| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4.1% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 180 |
| Yesterday: | 251 |
| This Week: | 180 |
| Last Week: | 2221 |
| This Month: | 4768 |
| Last Month: | 6796 |
| Total: | 129367 |
REACHING THE UNREACHED: TARGETING HIDDEN IDU POPULATIONS WITH CLEAN NEEDLES VIA KNOWN USERS
 |
|  |
| 
| Books - Drug Use as a Social Ritual |
Drug Abuse
REACHING THE UNREACHED: TARGETING HIDDEN IDU POPULATIONS WITH CLEAN NEEDLES VIA KNOWN USERS
Around 1985 the spread of HIV among injecting drug users (IDUs) in the Netherlands became a serious concern to policy makers, drug service agencies and users themselves, organized in so called Junkie Unions. The first AIDS prevention initiatives, aimed at IDUs were established by these pressure or interest groups of drug users. In Amsterdam the AIDS inspired needle exchange was initiated by the MDHG, a user-based organization in 1984. The earliest AIDS prevention leaflet for drug users in the Netherlands was produced by the Rotterdam Junkie Union. Already in 1981 this union was distributing clean syringes and needles at places in the drug scene where IDUs gathered to prevent the spread of hepatitis. When it became apparent that HIV would also mean a menace to Dutch IDUs the Rotterdam Junkie Union immediately started a needle exchange. This was long before the municipal needle exchanges opened. At first, these activities were exposed to firm opposition from the police, the treatment agencies and the municipal authorities. Insight in the magnitude of the AIDS epidemic was yet to come about at these levels. In Rotterdam, where this research was conducted, the municipal needle exchange system was established in the first half of 1987. This rather late start was due to resistance in some parts of the treatment system. Among other arguments, it was felt that needle exchange would encourage injecting and undermine drug free treatment (1). Nowadays, these arguments are generally seen as obsolete and, more important, they have proven to have no scientific basis (2). At the end of 1986 HADON, an at that time small and experimental outreach and drug information program, took the initiative and set up a needle exchange. Soon the rest of the city was to follow.
In Rotterdam, as in many other Dutch cities, needle exchanges are predominantly tied to the methadone programs, mainly methadone maintenance programs. The advantage of this Rotterdam approach is that these programs are in contact with approximately 1000 regular heroin users (both smokers and IDUs) on a daily basis. However, estimates of the number of heroin users in Rotterdam vary between 2500 and 3500, (3, 4) not counting those drug users from the suburbs, that are also oriented on Rotterdam, both for drugs and help. The proportion of IDUs is approximately 25% for both in and out of treatment groups (5). Although the needle exchanges at the methadone programs are open to non-clients, few actually use them. This means that on a daily basis at least 60 % to 70% of the target group is not reached by the municipal needle exchange system. Additionally, the composition of the in treatment cohort is often subject to rapid changes (4). Furthermore many users have switched from heroin to cocaine as their drug of preference (6) and for this reason methadone presumably has become less valuable for them. Based on these grounds the outreach and information project HADON, which in 1989 fused with the Odyssee foundation, made reaching hidden populations of active out of treatment drug users, generally the unreached, into its main AIDS prevention priority. This chapter gives a brief description of the working methods of this project and present some results of the pilot evaluation study conducted.
HADON is a neighborhood-based information program providing outreach, prevention and referral services to active out of treatment IDUs in the north of Rotterdam. The program started in 1985: before the health implications of the AIDS epidemic among the IDU population were generally acknowledged in Rotterdam. Due to this evolving epidemic the priority of the program has been shifted towards the prevention of HIV transmission. Besides the contacts in the project's storefront premises, the outreach workers visit on a regular base many places in the scene called User collectives. The outreach workers supply the attendants of these places with clean needles, condoms and up-to-date information on HIV/AIDS. The uniqueness of the program lies in its two-tiered organization of needle exchange. In addition to supplying these prevention materials in the storefront and while doing outreach, the workers stimulate certain key persons to exchange needles at their user collectives. This approach was initiated after several program attendants requested large numbers of needles, explaining they lived together with several other active IDUs. These user collectives are frequently visited by other IDUs from the same or related networks. Thus, visitors can exchange individual needles (individual exchange) or, upon special agreement, exchange containers of used needles for boxes of 100 new needles (collective exchange). The containers are plastic and can hold approximately 200 used needles. The HADON collective exchange tier has been experimentally initiated in order to determine if the outreach component of the program could be extended and improved. Secondarily, the experiment examined if the motivation of visitors could be reinforced through stimulating a willingness to both exchange and collect used needles and take more responsibility, not only for their own individual health, but also for the health of their IDU peers. This second aspect is based on the observation that social support is a common phenomenon in user networks, as was demonstrated in previous chapters.
In this pilot evaluation study needle exchange contacts of the HADON program were registered. For each exchange contact the program staff registered date, minimal demographics the number of needles and containers dispensed and the number of needles returned.
The collective exchange was defined as "making available large amounts of sterile needles and sharpsafe containers at strategic places in the scene so that there are always needles available at those places where drugs are used." Individual exchange has been defined as "those exchanges and supply transactions concerning small quantities of needles" (7). According to these program definitions a collective exchanger was defined as an exchanger who has at least once taken out a box with needles and a container and has at least once returned a container. When needles were returned in a container, the actual number of needles was estimated by a weighing procedure (8). Quantitative data analysis was conducted at the level of 1) the individual exchanger, and 2) the exchange contacts. Staff of the program was questioned on the contents of their work and their knowledge on the attendants and program routines were observed. Data on how the programs goals were addressed in the networks of contacted drug users was collected during the in this thesis reported ethnographic field research.
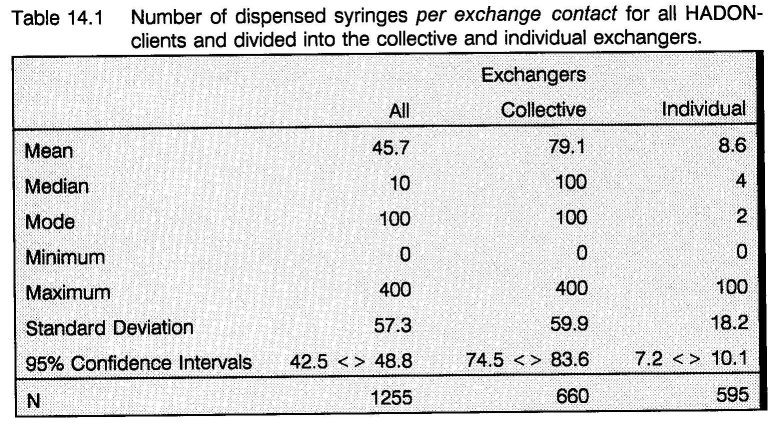
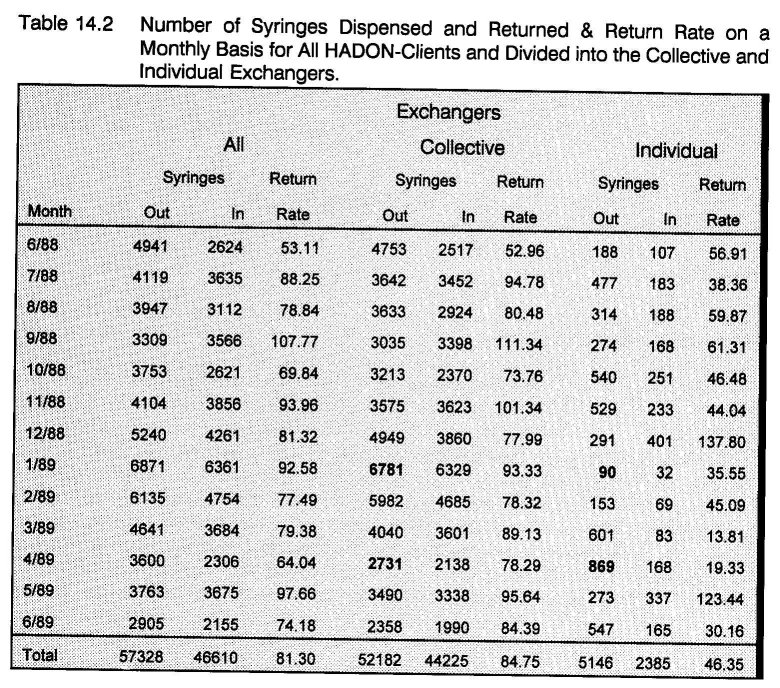
From May 1988 to June 1989 the HADON needle exchange project involved 104 regularly registered exchangers. 1255 needle exchange contacts were registered. 25 clients (24%) were classified as collective and 79 clients (76%) as individual exchangers. The mean number of supplied needles over the 595 individual needle exchange contacts is almost 9. For the 660 collective needle exchange contacts this number is 79. (table 14.1) During the research period a total number of 57328 needles were supplied of which 91% went out through the collective exchange. In total 46610 needles were returned, which gives an exchange-rate of 81.3%. Profound differences in exchange-rates were found between the two groups: 46.4% for individual and 84.8% for collective exchangers. (table 14.2)
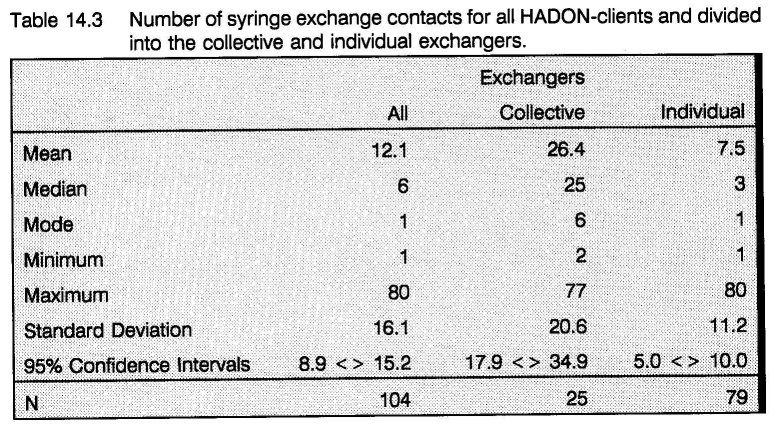
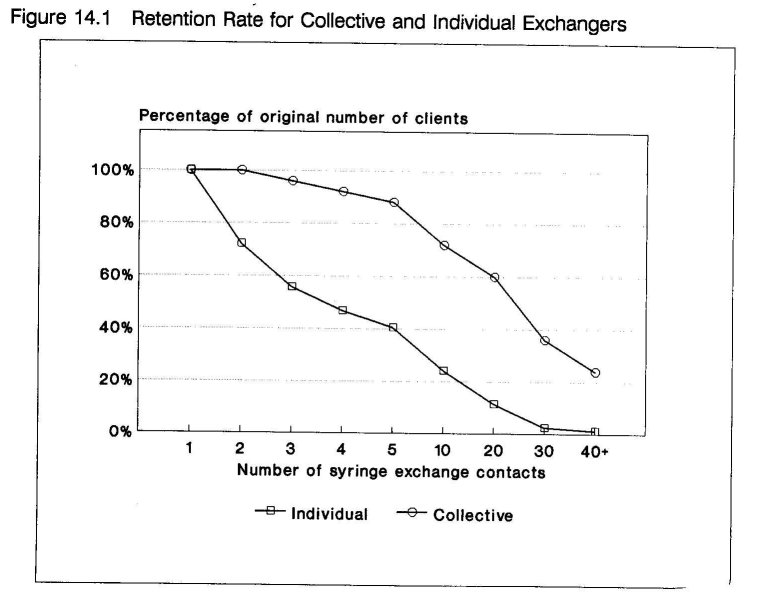
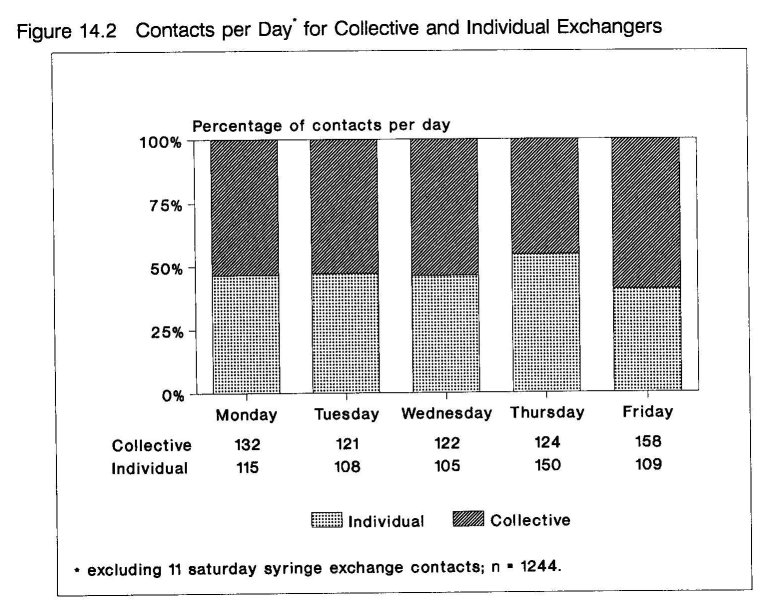
The program's holding power was remarkable in retaining especially the collective exchangers. The mean number of contacts of individual exchangers is 7.5, for the collective exchangers this is 26.4. (table 14.3) 52% of the collective exchangers visited the program 25 or more times. (figure 14.1) Moreover, the collective exchangers (only 24% of the clients) accounted for 52.6% of the total number of needle exchange contacts. The mean number of days between each needle exchange contact is 15.8. A breakdown for the days of the week does not show big differences in contact rate. Individual exchangers have their top day on Thursday and collective exchangers on Friday. (figure 14.2)
To complement these results, the ethnographic fieldwork data provide insight in how the program's goals are addressed in the networks of IDUs contacted by the program. Although during the fieldwork places were visited where hygiene regarding injecting was poor, the impression is that users who are engaged in the collective exchange are more aware of risk behaviors and put more energy in health maintenance and hygiene as can be seen in the following excerpts from fieldnotes:
When Freek had finished injecting he rubbed some Hyrudoid balsam on the needle wound. "One of you guys want some too?", he asked Ronald and Frits. Frits took some of the ointment and rubbed it on his arm. "It's good stuff for your veins", said Frits. "Yes it also disinfects the wound", Freek replied.
Richard is still cleaning up the room: "It is always possible someone is coming by and then I don't like this stuff laying around." The syringes, swabs and other papers go into the plastic bag that's already filled with other used spikes, bloody swabs, etc. "This is for Sak" (a worker of the neighborhood exchange program). For extra security Chris takes of the needle from the syringe. Then he takes out the piston totally and puts the needle inside the syringe. Then he puts back the piston and presses it so the needle inside crumbles together. "Now nobody can hurt himself on it. You have to be aware, I think."
As at many dealing addresses it is not allowed to inject the purchased drugs, IDUs often go to a friends place to inject. Karel is participating in the collective exchange and lets his friends and acquainted IDUs get off at his place:
Although it isn't out spoken, Karel agrees on Jerry wanting to take a shot at his place. Jerry wants to shoot up pure cocaine. He puts his spike on the table and asks Karel for a spoon. Karel asks, "Is that an old spike you want to use ?" Jerry replies, "Well, old, I've used it one time before, so it's still good for usage." Karel says, "I've got some new one's left from HADON", and hands one over to Jerry, "do you want some more for tonight or the weekend?" Jerry replies, "If you can spare them I'll take some with me." Karel gives him 4 in total.
The needles distributed through the collective exchange are thus having a reach beyond the user collectives. Besides for on the spot use they are distributed among other users to take home. For many IDUs the availability of clean injection equipment is a strong incentive to frequent those places. The ethnographic research was not limited to the work area of the outreach program. The following fieldnote was recorded at the shooting room of a dealing address in another neighborhood:
From the corner where she's still busy with the needle in her hand Anja asks, "Do you have a new syringe for me ?" Eric answers, "No, this is the only one I got. I was lucky, one minute before the pharmacy closed I bought it. Then Anja asks, "Can't I use it when you're finished. I can't use these anymore", pointing at the syringes laying around her on the floor. "They're all blunt, I can't hit a vein," she says as if she's crying or starting to cry. "Or let me only use the needle then. Please let me, I will clean it for you. Don't be afraid. I've got no AIDS. I've been tested recently at the methadone program." Eric still refuses, "I would like to help you but it's the only one I've got. I never lend out my spike to someone else, nobody, not when I have to use it myself again. When I'm not using it again it's their own risk."
Although needle sharing did not take place, the fieldnote illustrates the (often emotional) pressure to share a needle. In this case, in spite of the pressure Eric decided in the interest of his personal health and against the norm of sharing. Nevertheless, the situation can often be tense. When comparing fieldnotes 3 and 4 the functioning of a variable of perceived responsibility for safe use becomes apparent. In fieldnote 3, the perceived responsibility is given a collective quality. Because the needle exchange program dispenses supplies to IDUs, the possession of ample needles allows IDUs to reinforce subcultural norms of sharing, (9) yet in a safe way. In contrast, in fieldnote 4, traditional subcultural sharing norms conflict with the more recently emerged norms regarding safe use. The perceived responsibility is marked by a strong quality of the rugged individual junkie who resists the pressure of community sharing norms through adhering to a personal behavior code.
Not only were needles distributed among visitors of user collectives, an exchange of new needles among user collectives was also observed:
Harrie left with a bunch of new needles to the dealing place where Ronald and Frits had bought their dope. "They have a shortage of shooters there", he said before leaving.
When the goals (extending the outreach component of the program, stimulating the users to take an interest into their own health and that of other users) are considered, the program is making an important contribution. In the evaluation study of the British needle exchange schemes a return rate of 62% was found (10). Often it is felt that a high return rate is the result of strict rules regarding a one for one transaction. The findings do not support this thesis. The high return rate of the collective exchange is not accomplished by strict rules but through trust, respect and a shared responsibility in combination with supplying the necessary tools for save injecting practices. Likewise, the retention rate of the collective exchangers can be regarded very high when compared with the findings of the British evaluation study (33% over 5 visits) (10). However, the number of dispensed needles, exchange rates and even retention or drop-out rates are insensitive measures of effectiveness.
They are only crude indicators of the varying stages in the process of cultural change that is going on in the subcultures of IDUs. It is a fundamental misunderstanding to think that IDUs will confine their needle shopping to one distributor (11). An evaluation of the San Francisco Prevention Point needle exchange found that 13% of supplied needles were returned to exchange sites other than the supplying one (12). People use needle exchanges like they (and everybody) use any other shop and thus similar motivations determine when and what shop will be visited.
An interesting difference is found between the top days of individual and collective exchange. On Thursday most unemployed users receive their social benefit monies and the individual exchange rises markedly. Friday (weekends the program is closed) is the top day for collective exchanges. It seems that individual exchangers are more driven by situational determinants (the availability of money), while the collective exchangers have included getting clean needles in their daily life as a planned activity.
The ethnographic data show that the goals of the program were positively anticipated in the injecting community. Clean needles were at hand at high risk places when needed, distributed through IDU networks and even exchanged among user collectives. Similar results are found in the British needle exchange evaluation study by Stimson and colleagues. Not only did they find that the initially much higher needle sharing rates of the non-attenders of needle exchanges declined much more dramatically than those of the initially lower scoring attenders, but they concluded that, facilitated by needle exchanges, a climate is developing in which the sharing of used injection equipment is no longer the norm. The British researchers related this to the increased availability of needles in the community due to needle exchange, pharmacy sales and other sources. It was found that many attending users supplied their non- attending friends --the high risk group-- with new needles (13).Thus, sufficient availability of clean needles at places where drugs are injected supports the newly emerging norms regarding safe use in a way that these do not conflict with other subcultural rules regarding sharing (9).
A disturbing factor: police raids on dealing addresses
A closer look at table 2. shows that after a steady grow of the issued needles from june 1988 to january / february 1989 in march / april an immense downfall occurs. This collapse may be attributed to increased police raids on dealing / using addresses in that period. While the collective exchange is going down 60% from january to april, the individual exchange rises with almost 1000%. This may be called a short term effect as in the following months the individually issued needles join the downward trend of the collective exchange. This is due to the space reallocation of many of the regular visitors of the closed down addresses towards the west and other parts of Rotterdam. And in this west part of Rotterdam recently history again repeated itself (6). These findings do not only support the assumption that many active IDUs are actually reached by the collective exchange. They also show that repressive police activity can have a negative effect on AIDS prevention efforts (14, 15). A fine tuning of public health and judicial policy in favor of an effective AIDS prevention policy is urgently needed.
In conclusion, these findings suggest that the exchanging of needles can be made more effective by employing collective social means in contrast to individualistic psychological strategies. The use of naturalistic settings (e.g., the placing of the plastic container at user collectives and dealing addresses), existing drug user networks and appeals to injecting drug user's responsibility may be more powerful determinants of variations in needle exchange rates than psychological characteristics of individuals. In any case, engaging drug users themselves as an integral part and partner of the outreach work provides an interesting topic for further investigation and development. In Rotterdam, it will be interesting to see in the future whether this human resource and social manner of exchanging will be more effective than more technologically inspired approaches (e.g. needle exchanging machines) that are also planned for the city's AIDS prevention efforts.
- Heiningen RM van: Spuitomruilfaciliteiten: Voorstellen tot uitbreiding van de spuitomruilfaciliteiten binnen Rotterdam. Rotterdam: Odyssee, 1988.
- Buning EC: De GG & GD en het drugprobleem in cijfers, III. Amsterdam: GG & GD 1988.
- INTRAVAL: Harddrugs & criminaliteit in Rotterdam. Groningen: Stichting Intraval, 1989.
- Toet J: Het RODIS nader bekeken: Cocainegebruikers, Marokkanen en nieuwkomers in de Rotterdamse drugshulpverlening rapport 87. Rotterdam: GGD-Rotterdam e.o., Afdeling Epidemiologie, 1990.
- Grund J-PC, Kaplan CD, Adriaans NFP, Blanken P.: Drug sharing and HIV transmission risks: The practice of "frontloading" in the Dutch injecting drug user population. Journal of Psychoactive Drugs. 1991; 23(1): 1-10.
- Grund J-PC, Adriaans NFP, Kaplan CD: Changing cocaine smoking rituals in the Dutch heroin addict population. British Journal of addiction 1991; 86: 439-448.
- Barendregt C: Toen was er AIDS, of de ontwikkeling van de collectieve spuitenomruil. Rotterdam: HADON/Odyssee, September 1989.
- Blanken P: Spuiten ruilen bij HADON: Een evaluatie van de individuele en collectieve omruil. Rotterdam, 1990.
- Wieder DL: Telling the code. In: Turner R (ed): Ethnomethodology: selected readings. Middlesex, England: Penguin Education, 1974: 144-172.
- Stimson GV, Alldritt LJ, Dolan KA, Donaghoe MC, Lart RA: Injecting equipment exchange schemes: final report. London: Monitoring Research Group, 1988.
- Stimson GV: Personal communication, 1991.
- Guydish J, Clark G, Garcia D, Case P, Sorensen J, Chu G: Needle exchange: Where have all the needles gone? presented at the VI International Conference on AIDS, San Francisco, USA, 1990. [Abstract no. S.C.762]
- Donaghoe MC, Dolan KA, Stimson GV: Life style factors and social circumstances of syringe sharing in injecting drug users. London: Centre for Research on Drugs and Health Behaviour, 1991.
- Des Jarlais DC, Friedman SR:Shooting galleries and AIDS: Infection probabilities and 'tough' policies. Am J Public Health 1990; 80: 142-4.
- Chitwood DD, McCoy CB, Inciardy JA et al.: HIV seropositivity of Needles from Shooting Galleries in South Florida. Am J Public Health 1990, 80: 150-152.
| < Prev | Next > |
|---|