| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Appendix to report 4: country reports CZECH REPUBLIC
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
CZECH REPUBLIC
1 General information
Location:
Central Europe, southeast of Germany
Area:
78,866 sq km
Land boundaries/coastline:
1,989 km / 0 km (landlocked)
Border countries:
Austria 362 km, Germany 815 km, Poland 615 km, Slovakia 197 km
Population:
10,220,911 (July 2008 est.)
Age structure:
0-14 years: 13.8% (male 723,521/female 684,786)
15-64 years: 71.2% (male 3,653,679/female 3,619,872)
65 years and over: 15.1% (male 604,419/female 934,634) (2008 est.)
Administrative divisions:
13 regions and 1 capital city
GDP (purchasing power parity):
$251 billion (2007 est.)
GDP (official exchange rate):
$175.3 billion (2007 est.)
GDP- per capita (PPP):
6.6% (2007 est.) (CIA World Factbook)
Drug research
Addiction research started in the early years after the collapse of the communist system. Already in the late nineties there were quite some research publications on drug issues. Research is done by a number of experts at different research centres/universities. The Czech National Monitoring Centre for Drugs and Drug Addictions is responsible for monitoring drug issues and hosting the National Focal Point of the REITOX network of the EMCDDA. It coordinates collaboration and the exchange of information between research institutions, service providers, and public administration bodies. National scientific journals are also an important dissemination channel for drug-related research findings (Country overview).
Main drug-related problems
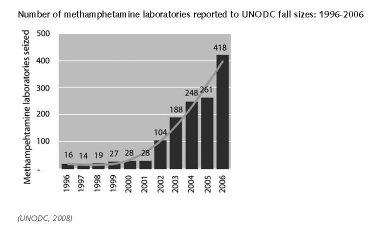
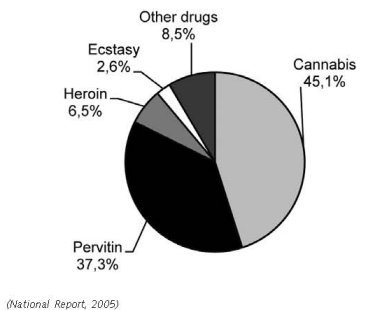
The main drug problem in Czech Republic is consumption (high prevalence rates of cannabis and ATS use). Czech Republic is also a major methamphetamine producer (pervitin). Part of this production is exported to Germany.
2 Drug problems
2.1 Drug supply
2.1.1 Production
Pervitin is produced in the Czech Republic exclusively, and is partly exported abroad, mainly to Germany.
There has been an increase in the hydroponic growing of marijuana with a high THC content (up to 20%). National Drug Squad data indicate that, to a growing extent, this activity also appears to be pursued by offenders of Vietnamese descent. Thirty-four hydroponic growing rooms were detected in the country in 2007, 4 of which were run by individuals of Vietnamese origin. The number of detected hydroponic marijuana growing rooms increased dramatically in the first 5 months of 2008; 61 growing rooms were detected and thousands of cannabis plants, dozens of kilograms of the final dry product, and extensive amounts of technical equipment were seized. 53 of the 61 growing rooms detected were run by Vietnamese operators.
The marijuana produced in these growing rooms was partially intended for illegal distribution on the Czech market, with the rest intended for export, mainly to Germany and the Netherlands (Annual Report, 2008).
2.1.2 Trafficking
1. Quantities (kg) of heroin seized, 1995 to 2005, EMCDDA Table SZR-8-SEIZURE-HEROIN-QUANTITY.htm
2. Number of heroin seizures, 1995 to 2005, EMCDDA Table SZR-7-SEIZURE-HEROIN-NUMBER.htm
3. Quantities (kg) of cocaine seized, 1995 to 2005, EMCDDA Table SZR-10-SEIZURE-COCAINE-QUANTITY.htm
4. Number of cocaine seizures, 1995 to 2005, EMCDDA Table SZR-9-SEIZURE-COCAINE-NUMBER.htm
5. Quantities (kg) of cannabis resin seized, 1995 to 2005, EMCDDA Table SZR-2-CANNABIS-QUANTITY.htm
6. Number of Cannabis resin seizures, 1995 to 2005, EMCDDA Table SZR-1-SEIZURE-CANNABIS-NUMBER.htm
7. Quantities (kg) of herbal cannabis seized, 1995 to 2005, EMCDDA Table SZR-4-SEIZURE-HERBAL-CANNABIS-QUANTITY.htm
8. Number of herbal cannabis seizures, 1995 to 2005, EMCDDA Table SZR-3-SEIZURE-HERBAL-CANNABIS-NUMBER.htm
9. Quantities (number of plants) of cannabis plants seized, 1995 to 2005, EMCDDA Table SZR-6-SEIZURE-CANNABIS-PLANTS-QUANTITY.htm
10. Number of seizures of cannabis plants, 1995 to 2005, EMCDDA Table SZR-5-SEIZURE-CANNABIS-PLANTS-NUMBER.htm
11. Quantities (kg) of amphetamine seized, 1995 to 2005, EMCDDA Table SZR-12-SEIZURE-AMPHETAMINES-QUANTITY.htm
12. Number of amphetamine seizures, 1995 to 2005, EMCDDA Table SZR-11-SEIZURE-AMPHETAMINE-NUMBER.htm
13. Quantities (kg) of Methamphetamine seized, 2001 to 2005 - EMCDDA Table SZR-18-SEIZURE-METHAMPH-QUANTITY.htm
14. Number of Methamphetamine seizures, 2001 to 2005 - EMCDDA Table SZR-17-SEIZURE-METHAMPH-NUMBER.htm
15. Quantities (tablets) of ecstasy seized, 1995 to 2005, EMCDDA Table SZR-14-SEIZURE-XTC-QUANTITY.htm
16. Number of ecstasy seizures, 1995 to 2005, EMCDDA Table SZR-13-SEIZURE-XTC-NUMBER.htm
17. National Report, 1999.
18. Csémy et al., 2002.
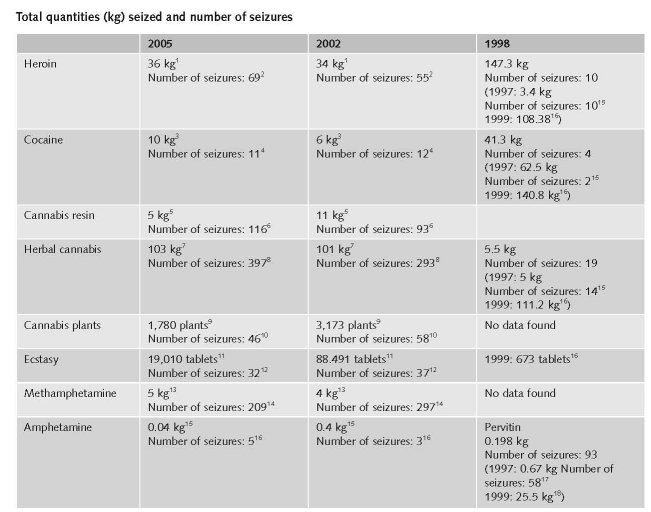
Although there are available data about the total quantity of drugs seized in the Czech Republic and Slovak Republic (table 1), we must note that the information value of the data is limited by the fact that it is difficult to determine whether some third country was the destination country or not and of course also by the fact that the police and customs only manage to seize a part of the transported drugs (Csémy et al., 2002).
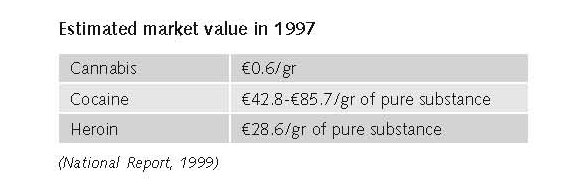
Estimated market value
in 2007
Cannabis1
Cannabis resin: Mean price €8.4/gr (min. €5.2/gr – max. €17.2/gr)
Herbal cannabis: Mean price €5.7/gr (min. €0.7 /gr – max. €12.1/gr)
Heroin2
Brown heroin: Mean price €37.5/gr (min. €17.2/gr – max. €69/gr)
Purity of heroin3
Mean price €41.5 (min. €4.7 – max. €89)
Cocaine products4
Mean price €78/gr (min. €51.7/gr – max. €103.4/gr)
Purity of cocaine products5
Mean price €56 (min. €12 – max. €100)
Synthetic drugs6
Amphetamine: Mean price €32.5/gr (min. €20.7/gr – max. €34.5/gr)
Purity of Synthetic drugs7
Mean price €54 (min. €3.3 – max. €75)
1. Price of cannabis at retail level, 2005, EMCDDA Table PPP-1 Part (i)-PRICE-CANNABIS.htm
2. Price of heroin at retail level, 2005, EMCDDA Table PPP-2 Part (i)-PRICE-HEROIN.htm
3. Purity of heroin at retail level, 2005, EMCDDA Table PPP-6 Part (i)-PURITY-HEROIN.htm
4. Price of cocaine products at retail level, 2005, EMCDDA Table PPP-3 Part (i)-PRICE-COCAINE.htm
5. Purity of cocaine products at retail level, 2005, EMCDDA Table PPP-7 Part (i)-PURITY-COCAINE.htm
6. Price of synthetic drugs at retail level, 2005, EMCDDA Table PPP-4 Part (i)-PRICE-SYNTHETIC.htm
7. Purity of synthetic drugs at retail level, 2005, EMCDDA Table PPP-8 Part (i)-PURITY-SYNTHETIC.htm
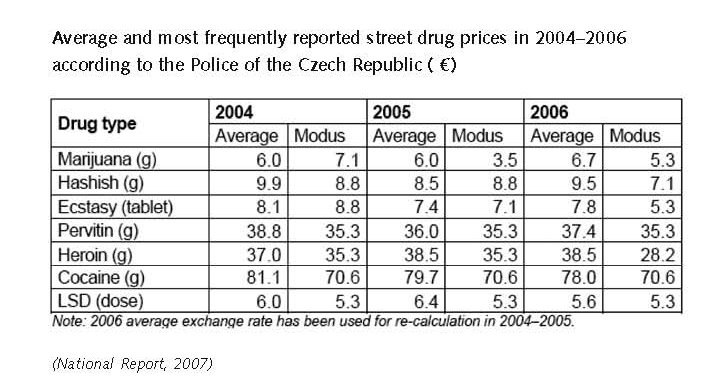
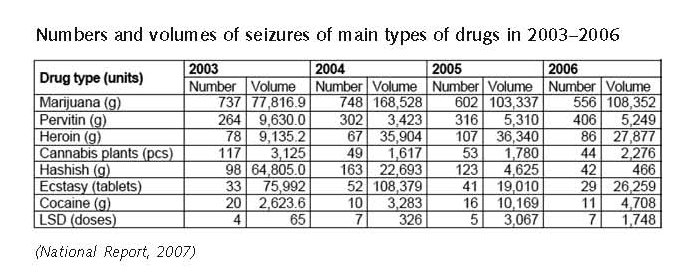
Heroin reaches the European market, including the Czech Republic, mainly through the Balkan route. The Balkan route is used for the transit of heroin from Afghanistan and neighbouring countries to Europe via some of the central and east European countries. Cannabis continues to be the most frequently trafficked drugs. In 2006, cannabis represented 51% of all drug seizures.
In 2004, Czech authorities observed an increase in pervitin (methamphetamine) exported to neighbouring countries such as Germany and Austria, and also detected clandestine pervitin laboratories. In 2005 and 2006, the quantity of pervitin was 5 Kg. Furthermore, in 2006 the police recorded a particular increase in the production of pervitin in the Central Bohemian, Olomouc, and Moravian-Silesian regions. There are no domestic sources of production of dance drugs in the Czech Republic. Most of the ecstasy tablets on the Czech market come from the Netherlands, Belgium and Poland (Country overview).
2.2 Drug Demand
2.2.1 Experimental/recreational drug users in the general population
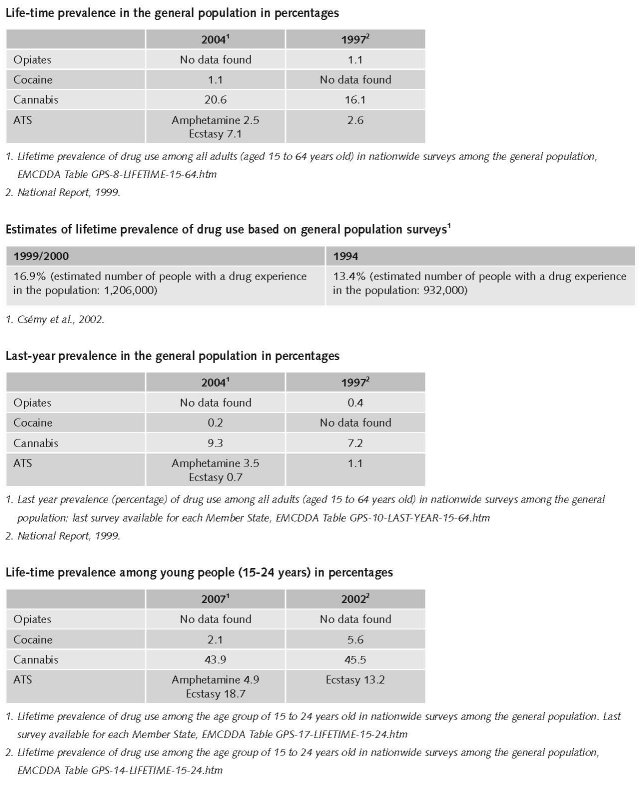
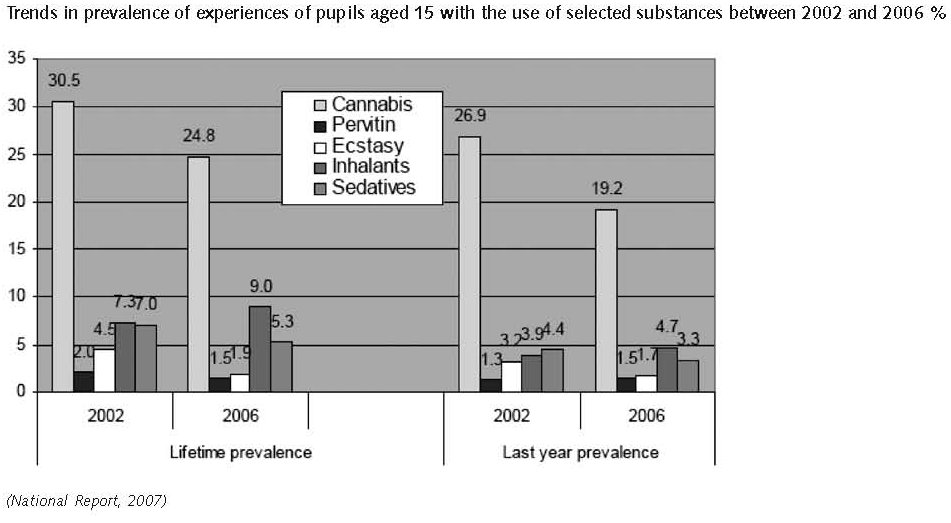
According to surveys from 2002 and 2004, approximately 20% of the adult population have tried an illicit drug, and the results suggest that the increasing trends from the previous decade have stopped or been reversed, even as far as cannabis is concerned, and this is also true among the group of young adults aged under 35. These favourable trends are also confirmed by the results of the 2006 HBSC survey among 15-year-old pupils of the ninth grades of elementary schools, which show a decline in prevalences of all types of illicit drugs (with the exception of inhalants), i.e. also with cannabis and ecstasy. According to data from available studies, approximately 2.6% of the adult population of the Czech Republic consume cannabis regularly (i.e. approximately 190,000 persons use cannabis at least once a week (National Report, 2007).
One of the most recent general population surveys on drug use was the 2004 General Population Survey on Health Status and Lifestyle of the Population of the Czech Republic, implemented among people aged 18–64 by the Institute for Health Information and Statistics (IHIS). Overall, the latest general population surveys suggest that the increases in lifetime experience of drug uses, observed during the previous decade, have now stopped. Lifetime prevalence for cannabis use was 20.6%, followed by ecstasy (7.1%), and magic mushrooms and other natural hallucinogens (3.5%) (Country overview).
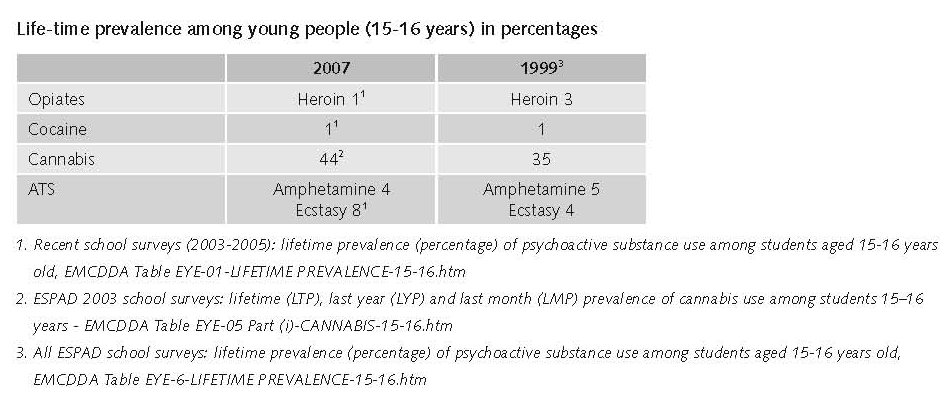
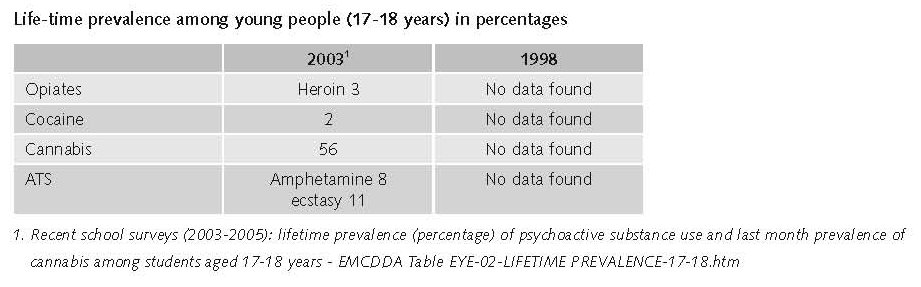
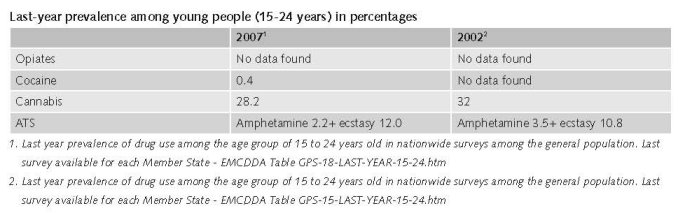
According to the results of ESPAD surveys on drug use among young people, the data available from 1995, 1999 and the most recent survey in 2003 show that the prevalence of use of illegal drugs increased in the second half of the 1990s. However it appears that the situation for different drugs began to diverge: while there was a further increase in the prevalence of cannabis and ecstasy use from 1999 to 2003, the prevalence of stimulant and opiate use declined (Country overview).
Lifetime experience with an illicit drug other than marijuana/hashish among 15–16 year olds increased from 4.3% in 1995 to 9.0% in 1999 and 11.2% in 2003 (ESPAD survey). In particular, marijuana (herbal cannabis) or hashish (cannabis resin) use is very prevalent among this age group. In 2003, 44% of 16-year olds reported that they had tried these substances at least once (compared to 35% in 1999 and 18% in 1995). Lifetime use of ecstasy for the same age range increased from 4% in 1999 to 8% in 2003. A decline was noted for lifetime amphetamine use, which decreased from 5% in 1999, to 4% in 2003 (Country overview).
The last HBSC study among 15-year-old students, conducted in 2006, reported 25% for lifetime prevalence of cannabis, indicating a declining trend compared to 2002 (31%). Lifetime prevalence of inhalants (9%) was the second most commonly reported. Last month prevalence of cannabis was reported to be 10%. Compared to 2002 results, the only increase in lifetime and last year prevalence involved inhalants; for all other substances a decline in the lifetime prevalence was noticed (Country overview).
2.2.2 Problematic drug users/chronic and frequent drug users
The EMCDDA defines problem drug use as the use of drugs by injection and/or the regular or long-term use of opiates and amphetamine-type drugs and/or cocaine. The Czech definition of problem drug use is the use of drugs by injection and/or the regular or long-term use of opiates and methamphetamine. Cocaine is not considered as a part of the definition, due to its very low prevalence in the Czech Republic. Ecstasy and cannabis are not included either (Country overview).
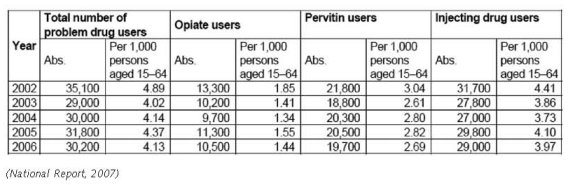
For the Czech Republic, the national estimate suggests (for 2006) that there are 30,200 problem drug users. Of these
19 700 are methamphetamine (pervitin) users; 6 200 heroin users and 4,300 Subutex users. The number of IDU (injecting drug users) was estimated at 27,000 (multiplier method) in 2004 and 29,000 in 2006 (Country overview).
A shift among opiate users to substitution treatment has been taking place in the Czech Republic in recent years, and this has shown a decreasing trend in estimates of problem opiate users, based on drug treatment data. On the other hand, the number of problem pervitin users increased slightly (8%) between 2003 and 2004, and this is in accordance with the trends among drug users undergoing treatment. The pattern of cocaine use still remains sporadic in the Czech Republic (Country overview).
Cocaine use in the Czech Republic is at a very low level; amphetamine-type drugs almost exclusively involve pervitin only, while opiate-type drugs mainly involve heroin and Subutex® (National Report, 2007).
Mean values of prevalence estimates of problem drug use carried out using a multiplication method with the use of data from low-threshold programmes in 2002–2006
Expert comments
The existing estimates on the number of problem drug users in the Czech Republic were carried out between 1999 and 2006 using the multiplier benchmark calculation, based on data from low-threshold centres. In 2006, the estimate was constructed as a sum of the estimate for Prague and the rest of the Czech Republic. For Prague, results of a study entitled ‘Sexual behaviour of drugs users’ were used to update the multiplier, where the value reached 71% (Country overview).
2.3 Drug related Harm
2.3.1 HIV infections and mortality (drug related deaths)
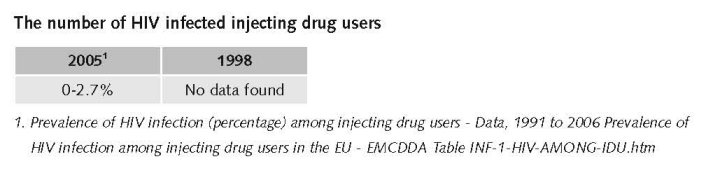
The 2007 NR states: The situation in the transmission of infectious diseases among drug users has remained stable. HIV seroprevalence among injecting drug users is far below 1%, and is so even in groups of at-risk users with a longer history of injecting use or groups with a high prevalence of viral hepatitis. The number of users newly infected with HIV in 2006 was the same as in 2005 (National Report, 2007).
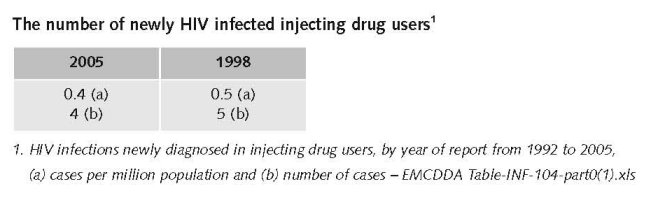
The reported incidence of new cases of HIV infection among injecting drug users and among the general population is relatively low in the Czech Republic; however, it seems to have been increasing during the last three years. 93 new cases of HIV were diagnosed in 2006 (i.e. 3.3% more than in 2005); 6 of these may have become infected as a result of injecting drug use. However, since 2000 the incidence for the same group is every year in the range between 2 and 7 (National Report, 2007).
The rate of infections (HIV-AIDS, HBV and HCV) among drug users has remained stable in recent years. Data are available from national registers and studies involving different drug user groups in the Czech Republic (Country overview).
HIV seroprevalence rates among IDUs remained consistently below 1% in the Czech Republic between 1996 and 2006. The number of newly-diagnosed HIV cases among the general population is relatively low, although it seems to have been increasing over the last three years. 93 new cases were diagnosed in 2006 (3.3% more than in 2005) (Country overview).
2.3.2 Drug related crime or (societal) harm
In an article published in 2002 with mainly data on the period late nineties till 2000 the following is stated: The illicit character of drugs is related to the second large issue, criminality. Only the lowest level of drug related criminality concerns drug users, because addicts often participate in street drug sales or they procure the means for drugs for themselves by criminal activities, most frequently by pilfering. Persons and organized groups that participate in production, transit and distribution of drugs only seldom use drugs. In the course of the nineties, drug-related criminality has increased in both the Czech Republic and Slovak Republic (table 3), and it represents approximately 2% of the total criminality (Csémy et al., 2002).
On the contrary, problem users come into conflict with the law more frequently because of property crimes by which they get the means for drugs than due to the direct commission of drug-related criminal offences. Actual estimates for 2002 are not available; the methodology of gathering data about the secondary criminal activity of drug users represents one of the tasks of the Criminal Law Sector Data working group of the Czech National Focal Point (National Report, 2005).
3 Drug policy
3.1 General information
3.1.1 Policy expenditures
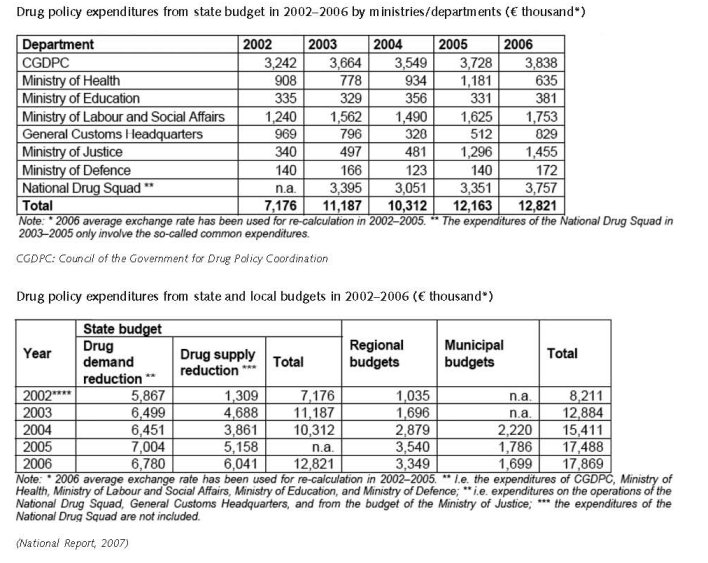
Compared to 2005, the drug policy expenditures from the state budget increased by approximately CZK 19 million in 2006 (€ 670 thousand); however, the expenditures from the budget of the Ministry of Health declined by 45% to CZK 18 million (€ 630 thousand). The year-on-year volume of financial resources expended by regions decreased by approximately CZK 5.5 million (€ 194 thousand) (National Report, 2007).
In comparison with 2005, drug policy expenditures increased by approximately CZK 19 million (€ 670 thousand); on the other hand, the volume of financial resources provided by regions has decreased by approximately CZK 5.5 million (€ 194 thousand) (National Report, 2007).
The developments in drug policy expenditures from the state budget by individual ministries are given in Table 1-4; it is obvious that the amount of resources from the budget of the Ministry of Health declined markedly, while the resources from the budget of the General Customs Headquarters increased markedly (National Report, 2007).
3.1.2 Other general indicators
The Czech national drug policy strategy covers the period 2005–09. It was first complemented by a 2005–06 action plan and was again complemented in July 2007 by a new action plan covering the period 2007–09. The strategy is comprehensive and is based on four pillars: prevention, treatment and resocialisation, risk reduction and supply reduction. The focus is mainly on illegal drugs but with some scope to address other drugs (alcohol, prescription drug misuse), if necessary. The strategy has two main goals: (1) to combat organised crime associated with the unauthorised handling of drugs and to enforce the observance of laws in connection with the distribution of licit drugs; and (2) to reduce the use of all types of drugs and potential risks and damage that may affect individuals and society as a consequence of drug use. The new 2007–09 action plan covers seven policy fields (primary prevention, treatment and aftercare, harm reduction, drug supply reduction and law enforcement, information/research/evaluation, coordination and funding, international collaboration) and contains 172 different objectives (Country overview).
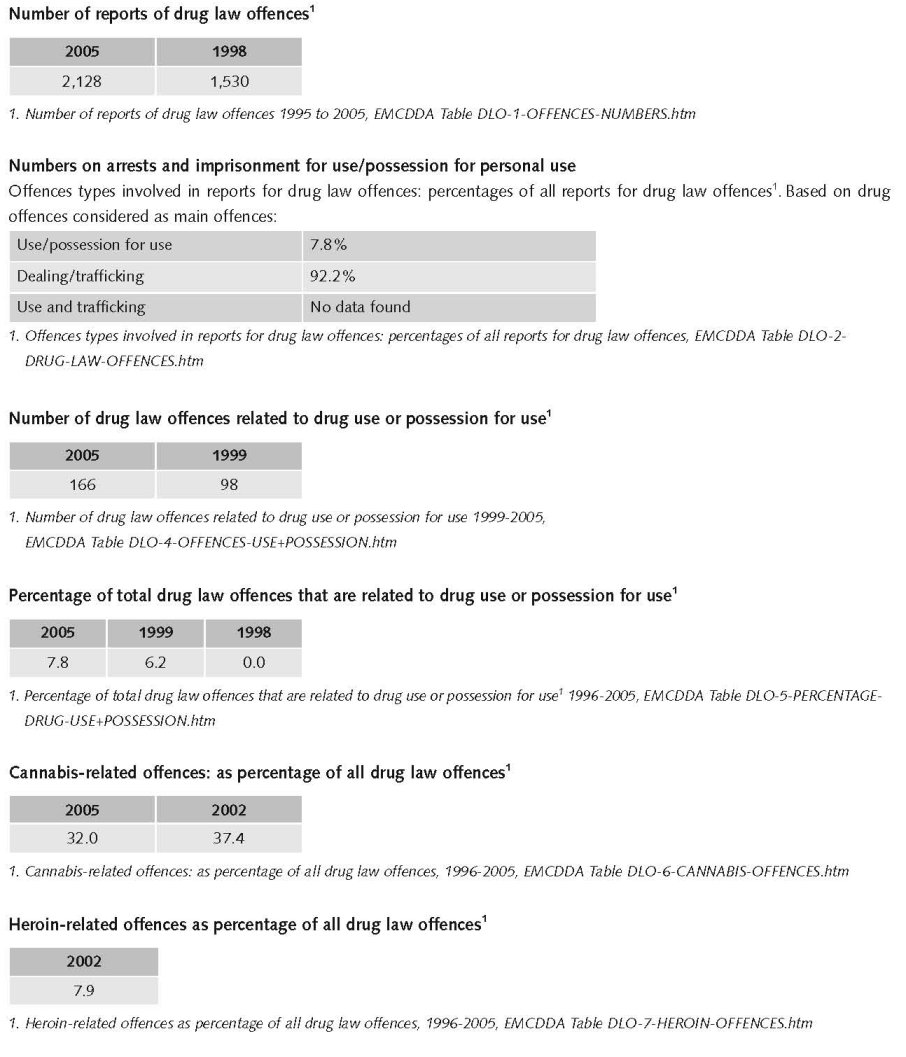
Since January 1, 1999, the Czech Penal Code included the provision to sanction the possession of narcotic and psychotropic substances for personal use “in a greater than small quantity”. The unclear definition of the term “greater than small quantity” resulted in difficulties in applying this provision. This problem was partly solved through instructions of the Police President and the Supreme Prosecutor. The number of criminal offences prosecuted according to this provision increased, as does the number of persons prosecuted; however, the proportion of those prosecuted among the total number of users is very low. The relatively low number of people prosecuted for an offence under this provision in comparison with the number of drug users suggests that the law has been applied selectively in practice. In 2002, this provision mostly affected the users of cannabis and amphetamines. Cannabis drugs users are also often prosecuted according to the provision of Section 187 or Section 188 of the Penal Code. In these cases, this often involves persons who grow cannabis for personal use (National Report, 2002).
In August 2006 (with effect from October 1, 2006), a general instruction No. 2/2006 on the penalties for the criminal offence of the unauthorised production of narcotic and psychotropic substances and poisons according to Section 187a of the Penal Code was issued by the Office of the Supreme Prosecutor. This instruction replaced the instruction of the Office of the Supreme Prosecutor from 2002, which had been in effect until then (No. 6/2002). Inter alia, this internal regulation (which is not a generally binding legal norm) provides guidelines for the attributes “quantity greater than small” and “in a larger extent”, which narrow down the punishability of possession of drugs for personal use in the new Penal Code (National Report, 2007).
The proposal of 2004 to distinct two categories of illicit drugs according to the level of social and health risks, i.e. between cannabis and other illicit drugs (National Report, 2004) was rejected in 2006 (National Report, 2006).
The Lower House of the Parliament of the Czech Republic definitively rejected the draft bill of the new Penal Code, which also contained changes regarding “drug-related” criminal offences, on February 21, 2006 (National Report, 2006).
Persons prosecuted for unauthorised possession of drugs for personal use by type of drug; n = 153
The judiciary is making increasing use of alternative sentences for drug offenders, especially in connection with marijuana (National Report, 2004).
It is positive that the judiciary is making increasing use of alternative sentences even for drug users; this involves both the prosecution of drug-related criminal offences and cases of secondary drug-related criminal offences (National Report, 2002)
Proportion of offenders prosecuted for possession of drugs for personal use (Section 187a TZ) among all offenders prosecuted for drug offences in 1999- 2006
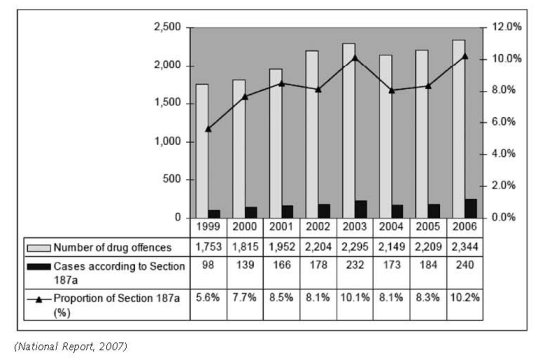
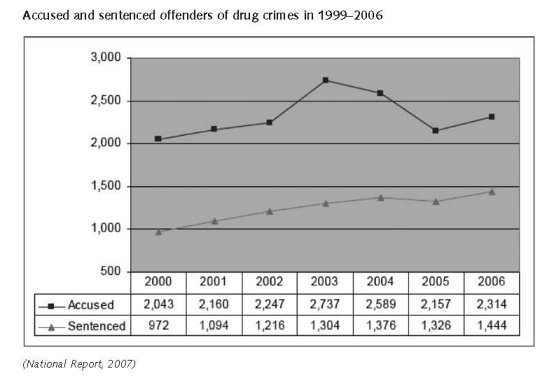
The number of drug offences has remained relatively stable in the Czech Republic in recent years. A slight increase in the number of prosecuted and sentenced drug offenders took place in 2006. The proportion of those prosecuted for offences involving possession of drugs in a quantity greater than small (Section 187a of the Criminal Code) among all detected drug offences has been around 8 to 10 per cent since 2001. The number of misdemeanours of the possession of drugs for personal use was approximately four times higher than the number of offences of the possession of drugs for personal use. Most (60%) drug offences were associated with pervitin, 30% with cannabis; in recent years, the proportion of pervitin has been increasing and the proportion of cannabis and other drugs has been declining. The number of offences in relation to cocaine and ecstasy has been low. In comparison with pervitin related offences, a markedly higher proportion of juveniles among those accused of and sentenced for cannabis related offences and a markedly lower proportion of custodial sentences were observed in cannabis-related offences. The highest number of those prosecuted for drug offences per the number of inhabitants was recorded in the Karlovy Vary, Ústí nad Labem, and Liberec regions; in absolute numbers in the Ústí nad Labem and Prague regions. According to a police estimate, drug users committed approximately 14,000 (11%) of all cleared-up offences and 74,000 (22%) of all detected criminal offences, of which approximately 9,000 offences involved cleared-up thefts and 66,000 detected thefts (National Report, 2007).
3.2 Supply reduction: Production, trafficking and retail
Main focus is on supply reduction is on retail and on trafficking.
Priorities of supply reduction covered by policy papers and/or law
Until 1990, articles dealing with drug-related criminality were included in law No. 140/1961, and they were amended in 1990 (law No. 175/1990 of the Code). Without any substantial changes, this arrangement remained operative in the Czech Republic in the whole period of the 1990s. Starting from 1999, the criminal sanctions for drug-related criminal offences became stricter and the sanctions for possession of illicit drugs for personal use that contained the famous and rather comical formulation ‘quantity greater than small’ were introduced (Csémy et al., 2002).
Since 1999, the Criminal Code and the Act on Misdemeanours state that possession of narcotic drugs and psychotropic substances in greater than small quantities is a criminal offence, and can attract sentences of up to 2 years’ imprisonment
(or 1–5 years in case of aggravating circumstances in the offence). In case of possession of small quantities without intention to supply, administrative sanctions (a fine or warning) are imposed (Country overview).
Penalties for drug trafficking can be up to 10–15 years of imprisonment, depending on aggravating circumstances. In the case of addicts committing a drug-related crime, a range of alternatives to imprisonment is available to the court (e.g. suspended sentences, community service and probation with treatment). In 2006, the draft bill of the Penal Code, which included major changes such as a differentiation of sanctions for possession of different drugs, was definitely rejected by the Lower House of the Parliament of the Czech Republic for unrelated reasons (Country overview).
3.3 Demand reduction: Experimental/recreational drug use + problematic use/chronic-frequent use
Prevention programmes implemented
School-based prevention and telephone helplines are available all over the country. Mass media campaigns are implemented once in a while (National Report, 2007).
Prevention activities in the Czech Republic are coordinated by the Ministry of Education and they are mainly implemented by schools and NGOs that provide services in the field of treatment and help to drug users. Among all primary prevention programmes, school-based prevention programmes represent the biggest share. These programmes are carried out within the framework of the ‘Minimum Preventive Programme’ at schools and educational facilities. Every school is obliged to prepare and implement this programme, based on the principle of education towards a healthy lifestyle and preventing risk behaviours (Country overview).
Selective prevention programmes in the Czech Republic focus mostly on specific groups of children, and target in particular children living in families from socially- or culturally-disadvantaged environments, those growing up outside their biological family, living in the families of alcoholics or drug users, children with non-specific behaviour disorders, and children with specific developmental disorders (Country overview).
Indicated prevention programmes focus specifically on at-risk groups such as those using drugs more regularly and frequently, and most planned early intervention programmes are now implemented. Both specialised governmental and non-governmental organisations work on indicated prevention programmes for this specific target group (Country overview).
There is a wide variety of treatment including detoxification (also in prisons), short-term, medium-term and long-term in-patient treatment, therapeutic communities, aftercare, substitution treatment, out-patient (health care) services, etc. (Csémy, 2002). Number of patients in treatment for illicit drug use stayed more or less on the same level since 1998, however number of opiate users is falling, whereas number of cannabis users and sedative/hypnotics is rising.
Number of first treatment demands by drug used in 1995–2006
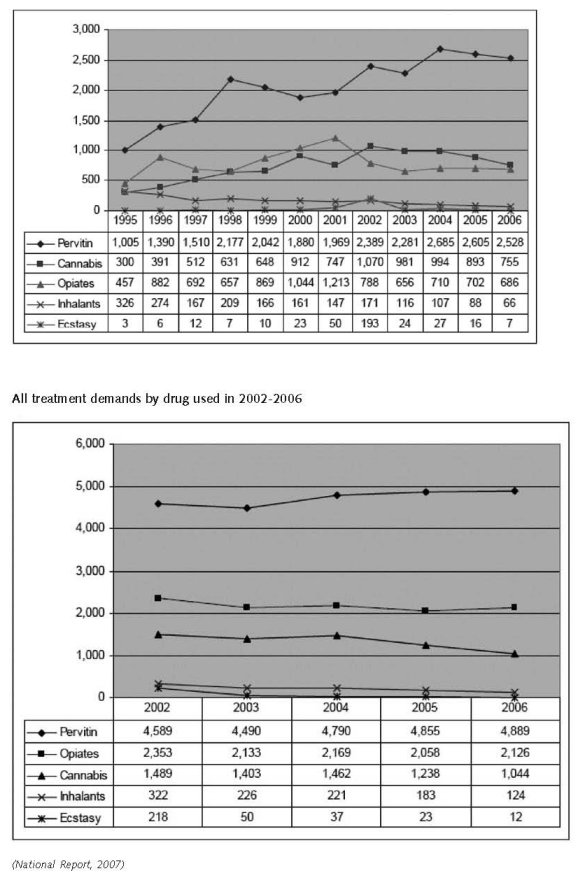
In 2006, a total of 8 164 drug users entered in treatment whereas, 4 119 persons sought treatment for the first time. Users of amphetamines (almost exclusively pervitin, i.e. methamphetamine) were the most commonly represented among all treatment clients entering treatment, at 58.6%, as well as among first treatment clients with 61.4%. This was followed by opiates users with 25.4% among all treatment clients and 18.3% of cannabis users among first time treatment clients (Country overview).
In 2006, 53% of all clients entering treatment were aged less than 25 years. A similar age distribution was also reported among new treatment clients, with 66% being under the age of 25 years. In 2006, the male to female ratio for all treatment clients was 68% for male and 32% for female clients. A similar trend was also reported among new treatment clients, with 66% being male and 34% female (Country overview).
The number of patients receiving out-patient treatment increased in 2006 in health care facilities (the increase has been apparent since 2000), as well as out-patient clinics operated by NGOs (a marked year-on-year increase). The number of patients hospitalised in in-patient psychiatric facilities has increased slightly in the last five years, especially in relation to the use of stimulants and combinations of drugs, while a marked decline has been taking place since 2001 in terms of opioids.
The number of patients in substitution treatment has been increasing, both in specialised centres and probably also in the clinics of other physicians prescribing Subutex®. However, the extent of treatment with Subutex® is not recorded in full in the substitution treatment register (National Report, 2007).
Methadone maintenance was introduced in 1998 and high-dosage buprenorphine treatment in 2000 (Year of introduction of methadone maintenance treatment (MMT), high-dosage buprenorphine treatment (HDBT) and heroin-assisted treatment, including trials - EMCDDA Table HSR-8-METHADONE-INTRODUCTION.htm).
Priorities of demand reduction covered by policy papers and/or law
The National Drug Policy Strategy 2001–2004 defines the current orientation of the Czech drug policy. Similar goals were set up in the National Fight against Drugs Programme 1999–2003 in Slovakia. In both strategies there is an emphasis on the balance between drug supply reduction and drug demand reduction, and harm reduction is also highlighted beside primary prevention and treatment. The expressed emphasis on harm reduction makes the main difference between the current Czech and Slovak policies and strategies (Csémy et al., 2002).
As in the previous years, two substitution preparations were available in 2006 – methadone and Subutex®. It is planned that Suboxone will be introduced in 2008 (National Report, 2007).
The methodology for substitution treatment is defined in the Standard of Substitution Treatment (Ministerstvo zdravotnictví
ˇCR, 2001). As the current version of the standard does not correspond to the current condition of substitution treatment provision, especially the development of prescription in non-specialised facilities, the Ministry of Health announced an updated version by the end of 2007 (National Report, 2007).
The Act 108/2006 Coll. on social services, which had been in preparation since the beginning of the 1990s, was adopted in 2006. The previous legislation in the field of social services was completely inadequate – as far as social services are concerned, it only used to involve institutional care and community care service; no legal regulations were available for other types of services (National Report, 2007).
According to the above-mentioned act, social services aim to assist people in an unfavourable living situation, including the prevention of their social exclusion. Social services are provided in the form of residential, out-patient, or low-threshold services. The act defines 31 types of social services, divided into: (1) social care services; (2) social prevention services, and (3) social counselling, which is the basic activity during the provision of all types of social services. The act mentions drug users as the target group of several types of social prevention: low-threshold centres, outreach programmes, therapeutic communities, and aftercare services (National Report, 2007).
3.4 Harm reduction
3.4.1 HIV and mortality
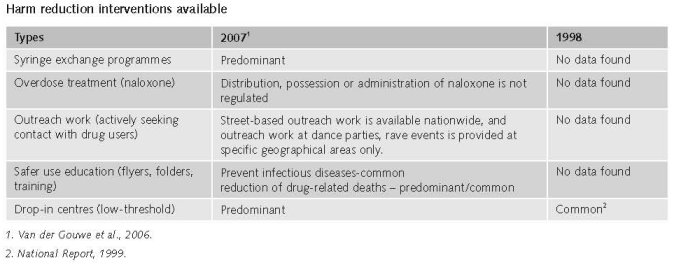
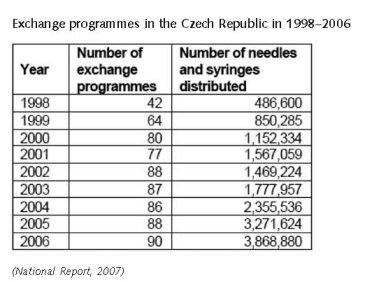
The Czech network of low-threshold facilities established since 1992 includes low-threshold centres, outreach programmes, street work and needle exchange programmes (altogether, 90 programmes). Programmes operate in all regions of the Czech Republic. The Czech NFP estimates that approximately 60% of injecting drug users in the Czech Republic use needle exchange programmes. It has also been observed that the number of problem drug users has not increased. However the number of syringes used has been increasing over recent years (an increase of 64% between 2004 and 2006). In 2006, nearly 4 million syringes were distributed through NSPs in the Czech Republic. The main sources of clean injecting material include exchange programmes (drop-ins and outreach work), but also pharmacies. A harm-reduction section of the Association of Non-Governmental Organizations was set up in 1999, which facilitates the communication flow between services and promotes standards of care (Country overview).
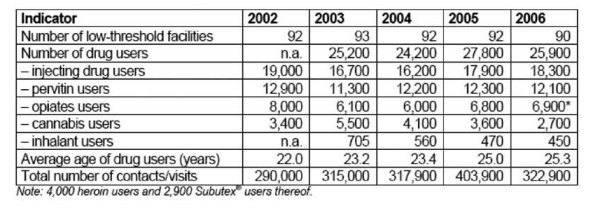
The measures targeted at the reduction of drug-related health risks are carried out by low-threshold facilities for drug users. The availability, capacity, and use of the facilities have been increasing continually since the second half of the 1990s. The proportion of problem users who are in contact with the facilities is relatively high (60–70%) (see more information in the chapter on Problem Drug Use, page 24). The number of injecting needles and syringes distributed in exchange programmes increased again in 2006. On the other hand, a decrease in the availability of testing for infectious diseases can be mentioned as a weakness – the number of HIV and HVC tests of clients of low-threshold facilities declined rapidly in 2006 to approximately half of the number in 2003–2005 (National Report, 2007).
Clients of Czech low-threshold facilities in 2002–2006, extrapolated to the total number of programmes
Priorities of harm reduction covered by policy papers and/or law
The Act on Measures for Protection from Harm Caused by Tobacco Products, Alcohol, and Other Addictive Substances (No. 379/2005 Coll.) - came into force on January 1, 2006 - defines legal measures which especially involve the prevention and harm reduction of substance use, as well as health care and the system of social services. One main goal is to reduce the harm caused by the use of addictive substances; unlike the previous one, this act briefly defines the types of professional care supplied to those who harmfully use tobacco products and alcohol and other addictive substances and those addicted to these substances (National Report, 2006).
The Act 108/2006 Coll. on social services – adopted in 2006 – defines the scope and objectives of social services, i.e. to assist people in an unfavourable living situation, including the prevention of their social exclusion. Social services are provided in the form of residential, out-patient, or low-threshold services. The act defines 31 types of social services, divided into: (1) social care services; (2) social prevention services, and (3) social counselling, which is the basic activity during the provision of all types of social services. The act mentions drug users as the target group of several types of social prevention: low-threshold centres, outreach programmes, therapeutic communities, and aftercare services (National Report, 2007).
3.4.2 Crime, societal harm, environmental damage
No information found on interventions/measures to reduce harm for society.
References
Consulted experts
V. Mravcik, Head of National Focal Point, Prague.
T. Zabranski, Research Fellow, Centre for Adictology, Charles University, Prague.
Documents
Annual Report 2008: The Czech Republic – 2007 Drug Situation. Available: txt.www.drogy-info.cz/index.php/english, last accessed 17 November 2008
CIA. The World Factbook: Czech Republic. Available: www.cia.gov/library/publications/the-world-factbook/geos/ez.html, last accessed 17 November 2008.
Country overview: Czech Republic. Available: www.emcdda.europa.eu/publications/country-overview/cz, last accessed
17 November 2008.
Csémy L, Kubiˇcka L, Nociar A. Drug Scene in the Czech Republic and Slovakia in the Period of Transformation. European Addiction Research 2002, 8: 159-165.
National Report to the EMCDDA. Czech Republic, 1999.
National Report to the EMCDDA. Czech Republic, 2002.
National Report to the EMCDDA. Czech Republic, 2004.
National Report to the EMCDDA. Czech Republic, 2005.
National Report to the EMCDDA. Czech Republic, 2006.
National Report to the EMCDDA. Czech Republic, 2007.
Van der Gouwe D, Gallà M, Van Gageldonk A, Croes E, Engelhardt J, Van Laar M, Buster M. Prevention and reduction of health-related harm associated with drug dependence: an inventory of policies, evidence and practices in the EU relevant to the implementation of the Council Recommendation of 18 June 2003. Utrecht, Trimbos Institute, 2006.
UNODC, World Drug Report 2008. Vienna, United Nations Office on Drugs and Crime, 2008.
| < Prev | Next > |
|---|