| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 198 |
| Yesterday: | 251 |
| This Week: | 198 |
| Last Week: | 2221 |
| This Month: | 4786 |
| Last Month: | 6796 |
| Total: | 129385 |
MAIN CONCEPTS FOR ASSISTING DRUG USERS IN PRISONS
 |
|  |
| 
Drug Abuse
MAIN CONCEPTS FOR ASSISTING DRUG USERS IN PRISONS
How can health risks related to drug use, sex or tattooing be avoided? We all know that individual habits, social rituals, norms and external factors and lack of information often form obstacles to changing behaviour that is perceived as risky or even damaging. From prevention theory we know that inside information, knowledge from personal experience and trust are important factors in the take up and cessation of a certain behaviour. In the fields of illegal drug use and risk behaviour, trust is a basic requirement. The peer group and the norms of the prison subculture are very important with regard to influencing the attitude of drug users towards safer behaviour. Self-efficacy by role modelling is another highly important feature. This means that providing social information plays a much more important role than simply providing mere facts. This is even more important in settings like prisons, where anonymity and confidentiality is hard to achieve and to realise. Quite often, the level of factual knowledge may be quite high. Elements of factual knowledge which have proved to be important generally refer to specific details (e.g. infection risk by sharing the spoon or the filter).
Being familiar with the group norms and being trustworthy for drug users also serves as a basis for getting reliable information on risk behaviour. Drug use, sexual contacts, tattooing have also to be understood as part of the inmates’ subculture. Being involved in this behaviour always includes an element of resistance against the prison system.
‘Dissonance-Shaping’ is a term from health psychology used to describe the notion that the gap between objectives (of risk reduction) and coping abilities should not be too big. If this gap is too big, then the health objectives we want to be achieved can be rejected easily and will not be integrated into the user’s sense of identity in everyday life. The strength of this ‘dissonance’ should remain ‘acceptable’ as a confrontation with the user’s fundamental goals is not fruitful.
This means:
Changes should be realised step by step. This generally means setting goals below the maximum objectives
Objectives should be acceptable and achievable, i.e. realistic
The credibility of message and messengers are vital
The initial point of departure is the user’s individual resources and living conditions.
But which factors do influence the user’s behaviour and beliefs? These can be illustrated by means of a model for behaviour change. Like all models, this model is a simplification of reality. For instance ‘attitude’ is a complex phenomenon - it is a fair way from being a result of rational decisions. More aspects are relevant: emotional, motivational and environmental aspects may contribute to changes in behaviour as well. It is, however, useful for clarifying how peer support activities can be initiated and how they can be realised. We will briefly describe these factors by giving some examples and indicate how one can influence them by peer support activities.
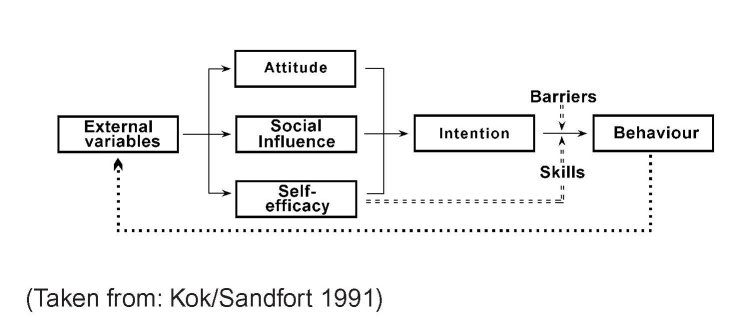
External variables Based on Trautmann / Barendregt ‘European Peer Support Manual’ (see References)
External variables include demographic factors which cannot be influenced (such as gender, age, race etc.) but also residential factors (serving a sentence in a prison) or the political reality (drug policy in prisons).
Examples
Elements of political reality are the drug law, drug policy, public opinion, prison reality, (e.g. no lobby or trade union for inmates etc.). These elements determine drug users’ daily life. For instance, whether or not allowing substitution treatment, distribution of syringes, bleach, general hygienic improvement, gender- and migrant specific services, overcrowding, segregation of (HIV+) drug users, etc.
Risk reduction measures
Proposing a survey of infectious diseases and the situa tion of drug-using inmates in prison to (local) health authorities
Discussing and assessing the drug and infectious disease situation with the prison doctor, colleagues in the medical department, prison staff members.
Trying to influence public opinion in favour of measures like bleach or condom distribution by offering valid reasons (Public health risks) for a risk reduction policy.
Developing a plan for a substitute drug program (detoxification and maintenance).
Attracting allies to support this policy, for example, journalists, scientists, politicians (i.e. local AIDS self-help groups or drug counselling agencies).
4.2 Attitude
Attitude says something about how a person values certain behaviour. Valuing behaviour is weighing advantages against disadvantages, which is not just a logical and rational process. Irrational habits, emotions and beliefs also influence the relative weight of advantages against disadvantages.
Examples
Clean syringe for each injection is valued positively for being hygienic, safe and sharp. But licking a drop of heroin from the needle after the air is pushed out is both unhygienic and ineffective, yet it is valued as positive by some drug users.
Not having a clean needle available in the prison does for many drug users not necessarily mean that they will stop using intravenously. Instead, they rely on trusting other inmates when they claim that they are HIV- or hepatitis negative.
The attitude towards the use of condoms is tremen dous important. Condom use is valued negatively by many people, as they see more disadvantages than advantages associated with their use. It is difficult to mention advantages because most advantages do not give immediate benefit (it’s all about avoiding some thing). The only benefits one could think of is that the sperm is instantly ready for disposal.
Many of the prison staff members might have the attitude that drug users are not capable of changing their behaviour in order to follow precautionary rules or of controlling their drug use in order to comply with health warnings.
Risk reduction measures
Discussing motives, ideas, beliefs towards safer behav iour.
Safer use: discussing with drug-using inmates their beliefs about effective disinfection practices. Which alternative routes of administration do they know? What are the reasons for not applying them?
Safer sex: discussing about the advantages and dis advantages of condom use in a partnership. It alsoshould be stressed that the chance of getting infected and re-infected among drug users and their partners is rel atively high.
Tattooing: discussing measures designed at preventing infections: which are known and applied by prisoners?
Discussing with staff the risks of becoming infected and their beliefs of how best to avoid a risky exposure (i.e. when searching the body or cell). What is their knowl edge of transmission of virus and bacteria?
4.3 Social influence
Direct social influence means that all social surroundings, i.e. the peer group, the institution, partners, family and friends expect certain behaviour. Not behaving in accordance with these expectations can lead to sanctions. Indirect social influence means that norms are internalised; people behave according to the norms as if they are their own rules.
Examples
Direct social influence: in many prisons it is common to share the syringe and needle of a trustworthy inmate simply by rinsing with clean cold water. Refusing a used needle needs to be justified.
Indirect social influence: smoking heroin by means of chasing the dragon was initiated in the Netherlands by people from Surinam, a former colony of the Netherlands. Meanwhile the majority of drug users in the Netherlands have adopted this behaviour.
Risk reduction measures
From different so-called peer support projects - both in and outside prisons - we know that positive social influence by peers can contribute to risk reduction. If some skilled drug-using peer supporters offer a good example of safer behaviour (e.g. proper injecting or alternative routes of administration), then other drug users will tend to follow them. An important prerequisite is that drug users active in a peer support initiative are so-called ‘peer leaders’ meaning that they are both influential and trustworthy, and that they serve as a role
model.
4.4 Self-efficacy
Self-efficacy is the assessment of a person’s abilities to carry out certain behaviour. “Will I succeed in avoiding the use of injectable drugs during this prison sentence?”, and if not, why not? Is my success due to myself, my experience, my intelligence, my persistence or the support of my partner? Do I have enough self-control to avoid simply taking any drug that happens to be available in prison (Including benzodiazapines and others)? Can I resist the various temptations? If a drug user is convinced that they will manage, they can be said to have a high level of self-efficacy. The opposite, however is extremely common. Many drug users regularly experience negative judgements from others in their environment. This influences not only their sense of self-efficacy but also their sense of self-esteem in a negative way. One example of limited self-efficacy is when people are acknowledging and complaining that things are not going well, but there is nothing they can do about it, because everything is the responsibility or product of other people’s actions.
Examples
Many drug users have tried several times to kick he habit. The failure to stay drug free has an influence on the decision to try it once again. Repeatedly relapsing results in low self-efficacy.
If a drug user in prison has some drugs but only has a used syringe, will they take the time to look for disinfectant and clean the syringe? If they are determined to do this and in the end actually manage to do so, then they have shown high self-efficacy.
Condom use depends, in part at least, on the self-effi cacy of the man: can he keep his penis stiff while put ting on a condom? If he doubts - due to disappointing experiences earlier on - he might not want to use a condom in order to avoid a failure.
Risk reduction measures
Successfully carrying out activities enhances one’s self-efficacy. Consequently. when it comes to safer injecting, techniques should be discussed and practised. From so-called self-control projects we know that every drug user does have control techniques that they apply in different situations, such as drug use, drug purchase, selection of other drug users etc. Sharing these control techniques to see if inmates can learn valuable things for their own situation from their peers can contribute to risk reduction. This can be done both intentionally and systematically in a training seminar setting but also on an individual basis. In the case of safer sex though, it is a little more complicated to practice proper techniques.
4.5 Intention
The intention is the actual plan or desire to carry out a particular behaviour. All conditions (positive attitude, supporting social influence and self-efficacy) are - at least for an important part - fulfilled. Now, strictly speaking, there are only two things that can prevent the person from carrying out the behaviour: barriers and lack of skills.
4.6 Barriers
Even when people do wish to change behaviour, in prison people often lack the means to facilitate this behaviour change - which can result in them being unable to make the desired changes in their behaviour.
Example
In general, a drug user might be used to using a clean syringe for each injection. Unfortunately clean works are generally unavailable in the prison setting.
Risk reduction measures
If new syringes are hard to find, or not available at all, then providing bleach or a hotplate, and giving out accurate information about cleaning and disinfecting syringes (see chapter 6.1 above) would be the next best solutions. Also, providing methadone is a measure to consider here.
Skills
If somebody wants to practice safer behaviour but does not know how, lacks experience or doesn’t have any routine to practice, then safer behaviour is much more difficult. People will need to acquire the necessary skills to enable them to engage in safer behaviour.
Example
Drug users who behave in a perfectly safe manner outside prison - using a new syringe for every fix - might run into problems inside prison. They might consider chasing the dragon but lack the necessary skills to do so. They might consider cleaning works but lack both the knowledge and the necessary skills to do so.
Risk reduction measures
Drug users often think of themselves as being experts in injec- ting, but analysing their injection procedure often reveals ‘hidden risks’: either hygienic precautions are not taken or sharing the drug or injection equipment is exposing the drug user to risks. One issue that requires almost permanent attention is that of the injec- ting practices of drug-using in prison, because the prerequisites for safe practice enjoyed outside are not available and drug use takes place in hidden and often unhygienic places. Support for either alternative routes of administration or on proper injecting can be organised, as well as information on disinfection methods. With the support of the prison medical or community health service, staff can provide safer use instructions that can be followed effectively.
Based on Trautmann / Barendregt ‘European Peer Support Manual’ (see References)
Last Updated (Thursday, 06 January 2011 20:54)