| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4.1% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 181 |
| Yesterday: | 251 |
| This Week: | 181 |
| Last Week: | 2221 |
| This Month: | 4769 |
| Last Month: | 6796 |
| Total: | 129368 |
CHAPTER III COCAINE CHLORHYDRATE: SCIENTIFIC ASPECTS
 |
|  |
| 
| Books - Cocaine the Legend |
Drug Abuse
CHAPTER III COCAINE CHLORHYDRATE: SCIENTIFIC ASPECTS
One of the longest standing and serious problems faced by medicine has been and still is pain. This is the one capital symptom that urges both the patient and the physician to seek relief.
Before the invention of anesthetics, the medical sciences, particularly in the practice of surgery, faced a great problem directly related to pain. The mere extraction of an aching tooth presumed an enormous task for both the patient and the dentist. The doctor had to struggle not only with the disease but also with the unrelenting resistance of the patient, a natural reaction to avoid the pain caused by surgical intervention. This matter was often resolved in ways beyond belief: a good knock on the head to render the patient unconscious, have him dead drunk, or simply immobilize the patient to prevent movement which made of him a terrorized and helpless witness of his own painful predicament.
We can, of course, imagine the difficulties or consequences derived from these old methods, often worse than the disease itself. Let us also think of the difficulties faced by the surgeon when attempting major surgery, such as the amputation of an arm or a leg.
The relief of pain is almost the end itself of medical science. Pain acquires particular interest when it is the physician himself who causes more pain than that he intends to cure. At one time, nitrous oxide or laughing gas improved things somewhat by inducing deep sleep on the patient, but this new type of anesthetic known as total, had the risks inherent to systemic action. A deep chemically induced sleep always implies the possibility of brain damage or cardio-respiratory arrest by the central nervous system. This is a calculated risk if surgical intervention will solve a life or death problem. Nevertheless, minor operations, such as tooth extraction, presume a risk not proportioned with the degree of the ailment.
It was Vassili von Anrep, of the University of Wursburg, who first perceived in 1880 the anesthetic properties of cocaine. Later Karl Koller, an associate and friend of Sigmund Freud had the opportunity of using the anesthetic properties of the new substance in eyeball operations. It fulfilled all requirements of a medication long dreamed by surgeons - the ideal anesthetic - a drug that would effectively and reversibly block the pain impulses sent to the brain, keep the patient fully conscious without the dangers of chemical sleep and, more specifically, without causing defensive behavior.
Long before, in 1859, Albert Niemann at the University of Gottingen had succeeded, in isolating this substance contained in the leaves brought in from the mountains of the Andes, the coca leaves. Its active component was cocaine, the famous compound which was a major player in American history of the twentieth century and its famous war against drugs.
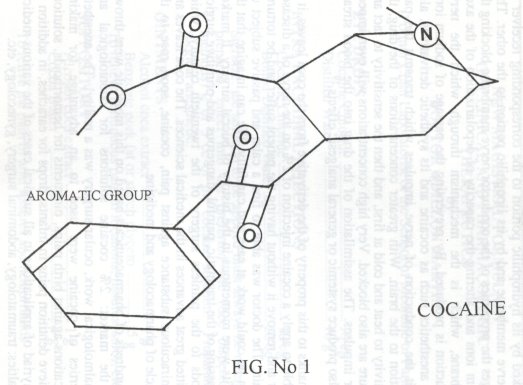
The substance is actually methyl-benzoyl-ecgonine. It is an ester of benzoic acid and a nitrogenated base which may be considered as a tertiary amine to which it owes its local anesthetic properties. 17
The fundamental structure can be viewed as formed by three portions: Lipophilic group, Hydrophilic group, and the Aliphatic group which joins the first two groups. 's (See figure 1)
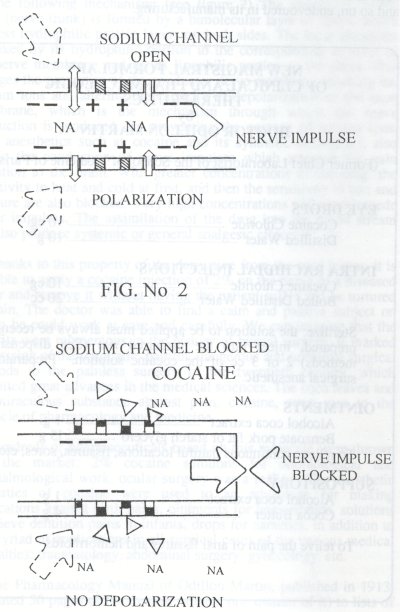
When the substance was applied to a nerve trunk, it either blocked or reversibly interrupted the passage of nervous impulses which transmit the sensation of pain to the nerve centers of the brain, and more importantly, without loss of consciousness. This peculiarity, since called the local anesthetic effect, we now know was produced by the following mechanism: (see figure 2) The membrane of the axon (nerve trunk) is formed by a bimolecular layer of lipids, which possess hydrophilic protein layers on both sides. The local anesthetic is linked by its hydrophilic portion to the corresponding receiver of the nerve membrane and by its lipophilic portion to the other. This changes the properties of the conductor nerve membrane blocking the sodium ions and altering the capacity of depolarization of the axon membrane, which is the mechanism through which the nerve conduction is produced. By preventing the passage of sodium ions, local anesthetics such as cocaine and its synthetic derivatives, also inhibit the conduction of nerve impulses which transmit the pain sensation to the brain. With greater concentrations of the drug, the sensitivity to heat and cold at first, and then the sensitivity to tact and pressure are also blocked. Very high concentrations will even impede motor impulses. The assimilation of the drug into the blood stream can also produce systemic or general analgesic effects. 19
Thanks to this property of the derivative from the coca leaves, it is possible to apply a cocaine injection of 2% on the nerve of a diseased molar and remove it without having the patient suffer and be tortured by pain. The doctor was able to find a calm and passive subject on whom he could work at ease and carefully. We can imagine that the benefits were momentous in the history of buccal surgery. It marked the passing of the traumatic, painful, dangerous and primitive surgical methods to the painless surgery of the twentieth century, which permitted great advances in the medical sciences. The coca leaves and the miraculous substance against pain, cocaine, soon rose to the pinnacle of pharmacology and medicine.
Hundreds of pharmaceuticals based on this molecule were thrown into the market: 2% cocaine solutions for odontological and ophthalmological work, ocular surgery was a reality!. The anesthetic properties of cocaine were used to an advantage for making medications against birth pains, ointments for hemorrhoids, solutions to relieve dentition pains in infants, drops for earaches, in addition to the myriad of applications in all surgical cases of the various medical specialties: traumatology, abdominal surgery, gynecology, etc.
The Pharmacology Manual of Odillon Martin, published in 1913, dedicated 50 pages of the treatise (almost one quarter of it) to lists of indications for the use of cocaine. The big pharmaceutical companies, such as Merck, le Pharmacie Centrale de France, later on Parke Davis and so on, endevoured in its manufacturing.
In 1923, Richard Willstatter of the University of Munich succeeded in creating, the first synthetic cocaine molecule based on the coca leaf alkaloid molecule, named procaine. The new molecule also had the anesthetic and psycho-stimulating effects of cocaine, but it has a serious shortcoming: its anesthetic power was 50% below cocaine and had no hemostatic properties (which prevent bleeding). It was necessary to add vessel constricting substances, such as epinephrine to match the hemostatic properties of natural cocaine. The vessel constricting effect is important: it prolongs the anesthetic effect by preventing the rapid reabsorbtion of the drug, which is what happens when the neighboring blood vessels are normally dilated.
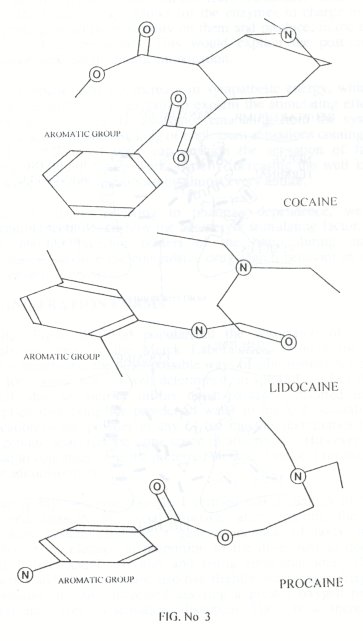
Shortly thereafter, other molecules, invariably superficial modifications of natural cocaine and having the same shortcoming: no vessel constricting or hemostatic properties, such as xylocaine, lidocaine, etc. (See figure 3) made their entrance into the huge vademecum of modern anesthetics. An so, like in the 1913 treatise of Odillon Martin, the cocaine molecule, with small variants and near the year 2000, continues to be the star of local anesthetics.
Modern local anesthetics have bee achieved through slight variations of the natural cocaine molecule (See figure 3). Thus, for instance, Novocaine, Tetracaine, etc., are tertiary amine esters of par-amino-benzoic acid instead of esters of benzoic acid or cocaine. Later on we will look into the current legal and multimillionaire aspects of this industry.
Parallel to the boom of cocaine as a local anesthetic in the world of surgery, the cocaine molecule entered in another scenario where it started as a hero and ended up as the villain or the culpable of all the evils of modem society: cocaine, and its modern derivatives also happened to be powerful stimulants of the central nervous system.
In man, the small doses of cocaine also act on the cerebral cortex, causing psychic stimulation with an increase of work capacity, possibly due to the absence of a feeling of fatigue (central analgesic action and reduction of the transmission of nerve impulses), then the production of excitement, even of a sexual nature, euphoria, loquacity, restlessness" states Manuel Litter in his Pharmacology Treatise.
On local anesthetics, he states: "Local anesthetics, once absorbed, produce stimulation, tremor, etc. Then (at highly toxic concentrations, most likely,) the stimulation phenomena is followed by central depression by exhaustion of the nerve centers." In reference to intoxication, Litter recommends: "...the best way to prevent and treat intoxication by local anesthetics is the dispensation of depressors. The same author, when dealing with opium and its derivatives qualifies them as selective depressors of the central nervous system. In other words, opium and cocaine, or local anesthetics are so contradictory that one of them is the antidote of the other. Later on we will examine why the Geneva Convention classified these substances as homologues.
Concerning the autonomic nervous system, the same author states: "Cocaine enhances the response of the innervated structures of the sympathetic system, as well as adrenaline and norepinephrine" (sympathetic chemical transmitters). In this way, they provoke vessel constriction, mydriasis and tachycardia (sympatho-mimetic action.).
For this reason, medium cocaine doses produce tachycardia and an increase of blood pressure on the heart. And, as in every excess, high doses revert their action and blood pressure can decrease intensely.
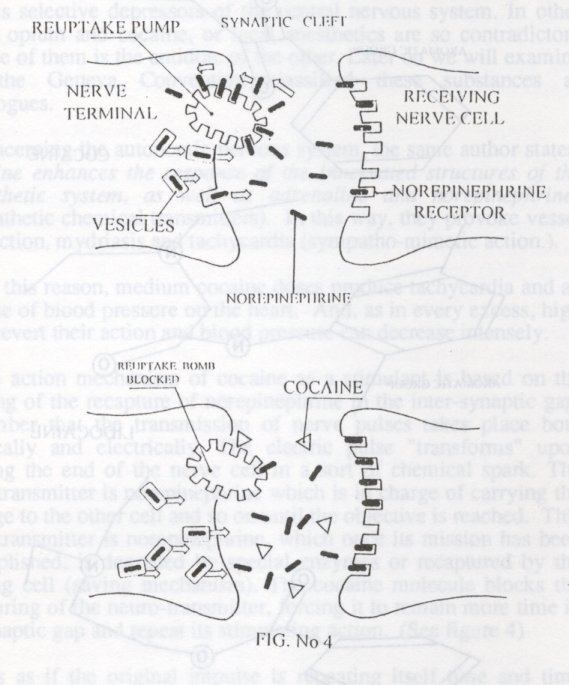
The action mechanism of cocaine as a stimulant is based on the blocking of the recapture of norepinephrine in the inter-synaptic gap. Remember that the transmission of nerve pulses takes place both chemically and electrically. The electric pulse "transforms" upon reaching the end of the nerve cell in a sort of chemical spark. The neuro-transmitter is norepinephrine which is in charge of carrying the message to the other cell and so on until the objective is reached. This neuro-transmitter is norepinephrine, which once its mission has been accomplished, is degraded by special enzymes or recaptured by the emitting cell (saving mechanism). The cocaine molecule blocks the recapturing of the neuro-transmitter, forcing it to remain more time in the synaptic gap and repeat its stimulating action. (See figure 4)
It is as if the original impulse is repeating itself time and time again. The final effect is a sympathetic energy many times higher, due to the summatory effect. For didactic purposes we could say that the adrenergic system undergoes a sort of "voltage increase"
On the other hand, the fact that the neuro-transmitter remains more time in the synaptic gap, allows for the enzymes in charge of their downgrading to act more steadily on them and produce, in the end, a depletion of its precursors. This would explain the post-cocaine depressive backlash in chronic intoxication.
It is probable that the increase in sympathetic energy, which by itself would suffice it to explain to explain the stimulating effect of cocaine, also receives the assistance emanating from the systemic analgesic action. 20 The blocking of unpleasant sensations coming from a tired or exhausted body can cushion the sensation of fatigue reaching the brain during work, thereby increasing the well known extra work tolerance mentioned by almost every author.
On the chapter referring to phanmaco-dependence, we will examine, in more detail, how the adrenergic stimulating factor, upon acting on the pleasure centers of the brain during massive dispensation, produce the compulsive drug-search behavior in search of the chemical orgasm.
Since Sigmund Freud popularized the absorption of cocaine crystals prepared by the Merck Laboratories, through the nasal mucous membrane, the other possible ways of administration were set aside for reasons not too well determined, in spite of the fact that he himself, due to injuries in his nasal passages, resorted to oral absorption dissolving the powder in water to drink it. Actually, the application of the powder in any of the mucous membranes (nasal, oral, genital, anal) has the same speed of absorption. However, nasal aspiration continues to be the preferred method, I suspect for reason of easier administration.
During my own observations, I verified that a quantity of 60 mg dispensed through the nasal mucoua, after entering the brain circulatory system produces a general increase of body energy. Metabolism accelerates in proportion to the dose, just as does the physical, intellectual activities and rising emotional tone. Cardiac frequency and blood pressure also rise slightly. Respiratory frequency and volume are also increased assuring a greater oxygen intake.
Hunger and tiredness sensations disappear. There is an increase of intestinal peristalsis, (something I did not observe in coca chewing), with the resulting lesser assimilation of nutrients. The latter, in association with the increase of metabolism, individual activity and the anorexia effect, explain the success achieved in weight reducing treatments, or the emotions produced in abuse cases.
The emotional areas are also stimulated. There is a pleasant peaceful feeling, and at higher doses one feels euphoria and enthusiasm. The user feels content, loquacious, uninhibited and courageous. If there was emotional depression before, it subsides rapidly, giving way to positive feelings about life in general.
Concerning the psychological effects, we observe an acceleration of all higher mental functions, such as capacity for thought course and association of ideas. The individual is wide awake, sleep can be postponed. The capacity for abstraction, concentration, attention and memory improves. The contents of thoughts is enriched and fantasizing or having more optimistic and pleasant ideas about life are facilitated. Sensorial perception becomes keen and sensitive.
In respect to sexual activity, cocaine has very definite aspects. It increases sexual desire and potency notoriously, according to reports from chronic cocaine users. A well known phenomenon, known through the traditional use of the leaves and evidenced by the Ecuadorian statuette which speaks for itself. (See figure 5)
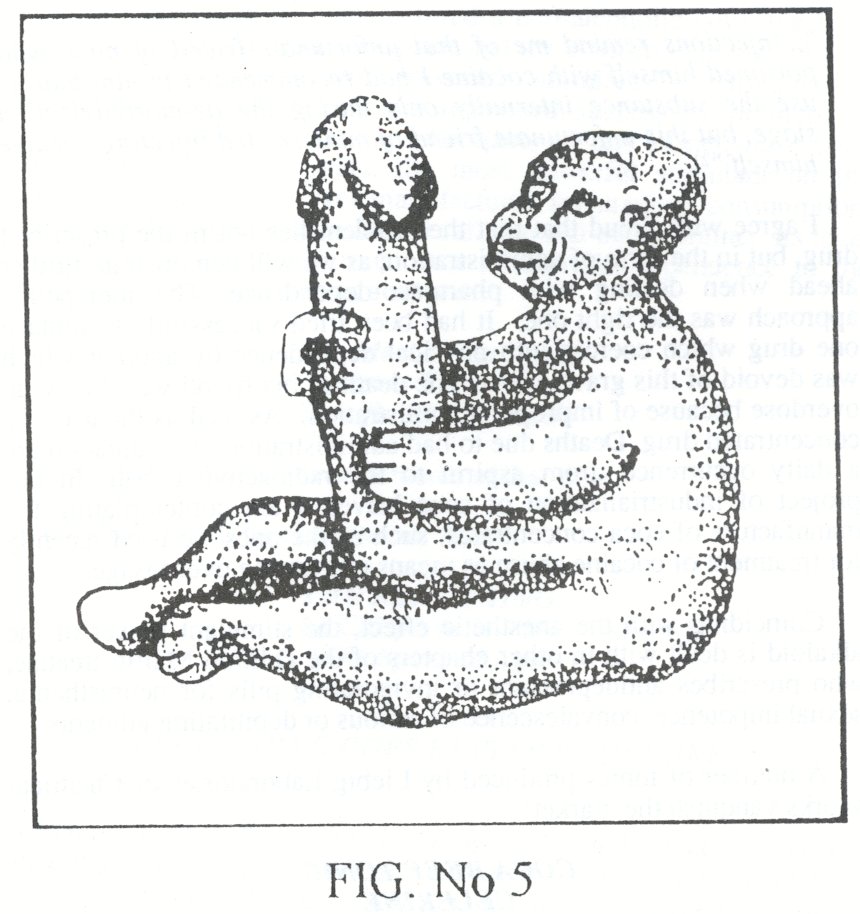
See the aculfco or coca leaves bolus swelling the cheeks of the phallic chewer. In general, a large percentage of users are in agreement that this effect is one of the reasons for its current increased use . Let us not forget that one of the mythical obsessions of man has been the fountain of youth, the prolonged life elixir, and associated with these myths is sexual power.
Such qualities of this substance allow us to presume very easily the other use, or rather abuse which made this molecule famous. Sigmund Freud is the one who continues disclosing the immense possibilities in another field of medicine, this time in psychiatry.
The founder of psychoanalysis observed that when cocaine was self administered through the nasal mucous membrane, the subject could achieve rapid relief of depressive symptoms. He was so enthused, that he ended up recommending it to patients and acquaintances, thereby playing a central role in the first attempt to cure morphine addiction through the use of cocaine. His friend, Ernst von Fleishl Marxow, following the amputation of an infected finger, became an opiate addict, which he used to relieve the pain. Freud recommended him cocaine to "leave" the morphine habit:
"...injections remind me of that unfortunate friend of mine who poisoned himself with cocaine I had recommended to him that he use the substance internally only during the de-morphinization stage, but this unfortunate friend of mine started injecting cocaine himself. "21
I agree with Freud that that the problem lies not in the prescribed drug, but in the form of administration, as we will demonstrate further ahead when dealing with pharmaco-dependence. The therapeutic approach was the right one. It had been tried successfully to replace one drug which coerces into physical dependence by another which was devoid of this grave effect. The death of his friend was due to an overdose because of improper administration. As well as the use of a concentrated drug. Deaths due to bad administration of medication are a daily occurrence, from aspirin to the radioactive cobalt. In our project of industrialization of coca leaves, I am contemplating the manufacture of coca concentrates, such as the ones we used recently for treatment of cocaine abuse as means of averting overdosage.
Coinciding with the anesthetic effect, the stimulant power of the alkaloid is dealt with in other chapters of the Odillon Martin treatise, who prescribes antidepressant or invigorating pills for neurasthenia, sexual impotence, convalescence of serious or debilitating ailments.
A number of tonics produced by Liebig Laboratories or Chemical Works vanquish the market:
COCA BEEF TONIC
CELERINE
CELERY COCA TONIC
(For the cure of apathy or sexual excesses)
In 1891, the boom of cocaine as stimulant begins with the famous Vin Mariani or Mariani Wine, distilled by Angelo Mariani, which in over 23 years of existence earned public praise from Popes, many heads of state and scientists the world over. The Vin Mariani was nicknamed the "elixir of life".
In 1887, Dr. Sttyth Pemberton from Atlanta gave birth to the world of Coca Cola when he manufactured a non-alcoholic beverage from the leaves of the Andean coca plant and the African cola nut. As we all know, it contains two powerful stimulants - caffeine and theobromine- which gave it the renowned success it continuos to enjoy today. As a result, the inhabitants of this planet, have been consuming, for many years, the most powerful stimulant on the central nervous system ever manufactured for massive consumption. It coupled the cocaine stimulant to caffeine and theobromine. Its level of acceptance and many true cases of outright dependence to the beverage should not come as a surprise:
The Ideal Brain Tonic
Relieves Exhaustion
Specific for Headache
read the celebrated advertisements of that time. Certainly it will be closer to our times
THE REAL THING
La Chispa de la Vida (spanish)
(The Spark of Life)
EVERYTHING GOES BETTER WITH COKE
"The real Thing" or (The Spark of Life) could, of course, be no other than the cocaine molecule. Is there another component that could be called the ideal brain tonic? One which relieves fatigue, stops headaches, etc. This is the only explanation of the commercial success achieved by the Coca Cola Company.
In 1903, in full bloom of cocaine as anesthetic and stimulant, and with out a coherent scientific or health explanation, a Presidential commission of the United States of America prohibited it use in foodstuffs. Coca Cola must withdraw its famous "spark of life", but retain the other two stimulants of the central nervous system: caffeine and theobromine.
The economic benefits must have been enormous, the more expensive component -cocaine- has been withdrawn from the beverage and sold aside. The "spark of life" goes on to join the millionaire world of local anesthetics. In 1914, the Harrison Act on narcotics of the United States declares cocaine and coca illegal, and through the International Conventions of 1925, 1931, the 1953 Protocol, and the Geneva Convention of 1961, extends the prohibition to the rest of the world. The stimulants made from coca leaves advertised and widely disseminated by Coca Cola, prohibited so rashly, conquer the world of the metropolitan underworld. The Twenties are initiated with apologies of cocaine, such as the Luke Jordan records, the Sherlock Holmes stories, Modem Times, by Charles Chaplin, etc., all silent witnesses of the epoch. The subversive music of the Sixties comes to the rescue of the secluded molecule: "Cocaine", by Erik Clapton and many others. The Eighties represent the natural response to any prohibition, to every persecution: resistance. The immense publicity spread by the war against drugs, becomes an encouragement for consumption, as has happened with every forbidden fruit. This was true not only of habitual consumers, but also of the large metropolitan moguls who do not delay in installing a gigantic transnational complex to market the forbidden molecule and whose general management is tried to be attributed, most unconvincingly to the illiterate, poor, disdained coca producer, who simply represents the lowest link of the chain, and the most ruthlessly exploited of the great drug-traffic transnational concern, the farmer who is simply producing something someone will buy.
SYNTHETIC ANESTHETICS AND THEIR COMMERCIAL SUCCESS AS PSYCHOTROPIC OR STIMULANT SUBSTANCES
The chemical structure defines the function. Synthetic anesthetics, by copying the chemical structure of cocaine, have not only succeeded in achieving the anesthetic effect, but also the stimulant or adrenergic effect (Figure 3). Already in 1949, the geriatric procaine properties were investigated by the Ana Aslan, a Rumanian doctor, who asserted in a work submitted to the Rumanian Medical Academy, to havefound the fountain of youth. According to her, procaine retarded the effect of cell aging and prolonged life. The fountain of youth. The dream of the alchemists.
Naturally, European aristocracy started to cue at the Aslan clinic in search of the magic remedy against old age. Celebrities of the epoch contributed to give commercial renown to Gerivital or KH3, the commercial brand of procaine. Among these were Nikita Khrushchev, Konrad Adenauer and General Montgomery.
Nowadays, procaine is the imperative component of geriatric tonics, such as Zellaforte, Lipogeron H3, or simply Procaine capsules called KH3, which indicate a recommended dosage of 15 to 20 mg, three times a day. That is the same amount consumed by drug addicts, but spread in three takes. Which assures, of course, the proper administration of the drug, which no independent drug addict ever complies with the resulting affects, as we shall see later on. This medical use shows irrefutably that modem pharmaceutical industry makes good use of the exhilarating effects of cocaine derivatives.
With respect to the presumed capacity of cocaine or its synthetic derivatives to retard cell aging, as asserted by Aslan, I do not know of any serious research which demonstrates this. But I believe that its anti-fatigue, euphoria causing, and particularly aphrodisiac properties are enough to justify the rejuvenating adjective with which it is marketed these days. After all, in our modern, hypersexual society of today, a synonym of youth is sexual prowess.
The use of the synthetic derivatives of cocaine are reserved not only to the legal trade. In the large urban centers, all cocaine derivatives have become in the object of use and abuse:
"And there was also procaine, lidocaine, benzocaine, tetracaine, butacaine, to "cut" coke one oneself before reselling it. An even powdered talcum, flour, starch, to fool the client.
One can find products to verify the purity of cocaine which one has just bought, such as methanol, pure soda. A whole series of cocaine substitutes, duly patented, are up for free sale, such as, for instance, Especial La Coke, a mixture of Ketamine and manitol), the California Brown (tobacco and meta-amphetamine, La Coco Snow (benzocaine, procaine and caffeine)".Says Alain Labrousse while telling about his trip to New York. ('The Cocaine Trail, 1986).
Van Dyke and Byck from Yale University demonstrated that experienced consumers of natural cocaine crystals could not distinguish lidocaine from cocaine when administered via nasal passages. They are in agreement that cocaine is not addictive, because that would assume that cocaine develops tolerance, i.e. it would be necessary to increase the intake progressively to achieve the same results, or even more, the drug would conduce to physical dependence, both of which have been shown to be absent in the use of cocaine. They compare the use of crystals with the behavior pattern some individuals experience with peanuts or potato chips. They are chronic consumers, when it is within their reach, and simply abstain when it is not around.
Experiments carried out in animals by the same research team showed that the drug-searching behavior can be caused both by procaine and cocaine. These authors conclude by stating; "...medically speaking, the drug is a relatively safe one, but in the hands of the wrong people it can lead to self destructive behavior. Many of the questions about the substance known as cocaine can be answered by scientific research, but the decision, in the last instance, will be political and economical". 22
Recent research, still unpublished, conducted by ICORI and the Bolivian Psychiatry Society (La Paz) reveal that encephalograms taken after nasal intake of 100-150 mg of cocaine chlorhydrate do not show any significant changes in cerebral functions.
| < Prev | Next > |
|---|