. Council supports the development of any potential treatment that would bring dependent users into regular contact with treatment services and reduce the harm associated with current drug use.
HEROIN PRESCRIBING
Heroin can be used as an alternative pharmacotherapy for dependent drug users. Heroin has been available to dependent people on a prescription basis in the United Kingdom for many years. One expert consulted by Council indicated that it is now losing popularity.
Council received numerous submissions supporting provision of replacement heroin to dependent users in a medically controlled manner. Many of these submissions indicated that the social, emotional and health harms of heroin are largely a result of heroin's illicit status. These submissions argued that if heroin were available to dependent users in a controlled manner, more dependent users would be attracted into treatment. Heroin prescribing would also reduce dependent users' involvement with the criminal justice system and enables controls of both the quality of the product and its administration.
The National Centre for Epidemiology and Population Health and the Australian Institute of Criminology have been responsible for planning the research, scientific design and evaluation of the following question: 'Should a carefully controlled and rigorously evaluated trial be conducted to determine whether or not the prescription of pharmaceutical heroin (diacetylmorphine) is a useful addition to current maintenance treatment for dependent heroin users?' (Stage 2 Feasibility Research into the Controlled Availability of Opioids, 1995).
Dr Gabriele Bammer, Fellow, National Centre for Epidemiology and Population Health at the Australian National University has been responsible for overseeing the project and was asked to give evidence. Council was impressed by the level of attention to detail, the scientifically rigorous design of the preceding and ongoing research and the proposed design of the pilot projects. The ACT Heroin Trial represents one attempt to develop sound research based experience of the effect of offering heroin in a controlled manner to heroin dependent clients.
Council is of the view that the trial is justified on research grounds and should be supported by the Commonwealth. The trial will assist in determining if there are groups of heroin dependent users for whom the availability of a heroin treatment option is more effective and cost-effective than offering methadone alone. Individual and social outcomes, and attraction and retention rates in treatment, will be examined.
The trial involves three sequential stages. It is proposed that there be two pilots conducted in the ACT followed by a multi state clinical trial. The decision to implement each stage is contingent on the successful completion of the earlier stage. This approach is appropriately cautious.
The proposers of the trial acknowledge that the organisation and administrative requirements of a controlled heroin prescribing service are necessarily complex. Council is also concerned that these difficulties may only be surmountable at considerable cost, or reduction in the relevance of the service to potential users. Council believes that a careful assessment of the outcomes of each pilot and the final trial is required. Council accepts that, on the basis of evidence collected in each of the three stages, heroin prescribing may appropriately be considered for inclusion in the range of pharmacotherapies.
Council has concluded that Victoria should seek to further develop its methadone program and develop proposals for clinical trials of new drugs which may offer additional benefits as alternatives to methadone or in support of withdrawal programs. In Council's view, priority should be given to the development of new drug trials. It could be appropriate that Victoria be involved with the formal heroin trial in order to undertake comparative assessment of the alternative drug choices. A judgement on this matter may be required if the formal trial proceeds and work on trialing other options is sufficiently advanced in Victoria.
HARMFUL CANNABIS USE
Council has also been concerned about the level of cannabis use that occurs in our community. Some people who use cannabis persistently become dependent on it, and seek treatment to change their patterns of use. Council notes that very little is known about effective treatment approaches for cannabis dependence. Council believes there is a need to develop and evaluate appropriate, responsive treatments for this group.
3.6.4 YOUNG PEOPLE
Youth are a heterogeneous group most of whom will experiment with licit and illicit substances, most notably tobacco, alcohol and cannabis. Drug dependence is usually a long term and damaging process. Preventing young people commencing use or reducing the levels of misuse is one of the potentially most significant initiatives that could emerge from this investigation.
The vast majority of young people who try illicit drugs are simply experimenting, primarily with cannabis, and will not develop a dependency on this or other illicit substances.
Council is concerned about the situation of young people from diverse cultural and/or linguistic backgrounds who have problems with illicit drug use. While many schools and services are endeavouring to provide appropriate support, many other organisations appear unable to cope with cultural diversity coupled with illicit drug use. This can occur because the organisation is too 'stretched', or through a lack of knowledge in dealing with a culturally diverse clientele. This, in turn, may lead to a lower level of utilisation of services by these groups and poorer information about the harms caused by drug usage.
With respect to substance use it is possible to conceptualise young people as belonging to the following categories:
• At 12-14, people who may begin with some experimental use of drugs.
• At 15-17, experimental use continues but becomes interspersed with `binge' use.
• At 18-20, any problematic use of substances begins to become integrated into the young persons life.
• At 21-24, problematic use of substances becomes entrenched (McDonald, 1996).
The risk of young people developing serious problems with drug use is more likely if other areas of their lives have been disrupted. Disordered family relationships, social disadvantage and early and prolonged periods of homelessness are predictive of serious problems with substance abuse as a young person and in later adult life (Chamberlain, MacKenzie, 1985; Spooner, Mattick & Howard, 1995).
Polydrug use (particularly amphetamines, alcohol, Ecstasy, inhalants and abuse of prescription drugs) is also a feature of problematic adolescent drug use (Spooner et al., 1995; McDonald, 1996).
On the basis of substantial advice, Council is concerned about the capacity of services to respond to young people with drug problems. Service gaps are seen in the primary, secondary and tertiary intervention sectors.
Council received many representations about the lack of alcohol and drug withdrawal facilities for youth. There are also few other services able to deal with young people whose health and wellbeing are seriously affected by drug misuse.
Council's commissioned work on treatment concluded that youth rarely experience clinical dependence. They do, however, experience distress after episodic abuse of illicit drugs, particularly within the context of crises and significant disruptions to their lives.
As with adults, many young people in contact with the justice system have drug problems. Council agrees that there are large gaps in the network of services able to support young people, particularly those with serious drug abuse and related problems. Initiatives in the following areas,
implemented in an integrated fashion, would address many of these deficiencies. Outreach: Workers who have the capacity to provide:
• Secondary consultation to agencies who come into contact with youth who are experiencing problematic drug use.
• Direct service to young people who are in need of specialist assessment and support, or referral to a residential service.
• Case management and support with other matters likely to be of concern to the young person such as family issues, accommodation and linkage to a range of local services.
Training, professional supervision and consultation: Training should be provided to outreach and other key youth workers, to build the skill base and knowledge of the field. This training would need to be provided as part of the broader training proposed in section 3.5.3. Council is also convinced that professional supervision and consultation is required to maintain focus and enhance the skills and training expertise of youth workers in the community and correctional systems.
Intensive supportive care: The most effective way to support young people is within the networks and services where they feel most comfortable. Serious drug problems and the behaviours that can, from time to time, accompany them exceed the capacity of these services and young people are evicted or rejected. Council believes that with periodic and highly skilled support these services can be supplemented and assisted to retain their caring role through these crises. This support would have to be very flexibly provided given the range of different situations in which it may be required. There also needs to be a new residential treatment service linked to this outreach support. This facility, with a small number of beds, should be associated with an acute hospital because of the possible need for emergency medical and psychiatric services. Access to this facility would have to be carefully managed and linked to the outreach support services, and supported by a specialist drug and alcohol agency.
Research and evaluation: There is little systematic, research based knowledge about young people who have specific problems with drug use. There is even less evaluation of models of care that could form a basis for further development of youth services. Victoria has not had a systematic, clear service system for these young people. Various sectors including education, health, welfare and correctional services are involved in the care and management of young people who have problems with drug use.
Council believes that Victoria requires appropriate research in adolescent health and harmful drug use to support the design, implementation, practice and evaluation of a system of care and specific services.
Monitoring: Throughout this report the volatility of the drug market has been highlighted. Comment has been made in public hearings and expert consultations about the importance of having current and local knowledge about the drugs being used, particularly by young people, and their quality. A database is required which is both current and able to provide direct feedback to people in contact with users about the drugs. This database will also facilitate informed policy making at a state and regional level. The database will require resources in terms of pathology expertise and data collection, analysis and dissemination.
Council believes this model or approach is likely to engage youth who are 'hard to reach' and who may be involved or at risk of being involved with the juvenile justice system. It also aims to retain the young person in their usual social environment and thus has the capacity to address the variety of other problems that beset young people who use drugs.
3.6.5 CRIMINAL JUSTICE SYSTEM
PEOPLE IN POLICE CUSTODY
People held in police custody who have problems with illicit drugs are vulnerable, particularly with regard to withdrawal. Their withdrawal could be from an illicit drug or prescribed methadone. Unsupervised withdrawal can be medically dangerous. Police face a difficult task in recognising that someone is at risk from withdrawal, and in providing an appropriate service. In the time available to Council it was not possible to investigate this issue in detail. As concern has been expressed to Council which accepts the importance of the issue, Council believes a review of standing orders and current police practice is justified.
THE COURT SYSTEM
A significant number of people who have serious drug problems come into contact with the court system and subsequently the corrections systems (see section 2.2.3).
Some people are motivated to change their behaviour as a result of contact with these systems. The courts have the power to require people to access information and treatment as part of their disposition. The experience of imprisonment can also contribute to a person's willingness to utilise treatment services, particularly if doing so contributes to earlier release through parole. This means that, either directly or indirectly, the corrections system can play a critical role in facilitating contact with treatment services within the community, or by providing these services within the prison.
Council believes that the state can better capitalise on these opportunities and the infrastructure that currently exists. Utilisation of the opportunity will depend upon courts and the Parole Board having confidence in using treatment as part of their disposition. They will also depend upon community understanding the potential harm reduction benefits of treatment rather than other punitive options for many drug offenders.
COURT SERVICES
Council has received comment from judges and magistrates that 'on the spot pre-sentence expert advice' about the availability and suitability of treatment services, as well as a specialist assessment about the nature and extent of an individual's drug problem, is inadequate. In Council's view the court system would be well served by the establishment of a specialist court drug advice service.
This service would include specialist assessments that may facilitate improved judgements regarding possible and effective treatment options which can be put before the judge or magistrate. The benefit of such an initiative is likely to be better targeting of community based orders and diversion of more drug offenders from prison. Council is not suggesting that drug offenders should receive more lenient sentences than other offenders. Rather it is suggesting that the damage done in a prison environment can be significant, and the offender and the community could benefit if offenders can be safely supervised and treated effectively in the community. This is particularly true for first offenders who may be diverted from a life of continuing criminal activity.
COMMUNITY-BASED CORRECTIONS
Victoria has a significant number of people subject to community based dispositions. Many of these people have a treatment condition attached to their order (see section 2.3.3). The Department of justice has recently established a specialist treatment service targeted at younger offenders. The Department of Health and Community Services, which administers treatment required under section 28 of the Sentencing Act 1991, provides funding to ensure treatment is provided for some of these people. The department also coordinates the administration of services required by people ordered to attend an assessment centre under section 11 of the Alcoholics and Drug-dependent Persons Act 1968. These arrangements need to be reviewed because they are inefficient. All others required to receive treatment are referred to existing specialist treatment services that are expected to accept these referrals in the normal manner.
Council supports the principle that people required to receive treatment should be assisted in exactly the same way as those who use services on a voluntary basis; however, Council believes current arrangements are deficient in at least three ways. Most specialist treatment services lack the capacity to deal effectively with forensic clients and those attending on a voluntary basis. There are no arrangements that ensure that people referred by the courts gain the preferential access to services required to meet the requirements of the court. Thus, there is a high likelihood that inadequate or no services will be provided despite a court order. Secondly, there are few guidelines or protocols to guide community corrections staff or the agencies in managing these clients and fulfilling their obligations to the courts. Finally, there is almost no training provided for staff of treatment agencies regarding their forensic obligations to clients and community corrections staff. The reverse is also the case. Community corrections officers often have case loads which comprise a variety of client problems leading to diffusion of expertise. Council believes community-based corrections staff's management of people with substance abuse problems could be improved if at least two staff in each community corrections office were required to develop expertise in the substance abuse field, and form positive liaison relationships with local and statewide specialist drug and alcohol services.
Council believes that it is possible to improve arrangements to better manage the decision making and referral process which ensure that the network of treatment agencies is supported to meet its obligations. This can be achieved by enabling the proposed specialist court advice service to purchase treatment services from drug and alcohol services. As well as providing more people, dealt with by the courts, with the opportunity to receive adequate treatment, the new arrangements are likely to free up service capacity in these agencies for other people. Similar working arrangements are also likely to assist more effectively the Adult Parole Board in its decision making and post-release supervision.
PRISONS
The prison system attracts a population with substance abuse problems of a serious and lifelong nature. Some studies suggest up to 78 per cent of persons within adult prisons have a substance abuse disorder (Taylor & Gunn, 1993; Herrman, McCorry, Mill & Singh, 1989). This is particularly true of women in prison (Pathé, 1993; Hurley & Dunne, 1991; Miner & Gorta, 1987).
The prison environment is simultaneously a difficult environment in which to deal with drug issues, and a valuable opportunity for people to confront their drug use, provided adequate treatment and support is available.
Council has been advised that while the frequency of illicit drug use by people in prison is low, the harms done are substantial.
Council has also been advised that prison-based treatment services are currently subject to review. This review is very important as Council has substantial concerns regarding the adequacy and appropriateness of existing services. While Council wished to explore this area in greater detail, the current review provides a means for urgent and broadly based input to future development. Council urges that the information and advice flowing from this review be considered by a wide range of groups, including people involved in operating community and support services. Participation by these kind of groups will help to ensure that treatment options and standards replicate those in the community.
Council assumes that the discussion and planning proposed following the current review will inform requirements in specifications for any privatisation of prisons.
3.6.6 INTERSECTORAL ISSUES
People who have problems with illicit substances commonly face multiple problems. Further, many people with substance abuse problems also live in family groups caring for young children. There is a known interaction between substance abuse, child abuse and neglect, the criminal justice system, mental health, and the disability fields. This represents an opportunity to address the delivery of services across health and community services and the criminal justice system in a manner that genuinely endeavours to address the problems of people with multiple needs (Scott & Campbell, 1994). Such an approach requires services to forget their traditional boundaries and work together for the benefit of clients and their families requiring multiple services.
In contrast, services are generally organised and provided by specialist services with tight eligibility criteria. The drug field, in common with others, is grappling with ways to provide effective and integrated services. It should be an active partner in enhancing several services' capacity to assess and manage people with drug problems.
Council has been told of an ongoing issue between drug and alcohol services and psychiatric services concerning a number of clients who do not appear to fit readily within either service. Tensions have arisen in crisis situations, usually in the context of agencies in one of the service systems refusing to assess or accept people who are both intoxicated and apparently suffering an acute psychiatric episode. Council has been advised that attempts are being made to better manage these tensions by developing in-service protocols. Council supports these efforts.
The Department of Health and Community Services is currently developing or upgrading a range of protocols between key program areas. Protocols are being developed with Child Protection, Psychiatric Services and Supported Accommodation and Assistance Program. Protocols aim to establish a model of collaboration between services to assist people requiring the services of both programs. H&CS is also funding a small number of integrated service models. These initiatives are being monitored to assess their usefulness as models of integrated care.
Potential exists to increase the confidence and backup needed for health and welfare practitioners working in generalist settings, such as general medical practice and accommodation and community health centres. Council believes that shared care models of service and secondary consultation should be actively explored as a means of making more creative use of specialist and generalist services.
The Departments of Justice and H&CS are collaborating on the development of aspects of the community corrections system. These initiatives, while important, may not provide an effective response to current need. Proposed developments in the support systems for people with drug problems should be integrated rather than divided between departments.
3.6.7 CONCLUSION
Council believes that the proposals outlined in this section could have significant impact upon the range and quality of support and treatment services in Victoria. The impact will be maximised as the training, research and service evaluation initiatives also begin to take effect. Consistent leadership and coordination of these activities will be required. Many organisations, some prominent in the field, others newcomers, will need to be involved and to share the responsibility for the leadership and coordination tasks.
3.7 Law Enforcement and Policing in a Harm Minimisation Strategy
Drug law enforcement is a national concern. Considerable public resources are invested in enforcing existing drug laws. In the time available to Council, only a limited and general assessment of the effectiveness of law enforcement has been possible. Law enforcement in this area is necessarily complex and the strategies, priorities and operational details are often confidential. Council has had the benefit of advice from senior officers in Commonwealth and State law enforcement agencies. It has also had the benefit of access to several, very recent analyses and reviews commissioned by law enforcement agencies. Council has been reliant, to a substantial degree, on the material provided by these sources.
As detailed in section 2.2.3, law enforcement includes policing, the courts and corrections system and it consumes the vast bulk of the State's investment in responding to illicit drug use. The direct costs relate to cases where formal drug offences were the most serious charge. These costs account for 10.6 per cent of all offenders processed by police (monthly Criminal Justice Statistics November 1995). They also account for 8.5 per cent of all charges in the Magistrates' Court and 5 per cent of matters dealt with in higher courts. Some 6.5 per cent of people in the correctional services system also have drugs as the most serious charge (monthly Criminal Justice Statistics November 1995).
These figures, while significant, understate the case. They exclude matters where drug offences were committed but were not the most serious charge. They also exclude a range of offences committed as a consequence of drug use, most commonly burglary and theft committed to support a drug habit. They also exclude crimes of violence committed as part of the drug trade, or as a consequence of a marginalised lifestyle. Council has heard that informed estimates indicate that some 70 per cent of burglary and theft offences are committed as a consequence of drugs.
Enforcing the drug laws and dealing with crime, arising from drug use and trafficking, is a major priority for the police, courts and corrections system. It will clearly remain a priority for the foreseeable future. The issues before Council relate to defining strategies that gain maximum benefit and more effective use of existing resources.
3.7.1 SCOPE FOR EFFECTIVENESS
Estimates of the rate of detection and seizure of heroin entering the country vary from 1 per cent to 10-15 per cent (Royal Commission into Drug Trafficking, NSW, 1979). Australian Customs Service barrier examination rates are fairly low (9 per cent of passengers searched and 1 per cent of containers 1992-93) (ACS, 1993). The drugs, whether domestically made or imported, are often relatively easily concealed. Finding them is essentially a very difficult task. There are clear limits to the capacity of even the most efficient enforcement arrangements (Reuter, 1993).
The best evidence available indicates that all law enforcement bodies achieve relatively limited success with regard to reducing supply. While regrettable, Council accepts the reality and believes that this information needs to inform the community's expectations regarding performance of law enforcement agencies. Reorganisation, and a change of strategies, tactics and priorities can help reduce demand and contribute to harm reduction. This would enhance the overall performance of law enforcement. Expanding the attempts of law enforcement to significantly reduce supply will achieve only marginal gains.
In considering police effectiveness, Council noted that inquiries held in many countries and in other states of Australia have confirmed that some degree of corruption is an almost inevitable consequence of the existence of prohibition. However, the investigation of this matter in Victoria is beyond the resources available to Council. While Council was presented at public hearings and in submissions with a range of information and comment relating to police effectiveness, it has neither sought nor received indications of systematic corruption in the Victoria Police with respect to illicit drugs.
3.7.2 PRIORITIES
Data available to Council indicates that drug use and possession charges considerably exceed those for trafficking and related charges (Figure 15). Council understands that most prosecutions relating to possession and use of drugs do not arise out of proactive drug law enforcement. Most charges concerning use and possession of small quantities of illicit drugs result from their discovery, incidentally, during enforcement that is related to other matters. Surprisingly, there is a considerable number of people charged where possession or use of drugs is the only, or the most serious, charge pursued by police. The numbers of people whose most serious charge relates to possession or use of cannabis is five times that whose most serious charge relates to trafficking.
There are substantial cost and other consequences in using the criminal law to deal with personal use or possession of any drug. In the context of a harm minimisation strategy, it is unlikely that this response will further reduce harm or represent the most cost-effective approach. There is also limited scope for `deterrence' if the chances of detection are low and unpredictable.
Council has heard that it is not current police policy to pursue drug users. Concerns were expressed to Council that this policy is not uniformly carried through to the community level.
According to advice received by Council, a major emphasis of law enforcement strategies in recent years has been on prosecuting major and large-scale participants (`Mr Bigs') in the financing, importing and trafficking aspects of the drug trade. Evidence suggests that strategies employed have not been particularly successful. Information about the proportion of matters relating to use or possession, as distinct from trafficking, is an indicator of poor targeting. A further indicator is that a high proportion of trafficking charges is not proven. In 1995, 38 per cent of trafficking charges were not proven, over three times the proportion for possession and use charges.
It was suggested to Council that the relative lack of success in pursuing large-scale traffickers, financiers and importers may reflect the relative absence of major funders and controllers in the Australian drug market. Council has also heard that low levels of success are a consequence of the high resource costs and risks of the enforcement operations involved. It was made aware of real limitations in the extent to which drug enforcement agencies can demonstrate their effectiveness in this regard (ABC!, 1995). It was also argued that restricted powers available to police, particularly with respect to search and seizure, have hindered their ability to move against large-scale and sophisticated traffickers. Council is not in a position to adequately assess all of these comments and explanations.
According to some reports, experience in the USA is similar and there has been a long-term move away from focussed pursuit of large traffickers on the grounds that success rates have been very poor.
3.7.2 THE APPROACH
It is clear that the complexity, scale and volatility of the market for illicit drugs presents major challenges to large and traditional organisations such as the police. Council is aware that apparently inescapable tensions between drug law enforcement and harm minimisation place police in a difficult position. Even operations directed at the seizure of drugs and disruption to supply can contribute to a range of unintended consequences.
There is some inconsistency between the stated priorities of police and the data about the patterns of arrests that result from police activity. This suggests there is a need for on-going priority setting, policy communication, training, and implementation management.
Active policing can contribute to reduced demand and reduced harm through misuse of drugs. Council has heard evidence that indicates that three broad areas deserve priority.
COMMUNITY POLICING
Council has heard a good deal about community policing as a potentially useful approach to the drug problem at a local level. While not having time to develop a sophisticated definition, Council believes community policing to mean that police engage the public in problem solving, and consider their input in determining and evaluating operational policy and procedures.
Community police involvement can disrupt drug markets and increase the difficulty with which buyer and sellers can get together. It has potential benefits and costs, particularly where vigorous activity in one area simply displaces drug dealing to another area or to another drug type. Council believes that the goal should be to maintain a constant presence and pressure that discourages low level dealers and novice users. These activities can form an important element of an area-based harm minimisation strategy, particularly where they are developed and implemented in association with local community health, and community service organisations. Senior police have confirmed their commitment to working with local communities on issues such as drugs.
Council has heard considerable comment about effective street level enforcement and engagement with local agencies, and some strong criticisms about police practice. Council was provided with evidence of high-quality internal collaboration at operational levels There was also information that indicated difficulties occur with respect to the sharing of information about patterns of drug availability, use and trafficking, and the utilisation of this information to formulate comprehensive strategic responses. If this advice is correct, steps should be taken to improve strategic planning and cooperation within the Force, particularly between the Drug Squad and specialist district support groups, and also in collaboration with community agencies and the community.
Street level enforcement also provides information and intelligence that will contribute to the pursuit of major participants in the trade.
MAJOR TRAFFICKING
As noted earlier, State and Commonwealth agencies have a role in pursuing people with a significant stake in the illicit drug industry. Council has heard about the sophisticated operations that are involved. It has also been advised that the trade is diverse and flexible. It has a rapidly changing structure that law enforcement agencies find difficult to tackle in anything other than a reactive way.
Council has heard that working relations between State and Commonwealth agencies have improved in recent years. It is clear that improved collaboration is a prerequisite to enhanced effectiveness in charging and convicting the major players. Council believes that this area deserves continued emphasis, in particular to ensure coordination and cooperation to enhance enforcement efforts.
Some advice suggested that dealing effectively with the big players in the drug trade requires different expertise than is commonly available in police forces around Australia. Council was impressed with the multidisciplinary task force models used by the National Crime Authority, Australian Federal Police and groups investigating white collar crime.
THE MONEY TRAIL
There is international recognition that the profits from the drug trade are large and that tracing money movements may assist in the apprehension of major figures in the trade. Tracking of this kind is a necessary precondition to any asset confiscation arrangement. There is international agreement about the need for nations to establish legislation to control and report on funds movement. Australia has acted on this agreement.
Council has received evidence and submissions which show that Australia has some of the most effective laws and administrative machinery (AUSTRAC) for monitoring national and international money movements. Council has been told that police may be able to make more effective use of the data from the Australian tracking system (Wardlaw, oral submission, 1995).
Council has been advised in submissions that the effectiveness of this approach may be improved by broadening the definitions of transactions and the number of agencies required to report. If obstacles exist in identifying beneficial ownership of investments, attention should be given to identifying means by which these can be overcome in retrieving the proceeds of trafficking. The potential benefits to be accrued may be significant and Council believes that further investigation of this area is justified.
DEVELOPING THE INFRASTRUCTURE TO ENHANCE POLICING
Council agrees that police make important contributions to harm minimisation. For some officers this is through work outside hours of duty but it could be seen, increasingly, as central to community policing. Council wishes to enhance that contribution.
Council has been made aware of the problems that can emerge when police activity is undertaken in the absence of impact and outcome-related data. This is especially the case regarding regional data that are most important for shaping and assessing harm minimisation activities at the local level. This data relates to:
• Consumption patterns.
• Health consequences.
• Violence associated with trafficking.
• The impact of law enforcement on use and supply.
• Crimes committed in relation to the consumption of drugs. These data are required for planning and
implementing law enforcement within a harm minimisation strategy.
Comment has been made on the inherent difficulty for police, particularly those working at street level, to meet the goals of a harm minimisation approach. This suggests the need for more training in harm reduction strategies and their implications for police work. Any such training would need to have a practical, as well as theoretical, aspect. Council believes training is a crucial element of its strategy and makes reference to this matter in more detail in section 3.5.3 on professional development. Police are a priority group in this context.
Comment was also made earlier about the importance of ensuring police engagement with, and encouragement of local community involvement in responses to drugs. During Council's consultation, it became apparent that levels of commitment to and involvement in drug-related community work varied considerably between local areas. In part, this appeared to reflect the ability and enthusiasm of particular officers. In other cases, much depended on success of local police-community liaison initiatives such as Police Community Consultative Committees. While these initiatives are valuable, there is need for a more systematic and sustained program of community policing and inter-agency cooperation with respect to drug use, particularly at local and district level.
Council does not believe that any single model for community development would be appropriate in this respect, as the variability of local problems, resources and appropriate vehicles needs to be recognised. It is proposed that further development of police strategies in this field provide increased guidance and support for police-community initiatives aimed at reducing the harms associated with illicit drug use. The issue of community involvement in drug issues is dealt with in the discussion regarding information and education (see section 3.5.4).
Council was made aware of the important contributions made by many police officers at the community level, including work in educational, welfare and recreational contexts. It was indicated on a number of occasions that such work is not highly valued in the Force, and that officers involved received neither adequate career recognition nor sufficient resourcing for their efforts. Council has heard of the approach to community policing being developed in Amsterdam and was impressed with its positive and preventive approach.
In view of the potential contribution of such activity to harm minimisation, Council believes that the resources available to support this work, and career recognition provided to officers involved, should be investigated and that appropriate responses to identified deficiencies be developed as a priority.
Council's assessment that law enforcement is relatively ineffective in controlling the supply and use of illicit drugs is not a criticism of the agencies involved. The time and data available to Council has not enabled any detailed judgement regarding the performance of any of the law enforcement agencies. The criticism is largely based on the structural difficulties of the task in the circumstances, and the limited amount of evaluative data available.
Overall, the contribution of law enforcement to the management of illicit drug use in Victoria needs to be more closely integrated with harm reduction strategies currently endorsed by the Victorian and Commonwealth Governments. Structural and process reforms should focus particularly on four major tasks:
• Ensuring that a clear, comprehensive and coordinated strategy and operational guidelines on drug activities are in place within the Victoria Police.
- Developing an appropriate monitoring and evaluative mechanism, with clear, well-defined success indicators.
• Increasing operational integration between police, and health and community agencies, that is designed to ensure collaboration on harm minimisation strategies and priorities at all levels, particularly in responding to users within local communities.
- Improving training on policing in a harm minimisation framework.
3.8 The Law
Reform of Victoria's drug-related legislation was one of the recurring themes in submissions to Council. A range of groups and experts alerted Council to perceived weaknesses, contradictions, dilemmas and tensions with current laws; other submissions argued strongly that current prohibitions should remain.
Legislation considered by Council included:
• Drugs, Poisons and Controlled Substances Act 1981.
• Crimes (Confiscation of Profits) Act 1986.
• Road Safety Act 1986.
• Sentencing Act 1991.
3.8.1 LEGISLATIVE OPTIONS
Legislative options were classified by Council using a framework developed by the South Australian Royal Commission into the Non-medical Use of Drugs (Sackville, 1978). Available options are:
• Total prohibition.
• Prohibition with civil penalties.
• Partial prohibition.
- Regulation.
• Free availability.
Under a system of total prohibition, the use, possession, cultivation, importation, sale and distribution of any amount of a specified drug is treated as a criminal offence. Current Victorian legislation and legislation in most other states reflect a policy objective of total prohibition. Despite significant resources directed toward achieving this goal, widespread use and trafficking occurs in illegal drugs.
Under the prohibition with civil penalties option, penalties for possession and use of small amounts of drugs for personal use are dealt with by penalties such as a fine, rather than criminal sanctions including imprisonment. Criminal sanctions still apply for possession, manufacture and trafficking of larger quantities of drugs. Examples are the South Australian Cannabis Expiation Notice Scheme,
introduced in 1987, the similar scheme introduced in the Australian Capital Territory in 1992, and the scheme to be introduced in the Northern Territory later in 1996. In the USA during the first half of the 1970s, criminal penalties for marijuana possession were removed in 11 States, which cover one-third of the nation's population.
Partial prohibition seeks to maintain controls on the production and trafficking of drugs while eliminating offences for possession and personal use and, in the case of cannabis, cultivation of plants for personal use. A number of countries (for example, Spain) have followed this model (McDonald et al., 1994).
Government regulation would broadly reflect current arrangements for tobacco, alcohol and many pharmaceutical products where Government, to a greater or lesser extent, controls production distribution and sale. Regulatory structures generally provide controls not only over purchase, but also over quality, standards and marketing. In respect of cannabis, the Netherlands exhibits some elements of the regulatory model. Free availability would mean the absence of any legislative or regulatory restrictions on a drug's production, sale or use.
The alternative legal responses to drugs form a continuum. The practical policy decisions regarding a particular drug involve who should be allowed to use it, under what circumstances, for what purposes, with what restrictions, and what sanctions are to be applied to violations of those rules, rather than simply whether the drug should be called `licit' or 'illicit'.
3.8.2 CHOOSING BETWEEN OPTIONS
Differences between supporters of existing law and those advocating alternative approaches revolve around three key issues:
• Assessment of benefits and costs of current laws, and whether a different policy mix would achieve greater benefit at an acceptable cost.
• The projected impact of changes to existing laws on demand and use.
• The health risks of the different illicit drugs. Issues include whether risks associated with a particular drug are serious enough to justify current sanctions, and how the known risks compare with well-documented consequences of misusing alcohol or tobacco.
Evidence relating to each of these issues is canvassed in this section. Other views, including a moral perspective that drugs are evil, were advanced in several submissions.
BENEFITS AND COSTS
A comprehensive assessment of benefits and costs of different responses to drugs concludes that drugs are a community problem for which there is no solution—only better or worse outcomes (Kleiman, 1992; Reuter & Caulkins, 1995). Each available policy regime increases some harms and reduces others. Victoria's current laws, for example, mean that prohibition and law enforcement, rather than drug use, generate the overwhelming proportion of direct costs and arguably most of the harms arising from drug misuse. At each step along the chain of production, distribution and consumption, illicit drugs divert law enforcement time, energy and resources away from other responsibilities with little apparent impact on either drug supply or use.
The fact that prohibitionist drug laws and law enforcement cannot eradicate, or even significantly reduce drug abuse is not necessarily a reason to change. Current laws aim, and arguably succeed in deterring many people from trying drugs and restrict their availability. However, these achievements must be balanced against not only the direct costs of law enforcement but a range of health and community costs, including the isolation of many drug-dependent people from health services.
Many submissions drew Council's attention to consequences of the failure of current legislation to support the harm minimisation objectives of the Victorian and national drug strategies. These include:
• Constraints on effective drug education, particularly by grouping cannabis with more harmful drugs, rather than alcohol and tobacco.
• Increased health risks when addicts are reluctant to call for emergency medical assistance (Zador et al., 1996).
• Corruption of enforcement agencies (Fitzgerald 1989, Wood 1996).
• Alienation of young people from the police and courts required to enforce prohibition.
• Individual and community costs caused by reduced educational, employment and other opportunities as a result of convictions for possession and use (Sackville, 1979; McDonald & Atkinson, 1995).
A recent attempt was made to consolidate available information about the various harms associated with drug use and whether they arise from drug use itself, laws or law enforcement. This information is presented in table 24 and suggests that prohibitionist laws and their enforcement create more harms and costs for a community than the known harms of drugs themselves. However, any overall assessment of whether harms are greater than benefits is constrained by the following factors:
• There is an absence of relevant empirical evidence of many of the harms that are at least quantifiable in principle.
• Many of the quantifiable harms cannot be easily translated into monetary terms.
• Many of the harms are inherently intangible and subjective.
• It is easier to perceive the presence of harms than their absence; in other words, policy may be blamed for harms that it allows or creates, but gets no credit for harms it reduces or prevents.
Three important conclusions emerge from McCount Reuter & Schelling's assessment of different legislation and law enforcement responses to drugs:
• Until better data is available, few confident assertions can be made about what will work more efficiently.
• Preference for a particular legislative response to drugs is often guided by a moral or ideological perspective rather than by significant disagreement about the findings of available evidence.
• Legislative responses can vary among different drugs depending on the level of harm they pose to society, and whether laws can be enforced in ways that achieve objectives at an acceptable cost.
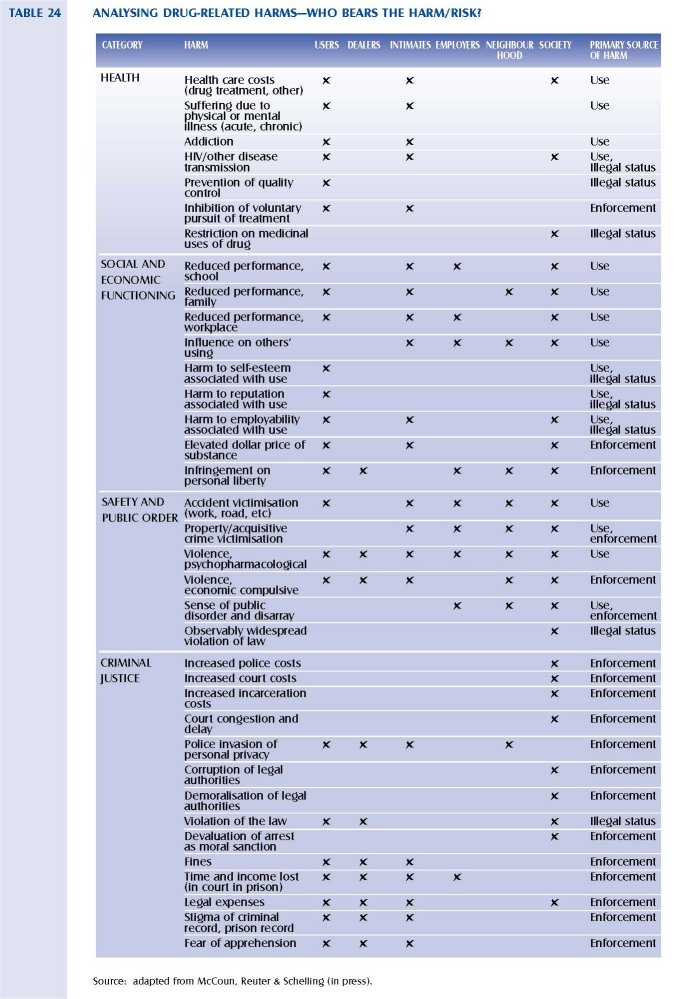
IMPACT OF LEGISLATIVE CHANGE ON DEMAND
While analysis of the impact of changes to existing laws is significantly constrained by a lack of reliable data in respect of heroin, amphetamines and cocaine, more comprehensive and reliable data is available to enable assessment of the likely impact of changes in respect of cannabis. Available data indicates:
• Cannabis use is not significantly constrained by current law. An estimated 30 per cent of Victoria's population have used it and it is the most widely used psychoactive drug after alcohol and tobacco (table 4A).
• Removing criminal penalties for minor cannabis offences in South Australia, the USA and Europe has had little impact on consumption (Atkinson & McDonald, 1995; Reuter & MacCoun, 1995; Korf, 1995; Reuband, 1995).
• Removing all penalties for minor cannabis use and possession offences in the Netherlands also appears to have little impact on consumption (Korf, 1995).
• Small changes in legislative provisions on cannabis also appear to have little impact on patterns of use, although the evidence is less clear in this area (Atkinson & McDonald, 1995).
• More generally, a recent cross-European comparison of drug use and drug law (Reuband, 1995) concluded that there is no clear-cut relationship between drug law and drug use. For example, while cannabis is readily available through the Netherlands' 2500 coffee shops, drug use by adults and youth is basically the same as in Germany where no such availability exists (Reuband, 1995).
HEALTH RISKS
Existing knowledge of health risks associated with use and misuse of existing drugs is considered in chapter 2. While there are excellent reasons why use and misuse of all illicit drugs should be discouraged, prohibition, particularly in relation to marijuana, has not achieved this result. Council believes an alternative approach should be considered in an effort to minimise use over the long term. More generally, if minimising harm from drug use remains the primary policy goal, early intervention and treatment should be developed as the first level response to drug abuse. Health risks associated with imprisonment for drug-related crime reinforce the current role of prison as a last resort for offences involving only drug use and possession. Information available to Council supports advice from police, magistrates and judges that current law enforcement practice means that almost no Victorians are jailed when the only offence is drug use. Council believes this practice should be made explicit and strengthened with earlier and better diversion to assessment and treatment services.
3.8.3 APPROACHES TO CANNABIS LAW REFORM
In its 1994 report, Cannabis and the Law in Queensland, the Criminal Justice Commission (CJC) assessed three legal options for dealing with cannabis: legalisation, retention of existing laws; and the introduction of an expiation notice scheme. In summary, its conclusions were:
• There is an overwhelming case for modifying the existing Queensland offence and penalty structure for dealing with minor cannabis offences.
• An expiation notice scheme should not be adopted in Queensland.
• The current Victorian model of adjourned bonds provides a useful starting point for developing a statutory scheme for Queensland.
The CJC arguments against the expiation option, along South Australian lines, are:
• The levels of penalties under the South Australian arrangements are too low.
• The South Australian scheme relies on the threat of a criminal conviction to induce expiation.
- In practice, the South Australian system seems to have caught up a larger number of people than would have been charged under earlier laws.
• There is no hierarchy of penalties for repeat offenders.
The Queensland CJC was attracted to Victorian provisions for a sentencing option for first-time cannabis offenders of an adjourned bond as:
• It allows for more substantial penalties to be imposed on second and subsequent offenders.
• The bond constitutes a formal denunciation on behalf of the community of drug use as unacceptable behaviour.
Arguments for and against different approaches revolve around issues such as whether any realistic regime will significantly deter consumption, what penalties best reflect the level of community concern about the health and other risks associated with marijuana use, and whether the costs of enforcing the law can be justified against competing demands for law enforcement resources. While the South Australian scheme was devised to reduce court costs, higher than projected failure to expiate fines has created additional court work and associated costs. Current Victorian arrangements reduce no police or court costs. The Queensland Criminal Justice Commission estimates of the cost to Queensland of apprehending and prosecuting people possessing cannabis was, on average, around $320 a case. If Victorian costs were broadly comparable, prosecution of cannabis possession and use would cost the criminal justice system at least $6.5 million a year.
Council also considered a range of related issues in assessing options for legislative reform relating to cannabis. These included:
e The possibility of different legal responses to different forms of cannabis. For example, should the same restrictions apply to marijuana as to other cannabis products?
• Whether adults should have less constrained access to marijuana, with tighter restrictions remaining for young people.
- Whether drug use posed sufficient risks in operating work-based equipment or driving cars to justify specific restrictions and testing procedures.
• If possession and use were decriminalised, should the drug be able to be sold openly? In Amsterdam, for example, not only is marijuana able to be used without risk of penalty, but it is sold openly in the `coffee shops'.
Council's conclusions on these issues are identified in its recommendations.
3.8.4 IMPACT OF INTERNATIONAL TREATIES
Any changes to existing legislation and/or penalties will need to take account of obligations entered into by the Australian Government under international treaties. The drug conventions ratified by Australia (see section 2.2.1) oblige the Commonwealth Government to ensure domestic laws are consistent with conventions. While State Governments are not directly prevented from passing or retaining laws that are inconsistent, they generally abide by the obligations. However, where a law is inconsistent, it is open to the Commonwealth Government to override the state law (Criminal Justice Commission, 1994).
The Single Convention on Narcotic Drugs 1961 codified all existing conventions and obligations of the nations that were parties to the convention. It also introduced an international prohibition in relation to cannabis. Within the various conventions, cannabis is listed alongside more dangerous substances. This labelling has arguably contributed to the confusion and misinformation about cannabis and its
effects (Criminal Justice Commission, 1994). Certainly on available evidence, the association of cannabis with more dangerous and addictive drugs such as heroin is difficult to justify.
While there are diverging legal opinions about what the conventions require, the Queensland Criminal Justice Commission concluded that legalising possession of cannabis for personal use would be outside convention terms (Criminal Justice Commission, 1994). However, there is less agreement about what the conventions require in terms of severity and types of sanctions. A former President of the New South Wales Court of Appeal, the Hon. A.R. Moffitt, QC, has argued in a paper submitted to Council that the expiation schemes in South Australia and Australian Capital Territory breach the international conventions. Another view is that the combined effect of the conventions preclude only one option: legalisation or total deregulation of drugs (Woltring, 1990). An opinion obtained from the Commonwealth Attorney General's Department by the Queensland Criminal justice Commission, concluded that the South Australian approach is consistent with the 1961 and 1988 Conventions (Criminal justice Commission, 1994).
Internationally, parties to the conventions have a variety of approaches for dealing with cannabis ranging from 'administrative' decriminalisation in the Netherlands, to decriminalisation at different times in Italy and Spain. Council is not aware that any action has been taken against these regimes.
The most recent convention (1988) also provides, in appropriate cases of a minor nature, the Parties may provide, as alternatives to conviction or punishment, measures such as education, rehabilitation or social interpretation, as well as, when the offender is a drug abuser, treatment and aftercare' (UN Convention 1988, Article 3, section 4).
Drug offences constitute a significant proportion of the current workload in Victoria's courts. In 1994, possession and use of a drug of dependence were respectively the third and fifth most frequent charges heard in the Magistrates' Court. Of the 26,077 drug offence charges finalised in the Magistrates' Court during 1994, nearly 80 per cent were for consumption-related offences, rather than provision and trafficking. In Victoria's higher courts, 5 per cent of total charges finalised were for drug offences, although, more serious cases were heard in higher courts. Around 90 per cent of all charges related to drug provision rather than drug consumption.
While data provided to Council did not allow offences to be distinguished between different drugs or first from subsequent offences, imprisonment is the penalty in only a small minority of drug consumption cases. just over 2 per cent of individuals convicted of 'drug consumption' in Magistrates' Courts were sentenced to gaol, and nearly 91 per cent received a fine or a bond. Drug provision (including trafficking) offences were dealt with more severely in Magistrates' Courts, with more than 21 per cent of those convicted receiving a custodial (7.8 per cent) or suspended custodial (13.7 per cent) sentence. In the Children's Court, trends over the 1991-94 period indicate greater use of community-based supervisory orders as well as fines or good behaviour bonds.
3.8.5 SENTENCES AND PENALTIES FOR DRUG OFFENCES
While large numbers of Victorians are in prison for drug-related offences, correctional services figures confirm the small number of people in prison for drug consumption. At 30 June 1995, a total of 22 prisoners were incarcerated for drug consumption offences. Australian Institute of Criminology 1993 Prisons Census data also indicated that Victoria's rate of drug consumers in custody, per 100,000 population, was 0.2 compared to 1.9 in NSW and 0.9 in Queensland.
While Victoria's figures for 'drug providers' in custody remained well below the New South Wales rate, they were more than double that of Queensland. At 30 June 1995, a total of 259 Victorians were in prison for 'drug provision' offences. While 1994-95 data on sentence length were not available to Council, average 'drug provision' sentences were around five years between 1990-91 and 1992-93.
The Council is aware also that the Attorney General is considering introducing into the Sentencing Act 1991 the concept of a 'serious drug offender, with consequences similar to those for serious sexual and violent offenders (see s.3 Sentencing Act). If persons are convicted of a serious drug offence (that is importing, cultivating, manufacturing or trafficking in commercial quantities) and have two or more convictions for similarly serious nominated drug-related offences in the past for which they have received a sentence of imprisonment, they could become a 'serious drug offender. When classified as a serious drug offender, certain sentencing consequences could be attached (see s.10 of the Sentencing Act). Taking into account the fact that the abolition of remissions would no longer apply, sentences would also be cumulative, and the sentencing principle of proportionality would not apply.
Maximum penalties are already severe under the Drugs, Poisons and Controlled Substances Act 1981, with trafficking attracting a penalty of up to 25 years and a fine of $250,000. However, such sentences are rarely imposed and a number of submissions to Council argued that some penalties did not reflect the seriousness of the offence. Other submissions to Council suggest that any changes proposed to the Sentencing Act to create a category of serious drug offender should seek to distinguish addicts trafficking at street level to support their addiction from larger scale traffickers. Council was not able to explore in detail reasons for variations in current penalties. However, further investigation is required of the levels and patterns of sentences actually imposed by courts for drug trafficking. Review findings should inform government decisions about whether penalties imposed by courts are appropriate.
3.8.6 DIRECTIONS FOR REFORM
After careful consideration of evidence available to it, Council concluded that some changes should be made to existing provisions of the Drugs, Poisons and Controlled Substances Act 1981. Proposed amendments are part of a much broader strategy developed by Council, and have been guided by Council's conclusions that:
• Some existing laws have created harms and costs greater than those that result from the drugs themselves.
- Criminal law and criminal sanctions will continue to fail to reduce supply of illicit drugs and will have little impact on use.
• Many young Victorians' lives are seriously damaged by the consequences of a combination of their drug use and their community's response to it.
• Respect for laws can be undermined when a significant portion of the population is committed to doing something that the government makes illegal. While community views and behaviour strongly support existing laws relating to heroin, amphetamines and cocaine, they are more divided on cannabis.
Council has also concluded that changes to laws relating specifically to marijuana will enable more effective education and health promotion. The broadly comparable risks of tobacco, alcohol and marijuana should be explained to young people free of the ignorance, misinformation and confusion that now differentiates learning about licit and illicit drugs. Resources currently devoted by police and courts to detecting and prosecuting marijuana offences will be available for other responsibilities. Recommended changes to cannabis cultivation laws may also weaken links between marijuana consumption and trafficking in drugs such as heroin and amphetamines.
3.8.7 ROAD SAFETY
One of the principal concerns arising from the short-term effects of cannabis use is its intoxicating effect, and the consequent impairment of motor skills and the ability to perform complex tasks, like operating machinery and driving. Submissions to the Council raised serious concerns about the risk to the community posed by drivers under the influence of drugs. Widely reported current use of cannabis highlights this concern.
Council is aware that this issue is being considered in detail by the Victorian Parliamentary Road Safety Committee. The committee is expected to report on the issue of drugs and road safety in May 1996. Implementation of Council's recommendations on road safety should be considered alongside the Parliamentary Committees report.
Evidence available to Council indicated that drugs other than alcohol were present in significant proportions of drivers killed in road accidents, although the contribution of an individual substance to the accident was unclear. The major drug types present in such drivers were cannabis, amphetamines, benzodiazepine, minor tranquillisers, heroin and methadone. Evidence concerning the impact of cannabis use on driving is equivocal. Hall, Solowij & Lemon hold that cannabis use in isolation increases the risk of a driver being involved in a road crash, while Chesher, in a study for the Parliamentary Road Safety Committee, suggests that risks are increased only by the use of cannabis in conjunction with alcohol (Chesher, 1994).
While driving a motor vehicle under the influence of any drug is prohibited under the Road Safety Act 1986, significant research and development work is required before police action could match current responses to alcohol and driving. This would include a test to detect short-lived metabolites of cannabis products in saliva and breath. When developed, this would allow the introduction of roadside testing for cannabis in a manner comparable to alcohol breath testing.
Driving dangerously, recklessly or carelessly are already offences under the Road Safety Act. Council believes that learner and provisional permit drivers found guilty of such an offence, and determined to be under the influence of marijuana, should automatically be disqualified from driving for an extended period, and required to participate in education programs. Protocols should be developed to assist the policing of these offences.
3.8.8 CONFISCATION OF PROFITS
Amendments to the Crimes (Confiscation of Profits) Act 1986 were also advocated to Council. The Justice Department's submission described the current Act as unnecessarily complex and difficult to implement, and it had not provided an adequate procedural structure for decision making. Particular attention was drawn to the lack of any body with general responsibility for operation of the scheme. Presumably in response to these acknowledged weaknesses, the Attorney General established a working party in August 1994, chaired by Mr Peter Faris, QC, to review the Act. While Council has been advised that the working part submitted a preliminary report in October 1994 and its final report in December 1995, copies of neither report were available until after Council had considered this issue.
Legislation to enable confiscation of profits of drug trafficking is widely regarded as an important tool in efforts to control drug crime. However, international experience suggests that the translation into legislation requires careful scrutiny and a realistic assessment of the likely benefits. Experience to date suggests that whatever benefits legislation has in depriving individuals of profits and providing government with additional funds, it has had little impact on deterring the supply of illegal drugs. Any wider reforms recommended by Mr Faris's report should be considered carefully to ensure they will achieve the legislation objectives at an acceptable cost. In the interim priority should be given to ensuring the objectives and intent of the current Act are able to be met, and administrative arrangements are in place to operate Victoria's confiscation of profits scheme as effectively as possible.
3.8.9 DRUG COURTS
Council's attention was also drawn to American experience with 'drug courts'. Although there are a number of distinct models in the more than 100 courts currently in operation, they all share four characteristics: defendants are diverted by the courts to drug treatment shortly after arrest; judges are closely involved in monitoring the defendants' progress; judges, prosecutors, defence lawyers, treatment providers and probation staff run the court as a team; and relapses are accepted as part of the treatment process and not considered an indication of failure.
Council has discussed elsewhere in this report ways to strengthen court access to specialist advice and expertise about appropriate responses to drug offenders. Development and implementation of protocols, and improved working liaison between courts and treatment services offer the prospect of improved outcomes for all parties. With such reforms in place, the additional benefits of specialist drug courts within Victoria are unclear. However, evaluation of the American experience should be monitored and if appropriate, easily adopted aspects integrated into Victoria's arrangements.
3.9 Infrastructure
A diverse range of government agencies and community organisations are necessarily involved in responding to illicit drug use and misuse. The potential for inconsistency, service gaps and unintended consequences across these sectors is considerable. The consequences of service system failures for potential and current users are significant.
The need for a structure to manage drug policy has been recognised in Victoria and Australia. Council's observations in relation to structural arrangements in the area of illicit drugs are:
• Australia is recognised worldwide for the enlightened pursuit of harm minimisation policies. Within Australia, Victoria is recognised as having played a lead role in the development of a range of multifaceted harm minimisation initiatives that are now taken for granted. These have often involved the regulation of legal drugs. Less has been achieved regarding illicit drugs.
• The harm minimisation policy framework and many associated structures and programs at both national and State level are sound, although there are opportunities for significant improvement.
• There is widespread support for attempts to manage and coordinate efforts to address illicit drug issues and reduce the harms of drug use. This provides an important base that can be used to develop agreed strategies for action. However, there is considerable debate about how this should be achieved.
• There is strong and well informed support for harm minimisation policies at senior levels of the relevant departments. Council considers this is a sound foundation for future efforts.
• Council has been made aware of possible structural and functional weaknesses in the current arrangements. The current structures seem to have emphasised cooperation at the expense of leadership. The intersectoral approach inherent in the delivery of the State Drug Strategy, with its multiple portfolio approach, has potential weaknesses:
- Opportunities for unintended consequences and gaps in delivery may develop and go unchecked.
- Shared responsibility may lead to shared priorities but not high levels of ownership in any one portfolio or across portfolios. Illicit drugs is an important, but small, issue confronting large State government departments.
- There are difficulties in maintaining momentum on many initiatives because agencies work at
different rates and have levels of effort and emphasis without review or critical scrutiny.
- Government departments are not always well equipped to manage the tension created by conflicting community views, particularly where there is no strong evidence to support a particular course of action.
While Council has had limited time and scope to address this issue in depth, there is broad agreement that effective action in response to drugs:
• Needs public engagement and support.
• Involves a wide range of government departments and community agencies.
• Requires coordinated work at state, regional and local levels.
• Depends on integrated government, community and family responses.
• Needs strategic leadership to maintain and gain momentum.
The Council has received direct criticisms of the current Victorian arrangements, including comment that the current structure coordinating the Victorian Drug Strategy is bureaucratic and cannot sufficiently engage with the range of community interests and the public to advance policy. Also, it does not ensure integrated harm minimisation strategies are implemented in a strategic and coordinated way. Representation on the senior officer committee has been downgraded from senior management to middle management reducing the direct leadership of change role envisaged for this group.
The National Ministerial Council on Drug Strategy is a significant body and, appropriately, reflects the importance of drug issues. Council has been advised about concerns regarding the National Drug Strategy Committee (NDSC) that supports the Ministerial Council. Concerns have been raised regarding membership, out of session inactivity, slow and ad hoc policy development, and overemphasis on licit drugs. The lack of investment in prevention programs and dominance by health departments that marginalise law enforcement interests has been highlighted. The Commonwealth Department of Human Services and Health also commented on the reluctance of states to take sufficient financial and organisational responsibility for the operation of the NDSC. Council understands that a review of the NDSC is underway. Council is not in a position to comment, in any detail, on national structural issues. The national significance and the cross jurisdictional issues, however, demand effective collaboration if responses to drug issues are to be consistent and effective.
A review of national and international approaches to the management and coordination of drug policy has demonstrated to Council that other places face similar problems and dilemmas to those in Victoria. Council was not presented with any existing model appropriate for Victoria (McDonald, 1996).
Council recognises the need for Victoria to have a set of structural arrangements that has the potential to lead debate and coordinate drug issues and policies. Council has used the following principles in suggesting improvements.
Interagency Coordination: Drug abuse is a problem that affects many portfolios. There is a need to have the capacity to integrate the roles and efforts of the various agencies when appropriate, in a whole government approach.
Leadership: Ongoing and high profile leadership is essential. The leadership needs the capacity to engage the public in this area and draw together the diverse strands of government and non-government service provision.
Information: Any structural arrangement must have an appropriate data and research capacity to inform policy and practice. Databases and intelligence must provide a responsive flow of strategic information to and from planners and practitioners to increase the effectiveness of services, and to support policy developments.
Policy and Monitoring: Any structural arrangement must have the capacity to develop quality policy outputs, and the ability to closely monitor program developments. Long- and short-term monitoring and evaluation models must be in place to explain what works, what doesn't, and why.
Early Warning: A critical matter, related to issues identified above, is the need to construct a system that alerts and warns the key stakeholders of movements and shifts in local activity that could necessitate refocussing of policy or practices and the timely reallocation of resources.
Community and Practitioner Input: A key element of any model would be to provide an avenue for engaging the community and receiving feedback in a simple and immediate manner. Advice is required from many groups to inform the policy and implementation processes, and to inspire ownership at community level.
Training and Support: Participants in the delivery of drug abuse programs need to be up to date with trends and quality practice. Structural arrangements must allow for the support and professional development of key participants and other relevant groups.
Recognition: Many people and organisations make outstanding contributions to minimising the harms illicit drugs cause in our community. In order to further promote high quality practice, the Council supports the introduction of a high profile award scheme to recognise:
• Quality work which provides leadership to the field.
• Exemplary practice, particularly in community projects.
• Outstanding contributions to research, evaluation and clinical practices.
The award scheme should have a high level of sponsorship and be presented and celebrated regularly, as an integral part of the implementation process as the reforms proposed in this report.
National Coordination: Given the nature of the drug problem, all relevant jurisdictions should be engaged on a national basis in the most effective way possible.
Other significant elements recommended in design of an administrative structure are:
• Minimal, but effective central bureaucracy.
• A focus on quality service provision.
• Simple and accessible structures.
• The harm minimisation approach promoted and complemented.
| < Prev | Next > |
|---|