| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 159 |
| Yesterday: | 251 |
| This Week: | 159 |
| Last Week: | 2221 |
| This Month: | 4747 |
| Last Month: | 6796 |
| Total: | 129346 |
Chapter 1 INTRODUCTION
 |
|  |
| 
Drug Abuse
Structure of the Manual
This manual has been devised for people who want to involve drug users in HIV/AIDS prevention activities for their peers. This could be either professionals working in drug or HIV/AIDS service organisations or drug user self-organisations.
In Chapter 1 we define some terms that will clarify different viewpoints on the work of drug users.
In Chapter 2 the manual offers tips, hints and considerations on the organisation of peer support groups and activities. This chapter contains material for both professionals and peer lead-ers.
Chapter 3 is all about what can be communicated to drug users. It contains information on hygienic injecting, alterna-tive ways of using drugs and safer sex techniques.
After having read what can be communicated to drug users, we give you idea’s on how to achieve this. Chapter 4, there-fore deals with the major vehicles of communication - outreach work and training courses. This chapter also consolidates the theory of the previous chapters and transforms them into work-able methods.
In the three annexes you will find some background informa-tion on chasing the dragon, nutrition and surviving in the win-ter. The annexes also serve as an example of how to commu-nicate in written language. Notably the article on chasing the dragon is an example of a ‘life style approach’.
Each chapter begins with a table of contents and has its own independent page numbering.
Background of the Project
In recent years there has been a growing acknowledgement that drug users can, and do, contribute to HIV/AIDS preven-tion. Peer support and peer education can be effective strate-gies in reducing risk behaviour in injecting drug user (IDU) communities. In different countries peer support or peer edu-cation projects have been developed not only by profession-als, but also by self-organisations. Efforts have been made to initiate and support drug user self-help groups and self-organisations, especially in the field of HIV/AIDS prevention in IDU communities. One of the reasons for this effort is the finding that HIV/AIDS prevention by regular drug aid services has not been a complete success. There are still drug users who lack information and who simply are not reached by drug aid programmes, or refuse to be reached because of - among other things - feelings of distrust. This distrust is one of the factors that makes peer support seem like a worthwhile at-tempt to get in contact with drug users who cannot be reached by regular drug aid institutions.
In The Netherlands, peer support in the field of HIV/AIDS pre-vention for drug users has been based on the work of autono-mous drug user self-organisations. (‘Autonomous’ meaning that these self-organisations were, and are, independent from pro-fessional institutions). These organisations began emerging in the early seventies and reached their peak in the early eight-ies. (The ‘Junkiebonden’ are a well-known example of this). There have also been other initiatives where drug users (and ex-users), professionals, doctors, social workers, parents of drug users and people that were simply interested in the drug problem worked together.
The approach and contribution of these self-organisations to the drug and HIV/AIDS problem have gained growing recog-nition. This has resulted in financial support from the Health Ministry and local authorities for some of these activities. In recent years the Health Ministry has funded peer support and peer education projects to assess the merits of this approach.
The Dutch National Institute for Alcohol and Drugs (NIAD), in Utrecht, has supported three of these projects. This support included (among other things), the production of a description of the approach and a global evaluation of three of these projects. This information has been disseminated to drug aid services as well as to self-organisations by the national net-work of the Project ‘HIV/AIDS and Drug Use’, NIAD . Through this work and receiving requests for information from organisations in other countries we came up with the idea to make this expertise available to the broader public.
A plan was developed to carry out a peer support project in six countries in the European Union that would be funded by ‘The Commission of the European Communities’. (The European Peer Support Project - ‘Encouragement, development and sup-port of HIV/AIDS prevention by peer support in intravenous user communities’). The project would run from October 1993 until October 1994. The main aim of the project is to encour-age, develop and support professional drug aid services and drug user self-organisations and networks to begin (or extend), peer support strategies especially in the field of HIV/AIDS pre-vention.
Basic elements
The basic elements of this project have been:
![]() Designing guidelines for safer use and safer sex training courses for (injecting) drug users aimed at causing a ‘snow-ball effect’. (These guidelines were developed by gaining expertise in different countries.)
Designing guidelines for safer use and safer sex training courses for (injecting) drug users aimed at causing a ‘snow-ball effect’. (These guidelines were developed by gaining expertise in different countries.)
![]() Organising ‘on the spot’ training courses for key persons (drug users and professionals), in six countries in the Eu-ropean Union (England, France, Germany, Italy, The Neth-erlands and Spain).
Organising ‘on the spot’ training courses for key persons (drug users and professionals), in six countries in the Eu-ropean Union (England, France, Germany, Italy, The Neth-erlands and Spain).
![]() Offering expertise knowledge to local organisations in the participating countries - either as follow-up to the training courses or at request of organisations not involved in the training courses.
Offering expertise knowledge to local organisations in the participating countries - either as follow-up to the training courses or at request of organisations not involved in the training courses.
![]() Producing a training manual (in the six languages of the involved countries), which can be used by professionals as well as self-organisations.
Producing a training manual (in the six languages of the involved countries), which can be used by professionals as well as self-organisations.
Main Concepts
Peer support as part of a harm reduction strategy
Peer support or peer education are part of a harm reduction strategy. The primary aim of harm reduction is to offer ser-vices to ameliorate the living conditions of drug users. ‘Get-ting off drugs’ is not unimportant, but secondary to the main issue which is to develop accessible drug aid programmes. The programmes of the Dutch self-organisations are conducted according to this philosophy. In their view, repressive drug policies (such as those defined by criminal law), are inappro-priate ways to deal with the drug problem. Accordingly, these policies are mainly responsible for what is called the ‘drug problem’.
The concept of ‘acceptance’ is a basic notion regarding HIV/ AIDS prevention methods adequate for reaching drug users effectively. The keynote of the so-called acceptance model is the recognition of the drug user as a human being with the same rights as other human beings. This means that the user has the right to choose how he/she wants to live and if he/she wants assistance. This model offers assistance without for-mulating prerequisites such as stopping drug use. Offering ‘low threshold’ drug aid services creates the possibility to reach drug users effectively.
Peer support and peer education fit well into this framework of harm reduction, as has been demonstrated by the work of the self-organisations in The Netherlands. Besides more general political aspects, HIV/AIDS has become a prominent issue in the work of these organisations. One example of this was a syringe exchange program in The Netherlands in 1984, which was carried out exclusively by the MDHG, (an Amsterdam in-terest group of drug users). Drug aid services at the time re-fused to carry out syringe exchange because they were afraid of supporting drug use, instead of discouraging it. By 1981 the Rotterdam Junkiebond had started distributing syringes on a small scale to prevent the spread of hepatitis. (This was before the discovery of HIV/AIDS.) This, and other initiatives were important to make safer use an issue among drug users. It had in itself a peer support or peer education effect. The distribution of syringes and needles meant drawing attention to the risk of HIV/AIDS and to the importance of safer use.
It stimulated drug users to talk about these issues, to ask ques-tions, to be frank about their fears, etc. Besides providing in-formation, the emotional aspects of this strategy played an important role at the beginning of the HIV/AIDS epidemic. Drug aid services are sometimes not able to deal effectively with these problems.
Intentional non-intentional influence
This partly non intended effect of syringe distribution shows that peer support does not necessarily mean intentionally in-fluencing one’s peers. Peer support is in fact (in a non-inten-tional way), real, everyday life in the drug scene. Drug users - as with everybody else - copy, judge and criticise the behaviour of their peers. Peer support is therefore not a new approach, it is simply intentionally making use of these everyday influences between peers.
The peer support effects of syringe distribution by drug user self-organisations have shown that different interventions in the drug scene can have - non-intentional - peer support side effects. This snowball effect also occurs with outreach work and training courses that are part of a peer support project. This multiplying effect has been used by many including the ‘Boule de Neige’ (French for ‘snowball’) Project in the so-called ‘Euregio’ region (Belgian-Dutch-German border area).
Self organisations: self-help interest group
There are two basic types of self-organisations; a self-help group, or an interest group. In The Netherlands, the central feature of drug user self-organisations has always been that of representing the interests of drug users. Consequently po-litical issues have played a prominent role in their work.
Even within the so-called ‘junkiebonden’ there has been de-bate about whether to call themselves a self-help group or an interest group. Their strong emphasis is however on being an interest group and not a self-help group.
According to the junkiebonden, using the term ‘self-help’ im-plies acceptance of the illness paradigm, which is the ideo-logical base of most drug service organisations. By calling themselves ‘a self-help group’ drug users accept the view that they are sick and need help ‘to cure their addiction’. (For psy-chologists this could be a clear case of ‘over-adaptation’ or ‘subjection to the aggressor’.)
However, one should not neglect the fact that the work of in-terest groups always contains an element of self-help; in the sense that people who join are motivated to re-estimate their situation. Being an active member of an interest group is for many drug users a positive experience enabling them to as-sess their abilities and to foster their self-esteem.
Due to the fact that the target group of the European Peer Support Project are active drug users the choice has been made to focus on the concept of an interest group. This con-cept entails a broader range of activities and is strongly based on the idea of acceptance.
Peer support - peer education
Although the concepts of peer support and peer education have a lot in common, there are important differences. One major difference is that peer education implies and emphasises a disparity between the educator and the educated. In an HIV/ AIDS prevention project for drug users based on the idea of peer education, it is the task of the educator to teach other drug users the rules of safer use and safer sex. Within the concept of peer support however, the idea of mutual support is prevailing and is seen as a broader concept than education. The emphasis is more on community and equality. Sup-port does not only mean influencing other drug users towards safer use and safer sex, it can also imply creating better conditions for safer use and safer sex: For example, the distribu-tion of clean syringes and needles. Because peer support entails equality and is a broad ranging concept, it fits well into the work of a drug user self-organisation - especially an inter-est group. Therefore, the emphasis of the European Peer Sup-port Project is not so much on peer education, but on peer support.
Peer support: knowledge, attitude, etc.
Experience has shown that peer education and peer support knowledge, do contribute to adequate HIV/AIDS prevention for drug users. ‘Inside information’, knowledge from personal experience and trust are important features in this approach. HIV/AIDS prevention in the sense of discussing personal matters such as drug use and sexual behaviour require an element of trust. Experience from other peer support activities has shown that social influence on the attitude of drug users to safer behaviour; and self-efficacy by role modelling, are the most important fea-tures of a successful peer support project. This means that providing social information plays a more important role than providing mere facts. Being trustworthy and familiar as a peer with the group norms also serves as a basis for attaining reli-able information on risk behaviour. (Detailed factual knowl-edge such as risk of infection by sharing the spoon or the filter has proved to be important information.)
It is worthwhile to look at some important factors which influ-ence behaviour. These factors can be illustrated by means of a model for behaviour change. Like all models, this model is a simplification of reality. It is however useful for clarifying how peer support activities can be initiated and realised. We will briefly describe these factors and provide relevant examples which will indicate how one can influence them by peer support activities.
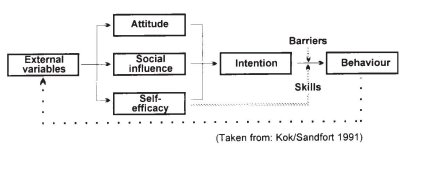
External (outer model) variables
Examples
External External variables are among other things, demographic factors that cannot (or are extremely difficult) to influence. These
variables include gender, age, race, place of residence etc. In this model we look at factors within a certain demographic context. An-other external variable is the political reality.
Elements of political reality are the drug law, drug policy, public opinion etc. These elements determine drug user’s daily life - whether to allow substitution treatment, distribution of syringes etc.
Peer support action
![]() Proposing to (local) authorities a plan for a substitution programme.
Proposing to (local) authorities a plan for a substitution programme.
![]() Trying to influence public opinion in favour of syringe distribution by demonstrating valid reasons for a harm reduction policy.
Trying to influence public opinion in favour of syringe distribution by demonstrating valid reasons for a harm reduction policy.
![]() Attracting allies to support this policy - journalists, scientists, politicians etc. (See chapter 2)
Attracting allies to support this policy - journalists, scientists, politicians etc. (See chapter 2)
Attitude
Attitude says something about how a person values certain Attitude behaviour. Valuing behaviour is weighing advantages against disadvantages, which is not always a logical or rational process. Irrational habits and beliefs also influence the weight of advantages against disadvantages.
Examples
![]() A clean syringe for each injecting is valued positively because it is hygienic, safe and sharp. Whereas, licking a drop of heroin from the needle after the air has been pushed out is, (although unhygienic and ineffective), valued as positive by many drug users.
A clean syringe for each injecting is valued positively because it is hygienic, safe and sharp. Whereas, licking a drop of heroin from the needle after the air has been pushed out is, (although unhygienic and ineffective), valued as positive by many drug users.
![]() The attitude to condom use is tremendously important. Condom use is valued negatively by many people because they see more disadvantages than advantages to using them. It is difficult to discuss the advantages because most advantages do not give immediate benefit (it’s all about avoiding something).
The attitude to condom use is tremendously important. Condom use is valued negatively by many people because they see more disadvantages than advantages to using them. It is difficult to discuss the advantages because most advantages do not give immediate benefit (it’s all about avoiding something).
Peer support action
Try to get a picture of the motives, ideas, beliefs of safer behaviour.
Safer use: Discuss with drug users the advantages and dis-advantages of different sorts of injecting practices. Safer sex: Discuss the advantages and disadvantages of safer sex prac-tices, (e.g. condom use).
It also should be stressed that the chance of becoming in-fected and re-infected is relatively high among drug users and their partners.
Social influence
Direct social influence means that the group expects certain influence behaviour and not doing so can lead to sanctions. Indirect social influence means that norms are internalised and people behave according to the norms as if they are their own rules.
Examples
![]() Direct social influence: In many countries it is usual to share a marihuana joint with others. Not doing so may lead to an argument.
Direct social influence: In many countries it is usual to share a marihuana joint with others. Not doing so may lead to an argument.
![]() Indirect social influence: Smoking heroin by means of chasing the dragon was initiated in The Netherlands by people from Surinam. Now many white Dutch drug users have adopted this behaviour.
Indirect social influence: Smoking heroin by means of chasing the dragon was initiated in The Netherlands by people from Surinam. Now many white Dutch drug users have adopted this behaviour.
Peer support action
The European Peer Support Manual aims at encouraging positive social influence by peers. If skilled drug using peer sup-porters offer good examples of proper injecting techniques, other drug users might copy them. Drug users active in a peer support initiative should be influential, trustworthy and a role model. (See chapter 2)
Self-efficacy
Self-efficacy is the assessment of a person of their possibilities to carry out a certain behaviour. “Will I succeed? Why/ why not? Is my success due to myself, my experience, my cleverness, my persistence?” If one is convinced that this is the case, he or she has a high level of self-efficacy. The con-trary however, is quite common with drug users. Many drug users have experienced negative judgements by their envi-ronment. This influences not only one’s self-efficacy but also one’s self esteem in a negative way. The expression of little self-efficacy can be noted when people complain that things are not going well because of other people.
Examples
![]() Many drug users have tried several times to kick their habit. The failure to stay drug free influences the decision to try it once again. This means they have low self-efficacy.
Many drug users have tried several times to kick their habit. The failure to stay drug free influences the decision to try it once again. This means they have low self-efficacy.![]() If a drug user has money to buy drugs the dilemma may arise about whether they should first go to the dealer, or first buy clean syringes. If they visit the dealer first they might spend all their money and not keep enough for sy-ringes. If they are determined enough to save money for syringes, they have succeeded and have shown high self efficacy.
If a drug user has money to buy drugs the dilemma may arise about whether they should first go to the dealer, or first buy clean syringes. If they visit the dealer first they might spend all their money and not keep enough for sy-ringes. If they are determined enough to save money for syringes, they have succeeded and have shown high self efficacy.
![]() Condom use depends (among other things), on the self-efficacy of the man: Can he keep his penis stiff while put-ting on a condom? If he doubts this, he might not want to use a condom to avoid a failure.
Condom use depends (among other things), on the self-efficacy of the man: Can he keep his penis stiff while put-ting on a condom? If he doubts this, he might not want to use a condom to avoid a failure.
Peer support action
Successfully carrying out activities enhances one’s self-effi- Peer Support cacy. So when it concerns proper injecting, techniques can be action discussed and practised the safest way. This can be done
intentionally and systematically in an outreach setting. When discussing safer sex options it is often more complicated to practice proper techniques.
Intention
The intention is the actual wish to carry out a certain behaviour. All conditions (positive attitude, supporting social influence and self-efficacy) are fulfilled. Only two things can prevent a person from carrying out a behaviour; barriers and a lack of skills. Intention
Barriers
The lack of necessary means can prevent people from carry- Barriers ing out a desired behaviour.
Example
![]() In general drug users are willing to use a clean syringe for Example every new injecting. Unfortunately clean works are not always at hand.
In general drug users are willing to use a clean syringe for Example every new injecting. Unfortunately clean works are not always at hand.
Peer support action
If someone is going to buy or exchange syringes, he or she should think of their peers as well. It is a good thing to buy or exchange more than one syringe at a time.
If syringes are difficult to obtain because there is no exchange programme, or pharmacies do not co-operate, or the police are confiscating syringes, undertake action for better services or try to influence local police policy (see external variables).
(Lack of) skills
It is difficult (and even impossible), for a person to practice safer behaviour if the/she doesn’t know what it is. People need to acquire the necessary skills of safer behaviour.
Example
Once people have decided to use drugs in a safer way they need to be aware of all the ‘ins and outs’ of proper injecting - otherwise they simply cannot do it safely. Making applications for social services such as housing can be pretty difficult. Skills of others are needed sometimes to get things done.
Peer Support action
A more or less permanent point of contention is the injecting practices of other drug users. If the situation is suitable, practical support on proper injecting should always be given. Support on proper injecting can also be organised. An interesting peer support action could be utilising the support of medical staff to provide safer use instructions for drug users.
Last Updated (Thursday, 06 January 2011 20:56)