| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Appendix to report 4: country reports CHINA
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
CHINA
1 General information
Location:
Eastern Asia, bordering the East China sea, Korea Bay, Yellow Sea, and South China Sea, between North Korea and Vietnam
Area:
9,596,960 sq km
Land boundaries/coastline:
22.117 km/14.500 km
Border countries:
Afghanistan, Bhutan, Burma, India, Kazakhstan, North Korea, Kyrgyzstan, Laos, Mongolia, Nepal, Pakistan, Russia, Tajikistan, Vietnam
Population:
1,330,044,605
Age structure:
0-14 years: 20.1% (male 142,085,665/female 125,300,391)
15-64 years: 71.9% (male 491,513,378/female 465,020,030)
65 years and over: 8% (male 50,652,480/female 55,472,661) (2008 est.)
Administrative divisions:
23 provinces, 5 autonomous regions and 4 municipalities
note: China considers Taiwan its 23rd province; see separate entries for the special administrative regions of Hong Kong and Macau
GDP (purchasing power parity):
$7.099 trillion (2007 est.)
GDP (official exchange rate):
$3.251 trillion (2007 est.)
GDP- per capita (PPP):
$5,400 (2007 est.) (CIA The World Factbook)
Drug research
Dr Lin Lu, director of the National Institute of Drug Dependence (linked to Peking University) is one of the key researchers in the field of drug addiction. Others include Wu Zunyou (AIDS), Konglai Zhang (Director of China AIDS Network).
Main drug-related problems
China plays a substantial role in methamphetamine production. Drug consumption is on the rise though still relatively low compared to Western countries. Heroin (injection) is popular though there are indications for a decline. Cannabis use is reported to increase. Also ATS and ketamine are getting increasingly popular.
2 Drug problems
This China report deals with China mainland. Excluded from the analysis are Macao, Taiwan and Hong KONG SAR’s.
2.1 Drug supply
2.1.1 Production
China, Myanmar and the Philippines are the world’s largest producers of methamphetamine. Large seizures of amphetamine have occurred in many Asian countries, including China, Hong Kong, Indonesia, Myanmar, Taiwan and Thailand (Cook & Kanaef, 2008).
Countries reporting to UNODC cite the origin of seized drugs as a means of identifying source countries of ATS manufacture. During the 2002-2006 period, the three countries in East and South-East Asia most often mentioned as sources for methamphetamine were China (38%), Myanmar (21%), and the Philippines (21%). Additionally, several countries have noted that organized drug syndicates are becoming increasingly transnational and substantially more sophisticated in their methods of trafficking (UNODC, 2008a).
In recent years China dismantled a number of laboratories: in the year 2005-2006 this included 90 methamphetamine & other ATS labs and 2 MDMA labs, 12 heroin and 2 opium labs (UNODC, 2008).
2.1.2 Trafficking
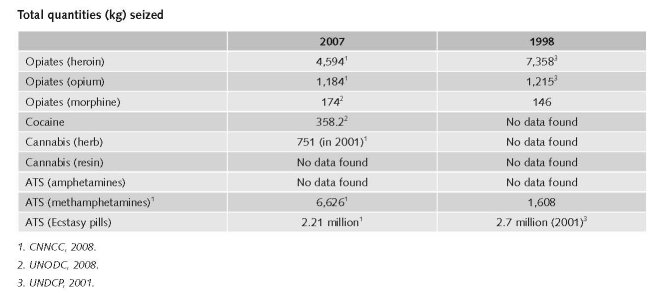
Heroin seizures increased in 2001 (13,200 kg) and remained stable for a number of years, but dropped in 2006 to 5,792 kg and 4,594 kg in 2007. Most heroin now comes from Afghanistan, but also from Thailand and Central Asia.
The Chinese authorities reported 18 seizures involving heroin trafficked into China via Pakistan, up from eight in 2005 and none in 2004. A rather high proportion of third country foreigners (mostly from West Africa) were involved (9% of the persons arrested in Pakistan and 33% of the persons arrested in China). The total volume of these seizures was still small (132 kg in 2006 out of 2.8 mt of heroin seized in Pakistan and 62 kg out of 5.8 mt seized in China) but the shipments indicate the development of emerging routes and changes in market supply chains (UNODC, 2008).
The World Drug Report 2008 reports a 6.1% decrease in trafficking in amphetamines in China. The Chinese authorities reported the detection and dismantling of 53 methamphetamine producing laboratories in 2006, a 43% increase over 2005 reports (UNODC, 2008).
According to the World Drug Report 2008, there has been an increase in China in 2006 in trafficking of cocaine with 0.4%. The largest cocaine seizures in Asia in 2006 were made in China (UNODC, 2008).
Legal cases and arrests related to seizures increased significantly over the last years (CNNCC, 2008).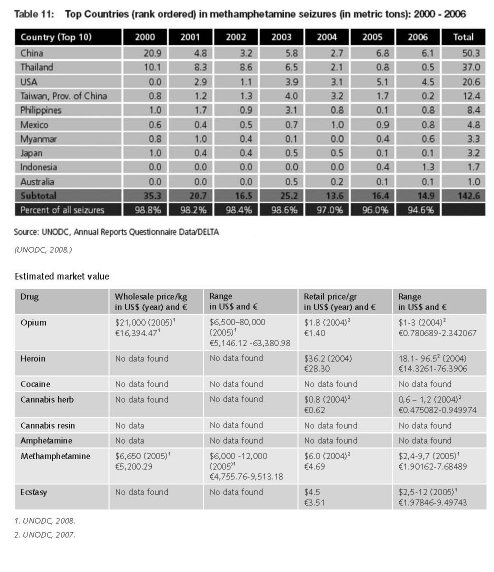
1 $1= €0.780689. Exchange rate 24 February 2009.
2.2 Drug Demand
Estimates on drug use prevalence in China vary greatly. It is also hard to make out whether certain figures refer to experimental/recreational or problematic drug users or simply to drug users in general. There is some good quality regional research but no hard national data. To date no national drug-related household survey has ever been undertaken in China.
2.2.1 Experimental/recreational drug users in the general population
The specifics of China’s drug problem have been thoroughly documented by Hao et al., who described the prevalence and patterns of illicit drug use in the heavily populated areas of Yunnan, Sichuan, Gansu, and Guangdong provinces between 1993 and 2000 (Lu et al. 2008). Hao and colleagues screened more than 50,000 individuals aged 15 or above in these communities and interviewed possible users. The data from these subjects showed that the lifetime prevalence of illicit drug use was 1.08, 1.60, and 1.52% in 1993, 1996, and 2000 respectively. Last year prevalence of use was 0.91, 1.11, and 1.17% in 1993, 1996, and 2000 respectively. Heroin was by far the most used drug: 51.8% of drug users had used the heroin in 1993, 83.4% in 1996, and 95.9% in 2000. The two most frequent routes of heroin administration were inhalation (89.2% in 1993, 60.1% in 1996, and 93.5% in 2000) and intravenous injection (27.2% in 1993, 31.0% in 1996, and 25.7% in 2000) (Lu et al., 2008).
Most countries of East and South-East Asia reported declines in opiate use in 2006, reflecting the strong declines of opium production in Myanmar and the Lao PDR in recent years. Countries reporting declines included China, Indonesia, the Philippines, Malaysia and Myanmar (UNODC, 2008).
According to the World Drug Report 2008, there was a large increase in the use of cannabis in China in 2006 (UNODC, 2008).
In terms of sheer volume, China has one of the world’s largest methamphetamine markets, although the methamphetamine prevalence rates are probably lower than in several of the other South-East Asian countries. Reports in 2006 identified large increases in the use of Methamphetamine pills and crystalline methamphetamine. China reports that, of registered drug users in 2004, 1.7% used ATS, while that number grew to 11.1% in 2007. These rates are consistent with increases in reported clandestine methamphetamine laboratories and rising seizures in recent years (UNODC, 2008).
The use of amphetamines in 2006/2007 is 0.3 – 0.5% of the population (annual prevalence) (UNODC, 2008).
The use of ecstasy in 2006 has largely increased (UNODC, 2008).
Heroin use is widespread in China, with an estimated 600,000 people using the drug (Cook & Kanaef, 2008).
As for consumption, heroin (injection) is popular and ATS and ketamine are getting increasingly popular. Cannabis and cocaine are not used widely (expert’s comments). Existing national and regional monitoring systems are often not capable of generating representative data. For example, neither India nor China – collectively accounting for 38% of the world population – has ever conducted a nationally representative survey on ATS consumption (UNODC, 2008).
Irregular or incomplete reporting from countries is compounded by the varying quality of data provided. Specifically, and similar to other drugs, information about the extent of ATS consumption (prevalence rate) is the weakest indicator, as household and other surveys are lacking or are outdated in some countries in several of the most affected regions (according to supply side indicators and/or expert opinion). Unfortunately, this happens to be the case in several populous countries (i.e. China and India), thus affecting regional and global prevalence estimates (UNODC, 2008).
2.2.2 Problematic drug users/chronic and frequent drug users
Illicit drug use, particularly heroin use, has quickly spread and has reached epidemic levels in the last 10 years. The number of registered drug users increased from 70,000 in 1990 to 1.16 million at the end of 2005; whereas in 2004 the estimated number of actual users was 3.5 million (CNNCC, 2008; Lu et al., 2008).
However, according to UNODC in China, the number of current drug users went down from 1,160,000 to 950,000, reason why UNODC believes that the situation regarding heroin is under control. UNODC China does not use ‘registered drug users’ as indicator as this number is biased by among others double counting (expert comment). According to the World Drug Report, there was also a strong decline in use of heroin and other opiates in China in 2006 (UNODC, 2008).
China is experiencing a rapid expansion in ATS use, particularly in urban areas, and ecstasy and methamphetamine appear to be the most popular drugs consumed (Cook & Kanaef, 2008).
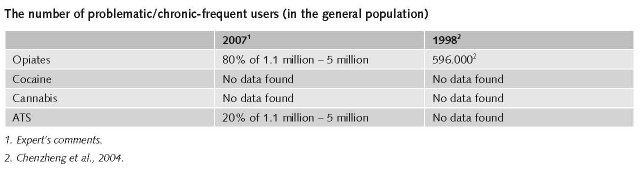
In 1999 there were 681,000 registered drug users. 71.5% (487,000) were using heroin (Narcotics Control in China, 2000).
In 2005 1.16 million drug users were registered. The use of ‘new’ drugs like MDMA and methamphetamine gained popularity in large and medium-sized Chinese cities (Lu et al., 2008).
In 2008 1.1 million drug users are registered at the Public Security Bureau PSB. The estimates of the real number of drug users is much higher, i.e. around 5 million. Around 80% of them use heroin/opiates. ATS use is rapidly increasing. There are probably 1 million ATS users in China. Cannabis and cocaine are not popular (expert’s comments).
Estimates of the number of people who inject drugs in China for 2008 range between 356,000 and 3.5 million, and numbers as high as ten million have been reported in Chinese media. Heroin, methamphetamine, diazepam, pethidine and morphine are the most commonly injected drugs. The level of involvement in sex work among female drug users is reported to be increasing, and in Guangxi it is estimated that 80% of female sex workers inject drugs. Heroin is also the most commonly injected drug in Hong Kong (Cook & Kanaef, 2008).
60-70% of all heroin users are estimated to inject. For ATS 10-20% of the users are IDU (expert’s comments).
A 2005 estimate mentions that the prevalence of injecting drug users age 15-64 is between 0.19% and 0.31% and the number of people who inject drugs is between 1,800.000 and 2,900.000 (Mathers et al., 2008).
The ever-increasing popularity of intravenous administration of heroin is seen as a key trend in Chinese drug use, fuelled by the switch many users make from ‘‘chasing the dragon’’ to intravenous injection. Another trend is the increasing use of new types of drugs. While opiates, especially heroin, remain the most commonly used drugs in China, MDMA (methylenedioxymethamphetamine or ecstasy) and methamphetamine have recently gained popularity in large and medium-sized Chinese cities (Lu et al., 2008).
2.3 Drug related Harm
2.3.1 HIV infections and mortality (drug related deaths)
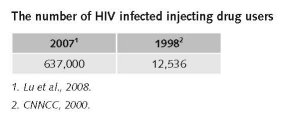
In China, it is estimated that over half of new HIV infections are occurring among the country’s estimated 1.14 million registered drug users. Almost one million people are currently living with HIV in China and drug users account for 63.7% of this population (Lu et al., 2008).
In China, the estimates HIV prevalence among IDUs varies greatly. According to Cook & Kanaef, adult HIV prevalence among IDU is estimated between 0-80% (Cook & Kanaef, 2008).
In China, it is estimated that 110 needles are distributed per IDU per year, and that only 7% of people who inject drugs have access to NSP services in areas where such services exist (Cook & Kanaef, 2008).
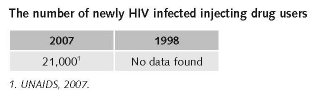
The number of HIV infections due to injecting drug use has increased during the past ten years, but since last year main cause for new infections is not IDU (this is decreasing) but unsafe sex (expert’s comments).
Among the 50,000 estimated new infections during 2007, heterosexual transmission was 44.7%, and transmission through IDU was 42% (UN Theme Group, 2007). 2007 was the first year in which injecting drug use was not the number one reason for infections, which was transmission through heterosexual sex (expert’s comments).
The estimated HIV prevalence of people who inject drugs is between 7.96 and 19.2 (Mathers et al., 2008).
Priorities of harm reduction covered by policy papers and/or law
No published national data found in English on priorities of harm reduction covered by policy papers and/or law.
The number of drug related deaths by overdose
This is not monitored systematically in China. There are no data available on drug related deaths by overdose (expert’s comments).
2.3.2 Drug related crime or (societal) harm
No published data in English found on drug related crime or (societal) harm.
3 Drug policy
3.1 General information
3.1.1 Policy expenditures
It is estimated that more than 100 billion yuan (€11.4 billion)2 is spent (2007) on drug control, and maybe 10 billion yuan (€1.1 billion) on harm reduction (expert’s comments).
The policy expenditures as a whole increased over the past ten years, as supply reduction, demand reduction and harm reduction measures have increased (expert’s comments).
3.1.2 Other general indicators
In June 2000, Information Office of the State Council of the People’s Republic of China issued the strategy of Narcotic Control in China, including:
• Sticking to the position of strict drug control;
• Constantly strengthening drug control legislation;
• Cracking down on drug-related crimes;
• Exercising strict control over the precursor chemicals;
• Treatment and rehabilitation;
• Raising the consciousness of the entire people versus drugs;
• Developing international cooperation in drug control.
The most striking event was that on 15 April 2005, the Politburo Standing Committee (PBSC) of the Communist Party of China Central Committee (CPCCC) held an unprecedented meeting to discuss anti-drug policy. President Hu Jintao himself chaired the meeting and called for a “People’s War against Drugs”. Right after that, the State Council issued a five-year anti-drug plan. Since then, greater efforts in fighting drugs have been witnessed in China, with more integrated law enforcement, more comprehensive public drug awareness campaigns, more flexible treatment and rehabilitation measures, and more productive international cooperation.
In conclusion, currently, the Chinese government adopts more comprehensive and pragmatic policies and takes measures targeting both the supply and demand of the drug use problem. The measures targeting the supply include continuously cracking down on drug smuggling activities and many international collaboration and cooperation. The measures targeting the demand reduction include discouraging new users through anti-drug education campaigns and treatment and rehabilitation work. Chinese mass media have increased anti-drug education to the general population. Anti-drug education has been included in the curricula for primary and secondary school students. More importantly, harm reduction strategy also supported by central government (Hao, 2007).
Numbers available on arrests and imprisonment for drug-law related offences
According to the China National Narcotic Control Commission, in 1999 there 65,000 drug-related criminal cases were reported against 56,000 in 2007. 67,000 suspects were arrested (an increase of 38.6% and 36.3% resp. compared to 2006). In 2007, 36,111 drug criminal cases were brought before court (all courts in China) resulting in 33,285 sentences (Narcotics Control in China, 2000; CNNCC, 2008).
There are no data available on arrest for possession for personal use (expert’s comments).
Additional information
Death is imposed on possession of 50 grams or more of heroin. On possession of lower quantities life sentence is imposed (expert’s comments).
2 1 CNY = €0.114. Exchange rate in December 2008.
3.2 Supply reduction: Production, trafficking and retail
Main focus in China is on production and trafficking. In recent years China has put a lot of efforts in both drug supply measures and scaling op drug treatment including harm reduction facilities.
The information on actually implemented supply reduction measures is limited. Besides policy statements delineating general objectives no information could be found. Laws and policy papers underline the importance of supply reduction. These statements include general principles, drug control publicity and education, drug control, drug treatment measures, drug control international cooperation, legal responsibilities and supplemental articles.
3.3 Demand reduction: Experimental/recreational drug use + problematic use/chronic-frequent use
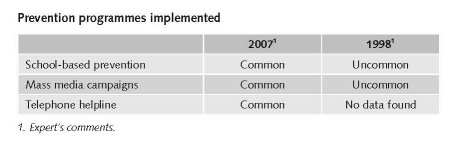
School based drug prevention has been available for some years. Schools are obliged to run programmes. This is basically anti-drug education.
Mass media campaigns exist and usually include celebrities like movie stars that take part in the anti-drug programme.
A national website and telephone helpline has existed for 5 years (expert’s comments).
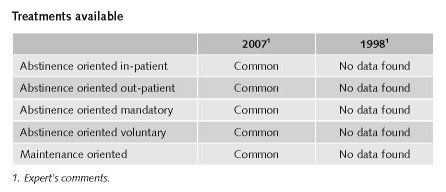
Abstinence-oriented drug treatment is available both mandatory and voluntary but covering only parts of the country. This treatment includes detoxification centres, rehabilitation camps (reform through labour/ re-education), and community centres (this is a new feature, that was approved June 2008).
In 2004, in China officially 105,151 people treated were treated for drug addiction, of which 90% for opiates, 0.6% amphetamines, ecstasy 6.2% and sedatives 3.3% (UNODC, 2008).
In the past decade more drug rehabilitation centres were established, a new model of drug treatment was explored in which physical detoxification, psychological rehabilitation and social reunification was integrated (community centres). The coverage of the community-based drug maintenance treatment was expanded, the number of drug free communities increased (expert’s comments).
Since 2005, there is a big increase in number of Methadone Maintenance Treatment clinics and other harm reduction services (experts’ comments). China, which had 320 opioid substitution therapy (OST) sites in late 2006, has pledged to scale up methadone provision to more than 1,000 sites by the end of 2008. A recent estimate reported that 95,000 people are accessing MMT from 503 clinics (Cook & Kanaef, 2008).
There are more than 700 Methadone Maintenance Treatment Clinics now (June 2008). It is expected that by the end of the year 2008 this number will be 800 MMT (expert’s comments).
Priorities of demand reduction covered by policy papers and/or law
Ten years ago there were no drug policy statements regarding drug treatment (expert’s comments).
On January 12, 1995, the State Council issued The Procedures for Compulsory Drug Addition Treatment which marked the beginning of Chinese government’s comprehensive thinking in addressing the demand reduction of illegal drug problem (Swanstrom & He, 2006).
There are instructions for the establishment of drug rehabilitation centres. NNCC issued the “Notice on Implementing the Guiding Principles of President Hun Jintao’s Important Instructions and Promoting Forcefully the Construction of Drug Rehabilitation Centers” (CNNCC, 2008).
There are also Drug Treatment regulations in effect (expert’s comments).
3.4 Harm reduction
3.4.1 HIV and mortality
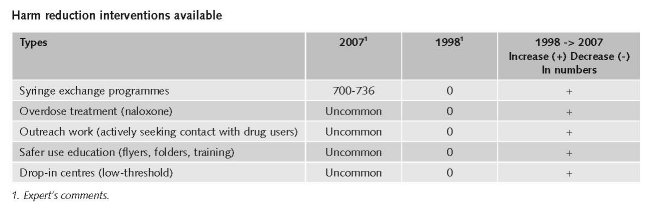
Needle and syringe exchange started in 2000, along with some other Harm Reduction interventions on small scale.
In the last year (2007), the number of NSP sites is reported to have increased in China, India, Malaysia, Myanmar, Taiwan and Nepal (small increase), although decreasing in Bangladesh. NSP services have been rapidly scaled up in China in recent years, from 92 sites in early 2006 to an estimated 775 sites in seventeen provinces in 2007 (Cook & Kanaef, 2008)
Expert comments
Everything started to change in 2003, with the outbreak of the SARS epidemic. The commitment of the government to the issue of HIV prevention is sincere. It approved many interventions including harm reduction measures and is taking care for funding of these interventions (expert’s comments).
Priorities of harm reduction covered by policy papers and/or law
In China, there is an explicit supportive reference to harm reduction in national policy documents (Cook & Kanaef, 2008).
A national policy framework to control and prevent HIV/AIDS was developed by the State Council in 1998, comprising two national strategic plans: the Chinese National Medium- and Long-term Strategic Plan for HIV/AIDS Prevention and Control, 1998-2010 (State Council Document No. 38), and the China Action Plan for Stopping and Controlling AIDS, 2001-2005 (State Council General Office Document No. 40). As a follow up to these plans, the State Council Coordination Committee on HIV/AIDS was upgraded to a State Council AIDS Working Committee (SCAWCO) in 2004 the revised Law on the Prevention and Control of Infectious Diseases, issued in August 2004, which strengthens the principles of prevention/intervention, mass education, non-discrimination and reiterates the responsibility of all levels of Government to respond to the AIDS epidemic. From year 1995 to 2000, more actionable programs were conducted. Several trial programmes3 were set up and key workshops conducted (1st workshop on effective intervention strategies – November 1997) and long term plans4 issued. For example, medium - long term plan on prevention and control HIV/AIDS 1998 -2010 issued in November 1998.
Virtually all provinces, municipalities and autonomous regions have established Long- and Medium Term Plans and Plans of Action, and strategic plans developed by certain ministries, the All China Federation of Trade Unions (ACFTU), the All China Women’s Federation (ACWF), and the Youth League. However, some Ministries as Communication and others would only have Annual Program on HIV, instead of Plan of Action.
Under China’s Action Plan for Reducing and Preventing the Spread of HIV/AIDS (2006-2010) issued on February 27, 2006, it is required that in the year of 2007, the awareness on HIV/AIDS among all the population aged between 15-49 of age should reach 75% in the urban areas, 65% for people living in the rural areas while 70% for mobile population (Tung, 2008).
Changes regarding drug policy during the past ten years
Fundamental bill on HIV/AIDS regulation 2006 include HR interventions. It sanctions officially harm reduction, but not needle exchange. In general, the Central Chinese government now supports harm reduction measures (expert’s comments).
3.4.2 Crime, societal harm, environmental damage
No information found on interventions/measures to reduce harm for society.
3 For example, 1st condom trial – September 1996; 1st needle exchange program trial – October 1999.
4 For example, medium - long term plan on prevention and control HIV/AIDS 1998 -2010 issued in November 1998.
References
Consulted experts
Y. Jianping, AIDS/STD control and prevention officer, CDC China.
Y. Liang, Freelance consultant HIV/AIDS prevention.
L. Lu, Director at the National Institute on Drug Dependence, Peking Union Medical College.
P. Lunding, Senior HIV advisor, UNAIDS China Office.
W. Luowi, Policy officer, CDC China.
G. Nicotera, Project manager UNODC Project Office China, UNODC China.
Y. Sheng Zhang, Nurse, Ping An Hospital, Methadone Maintenance Treatment.
K. Zhang, Professor, Epidemiologist, Vice-president Nation Expert Consultation Committee on AIDS Prevention and Control, Peking Union Medical College.
Documents
Chengzheng Z, Zhimin L, Dong Z, Yanhong L, Jianhui L, Jilang T et al. Drug Abuse in China. Beijing, 2004.
CIA. The World Factbook: China. Available: www.cia.gov/library/publications/the-world-factbook/geos/ch.html, last accessed 10 January 2009.
CNNCC (China National Narcotics Control Commission). Annual report on Drug Control in China, 2008. Beijing, 2008.
Cook C, Kanaef N. Global state of harm reduction 2008. Mapping the response to drug-related HIV and hepatitis C epidemics. London, International Harm Reduction Association (IHRA), 2008.
Hammett TM, Wu Z, Duc TT, Stephens D, Sullivan S, Liu W et al. Social evils’ and harm reduction: the evolving policy environment for human immunodeficiency virus prevention among injection drug users in China and Vietnam. Addiction 2007, 103:137-45.
Hao W. The Status of Drug Abuse and Policy in China. WHO Collaborating Center on Psychosocial Factors, Drug and Health. Mental Health Institute, Second Xiangya Hospital, Central South University China, 2007.
Lu L, Fang Y, Wang X. Drug Abuse in China: Past, Present and Future 2008. Cell Mol Neurobiol 2008, 28: 479-90.
Mathers BM, Degenhardt L, Phillips B, Wiessing L, Hickman M, Strathdee SA et al. for the 2007 Reference Group to the UN on HIV and Injecting Drug Use. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review, 2008.
Narcotics Control in China (2000). Available: www.english.gov.cn/official/2005-07/27/content_17679.htm, last accessed 28 December 2008.
Swanstrom N, He Y. China’s war on narcotics: two perspectives, 2006.
Tung B, Zhang K, Policy Recommendations for HIV/AIDS prevention for Major Infrastructure Projects and Workplace Education Program in China. Project Proposal 2008.
UNAIDS. A Joint Assessment of HIV/AIDS Prevention, Treatment and Care in China (2007), jointly prepared by State Council AIDS Working Committee Office, UN Theme Group on AIDS in China, Beijing, 2007.
UNDCP (United Nations International Drug Control Programme). Studies on Drugs and Crime. Global Illicit Drug Trends 2000. Statistics. Vienna, UNDCP, 2001.
UNODC (United Nations Office on Drugs and Crime). World Drug Report 2007. Vienna, UNODC, 2007.
UNODC. World Drug Report 2008. Vienna, UNODC, 2008.
UNODC. World Drug Report 2008: Global ATS Assessment. Vienna, UNODC, 2008a.
UN Theme Group. A joint assessment of HIV/AIDS prevention, treatment and care in China, State Council AIDS Working Committee Office UN theme Group on AIDS in China, 2007.
WHO (World Health Organization). HIV AIDS care and treatment for people who use drugs in Asia and the Pacific:
an essential practical guide, 2008.
| < Prev | Next > |
|---|