| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 203 |
| Yesterday: | 251 |
| This Week: | 203 |
| Last Week: | 2221 |
| This Month: | 4791 |
| Last Month: | 6796 |
| Total: | 129390 |
6. American Heroin Policy: Some Alternatives
 |
|  |
| 
| Reports - Drug abuse council report |
Drug Abuse
6. American Heroin Policy: Some Alternatives
Erik J. Meyers
The author gratefully acknowledges the contributions of the following individuals in preparing background materials for this chapter (However, the opinions expressed are those of the author and do not necessarily reflect the views of these contributors): Leon G. Hunt, Troy Duster, Jane McGrew, Charles Morgan, Jr., Hope Eastman, Norman Siegel, and Gerald F. Uelman.
THOUGHTFUL OBSERVERS OF the American drug situation have frequently stated the belief that our problems may be caused more by our policies than by the drugs they seek to regulate. As one writer has commented, the United States may have "created a monster out of what was initially a gnat" in moving from a nineteenth-century laissez-faire approach to drugs to a twentieth-century preoccupation with eliminating use of certain drugs.' If we look at present studies on the "social costs" of drug use, we see that they examine more the costs of present drug policies to American society than the intrinsic social costs of drug use itself. Nowhere is this dilemma over drug policy more clearly shown than in our national response to heroin use.
The discussion of alternative heroin policies that follows is meant to stimulate and focus public discussion of drug policy. We hope to promote reasoned, nonrhetorical consideration of the nature of the problems and the most appropriate means of minimizing social disruption and harm to individuals. While no policy will eliminate all problems, our analysis shows that some policy responses are more likely than others to minimize detrimental effects. This discussion begins with a look at the full spectrum of policy choices available and at specific policy models along that spectrum. Following that, we will examine the key issues heroin policy must deal with, in terms of four selected policy choices.
Our list of potential policy choices ought not be viewed as a serial progression, nor does this identification of separate, individual options necessarily preclude the adoption of more than one at a time. Implementation of one option may preclude others or instead stimulate consideration of others. The policy choices examined in the following discussion are merely illustrative of the existing possibilities; they are not intended as a complete and final list nor as a timetable for change.
The Choices
The range of possible heroin policy options is wide, extending from efforts to prohibit and eliminate all types of heroin use to official promotion of nonmedical heroin use by means of a government monopoly. The shades of difference within this spectrum of policies are nearly infinite. For example, a heroin policy could be fashioned to subject illicit sellers and distributors to criminal penalties while levying only small civil fines on those possessing small amounts of heroin for their own use. Another approach would be to subject all convicted users to long, mandatory jail terms, with lifetime parole. Both of these approaches are consistent with a policy seeking to deter use and ultimately eliminate consumption, in spite of their obvious differences in the means employed to achieve these goals. Other possible heroin policy choices falling between the poles of stringent prohibition and totally unregulated sale and consumption are: experimental use of heroin in medical and drug treatment research, development of government-sponsored heroin treatment clinics, removal of criminal penalties for personal possession, prescription of heroin by private physicians, regulation of heroin as an over-the-counter drug; and development of a "pure food and drug" model for distribution of the drug.
Complete Prohibition.
This is current American policy, in which laws provide criminal penalties for the possession, use, sale, and distribution of heroin. Federal law and a few state laws treat possession as a misdemeanor (maximum penalty: one year in jail), while other jurisdictions treat it as a felony. All jurisdictions treat sale and distribution as felonies (more than one year in jail), though penalty provisions as to fines and terms of imprisonment vary widely.
Many jurisdictions provide for the diversion of certain classes of heroin offenders into treatment programs. Successful completion of a treatment regimen may result in the dropping of pending criminal charges or may be considered evidence of rehabilitation at sentencing. Failure in treatment returns the offender to the normal criminal justice process for trial and sentencing if found guilty.
In practice, many urban criminal justice agencies do not attempt to fully enforce laws against personal use or possession of heroin. For these jurisdictions, "total prohibition" means that occasional "sweeps" may be made in areas where use levels are high or that the laws may be used selectively to punish some users while others are ignored. Conversely, many jurisdictions do not have a great many heroin users, and are inclined to arrest and fully charge every heroin offender who is apprehended.
Medical and Drug Treatment Research with Heroin.
Current federal law does not permit heroin to be prescribed for legitimate medical purposes or for "maintenance" treatment of compulsive users. The only permissible use is for certain highly restricted research projects. For example, heroin was used several years ago to test the effectiveness of narcoticdrug antagonists. However, recent interest from the medical community and segments of the general public in using heroin to alleviate the pain associated with certain types of cancer could play a role in ending official reluctance to permit research into therapeutic applications for the drug.2 Still, despite interest in the scientific and medical communities to test the efficacy of heroin as an analgesic, an antitussive, or as a tool in opiate addiction treatment, the Food and Drug Administration (FDA) and Drug Enforcement Administration (DEA)—the agencies whose administrative approval is required—have discouraged heroin research. It is because these agencies have been so reluctant to allow research with heroin that we have identified medical and drug treatment research as an independent policy option.
Our further discussion of this option below pertains to experimental research into drug abuse treatment applications for heroin, rather than to investigation into other medical uses for the drug. The decision to confine our discussion to drug treatment research reflects the primary concern of this chapter—control of the nonmedical use of heroin. However, it should be noted that research indicating useful therapeutic applications of heroin would probably have a spillover effect on general public attitudes toward the drug.
Government-sponsored Heroin Treatment Clinics.
The "heroin treatment" envisioned by this policy could take many forms. One form would be a proposed heroin "induction" or "lure" model using heroin or injectable morphine to entice otherwise reluctant heroin users voluntarily into treatment, essentially a short-term detoxification program using heroin in the initial state and methadone in the intermediate one.3 This model, in fact, is similar to the original Dole-Nyswander research program with methadone maintenance; in that study, morphine was administered to patients who at admission showed signs of withdrawal. Substitution of methadone (administered orally) would quickly follow that initial stage, as is generally contemplated with the "heroin-lure" model of heroin treatment. However, abstinence from all opiate use within a relatively short, one-to-two-year period is often stated as the goal of the "lure" or "induction" model, whereas the Dole-Nyswander approach contemplated indefinite maintenance on oral methadone.
Another possible form for American heroin treatment is provided by the British. The current American approach to heroin treatment differs significantly from prevailing British drug treatment practice, which allows indefinite opiate maintenance—intravenous heroin, intravenous methadone, oral methadone, or any combination of methods—for opiate drug dependents.' In the United States, while the new proposed federal regulations on oral methadone treatment do not require programs to drop patients within any definite period of time, they do, however, continue to emphasize strongly the patients' withdrawal from methadone and achievement of a completely drug-free state.5 In England the choice of both the opiate and the method of administration is left to the discretion of the clinic physician; although abstinence is stated to be desirable, the British consider stabilization and normalization of an addict's life and keeping track of as many addicts as possible to be equally desirable goals. Therefore, if stabilization or continued treatment-involvement can be attained only by the continuing prescription of an opiate at stable dosage levels, then such maintenance meets the social policy objectives of British treatment.
A wide degree of flexibility marks the British response to the treatment of heroin dependency. In discussing the potential effects of a heroin treatment clinic policy in the United States, we include this characteristic in our policy model. Rather than one specific type of treatment model, the clinic policy examined could encompass a variety, whether "lure," induction, true maintenance, or other types. Attention will be called to potential differences among various models in the following discussion of the issues affecting heroin policy.
Prescription of Heroin by Private Physician.
This option is still further removed from total prohibition and total government control of heroin. Practicing physicians—rather than special-purpose, government-sponsored clinics—would be the primary dispensers of licit heroin. However, this could still permit tight controls over heroin's legal availability, in that both recipient and prescribing physician would be subject to registration, reporting requirements, and official surveillance. The strictness of these controls could vary. Prescription could be limited either to legally or medically defined addicts or to those with a legitimate medical need for heroin other than for drug abuse, such as for relief of the severe pain associated with certain cancer conditions. Distribution and administration could be handled either directly in the prescribing doctor's office or by the British practice of filling the prescription through general pharmaceutical outlets and self-administration of the drug.
For this to take effect, heroin would have to be rescheduled from Schedule I to a lower control schedule of the federal Controlled Substances Act and to lower state schedules as well (for those states that have adopted a form of the Uniform Controlled Substances Act). This rescheduling process would also have to occur in order to implement medical and treatment research and the over-the-counter drug and pure food and drug models which are discussed below.
A variant "option within an option" would be to allow physicians to exercise professional discretion in determining whom to treat with heroin, how long treatment should be continued, and what amounts of heroin are required. Such a model is analogous to the British pre-maintenance clinic "system" (i.e., pre-1968 practices) and is subject to the same risks namely, the abuse of discretion or outright drug-prescription profiteering by a few physicians. (The British experience with heroin regulation is discussed in greater detail on pages 216-219.) Government supervision would be minimal, similar to present FDA and DEA monitoring of Schedule III prescription drugs, where some reporting and recordkeeping is required and prescription refills are limited.
Removal of Criminal Penalties for Personal Possession.
This policy model could be referred to as heroin "decriminalization" or "legalization." However, those terms are at best ambiguous and imprecise. The heroin treatment clinic policy previously described is, of course, a form of heroin decriminalization, since it would permit heroin to be used and possessed legally under certain circumstances. The fact that such different schemes could be termed heroin "decriminalization" is reason enough to avoid use of that term.
The marijuana decriminalization legislation of recent years has largely consisted in the removal of the possibility of a jail sentence for first-time possession of a small amount of marijuana, generally an ounce or less. In most states adopting such legislation, the offense is a civil rather than criminal one, and the offender pays a fine (generally in the $20-200 range) as if for a traffic violation. This policy model anticipates a similar, though not necessarily identical, legislative scheme for heroin. Our discussion of this option will be predicated on a policy which eliminates all criminal penalties for possession of a small amount of heroin for personal use. It, like the new policy for marijuana, does not contemplate a legal, regulated source of supply, but merely changes the penalty for illicit possession.
Removal of criminal penalties for heroin possession could be implemented at various jurisdictional levels. For example, Congress has not changed the federal law pertaining to simple possession of marijuana; possession continues to be a federal criminal offense punishable by a prison term of up to one year. However, since 1973 several states have enacted legislation making marijuana possession a civil offense—the equivalent of a traffic violation—within their borders. Although the marijuana user remains subject to both federal and state laws, since little federal enforcement effort is directed against simple possession offenses the state law has a greater impact on users. Similarly, in states that permit "local option" ordinances, some cities have formally adopted a civil-fine procedure for marijuana offenses that differs from the otherwise applicable state law. The same pattern of piecemeal implementation of the removal of possession penalties could occur with this heroin policy model.
Over-the-Counter Drug Regulation.
Dispensing heroin without a prescription would require changes in both the federal Food and Drug Act and the Controlled Substances Act. States could not implement this policy on their own in the face of a continuing federal prohibition of heroin. Currently, the only controlled substances afforded over-the-counter regulation are those listed in Schedule V of the Controlled Substances Act. It is likely that the recipient of heroin regulated according to this policy would have to meet a minimum age requirement, offer some form of identification, and have his name entered on a record kept by the pharmacist.
In addition to the registration and minimum-age requirements, heroin sold in this manner would have to be subject to standards of purity, safety, and effectiveness set by the Food and Drug Administration. (This, however, would also be true of heroin dispensed in treatment clinics, by a physician's prescription, or in the pure food and drug model discussed below.) The Federal Trade Commission could set rules on labeling requirements and warnings as well as establish any advertising restrictions desired. Basically, this model places the decision to use heroin directly with the consumer and regulates closely only those who manufacture or distribute the drug.
Pure Food and Drug Model.
This model would allow heroin to be marketed and consumed in the United States rather as caffeine presently is in coffee, tea, soft drinks, and candy. Obviously, significant statutory changes would be required at all levels of government to change heroin from a contraband substance to a legitimate product. Formal government involvement would be limited to the regulation of the quality and purity of the heroin offered for sale. Any retail establishment permitted to sell food, drugs, or other consumables would be able to market heroin. Advertising might be limited, however, in ways similar to present restrictions on the advertisement of alcoholic beverages and tobacco products in certain media.
This policy model could also be varied so that either the federal government or the states could be in direct control of manufacture and distribution. As with state lotteries, a governmental agency could have monopolistic control over the production and sale of heroin; in that case revenues realized from sales would devolve directly to the government producer. Alternatively, private production might be allowed but with sale to consumers done only by "state stores," as is currently required for alcoholic beverages in several states.
The policy models discussed above provide an idea of the variety of ways in which we control certain psychoactive substances in the United States, ways in which heroin could also be controlled. Of these policy options four have been selected for a detailed examination of their probable effects. These four—medical and treatment research, government-sponsored heroin clinics, removal of criminal penalties, and over-the-counter drug regulation—represent a diverse yet feasible sampling of points along the overall spectrum of policy choices. Research with heroin in treatment and "heroin maintenance" clinics frequently crops up as a topic in public discussions of drug abuse. Likewise, the removal of criminal possession penalties is frequently mentioned as a possible solution to present illicit drug control problems. All of these options, however, are important only insofar as they provide an analytical framework for dealing with specific concerns regarding heroin and appropriate public policy. The following discussion deals with the major issues influencing heroin policy.
The Issues
The importance ascribed to a particular issue will vary from person to person. It will also vary according to specific policy attributes. The aim of this chapter is to provide a basis for comparing the effects of different policy variables on several major areas of concern. In this way we can begin to identify those policy variables which hold special promise. An outline chart has been included (Table 6.8, pp. 244-246) to permit a summary overview of the four policy options and their predicted impact. In addition, other tables (6.1-6.7) summarize the anticipated impact of the four policy options on each specific issue.
The section below entitled "Patterns of Use" reviews the historical experiences with the fluctuating availability of other psychoactive substances as well as recent research into the extent and type of heroin use in the United States. Compulsive or dependent heroin use is a matter of particular concern in this discussion.
"Crime and the Fear of Crime" as related to heroin use is a frequently discussed topic, yet surprisingly little factual information is available on the true nature or extent of the heroin-crime link. Public attitudes and perceptions of this issue have had and will have great influence on the selection of any policy response; they are given special attention in this section.
"Community Impact" takes into account the differing impact that heroin has within the various regions, communities, and ethnic populations of the United States. Minority populations and inner-city neighborhoods are disproportionately affected by heroin at present, and are therefore emphasized in this discussion.
"Impact on Existing Drug Treatment and Prevention Efforts" and "Effects on the Criminal Justice System" deal with the impact of alternative heroin policies on these institutions, an impact depending primarily on their goals and practices. Specific policy issues such as the effect of criminal justice referrals on treatment are equally important in alternative, as well as present, policy responses.
The remaining sections deal with civil liberties, health, worker-productivity, and welfare issues. While civil liberties and health issues are matters of concern under current policy, the effect of alternatives can by no means be expected to be uniform: One policy option may create new problems to replace present ones, and another may eliminate some concerns but not others. In short, the following discussion points to no policy panacea. However, as the previous chapters herein indicate, present heroin policy is fraught with substantial shortcomings, questionable assumptions, and few identifiable benefits. The task of the policymaker is to begin to identify issues of real—as opposed to imagined—significance and reduce the costs of American heroin policy.
Patterns of Use.
The general assumption about heroin use has been that criminal penalties for possession, use, and trafficking activities deter many would-be users and keep supply at the lowest possible level by maintaining legal pressure on traffickers and consumers. Thus the conventional wisdom on proposed changes in heroin policy has been that any reduction in this pressure would result in a substantial increase in total use—and consequently in dependent use. Despite the general acceptance of these conventional theories, they have not been proven. In fact, substantial data exist on both heroin and other psychoactive substances that lead to far different conclusions.
When exploring the relationship of heroin's availability to its use, it is important to realize that there are wide variations in use patterns among those who use the drug.6 The National Commission on Marihuana and Drug Abuse identified five primary patterns of use: experimental, recreational, circumstantial, intensified, and compulsive.' The latter two types of using-behavior constitute patterns most commonly considered misuse of drugs. The greatest policy concern, therefore, ought to be to minimize these intensified or compulsive use patterns.
In order to determine whether compulsive heroin use is likely to increase as a result of any specific policy decision we will need information on several other related issues. We need to ask whether a given policy change would increase the drug's availability; we need to know whether increased availability is likely to lead to increased use of all types; and we need to know about the relationship of compulsive use to total use. To help answer these questions we must look to data on the spread of use of both heroin and other psychoactive substances.
One potential source of data is the American experience with alcohol prohibition from 1917 to 1933, which provides some information on the effects of varying control measures on excessive consumption. However, these data are not uniform. For instance, while an old Bureau of Prohibition study showed a decrease in per capita alcohol consumption, the Department of Commerce found the opposite to be true.8 Other indicators of excessive alcohol use during the period—alcoholism deaths, alcoholic psychosis incidents, arrests for public intoxication—are equally inconclusive.9
Another possible source of information is the "gin mania," a dramatic shift from beer drinking to gin consumption that the English experienced during the period 1700-50. While the figures on taxed gin consumption suggest a tenfold increase in per capita alcohol consumption, very little is known about the causes of the "mania" or its effect, other than to say that heavy use (drunkenness) did increase as the more potent gin gained popularity relative to beer.''
The more recent use of cigarettes in the United States provides another example of how compulsive use of a psychoactive drug (nicotine) can develop after use is already widespread. Although tobacco had been used in various forms in the United States since 1613, its use did not really expand until the invention of the automatic cigarette-making machine in the late nineteenth century. However, the most significant factor in the growth of cigarette use in this country appears to have been not this new invention but rather the relentless, competitive advertising among manufacturers during the period 1918-50." Heavy advertising by commercial interests now seems to be a key factor in the rapidly escalating cigarette consumption in "third-world" nations.12 The American experience with cigarette use also indicates that a particular form of a psychoactive drug can spread at the expense of other forms, and that increasing availability, as expressed by declining price, is not necessary for rapid growth.
These historical examples of substance control and spread provide conflicting answers on whether compulsive use is roughly constant regardless of the number of users, or whether it fluctuates in response to increased consumption.13 The normal distribution of using behavior for most psychoactive substances (alcohol, for example) is assumed to be that represented by Figure 6.1A. According to conventional views, heroin use is distributed as shown in Figure 6.1B. However, recent studies of heroin use indicate that it is really closer to the normal curve (Figure 6.1A) than an atypical pattern of its own (Figure 6.1B). These recent studies postulate the existence of from two to four million nonaddicted users." Previous information on heroin use has tended to focus on discussions of "addicts," failing to acknowledge that heroin, like other psychoactive substances, can be used in a wide variety of patterns.
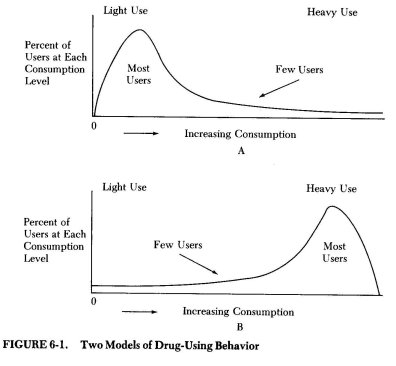
The measurement of total consumption of all types of psychotropic drugs in "normal" (i.e., non-treatment sample) populations of users shows a distribution of using behavior like that of Figure 6.1A. Since these drugs include not only heroin but also marijuana, pharmaceutical stimulants and depressants, and alcohol, it would appear that availability alone is not a controlling factor in the shape of the consumption distribution. Roughly speaking, if a drug is easy to get more people will tend to use it, but only a relatively few will be heavy consumers. If the same drug is hard to get it will tend to have fewer total users, but about the same proportion of heavy users. This argument cannot be pursued very far, of course, since we know little about the exact nature of the distributions in Figures 6.1A and B. Conceivably, the shape of the consumption- distribution curve may change somewhat as supply increases, but there is no evidence to suggest that a normal distribution curve would turn into its obverse in response to increasing supply.
It is far from certain, however, that any movement away from current policies will have the effect of increasing supply. Looking at the following specific policy models will help us to see how the availability of heroin and the behavior of users and nonusers would be affected, if at all, by the kinds of policy adjustments considered. Table 6.1 summarizes the anticipated effects.
Medical and Drug Treatment Research with Heroin. With this very limited change in policy no great impact on current patterns of use would be likely. The very nature of this option is to permit the use of heroin only by small research populations in strictly clinical settings. However, some people have expressed concern over permitting even this very limited use of heroin, on the grounds that it would lessen the strong societal disapproval that now exists. '5 Any lessening of the rigidity of official policy would, according to this view, lead inexorably to increased nonmedical use of the drug. The use of heroin as part of an experimental drug abuse treatment plan, however, hardly constitutes a major change in official policies or social attitudes toward its use. An experimental program of any type is unlikely to affect continued societal disapproval of nonmedical heroin use—unless opponents of such a change convince the public otherwise.
Government-Sponsored Heroin Treatment Clinics. Critics opposed to the experimental use of heroin would probably be equally opposed to the broad implementation of a program of treatment clinics using heroin. Objections would almost certainly be raised, in spite of the fact that abstinence would be the most likely treatment goal of heroin treatment clinics in an American context.
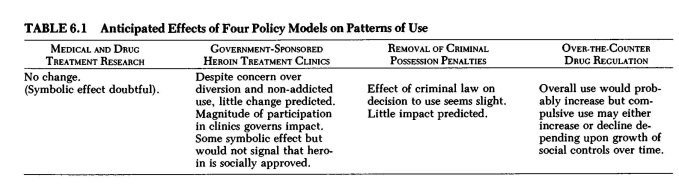
Once again, however, it is doubtful that a symbolic message that heroin can be used legitimately in the context of addiction treatment would have much of an effect on general use. Permitting heroin to be given to addicted users in abstinence-oriented treatment would be unlikely to reduce the revulsion commonly felt for drug addiction by the mainstream of American society. It is likely that those inclined to use heroin—recent estimates say from 2 to 4 million persons use it in a variety of using styles—already do so in the face of strong antiheroin symbolism and actions. The symbolism of this new policy message is unlikely to affect either the numbers of users or the patterns of use any more effectively than do current efforts.
More serious are the objections to heroin treatment clinics based on potential problems of diversion and nonaddicted users, or even nonusers, being mistakenly admitted to the clinics.10 The evidence from both American and British opiate maintenance programs indicate that these problems are manageable. In the rapid expansion of American methadone treatment capacity in the early 1970s, some law enforcement officials noted appreciable illicit diversion." However, it is now generally true that methadone diversion is relatively insignificant—few if any persons have become addicted to the drug who were not already addicted to heroin.12 Assuming that the security systems adopted in an American herein treatment clinic would be at least as stringent as those in present methadone programs, it is unlikely that heroin diverted from licit supplies would be a significant problem. Likewise, admission of nonusers does seem not to be an insurmountable problem.
Additional insight into these issues can be gained from the United States' brief experience with morphine and heroin maintenance clinics.19 Opened around 1918 but closed by federal government action by 1922, the clinics—forty-four total around the country—provide valuable if disputed information on the efficacy of opiate maintenance20 Although some problems definitely did occur and, in the case of the New York City clinic, were heavily reported in the popular press, most of the clinics appear to have been operated efficiently and effectively.21 The closings were motivated more by a desire to see a reduction in the number of opiate addicts than by any proved failure of the clinics to contain the level of addictive drug use or aid in the social stabilization of clinic patients. Diversion of clinically supplied drugs and the administration of drugs to nonaddicted clientele do not, according to historical studies, appear to have been significant problems in practice. With illicit opiates still widely available on the street, there seemed to be little pressure to divert legal drugs.
A review of the British experience with clinic dispensation of heroin also gives credence to the view that drug diversion is not likely to be overly significant, nor is the possibility of nonaddicted users being drawn into the clinic. Factors other than the clinics themselves figure into the British heroin situation, but it appears that the clinics have contributed to a low-keyed societal response which has helped keep the heroin dependency at a fairly low level. The prevailing British view of their clinic system is one of "containment," rather than "maintenance," of opiate addiction.22 In fact, very little heroin is currently dispensed, although clinic physicians have the discretion to prescribe it for treatment clients. The clinic system has received steady support in its effort to limit nonmedical opiate use to those already addicted and avoid creating an environment for the growth of a large, entrenched illicit heroin distribution system. Despite the presence of illicit heroin in England, the "black market" appears not to be currently large, nor is it predicted likely to grow.23
Adolescent heroin use is also a matter for concern. The clinic option would not necessarily exclude nor include adolescent users from treatment. The legitimate receipt of heroin by youthful clinic patients would predictably be even more explosive politically than the admission of youthful users into traditional methadone programs. Whether the perceived advantages of providing treatment attractive to the youthful user outweigh the perceived disadvantages is a matter requiring more detailed examination and the exercise of careful judgment.
Removal of Criminal Penalties for Personal Possession. Implementation of this option would lead many to expect a dramatic increase in heroin use, an attitude that stems largely from our traditional reliance on law enforcement measures to control it. Many people believe that the only way to regulate drugs is to prohibit their use, enforcing that prohibition with criminal sanctions. However, drug policy seems to have less influence than is commonly presumed on personal decisions whether to use particular drugs. For example, an exhaustive study of the effects of the 1973 "get-tough" drug law in New York State showed that this strict law, even in areas where it was fully implemented by the court system and backed by law enforcement agencies, failed to demonstrate a discernible influence on the level of heroin use.24 Similarly, annual surveys conducted in the state of Oregon reveal that use patterns have changed little following the substitution of civil for criminal penalties for simple possession of small amounts of marijuana.25
The other chapters of this report have emphasized that the decades of efforts to apprehend, jail, or treat heroin users and interdict and destroy supplies of the drug appear to have had little more than transient effects on use patterns. The criminal law seems particularly ineffective in influencing the behavior of the compulsive heroin user, who is not as prone to consider the risks involved in continued use as those less involved with drug consumption. Thus, merely changing the criminal penalty structure for personal possession seems unlikely to in itself affect personal decisions whether to use heroin.
Over-the-Counter Drug Regulation. This option would make heroin far more accessible to far greater numbers than would any other. Yet one cannot conclude with any certainty that compulsive use would necessarily increase, even though it seems reasonable to predict that both general use and dependent (compulsive and intensified) use would increase to some extent. We do not know if destructive behavior would continue at the present or an increased rate; perhaps changes would also have to occur in institutional structures to promote more controlled using behavior in place of destructive patterns.
However, even though in all likelihood availability would increase, that does not seem to be the only important factor in the normal distribution curve for psychoactive drug using behavior. (See Figure 6.1 and discussion, pp. 198-200. For example, the previous discussion pointed out the role of advertising in increasing heavy, compulsive use of cigarettes in the United States and elsewhere. Heroin, contrary to sixty-year-old beliefs, appears to have developed, or is developing, a normal distribution curve similar to alcohol and marijuana use patterns.
If this is correct, one would anticipate compulsive use to continue to represent a small fraction of overall use. Nonetheless, that compulsive use would probably remain relatively small in comparison to overall use does not diminish our concern over the possibility of a net increase in compulsive or adolescent heroin use. Additionally, in light of the present widespread anxiety over any type of heroin use, any increase in general use would be of concern to most Americans. Still, current patterns of enforcement seem to be a key factor in inhibiting t íe denment oTiTóréwidely followed cntr'o o using beTiay. oi.2wWhile here is evidence of a substantial nu`~mof controlled users of heroin,27 social controls on heroin use are probably not sufficiently advanced to prevent some increase in dysfunctional use were OTC regulation to be substituted for the current prohibition approach without other intermediate policy steps.
Crime and the Fear of Crime.
Crime is perhaps the single most important consideration in both past and present heroin policy. Were it not for the assumed close connection between heroin and crime, new use—even compulsive use—would not be as great a public concern. Yet there is remarkably little information on the relationship of heroin to crime; however, that lack of knowledge has not undercut the widespread belief that there is a proved link between heroin use and consequent criminality.2B Heroin addicts are still presumed to support at least 60 percent of their heroin purchases through theft and robbery, for an estimated $695 million annual bill.29 The prediction of this annual loss is given as justification for continued, even increased, law enforcement spending on programs aimed at eliminating heroin use.
The American attitude towards heroin is deeply rooted in the history of our drug laws.30 Suppression of "narcotics"—an early catch-all word which encompassed opium, heroin, morphine, cocaine, and marijuana—proved to be popular politically. Fears of minority and immigrant groups went hand-in-hand with the fear that revolutionaries were seeking to undermine American society through drugs. For example, the Mayor of New York City established a Committee on Public Safety in 1919 to investigate "the heroin epidemic among youth and the bombings by revolutionaries."3' Such fears repeatedly surface in the development of American drug control laws;32 they were joined in the late 1960s by the idea that heroin was largely responsible for the rapidly rising rates of street crime.33
The proposition that heroin and crime are interrelated can be broken down into three more manageable concepts. The first is the "pharmacological theory," which holds that the pharmacological properties of the drug cause users to commit a variety of criminal acts, including both violent and property crimes. This view is similar to the prevailing legal view of insanity that a person can be compelled by an "irresistible impulse" to do wrong. Although this relationship is frequently assumed to exist, exhaustive studies of heroin and its pharmacological effects have not shown it.34
The second is the "social theory," which holds that because the law defines heroin use as illegal, the user will tend to be a criminal. By definition, possession or use of heroin constitutes a crime; therefore, by definition the user is a criminal. Similarly, heroin distribution activities are criminal because the law so states. The point that it is the law which ordains who is a criminal is often overlooked in discussions on drug policy. Because the heroin user is a "criminal," it is easier for the public to assume that he or she will commit other, unspecified criminal acts.
The third is the "price theory," which holds that users commit crimes such as theft, robbery, or property crimes to support their habits. The concern over acquisitive crimes purportedly committed to support use is at the heart of recent government and public concern with increasing heroin use.
The commonly held views of heroin use and crime contribute to the general belief that property crime is a necessary concomitant of use. Thus, the ordinary citizen is led to believe that the drug itself overbears the will of the user—by definition already a criminal—and causes him to commit crimes of theft or violence in order to obtain his drug. It is on this theory of a heroin-crime relationship that our discussion will focus.
There is no doubt that some, perhaps many, heroin users commit property crimes. Undoubtedly, heroin is an expensive drug which for many can only be obtained by additional, often illegal, income. However, compulsive heroin users often have a criminal history predating their heroin use,35 and it is possible that "persons who are very successful in income-generating crime may spend a sizeable portion of their income on a luxury good—heroin."38
Recent evaluations of treatment programs for heroin users show only marginal effects on reducing crime rates for enrolled patients.37 This finding supports the view that heroin use—even compulsive, daily use—is frequently an aggravating factor in property crime but is often not the primary cause. However, the conventional response is that for the criminal who uses heroin the primary cause of crime is the heroin; cessation of use is commonly equated with the "solution" of the crime problem.
Similarly, a study on the relationship between heroin price and non-drug crime rates in a large urban area (Detroit, Michigan) indicated that temporary reductions in heroin availability led to marginally higher crime rates (higher in poorer neighborhoods than in wealthier sections). 38
While these studies do have many limitations, they do seem to indicate that, to the extent that a relationship between heroin use and property crime exists, it exists because of the high cost of heroin. Thus, to the extent that drug policies increase the cost of heroin, property crimes can be expected to increase in areas where compulsive use is high and income levels low. If it is true that an increase in heroin price may lead to increased crime, it is probably also correct to predict that lower heroin prices may lead to some decline in crime rates.
It is difficult, however, to say much at all about crime rates. Reported crimes are but a fraction of actual crime, and crimes resulting in an investigation or arrest are an even smaller fraction. Increases or declines in the number of those arrested for non-drug offenses who are also heroin users mean little if their relationship to total crime is unknown. For example, the recent report on the effects of New York's so-called "Rockefeller drug law" found that in New York City during a period of rapidly increasing crime the percentage of narcotics users among those arrested for non-drug felonies declined (from 52 percent in 1971 to 28 percent in 1975)." Data such as these still give an incomplete picture, since we do not know the relative proportion of reported crime to actual crime or, in fact, of heroin users to nonusers for either reported or actual crime.
While the true nature of the heroin and crime relationship may eventually be better understood, at the moment how the public perceives that link is of paramount importance. The development of our antinarcotics laws reflects a history of shifting fears about certain proscribed drugs and their users. Apart from whatever the danger actually was, these fears motivated public support and prompted policymakers' support of stringent law enforcement policies. Fear of crime, much more than actual crime, underlies our current response to heroin.
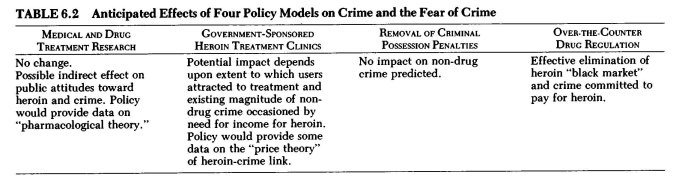
Table 6.2 summarizes the anticipated effects of the four selected policy models—research, clinics, removal of penalties, and over-the-counter drug regulation—on non-drug crime and public perceptions of the victimization risk.
Medical and Drug Treatment Research with Heroin. Implementation of this policy option would offer the possibility of developing substantial empirical data on the pharmacological effects of heroin on compulsive users. Such information might help to put to rest the notion that the effects of the drug cause users to commit crimes.
Permitting scientific research with heroin in a treatment setting would not in itself alter our current prohibition on the use of the drug outside of that small experiment. Greater public understanding about heroin and its effects would affect public attitudes toward those using the drug. For example, wide public recognition that the high cost of heroin, rather than its pharmacological properties, leads to the revenue-producing crimes some users commit would have important public-policy ramifications.
It is also possible, however, that the experimental programs may indirectly harden public attitudes toward heroin and crime. For instance, any incident involving a participant of an experimental program in a criminal act may be viewed as substantiating a firm heroin-crime link. We are all familiar with news reports headlining a person's past involvement with a mental health institution, no matter how incidental that contact is in relation to other aspects of the person's life or the incident being reported. Likewise, the tenacity of the myths and misconceptions about heroin cannot be overestimated.
Government-sponsored Heroin Treatment Clinics. For heroin treatment clinics of any type to become a reality, there must almost certainly be a strong belief in their crime-reduction potential. Substantial doubts about clinics' ability to reduce crime would leave humanitarian concern for the addicted heroin user as the chief reason for the approach, and such concern for the user's welfare really has not been a primary element in past heroin control policies; it seems unlikely to emerge as a critical consideration at this juncture. Even given an initial atmosphere of support, the public mood could shift rapidly if there were adverse publicity of clinic problems (such as occurred with morphine and heroin maintenance clinics in the period 1918-2240) or a lack of noticeable results in crime reduction (especially if there were a "hard-sell" public relations campaign on that issue). Because public fears about crime are based so much on perceptions, rather than actual levels of crime, the effect of heroin clinics would depend upon these intangibles and could only be assessed accurately in retrospect.
Nonetheless, studies of drug treatment reveal that criminal activity generally declines to some undetermined degree (although not completely) while a person is enrolled in treatment. '41 The real difficulty is in determining the magnitude of this reduction and which influences are responsible for it. If the addition of heroin to a treatment program—whether it be "maintenance," "lure," or some other concept—would at- ' tract a substantial portion of the large population of compulsive users who have never been in treatment, it may be possible for these clinics to have a measurable impact on non-drug crime. Even if they did not attract significant numbers of clients, they might, as current programs do, help reduce the total amount of crime. To the extent that crimes are committed to secure funds to pay for high-priced illicit heroin, enrolled clinic patients would have one less need for income.
Removal of Criminal Penalties for Personal Possession. This option would lead us to expect no change in the market prices of heroin; the mere removal of penalties for possession of small amounts would not create a legal supply of heroin nor would it effectively reduce the profitability of illicit heroin sales. Thus, one could expect whatever crime is being committed to pay the street price of heroin to continue whether possession were punishable or not.
Over-the-Counter Drug Regulation. More than the other three options, this policy could only come about after significant changes in public attitudes toward heroin and crime had occurred, rather than be a factor in changing those attitudes. Putting aside the question whether this option would have a realistic chance of being implemented, the potential impact of over-the-counter regulation on non-drug crime would be enormous. As noted previously, heroin's high street price is undeniably a factor in the resorting to theft and other illegal sources of income by some users. Should heroin become as cheap as aspirin or Valium, it seems logical that the need to resort to theft to pay for even a heavy heroin habit would be effectively eliminated."
Community Impact. It is clear that the effects of heroin policy are felt most acutely at the local community, neighborhood level. Some neighborhoods are much more affected than others by heroin users and governmental heroin policy. There is therefore an obvious danger in talking about the effects of alternative policies on the "community" as if there were a common reference point. Certain aspects of heroin policies will have disproportionate effects on specific communities within larger metropolitan areas.
Compulsive heroin use tends to cut the user off from the society of nonusers and enmesh him deeply in that of other deviants. This "disenfranchising" effect is the most notable community impact of heroin use at present. Laws making use a criminal act stigmatize the user, as does the association of revenue-raising crimes with heroin use.
The communities most affected by heroin are those most affected by a deeply rooted set of social maladies—poverty, unemployment, racial prejudice, inadequate housing and transportation, poor education, and poor vocational training opportunities. These communities experience heroin dependence and trafficking as additional hardships.
Permitting a degree of "local option" among policy alternatives may help to minimize potential negative consequences and increase the opportunities for community improvement. Many localities—entire states, even—today have little problem with heroin use and associated social problems; for these areas it may be logical to continue a prohibitionary approach. For other areas, where the use of illicit drugs is high despite efforts to prevent it, it might be more appropriate to allow greater local discretion in the formulation of drug policies and programs. To some extent, local option occurs even under present policies; for example, some metropolitan police departments choose to ignore heroin possession offenses, and some courts establish informal penalty structures for them.
There are many precedents for "local option" in the regulation of substances or activities. Alcohol consumption regulation, for example, has been left largely to the individual states. The federal government regulates only international aspects, production, interstate transportation, and unfair practices regarding alcohol." States have come up with a considerable variety of regulatory control schemes; the majority of them also provide some form of "local option" for municipalities, counties, or other organs of local government.
Other examples exist as well. Gambling is now primarily a subject for state or local, rather than federal, control." Laetrile, a compound derived from apricots and claimed by some to be a cancer cure, is at present only regulated by the states (though the federal government may intervene in the future). Likewise, as discussed previously, some degree of "local option" has emerged with marijuana regulation; differences among the states and the federal government on marijuana, however, have been confined to the severity of the penalty for possession. Table 6.3 summarizes the predicted impact of particular heroin policy options at the neighborhood level and indicates where "local option" may be feasible.
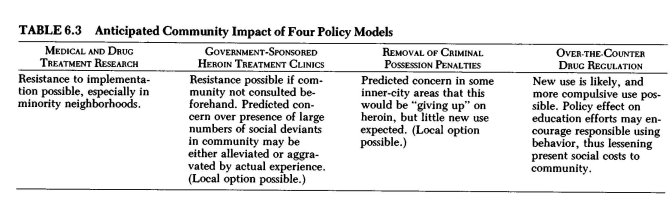
Medical and Drug Treatment Research with Heroin. Implicit in this option is a very limited scale of closely monitored experiments. Experimental research with heroin under these circumstances would not be likely to have much immediate impact on the community, local or otherwise. For example, the use of heroin as an analgesic for cancer patients would occur within established hospitals; no new facilities would have to be created nor additional patients sought. Similarly, the use of heroin in experimental drug treatment therapy would most likely be undertaken in existing medical research centers, hospitals, or drug treatment programs, carefully selected for program quality and security.
There is, however, great concern expressed by some community spokesmen that experimental heroin treatment research would lead to the rapid expansion and permanent establishment of "heroin maintenance" clinics. Those in minority communities often suspect that their desires and needs on the local level will be ignored by federal policy makers, and, just as the initial success of Drs. Vincent Dole and Marie Nyswander with methadone maintenance led to large-scale federal support for methadone clinics, so the fear is that, regardless of community feelings, experiments with heroin in drug treatment will inevitably lead to a national heroin clinic system with most centers located in inner-city areas.
Although this apprehension persists, many local leaders seem convinced of the need for heroin treatment research. The National League of Cities (NLC), as part of its 1977 National Municipal Policy Statement, passed a resolution which supported further study of heroin maintenance, including specific research studies with heroin. Reaffirmed in 1978, this action by the NLC is an indication that experimental research may indeed be not just possible but actually welcome in certain communities. Local officials and their constituents express concern over the continuing high social costs of compulsive heroin use under present policies, and seem more willing now to consider and examine alternatives previously regarded as too radical or controversial.
Medical heroin research could have a widespread educational effect, and could help break down many of the present misconceptions about the drug. Public acknowledgment that heroin is a drug with a capacity for both beneficial and adverse effects, depending upon the circumstances of its use, would be a significant advance in public understanding regarding the drug. Research studies may help to produce this public understanding.
Government-sponsored Heroin Treatment Clinics. Resistance to the location of drug treatment facilities in residential neighborhoods has frustrated the desire of many drug treatment programs to be close to the population to be served. While in the abstract everyone is eager to have community-based drug treatment, a caveat is that the proposed facility should be on someone else's block, near someone else's home, family, and neighbors. Heroin treatment clinics would face even greater hurdles of public resistance than other, existing forms of drug abuse treatment in the United States. The treatment in using heroin to stem compulsive use will have to be fully and carefully explained. In spite of explanations of the treatment process, there may still be objections to the clinics because of the fear of new crime they may engender.
To the extent that clinically supplied heroin would reduce a user's need for illegal income to pay for street heroin, the community would be better off. However, users who support their use through crime tend to rely on criminal activities to satisfy their other income needs as well. Despite the provision of clinic heroin, crimes by some program clientele can be expected, since such behavior already occurs in existing treatment situations. However, it would be unfortunate and inaccurate for the local community to point to such crimes as evidence of the failure of the treatment programs.
Regardless of the crimes actually committed, the presence of a group of social deviants—often criminal—within a residential area is a frightening prospect to those who see themselves or their children as likely victims. If experimental treatment programs using heroin precede the institution of heroin clinics, community perceptions of the risk involved may change. A successfully run experimental research program may help ease fears of heightened criminal activity in the neighborhood of the program. Attitudes may evolve sufficiently to permit clinics to be established within neighborhoods where the problems of compulsive heroin use are most severe. However, the potential for reversal is also great, since highly publicized, negative incidents involving a program or one of its clients could conceivably affect acceptance of all such programs and lead to demands for their abolition. This scenario occurred during the early 1900s with American morphine and heroin maintenance clinics,45 and to a lesser degree with the more recent methadone clinics.
Removal of Criminal Penalties for Personal Possession. To the extent that crimes are committed to pay for heroin, this policy change would not alter the present situation. While this change would eliminate the social deviance labeling of heroin use which may contribute to users' criminal behavior, it is unlikely to alter significantly present patterns of criminal behavior.
In some black and Hispanic communities, spokesmen have charged drug law enforcement authorities with an abdication to lawlessness by failing to strictly enforce penalties against heroin use and possession. This tension between the community and the authorities is heightened by both real and perceived differences in police effort between poor and wealthier sections of our cities. A policy mandating the uniform application of decriminalization of heroin possession may help end such discriminatory law enforcement practices, or may instead stimulate renewed charges of an official surrender to widespread drug use.
The policy is also unlikely to satisfy concern over new use, especially use by the young, school-age segment of the population. While white, black, and Hispanic neighborhoods are equally concerned with spreading heroin use, it is unlikely that new use would be evenly split between predominantly white suburban areas and predominantly black or Hispanic inner-city areas. At least one study suggests that inner-city neighborhoods are already nearly saturated with heroin in that it seems to be readily available.4B However, the notion persists that removing criminal penalties would further increase availability in these inner-city neighborhoods and result in higher rates of use.47 To the contrary, easier availability would seem to have the greatest potential impact in those neighborhoods where heroin is now typically more difficult to obtain, for example, in largely white, middle-class suburban areas.
Even in these areas new use may not automatically result from mere removal of criminal penalties for possession. Studies of drug use over a ten-year period among the school population of a suburban California school district suggest that in many communities heroin is seldom used even when available.48 However, other recent studies suggest that the use of heroin is more prevalent than is commonly believed.49 Regardless, the rates in inner-city areas are conceded by all to be the highest, and are thus the least likely to be greatly affected by this policy option.
If criminal penalties for possession of heroin were to be removed, there is some evidence to support the view that many people would come to eventually favor the policy. During the four years following the decriminalization of marijuana in Oregon, surveys noted increasing support for the policy, even for more liberal extensions of it.5° However, public support of drug decriminalization does seem highly drug-specific. To suggest that such support would grow for heroin at the same rate as for marijuana would be to ignore the very real social stigma and fears in every American community surrounding heroin use, as well as the actual differences between the two drugs.
Over-the-Counter Drug Regulation. Some information on the potential impact of over-the-counter drug regulation of heroin can be obtained by examining the British experience prior to 1968. Before enacting the Dangerous Drug Act of 1967, the United Kingdom had experienced a rapid growth in the number of known heroin addicts, from 342 in 1964 to 2,240 in 1968.5' This growth, while minimal compared to the estimated population of American addicts, alarmed the British public and their lawmakers. At the time any physician could prescribe heroin or cocaine for nearly any reason, and a very small number abused this public trust by writing prescriptions on demand to increasing numbers of users. The 1967 act and, ten years later, the 1977 Misuse of Drugs Act (which required physicians to be specially licensed), were passed in response to this problem of overprescribing.
One view of this relatively unrestricted access to heroin is that sooner or later new users will come forth, and more compulsive users will result. Doubtless this situation will be feared in nearly all communities, even though relatively little problem exists with morphine and codeine which are available now in any corner pharmacy. Some experts have postulated that for many compulsive heroin users the attraction to the needle may be as great as the attraction of the drug itself.52 An over-the-counter policy for heroin, while unlikely at present, could conceivably become an appropriate regulatory vehicle for the control of dysfunctional heroin use at some time in the future.
Impact on Existing Drug Treatment and Prevention Efforts. The primary modes of American drug treatment for heroin addiction at present are methadone maintenance, detoxification using methadone or other pharmacological assistance, and various types of drug-abstinent programs such as "therapeutic communities." The quality and number of supportive services—which include employment, education, and psychiatric counseling—vary widely within these broad treatment categories.
The largest single mode of drug treatment in terms of numbers of heroin-using clients and official expenditures is methadone maintenance. Short-term detoxification programs generally operate within existing health facilities and are also numerous. Therapeutic communities, while fewer in number and smaller in size, provide an alternative for heroin users motivated to become totally abstinent.
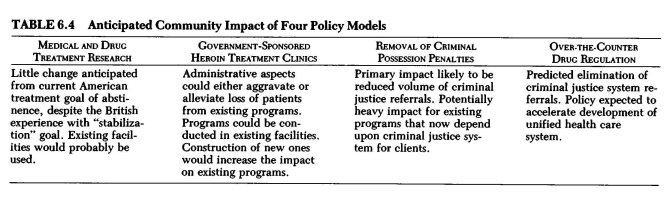
As the federal effort to eliminate illicit drug use expanded rapidly in the early 1970s, court referral and diversion programs for illicit drug users emerged as an important new ingredient in the modern American heroin use treatment scheme. Clients are now referred to treatment as a condition of probation or parole or are "diverted" into it before trial. These referrals from the criminal justice system now comprise a significant portion of all treatment populations.53 Although the selection of treatment in lieu of continued imprisonment or criminal trial proceedings is technically voluntary, the client is faced with a difficult choice between alternate forms of official supervision and control; since at least some element of coercion is involved, he or she cannot be considered an entirely "voluntary" entrant into treatment. One would therefore expect the greatest impact of alternative policies among drug treatment clientele to be felt by this group, a highly significant and numerous segment of the total heroin treatment population. Particular types of drug treatment may be disproportionately affected, depending upon the policy alternative, as is shown in Table 6.4.
In the face of rising drug use among the young in all social and economic settings, "drug abuse education" and "prevention" became national concerns by the late 1960s. The earliest school-based education programs tended to rely more on fear than fact. Later programs were geared more toward providing factual information and avoiding value judgments. However, the underlying assumption of educators seemed to be that once the pupil had the "true facts" he or she would decide not to use illicit drugs. The goal sought by all educational programs was and still is complete abstinence from illicit drugs. (In fact, in some communities the abstinence goal is so strong that undercover police activity has been termed part of those school "drug education" efforts.)54 The reason most often given for continuing heroin prohibition is that any relaxation in official attitudes would diminish the present stigma attached to heroin use and lead to increased use.
More recently, programs have sought to reduce the use of licit psychoactive substances like alcohol and tobacco products as well as illicit drugs. However, the arbitrary and pharmacologically artificial distinctions between illicit and licit drugs place educators in a difficult position. Drug educators are caught in an inherent contradiction in telling students that licit drugs can generally be used responsibly (though they can be mis-used), but that illicit drugs must never be used. However, policies focused less on the drugs themselves might be better able to promote the concept of responsible use whatever the substance.55 Policy changes which demonstrate heroin to have the capability for both harmful and beneficial applications (i.e., use as analgesic for cancer patients) might increase the understanding of the general public about drug use and misuse. Drug education of this very broad sort is the kind that seems most needed.
Table 6.4 summarizes the predicted impact on existing drug treatment and prevention efforts discussed below.
Medical and Drug Treatment Research with Heroin / Government-sponsored Heroin Treatment Clinics. The research model envisions a trial of new treatment modalities for attracting, retaining, and treating compulsive heroin users. What is curious is that many current drug treatment and drug education workers are alarmed by discussion of experimental heroin treatment research. All recent proposals to try injectable opiates as part of an experimental heroin addiction treatment program have as their ultimate goal complete abstinence,56 as do current methadone and drug-free approaches to heroin addiction. From all appearances, the intent of proposed experimental approaches using heroin is identical that of the existing American efforts with methadone.
There are, of course, other possible program goals which do not necessarily include total abstinence from drug use. For example, a former federal drug policy spokesman has described opium maintenance in Iran, heroin maintenance in Great Britain, and methadone maintenance in the United States as identical in their predominant objectives: reduction of social costs, stabilization of the treatment patient's life, and establishment of a means of control over the patient so that a therapeutic relationship has a chance to develop between the patient and treatment personne1.57 Heroin research and treatment programs suggested for American investigation would be unlikely to differ from these goals.
Should American researchers prove—as English clinicians have done already—that heroin can be used appropriately in a treatment setting, current American treatment and education efforts may be led to reevaluate their positions on heroin. They may consequently focus less on heroin use per se and more on making the treatment client functional in society. On the other hand, present goals expressed by treatment programs—lower social costs, stabilization, and control leading to eventual abstinence—would probably remain. The important changes would be in the general philosophical consensus on how to achieve these goals.
A fear frequently expressed when "heroin maintenance" is proposed is that new clinics would be implemented as methadone maintenance clinics were only a few short years ago, raising the public's expectation of a quick and easy solution to the social problems associated with heroin use. Leaving aside for the moment objections to using pharmacological supports in the treatment process, one can see the risks in this. Although treatment professionals can point with pride to certain benefits of methadone treatment, it has been far from the quick solution to urban crime and heroin addiction overzealous advocates promised. To make unfulfillable promises in connection with heroin clinics would tend to undermine all drug treatment, despite very real accomplishments and reasonable potential. The impact on existing treatment would largely depend upon what results are predicted from the use of heroin in treatment.
Another fear is that a large-scale program using heroin for drug treatment purposes would draw clients away from existing programs. This belief seems to be based on the assumption that heroin is so intrinsically desirable that, given the choice, people would prefer to use it over any other substance. Despite solid evidence to the contrary,58 this belief in heroin's overwhelming attractiveness persists, convincing many that the use of heroin in treatment would virtually force other treatment modalities to cease operation.
There is another reason for believing that new-style heroin treatment clinics might draw clients from existing programs: the quality of treatment services provided. The high volume of criminal justice-referred clients in "drug-free" programs and the frequently criticized "gas station" approach of some methadone programs are just some of the problems of existing programs. These problems lend support to the view that voluntary clients would, if possible, leave present programs for the new clinics.
However, it would not be necessary for new programs to be completely independent of present treatment efforts. For example, some dependent individuals might not be ready to become abstinent or switch drugs (methadone), but they might be prepared to take an initial step toward controlling their heroin use by enrolling in a treatment program that supplied the drug; later they could be directed toward another treatment regimen. It is also possible that treatment efforts might not focus so intently upon achieving abstinence, but would tolerate or encourage controlled using behavior in return for personal and social stabilization.
Administrative regulations could either alleviate or exacerbate the potentially adverse impact on existing programs. For instance, if failure in other types of treatment were made a prerequisite for admission to the new clinics, it is possible that some would enroll in existing programs just to "fail" and be eligible to participate in a heroin clinic. Decisions on whether to allow "take home" drugs or require on-site administration would influence the relative attractiveness of the new heroin clinics over existing methadone programs. Also, having to visit a clinic for a heroin injection more than once a day, if required, might make heroin clinics relatively unattractive to those interested in stabilizing and normalizing their lives.
Some information can be obtained by looking at the English experience with heroin treatment. In what is commonly referred to in America as a "heroin maintenance system," English law and medical practice permit clinic doctors to prescribe injectable heroin to maintain addicted users, generally on a weekly basis; these prescriptions are filled through local pharmacies and reviewed frequently for dosage level—and for the question of the necessity of continuing to prescribe heroin. The ultimate decision of whether to prescribe heroin is left to the clinic physician. Actually, little heroin is currently prescribed; oral and injectable methadone are increasingly preferred by clinicians as maintenance drugs.59 However, heroin may still be prescribed, should the clinic physician feel it to be in the best interest of the patient.
The British situation provides evidence that methadone and heroin treatment need not be incompatible. If American treatment programs would use heroin along with or in place of methadone, this addition of heroin as a support drug in the treatment process might enhance the overall attractiveness of treatment. Drug treatment therapists stress the importance of establishing contact with the user as a first step toward controlling compulsive drug use. It is possible that heroin clinics would encourage more troubled users to seek treatment, whatever the type, rather than merely redistributing the same individuals being treated at present.
The impact of such new clinics on existing American drug treatment programs would also depend somewhat on whether new, separate facilities are required. Separate facilities for new programs would probably mean that the prospective treatment client, not the physician, would have the most control over the choice of treatment program, since current programs tend to compete for similar clientele. New facilities would require initial capital expenditures for construction, and this would either draw funds away from existing funded treatment programs or require additions to the drug abuse treatment budget. Since federal government treatment funding has been relatively stable over the last few years—reflecting both budgetary constraints and reduced interest in drugs—reallocation of existing funding is more likely than new budget additions.
However, nothing necessitates separate facilities to implement this policy. In fact, the variety of ways in which heroin could become a part of addiction treatment—e.g., use with other drugs, use only in the beginning, and so forth—suggests that its integration with existing efforts could be an eminently reasonable approach. Existing methadone programs with appropriate counseling and support services and adequate security could be adapted relatively easily to accommodate the ancillary use of heroin in treatment. And other medical delivery systems could be utilized; for example, one writer has proposed utilization of health maintenance organizations (HMOs) to provide heroin treatment."
Removal of Criminal Penalties for Personal Possession. Enactment of heroin decriminalization measures similar to current marijuana legal reforms would greatly affect the numbers of court-referred treatment clients. "Drug-free" treatment modalities would be especially affected, since most referrals at present go to them rather than to methadone programs.e1 However, should heroin decriminalization impose a requirement that the offender be referred to treatment rather than given a civil fine, more criminal justice referrals would be likely.
Aside from that possibility, indications are—despite our inability to predict precisely—that the level of treatment referrals (if treatment referrals are not mandatory) would drop. Marijuana decriminalization in California led to a dramatic drop in the number of marijuana law offenders sent to treatment or education facilities by judges who felt jail was an inappropriate or extreme punishment. Any decline in drug treatment populations is significant to the programs involved, since government funding is tied to the number of clients. If existing treatment programs were unable to enhance the quality of their present services and attract an increased number of purely voluntary entrants, treatment populations would probably decline substantially, and with that decline would come a funding reduction.
Despite removal of possession penalties for heroin, court referrals could continue to be significant to treatment programs if heroin users arrested for non-drug crimes were referred to treatment in lieu of imprisonment or trial or as a condition of probation or parole.
Implementation of decriminalization of heroin may also lead to greater acceptance of the concept of "responsible use" by drug treatment, education, and prevention professionals. No longer compelled indirectly by law to concentrate on abstinence, these professionals might begin to narrow their efforts in order to deal with truly compulsive or dysfunctional using patterns. On the other hand, the strength of the current abstinence goal of treatment programs would indicate substantial difficulty in making this conceptual change.
Over-the-Counter Drug Regulation. Over-the-counter regulation of heroin would seem to spell an absolute end to criminal justice referrals to treatment. Whatever treatment was provided would have to be done on a purely voluntary basis, except for some minor mandatory programs similar to those for intoxicated drivers (the driving-while-intoxicated [DWI] programs) that now exist in many states.
Over-the-counter regulation of heroin would tend to accelerate the trend toward a unified health care delivery system for a variety of medical, psychiatric, and social needs. The expansion of general health services to include antiaddiction, detoxification, and similar services for those with drug problems may come through existing health maintenance organizations or similar group-care programs. Alcoholism treatment programs are presently offered by a variety of medical service systems—hospitals, HMOs, individual doctors, and private self-help organizations. Over-the-counter heroin regulation would provide an impetus for these medical care providers to expand their services to include persons with other drug problems, including heroin.
In an expansion of the traditional health care delivery system to meet the special problems of the misuse of no-longer-illicit drugs large-scale separate drug treatment programs would probably cease to exist. However, the continuation of privately funded therapeutic communities and self-help, drug-free programs would be likely; it is possible that these programs would be able to reestablish their attractiveness to voluntary clients. For example, Alcoholics Anonymous is currently a widely recognized self-help program for those with alcohol problems.
Adoption of OTC regulation for heroin would almost inevitably mean that the consensus of opinion on a relationship between heroin and crime had changed. Abandonment of the crime-control aspect of drug treatment—particularly for methadone maintenance—would also be a factor in the absorption of existing treatment into a broader health and social-service provision mechanism and the consequent disappearance of separate facilities for drug treatment.
Effects on the Criminal Justice System. The phrase "criminal justice system" refers to a varied group of institutions and individuals who together enforce and administer American criminal law. There are three major subgroups: law enforcement, the courts, and corrections. Within each of these subgroups are divisions based on a specialized function and the jurisdictional authority of the government agency in question. Federal, state, and local authorities overlap and occasionally conflict in the enforcement and administration of drug laws. In order to gain a better understanding of how alternative policies may affect particular criminal justice agencies, it is important to keep in mind the complexity of the system and its interrelationships and note that policy enacted by one level of government may conflict with that of another.
Law Enforcement. Local and state police comprise the bulk of the drug law enforcement effort. However, there are several agencies at the federal level that are significant in terms of policy leadership and as a source of law enforcement funding. These agencies—primarily the Drug Enforcement Administration, the Customs Service, and the Law Enforcement Assistance Administration—have major responsibilities and interest in American heroin law enforcement. However, their policy missions are more narrowly drawn than those of the ordinary police force.
Numerically, the most important heroin law offense involves "simple possession" of the drug. Studies of drug law arrests across the country show that, of those involving heroin, the vast majority are for "simple possession" (an amount set by each state or by federal law, corresponding to the lowest penalty for possession of heroin).82 In about a dozen states and also under federal law, simple possession of heroin is a misdemeanor (punishable by up to one year in prison), while it remains a felony in the remaining American jurisdictions. Second in importance in terms of numbers of arrests are the "ancillary offenses," which involve such activities as being under the influence of heroin, possessing hypodermic syringes to inject the drug, or being present where drugs are sold or used. Possession with intent to distribute and sale, importation, or other heroin trafficking activities, while subject to severe criminal penalties, produce few arrests compared with possession and ancillary offenses.
However, because the practice of "overcharging"" is common with heroin law offenses, numbers of arrests and convictions do not tell the complete story. The vast majority (over 90 percent) of all convictions for opiate offenses are based on a guilty plea resulting from plea-bargaining between the defendant and the prosecutor. Since it is therefore likely that the initial charge will be bargained down, it is not unusual for both the arresting officer and the prosecutor to charge the defendant with the highest charge plausible (hence the term "overcharging"). Thus, neither arrest nor conviction statistics may portray the precise nature of the activity which led to the involvement of the criminal justice system.
The Judicial System. A second major subdivision within the criminal justice system fits loosely under the label of the judicial system. Comprising this apparatus are the various courts (state and federal, trial and appellate), prosecutors, public defenders, and private attorneys. It intersects at numerous junctures with law enforcement and corrections.
Since law enforcement efforts produce primarily heroin possession arrests, it is with possession offenses that the courts most often deal. During 1976 there were an estimated 60,200 arrests in the United States for violation of drug laws involving opium or cocaine.84 Unfortunately, the national crime statistics do not separate heroin ("opium") from cocaine, nor do they indicate the level of offense—e.g., possession, distribution, or being under the influence. However, studies have been done that give some idea of the relative importance of the various offenses within the total arrest picture. One reputable study found that heroin was involved in roughly 48 percent of all non-marijuana arrests.85 Marijuana still produces the overwhelming number of all drug arrests—approximately 441,000 during 1976.86 However, with all but a small fraction of heroin arrests for possession, changes in policy affecting the status of possession would have a substantial impact on court resources.
It should be noted that state courts deal with the bulk of heroin possession cases. The federal enforcement effort is aimed primarily at trafficking activities,B7 and those who find themselves in federal court are most often there on charges of selling or transporting the drug. Federal and state appellate courts also have a significant number of cases concerning constitutional challenges to drug law convictions. Many of these constitutional attacks stem from possession-related convictions or charges; a change in that aspect of heroin's legal status would affect their numbers as well.
Corrections. The most varied set of criminal justice institutions comes under the heading of "corrections". Not only jails and prisons at the local, state, and federal levels, but parole, probation, and diversion to treatment programs can be grouped together as correctional in nature.
Although drug treatment services are ordinarily considered to be apart from the correctional system, in recent years the separation of the two systems has become less distinct. Pretrial programs of diverting drug-using criminal offenders (especially heroin users) into treatment are based on the notion that the drug use is the individual's dominant problem and is largely, if not totally, responsible for his or her criminal behavior. The courts and prosecutors have increasingly utilized treatment agencies as an alternative sentencing mode, frequently requiring treatment as a condition of probation or parole. Because treatment has become so closely allied with the criminal justice system, our discussion of the effects of alternative policies on that system will include their effects on treatment referrals.
The over sixty thousand arrested in 1976 for violations of heroin and cocaine laws comprised only about .06 percent of the national total arrests of 9.6 million for all offenses.88 Case dispositions are more difficult to determine than arrests, but 1976 FBI crime data indicate that around half of all drug offenders (including those for marijuana) were found guilty of the offense charged or a lesser one.B9 However, since the data base is small and all drugs are grouped together here, the actual conviction rate for heroin law offenses may be very different.
Aggregate studies of rates of incarceration and length of time served by heroin offenders are scarce. A study conducted by the National Commission on Marihuana and Drug Abuse reviewed arrests and disposition data for illicit drug offenses in six major metropolitan areas (Chicago, Dallas, Los Angeles, Manhattan, Miami, and Washington, D.C.)70 The study found that where only opiates were involved, the case was least likely to be dismissed.71 Approximately 36 percent of those charged with opiate (heroin) offenses were convicted.72 Of those convicted, only 8 percent were found guilty by trial; the remainder used the plea bargaining process.7" Nearly half received a sentence of incarceration.74 Of those convicted of only one offense of possession of an opiate (generally heroin), slightly over half (53 percent) received sentences of incarceration. Sixty-eight percent of those convicted for selling an opiate were incarcerated.75
Thus, the study indicates that while conviction is more likely for heroin offenses than for those with other drugs, only a little more than a third of those arrested are convicted and, if their offense is possession, only half of this number go to jail. Furthermore, few of those sent to prison receive long sentences. The National Commission's study of six metropolitan areas found that of those sentenced to incarceration with no time suspended, most received a term of a year or less.78
Nevertheless, American jails are overcrowded, and the addition or elimination of a few thousand offenders would have a considerable impact. At present there are some 191,400 inmates in state correctional facilities,77 28,000 in federal penitentiaries,78 and an estimated 136,388 adults detained in local jails and lock-ups.7B Further increases in the nation's inmate population are predicted.B° Expanding the housing capacity of our nation's prisons is expensive, as are the yearly costs of maintaining an inmate in an institutional setting.81 Heroin policies that change the numbers of those sent to prisons can certainly affect the costs of our correctional system.
The most common sentencing outcome for heroin possession convictions, aside from incarceration, is probation. Roughly a third of those convicted in the study sample examined by the National Commission received a probated sentence.82 Probation costs vary, but the nationwide average is around $2,000 a year per probation "slot."83 Treatment is frequently required for heroin law offenders receiving a probated sentence,84 and this increases the cost.B5 Policy changes could affect the number of those probated for heroin offenses as well as the number sent to certain types of treatment as a condition of probation.
Parole, the conditional release of an inmate, is frequently utilized for at least part of the heroin offender's sentence. These costs vary, but are roughly comparable to those for treatment required by probation or court referral. Again, changes in heroin policy may affect the numbers of those paroled for heroin offenses, the conditions of parole, and the aggregate cost to society.
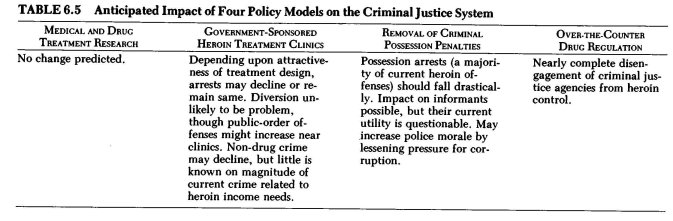
Table 6.5 outlines the predicted impact on corrections and the rest of the criminal justice system of each of the four alternative models under examination.
Medical and Drug Treatment Research with Heroin. Little effect, if any, can be expected on the criminal justice system if the medical and treatment research option is adopted.
Government-sponsored Heroin Treatment Clinics. Law enforcement, in particular, would be concerned over the potential here for diversion of legal heroin to "street" use. This concern is often expressed over proposals to try heroin maintenance in the United States, despite the fact that various powerful narcotic drugs are already used by existing drug treatment programs, are allowed in "take-home" form, and are available by doctor's prescription. With none of these practices has there been a significant diversion problem. Whether heroin obtained through a legitimate clinic system would be more susceptible to diversion than methadone or morphine remains an open question. It does, however, seem possible to design dispensing arrangements that could keep diversion to a minimum.88 The British experience with allowing treatment clinic doctors to prescribe heroin and ordinary pharmacies to fill the prescriptions without significant diversion problems may be unique to their heroin situation, population, and setting. It may also be significant that little heroin is currently prescribed there for drug treatment purposes. However, their success does provide an additional basis for believing that diversion need not be a major criminal justice problem.
If heroin clinics prove to be attractive to large numbers of compulsive users who are not at present involved in or attracted by drug treatment programs, the potential exists to reduce the amount of possession arrests and subsequent judicial and correctional involvement.87 However, experience with existing drug treatments indicates that there are a sizable number of addicted users who do not seek treatment. The addition of heroin to the treatment pharmacopeia, especially in a strictly supervised, heavily controlled program designed to prevent diversion, may make little difference to this group. If this proves to be the case, little impact can be expected on heroin offense arrest rates.
Allowing heroin to be used in treatment would not provide legal access to the drug for "chippers" or other nonaddicted users. They can be expected in this situation to continue to deal with illegal traffickers. Even some of those involved in treatment with heroin could be expected to supplement their clinic dosages with street-obtained ones. For example, British heroin clinic patients occasionally use street drugs, and there is a continuing, albeit small, black market for heroin in that country.88 While the provision of heroin through clinic programs could not be expected in itself to banish the enormously profitable and sizable American black market, it might significantly reduce the size and profitability of that market by drawing away the heaviest users.
Similarly, heroin treatment clinics could have an impact on non—drug crime. To the extent that the provision of heroin in a treatment setting would attract heavy users who cannot support their use solely through legitimate income, non—drug crimes committed to produce revenue would probably decline. What the public perceives to be the effect of the proposed clinics may, to an extent, prove to be self-fulfilling. It is notable that in the United Kingdom the notion that heroin users are invariably involved in other criminal activities has never surfaced as a public or governmental concern.89
The potential for an increase in public-order offenses like loitering, harassment and public intoxication and minor criminal offenses like shoplifting in the immediate vicinity of treatment clinics is high. Addicts' generally unsavory reputations and reports of their activities in the surrounding communities were key factors in the hurried closing of America's heroin and morphine maintenance clinics in the early 1900s.90 However, news accounts of the time tended to sensationalize matters, emphasizing programs that were poorly administered and overlooking those that functioned smoothly, just as do modern media accounts of methadone program problems. Administrative considerations could either aggravate or virtually eliminate the problem of clinic patients' offenses in the area of the program.
Removal of Criminal Penalties for Personal Possession. Dropping criminal penalties for the "simple" possession of heroin would mean that fewer heroin law offenders would be arrested or found in court or the corrections system. Since over 80 percent of current heroin law arrests are for possession, removing that activity from the criminal law would have a major impact on the involvement of the American criminal justice community with heroin use.91 However, a significant relationship could continue if treatment or education referrals were to be mandated in place of the former criminal penalties. Such a substitution would accelerate the absorption of drug treatment into the criminal justice system as an alternate form of supervised release.
Affected law enforcement and judicial resources could of course be reallocated to other offenses should penalties for heroin possession be dropped altogether. While most drug law arrests are "spontaneous" (no prior investigation done), the involvement of special narcotics officers, as opposed to ordinary patrolmen, is more extensive in opiate arrests than with other drugs.92 Some savings, therefore, in the form of redirected law enforcement resources could be anticipated.
Law enforcement officials often stress the importance of penalties for relatively minor offenses like heroin possession as "leverage" on users in order to reach traffickers. The available evidence does not provide a clear answer whether informants would be harder to obtain. The National Commission has found that less than one-quarter of opiate arrests have been the subject of prior investigation,93 and less than a quarter of these have involved an informant.94 Yet while only 6 -7 percent of all opiate arrests involve informants, these arrests could involve a high percentage of trafficking or distribution offenses (available data does not identify the type of case).
However, other data, particularly on the size of ordinary drug buys, provide some substantiation of the view that most trafficking cases involve low-level distribution offenses.95 Most users and low-level dealers cannot lead enforcement authorities very high into the distribution system.B° It is still possible that enforcement officials might be somewhat hampered in developing cases against major traffickers without the possession offense to hold informants, but existing data on the use of informants in major narcotics case development do little to substantiate these fears.
However, critics of the current American law enforcement approach to narcotics offenses believe that reducing the role of the informant may be a healthy development. Police corruption has been a perennial problem in drug law enforcement. For example, the involvement of police in buying and selling drugs, protecting informants, blackmailing users, taking bribes, and partaking in other related corrupt practices led to a well-publicized investigation and resultant shakeup in the New York City Police Department in the early 1970s.97 Removing criminal penalties may lessen for enforcement officers the opportunity and pressure to participate in corrupt practices or illegal activities (illegal search and seizure, for instance).88 However, the national experience with police corruption connected with gambling offenses suggests that the problem will not totally disappear.99 Still, by eliminating the source of most arrests, it may be substantially reduced. Societal respect for the law and its enforcement officers, rather than lessening, may increase as a result.
The argument that heroin decriminalization would increase the difficulty of enforcing antitrafficking laws gains some support from an analogy to gambling law enforcement: The accepted general proposition with gambling is that if not all participants are subject to penalties, enforcement against the "supplier" becomes more difficult.10° Another argument against decriminalization (frequently expressed regarding marijuana) is that such laws signal societal approval—or at least an end to strong disapproval—of that drug's use. Yet the actual effect of decriminalization on enforcement efforts is difficult to measure. Most simple possession arrests for heroin at present lead to discharge, probation, or treatment in lieu of prosecution and prison terms. In some jurisdictions, police, prosecutors, and judges are highly skeptical of the value of arrests, trials, and convictions for simple heroin possession and have instituted de facto decriminalization; arrests for possession are not vigorously pursued nor, when made, are they generally prosecuted, in these jurisdictions.101 Formal legislative action in these areas to remove criminal penalties would seem only to assure that policies already in practice there would be applied in an even-handed fashion. It is worth noting that federal enforcement efforts are already focused upon distribution offenses and international trafficking activities.'o2
Internationally, there may be criticism and even cynicism expressed about an American heroin decriminalization policy. American officials have vigorously campaigned against illicit drugs in other countries for more than sixty years. Any retreat from our current hard-line stance on heroin may seem ironic to foreign governments long accustomed to U.S. pressure to subject their narcotics activities to stringent controls and penalties.
Over-the-Counter Drug Regulation. With this policy option, for other than relatively minor regulatory infractions—e.g., dispensing to underage minors, possession by them, use of false identification or a false name to register for receipt of heroin, intoxication or driving while intoxicated—criminal justice agencies would probably be almost completely disengaged from their present involvement with heroin. Despite the present existence of a large, reasonably well-organized, and prosperous black-market distribution apparatus, it would seem likely that the advantages to consumers of legally obtainable, low-priced heroin would help end these illicit trafficking arrangements. An appropriate analogy is the virtual disappearance of the American bootlegging industry after the repeal of alcohol prohibition in 1933. In any case, the impact of OTC heroin regulation on criminal justice agencies of all types, at all levels, would be profound when contrasted with their present involvement.
Civil Liberties Aspects. Critics of current American drug policies often single out the adverse consequences of present drug law and enforcement practices not only on general respect for law but on the preservation of individual rights and liberties guaranteed by the Constitution. The prohibition approach to heroin in particular has raised numerous civil liberties issues: Illegal searches and seizures, wiretapping, illegal detention, and warrantless entries into private homes have all been documented in innumerable court cases and press reports. Perhaps even more disturbing are the less visible inroads into individual rights, implemented without opposition because they are supposed to be for the public's protection—the "good of society." For example, the diversion of drug users from the ordinary criminal process into treatment, even for non-drug offenses, has been widely implemented and frequently commended; but by so doing we have allowed the blame for non-drug criminal activity to be foisted on the drug itself, and tend not to hold the defendant personally responsible. It also places the criminal justice system in the curious position of "sentencing" a defendant to receive medical and psychiatric therapy for a condition that was not even the cause of arrest, and either dropping the actual charges or considering successful completion of treatment as evidence of rehabilitation in the ultimate sentencing process.103
The key effects of the alternative models considered are noted in Table 6.6
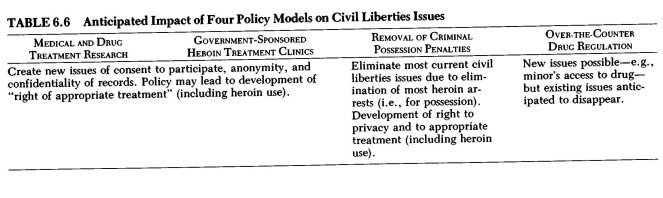
Medical and Drug Treatment Research with Heroin / Government-sponsored Heroin Treatment Clinics. A new civil liberties issue posed by the possible implementation of either of these policy options is that of the consent of research or clinic patients to participation in the proposed program. The history of medical research projects indicates that frequently those chosen as subjects are people who are the least capable of giving fully informed, voluntary consent.104 To avoid problems, heroin treatment clinicians and researchers would need to explain to potential participants the nature of the program, the extent of supervision and monitoring required during and after the treatment of research, and the medical implications of heroin use. The extent to which the subject's anonymity would be maintained is a necessary part of the information to be given, as is acknowledgment of the patient's right to withdraw consent.'°5
Confidentiality in any drug treatment or research program is of paramount concern to both client and program because of the stigma attached to illicit drugs, especially heroin. Current federal regulations prohibit the disclosure of patient-identifying information except under certain limited circumstances.1" However, recent proposals would allow more extensive use to be made of research subject identification for research and law enforcement purposes.107 Regulatory interpretation of the vague statutory language concerning confidentiality changes from time to time, and usually has reflected a bias toward permitting law enforcement and "evaluation" use of identifying data. To gain and keep the full confidence of treatment clients and research subjects, the clinic must itself be relatively immune from court-ordered or enforcement-demanded disclosures of patient identity.
In the event that heroin clinics are implemented on a permanent basis, the growing judicial doctrine of a right to "appropriate" medical treatment may come to include the right to receive heroin to prevent withdrawal stress or for other legitimate reasons. For instance, the Karen Ann Quinlan case in New Jersey set forth a legal rationale for the right of the patient (or the patient's guardian) to determine appropriate treatment for herself.108 Similarly, several courts have found a right to use laetrile as a cancer treatment, even in the face of official opposition. These recent developments suggest that it would not be unreasonable to expect a right to appropriate treatment to be applied to access to heroin in a clinical setting.109
Removal of Criminal Penalties for Personal Possession. Critics of
current heroin policy cite law enforcement abuses as a major reason for scrapping the prohibition approach. Warrantless seizures and searches of persons and homes and other similar violations of constitutional rights are natural outgrowths of a "war-on-drugs" philosophy where any breach of constitutionally guaranteed rights may be considered acceptable in the name of stopping the "drug traffic." The decriminalization of heroin is often posited as a potential solution to these civil liberties abuses. Certainly removing simple possession penalties for heroin would be a significant step toward ending the "war" mentality against the drug. Absent the removal of penalties for all present heroin offenses, however, it is likely that some civil liberties problems would continue, albeit at a lower rate than previously. Certainly the removal of criminal possession penalties would substantially lower law enforcement interest in identifying mere heroin users, except as they could assist in apprehending and prosecuting traffickers.
A right to privacy—which would encompass the right to use heroin, at least in one's home—is another factor indicating that criminal heroin possession penalties should perhaps be dropped. Many civil libertarians have long argued that individuals ought to be free to take drugs—or engage in any other personal activity—so long as no one else is hurt. A Supreme Court justice has described the notion of a constitutional right to privacy as "the right to be left alone—the most comprehensive of rights and the right most valued by civilized man."10 Although the extent and exact nature of the consitutional right to privacy have not been fully defined, recent cases have declared it to encompass the right to possess "obscene" material in private", the right to possess and use contraceptives even if unmarried, m, '13 and the right to have an abortion."4 The Alaska Supreme Court found the use of marijuana in the home to be protected under a right to privacy provided for explicitly in the state constitution and ... implicitly in the federal Constitution""; however, the same court decided against a similar privacy right to use cocaine.1° The interpretation of this right as applying to heroin use, like the right to appropriate treatment discussed above, is a possible, but far from certain, outcome of this policy option. However, it is also possible that judicial development of these concepts may precede, and in fact lead to, policy changes.
There is some precedent for court-ordered heroin decriminalization under present law. The Supreme Court in a famous 1962 decision declared that it was "cruel and unusual punishment" to penalize the mere status of being an addict."7 More recently, long terms of imprisonment for minor marijuana offenses have been found to violate the same constitutional prohibition.'ra
The rationale of the insanity defense has been used in the context of arrests for heroin use to assert that the defendant had an "irresistible impulse" to use the drug and therefore could not be held accountable.119 This popular stereotype of every heroin user as controlled by the drug and unable to stop using heroin or committing other crimes is at variance with the existing and emerging data on heroin use (see pp. 197-204 above). Removing criminal possession penalties for heroin may shift public and judicial attitudes away from this criminal image toward an acceptance of the medically or mentally "sick" model. However, continued judicial acceptance of the idea of "irresistible impulse" in heroin use is certainly possible even though the concepts on which that theory is based are more folklore than scientific fact.
Over-the-Counter Regulation of Heroin. Individual rights and civil liberties would tend to suffer little with over-the-counter drug regu-
. lation, in contrast to present policy. Some problems are always possible, however. For instance, requiring the registration of heroin purchases presents the risk of unauthorized public disclosure and the possibility that some may decline to obtain needed drugs due to fear of thus being stigmatized. The U.S. Supreme Court has considered a challenge to such a filing system in New York State, and has found that it passed constitutional muster.'2°
Other issues may also appear, such as that of the right of minors to obtain and use heroin legally under an OTC system with a minimum age requirement. There are indications that some courts may rule favorably on the question of a minor's right to obtain heroin if medical necessity can be shown .121 Enforcement response to possible diversion and fraud problems with an OTC system could perpetuate some current civil liberties issues—e.g., unreasonable search and seizure. For those disqualified from obtaining heroin legally, illicit possession would still be a punishable offense, and the current defenses of "cruel and unusual punishment" and "irresistible impulse" would probably continue to be asserted in court.
Health Issues. Present prohibitionary policies toward heroin make it necessary, of course, for users to obtain and use it illicitly in a street setting. This illicit heroin is often mixed, in order to increase the seller's profits, with a variety of substances and adulterants, some of which can lead to serious medical consequences. In contrast, heroin in a pure form, administered in a sterile manner, is relatively benign in terms of its physiological effects.122 Thus many of the most serious health risks associated with heroin use appear to be the indirect results of the laws that ban its use. "Overdose" deaths commonly occur from the consumption of heroin in combination with certain other drugs or from adulterants contained in illicit heroin. Hepatitis and endocarditis are frequent ailments of Amer-cAn heroin users brought on by the failure to observe sterile conditions in intravenous self-administration of the drug. Other diseases reflect the street setting of current heroin use in different ways; for example, "The high incidence of venereal disease reflects the occupational hazard of the many females who earn their drug money through prostitution."123
On the other hand, other aspects of the drug indicate that there are health problems involved that cannot be eliminated by policy change. Heroin does have a strong potential for creating a physiological dependence complicated by increasing tolerance to the drug's effects. Although this potential may have been overstated in the past, its existence is beyond dispute. (The potential for dependence is also strong for other, currently legitimate drugs like alcohol and certain barbiturates.) One must also note that individuals vary widely in their response to both tolerance and toxic aspects of drug use. These factors are particularly critical for younger users.
Considerations other than their drug-taking behavior will influence the health of heroin users under any drug policy mechanism. Living in an impoverished setting, lacking adequate shelter, and having neither a balanced diet nor adequate access to medical care are as important in determining the level of individual health as heroin use itself. For all our concentration on the aspects of physical well-being that can be affected by drug policy, we sometimes overlook these external influences on health and the degree to which they affect heroin users.
Medical and Drug Treatment Research with Heroin. Implementation of this policy would offer the possibility of substantial gains in knowledge relating to heroin's usefulness in general therapeutic as well as drug treatment applications. Recently some leading public health officials have announced their backing of proposals to look into analgesic applications of heroin for those terminally ill with cancer.124 Drug treatment research would help determine the extent to which the health of chronic, compulsive users can be improved through the provision of pure drugs in sterile settings with medical and nutritional counseling available.
Government-sponsored Heroin Treatment Clinics. To improve their health as it relates to heroin use, chronic users would have to be attracted into the treatment setting where medical services and pure drugs can be made available. As stated previously, there is a wide variety of possible program designs for use of heroin in a drug treatment setting. The specific program design and administrative aspects will determine its attractiveness to the street user, especially the compulsive one not interested in present treatment options. For clients of the new clinics, the incidence of disease from infected needles and the risk of poisoning or overdose from adulterated street heroin of uncertain potency would be lessened. The extent of the improvement would appear to depend on two major factors: the extent to which clinic patients would supplement their clinic heroin with other drugs, including street opiates, and whether the heroin is administered at the clinic or by the user himself in a "take- home" procedure. "Take-home" administration may increase the risk of hepatitis, endocarditis, and other infections from unsterile conditions. Supplements of illicit heroin would also increase the possibility of health complications. The possibility of accidental overdose would be increased by either factor.
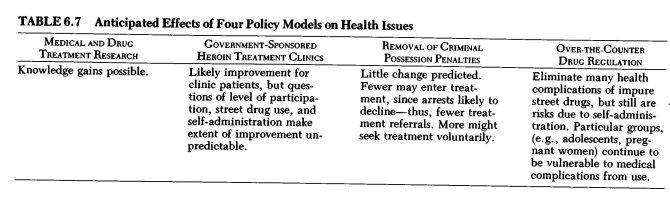
It is undisputed that clients' use of street drugs continues in American drug treatment programs as well as in British ones. One recent study found that in England heroin maintenance patients were more likely than oral methadone maintenance patients to use street drugs of all types, and to have more frequent hospital visits for treatment of physical complications associated with illicit drug use.1E5 Such evidence shows that illicit heroin and other injectable drugs may be used by a minority of clinic patients despite the provision of legally supplied heroin. This supplementing of licit heroin may be a greater problem in the United States—with its large, well-established black market—than in Great Britain, which has never had any large-scale illicit heroin trafficking.
Removal of Criminal Penalties for Personal Possession. Implementation of this form of heroin decriminalization would probably do little to improve the health of the user. The policy would amend the criminal law by removing penalties for certain activities involving controlled substances, but would not add to existing treatment nor provide a licit, supervised, and standardized source of supply for heroin users. Present diseases associated with street heroin use can be expected to continue, as would occasional poisonings and overdoses.
If criminal justice referrals to treatment drop by reason of fewer heroin users coming into contact with enforcement authorities, this option could actually lead to a higher incidence in health problems among compulsive users. On the other hand, should the option require treatment for those cited for heroin possession, some improvement in health for compulsive users might be achieved. Removing criminal penalties may also encourage heroin users with health problems to seek medical help who would otherwise fear being reported to law enforcement authorities.
Over-the-Counter Regulation of Heroin. Guaranteed purity levels and sterile hypodermic syringes available at local pharmacies with an over-the-counter regulatory approach would probably eliminate most black-market heroin use and resultant health complications. This policy, among all those examined, has the greatest potential to reduce the current disease complications of heroin use. A legal, readily available, reasonably priced supply of heroin would seem to virtually eliminate the competitive edge of black-market heroin.
Nonetheless, some health hazards would be expected to continue. For instance, the possibility of addicted infants as a result of maternal prenatal use is currently a problem both for heroin-using pregnant women and those on methadone. Allowing the over-the-counter purchase of heroin would not end this health problem, which is likely to be present under any policy (including the current prohibition approach). The problem with individual variations as to tolerance and toxicity levels would also continue. In addition, self-administration would continue problems of the sterility of works and uncontrolled, compulsive use.
Another area of uncertainty regarding potential health hazards in this model as well as the others, is heroin use by adolescents. An OTC model would probably establish minimum-age requirements for the purchase of heroin. While adolescent and preadolescent use appears to be low at present, it is significant enough to cause concern. Continuing adolescent heroin use means a continuing risk of overdose complications, due to the lower tolerance of youthful users to heroin toxicity. It may also provide another outlet for black-market sales, which would be expected to decline appreciably among adult users.
Adverse effects from the use of heroin in conjunction with other drugs would also be a continuing problem, as with use of prescriptive drugs before or after alcohol use, a common present-day hazard. Mixing other legal and illegal substances with heroin—whether by design or accident—quite often leads to medical complications. Over-the-counter regulation may play a role in increasing public awareness of the risks of using heroin in conjunction with other drugs, but it is unlikely to end all accidental or intentional drug mixing.
Other Issues: Worker Productivity and Welfare. Attempts have been made to quantify in economic terms the costs to American productivity that result from heroin addiction.126 A recent study commissioned by the National Institute on Drug Abuse estimated the loss of productivity due to heroin "abuse" at between $4.167 and $6.644 billion.127 The greatest single component in these calculations is the cost of unemployment.'28 However, there is considerable doubt about the extent of total unemployment that can be ascribed solely to heroin use. In fact, when data are compared for heroin users and nonusers from the same socioeconomic background, there seems to be little difference in employment rates. At the very least, studies that ascribe the total cost of unemployment and absenteeism to heroin use overstate the connection. Even if unemployment were causally related to heroin use to a significant degree, the costs are largely due to the present system of control rather than intrinsic to heroin use.
Among the various costs other than unemployment associated with loss of productivity are absenteeism, heroin-related deaths, incarceration, and those associated with medical treatment—whether emergency room visits, inpatient hospitalization, mental hospitalization, or drug treatment programs. The losses due to drug-related deaths and medical treatment time away from the job might decline under some—but not all—alternative policies. As mentioned above, unemployment and absenteeism appear to be rooted in other, deeper, socioeconomic problems and policies than heroin use. Consequently, the possibility of a heroin policy change making a great impact on them one way or the other is remote, especially since the stigma of drug use would linger and lead many employers to discriminate.12° Costs to productivity due to incarceration would probably be affected dramatically by the removal of criminal penalties for possession of heroin, but not a great deal by the other alternatives.
Our society has provided several mechanisms by which those in need receive limited funds from the public coffers. These mechanisms include public assistance payments, disability (either Social Security or Supplemental Security Income), unemployment benefits, medicaid, housing subsidies, and food stamps. The level, duration, and eligibility requirements of such payments vary widely from state to state and also among the individual recipients within any given state.
Chronic heroin users tend to come from disadvantaged backgrounds, are often undereducated and unskilled, generally cannot find jobs, and face several levels of discrimination and frustration at every turn. To identify heroin use as the sole reason for welfare payments to a person facing these handicaps is to seek a scapegoat for society's ills. Although heroin use may play a role in the equation, to design policies as if it were the only or the most important factor would be to miss the mark. The numerous attempts to make educated guesses at the amount of welfare assistance that results from heroin use remain, at best, guesses.
The effect of policy changes on these and other costs would depend upon the type and extent of heroin use developing after the particular policy change. For example, if over-the-counter regulation of heroin were adopted and compulsive use levels were to rise sharply among the present low-level or nonusing population, one would expect welfare costs to rise as well. On the other hand, if in this situation controlled use grew but the chronically using population remained about the same, one would expect little change in welfare costs. Other outcomes would also be possible, though, depending on the real relationship between heroin use and worker productivity; even with all types of use increasing under a given policy we might experience a dramatic drop in welfare costs if, simultaneously, more jobs were available in those inner-city areas with the highest incidence of compulsive heroin use.
Changing the Law: Legal Aspects of Alternative Policies. More often than not, official obstacles to innovative heroin control measures are rooted in the attitudes of the bureaucratic agencies charged with implementing and administering the law rather than in any rigidity of the law itself. What commonly passes for "law" is frequently only the prevailing view; in practice, statutes are susceptible to a considerable range of interpretation. Present American domestic law—federal and state—permits a fairly extensive range of control policies, as do our international treaty obligations.
In the international sphere, heroin is subject primarily to the controls of the 1961 Single Convention on Narcotic Drugs as modified by the Protocol of 1972,130 where it is listed as a Schedule I drug along with such other drugs as morphine, cannabis, and methadone. The Single Convention requires party nations, of which the United States is one, to limit opiate use and production to "medical and scientific purposes."131 The purpose of the Single Convention is twofold: to limit the quantity of world narcotics to that needed for medical and scientific purposes, and to regulate the manufacture and use of scheduled drugs to ensure that they are used only for those approved purposes. The treaty also demands that party nations prohibit the possession of any Schedule I drug, such as heroin, "except under legal authority."132
"Legal authority" in the United States is supplied by the Controlled Substances Act,13 a portion of the Comprehensive Drug Abuse Control and Prevention Act of 1970.134 The Controlled Substances Act, like the Single Convention, arranges drugs according to schedules, but its classifications have a different meaning than do the Convention's: By definition, a Schedule I substance in the act cannot have an "accepted medical use in treatment in the United States."135 Heroin, then, has no currently approved medical use in the United States, although related opiate drugs such as morphine are listed under Schedule II of the act as having legitimate medical usefulness. This distinction between the two drugs results from domestic policy, not international law.
The Food, Drug and Cosmetic Act also applies to narcotics controls.136 This act requires FDA approval of any new drug prior to its marketing or general medical use. Thus, FDA approval may be required for heroin policy to change.
The last layer of control and regulation consists of state and local laws. Federal law preempts conflicting state rules in the areas of manufacture and medical dispensation; however, the states are deeply involved in criminal heroin law enforcement. Many—in fact, most— states have adopted the Uniform Controlled Substances Act, but there is considerable variation in their penalties and other criminal provisions. Penalties for possession, for example, range from conditional discharge to life in prison. Since the federal laws relating to possession are largely unenforced, state laws have great practical significance in this area.
Medical and Drug Treatment Research with Heroin. Existing law does permit tightly controlled, experimental medical research with any Schedule I drug, including heroin. Federal administrative action is required for this, but U.S. manufacturers can be registered to produce the heroin needed for research purposes, and practitioners registered to employ heroin in a research project.137 Both the Drug Enforcement Administration (DEA) of the Department of Justice and the Food and Drug Administration of the Department of Health, Education, and Welfare must approve the application of a person wishing to conduct such research. Once the FDA (acting for the Secretary of Health, Education and Welfare) approves the research application, DEA (acting for the Attorney General) can reject it only on very limited grounds, such as fraud.18 Recently, upon solicitation from the National Institute on Drug Abuse (NIDA), the Sloan-Kettering Institute for Cancer Research has received approval and funding for a five-year study evaluating heroin in relation to other narcotic analgesics in cancer therapy.'"B
The Single Convention—the international law controlling American regulation of heroin—similarly permits heroin research to be conducted at the discretion of signatory nations. The official commentary on this treaty indicates that heroin maintenance treatment of addicts was contemplated by its drafters to be within the "medical purposes" restriction.L40
Since federal law preempts conflicting state law in the regulation of heroin, heroin research, once approved by the appropriate federal agencies, could not be prohibited by state action. Federal law would preclude any state action to stop the work of a federally-approved heroin researcher from going forward."'
Government-sponsored Heroin Treatment Clinics. Using heroin in the addiction treatment process comports with international law in that both the Single Convention and the 1972 Protocol make clear that the use of heroin to maintain or otherwise treat addicts was contemplated by the treaties' drafters.12 The United Kingdom has utilized this section of the treaty to authorize heroin maintenance programs on its home soil.
To permit treatment clinics to use heroin in their programs on a nonexperimental basis, however, heroin would have to be transferred from Schedule Ito Schedule II of the Controlled Substances Act.143 Such a scheduling transfer is accomplished by administrative action involving three federal agencies: the Department of Health, Education, and Welfare, the Drug Enforcement Administration of the Department of justice, and the Food and Drug Administration of HEW. The rescheduling move could come about by one of three means: initiation by the Attorney General, by the Secretary of HEW, or by petition.144 The Attorney General cannot control a drug HEW says should not be controlled, but he has the ultimate authority to decide appropriate scheduling once HEW agrees that a drug ought to be controlled. However, HEW findings on scientific and medical matters are binding.
The Attorney General is also responsible for registering practitioners who dispense narcotic drugs for use in treatment—not only methadone, but heroin as well.145 Once a practitioner is found qualified by the Attorney General, he must approve the registration, unless he finds that the practitioner will not comply with controls against diversion. The Comprehensive Drug Abuse Control and Prevention Act of 1970 authorizes the Secretary of HEW to determine "appropriate methods of professional practice in the medical treatment of narcotic addiction of various classes of narcotics addicts."148 If the Secretary found heroin appropriate in a treatment setting, a clinic could be established in the hospitals and other health care institutions under HEW control.
The FDA as well would be involved in a decision to permit heroin to be used as a treatment drug. Generally FDA approval is required for all "new drugs" prior to marketing.147 If heroin is recognized as "safe and ef- fective" for treatment use, and if it has been found to have been used to a "material extent or for a material time,"18 it will not be required to go through "new-drug" application procedures. Since some forty-four American heroin and morphine clinics existed during the period 1918-22,19 it is possible that the prior use requirement may in this way be met for "new-drug" purposes. Heroin might also be exempt from "new-drug" requirements through operation of the "grandfather clause" of the Food and Drug Act of 1938, which recognized prescribed drugs permitted under the earlier 1906 act.1S0
Further action would be required in order to secure an adequate supply of heroin for the clinics. Opium is currently prohibited from import for the purpose of manufacturing heroin,15' and none is grown domestically. However, DEA might make its heroin seizures available for either research projects or established heroin clinics. Another possibility is to manufacture heroin from the concentrate of poppy straw that is now imported to manufacture codeine.152 A more permanent source of supply—legal importation of raw opium or refined heroin or domestic cultivation—would require statutory amendment of federal law.
Without the federal administrative action above described, states cannot implement heroin clinics of their own. Conversely, they could not enforce state criminal laws against clinic patients or clinicians for heroin possession or distribution offenses if the federal government were to sponsor heroin treatment clinics. State law on controlled substances—whose regulation is a legitimate national concern having interstate commerce implications—must give way to federal law if it directly conflicts.'53 Whenever the two laws can coexist, the courts will generally let both stand. For instance, amendments to federal law could permit states to allow treatment programs using heroin without requiring all states to adopt such programs. In order to achieve more state initiative, however, it may be necessary to have an explicit federal statutory expression setting out a policy permitting states to determine appropriate treatment policies, including the use of heroin within their borders.154
Removal of Criminal Penalties for Personal Possession. This policy could be achieved without altering present international agreements by amending either federal or state law or both. Nothing in the 1961 Single Convention prevents the United States from lifting criminal penalties for the possession of heroin. The convention merely requires that possession not be allowed "except under legal authority,"155 and permits (but does not require) signatory nations to prohibit the manufacture or use of the drug.'" If a control measure other than prohibition seems to be the "most appropriate means of protecting the public health and welfare," that measure may be adopted.'57
However, complete removal of criminal heroin possession penalties at the federal level would require statutory amendment of the 1970 Comprehensive Act. Rescheduling heroin to Schedule II would result in decriminalization only for those receiving clinic heroin. Such partial decriminalization of heroin possession could occur also as a result of a clearly enunciated policy position of the Department of Justice through DEA.158 In fact, DEA has already declared its policy is to concentrate on traffickers, rather than on "the ultimate user of drugs."159 However, a policy of nonenforcement would simply be de facto decriminalization, which could be revoked without notice or disregarded selectively for certain offenders.
States could remove criminal possession penalties from their statute books even in the face of continued federal prohibition. Such an action is not inconsistent with "supremacy requirements," since federal enforcement agents could still enforce federal law even in a heroin- decriminalized state. Only where a positive and irreconcilable conflict between federal and state law exists must state law give way.
Over-the-Counter Regulation of Heroin. Once again, international law poses no obstacle to implementation of an American domestic policy allowing heroin users to obtain the drug as an over-the-counter preparation. The discussion above about the obligations of parties to the 1961 Single Convention to prevent "unauthorized" possession applies here as well.
Federal law would require statutory change in order to allow access to heroin as an OTC drug without prescription.1ß0 Specific aspects of an OTC heroin regulatory scheme, such as identification and registration of the buyer, would also require statutory action. Prescription sale of heroin, on the other hand, could be accomplished simply by administrative action to reschedule heroin to Schedules II or III of the Controlled Substances Act. FDA approval of heroin as a "new drug" would also be required, unless it was found to be exempt as discussed above.
Since statutory change is required at the federal level to accomplish over-the-counter regulation of heroin, legislative action at the state level alone could not effect this policy change. An independent over-the-counter state legislative scheme would almost certainly conflict with contrary federal law and be invalid. However, with appropriate enabling legislation at the federal level, individual states could promulgate various regulatory measures pertaining to the process of dispensing the drug, registering sales, and the like.
Concluding Thoughts
The alternative heroin policies discussed in this chapter are only a few of the many possible choices available to American policymakers. They are not a timetable for liberalizing present heroin policies, nor should the order in which they are discussed be regarded necessarily as a logical policy progression. Some policy changes could occur simultaneously with others; while the selection of some other policies would necessarily preclude certain others from being put into force at the same time. Any policy change will lead to more knowledge of the ways in which heroin policy affects both individuals and society in general, knowledge which is in large measure lacking at present. This new knowledge may give hints of promising new directions, or it may indicate what policy aspects may produce problems.
The use of heroin itself may increase even more, or may gradually decline over time. History provides no evidence on which to base a belief that the drug could ever be entirely eradicated, and one might well wonder why this particular drug should be the focus of so much attention when many other substances of equal or greater potential for abuse are readily available. More than six decades of effort to eliminate the drug from the United States through strong law enforcement measures have not caused the number of users to drop below levels observed at the beginning of this century. Even if there is general agreement that heroin use is not desirable, absolute prohibition is difficult, if not impossible, to achieve in the real world—particularly in a democratic, nonauthoritarian society such as ours.
As a society we ought to remember that by maintaining current heroin policies we are also making a choice. If we choose this option, we should evaluate the probable costs and benefits at least as carefully as with alternative policy proposals. The benefits and shortcomings of current policies can, perhaps, be judged by different and stricter standards, since so many years and so much effort have been put into the task of trying to make them work.
This chapter and those preceding it clearly question not only current drug policies but the premises on which those policies are based. Our analysis rejects stereotypical notions about heroin users and challenges the rationale for a continued strict prohibition approach. The discussion has focused on the issues involved, rather than on the policy models themselves. That the latter are by no means the only possible options is a statement that bears repetition. At the same time, it is useful to sum up some conclusions based on this discussion.
First, there appears to be no good reason to continue to withhold approval of serious research proposals to investigate the utility of heroin in either general therapeutic or drug treatment applications. The potential knowledge to be gained is considerable and the risk minimal.
Second, the immediate implementation on a broad scale of treatment clinics using heroin is inadvisable. However, there does not seem to be good cause for rejecting carefully designed proposals submitted by individual states or local governments to initiate such clinics on a limited, test basis. Permitting greater flexibility and diversity in the national response to heroin problems is critical to the development of policies that match the needs and desires of the communities involved.
Third, while the removal of criminal penalties for possession of heroin would have a salutary effect on civil liberties, it would not be an effective response to the crime problems caused by heroin's high "black-market" cost. Greater consideration ought to be given to combining variants of this policy with the treatment clinic option or others (such as greater physician discretion and over-the-counter regulation for further detailed examination) .
Fourth, our heroin policy need not be monolithic, at least not as monolithic as it is currently. The nature and extent of heroin problems vary widely from city to city and region to region. Requiring a uniform policy has proven to be self-defeating in the long run. The participation in the planning and implementation of heroin policies of the states and cities where heroin problems are most severe is a vital need.
Fifth and finally, we recognize that by proposing the serious consideration or adoption of alternative policies we run the risk of being branded as "pro heroin." Insistence on the single, unrealistic goal of the elimination of heroin has led many to mistakenly believe that our national choice is between control and no control, rather than among differing degrees of control. It is not a black-and-white issue; we feel it is important to take the risk of being misunderstood in the hope of achieving greater understanding and of effectively addressing the very real problems we face today.
In the absence of absolute knowledge and the power to foretell the future, we need to pursue more vigorously policies that minimize individual and social harm and abandon those that cause more harm than they relieve. An honest evaluation of the adequacy of our response to heroin and to all psychoactive drugs calls for the reasoned consideration of a full range of alternative policy choices.
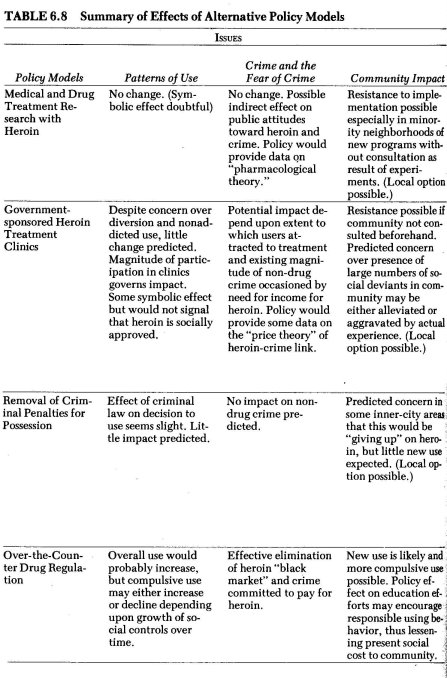
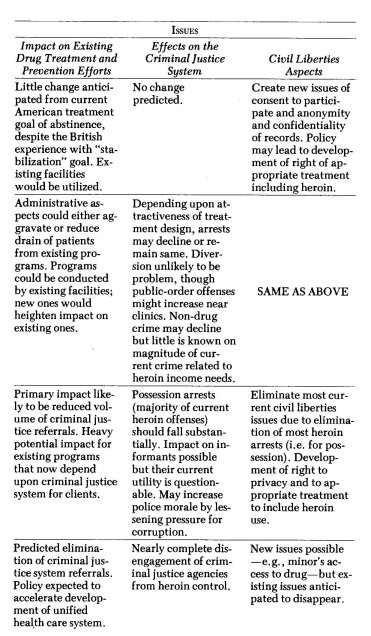
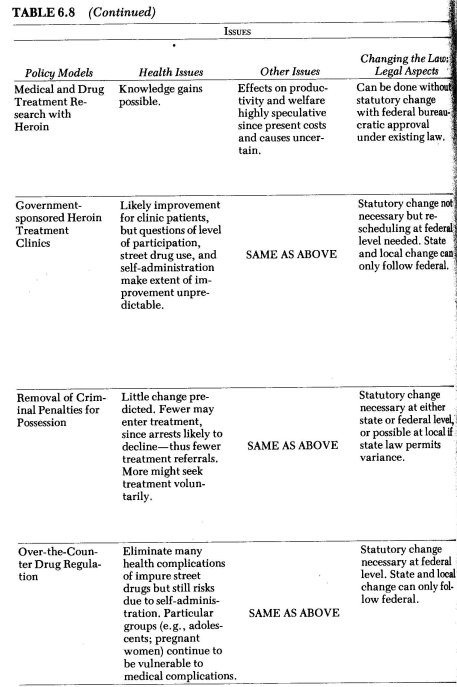
| < Prev |
|---|