| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 159 |
| Yesterday: | 251 |
| This Week: | 159 |
| Last Week: | 2221 |
| This Month: | 4747 |
| Last Month: | 6796 |
| Total: | 129346 |
Chapter 4 METHODS OF DELIVERY
 |
|  |
| 
Drug Abuse
Chapter 4 METHODS OF DELIVERY
Table of Contents
INTRODUCTION
OUTREACH WORK
Introduction
How to make contact
The first steps
Making a new contact on your own
Outdoor, on the street
Indoor, in a pub or youth centre
Being introduced by someone
Counselling
How to raise the subject of safer behaviour
How to discuss safer behaviour
Attitude and behaviour
Practical rules
Methods and material to assist outreach work
Introduction Distribution of syringes, needles and condoms Collecting information
Describing the drug scene
Assessing the needs of drug users
Identifying shortfalls in the drug treatment system
Conducting an inquiry by means of a questionnaire
Pamphlets
Magazines/newsletters
Organising activities
Interest related issues
Leisure
TRAINING COURSES
Introduction
General considerations when organising a training course for drug users Safer use exercises
Introduction
Safer sex exercises
Introduction 151
Organisation exercises
Introduction
Introduction
In this chapter, two major approaches of peer support will be discussed:
![]() Outreach work, and
Outreach work, and
![]() Training courses
Training courses
Generally most peer support projects range somewhere between these two basic approaches. Outreach work is used for the unstructured setting of the street; and training courses are used for a more structured, indoor setting.
![]() HIV/AIDS prevention by outreach work normally is confined to what could be called 'spontaneous counselling' (short, incidental talks about HIV/AIDS). Whereas, HIV/AIDS prevention by training courses offers the opportunity to deal with issues at length and intensively. These two methods in fact complement each other quite well; and hence a combination of these two approaches is especially effective. An intensive introduction to HIV/AIDS prevention at a training course can get more impact if it is supported by short, incidental talks. These talks serve as reminders and focus attention to the subject at hand.
HIV/AIDS prevention by outreach work normally is confined to what could be called 'spontaneous counselling' (short, incidental talks about HIV/AIDS). Whereas, HIV/AIDS prevention by training courses offers the opportunity to deal with issues at length and intensively. These two methods in fact complement each other quite well; and hence a combination of these two approaches is especially effective. An intensive introduction to HIV/AIDS prevention at a training course can get more impact if it is supported by short, incidental talks. These talks serve as reminders and focus attention to the subject at hand.
Outreach Work
INTRODUCTION
Outreach work has a lot in common with social work which is based on a harm reduction model. The difference is that the worker leaves the office and 'hits the street'. This means that the worker is meeting people on their own territory and working outside of the normal office-hours model.
Outreach work covers two levels:
![]() An individual approach aiming at personal behaviour change.
An individual approach aiming at personal behaviour change.
![]() A group oriented approach aiming at a socio-cultural change.
A group oriented approach aiming at a socio-cultural change.
As these two levels are intertwined in everyday work, we will not deal with them separately in this chapter.
Outreach work can include different tasks:
![]() making/maintaining contact
making/maintaining contact
![]() collecting information
collecting information
What is going on, what drugs are used, what problems of the target group have priority, etc.?
![]() advice and information
advice and information
Where to find a lawyer, certain services, education, etc.; and also provision of safer behaviour information e.g. concisely repeating the message on different occasions and from different angles.
![]() referral
referral
To other services, therapeutical programmes, etc.
![]() aid and assistance
aid and assistance
In case of psycho-social problems, when referral is impossible, etc.
![]() prevention
prevention
Information about health, drug use, safer use and safer sex, etc.
![]() representing the interests of the target group
representing the interests of the target group
Informing other services and organisations about the living situation and the needs of the target group(s), etc.
This chapter will focus on two issues:
![]() how to make contact
how to make contact
As stated earlier, making and maintaining contact with the target group(s) and collecting information about them, are usually linked. Collecting information is in fact the start of establishing contact with the target group(s). (See chapter 2 p 14).
![]() counselling
counselling
Counselling entails providing advice, information, aid and assistance, referral and prevention strategies on HIV/AIDS and other health related issues. This manual will especially focus on prevention strategies.
HOW TO MAKE CONTACT
Making contact is the key point and most difficult part of outreach work. It is in fact a task on its own, even if it does not result in other activities. Outreach work exists after all, to reach the 'difficult-to-reach' or previously 'un-reached'.
One problem with using the term 'unreached' is that it is not very specific. Before going into detail about how to initiate contact it is worthwhile defining what is meant by it. This can be helpful for establishing the target group (see chapter 2).
The 'unreached' can include:
![]() A person who has never really had any contact with a HIV/ AIDS or drug aid service.
A person who has never really had any contact with a HIV/ AIDS or drug aid service.![]() A person who does not have contact anymore with the above services.
A person who does not have contact anymore with the above services.
![]() A person who does have contact; but is not reached by HIV/AIDS prevention measures.
A person who does have contact; but is not reached by HIV/AIDS prevention measures.
![]() A person who is not reached successfully by HIV/AIDS prevention, due to:
A person who is not reached successfully by HIV/AIDS prevention, due to:![]() deficient information, or
deficient information, or![]() an inadequate approach, or
an inadequate approach, or![]() factors or problems on the client's side; motivation, attitude, social norms, lack of resources, etc.
factors or problems on the client's side; motivation, attitude, social norms, lack of resources, etc.
Making contact with these target groups is generally much easier for drug users, than it is for professionals. Drug users already know a lot of their peers; they are familiar with the norms and codes of the drug scene and they usually do not encounter the same distrust as professionals, etc. However, even peers have limits in establishing contact with drug users. Their success will largely depend on the 'approachability' of the drug using community. In general you could say that: The more repressive the drug policy; the more difficult it is to approach drug users.
Another major factor here is that the drug using population is not homogenous. There are differences in the types of drugs that are used, the ways of administrating drugs, ethnic background and sexual preferences. These differences can stand in the way of developing contacts. This problem can partly be solved by selecting outreach workers of the same gender or the same ethnic background as the target group(s).
The first steps
Before actually making contact with the target group, it is important to have a vague idea who you want to reach and what you want to achieve. With a broad notion of target group(s) and ideas on the aims of the project; you can take the first outreach steps, i.e. 'taking to the streets' and exploring the situation. Important observations are:
![]() Where does the target group meet?
Where does the target group meet?
![]() When do they meet?
When do they meet?
![]() Which drugs are used?
Which drugs are used?
![]() How are they used?
How are they used?
![]() Where are they used ? etc. (Also see Chapter 2 'Collecting information', 'Setting the aims' and 'Selecting the target group(s)')
Where are they used ? etc. (Also see Chapter 2 'Collecting information', 'Setting the aims' and 'Selecting the target group(s)')
Identifying the meeting places of the target group(s) must be done at various time of the day and night to ensure you obtain a realistic picture of the situation. Involving drug users (or ex-users) in this process will undoubtedly provide you with a lot of valuable information: They will either have the necessary information at hand or they will be able to obtain it from their peers. The gathered information serves as the basis for redefining and choosing the target group (criteria, priorities, etc.). Now contact can be made with the target group. (Through obtaining the above information you probably will have established some contact.)
![]() One issue with outreach work has always been whether to work in couples or alone. Working in couples has its advantages regarding the safety of the workers. Nonetheless, working as a couple might be less productive than working alone. Working in couples can result in more talks between the workers than with the target group.
One issue with outreach work has always been whether to work in couples or alone. Working in couples has its advantages regarding the safety of the workers. Nonetheless, working as a couple might be less productive than working alone. Working in couples can result in more talks between the workers than with the target group.
Establishing contact entails:
![]() Visiting the meeting places, observing how people interact, who is a 'leader', etc.
Visiting the meeting places, observing how people interact, who is a 'leader', etc.
![]() Begining a conversation; generally it is good to start with a casual chat to get on speaking terms and to create a basis.
Begining a conversation; generally it is good to start with a casual chat to get on speaking terms and to create a basis.
![]() Introducing yourself;
Introducing yourself;![]() explaining what your task is
explaining what your task is
![]() what organisation/group you are working for (you can leave a business card)
what organisation/group you are working for (you can leave a business card)![]() what you stand for
what you stand for![]() what you can do for the target group, etc.
what you can do for the target group, etc.![]() Establishing trust and credibility with the target group(s). This can be done by;
Establishing trust and credibility with the target group(s). This can be done by;![]() proving that you are one of them (e.g. by referring to your own drug use experience)
proving that you are one of them (e.g. by referring to your own drug use experience)![]() always being honest (about who you are, what you are able to do, etc.)
always being honest (about who you are, what you are able to do, etc.)![]() offering support in case of problems (only offer what you can fulfil).
offering support in case of problems (only offer what you can fulfil).
It is often a long-term and frustrating enterprise working out how to really make contact and how to actually begin a project. This is especially so if you have to start in a new site or neighbourhood. You have to decide:
![]() Where to hang out (at which site, at a distance or near by people, etc.).
Where to hang out (at which site, at a distance or near by people, etc.).![]() When to visit a place.
When to visit a place.![]() What is the right moment to approach people (do they have time, are they in the mood for a talk, etc.)
What is the right moment to approach people (do they have time, are they in the mood for a talk, etc.)![]() Which person to contact first.
Which person to contact first.![]() What is the right way to make contact (direct or less direct).
What is the right way to make contact (direct or less direct).![]() What can you offer.
What can you offer.![]() When to stop (when to give it a break and leave).
When to stop (when to give it a break and leave).
It is important to distinguish the two ways of establishing a new contact:
![]() Doing it on your own.
Doing it on your own.
![]() Being introduced by someone.
Being introduced by someone.
Making a new contact on your own
The first step is to visit the meeting place of the target group.
This can be either: ![]() outdoor, on the street, or
outdoor, on the street, or ![]() indoor, in a pub, a youth centre, etc.
indoor, in a pub, a youth centre, etc.
Outdoor, on the street
The most difficult point without a doubt is 'how to start'. Sometimes just 'hanging around' for a while can be helpful. This can provide the opportunity for a chance to make contact, to start a casual conversation, to ask a question or be asked what you are doing there. However, just hanging around at a meeting place of the target group can also make people suspicious.
Sometimes it is better to immediately tell them that you are an outreach worker on behalf of a drug aid service, etc.
It can be helpful to develop a schedule to regularly visit a site, starting with shorter visits which can gradually be extended.
![]() An example of how to make use of an outdoor setting ,if the target group like playing soccer: Is to: 1. join in one of their games, or 2. explicitly invite people to join one of your games, or 3. be in a place where you have seen the target group playing soccer, and encourage them to 'join in'.
An example of how to make use of an outdoor setting ,if the target group like playing soccer: Is to: 1. join in one of their games, or 2. explicitly invite people to join one of your games, or 3. be in a place where you have seen the target group playing soccer, and encourage them to 'join in'.
Contact can be established either:
![]() Indirectly; e.g. by starting a casual chat (about soccer, the neighbourhood, etc.). This can develop into a more personal talk, where you can introduce yourself, or maybe you will be asked to introduce yourself
Indirectly; e.g. by starting a casual chat (about soccer, the neighbourhood, etc.). This can develop into a more personal talk, where you can introduce yourself, or maybe you will be asked to introduce yourself![]() Directly; introducing yourself as a drug aid and/or HIV/ AIDS prevention worker;
Directly; introducing yourself as a drug aid and/or HIV/ AIDS prevention worker;![]() explaining what your task is
explaining what your task is![]() what you stand for
what you stand for![]() what you can do for the target group, etc.
what you can do for the target group, etc.
A direct approach can be quite difficult, however it can be made much easier by using some strategies. Useful instruments for an outreach project can be:
![]() an inquiry using a questionnaire, e.g. on the needs and/or problems of the target group(s)
an inquiry using a questionnaire, e.g. on the needs and/or problems of the target group(s)![]() handing out a leaflet which contains information on the project
handing out a leaflet which contains information on the project![]() handing out a newsletter/magazine
handing out a newsletter/magazine![]() distributing condoms/syringes
distributing condoms/syringes![]() organising activities (a meeting, sport, music, etc.)
organising activities (a meeting, sport, music, etc.)
More information on the above strategies for making contact, can be found in this chapter under the heading 'Methods and material to assist outreach work' (see page 20).
Indoor, in a pub or youth centre
It can be easier to make contact indoors than on the street. In public meeting places such as a pubs and youth centres, it is generally easier to legitimise why you are there. You can have a drink, read a newspaper or a magazine, or just sit there and look around. In a meeting place for one specific group, a stranger may be viewed curiously and/or with suspicion. Curiosity can lead to some questions, which give the outreach worker the chance to introduce him or herself.
Indoor, there are some practical things worth keeping in mind, such as:
![]() sitting/standing at a bar will make it easier to get in contact than sitting alone at a table
sitting/standing at a bar will make it easier to get in contact than sitting alone at a table![]() always offer people the chance to avoid/stop the contact you can start a conversation about the weather, soccer or an interesting event
always offer people the chance to avoid/stop the contact you can start a conversation about the weather, soccer or an interesting event![]() you can join in a game, like pinball, pool, table football, etc.
you can join in a game, like pinball, pool, table football, etc.
Furthermore, the strategies outlined above can also be helpful in an indoor setting.
![]() In an indoor setting it may be somewhat easier to approach Being someone in a direct way. An example of a direct approach introduced by is: An outreach worker visiting a youth centre heard some someone boys talking 'macho' about sex. He threw some condoms on the table which made them laugh. This was a chance to direct the subject to safer sex.
In an indoor setting it may be somewhat easier to approach Being someone in a direct way. An example of a direct approach introduced by is: An outreach worker visiting a youth centre heard some someone boys talking 'macho' about sex. He threw some condoms on the table which made them laugh. This was a chance to direct the subject to safer sex.
![]() This example demonstrates that humour can be an important element in making contact and introducing a serious subject. It also makes clear that an appropriate assessment of the situation is of utmost importance; where you cause laughter in one group you may be beaten up in another. It shows that attitude, intuition and inventiveness are vital. An outreach worker should be able to correctly interpret a situation and find an adequate approach. Therefore personality and finding tactful ways of operating are of major importance.
This example demonstrates that humour can be an important element in making contact and introducing a serious subject. It also makes clear that an appropriate assessment of the situation is of utmost importance; where you cause laughter in one group you may be beaten up in another. It shows that attitude, intuition and inventiveness are vital. An outreach worker should be able to correctly interpret a situation and find an adequate approach. Therefore personality and finding tactful ways of operating are of major importance.
As soon as the outreach worker has made some contact with people from the target group(s), things can become easier. Making new contacts can be done by being introduced by the people you already know. If people trust the outreach worker they might introduce their friends to him or her.
The first can also be a relatively easy job. If you are an outreach worker at a meeting place of the target group (either indoor or outdoor), where you already know some people and you want to make more contact with other people: You can either:
![]() Join a group with some people you know and start a talk with them. By doing so you generally will be introduced or otherwise you will have the chance to introduce yourself to the people you do not know.
Join a group with some people you know and start a talk with them. By doing so you generally will be introduced or otherwise you will have the chance to introduce yourself to the people you do not know.
![]() Explicitly ask one of the people you know to introduce you to people you want to make contact with. You also can ask if people know others who could benefit from information on HIV/AIDS, etc.
Explicitly ask one of the people you know to introduce you to people you want to make contact with. You also can ask if people know others who could benefit from information on HIV/AIDS, etc.
Again, your success will depend on an appropriate assessment of the situation.
It can be helpful to visit the meeting places of the target group(s) on a regular basis; i.e. the same time, on specific days. The meeting places of the target group could either be on the street or indoor, in a pub or youth centre, etc. This makes it easier for the target group(s) to find the outreach worker, either for their own needs, or for introducing, or referring a friend to him/her e.g. 'If you go to this place on Friday at 10 o'clock you can meet him/her'.
Building up contacts can also be facilitated by handing out something to the target group(s). (See also 'Making a new contact on your own' page 5).
Being introduced by people you already know is often called 'snowballing'. The starting point for snowballing can also be a drug agency. The drug users you are meeting there can be interviewed and asked if they can introduce the worker to their peers. If this process is carried out systematically a lot of people can be seen in a relatively short amount of time.
Before initiating outreach work it is worthwhile to find out if this approach is needed. It is wise to examine existing services to see why they do not reach certain groups of drug users. It might be much more cost effective to make existing services more attractive or accessible. Consider alternatives, e.g. needle exchange/distribution can be done by both outreach workers and/or syringe vending machines (if they are strategically placed).
COUNSELLING
Counselling plays an important role within the different tasks of outreach work. Counselling can be providing short advice, information and/or referral. It can also be prevention. In this manual we have concentrated on prevention, although the information we will discuss may also be useful for other tasks. The following issues will be dealt with:
![]() How to raise the subject of safer behaviour?
How to raise the subject of safer behaviour?![]() How to discuss the subject of safer behaviour?
How to discuss the subject of safer behaviour?
How to raise the subject of safer behaviour
Making contact with drug users is one thing; starting a conversation about HIV/AIDS is another. Outreach work is work without a clear agenda and without a well defined structure. An outreach worker is dependent on accidental contacts as appointments are generally difficult to make. However, it is worthwhile to make a plan before you go on the streets; giving thought to which person(s), group(s) and subjects have priority. This can result in some guidelines, which will give you some structure for your work on the streets'.
Working in an unstructured setting has a lot of advantages:
![]() It can be very effective because you are 'working' in the target group(s)' own environment. You are not dependent on set appointments and daily life in an office. You can respond directly to real life and spontaneous situations and to questions people have, etc.
It can be very effective because you are 'working' in the target group(s)' own environment. You are not dependent on set appointments and daily life in an office. You can respond directly to real life and spontaneous situations and to questions people have, etc.![]() Operating in the familiar surroundings of the target group(s) generally facilitates an atmosphere of trust.
Operating in the familiar surroundings of the target group(s) generally facilitates an atmosphere of trust.![]() You are obtaining valuable information about the actual living situation and behaviour of the target group(s).
You are obtaining valuable information about the actual living situation and behaviour of the target group(s).![]() If people know what your are doing, sometimes they will start talking to you about HIV/AIDS or other health related issues.
If people know what your are doing, sometimes they will start talking to you about HIV/AIDS or other health related issues.![]() There are various other ways to raise the issue of safer behaviour:
There are various other ways to raise the issue of safer behaviour:![]() Looking for openings in either casual or planned contracts. An outreach worker can give a short reminder about safer use when confronted with a drug user having an abscess. Other opportunities are if someone has been to hospital, or someone has had an overdose. Making use of all unexpected situations is very important.
Looking for openings in either casual or planned contracts. An outreach worker can give a short reminder about safer use when confronted with a drug user having an abscess. Other opportunities are if someone has been to hospital, or someone has had an overdose. Making use of all unexpected situations is very important.![]() It will soon become tiring if you only focus on HIV/AIDS prevention when discussing safer use and safer sex with drug users (see chapter 2, page 13). Therefore, it is advisable to incorporate HIV/AIDS preventionmessages in a broader framework of drug users 'subculture', e.g. focusing on health in general, or even in the form of a general interest group.
It will soon become tiring if you only focus on HIV/AIDS prevention when discussing safer use and safer sex with drug users (see chapter 2, page 13). Therefore, it is advisable to incorporate HIV/AIDS preventionmessages in a broader framework of drug users 'subculture', e.g. focusing on health in general, or even in the form of a general interest group.![]() If you meet people you know but, haven't seen for a while, questions such as 'How are you ?' and 'How are things going?', may be enough to begin a conversation which also includes issues to do with their health.
If you meet people you know but, haven't seen for a while, questions such as 'How are you ?' and 'How are things going?', may be enough to begin a conversation which also includes issues to do with their health.![]() The instruments for making contact which were previously outlined (on page 20) can also be useful here:
The instruments for making contact which were previously outlined (on page 20) can also be useful here:![]() giving out condoms/syringes
giving out condoms/syringes![]() colecting information
colecting information![]() an inquiry using a questionnaire, e.g. what are the needs and/or problems of the target group(s)?
an inquiry using a questionnaire, e.g. what are the needs and/or problems of the target group(s)?![]() handing out a pamphlet which provides information on the project
handing out a pamphlet which provides information on the project![]() handing out a newsletter/magazine
handing out a newsletter/magazine![]() organising activities (a meeting, sport, music, etc.)
organising activities (a meeting, sport, music, etc.)
More information on ways of making contact with the target group(s) can be found in this chapter under the heading 'Methods and material to assist outreach work' (see page 20).
It is vital to have a broad repertoire of ways to raise HIV/AIDS prevention issues. It is not enough to simply once raise/discuss the issue. Short reminders and repeats of the messages from different angles and approaches can be very effective.
How to discuss safer behaviour
Most counselling occurs in a structured and/or therapeutic setting. However, outreach counselling does not take place in a specific setting, nor does it have a clear structure of well defined roles. An outreach worker has to create a setting for talking confidentially which is dependent on spontaneous opportunities. There are some rules for discussing the subject of safer behaviour.
Attitude and behaviour
![]() Do not be judgmental e.g. condemning risk behaviour as 'stupid or ridiculous' will not change the way a person behaves.
Do not be judgmental e.g. condemning risk behaviour as 'stupid or ridiculous' will not change the way a person behaves.![]() This also means, do not ask 'why'? Posing the question 'why' often shows that you don't understand and therefore you place judgement on the person. Open questions, which invite people to tell their story brings about more important information.
This also means, do not ask 'why'? Posing the question 'why' often shows that you don't understand and therefore you place judgement on the person. Open questions, which invite people to tell their story brings about more important information.
![]() Do not patronise. Avoid giving advice about personal matters such as whether a person should be tested for HIV. Also avoid statements on how to behave (If I were you I would ...'). Try to offer relevant and complete information and also discuss alternatives. Making your own decision about a matter is more important and effective than simply adopting someone else's view. In impersonal or objective matters, advice can be very useful; here are some examples, 'In this case you need a lawyer. You can refer to ...'; 'For getting tested you can go to this doctor/hospital. You first have to make an appointment by phone'; 'You should boil a syringe for 15 minutes and not only flush it with boiling water'.
Do not patronise. Avoid giving advice about personal matters such as whether a person should be tested for HIV. Also avoid statements on how to behave (If I were you I would ...'). Try to offer relevant and complete information and also discuss alternatives. Making your own decision about a matter is more important and effective than simply adopting someone else's view. In impersonal or objective matters, advice can be very useful; here are some examples, 'In this case you need a lawyer. You can refer to ...'; 'For getting tested you can go to this doctor/hospital. You first have to make an appointment by phone'; 'You should boil a syringe for 15 minutes and not only flush it with boiling water'.
![]() Do not take over the responsibility of someone else's problems. Try to motivate and support people to solve their own problems by themselves.
Do not take over the responsibility of someone else's problems. Try to motivate and support people to solve their own problems by themselves.
![]() Listen carefully. This means do not talk too much and do not interpret. Ensure however, that you have understood correctly what a person is saying by recapitulating what he/she has just said and asking if this is what they meant by it.
Listen carefully. This means do not talk too much and do not interpret. Ensure however, that you have understood correctly what a person is saying by recapitulating what he/she has just said and asking if this is what they meant by it.
![]() Stick preferably to the 'here and now'. What do people feel or think now? What do certain things or emotions mean to people now? What are their possibilities? etc. This approach generally provides more relevant information for realising safe behaviour than discussing the past.
Stick preferably to the 'here and now'. What do people feel or think now? What do certain things or emotions mean to people now? What are their possibilities? etc. This approach generally provides more relevant information for realising safe behaviour than discussing the past.![]() Pay attention to emotions. How and what do people feel? What do certain events mean to them? etc. This can give insight into why people behave as they do.
Pay attention to emotions. How and what do people feel? What do certain events mean to them? etc. This can give insight into why people behave as they do.
![]() Show that you understand and care by showing interest. Ask people how they are, how things are going, where have they been? If a person has disappeared for a while, ask their 'mates' where he/she is. If you know where a person is, you could even visit him/her (at home, in hospital, in prison etc.).
Show that you understand and care by showing interest. Ask people how they are, how things are going, where have they been? If a person has disappeared for a while, ask their 'mates' where he/she is. If you know where a person is, you could even visit him/her (at home, in hospital, in prison etc.).
![]() Treat people with respect. For example: Thank people for their information and/or assistance; apologise when you are bothering someone; invite them for a cup of coffee at a cafe or at your office, etc.
Treat people with respect. For example: Thank people for their information and/or assistance; apologise when you are bothering someone; invite them for a cup of coffee at a cafe or at your office, etc.
![]() Do not play therapist or 'shrink'. It is important to listen carefully and pay attention to what someone is saying. Avoid playing the role of an untouchable, personally uninvolved therapist. Questions like 'Tell me, how does it feel?', 'What does this mean to you?', can raise feelings of aversion, especially when asked in reaction to questions for advice or help. Drug users might know this way of counselling by their attempts to 'kick their habit'. Their experiences with therapeutic treatments are frequently bad.
Do not play therapist or 'shrink'. It is important to listen carefully and pay attention to what someone is saying. Avoid playing the role of an untouchable, personally uninvolved therapist. Questions like 'Tell me, how does it feel?', 'What does this mean to you?', can raise feelings of aversion, especially when asked in reaction to questions for advice or help. Drug users might know this way of counselling by their attempts to 'kick their habit'. Their experiences with therapeutic treatments are frequently bad.
![]() Most of these rules are closely linked to the personality and attitude of the outreach worker. It is evident that an outreach worker has to be genuine in his/her care and understanding. Just pretending and using these rules is not enough. It is inadvisable to use the 'jargon or codes' of the target group(s) if the outreach worker does not feel familiar or comfortable with them. An outreach worker has to integrate these 'rules and codes' into his/her own, personal style of behaviour.
Most of these rules are closely linked to the personality and attitude of the outreach worker. It is evident that an outreach worker has to be genuine in his/her care and understanding. Just pretending and using these rules is not enough. It is inadvisable to use the 'jargon or codes' of the target group(s) if the outreach worker does not feel familiar or comfortable with them. An outreach worker has to integrate these 'rules and codes' into his/her own, personal style of behaviour.![]() To get an understanding of how an outreach worker is developing his/her personal style of working, regular feedback is necessary. This can be done by external supervision and/or by accompanying an outreach worker on the street. As supervision is not based on direct observation of how someone is working, immediate feedback is not possible.
To get an understanding of how an outreach worker is developing his/her personal style of working, regular feedback is necessary. This can be done by external supervision and/or by accompanying an outreach worker on the street. As supervision is not based on direct observation of how someone is working, immediate feedback is not possible.
Practical rules
![]() Try to find a quiet place to talk where you have an undisturbed conversation, e.g. a quiet bar or street (where you can sit down), at a person's home, etc.
Try to find a quiet place to talk where you have an undisturbed conversation, e.g. a quiet bar or street (where you can sit down), at a person's home, etc.![]() Ensure that a person has time and that he/she feels like talking. Generally it is obvious if somebody is in a hurry, or in search for drugs, etc. If your aim is a longer conversation you can explicitly ask if someone has time. You can also invite someone to have a cup of coffee with you.
Ensure that a person has time and that he/she feels like talking. Generally it is obvious if somebody is in a hurry, or in search for drugs, etc. If your aim is a longer conversation you can explicitly ask if someone has time. You can also invite someone to have a cup of coffee with you.![]() Use appropriate language, i.e. language that is readily understood and accepted. It is important to know/learn the 'jargon and the codes' of the target group(s).
Use appropriate language, i.e. language that is readily understood and accepted. It is important to know/learn the 'jargon and the codes' of the target group(s).![]() Provide consistent, complete and objective information which offers people choices (see chapter 3). Informing people is not only telling them something, it is also listening to what they have to say. When asking personal questions it is important to state clearly that people don't have to answer if they don't want to. Explain the reason why you are asking this question (so as not to be seen as offensive), e.g. to gain valuable information on the needs of the target group(s).
Provide consistent, complete and objective information which offers people choices (see chapter 3). Informing people is not only telling them something, it is also listening to what they have to say. When asking personal questions it is important to state clearly that people don't have to answer if they don't want to. Explain the reason why you are asking this question (so as not to be seen as offensive), e.g. to gain valuable information on the needs of the target group(s).![]() Provide relevant information. This can be done by a conducting a formal risk assessment:
Provide relevant information. This can be done by a conducting a formal risk assessment:![]() using a form to collect relevant information on level of knowledge (e.g. what do people know about HIV/AIDS?), attitude (e.g. how do people view condom use?) and risk behaviour of the target group members (e.g. do they share their injecting equipment?).
using a form to collect relevant information on level of knowledge (e.g. what do people know about HIV/AIDS?), attitude (e.g. how do people view condom use?) and risk behaviour of the target group members (e.g. do they share their injecting equipment?).![]() explaining the basics of HIV/AIDS (e.g. transmission of the virus, risk behaviour, etc.)
explaining the basics of HIV/AIDS (e.g. transmission of the virus, risk behaviour, etc.)![]() asking and answering questions
asking and answering questions![]() discussing possibilities to reduce risks, etc.
discussing possibilities to reduce risks, etc.
A formal risk assessment enables both prevention worker and drug user to set risk reduction goals and structure outreach prevention. However, it generally will not be possible to reach all outreach contacts with this formal instrument. For people who cannot be reached by this instrument it is necessary to have a less formal, appropriate variant. This means that you will have to be able to improvise.
![]() Besides explicitly talking about HIV/AIDS related issues, an outreach worker can also discuss safer behaviour information that can be 'read between the lines'. For example; you can talk about other health subjects (e.g. how to survive on the street, how to have a balanced diet.); about drug users life-style (e.g. not only misery, but also having fun and enjoying life). This strategy can be effective to prevent people from being bombarded with HIV/AIDS prevention information.
Besides explicitly talking about HIV/AIDS related issues, an outreach worker can also discuss safer behaviour information that can be 'read between the lines'. For example; you can talk about other health subjects (e.g. how to survive on the street, how to have a balanced diet.); about drug users life-style (e.g. not only misery, but also having fun and enjoying life). This strategy can be effective to prevent people from being bombarded with HIV/AIDS prevention information.
![]() Do not talk exclusively about HIV/AIDS prevention. Outreach work involves working in the 'daily life' of people. It is therefore, impossible and inadequate to confine yourself only to HIV/AIDS prevention. If you have gained people's confidence they will regularly seek contact with you on other issues besides HIV/AIDS prevention. Most likely their first priority will not be information about safer use and safe sex. They might be more in need of other services. Those needs cannot be denied when working on the streets. If you do, you lose your credibility. Therefore it is important to have knowledge of, and contacts with relevant services (see chapter 2, page 37).
Do not talk exclusively about HIV/AIDS prevention. Outreach work involves working in the 'daily life' of people. It is therefore, impossible and inadequate to confine yourself only to HIV/AIDS prevention. If you have gained people's confidence they will regularly seek contact with you on other issues besides HIV/AIDS prevention. Most likely their first priority will not be information about safer use and safe sex. They might be more in need of other services. Those needs cannot be denied when working on the streets. If you do, you lose your credibility. Therefore it is important to have knowledge of, and contacts with relevant services (see chapter 2, page 37).![]() Support positive changes in behaviour and attitude. Supporting changes towards safer behaviour is important to foster self-esteem and self-efficacy (see chapter 1, page 8). This also provides the basis for ongoing change.
Support positive changes in behaviour and attitude. Supporting changes towards safer behaviour is important to foster self-esteem and self-efficacy (see chapter 1, page 8). This also provides the basis for ongoing change.
![]() Do not judge or reject a person if he/she has a negative change of behaviour.
Do not judge or reject a person if he/she has a negative change of behaviour.
![]() Encourage and support 'snowballing'
Encourage and support 'snowballing'
by simply asking drug users to pass on the information to their peers, by discussing how this can be done, by involving drug users in the production and distribution of information.![]() Do not force people to continue talking. Do not ignore the implicit, unspoken signals that may force someone to continue talking against their will. Do not explicitly force people to talk e.g. 'Wait a minute, I want to ask you another question? Indicators for stopping (or not beginning) a talk can be:
Do not force people to continue talking. Do not ignore the implicit, unspoken signals that may force someone to continue talking against their will. Do not explicitly force people to talk e.g. 'Wait a minute, I want to ask you another question? Indicators for stopping (or not beginning) a talk can be:![]() if the conversation 'loses it's flow', e.g. if people stop asking questions or barely respond to your questions — if people are becoming restless
if the conversation 'loses it's flow', e.g. if people stop asking questions or barely respond to your questions — if people are becoming restless![]() if people's attention is diverted frequently, e.g. if they start talking with somebody else or change the subject. If you want to talk further, you can try to make an appointment and/or let them know you will be back to continue your discussion.
if people's attention is diverted frequently, e.g. if they start talking with somebody else or change the subject. If you want to talk further, you can try to make an appointment and/or let them know you will be back to continue your discussion.
METHODS AND MATERIAL TO ASSIST OUTREACH WORK
Outreach work can be assisted by using some useful 'tools'
These tools include:![]() giving out condoms/syringes
giving out condoms/syringes![]() collecting information
collecting information![]() conducting an inquiry by means of a questionnaire
conducting an inquiry by means of a questionnaire
![]() a pamphlet
a pamphlet![]() a newsletter/magazine
a newsletter/magazine![]() organising activities
organising activities
Distributing material and conducting an inquiry, invites the target group(s) to talk with the outreach worker.
![]() The commercial sector has shown us how important it is to keep communicating with your potential clients. This means establishing a steady relationship between product and client. In this respect there is not much difference with way services are conducted in the public health sector.
The commercial sector has shown us how important it is to keep communicating with your potential clients. This means establishing a steady relationship between product and client. In this respect there is not much difference with way services are conducted in the public health sector.
Prevention materials can be anything that draws the attention of the target group(s). Materials are always more effective when they can be utilised by the target group(s). Therefore, ensure that prevention materials support the goals you are aiming at. For example; to stop injecting drugs, to stop the sharing of injecting equipment and disinfecting used needles. Prevention materials should also meet the needs of people you are aiming at. Do not distribute 1 ml barrel syringes if people are using 2m1 ones.
Distribution of syringes, needles and condoms
![]() Talking about HIV/AIDS risk reduction alone is not enough. It should be accompanied by materials. When providing HIV/AIDS prevention in an outreach setting it can be very effective to distribute syringes, needles and condoms. Handing out prevention materials should be accompanied by talking about HIV/AIDS prevention. Handing out prevention materials should create an atmosphere which allows a person to start talking about HIV/AIDS or the materials handed out.
Talking about HIV/AIDS risk reduction alone is not enough. It should be accompanied by materials. When providing HIV/AIDS prevention in an outreach setting it can be very effective to distribute syringes, needles and condoms. Handing out prevention materials should be accompanied by talking about HIV/AIDS prevention. Handing out prevention materials should create an atmosphere which allows a person to start talking about HIV/AIDS or the materials handed out.![]() Distribution of needles and syringes and other injecting equipment can be an effective way to penetrate injecting drug user (IDU) communities. If it is illegal to carry syringes without prescription, bleach and other legal injecting equipment can be distributed.
Distribution of needles and syringes and other injecting equipment can be an effective way to penetrate injecting drug user (IDU) communities. If it is illegal to carry syringes without prescription, bleach and other legal injecting equipment can be distributed.
![]() Distributing needles, syringes and condoms makes it immediately clear what you stand for. It also shows that you have an accepting attitude towards people who use drugs.
Distributing needles, syringes and condoms makes it immediately clear what you stand for. It also shows that you have an accepting attitude towards people who use drugs.
![]() It is recommended to provide other materials as well as the basics, e.g. alcohol swabs, filters and ascorbic acid to dissolve brown heroin. Some outreach prevention projects only supply the basics.
It is recommended to provide other materials as well as the basics, e.g. alcohol swabs, filters and ascorbic acid to dissolve brown heroin. Some outreach prevention projects only supply the basics.
![]() Before choosing to distribute syringes and needles make sure you choose the preferred type and size. It is better is to have a range of different types and sizes available. Different people have different needs. The same reasoning applies for condoms.
Before choosing to distribute syringes and needles make sure you choose the preferred type and size. It is better is to have a range of different types and sizes available. Different people have different needs. The same reasoning applies for condoms.
![]() It is also useful to strategically place containers for used syringes and needles. From a public order point of view syringe/needle containers are important because less syringes will be found on the street.
It is also useful to strategically place containers for used syringes and needles. From a public order point of view syringe/needle containers are important because less syringes will be found on the street.
![]() Distributing syringes and needles can be used as a prompt to begin a discussion about preparing drugs for proper injecting. The distributor should possess the ability to assess whether the situation is suitable to start such a conversation.
Distributing syringes and needles can be used as a prompt to begin a discussion about preparing drugs for proper injecting. The distributor should possess the ability to assess whether the situation is suitable to start such a conversation.
![]() Make sure that people who distribute syringes and needles carry some kind of ID which can be used in case of police harassment.
Make sure that people who distribute syringes and needles carry some kind of ID which can be used in case of police harassment.
![]() In cities where the accessibility to injecting equipment is relatively easy, syringe and needle distribution is a means to make contact with drug users. If drug users become dependent on outreach workers who distribute needles something has gone wrong. Outreach workers should make efforts to enable drug users to take care of their own health and not make them 'doubly dependent'. Keep in mind the classic metaphor `do you give the hungry man a fish or do you teach him to fish?'. However, in cities where the distribution of injecting equipment is limited the distribution conducted by outreach workers is vitally important.
In cities where the accessibility to injecting equipment is relatively easy, syringe and needle distribution is a means to make contact with drug users. If drug users become dependent on outreach workers who distribute needles something has gone wrong. Outreach workers should make efforts to enable drug users to take care of their own health and not make them 'doubly dependent'. Keep in mind the classic metaphor `do you give the hungry man a fish or do you teach him to fish?'. However, in cities where the distribution of injecting equipment is limited the distribution conducted by outreach workers is vitally important.
![]() As mentioned earlier, HIV/AIDS is a narrow basis to establish an interest group. This is also so if you relied on the distribution of syringes and needles for contacting and maintaining valuable relationships with drug users. For example: In The Netherlands only 30 to 40 % of the opiate users, `shootup'. So for the majority of dependent users distributing syringes and needles is useless. Additional strategies are therefore required.
As mentioned earlier, HIV/AIDS is a narrow basis to establish an interest group. This is also so if you relied on the distribution of syringes and needles for contacting and maintaining valuable relationships with drug users. For example: In The Netherlands only 30 to 40 % of the opiate users, `shootup'. So for the majority of dependent users distributing syringes and needles is useless. Additional strategies are therefore required.
Collecting information
An important task for people working 'on the street' is collecting information. Collecting information is a means to make contact with people. It also legitimises outreach workers to continue their work 'on the street', even in tad times' when they meet only a few people. Collecting information includes three main goals:
![]() describing the drug scene
describing the drug scene
![]() assessing the needs of drug users
assessing the needs of drug users
![]() identifying short falls in the drug treatment system
identifying short falls in the drug treatment system
Describing the drug scene
It is necessary for outreach workers and peer supporters to know what is happening in the drug scene. If this is done systematically, valuable information can be obtained. Observation is the keyword here. A standard observation form could be used to collect data. Subjects to be observed could be:
![]() What drugs are used?
What drugs are used?
![]() How are they used?
How are they used?
![]() Who uses drugs? Ethnic backgrounds?
Who uses drugs? Ethnic backgrounds?
![]() Where do people live?
Where do people live?
![]() What do they do during the day?
What do they do during the day?
![]() How do they get money?
How do they get money?
![]() Where do they inject drugs?
Where do they inject drugs?
![]() Who do they inject drugs with?
Who do they inject drugs with?
![]() How do they relate to each other?
How do they relate to each other?
![]() Is there a social hierarchy in the network?
Is there a social hierarchy in the network?
![]() What are the norms and values relating to high-risk behaviour?
What are the norms and values relating to high-risk behaviour?
![]() Consider making observations about the frequency drug users use certain services and the way they experience these services (see 'Conducting an inquiry by means of a questionnaire').
Consider making observations about the frequency drug users use certain services and the way they experience these services (see 'Conducting an inquiry by means of a questionnaire').
![]() Observation forms should be quick and easy to fill in, and not take more than 5 minutes a day. Consequently not all issues can be covered in one observation form. We suggest dealing with one subject for a limited period and then changing to another one. (see chapter 2, 'General organisational aspects').
Observation forms should be quick and easy to fill in, and not take more than 5 minutes a day. Consequently not all issues can be covered in one observation form. We suggest dealing with one subject for a limited period and then changing to another one. (see chapter 2, 'General organisational aspects').
Assessing the needs of drug users
The basic principle in assessing the needs of drug users is to listen to what they have to say. Outreach workers should be open minded to the stories and complaints of drug users. A lot of needs are easily assessed by just observing drug users daily life; scoring drugs, being homeless, malnutrition, medical treatment etc.
![]() Outreach workers should list the problems they encounter in the streets. Listing problems and needs should be done as systematically as possible (see above).
Outreach workers should list the problems they encounter in the streets. Listing problems and needs should be done as systematically as possible (see above).![]() In the framework of peer support, drug users can make an inventory of the needs of their peers.
In the framework of peer support, drug users can make an inventory of the needs of their peers.
![]() People 'in the streets' are not always used to making their needs known in a structured way. Part of the skill of being an effective outreach worker and peer supporter, is interpreting and classifying the needs and problems of drug users.
People 'in the streets' are not always used to making their needs known in a structured way. Part of the skill of being an effective outreach worker and peer supporter, is interpreting and classifying the needs and problems of drug users.
![]() The needs of drug users can vary. Drug users in methadone treatments have different needs to that of homeless drug users. Different needs also require different types of action. Some needs require immediate action e.g. medical treatment other needs require a long term policy e.g. making substitution treatment available.
The needs of drug users can vary. Drug users in methadone treatments have different needs to that of homeless drug users. Different needs also require different types of action. Some needs require immediate action e.g. medical treatment other needs require a long term policy e.g. making substitution treatment available.
Identifying shortfalls in the drug treatment system
A needs assessment of the drug treatment system ought to result in concrete action towards the services who should be meeting these needs.
Interest groups have several tools for action available:
![]() publishing a report of the results of the needs assessment
publishing a report of the results of the needs assessment![]() meetings with policy and decision makers
meetings with policy and decision makers![]() raising media awareness by press releases and public actions
raising media awareness by press releases and public actions![]() organising a workshop
organising a workshop![]() or a combination of the above tools.
or a combination of the above tools.
![]() If a needs assessment has been carried out systematically it is easier to discuss these needs with local politicians and drug agencies (see 'Conducting an inquiry by means of a questionnaire').
If a needs assessment has been carried out systematically it is easier to discuss these needs with local politicians and drug agencies (see 'Conducting an inquiry by means of a questionnaire').
Raising an awareness is one thing, changing policy is another; and far more difficult. Be conscious of the fact that accomplishing real change demands more than just one action. Defending your interests is a long term strategy. Set realistic goals and be satisfied with small achievements. These small achievements can contribute to the continuity of the self organisation/ peer support initiative.
Conducting an inquiry by means of a questionnaire
An effective way to contact drug users in their own environment is to use questionnaires which form an inquiry. In the Netherlands drug user self organisations in various cities have carried out research by means of questionnaires. The use of questionnaires by drug user self organisations has two aims:
![]() gaining insight in the theme studied (see need assessment)
gaining insight in the theme studied (see need assessment)![]() getting known as a (self)organisation in the scene.
getting known as a (self)organisation in the scene.
Asking for information shows that you take people seriously; that you are dependent on the information they provide.
The results of the inquiry can be the basis of a change in the local drug policy.
The effect of an inquiry can be an increased consciousness on the subject that has been dealt with. For example: If a study is done on people's experience with methadone programmes, people will become aware of the way they are treated.
Questionnaires should collect the basic demographics of the target group(s). This includes: age, gender, nationality, residence, level of education, source(s) of income. The questionnaires should be completed anonymously. If anonymity is not guaranteed it is likely that you will obtain false data or no cooperation at all (chapter 1).
Inquiries can be conducted on a range of subjects. Some big issues for drug users are:
![]() methadone treatment
methadone treatment![]() syringe and needle exchange
syringe and needle exchange![]() police actions
police actions
Obviously, big issues are important as the results can have political impact. However they demand very precise preparation and a complex analysis of the data. This usually requires an experienced organisation. For some self organisations it is recommended to examine smaller issues first, such as:
![]() the use of filters
the use of filters![]() how injecting equipment is cleaned
how injecting equipment is cleaned![]() how needles and syringes are disposed of, or
how needles and syringes are disposed of, or![]() ask people to try the femidom and report their experiences
ask people to try the femidom and report their experiences
![]() Preferably the questionnaire should be designed in conjunction with a researcher or somebody else with compatible skills.
Preferably the questionnaire should be designed in conjunction with a researcher or somebody else with compatible skills.![]() Everyone involved in using the questionnaire should be instructed on the structure and content of the questionnaire. It is also important to discuss possible difficulties which may arise during the interview.
Everyone involved in using the questionnaire should be instructed on the structure and content of the questionnaire. It is also important to discuss possible difficulties which may arise during the interview.![]() Limit the time for collecting data to a set period. Keep in mind that the analysis of the collected data takes the same amount of time as collecting the data. Again, the support of experienced people will be very helpful.
Limit the time for collecting data to a set period. Keep in mind that the analysis of the collected data takes the same amount of time as collecting the data. Again, the support of experienced people will be very helpful.
Pamphlets
Pamphlets can be used in outreach work to inform drug users Pamphlets on different issues. They should assist you in making contact with drug users and also help you to make yourself known in the drug scene.
The general rule is that they should be easy to read; using pictures increases the readability of a pamphlet. A pamphlet should always name the organisation or project who produced it. If the name is always the same and the information is useful and credible, the pamphlets and the person who is handing them out, will gain the confidence and trust of the target group.
Pamphlets can be used for the following:![]() announcing the foundation of a self organisation/peer support initiative
announcing the foundation of a self organisation/peer support initiative![]() when a self organisation/peer support initiative has found a place to meet
when a self organisation/peer support initiative has found a place to meet![]() when organising activities or actions for and with drug users
when organising activities or actions for and with drug users![]() Making contact in the drug scene is a difficult job which requires skill and time. Using pamphlets can ease the establishment of contacts. Ensure that you don't fall into the trap of allowing pamphlets to replace human contact. If this occurs, pamphlets are not serving their purpose. Pamphlets can never replace a face to face conversation.
Making contact in the drug scene is a difficult job which requires skill and time. Using pamphlets can ease the establishment of contacts. Ensure that you don't fall into the trap of allowing pamphlets to replace human contact. If this occurs, pamphlets are not serving their purpose. Pamphlets can never replace a face to face conversation.
Magazines/ newsletters
A magazine can be an extra helpful tool if it becomes known in the target group. Distributing a new edition and having new copies with you, helps to make contact with people you don't know, but who do know the magazine.
Before choosing to publish a newsletter you should be clear on what the goals are. For example; is the newsletter:![]() A voice for drug users to communicate to other drug users. Keeping people updated on activities is an important topic.
A voice for drug users to communicate to other drug users. Keeping people updated on activities is an important topic.![]() A voice for drug users to inform drug workers, policy makers and the police. It is important for drug users to express their point of view.
A voice for drug users to inform drug workers, policy makers and the police. It is important for drug users to express their point of view.![]() To inform drug users about health related issues. Information is the key word.
To inform drug users about health related issues. Information is the key word.
In reality newsletters will include more than one of the objectives mentioned above. However it is worthwhile to define the primary objective. This will help people to choose the right angle when writing an article or doing an interview.
Informative material, especially if it is lifestyle oriented can be effective, as the work of Mainline in The Netherlands has shown. Among other things, Mainline produces a professionally designed magazine in which HIV/AIDS prevention information and general information on health for drug users is incorporated into a life-style' formula. In 'Mainline' (the magazine) you can find articles on street life, prostitution, falling in love, services for drug users, different ways of using drugs, life stories and a comic strip. Nearly all the articles are based on and/or reflect the experiences of drug users. The magazine is distributed to drug users personally on the streets. This is where contacts occur and information is exchanged about health problems, or confidential matters such as safer use and safer sex. This mutual exchange of information, means that Mainline not only gives out information to drug users but it also obtains information from them. This 'street information' is one of the strengths of the articles in the 'Mainline' magazine.
This example clearly demonstrates, that outreach work is important for getting the message across. Discussing personal matters such as using drugs and sexual behaviour, is often easier in your own familiar surroundings than in someone else's space, e.g. the premises of a drug service.
A newsletter or magazine can in various ways assist outreach work by:![]() making/keeping contact with the target group(s) through distributing the newsletter or magazine
making/keeping contact with the target group(s) through distributing the newsletter or magazine![]() collecting information for an article
collecting information for an article![]() raising a subject by referring to an article
raising a subject by referring to an article![]() a readership study
a readership study![]() Issuing a magazine on a regular basis is an enormous job. Ensure to adapt the size and frequency of a newsletter or a magazine to the capacity of an organisation. It is better to publish a small newsletter which is issued regularly, than a fancy magazine which is only published every now and then.
Issuing a magazine on a regular basis is an enormous job. Ensure to adapt the size and frequency of a newsletter or a magazine to the capacity of an organisation. It is better to publish a small newsletter which is issued regularly, than a fancy magazine which is only published every now and then.
Organising activities
Organising activities for and with drug users can be a tool in establishing a credible self organisation/peer support initiative. Activities can be divided into two main area's: leisure and interest related issues.
Interest related issues
Interest related issues need ongoing attention. Organising special meetings is important to inform volunteers, peer supporters and other drug users. Consider inviting experts e.g. medical doctors, lawyers, epidemiologists, policy makers. Topics which can be discussed in special meetings include:![]() legal rights
legal rights![]() epidemiological update
epidemiological update![]() medical subjects (hepatitis C)
medical subjects (hepatitis C)![]() changes in the law etc.
changes in the law etc.
A successful meeting depends on how well it has been organised. A meeting will be well attended by drug users if the self organisation/peer support initiative has a certain status in the drug scene, and if the issue(s) to be discussed is relevant. A strategy for reaching as many people as possible is important. Consider the use of pamphlets in combination with 'snowballing' (see 'Being introduced by someone').
Leisure
In general less attention is paid to leisure activities. Working for drug users interests and on HIV/AIDS issues can make people forget that having fun is important. Fun activities can be important for volunteers and peer supporters. Think of sports and/or tournaments such as chess, table football, darts etc.
Before organising an activity, ensure people are interested in participating.
Cultural activities can include benefit gigs of bands who are sympathetic to HIV/AIDS and drug use. Inevitably large amounts of money will be involved in such events, therefore, consider co-operation with other organisations.
![]() Drug users have different backgrounds and preferences. It is possible that some people will only want to put energy into defending the common interests of drug users and will not be interested in organising leisure activities.
Drug users have different backgrounds and preferences. It is possible that some people will only want to put energy into defending the common interests of drug users and will not be interested in organising leisure activities.
Training Courses
INTRODUCTION
This part of the manual reflects a considerable part of the experience the editors have had conducting training courses in different European countries. Training courses are distinct from outreach work, by the fact that they take place indoor and have a well defined structure. However, the issues that are dealt with in training and outreach work are similar.
Two levels of training courses can be organised in the framework of peer support.
![]() Training small groups of drug users about safer use and safer sex, possibly resulting in a snowball effect
Training small groups of drug users about safer use and safer sex, possibly resulting in a snowball effect
![]() Training drug users about safer use and safer sex and as 'peer supporters' involved in a project.
Training drug users about safer use and safer sex and as 'peer supporters' involved in a project.
Both training courses have their own perspective. The first type is usually for drug users who do not initially intend to become active peer supporters on behalf of a self organisation, or a peer support project. However, our experience shows that a training course can have an impact on both the participant and his/her peers. It is not hard to imagine that a training course will be discussed with friends and peers. This is where the snowball starts 'to roll'. In our opinion this type of training course can be organised and conducted by both professionals and drug users.
The latter type of training course demands a broader peer support framework. These kinds of training courses are usually conducted as a starting point for peer support activities. It can be valuable to invite professionals to participate. Professional support is therefore facilitated.
This type of training course can also fit into already existing drug user activities. For example; it can be organised for drug users who want to become seriously involved in a drug user peer support initiative. It is needless to say that in these courses, attention should be paid to the organisational aspects of peer support, safer behaviour messages and lastly, delivering the message to the target group(s).
In training courses the emphasis should not only be on knowledge about safer use and safer sex, but also on attitude, social norms and self-efficacy. To ensure that more than factual knowledge is communicated, it is important that training sessions are interactive. Participants should not be taught, but stimulated, or even provoked to take part in the discussions. Therefore, we have chosen exercises which are based on active participation. The role of the trainer is basically to guide the discussion and to ensure that accurate information is provided and nothing is missed.
This manual presents exercises on three major peer support subjects: safer use, safer sex and organisation of peer support. These exercises need to be integrated into the general framework of a particular training course. This framework includes:
![]() introducing the participants
introducing the participants![]() explaining 'why' there is a need for the training course
explaining 'why' there is a need for the training course![]() outlining the programme
outlining the programme![]() providing regular breaks etc.
providing regular breaks etc.
GENERAL CONSIDERATIONS WHEN ORGANISING A TRAINING COURSE FOR DRUG USERS
This framework has not been discussed in this manual. We assume that the basic knowledge on how to conduct a training course is present, or at least, easy to obtain.
![]() Invite potential participants well in advance. People have to get used to the idea of being invited to attend a training course. The background of the training course should be discussed and explained. An official letter emphasises that their presence is appreciated.
Invite potential participants well in advance. People have to get used to the idea of being invited to attend a training course. The background of the training course should be discussed and explained. An official letter emphasises that their presence is appreciated.![]() In the mean time, keep people informed about the development of the training course.
In the mean time, keep people informed about the development of the training course.![]() Do not stop motivating people to attend the training course until they have actually arrived.
Do not stop motivating people to attend the training course until they have actually arrived.![]() Invite more people than you in fact want to train. Due to the illegality of drugs, people are sometimes forced to do other, more urgent things.
Invite more people than you in fact want to train. Due to the illegality of drugs, people are sometimes forced to do other, more urgent things.![]() Training non-substituted drug users can be of great value. However it is even harder to get these people to a training course due to their daily needs. Consider temporary substitution during the training course.
Training non-substituted drug users can be of great value. However it is even harder to get these people to a training course due to their daily needs. Consider temporary substitution during the training course.![]() The number of people to be trained should not exceed 20.
The number of people to be trained should not exceed 20.![]() It is better to organise a training course in three afternoons, than to organise a training course which takes an entire day.
It is better to organise a training course in three afternoons, than to organise a training course which takes an entire day.![]() It is important to take the level of skill and experience of the participants as a starting point when conducting a training course.
It is important to take the level of skill and experience of the participants as a starting point when conducting a training course.![]() Keep in mind that the gender, sexual orientation and ethnicity of a trainer can play an important role.
Keep in mind that the gender, sexual orientation and ethnicity of a trainer can play an important role.![]() Give a small present to the participants as an appraisal for their presence.
Give a small present to the participants as an appraisal for their presence.![]() Consider paying people for their presence. This is because they could have been out on the street making money, instead of attending your training course.
Consider paying people for their presence. This is because they could have been out on the street making money, instead of attending your training course.![]() Consider giving people a diploma after the course.
Consider giving people a diploma after the course.![]() Always end a training course with an oral/written evaluation. Including information on, what have they learnt, what was lacking, suggestions for improvement etc.
Always end a training course with an oral/written evaluation. Including information on, what have they learnt, what was lacking, suggestions for improvement etc.![]() Choose a room for the course close to where people live or 'hang out'. The room will have a higher 'psychological' accessibility.
Choose a room for the course close to where people live or 'hang out'. The room will have a higher 'psychological' accessibility.![]() Organising a training course for drug users can become more valuable if some kind of follow-up activity is organised.
Organising a training course for drug users can become more valuable if some kind of follow-up activity is organised.
Almost all of the exercises presented in this manual have been used in training courses with drug users. The key to a successful training course is the active involvement of the participants by taking their knowledge and experience as a starting point.
SAFER USE EXERCISES
Introduction
Proper injecting is a skill which is not learned overnight. A skill is learned and improved by practise i.e. writing. For injecting drug users injecting is an important skill. Unfortunately, some drug users have not learned the skill correctly, or are not always capable (due to difficult situations) to practice proper injecting according to hygienic standards.
The exercises in this manual aimed to improve drug users injecting skills. Some of the exercises are designed to develop HIV/AIDS prevention skills in an outreach setting.
Each exercise should be valued whether it is suitable for the local situation. Where necessary, trainers should adapt the exercises to local needs.
The video tape which is enclosed with this manual has been designed to show only to drug users and to people working with drug users. DO NOT PUBLICLY BROADCAST THE VIDEO. We have enclosed the video because we believe it is necessary to have an example of 'proper injecting'. The injecting sequence is shown in full, without any comment. In some of the following exercises we suggest you show a part of the video.
Safer Use 1 Excercise with video
This exercise uses a part of the video with the complete proper injecting sequence. The trainer can choose from:
a shot of heroine with detachable needle
a shot of cocaine with non-detachable needle.
Objectives:
![]() Introducing the subject of safer use
Introducing the subject of safer use![]() Showing the correct self injecting sequence.
Showing the correct self injecting sequence.
Duration of exercise: 15 to 30 minutes
Number of participants: Minimum 4, maximum 20
Material needed: European peer support video
Video equipment
Exercise outline:![]() Show the video.
Show the video.![]() Ask for comment afterwards. Focus on the different ways participants inject and the possible hygienic mistakes made by the actor.
Ask for comment afterwards. Focus on the different ways participants inject and the possible hygienic mistakes made by the actor.
Variation:
If you are not using the video![]() You can ask one of the participants to show how he/she prepares a shot and how he/she would inject it.
You can ask one of the participants to show how he/she prepares a shot and how he/she would inject it.![]() The other participants watch carefully and provide comments afterwards.
The other participants watch carefully and provide comments afterwards.
Safer Use 2 Exercise with video
This exercise uses the last part of the video in which the complete chasing the dragon sequence is shown (see also Annex 1)
Objectives:
![]() Introducing 'chasing the dragon' as an alternative way of taking heroin.
Introducing 'chasing the dragon' as an alternative way of taking heroin.![]() Discussing safer use techniques.
Discussing safer use techniques.
Duration of exercise: 15 to 30 minutes
Number of participants: Minimum 4, maximum 20
Material needed: European peer support video Video equipment
Exercise outline:![]() Show the 3rd part of the video.
Show the 3rd part of the video.![]() Ask for comment on this way of taking drugs.
Ask for comment on this way of taking drugs.![]() Discuss the opinions of 'chasing the dragon'
Discuss the opinions of 'chasing the dragon'
Safer Use 3 'in case of...'
Every injecting drug user is interested in injecting drugs quickly and efficiently. To be successful in doing so, certain conditions must be fulfilled:
— all equipment must be at hand
— veins should be easy to inject
— the drug user should have the skills to inject properly
— being undisturbed and comfortable
Unfortunately these conditions are not always fulfilled. It often happens that the conditions are unfavourable at the very moment that drugs are available. For drug users it is extremely handy to have a repertoire of alternatives available which can limit the harm due to unfavourable circumstances.
Objectives: 0 How to respond effectively to unfavourable circumstances for proper injecting.
0 Drug users share the improvising skills they have for proper injecting.
Duration of exercise: 30 to 60 minutes
Number of participants: Minimum 4, maximum 20
Material needed: Copies of the 'in case of...' list (see next page) Pen and paper
Exercise outline:
• The trainer splits the group into two groups (A and B) or in couples.
• Each group is given some unfavourable circumstances which they have to respond to as if it were a real life situation.
• After some time, the group should come together again and discuss several of the responses.
On the following pages you will find a list of unfavourable factors and possible alternatives for safe injecting.
SAFER USE 3
(Copy sheet)
'IN CASE OF...' (a selection)
A no clean needles are available
B no bleach is available
A no fresh tap water is available
B a shot of cocaine and the needle clogs
A a shot of heroine and the needle clogs
B the syringe has a bad vacuum (piston/plunger leaks)
A the needle has a wire-edge (burr)
B no drugs and 10 clean needles and syringes
A no spoon is available
B no fresh cotton is available
A no alcohol swab is available
B the plunger cannot be pulled back any further
A you notice you hit next to the vein (bubble)?
B you have difficult veins; hard, rolling, deep laying
A you do not have a quiet place of your own.
B you have an abscess
A you hit an artery
IN CASE OF... SOME ALTERNATIVES
• no clean needles are available
— boil it out for 15 minutes
— clean it with bleach
— take the drugs by chasing the dragon
— snort the drugs
• no bleach is available
— boil it out for 15 minutes
— chase the dragon
— snort the drugs
— clean it carefully with anything else (cola, alcohol etc.)
• no fresh tap water is available
— use mineral water
— or boil water for 15 minutes
• one portion of drugs, one clean syringe, one used syringe and two persons willing to share the drugs equally.
— boil out the used syringe or clean it with bleach
— both chase the dragon
— one person divides the drugs into two equal portions, the other chooses
• one portion of drugs, two persons each with a used syringe of their own and willing to share the drugs equally.
— boil out the used syringes or clean them with bleach
— or second best: rinse your own syringe well
— one person divides the drugs into two equal portions, the other chooses
• a shot of cocaine and the needle has clogged.
— stop injecting, put the liquid back on the spoon, remove the clot, add some cold water, put on a new needle, or use a new syringe and needle
— to unblock the needle: warm the needle with a lighter to expand it
— pull up some fresh cold water and shake the syringe
• a shot of heroine and the needle has clogged
— stop injecting, put the liquid back on the spoon, put on a new needle, or use a new syringe and needle.
• the syringe has a bad vacuum (piston/plunger leaks)
— take a new syringe
— make the rubber of the piston wet and try again
• the needle has a wire-edge (burr)
— sharpen it on a match-box and clean it with a lighter flame.
• no drugs and 10 clean needles and syringes stupid question
try to make some money with it.
• no spoon is available
— prepare the bottom of a tin (e.g. coke can), clean it with a flame
• no fresh cotton is available
— use the filter of a cigarette
— use whatever else is available such as; an alcohol swab, the lining of a coat etc.
— use no filter; carefully tip the spoon and keep the residue at the other end from where you draw up.
• no alcohol swab is available
— clean injection spot with water and soap
— clean it with water only
— do not clean it.
• the plunger cannot be pulled back any further
— stop injecting, untie the tourniquet, place half the contents of the barrel back on the spoon, or in a second syringe, then let your arm hang down; tie off again and
— look for another vein.
— take a second syringe
• you notice you hit next to the vein (bubble)?
— cover it with wet bandages
— smoothly massage the bubble
• you have difficult veins; hard, rolling, deep laying
— learn to chase the dragon
— ask someone to help you
• you don't have a quiet place of your own
— find a friend with a quiet place
— public toilet. Be aware of public toilet doors that open inwards. If you overdose, you will fall against the door and nobody will be able to open it to help you.
• you have an abscess
— make a compress of wet bandages
— see a doctor as soon as possible.
• you hit an artery
— untie the tourniquet immediately and pull out the needle press on the spot with a bandage for at least 5 minutes, until you are sure it has stopped bleeding.
(Alternatives contributed by drug users of HKPD, Vlissingen, the Netherlands and from Oxford, UK)
Safer Use 4 negotiation skills
Apart from different individual 'technical' problems (as was outlined in exercise 2), drug users can run into situations where problems have to be sorted out with other drug users. This exercise raises the subject of solving problems together.
Objective: To prepare drug users for high
risk situations.
Duration of exercise: 30 to 60 minutes Minimum 4, maximum 20
Number of A flip chart to write down reactions/solutions
participants: Marker pens
Material needed:
Exercise outline:
• The trainer splits the group into small groups of about 5 people.
• Each group gets one or two high risk situations (giving different groups the same situation might lead to an interesting comparison).
• The participants are asked to sort out the safest solution.
• In a plenary discussion the solutions found are compared and discussed.
HIGH RISK SITUATIONS:
• Two people and 1 gram of cocaine. It is 10.00 PM you are at someone's house and you have only one syringe. How do you both get a 'hit' and not become infected?
• One portion of drugs, two people with a used syringe of their own and are willing to share the drugs equally.
• Two people and 1/2 gram of heroine. It is 8.00 am and both of you are suffering withdrawl symptoms. The pharmacist opens at 9.00 am and you do not have any needles.
• Three friends take a good shot of heroine, all with their own clean needle. Everyone gets really stoned for a while. They then want to take another 'hit' but are not sure whose syringe is who's.
• Fifty drug users in prison. One syringe available.
• Let the participants bring in a high risk situation which has been solved in a safe way.
• Let the participants bring in a high risk situation which could not be solved 100% safely.
Safer Use 5 outreach situations
Outreach workers and drug users conducting HIV/AIDS prevention, run into situations where drug users are practising self injecting. It is a question of the right timing to raise the proper injecting issue. In this exercise we try to find out what a third person (friend, a relative, health worker) can do to improve proper injecting. By means of discussion and practice several situations for proper injecting are reviewed.
Objectives:
Duration of exercise: Number of participants:
O Discuss the right timing to raise the subject of proper injecting in outreach situations.
O Discuss how to support drug users with proper injecting.
O Exercising practical support
30 to 60 minutes Minimum 4, maximum 15
Material needed: The European peer support video Video equipment
A tourniquet.
Exercise outline:
• Show one of the injecting parts of the video.
• Ask participants, "If you were in the same room as the drug user, when and how would you start a conversation about safer use?".
In general:
• What kind of situations are most suitable for starting a conversation about safer use with drug users on the street? Or As a drug user, when do you definitely not want to be disturbed by a talk about safer use?
• What kind of introductions are appropriate to raise the safer use subject e.g. the weather, police harassment, availability of needles etc.
Technique:
• An explicit peer support action is to help each other find good veins. Participants look for good injecting veins on their neighbour's arms. Roll up the sleeves and examine your neighbour's arms carefully.
• Correctly using a tourniquet is essential for many drug users. Participants practice the correct and incorrect use of a tourniquet. The results are watched closely (veins coming up, going down). This exercise is particularly interesting if done by people with difficult veins.
• Question: What can be done to make veins come up?
— if there is no tourniquet available
— if it is cold and veins are deep down
Safer Use 6 where to inject
Objectives:
Duration of exercise:
Number of participants:
O Participants look critically at their in-
jecting technique.
• What alternatives do participants use
for intravenous injecting (for example intramuscular and subcutaneous injecting).
30 to 45 minutes
Minimum 4, maximum 15
Material needed: Copies of a drawing of the human body (see next page).
Exercise outline: A large (A3) copy of the drawing for use in the plenary. (Using a mannequin is even better.)
• The trainer splits the group into small groups of two to four people.
• Each small group receives a copy of the 'copy sheet'.
• Ask participants to judge and mark possible injecting spots on the copy sheet according to the following standards, (allow 20 minutes):
1=well suitable
2=only in an emergency
3=risky
4=never
• In a plenary session the small groups present their work. On the large drawing of the human body the correct standard is marked.
Please judge and mark the possible injecting spots according to the following standards:
1 = well suitable
2= only in an emergency
3 = risky
4 = never
(Copy sheet)
where to inject
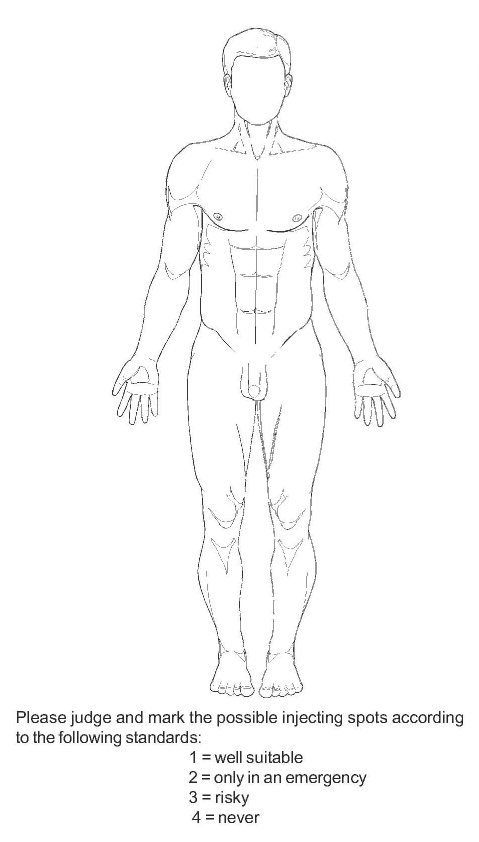
SAFER SEX EXERCISES
Safer sex is an important topic because it can prevent the Introduction transmission of HIV. Research has revealed that safer sex is
a badly practised behaviour; especially among heterosexuals. In 1994, in many western European countries, the highest incidence of new infections with HIV is among heterosexuals. Drug users often find it easier to talk about safer use than safer sex. Sex is generally a hard topic to discuss.
General considerations
• In some situations it is recommended to avoid a group of mixed gender.
• Agree with the group to be respectful towards participants' sexual orientation.
• The trainer should not be inhibited to talk freely about sex and sexuality.
• Consider involving a second trainer of the opposite sex.
• When using a dildo, choose a colour which is appropriate to the group. Do not offend coloured people by using a white dildo.
• It is widely experienced that people are reluctant to practice the 'condom technique' on a dildo. This emphasises the need to conduct exercises which encourage people to practice using condoms. We suggest using other, less intimidating, 'phallic' objects as well.
• The exercises in this part of the manual deal with safer sex in various ways. We have begun with some exercises which aim at making sex a subject of discussion. After that the safer sex part comes in. Our experience has shown that this is an effective way to train.
Safer sex 1
Dirty words
Objectives: 0 Participants discuss sex in order to
make them more comfortable with the subject.
A Making clear that different language is used for different people.
Duration of
exercise: 15 to 30 minutes
Number of
participants: Minimum 4, maximum 15
Material needed: Pens, paper, flip-chart Exercise outline:
• Give all participants a pen and paper and ask them to write down as many words possible for the male genitals; medical words, dirty words, pet names etc. (Allow 5 minutes).
• Write down the results on the flip chart. The person who came up with the most words is the 'winner'.
• Repeat this procedure; but with words for the female genitals.
• Discuss the results afterwards and ask participants which words can be used for different categories of people, e.g. parents, children, partner, peers.
Safer Sex 2 Sexual or not
Objective: Make participants conscious of the im-
pact different words can have on different people.
Duration of
exercise: 30 to 45 minutes
Number of
participants: Minimum 6, maximum 20
Material needed: List of words, participants sheet, pens.
Exercise outline:
• Preparation: Compose a list of words suitable for the group (see: example list below).
• Make copies of the participants sheets (see next page).
• Distribute participants sheets.
• Read out aloud the words on your list and ask participants to write them down in the columns which they think is right (no discussion).
• Split the group into two, or even more smaller groups, and ask participants to compare and discuss the results.
• In order to unite the group again, compose a list of words on which everybody agrees.
Example list of words
to hug exciting to lick
horny sucking to rub
security sensitive toys
kissing tenderness partner
warm tickle confidence
dick fuck dark
scratching surrender ecstasy
caressing smell sharing
safe hold tight
Write down the words mentioned in one of the columns.
(Copy sheet)
Sexual or not Participants sheet
SEXUAL
NOT SEXUAL SAFER SEX 2
Safer Sex 3 Sex education
Most people have not learned to speak freely about sex, and therefore, safer sex. It is vitally important to talk about safer sex because of HIV/AIDS. This exercise makes clear to everyone that it is 'normal' that we feel shy talking about sex. We have never been taught to do it. In this exercise the plenary discussion is limited in order to maintain privacy.
Objectives: 0 Introducing the issue of safer sex in a
non threatening way.
0 Making clear that most people's sex education was not very good and therefore it is valuable to discuss this subject.
Duration of
exercise: 15 to 30 minutes
Number
of participants: Minimum 6, maximum 21
Material needed: None
Exercise outline:
• Split the group into small groups of threes.
• Each participant in these smaller groups has a maximum of 3 minutes to tell the other two participants about their sex education. Key questions are: when did it happen, who did it, and what were you told?
• After participants have told their history, the general outcome is briefly discussed in a plenary session.
Safer Sex 4 0 Catalogue to what extent participants have knowledge of safer sex techniques and supply lacking information
Safe or not? A Raise awareness regarding the fact that safer sexual practices outnumber risky ones
Objectives:
Duration of exercise: 30 to 45 minutes Minimum 6, maximum 20
Number of participants: 3M post-it memo-blocs (the little yellow self-adhesive sheets)
Material needed: Pens
Exercise outline: 4 flip-chart sheets of a naked man and woman
1 flip-chart sheet with safe/unsafe
• Split up the group into two or more smaller groups.
• Supply each group with a post-it bloc, a pen and the instruction to write down as many as possible variations on making love (e.g. techniques, positions, acts) they can think of. One variation per sheet. Sheets should be stuck on the table for the time being. (Allow 10 minutes.)
• Stick the 4 prepared flip-chart sheets on the wall. On the flip-chart the naked front and back of a man and woman are pictured.
• The participants have 5 minutes to put the post-it sheets on the parts of the body where they think a certain variation belongs.
• Then stick the 5th flip-chart sheet on the wall. This sheet has to two columns: one with safe and the other with unsafe.
• Allow each participant to take some attached post-it memo's and read aloud the variation. The participant should then stick the sheet in the right column.
• To conclude, discuss the result and provide additional information if necessary.
Safer Sex 5 Merry go round
Objectives: 0 Participants experience talking about
intimate sexual subjects.
0 Participants experience posing intimate questions.
Duration of
exercise: 30 to 60 minutes
Number of
participants: Minimum 12, maximum 30.
Material needed: Cards with questions. Exercise outline:
• Preparation: Copy the questions on the following pages onto cardboard and cut into cards.
• Form an inner and outer circle with the group. Ensure that each circle has an equal number of people. Participants should sit in pairs, face to face.
• Give the people in the outer circle a pile of cards.
• The participants in the outer circle, ask a question from the cards to the person sitting opposite; but only if he/she would have answered the question him/herself. (Allow 5 minutes.)
• The outer circle moves two places and the procedure is repeated. (Allow 5 minutes.)
• Depending on the available time and the number of participants the procedure can be repeated again.
• The pairs change chairs (inner circle becomes outer circle).
• The new outer circle moves one place and the questioning starts again.
• Some experiences can be exchanged in a plenary session.
1. Do you think you are 'good' 2.Did you ever play 'doctors
in bed? and nurses or any other for-
bidden games?
3. Do you think there is a dif- 4. Do you talk occasionally ference between what men about your sexual experiand women experience dur- ences?
ing making love?
5. Do you communicate what 6. Have you ever been afraid you like to your partner when of your sexual feelings?
you are making love?
7. What does promiscuity 8. Do you feel that your ideas mean to you? about sex are further devel-
oped than your behaviour?
9. Do you have sexual 10. Have you ever wondered
dreams? how your parents make love?
And how your children make
love?
11. In a movie you see an 12. Do you sometimes pun-extended scene of homo- ish your partner by refusing sexual love making; what sex?
does that do to you?
(Copy sheet)
Questionnaire 1/5
13. Do you like to be touched, 14. What do you prefer: to SAFER SEX 5
caressed? tempt or to be tempted? (Copy sheet)
Questionnaire 2/5
15. Do you tell your children 16. Do you know what makes about your sexual feelings? you horny?
17. Do you fuck during you period? 18. Do you consider it a sign of weakness to look for help for a sexual problem?
19. Have you ever had a fight 20. What do you think about about sex? extra-marital relations?
21. Should people stay to- 22. What do pornographic gether for the 'sake of the photo-graphs and films to kids'? you?
23. Do you onlyfall in love with 24. Have you ever been people who are in love with afraid that you were homoyou? sexual?
• 25. Have you ever kept a relationship/affair secret from
• your parents and/or partner?
Training Courses 167
26. In what way do you like SAFER SEX 5
to be hugged most? (Copy sheet)
Questionnaire 3/5
27. Do you day dream a lot? 28. Do you like body fra-
grance?
29. Have you ever been 30. What was your most unafraid that you or your part- • pleasant sexual experience? ner was pregnant?
31. What do you think about 32. If your partner wanted oral sex? anal sex, would you do it?
33. Are you satisfied with • 34. Do you know and do you your 'sexual equipment'? like your partner's taste?
• 35. Do you 'checkout' good 36. If your partner had another looking people from the lover, how would you react? same sex?
37. How do you feel if a per- 38. Were you hugged a lot by SAFER SEX 5
son of the same sex feels at- your parents? Do you hug tracted to you? your children a lot?
39. Can you accept that your 40. Whatt do you think of the partner does not want sex taste of your partner's geniwithout feeling rejected? tals?
41. How often do you mas- 42. Can you show your affectu rbate? tion as well with your body as
with words?
43. Does somebody's voice 44. What do you think of vi-have asexual impact on you? brators and other sex-toys?
45. Do you get jealous eas- 46. What does the size of ily? your penis or your breasts
means to you?
47. Do you see your partner's 48. Do you ever go some-need for independence as a where to meet sex partners? rejection of their relationship
with you?
(Copy sheet)
Questionnaire 4/5
49. Tell something about your 50. Which sexual position do SAFER SEX 5
homo-sexual experiences? you prefer and why? (Copy sheet)
Questionnaire 5/5
51. Why do you fuck? 52. Do you think you are as
sexy as other people?
53. Where you desired as a 54. Have you ever felt ex-
baby and of the desired gen- ploited in a sexual relation-
der? ship and have you ever ex-
ploited someone?
55. Have you ever had sexually transmitted disease? 56. For men: Have you ever been to a prostitute?
For women: What do you think if your partner visited a prostitute?
57. Have you ever fucked 58. Have you ever pretended without contraception? that you were coming?
59. What fantasies do you 60. Do you masturbate occahave when you make love? sionally in your partner's
presence?
Safer Sex 6
Instructions for condom use
Objective:
Participants practice providing instructions on condom use and experience the obstacles that they can be confronted with.
30 to 45 minutes Minimum 4, maximum 16
Several dildo's (or other phallic objects) Different types of condoms.
Instructions for condom use.
Duration of exercise: Number of participants:
Material needed:
Exercise outline:
• Preparation: Photocopy the instructions for condom use on the following page.
• Split up the group into pairs and give each pair a condom and a dildo (or a dildo look alike).
• One participant teaches the other how to use a condom. (Allow 5 minutes).
• Bring the group together for an inventory of the reactions.
• Distribute the instructions for condom use and allow participants to read them carefully.
• The same pairs should sit together again, however this time the exercise is conducted the other way around, i.e. the other person with a new condom, provides a condom instruction lesson according to the recently read instructions. (Allow 5 minutes)
• To conclude, allow participants to respond to the instructions given and stress the obstacles one can face while demonstrating the use of condoms.
SAFER SEX 6
(Copy sheet)
Instructions for condom use 1/2
Instructions for condom use
• Check if you have the right condom:
— is it for vaginal, oral or anal sex; if you require it for anal sex, use only special, thicker condoms.
— is it big enough?
— is the brand registered and approved?
— check the expiry date.
• Open the package carefully:
— not with teeth or scissors. This will avoid tearing the condom.
• Take out the condom:
— be extra careful if you have long nails
— make sure you have the condom the right way up (i.e. not inside out).
• The tip (for semen reservoir), should be squeezed so that there is no air left
— this will decrease the chance of the condom tearing as the reservoir will not come under pressure
— if the condom has no tip make one yourself by squeezing the air out of the top of the condom (1-3 cm).
• Put the condom on top of the penis and unroll it carefully to the base of the penis
— wait until the penis is completely hard before putting the condom on
— when fully unrolled there is less chance that the condom will slip off again, be careful if you have long nails.
• Use only a water based lubricant
— always use lubricant for anal penetration
— a non water based lubricant will perish the condom. Do
not use Vaseline, hand cream, body lotion, oil or butter.
SAFER SEX 6
(Copy sheet)
Instructions for condom use 2/2
• Withdraw the penis carefully, immediately after ejaculating. While withdrawing, hold the condom at the base of the penis to avoid it slipping off
— if you wait too long before withdrawing the penis becomes soft, the con-dom slips off and the semen drips out.
• Tie a knot in the condom and dispose of it.
— Do not flush it down the toilet as condoms can block drain pipes.
Use a new condom each time you start fucking. Never use two condoms on top of one another: This can cause condoms to tear.
Safer Sex 7 Condom relay race
Objective: Participants practice in a 'gamesome'
way the use of condoms.
Duration of
exercise: 10 to 20 minutes
Number of
participants: Minimum 6, maximum 12
Material needed: Dildo's
Condoms,
Written instructions for condom use
Exercise outline:
• Instruct participants on how to use a condom.
• The written instructions are used as the 'Royal' standard, see copy sheet exercise 6.
• Split the group equally in half.
• Give each participant two condoms (one as a spare).
• Participants should stand in a line.
• The first person of each group is given a dildo and has to put the condom on it and take it off, in the proper way. Then the second person can start to do the same procedure.
• The group that finishes first is the 'winner'.
Remarks:
• The trainer can decide to appoint referees to judge the participants actions.
• If a participant makes a mistake he/she should start again.
• The 'winning' group should receive a small prize.
Safer Sex 8 The safer sex debate.
People use all kinds of pretexts for not using condoms. The aim of this exercise is to discuss the pretexts and provide valid counter arguments.
Objective: Discussing the 'pro's' and 'con's' of us-
ing condoms.
Duration of
exercise: 30 to 45 minutes
Number of
participants: Minimum 6, maximum 20
Material needed: Two case scenarios (see following
pages)
Exercise outline:
• Split the group into two; one group 'pro' condom use the other 'contra' (against) condom use.
• Each group is handed out the participants sheet (see following pages).
• The groups prepare their assignments. (Allow 10 minutes.)
• The group comes together again and sits face to face. The 'contra' condom group first provides reasons why people should use condoms. The 'pro' group is given the possibility to respond. The 'pros' and 'cons' are discussed in pairs as much as possible.
Write down the arguments for condom use and keep in mind that your partner will probably not agree with you.
Short stories PRO condom use
"You have been 'checking out' a gorgeous guy/girl for the past few weeks. Finally, you both have met and 'fallen in love'. After an EXITING night out you find yourself in bed wanting to fuck. You want to use a condom but you are not sure how to raise the subject. The last thing you want is to say is that you are HIV positive. Convince your partner to use a condom".
SAFER SEX 8
(Copy sheet)
The safer sex debate participants sheet 1/2
"You are having your period (it's the first day, so lots of blood). It is your last night in Amsterdam and your final chance for romance with the sexy man you met in the hotel. You know he has a history of drug use and a regular partner with high risk behaviour. It's 1.30 in the morning and you have only one hour before he has to return home to his fiancee. There are no condoms available. What do you do?"
"After months of heavy quarrels about money and drug use with your partner, the situation has become unbearable and you leave the house. You are lucky to find a place to sleep at one of your friends' houses. After being his guest for a week, he wants you to have sex with him in 'payment' for rent. When you are in bed with him it appears that he does not want to use a condom".
SAFER SEX 8
(Copy sheet)
The safer sex debate participants sheet 2/2
Write below the arguments against condom use and keep in mind that your 'partner' probably will not agree with you.
Short stories CONTRA condom use.
"You have been 'checking out' a gorgeous guy/girl for the past few weeks. Now you both have met and 'fallen in love'. After an exciting night out you find yourself in bed and wanting to fuck. You hate condoms and you are not going to use them because you are not HIV positive. Then your partner proposes using a condom. Explain why you don't want to use it".
"You and your girlfriend have been using drugs for the past 10 years. Your girlfriend works 'on the street' and is making enough money to supply both of you with drugs. She has kept you from becoming 'dope sick'. One night she suddenly says that she wants to use condoms. You are surprised because condoms are only for clients. You refuse. "
ORGANISATION EXERCISES
"Why should drug users organise themselves?" Drug users Introduction should organise themselves to defend their interests and in-
form policy makers and drug agencies of what they are. Too often drug users are treated as criminals, victims or mentally ill patients, instead of people with the same rights and responsibilities as 'non drug users'. The AIDS epidemic has demonstrated the importance of information to curb the spread of HIV. Taking preventative measures should recognise drug users as human beings and take into account a drug users' lifestyle. It is important for drug users to break the stereotypes and confront policy makers, drug workers etc. with a positive and combative attitude.
This manual only supplies a thumbnail of ideas about organising drug users for legal purposes and defending their own interests.
Organisation 1
Drug users' place in society
This exercise can be used as an introduction exercise in a training course with drug users. The exercise begins with 'brainstorming' the experience one has as a drug user. The second part, assesses people's opinion and can sometimes make people hesitant about coming forth with information. Our experience shows that in the beginning many associations are valued negatively, however this later develops into an awareness that is valued. Even negative terms such as 'dealer' have positive sides as well.
Objectives: O Orientation on drug users' place and image in society.
O Identify drug users awareness of the role and importance of drug related issue's.
Duration of
exercise: 30 to 60 minutes
Number of
participants: Minimum 4, maximum 20.
Material needed: Flip-chart
Marker pens
Exercise outline:
• The group brainstorms on associations with the word 'junkie': "What associations do you have on the word 'junkie'?"
• After having listed the groups associations, the trainer asks the group to value each association as positive or negative. Experience shows that it takes too long to work through the entire list. The trainer can choose some key association to work on.
• Continue with the associations until people are really aware that issue's which are valued negatively by society do have positive sides for drug users.
Remark:
• At the same time one is discussing drug users' place in society, one is reflecting drug users' self esteem.
Organisation 2a Inventory of problems
Organisation exercises 2a and 2b are in fact one exercise. They have been separated because experience has shown that it is best if some other exercises are done inbetween 2a and 2b. If possible spread the exercise over two days.
The exercises are basic self-organisation exercises. They aim to transform ordinary complaints into concrete actions to be undertaken by a self organisation. The work carried out in the frame work of this exercise provides concrete examples of the theory in chapter 2 of this manual.
This exercise is best to be done in combination with 2b.
Objectives: 0 Identifying all kinds of problems people
experience in day to day life.
0 Taking the first step towards expressing these needs.
Duration of
exercise: 15 to 25 minutes
Number of
participants: Minimum 4, maximum 20.
Material needed: Flip chart
Marker pens
Exercise outline:
• Simply ask participants to come up with all the kinds of problems drug users are confronted with in daily life. Write all problems and items mentioned down on the flip chart.
• Variation. Mention some big issue's in advance and use them as a guideline for the inventory of problems e.g. homelessness, price of drugs, substitution, HIV/AIDS, needle exchange etc.
Organisation 2b Working out the inventory
This exercise is best done in combination with exercise 2a.
Objectives: 0 Examine a particular problem.
0 Prepare steps towards solving the problem.
Duration of
exercise: 60 to 90 minutes
Number of
participants: Minimum 4, maximum 20.
Material
needed: Pens Paper
A table (to write).
Exercise outline:
• Preparation: The inventory (from exercise 2a), has resulted in a list of drug-related problems. Before continuing, problems of the same nature should be clustered. Make clusters which are comprehensive and down to earth. Also prepare an assignment for each cluster.
• Present the clusters with problems to the participants.
• Let participants vote for their cluster (try to balance the number of people in each cluster). For each cluster the trainer(s) has worked out an assignment. There are examples of clusters and assignments on the next page. We assume that if somebody votes for a specific cluster that he/she has something to contribute to this subject.
• The formed groups split to work out the assignments. Each group appoints a spokesperson.
• After 30 to 45 minutes of working on an assignment, the group is brought together again to present and discuss the results.
Variation:
The first part of this exercise (2b) involves the trainer(s) preparing the clusters.
• The clustering can also be carried in collaboration with the participants immediately after the inventory.
• Besides clustering the problems, an initial estimation of priorities can be made.
• The problem is assessed to see whether or not it should be tackled by a self organisation.
• And if 'yes' is the answer; Can a self-organisation do this alone, or does it need support from a sympathising organisation?
EXAMPLES OF CLUSTERS
with assignments
• Methadone
Design 5 basic 'rights and obligations' for clients of substitution programmes. Work-out a maximum of 5 steps to implement these rights and obligations at an existing programme.
• HIV-testing
Make a plan for a 'black book' about HIV testing in hospitals.
• A voice for drug users
Design a table of contents for the first two editions of a newsletter of a local drug user self-organisation. (Who will make the illustrations, who will write a guest-column). Think hard about who this newsletter is targeting, drug users, or non-drug users, or both?
• The attitude of drug workers
Design a training course for drug workers concerning 'street-life' and drug use.
Prepare the agenda for a meeting with the programme coordinator to discuss the course rules.
• Police harassment
Develop a strategy to make contact with the police chief without getting 'into trouble'. Prepare an agenda for the meeting.
• Accessibility to clean injecting equipment
Organise a public demonstration of how needle exchange occurs.
How do you obtain free needles? How do you organise drug users to come and exchange syringes? How do you inform the press? How do you plea for a greater variety of needles at the exchange programme?
Last Updated (Thursday, 06 January 2011 20:56)