| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 206 |
| Yesterday: | 251 |
| This Week: | 206 |
| Last Week: | 2221 |
| This Month: | 4794 |
| Last Month: | 6796 |
| Total: | 129393 |
Chapter Two: The Present Situation
 |
|  |
| 
| Reports - Drugs and the Law |
Drug Abuse
Chapter Two: The Present Situation
Introduction
1 It is nearly 30 years since the Misuse of Drugs Act was introduced. The purpose of this chapter is to describe the present situation and the main changes that have taken place in these three decades. The chapter reviews what is known about the scale and nature of drug use in the United Kingdom. It reviews the drug seizure and offender statistics, in terms of the numbers of drug offenders and how they are dealt with. Finally, it presents important new evidence from a survey specially commissioned by the Inquiry which explores public attitudes towards drugs in today's Britain.
2 A major change has been the steady increase in problem drug use. In the late 1960s there had certainly been a sharp increase in heroin use and addiction which had prompted various government enquiries prior to the 1971 Act. Even so, the difficulty was almost entirely confined to certain sections of London and involved not many more than 1,000 known addicts. By the mid 1980s there had been a significant increase in both the scale and geographical spread of problem drug use, and that trend has continued to the present.
3 An important feature of the last two decades has been the growth in injecting among problem drug users, particularly of heroin and amphetamines. This has given rise to major public and individual health problems, in particular HIV and more recently hepatitis C. From the mid-80s the HIV-risks of injecting drug use have given grounds for serious concern. The risks of an epidemic were starkly illustrated in Edinburgh where by 1988 the prevalence of HIV among injecting drug users was reported to be as high as 50%. A national strategy of harm reduction measures to curb the spread of HIV through injecting drug use was adopted and energetically pursued. A key component of the strategy was an increase in services, including needle exchanges and substitute prescribing.
4 There was a substantial fall in the proportion of problem drug users injecting, from 65% to 47% between 1989 and 1996. Currently HIV prevalence among injecting drug users in the United Kingdom is lower than in any other Western European country of similar size. However, the continuing increase in problem drug use and the current evidence of a slight growth in the proportion of those who inject underlines the need to sustain and increase such interventions. High levels of hepatitis C among problem drug users are a new and perplexing challenge.
5 Since the 1970s, and at an accelerating pace during the 1980s and 1990s, increasingly large numbers of people have been prosecuted under the MDA. The vast proportion of these have been for the simple possession of controlled drugs, particularly cannabis, rather than for offences of importation, production and supply. Since the 1980s there has also been a growing concern about drug-related crime, not just drug offences themselves, but acquisitive crimes such as burglary, shoplifting and robbery as well as violence surrounding the control of drug markets. These crimes have a grave impact both on the community and on the criminal justice system.
6 On some estimates, as much as one-third of all property crime in the United Kingdom is reckoned to be drug-related - particularly to heroin and cocaine. Pilot studies which test for drug use among people arrested for a variety of offences show that in some areas between one-fifth and one-third tested positive for opiates, and one-quarter tested positive for cocaine [1]. These consequences of problem drug use were simply unknown thirty years ago.
7 An equally striking change is that a much larger section of the population is familiar with the more commonly used illicit drugs, such as cannabis and amphetamines. The majority of people do not use illicit drugs and, of those who do, most do not do so regularly and frequently. Nevertheless, familiarity and experimentation with drugs has become much more commonplace, involving important changes in attitudes and experience.
8 Well past the 1960s illicit drug use remained a minority pursuit. By the late 1990s surveys consistently show that a majority of young people between 16 and 29 years admit to having tried illicit drugs. As many as one-quarter to one-third of this group might have used cannabis and other drugs on a casual basis within the last year or last month.
9 A major cultural shift in attitudes to drugs and their use has occurred in the United Kingdom over the past 30 years. Social attitudes towards drug use have become more nuanced and sophisticated, not only among the young. The survey conducted for us by MORI shows that among adults aged 16-59 twice as many as not regard cannabis as less harmful than alcohol - but the great majority do regard heroin, cocaine, ecstasy and tobacco as particularly harmful. Perhaps surprisingly in terms of common stereotypes, there is no evidence of a generation gap in these matters. If anything, more people aged 45-59 years saw cannabis as less harmful than alcohol than did those aged 16-24.
10 Taken together, the changes in the scale of drug-related problems, much wider familiarity with some forms of illicit drug use, and social attitudes which no longer lump all drugs together, provide the context for our examination of current illicit drug use and efforts at its control.
Scale and nature of drug use
11 A picture of drug misuse and the law’s response can only be put together by looking at information from several sources. These include the Home Office statistics of people notified by doctors as addicts, the Department of Health statistics from the regional drug misuse databases of people who begin attending drug treatment services, and information from national and regional surveys of self-reported drug use. The annual Home Office Statistics of Drugs Seizures and Offenders Dealt With is also an important information source. Several of these sources have significant limitations, which we note at the appropriate points. Often this means that the figures from some sources must be regarded as indications of trends rather than actual numbers.
The Addicts Index
12 From 1968 until April 1997 doctors had a statutory duty to notify the Home Office of patients who, in their judgement, were addicted to one or more of a number of Class A drugs, including cocaine, heroin and methadone. The annual statistics of this Addicts Index identified separately the number of addicts who had been notified for the first time and those who had been notified previously. But the numbers were serious understatements of the true position because many addicts did not seek treatment, and many of those who did were not notified by their doctors.
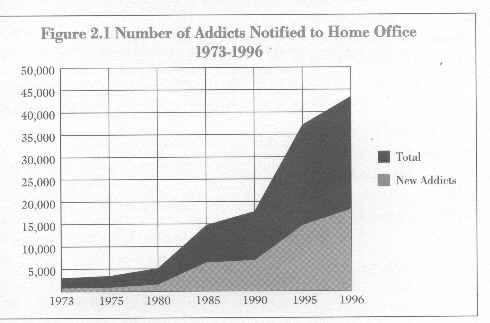
13 Between 1973 and 1996 the total number of new and renotified addicts increased by over 1000%, from 3,022 to 43,372, with the number of new addicts increasing by 2000%. Between 1974 and 1996 the number of notified heroin addicts increased by almost 2000% (from 607 to 15,271). Local studies over the years have led to general agreement that the real number of addicts was between two and five times the number notified, the true figure in the mid-to-late 1990s was probably between 100,000 and 250,000 addicts in the UK.
Figure 2.1 Number of Addicts Notified to Home Office 1973-1996
The regional drug misuse databases
14 Since 1993 the Department of Health has published six-monthly statistics of problem drug users. These are figures of people reported by drug treatment agencies to regional drug misuse databases in Great Britain as beginning attendance at a treatment agency or returning after a break of six months or more. However, the information is seriously defective. There is no legal requirement for treatment agencies to report, and those who seek treatment for the first time are not separately identified. There is no certainty that all problem drug users who attend agencies are included in the databases or that there is no double counting between agencies. Because of the time lag in their production, the statistics cannot provide early warning of new local outbreaks of problem drug use. Since, however, doctors are no longer required to notify their addict patients, these statistics now provide the best available indicators of the extent, pattern and nature of heroin and other problem drug use in Great Britain.
15 What the regional drug misuse databases appear to tell us is that between 1993 and 1998 the number of people seeking help increased from approximately 20,000 to 35,000. In this same period, males consistently outnumbered females by 3 to 1. Slightly more than one-half were aged 20 to 29 years, with roughly one in six aged 19 years or younger. The remainder, slightly less than one-third, were aged 30 years or more. The proportion saying heroin was their main drug of misuse rose from 43% to 56%.
National and regional surveys
16 There is no systematic national survey evidence of self-reported drug use for the period to compare with the Addicts Index and its evidence of steady increases in heroin addiction and other forms of problem drug use since the early 1980s. This is because surveys of this kind are largely a phenomenon of the 1990s.
17 Such surveys have their critics who point to their unreliability: sample sizes vary, and are generally too small to measure meaningful changes; despite reassurances of confidentiality, respondents may conceal or exaggerate their drug taking, or they may be less willing to admit to the use of more stigmatised drugs such as heroin and cocaine. Furthermore, surveys tend to ask 'Have you ever used a drug?’ which is not a sound indicator of current behaviour. The important issues are whether people are using drugs regularly, and if so how often and how recently.
18 All these are reasonable objections, and certainly such surveys are unlikely to capture highly problematic drug users with chaotic lifestyles, homeless, or in institutions. Even so, such surveys show a great deal of consistency and tell us something about current patterns of drug use in the United Kingdom.
19 The first survey in England and Wales to inquire about the use of particular drugs was in 1969 [2], and offers a broad brush-stroke comparison with the 1990s. Four per cent of respondents (aged 16-69 years) said that they had used amphetamine at some point in their lives, 2 per cent had used cannabis, and less than half a per cent mentioned the use of any other drugs. Comparable figures from the 1998 British Crime Survey (BCS) of people aged 16-59 years are 32 per cent saying that they had ever used any drug, including 10 per cent saying that they had ever used amphetamine, and 25 per cent saying that they had ever used cannabis.
20 The 1994, 1996 and 1998 BCS [5] all found that around twice as many people admit to having ever taken drugs as admit to taking them in the last year. This suggests that much drug use is experimental, although people may be more willing to say they have taken drugs on an occasional basis a long time ago.
21 If we look only at those who admit that they had taken drugs in the last year or month, better indicators of regular use, we find little change between 1994 and 1998 as the figures below show.
Table 2.1 British Crime Surveys: people who said they had taken any drug last year and last month. Percentages of age groups.Aged: 16 to 59 16 to 29
---------------------------------------------
1994
Last year 10 23
Last month 6 14
---------------------------------------------
1996
Last year 10 24
Last month 6 15
---------------------------------------------
1998
Last year 11 25
Last month 6 16
---------------------------------------------
22 Cannabis is by far the drug most likely to have been used either last year or in the last month. Using the 1998 BCS figures it is estimated that almost two and a half million 16-29 year olds in England and Wales had taken cannabis last year, and one and a half million had done so last month - that is, almost one-third of the sample said they had used it in the last year and one in five in the last month. Half of those who admitted taking any drug last year said they had used cannabis only. The other half had used cannabis as well as other drugs, or other drugs only.
23 BCS data regularly show that only a very small percentage - one per cent or less - admit to using heroin or crack cocaine. There is some indication of an increase of powder cocaine use during the 1990s, although among younger people amphetamine remains by far the most popular drug after cannabis. The 1998 BCS reports 5% of 16-29 year olds saying that they used it in the last month, and 8% in the last year.
24 16 to 19 year olds are the age group most likely to say they take 'hallucinants' (amphetamines, ecstasy, LSD, magic mushrooms and amyl nitrite). The proportion in this age group taking any of these drugs in the last year dropped between the 1994 and 1998 BCS from 18% to 12%.
25 The findings of the 1993 and 1996 Scottish Crime Surveys [4] are broadly similar to those of the BCS, with cannabis the drug of choice. The Northern Ireland Crime Survey [5] of 1994/95 indicates far lower levels of drug use, with only 5 % of the total sample admitting to the use of cannabis, again the most popular drug by far. A recent study of ecstasy use in Northern Ireland [6] does point to pockets of much higher levels of illicit drug use - reflecting the wide regional variations in levels of use evident elsewhere in the United Kingdom.
26 The only regularly collected information on drug use by 11 to 15 year-old schoolchildren comes from the annual surveys on health behaviours carried out by the Schools Health Education Unit [7]. These surveys are useful although not nationally representative. The surveys from 1990 to 1997 found that one in ten of the 11-13 year-olds sampled said that they had ever taken drugs. Of the 14-15 year- olds, a third said that they had ever taken drugs in 1995 and 1996; this fell to a quarter in 1997 and 1998. The nationally representative 1998 figures from the Office of National Statistics show the first downturn in the number of schoolchildren ever having used a drug [8]. At the other end of the educational spectrum, a national survey of second year university students in 1995 [9] found that 20% said that they were regular (i.e. at least once a week) cannabis users. 4% said that they used amphetamines regularly and 3% ecstasy. Less than one per cent said that they used any other drug.
27 The heaviest drug users and those with serious problems are unlikely to be found by household or school surveys. A new source of trends in high-risk groups is provided by those surveys of people held in police custody for a variety of offences. These combine voluntary and confidential urine testing of arrestees with interviews on drug use. This is a method used in the United States for more than ten years. In a pilot study begun in 1996/97, a sample of arrestees in five police areas in England agreed to provide urine samples for drug testing [10]. The urine tests showed that 61% had taken at least one drug. Cannabis was the drug most likely to be found. It occurred in the tests of 54% of the 16 to 20 year-olds, 47% of those aged 21 to 30, and 37% of those aged 31 and older. The 21 to 30 year-olds were most likely to test positive for opiates (26%), cocaine (14%), amphetamine (14%) and benzodiazepines (15%). These proportions are very much higher than those found for the most comparable age groups in the 1998 BCS. There were also some sharp regional variations.
European comparisons
28 International comparisons are difficult to make because different countries use different survey methods, track different drugs and define age groups differently. The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) brings together the available information in their annual reports on the state of the drugs problem in the European Union. Unfortunately they have been unable to establish true comparability in the face of the national variations in collecting statistics.
29 There are, however, some comparable figures for the proportions of young adults taking drugs in the last year. See Table 2.2, below. The figures derive from surveys conducted in 1995 or 1996 [11]. Although care must be taken in drawing inferences from this information as the age ranges are dissimilar, they do offer some indication of comparative use between countries.
Table 2.2 Last 12 months' prevalence of drug use in recent nationwide surveys among the general population in some EU countries
Country Age range Cannabis Cocaine Amphetamines Ecstasy
---------------------------------------------------------------------
Belgium 18 - 39 2.7% 0.5% 0.7% 0.5%
(Flanders)
---------------------------------------------------------------------
Germany 18 - 39 8.8% 1.6% 1.5% 1.6%
(former West)
---------------------------------------------------------------------
Spain 15 - 39 11.6% 3.2% 1.7% 2.2%
---------------------------------------------------------------------
France 18 - 39 8.9% 0.3% 0.6% --
---------------------------------------------------------------------
Finland 16 - 34 5.2% -- -- --
---------------------------------------------------------------------
Sweden 15 - 34 1% [1]
---------------------------------------------------------------------
United 16-29 21% 1% 8% 4%
Kingdom
----------------------------------------------------------------------
Note 1. All illegal drugs
30 Surveys of schoolchildren aged 15 or 16 were carried out in most EU countries between 1995 and 1997 [12]. These surveys asked respondents if they had ever taken drugs. The highest proportions of those who had used cannabis, over 30%, were found in the United Kingdom, Ireland and the Netherlands. The lowest, less than 10%, in Luxembourg, Finland, Sweden and Portugal. The United Kingdom also had the highest proportion who had used solvents, amphetamines and LSD, and with Ireland and the Netherlands it had the highest proportions who had used ecstasy.
Drug-related deaths
31 Deaths resulting from the use of controlled drugs are obviously a matter of social importance, and also attract a great deal of publicity when they occur. Regrettably, the available public information on drug-related deaths mainly coroners' statistics are notoriously difficult to interpret, since coroners might not always know or record whether controlled drugs are involved. Nor do figures record deaths from conditions associated with injecting drug misuse. A working group of the Advisory Council on the Misuse of Drugs has been examining the whole subject of drug-related deaths, including the collection of more reliable and complete statistics, and will report during 2000.
32 In the meantime, it is only possible to say that recorded drug-related deaths have undoubtedly risen since the early 1980s, and that these are mainly resulting from the use of heroin, methadone and other opiates. In England and Wales recorded deaths associated with drug dependence, non-dependent abuse, or poisoning by controlled drugs rose from about 1,800 to 2,100 between 1979 and 1997 [13].
Seizures, prices and purity of controlled drugs
33 The purpose of seizures of drugs together with related law enforcement activity is to disrupt the illicit drugs market. To see whether this has been successful, we looked for evidence of a decrease in the availability of drugs, increases in prices, and reductions in purity.
34 The number, type and quantity of seizures varies from year to year with the resources and activities of the enforcement agencies as well as the traffickers. In 1997, the number of seizures of controlled drugs by HM Customs and the police, at 139,174, was the highest ever recorded, and over twice the 1990 number.
35 The number of heroin seizures more than doubled between 1990 and 1995, and almost doubled again to over 12,000 in 1997. The quantity seized almost quadrupled to 2,200 kgs. in 1997. Between 1990 and 1997 the number of seizures of powdered and crack cocaine rose from 1,805 to 5,432, with the quantity seized quadrupling to 2,350 kgs. There were also increases both in the number of seizures and in the quantities seized of amphetamines and cannabis. However, there were fewer seizures of LSD, and smaller quantities of this substance seized. After the dramatic increase in the number of seizures of ecstasy-type drugs between 1990 and 1996, rising from 399 to 6,211 (with the number of doses seized increasing from 44,000 to almost six million) there was a drop to 5,087 seizures in 1997 (with two million doses seized).
36 Cannabis accounted for much the largest number of seizures and quantity of any drug seized. It was involved in 87% of seizures in 1990 and 77% in 1997, with the weight seized increasing nearly fivefold to 150,000kg. The number of cannabis plants seized increased from 34,299 to 114,988, virtually all seized by the police.
37 A report by the National Audit Office [14] noted that the street prices of most types of drugs have shown a flat or falling trend over the period 1990 to 1997/98. Information supplied by Europol suggested that in April 1998 the street price of many drugs was higher in the United Kingdom than in Germany and the Netherlands.
38 Average purities of drug seizures analysed by the Forensic Science Service show fluctuations. The average purities of police seizures of heroin between 1990 and 1997 showed, with small annual fluctuations, that purity decreased slightly between 1990 and 1997. During the same period the purity of cocaine had increased.
39 The 1999 EMCDDA annual report on the state of the drugs problem in the European Union [15] says that cannabis prices appear to be stable. On heroin it says '‘The general impression is of price stability after a decrease in previous years’ except in Italy where the price is believed to have risen. Much the same report is given for cocaine, with the addition that 'the overall picture is of an expanding market with increased availability'. Prices are said to have decreased for amphetamines and ecstasy.
40 In summary, we found little evidence to indicate that enforcement efforts have led to increased prices, decreased availability or decreased purity.
Drug offenders
41 People arrested for offences may be dealt with in a variety of ways. They may be prosecuted or, in England and Wales and Northern Ireland but not in Scotland, the police may formally caution them. In Scotland procurator fiscals have two options for dealing with offenders in lieu of prosecution. They can issue written warnings and may make a conditional offer of a fixed penalty known as a fiscal fine. Under the Customs and Excise Management Act 1979 (CEMA), H.M. Customs and Excise may offer compounding (the payment of a monetary sum in lieu of prosecution) to people attempting to import small quantities (10 grams or less) of cannabis. The police or prosecuting authority may, as an alternative to any of these responses, decide to take no further action. Such cases do not appear in the criminal statistics.
42 Since 1974, the first full year of operation of the Misuse of Drugs Act 1971, the number of offenders against the MDA found guilty, cautioned, given a fiscal fine or dealt with by compounding has risen steadily from 11,811 to 111,384 in 1997, an almost tenfold increase. If offenders against related legislation (mainly CEMA) are taken into account, the scale of the increase is similar since 1974, from 12,532 to 113,154.
43 The great majority of persons dealt with for drug offences are dealt with for possession offences (89% in both 1974 and 1997). In contrast only 16% of drugs offenders dealt with in 1997 were found guilty or cautioned for trafficking offences (defined in the Drug Offences Act 1994 as including importation, production, supply and possession with intent to supply). It should be noted that production figures since 1995 include cases of cultivation of cannabis.
44 Cannabis dominates possession offences, and cannabis possession dominates all offences against the MDA. Since the early 1970s over three-quarters of all possession offences have consistently involved cannabis. Cannabis possession has accounted for between 70% and 85% of all offences against the MDA.
Figure 2.2 Relationship of Cannabis Offenders to Total Drug Offenders, 1985-1997
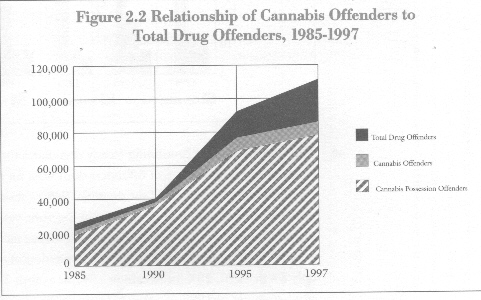
45 If the vast majority of offenders are dealt with for offences involving cannabis, amphetamine is next most frequently involved, 12% in 1974 and 1997; followed by heroin, 4% in 1974 and 8% in 1997; and cocaine, 3% in 1974 and 1997. In 1990 1% were dealt with for offences involving ecstasy, and 4% in 1997 for offences involving ecstasy-type drugs.
46 Most people dealt with for drug offences are male, around 90% in each year. The average age of offenders has remained constant at 25. In 1997 6% were aged under 17, doubling since 1974, and about 25% between 17 and 20 years.
How drug offenders are dealt with
47 The ways that drug offenders are dealt with, and in what numbers and proportions, arc set out in Table 2.3. In overall numbers, there has been a four-fold increase between 1985 and 1997. The number of offenders receiving fines has doubled, as has the number sentenced to immediate custody. The number receiving community sentences has increased four-fold in the same period, while the number receiving cautions has increased sixteen-fold.
48 The trend revealed in Figure 2.3 is of a massive increase in the proportion of offenders cautioned. These now account for half of all offenders dealt with. This has been matched by a sustained decrease in the proportion fined. By contrast, the proportion imprisoned or receiving community sentences has remained relatively stable, with some year-on-year variations.
Figure 2.3 How Drug Offenders Were Dealt With, 1974-1997. Percentages
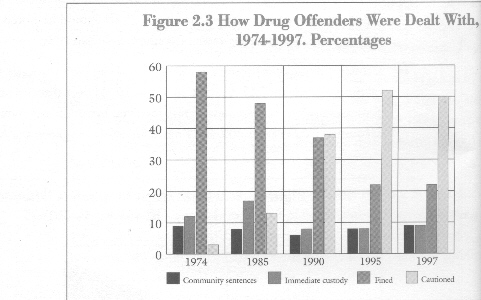
49 The increased use of cautioning clearly dominates the picture. This is largely a result of a preponderance of offenders dealt with for the possession of drugs, especially cannabis. In 1997 for example, 96% of those cautioned for drug offences involved the possession of drugs, and in the same year 58% of those dealt with for cannabis possession were cautioned. Cautions are increasingly used in cases of possession of other drugs: 26% for the possession of cocaine in 1997 as against only 8% in 1990; 23% for heroin in 1997 as against 7 % in 1990; and 33% for amphetamines in 1997 as against 10% in 1990.
Table 2.3 How drug offenders were dealt with [1] in the United Kingdom 1974 to 1997. Numbers and percentages.
1974 1985 1990 1995 1997
Cautioned 394( 3%) 3,624(13%) 17,025(38%) 48,824(52%) 56,156(50%)
Dealt with by - 362( 1%) 1,184(3%) 668( 1%) 547(*)
compounding
Fiscal fine - - - - 484(*)
Immediate custody [2] 1,531(12%) 4,535(17%) 3,402( 8%) 7,086( 8%) 10,422(9%)
Fined 7,276(58%) 12,985(48%) 16,437(37%) 20,867(22%) 24,421(22%)
Community sentence [3] 1,068(9%) 2,219(8%) 2,693(6%) 7,780( 8%) 9,907(9%)
Absolute/Conditional 1,261(10%) 1,711(6%) 2,558(6%) 6,036(6%) 7,311(6%)
discharge
Otherwise dealt with 1,001( 8%) 1,522( 6%) 1,623(4%) 2,370( 3%) 3,308(3%)
Total [4] 12,532 26,958 44,922 93,631 113,154
(*) less than 1%
Notes:
1. When a person is found guilty of two or mote drug offences at the some
court appearance, the sentence or order shown is the most severe penalty.
2. Includes unsuspended imprisonment, partly suspended imprisonment and
youth sentences.
3. Includes Combination Orders (since 1993), Community Service Orders,
Probation and Supervision Orders.
4. There are small errors in the published totals for 1974 and 1997.
Source: Home Office
50 The use of cautions declines rapidly for the most serious offences. Even so, it remains an option that is sometimes employed over the whole range of offences. In 1997 25% of those dealt with for production offences (which includes the cultivation of cannabis) were cautioned, 10% for supply and 6% for possession with intent to supply unlawfully.
51 Where these more serious drug trafficking offences are concerned. involving importation or supply, offenders are most likely to be brought before the courts and to be subject to more severe penalties, including imprisonment. The percentage of drug offenders in the prison population has increased substantially - from 9% (3,417 out of 34,754) of the sentenced prison population in England and Wales on 30 June 1990, to 15% ( 7,174 out of 48,674) by the same date in 1997. The length of prison sentences for importation and supply offences has increased during the 1990s, whereas for other offences it has remained stable.
52 It is important to note, however, that in each year since 1990 over 80% of those found guilty of drug offences were sentenced for possession. Moreover, in terms of the sentencing options available to the courts, the fine remains by far the most commonly used penalty, in spite of its overall decline. In 1997 it still accounted for almost half of all sentences passed by courts for drug offences. In the same year, one-fifth received sentences of immediate imprisonment, the same proportion received community sentences, and the remainder (14%) received conditional or absolute discharges.
53 We should note two other ways of dealing with drug offences: the use (since 1995) of fiscal fines in Scotland and compounding by HM Customs and Excise (see paragraph 41 above). In 1997, the first year for which figures for fiscal fines are available, 499 were accepted, 432 for the possession of cannabis, 60 for the possession of other drugs and 7 for other offences. The percentage of customs cases involving cannabis in which compounding was used increased from 20% in 1985 to 48% in 1990, but has since fallen back to 31% in 1997.
54 In conclusion, the history of sentencing and penalties associated with drug offences is dominated by two features. First the increasing number of offenders, and second a marked trend over the years towards the use of less formal sanctions and penalties. In particular, the caution is used more, diverting offenders away from the courts.
Public attitudes
55 As part of our work, we felt that it was important to try and learn something about public attitudes towards drugs, the harms associated with them, and the role of the law. A survey was commissioned from MORI which provided some surprising responses and proved particularly revealing about attitudes towards drugs in contemporary Britain.
56 The surveys were conducted among adults and school students, and asked a range of questions concerning the perceived harmfulness of different drugs. The adult survey involved face-to-face interviews with 1,645 people aged 16 to 59 years between 9 - 13 April 1999. The schools survey was conducted between 18 January and 12 February 1999, and collected completed questionnaires from 3,529 pupils aged 11-16 years.
57 One key question was how people assessed the relative harmfulness of different drugs. Where adults were concerned, substantial majorities of 90 per cent or so across all age ranges - from 16 to 59 years, judged heroin, cocaine, ecstasy and amphetamines to be either very or fairly harmful. By contrast, only one-third judged cannabis to be as harmful, and again this judgement hardly varied with age. Attitudes tended to vary with age where alcohol and tobacco were concerned, with a marked tendency to see these substances as increasingly harmful with increasing age. Among adults from 18 to 59 years, cannabis was seen as by far the least harmful of all these drugs.
Figure 2.4 Ranking of drugs as very or fairly harmful by 16-59 year olds. Percentages.
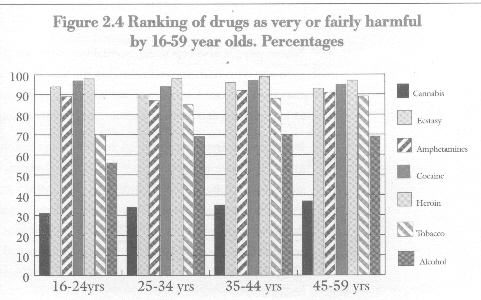
58 Public attitudes, therefore, do not lump all drugs together, but adopt a more considered view of the harmfulness of different substances; a view, moreover, which tends to conform with medical and scientific opinion (see Chapter Three, paragraphs 23 and 24). The one exception to this is that people judge ecstasy to be almost as harmful as heroin and cocaine, whereas scientific opinion tends to judge ecstasy as considerably less harmful.
59 In the schools survey, attitudes towards the perceived harmfulness of drugs were different in important ways. Children aged 11 - 12 years offered a much simpler testimony, seeing all illicit drugs (including cannabis) as more or less equally harmful. In contrast, 11 to 12 year-olds see alcohol and tobacco as relatively much less harmful, and this view does not change with age among 11-16 year-olds. Attitudes towards cannabis change considerably as young people grow older - so that by age 15-16 years they see cannabis in the same way as adults, that is as among the least harmful of drugs.
Figure 2.5 Ranking of drugs as very or fairly harmful by 11-16 year olds. Percentages.
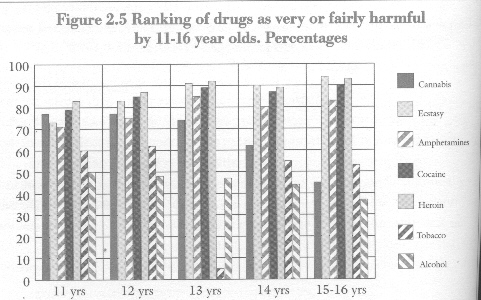
60 Young people also reported increasingly with age that they knew someone of their own age who had smoked cannabis. By age 15-16 years, only about one in ten said that they did not know someone who had used cannabis. Young people of all ages, as with adults, see heroin, cocaine, amphetamines and ecstasy as very harmful.
61 Between the ages of 11 and 16 years the perceptions of children as they grow older gradually move to approximate the views of adults. The exception is attitude to alcohol and tobacco: only adults see these substances as particularly harmful. The most frequent reasons given by both children and adults for people not taking drugs were 'health reason' (33% and 51%) and 'just don't want to take drugs’ (27% and 56%). By comparison only 19% of children and 30% of adults mentioned 'illegality' and 12% of children and 17% of adults cited 'fear of being caught by the police'.
62 People did nevertheless want to see strong and effective drug laws. Two-thirds of adults thought that the law against drugs 'is not tough enough', and tended not to agree that the use of drugs was merely a matter of personal choice. Once again, views differed sharply between different drugs. Whereas two-thirds expressed the view that drug laws should be tougher, approximately one-half of all adults felt that the law should be changed so that the use of cannabis was no longer illegal. In the schools survey a higher number of children and young people said that fear of being caught by their parents (21%) was more of an influence than fear of being caught by the police. The latter view was held a little more strongly among younger age groups, although in all age groups a clear majority of those who expressed a view felt that the law with regard to cannabis should be changed.
63 The MORI survey evidence suggests that people view the health consequences of drug use as a more important deterrent than legal controls. They do want strong and effective drug controls, but do not believe that the police alone can be effective in curbing the damage caused by drug misuse. When asked to state what priority the police should give to a variety of different offences, heroin dealing and sexual assaults were seen as by far the most important. They were mentioned by two-thirds of respondents. Assault, racial violence and drink-driving were mentioned by one-third, with burglary and muggings mentioned by one in five. At the lower end of the spectrum heroin users (as opposed to dealers) were mentioned by only 8%, and cannabis dealers by 9%. Cannabis users, on the other hand, were hardly mentioned at all as a police priority - by less than half of one per cent of respondents.
Table 2.4 Which three of the following do you think should be the highest priority for the police? Percentages.
Sexual assaults 71
Dealers who sell heroin 66
Assault 32
Racial violence 32
Drink-driving 32
Burglary 22
Mugging 17
Dealers who sell cannabis 8
Heroin users 8
Vehicle theft 4
Cannabis users 0.5
64 It is clear on this evidence that cannabis stands out as a special case in public attitudes towards drugs in modern Britain. It is seen by adults as by far the least harmful of all drugs, including alcohol and tobacco. The possession of cannabis is seen as the very lowest of priorities for the allocation of police resources. A majority of adults, young and old, even feel that its use should be legalised. Where other drugs are concerned, public opinion fully supports strong drug laws, while emphasising concern with the health risks resulting from drug use. We were particularly impressed by the uniformity of these attitudes towards cannabis and other drugs across different social groups and age groups. Perhaps most surprisingly in terms of the way in which public debate is often constructed, there was no evidence of a 'generation gap' in public attitudes towards the use of cannabis.
65 This last point perhaps indicates as well as anything how far public attitudes towards drug use may have changed in the past thirty years. Unfortunately, there are no directly similar surveys from the past to compare with our own findings. The MORI poll which we commissioned is undoubtedly the most comprehensive survey of its type to be as yet conducted in Britain. Even so, we can offer some idea of how attitudes seem to have changed on some questions, although unfortunately most of these relate only to the legal status of cannabis.
66 Since 1969 surveys of representative samples of the adult population have shown an increasing proportion agreeing with variations on the statement 'Cannabis should be legalised’, rising from one in eight in 1969 to one in three in 1997. In the 1990s between 50% and 60% of people who responded to questionnaires in magazines aimed at the young adult market or broadcast by radio stations agreed that cannabis should be 'legalised' or 'decriminalised'. Surveys of chief constables, doctors and Members of Parliament have also found substantial minorities agreeing that the controls on cannabis were too harsh or should be relaxed [16] .
67 Our survey therefore falls broadly into line with these others, indicating that while cannabis is seen as one of the least harmful of all drugs, other drugs such as heroin, cocaine, amphetamine or ecstasy are seen differently. Earlier surveys have also shown that the public response to cannabis is markedly different than towards other drugs. A 1995 survey [17], for example, asked 'which drug, if any, that you may not take yourself do you feel its acceptable for others to take if they wish to?’ Apart from alcohol and tobacco, cannabis was the most acceptable drug to all age groups, to 40% of 16-19 year-olds, 47% of 20-24 year-olds, 36% of 25-34 year-olds, 25% of 35-54 year-olds. Among 16 to 19 year-olds, the dance drugs, amphetamines (17%), LSD (15%) and ecstasy (12%) were the next most acceptable drugs. In 1998, a similar survey [18] found that among people aged 18-34 years 50% agreed that 'using cannabis is no worse than smoking or drinking' compared with 29% of those aged 35 years and older.
68 In conclusion, earlier surveys have found increasing levels of acceptance of illegal drug use, but restricted almost entirely to the use of cannabis. These surveys invariably find that younger people are more tolerant towards cannabis use. Where our own survey is concerned, although there was undoubtedly less strong support for legal change among older age groups, when asked about the comparative harmfulness of different drugs these age differences all but disappeared.
Conclusions
69 All the indicators point to a steep increase in the number of drug users in the United Kingdom since 1973 when the Misuse of Drugs Act 1971 came into force, although the extent of the increase varies between regions and countries. In particular, there has been a substantial rise in the number of problem drug users, especially of heroin users. Since 1990 the largest increase in problem drug users has occurred amongst those aged under 21. Despite the weaknesses of the data, they are meaningful. They represent the minimum extent of a type of drug use whose harm to the individual and society is definable.
70 The nationally representative self-report surveys indicate there has also been a substantial increase in the number of casual drug users. The use of cannabis dominates the figures, followed by amphetamines. Important additional information from local studies, especially longitudinal studies, shows how the picture of use is changing ahead of national indicators. These surveys indicate that, while cannabis predominates, its use in combination with other drugs (ecstasy, amphetamines, LSD) is not uncommon.
71 The big divide in drug use is between those under and over 30 years old. Although the onset of use occurs between the ages of 15 and 16, the indicators suggest that the majority of these users are casual drug users who do not go on to become problem drug users. The social profile for the casual drug user is different from that of the problem drug user and shows no significant correlation with deprivation. Early use in combination with deprivation remain the strongest indicators of progression to problem use. However, we do not yet know the implications for adult drug use of the large increase in casual use, especially of stimulants, by young people in the 1990s.
72 It is not surprising that the prevalence of use is mirrored in the statistics on drug seizures and offending against the MDA. Since the first full year of operation of the Misuse of Drugs Act 1971 in 1974 the number of offenders against the MDA and related legislation has risen steadily, more than a nine-fold increase. The number of seizures by enforcement agencies and the amounts seized of heroin, cocaine, amphetamines, cannabis and ecstasy have significantly, indeed in some cases dramatically, increased since 1990. Nonetheless the scale of availability as implied by the prevalence of use, especially when set against the reported stability in prices on the street, makes it difficult to avoid the conclusion that efforts to choke off supply have largely failed.
73 The evidence on sentencing indicates that the courts view trafficking offences such as importation, production and supply as serious crimes. However, it seems to be indisputable that enforcement resources are chiefly taken up with possession offences, especially cannabis possession. Even though the decisions by the police, Customs and Excise and the courts to use cautions, compounding and fines reflects more realistically the relatively minor seriousness of these offences, this concentration of effort appears out of line with the attitudes of a significant portion of the public. The findings from our own and previous surveys seem clear: there is majority support for a firm law on drugs alongside substantial and increasing minority support (a third to a half) for relaxation of the law on cannabis. Our own survey indicates that the public's highest priority for enforcement is trafficking in the seriously addictive drugs such as heroin rather than offences reflecting personal use, especially but not exclusively of cannabis.
74 The government's 10-year drug strategy adopted in 1997 urges that resources should be focused on those drugs that do the greatest damage. Indeed, it is the combination of the most dangerous drugs - principally heroin and crack-cocaine -and the forces of social exclusion that provide the greatest challenge to combating drug misuse in Britain in the new millennium. In a recent report the Advisory Council on the Misuse of Drugs observed that:
'We thus assert without any of the familiar hedging with "on the one hand but on the other", that on strong balance of probability deprivation is today in Britain likely often to make a significant causal contribution to the cause, complication and intractability of damaging kinds of drug misuse... We want now and in the future to see deprivation given its full and proper place in all considerations of drug prevention policy, held in that policy consciousness, and not let slip from sight' [19]
We believe this to be an important conclusion, and stress that tackling problem drug use must always also involve tackling social deprivation.
75 The flaws and gaps in the information and research base necessary to investigate adequately the extent of drug use and its control are striking. Since doctors are no longer required to notify their addict patients the national data on the scale and changes in problem drug use over time are arguably less adequate than they were. Procedures for mapping local variations in drug use are seriously wanting. Available information provides little insight into how drug use behaviours are formed or changed, or on the pathways from casual to problem use. A commitment to longitudinal studies is needed.
76 Equally striking is the relative absence of detailed cost information about drug use. From our investigations estimates of drug related healthcare, enforcement and other social service costs appear rudimentary. Such information, together with the results of systematic evaluations of prevention, treatment and control initiatives, would facilitate a realistic assessment of drug control and prevention strategies. None of the attitude surveys throw any light on the influence, if any, of the law in controlling illicit drug use. The impact of the law may appear disappointingly limited but the majority of the population does not appear to take drugs and it may be that the law has some effect on some of them.
77 As a matter of priority, we recommend that renewed attention is given to the information and research base which facilitates understanding of the evolving picture of drug use and the cost effectiveness of welfare and control responses. Routine statistics should be improved to reduce gaps in the understanding of the scale, nature and extent of drug use. Enforcement and treatment policies should be evaluated thoroughly, making full use of the available range of social science research methods.
Footnotes:
1. T. Bennett, ‘Drugs and Crime: the results of drug testing and interviewing arrestees’, Home Office Research Study 183, London, Home Office, 1998.
2. P. Marks et al, ‘Public attitudes to drug taking: short report on work carried out through the OPCS for the Home Office’, unpublished 1973.
3. M. Ramsay and A. Percy, ‘Drug Misuse Declared: results of the 1994 British Crime Survey’, Home Office Research Study No.161, London, Home Office 1996.
M. Ramsay and J. Spiller, ‘Drug Misuse Declared in 1996: latest results from the British Crime Survey’, Home Office Research Study No.172, London, Home Office 1997.
M. Ramsay and S. Partridge, ‘Drug Misuse Declared in 1998: results from the British Crime Survey’, Home Office Research Study No.197, London, Home Office 1999.
4. S. Anderson and M. Frischer, ‘Drug Misuse in Scotland: findings from the 1993 and 1996 Scottish Crime Surveys’, Research Findings No.17, Edinburgh, The Scottish Office Central Research Unit 1997.
5. ‘Experience of drugs in Northern Ireland: preliminary findings from the 1994/5 Northern Ireland Crime Surveys’, Research and Statistics Branch Research Findings 1/96, Belfast, Northern Ireland Office 1996.
6. K. McElrath and K. McEvoy, ‘Ecstasy Use in Northern Ireland’, London, The Stationery Office 1999.
7. J. Balding, ‘Young People in 1998’, Exeter, Schools Health Education Unit 1999.
8. Office of National Statistics, ‘Smoking, Drinking and Drug Use Among Young Teenagers in 1998’, Volumes 1 and 2, London, The Stationery Office 1999.
9. E. Webb, C. Ashton, P. Kelly and P. Kamali, 'Alcohol and drug use in UK university students', The Lancet, 346 (1996), 922-925.
10. Report cited at footnote 1.
11. European Monitoring Centre for Drugs and Drug Addiction, ‘Annual Report on the state of the drugs problem in the European Union 1998’, Luxembourg, Office for Official Publications of the European Commission 1998. Table 2.
12. In the report cited in the previous footnote, Table 3.
13. Office of National Statistics Mortality Statistics.
14. House of Commons Committee of Public Accounts, Fifteenth Report, ‘HM Customs and Excise: The Prevention of Drug Smuggling’, London, The Stationery Office 1999. Paragraph 30 and Figure 5.
15. European Monitoring Centre for Drugs and Drug Addiction, ‘Annual Report on the state of the drugs problem in the European Union 1999’, Luxembourg, Office for Official Publications of the European Commission 1999. Page 23.
16. R. Newcombe, ‘The people on drugs', Druglink, (14) Issue 4(1999), 12-15.
17. MORI, Modern Britain, survey conducted for the Independent on Sunday newspaper.
18. ICM survey for The Guardian newspaper.
19. ‘Drug Misuse and the Environment’, London, The Stationery Office 1998.
Paragraphs 9.49 and 9.59.
| < Prev | Next > |
|---|