| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 206 |
| Yesterday: | 251 |
| This Week: | 206 |
| Last Week: | 2221 |
| This Month: | 4794 |
| Last Month: | 6796 |
| Total: | 129393 |
Chapter Seven: Cannabis
 |
|  |
| 
| Reports - Drugs and the Law |
Drug Abuse
Chapter Seven: Cannabis
Introduction
1 As the preceding chapters show, cannabis is the drug most likely to bring people into contact with the criminal justice system. It is, by far, the drug most widely and commonly used. It is the drug most often involved in the main drug offences and is the drug that is most often seized. Because of the frequent use of discretion by the police and customs, it is the drug where there is the widest gap between the law as formulated and the law as practised. Cannabis is also less harmful than the other main illicit drugs, and understood by the public to be so. If our drugs legislation is to be credible, effective and able to support a realistic programme of prevention and education, it has to strike the right balance between cannabis and other drugs.
2 Thirty years ago the Wootton Report [1] identified the crucial issue:
'The controversy that has arisen in the United Kingdom about the proper evaluation of cannabis in the list of psycho-active drugs, should be resolved as quickly as possible, so that both the law and its enforcement as well as programmes of health education, may be relevant to what is known about the dangers of cannabis-smoking in this country, and may receive full public support.'
This is the task that we set ourselves in this chapter. In it we bring together the evidence which appears at many different points in this report, and which forms the basis of our conclusions. In this chapter, except in the section on therapeutic use, we discuss cannabis only in its natural plant form, that is herbal cannabis and cannabis resin.
Prevalence, availability and price
3 Three successive British Crime Surveys (in 1994, 1996 and 1998) show that cannabis is, by far, the drug most likely to have been used by all age groups in the last month, last year or at any time. A 1998 survey of 11 to 15 year-old [2] school children suggests that taking cannabis is relatively rare among 11 - 13 year-olds, but increases from the age of 14.
4 Younger people aged 16 to 29 are more likely than those aged 30 and older to say that they have used drugs. About one in five people aged 16-29 in England and Wales say they have used cannabis in the last year, and one in eight say they have used it in the last month (British Crime Surveys since l994). An estimated two and a half million 16-29 year olds used cannabis at least once last year, and around a million and a half used it least once last month (based on the 1998 British Crime Survey).
5 In their evidence to the House of Lords Select Committee on Science and Technology [3], the Department of Health said 'cannabis is now the third most commonly consumed drug after alcohol and tobacco'. The House of Lords report noted that the extent of cannabis use in the United Kingdom is not dissimilar to that in other European countries and somewhat lower than in the United States, Canada and Australia.
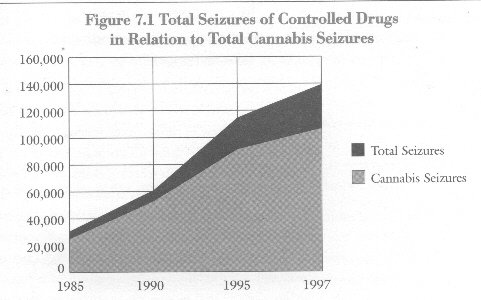
6 Both our MORI surveys and our meetings with young people make it clear that there is no difficulty in obtaining the drug, nor is there any sense that the law is a deterrent for the majority. This is so despite record levels of seizures by police and customs. In 1997, 77% of all drugs seized were cannabis - 150,000 kg. were seized by customs and the police as well as 115,000 plants, almost all seized by the police. In 1990 the comparable figures were 31,000 kg. of cannabis and 34,000 plants.
7 Despite these efforts, the average price of cannabis appears to have been virtually unaffected, decreasing slightly according to the National Criminal Intelligence Service between December 1997 and December 1998, although there are significant local and regional variations. Whether in herbal or resin form, cannabis is commonly sold to consumers in fractions of an ounce, with a deal consisting of 1/8 of an ounce. The evidence suggests that 60% of sales are in the form of resin, 40% in the form of herbal cannabis (of which 60-70% is said to be home grown). The present average price of a 1/8 ounce is put at between £5 and £25 depending upon the form of the substance and its purported potency.
8 We have considered the evidence put to the House of Lords Select Committee on Science and Technology [4] on the potency of cannabis in its various natural plant forms. The evidence is conflicting. It appears that, while some forms of herbal cannabis grown by hydroponic methods may have concentrations of tetrahydrocannabinol (THC), the main psychoactive ingredient of cannabis, of as much as 20%, the average THC content in both herbal cannabis and cannabis resin as analysed by the Forensic Science Service from seizures by the police is around 4-5%. There is no evidence that the presence of THC in higher concentrations leads to significantly higher health risks, just as it cannot be claimed that the risks would be eliminated if only lower-strength varieties of cannabis were available.
Figure 7.1 Total Seizures of Controlled Drugs in Relation to Total Cannabis Seizures
Relative harmfulness of cannabis
9 The main issue for any consideration of the current law on cannabis is how harmful it is compared with other major illicit drugs and whether that harm is properly reflected in the law. We have consulted a wide range of addiction specialists on the relative harm of the major drugs. We asked them to compare drugs independently of their legal classification. The specialists' views underpin the legal classification of cannabis that we propose [5]. We have also carefully considered the work of other experts, including the written and oral evidence presented to the House of Lords. We regard the following conclusions as a fair representation of the current weight of professional opinion.
10 Cannabis is not a harmless drug. That is not in dispute. We cannot do better than quote the summary of harms from cannabis set out by the House of Lords:
'...cannabis is neither poisonous..., nor highly addictive, and we do not believe that it can cause schizophrenia in a previously well user with no predisposition to develop the disease. However, we are satisfied that:- It is intoxicating enough to impair the ability to carry out safety-critical tasks (such as flying, driving or operating machinery) for several hours after taking...;
- It can have adverse psychic effects ranging from temporary distress, through transient psychosis, to the exacerbation of pre-existing mental illness...;
- Regular use can lead to psychological dependence...; and, in some dependent individuals (perhaps 5-10 per cent of regular users), regular heavy use can produce a state of near continuous intoxication, making normal life impossible;
- Withdrawal may occasionally involve unpleasant symptoms...;
- Cannabis impairs cognitive function during use...;
- It increases the heart rate and lowers the blood pressure, carrying risks to people with cardiovascular conditions, especially first-time users who have not developed tolerance to this effect....
...In addition, smoking cannabis carries similar risks of respiratory disorders to smoking tobacco.’ [6]
11 There is considerable concern that cannabis use may contribute to transport accidents since laboratory tests show it can impair performance including driving. However, a review of the scientific literature on drugs and driving commissioned by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) [7] found that evidence as to whether cannabis impairs driving and increases the risks of road accidents was not entirely consistent. Some studies found no significant effects on perception, and others pointed to some impairment of attention and short-term memory, although these effects are typically observed at higher doses. Still others suggest that drivers under the influence of cannabis actually drive more carefully. Interpretation of the causal contribution of cannabis to road accidents is further complicated by the concurrent presence of other drugs, especially alcohol.
12 This situation may change if use increases and the most recent Department of Environment Transport and the Regions report on road traffic deaths shows more cannabis positive cases as compared with ten years ago. Moreover, ongoing research suggests that when cannabis and alcohol are taken together, their effects on driving are at least additive, and that they may even increase each other's effects. We therefore support the active discouragement of driving under the influence of cannabis, especially when in combination with alcohol.
Long-term risks
13 There are also long-term risks. It is worth noting the increasing numbers presenting themselves for treatment for problems brought on by cannabis use. The regional drug misuse databases [8] show that the number of people seeking help from a wide range of drug agencies for problems with cannabis use has doubled from 1,400 in 1993 (7% of the total seeking help) to 3,300 in 1998, (10% of the total). This is, of course, a small fraction of the total number of people who take cannabis but the results must not be discounted. The figures show people who identified cannabis as their 'main drug' when seeking help. They do not, however, reveal the nature of the problems for which the help was sought.
The gateway theory
14 Perhaps the most serious charge against cannabis is made by the so-called 'gateway theory'. This argues that cannabis use leads to the use of more dangerous drugs such as heroin and cocaine. The basic idea of the gateway theory comes from the observation that most users of heroin and other hard drugs have a history of using cannabis. In addition, various mechanisms have been suggested to explain the supposed tendency of users to move from cannabis to harder drugs. One such mechanism is said to lie in the structure of illegal markets, which leads dealers to encourage cannabis users to try other drugs in the hope of increasing profits. Another suggestion is that the pharmacological action of cannabis somehow predisposes the users to try other drugs. We examine these suggestions below.
15 It is certainly true that the use of hallucinogens, amphetamines, cocaine and heroin is almost always preceded by experimentation with cannabis use. It also seems that the earlier the initiation into cannabis, and the greater the involvement with it, the greater the likelihood of progression to the use of other drugs. But these facts are not nearly enough to support the gateway theory. The theory has to show that there is a high probability that a cannabis user will become a heroin user, not just that there is a high probability that a heroin user has been a cannabis user. In fact, the vast majority of cannabis users do not progress to the most dangerous drugs such as heroin. Any significant causal relationship in that direction would have resulted in a far higher population of hard drug users than we have.
16 In our view nothing has emerged to disturb the conclusions of the Advisory Committee on Drug Dependence in 1968 [9], when they said that there was no convincing evidence that cannabis use in itself led to heroin use. This has been largely confirmed by more recent studies. The World Health Organisation noted in 1997 [10] that in some countries there had been a predictable sequence of adolescent drug use with cannabis preceding the use of other drugs including cocaine and heroin but that this
'does not imply that a high proportion of those who experiment with cannabis will go on to use heroin, for example'.
Studies have also shown that cannabis is seldom the first drug that people take for recreational purposes. They almost invariably start with cigarettes or alcohol or both [11]. There is good evidence that the likelihood of 11 to 15 year-olds having ever used an illicit drug is strongly related to regular underage smoking and drinking [12].
17 The suggestion, already mentioned, that there are pharmacological properties of cannabis that predispose users of it to later heroin use, has been discounted in a recent review of the United States literature [13]. Taking cannabis is not by itself an indicator of future heroin or cocaine use unless the cannabis use is heavy and combined with psychiatric or conduct disorders and a family history of psychopathology.
18 Social, cultural and market conditions associated with cannabis use are a different matter. It may be that some cannabis users will go on to other drugs through the influence of friends or the pressure of other factors associated with problematic drug use, such as poverty and unemployment. The WHO concluded that the most plausible explanation for some cannabis users also using other drugs was
'....a combination of selective recruitment into cannabis use of non-conforming and deviant adolescents who have a propensity to use illicit drugs, and the socialisation of cannabis users within an illicit drug-using subculture which increases the opportunity and encouragement to use other illicit drugs.'
In particular, we take seriously the suggestion that pressure may be exercised by dealers on cannabis users to try harder drugs. If there is anything at all in the gateway theory, it is likely to be found in the structure of illegal markets.
19 There is no evidence that cannabis use is crime-related in the same way as heroin or crack cocaine. Nevertheless, when people are arrested for other crimes, cannabis is frequently found in their possession or traces of it detected in their urine through analysis. In a study of a sample of 622 offenders arrested in five police areas in 1996/97 [15], cannabis was the most common illicit drug found in their urine. 46% of those arrested tested positive for it compared with between 72% and 82%, depending on the area, testing positive for alcohol. No particular offence was typical of those testing positive for cannabis and they were not heavily involved with acquisitive crime. Given the wide prevalence of cannabis use in the population at large (and even more so among the age groups likeliest to be committing crime) this is hardly surprising. The difficulty of assessing the significance of drugs in drug-related crime lies in the absence of any evidence that it is the drug that causes the crime rather than other factors also associated with criminality.
Overall assessment of the harmfulness of cannabis
20 The British Medical Association has said [16] 'The acute toxicity of cannabinoids is extremely low: they are very safe drugs and no deaths have been directly attributed to their recreational or therapeutic use.' The Lancet published an article [17] summarising the evidence on the most probable adverse health and psychological consequences of acute and chronic use, and its editorial in the same issue comments that '...on the evidence summarised by Hall and Solowij, it would be reasonable to judge cannabis less of a threat than alcohol or tobacco....We...say that, on the medical evidence available, moderate indulgence in cannabis has little ill-effect on health, and that decisions to ban or legalise cannabis should be based on other considerations.'
21 New medical and scientific knowledge can still be expected to add to the evidence of long-term harm from cannabis, despite the length of time it has been available and the extent of its use. Nevertheless, as the House of Lords report remarks, the harms must not be overstated. When cannabis is systematically compared with other drugs against the main criteria of harm (mortality, morbidity, toxicity, addictiveness and relationship with crime), it is less harmful to the individual and society than any of the other major illicit drugs or than alcohol and tobacco. This is why our consideration of the relative harmfulness of drugs has led us to the conclusion that cannabis is wrongly placed in Class B of Schedule 2 to the MDA.
22 These conclusions are also consistent with public perceptions of the comparative harm of individual drugs. As the surveys conducted for us by MORI show [18], children below the age of 15 see cannabis as almost as harmful as other drugs. From the age of about 15 or 16, however, though their perceptions of other drugs remain stable, their views on cannabis change remarkably. About 34% of 16 to 59 year-olds in our older sample considered cannabis harmful or very harmful, far fewer than those who held that view about other illicit drugs (90-98% depending on the drug) and about alcohol (67%) and tobacco (84%).
The Law on Cannabis
The United Nations Conventions
23 We have set out [19] the general implications of the United Nations conventions and discussed them further [20] in relation to trafficking and possession offences. For cannabis the implications may be summed up as follows:
i) cannabis, cannabis resin and extracts and tinctures of cannabis are included in Schedule I to the Single Convention while cannabis and cannabis resin are also included in Schedule IV. The main MDA offences have therefore to apply to cannabis as to other drugs;
ii) but there is no requirement to place cannabis in one Class rather than another in the MDA, not least because the imposition of penalties is largely a matter of domestic law. It is already dissociated from the other Single Convention Schedule I drugs, most of which are Class A;
iii) imprisonment is not required by the conventions as a sanction either for possession or for cultivation for personal consumption. Alternatives to conviction and punishment may be considered, including treatment, education, aftercare, rehabilitation, or social reintegration;
iv) some trafficking offences where cannabis is involved may also be ‘appropriate cases of a minor nature' where the same alternatives to conviction and punishment could be considered;
v) for reasons that we explain in detail below, it would be possible without renegotiating the conventions to permit the therapeutic use of cannabis, cannabis resin or extracts and tincture of cannabis. The conventions do, however, prevent the prescription of cannabinols (except nabilone and dronabinol) for medical treatment.
The UK law on cannabis
24 Under the MDA, cannabis and cannabis resin are placed in Class B. Those in possession can incur a maximum prison term on indictment of 5 years with an unlimited fine. Traffickers may incur 14 years and an unlimited fine with a liability to confiscation of assets in addition. Growers may also be sentenced to 14 years and treated as traffickers because they are normally prosecuted for production under section 4 of the MDA, not for cultivation under section 6. The owners or managers of premises who knowingly permit or suffer the smoking of cannabis are also exposed to a maximum prison term on indictment of 14 years.
25 If, as we argue, the present classification of cannabis is not justified, it follows that the response of the law is disproportionate to the drug's harm, and may bring the law into disrepute. In our view, therefore, the maximum penalties for cannabis offences should be reduced. This would bring them more into line with penalties in other European countries.
The operation of the law on cannabis
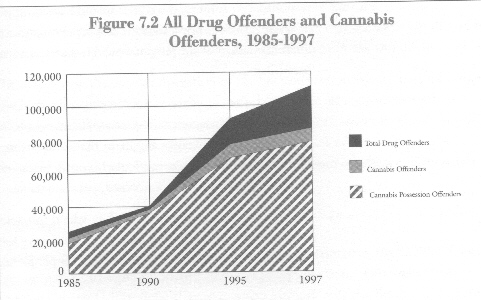
26 The number of people dealt with for drugs offences involving cannabis rose from 40,194 in 1990 to 86,034 in 1997. This was an increase of 114% and represented 76% of all drugs offences in 1997.
27 Enforcing the drugs laws, especially against the possession of cannabis, inevitably involves the police in large numbers of stop and searches. Over 300,000 were carried out for drugs in 1996-97 in England and Wales, bringing the total for four years to over a million. These resulted, over that period, in 134,500 arrests where drugs were found - the great majority of which were for cannabis. While the number of stop and searches has grown, the proportion where drugs have been found and arrests made has declined from 18% in 1988 to 12% in 1997/8 [21]. Stops and searches bear disproportionately on young people from minority ethnic communities in inner city areas. They certainly appear to be discriminatory, although there may be demographic and socio-economic reasons which would make it hard to eliminate the appearance of discrimination altogether.
Figure 7.2 All Drug Offenders and Cannabis Offenders, 1985-1997
Diversion from prosecution
28 Many cases are kept away from the courts by cautioning and compounding and, in Scotland, warning letters and fiscal fines. By far the largest increase in police cautioning in England and Wales has been for cannabis offenders, from 41% in 1990 to 55% in 1997. This has meant in practice a tripling in the number of cannabis offenders for which a caution was given, from 16,500 to 47,000. Cautions are part of an offender's criminal record. There is no provision at present for these records to expire under the Rehabilitation of Offenders Act 1974. The Government has recently issued a consultation paper proposing that this anomaly should be corrected and that cautions should be immediately spent. This would also apply to reprimands and warnings, which are to replace cautions for young people under 18 under the Crime and Disorder Act 1998.
29 Cautioning is not used by H.M. Customs and Excise or in Scotland. For importation and exportation offences, compounding - a monetary penalty in lieu of prosecution - may be used in cases involving cannabis not exceeding 10 grams in weight. While compounding does not necessarily become part of an offender's criminal record, it may be mentioned in subsequent court proceedings. Its use for cannabis importation offenders fell between 1990 and 1997 from 58% to 45%.
30 In Scotland, the procurator fiscal service which brings prosecutions in criminal cases may, if the offender agrees, offer a fine instead of prosecution. Such fines have only recently been used in drugs cases and in 1997, the first year for which figures are available, fines were accepted by 432 of 499 persons dealt with for possession of cannabis.
31 This discretion in the implementation of the MDA is desirable but produces anomalies in the differing regimes of cautioning and compounding, and inconsistencies in the cautioning rates between police forces. More than half of the arrests for cannabis offences result in a caution. We do not criticise the police for their extensive use of cautioning. It is currently the only realistic and proportional response. Without it, the courts would have ground to a halt. However, the use of discretion does not lessen the disproportionate attention that the law and the implementation of the law unavoidably give to cannabis and cannabis possession in particular.
32 Even with the use of discretion on this scale, the law's implementation damages individuals in terms of criminal records and risks to jobs and relationships to a degree that far outweighs any harm that cannabis may be doing to society. Moreover young people, particularly young black and Asian people and particularly where stop and search is concerned, perceive the law as unfair.
33 Discretion needs a clear framework in which to operate. That is why we recommend that cautioning be put on a statutory footing, with guidelines in regulations. This has already been done for people under 18 in the provisions of the Crime and Disorder Act 1998. We do not favour less use of discretion. Better the present, somewhat informal, arrangements than a tightening up that leads to more people being brought needlessly into the criminal justice system.
Sentencing of offenders
34 Even with diversions from prosecution on the present scale, between 1990 and 1997 large numbers of cases involving cannabis, 38,000 in 1997 - far more than any other drug - continued to be tried by the courts. Between 1990 and 1997, the proportion of people fined after being found guilty of cannabis offences fell from 67% to 49%. The proportion imprisoned rose from 10% to 14%. Despite Court of Appeal guidelines recommending fines as the normal penalty for cannabis possession, fines for possession - by far the most frequent offence - declined markedly from 70% to 55% of cases. Over the period there was a small rise in the proportion sentenced to imprisonment, from 6% to 8%. While the reasons for imprisonment are not completely clear, there are indications that almost no one is given an immediate custodial sentence solely for possession of cannabis, unless there is evidence of persistent flouting of the law.
35 Between 1990 and 1997, the likelihood of being imprisoned for the more serious, mainly trafficking, offences increased and the likelihood of being fined declined. For example, the proportion of people fined for production of cannabis fell from 63% to 37%, while the percentage given immediate custodial sentences rose from 6% to 16%. The proportion of offenders fined for allowing premises to be used for cannabis offences halved to 22% in 1997, while the percentage given sentences of immediate custody more than doubled to 19%.
36 The concentration on cannabis as an objective of law enforcement is at odds with the views of a significant proportion of the population. The surveys conducted for us by MORI show that two-thirds of adults want strong legal controls on drugs and do not regard drug use as a private matter beyond the law. But most of them do not include cannabis among the drugs that need controlling. Almost one-half (46%) thought that the law should be changed so that it is not against the law to use it. When asked to select three things they thought should be the highest priorities for the police, less than 1% of respondents mentioned cannabis use as opposed to 8% who selected heroin use. Only 9% chose cannabis dealing as compared to 66% who chose heroin dealing. 54% said that cannabis use should be the lowest priority as compared to 1% who said that heroin use should be.
37 In considering the current operation of the law and sentencing patterns we are of the view that the possession of cannabis should not be an imprisonable offence. Consequentially, it should no longer be an arrestable offence in England and Wales under section 24 of PACE. Further, the prosecution of offences of cannabis possession should be the exception and only then should an offence, if there is a conviction, incur a criminal record.
Cultivation of cannabis
38 Cultivation of cannabis is a separate offence under section 6 of the MDA but cases are generally prosecuted under section 4 (2) as production. This was not the position in 1971. The definition of cannabis covered only the flowering or fruiting tops of the plant, with the result that a person found growing plants that had not yet flowered or produced fruiting tops was not guilty of production, though he could be prosecuted for cultivation. Section 52 of the Criminal Law Act 1977 widened the definition of cannabis in the MDA to include almost the whole plant. Since then, cases have been brought under section 4; section 6 has become virtually a dead letter.
39 This change is more than a legal technicality because production, but not cultivation of cannabis, is designated as a trafficking offence for the purposes of the Drug Trafficking Act 1994. Confiscation of assets may result from a conviction. This may be disproportionate in cases involving a few plants for personal use. Although we have heard no reports of the courts ordering confiscation in such cases, the law as it stands seems to allow the possibility.
40 This situation is not required by the United Nations conventions. The 1988 convention against illicit traffic in narcotic drugs and psychotropic substances [22] permits two separate offences: one of cultivation for the purpose of the production of narcotic drugs (in effect the trafficking offence); the other cultivation for personal consumption (an offence for which imprisonment as a sanction is not required). This approach to cannabis cultivation seems clear and logical compared with that of the MDA. There are real differences, which United Kingdom law does not currently reflect, between activities that are production for the purposes of supply, and those that are cultivation for personal use.
41 We recommend that the cultivation of small numbers of cannabis plants for personal use should be a separate offence from production, and should be treated in the same way as possession of cannabis.
International Comparisons
42 In coming to our conclusions we were influenced by the experience of other countries. The position in the Netherlands has been of particular interest as the country where tolerance of cannabis has been taken furthest. Dutch law divides drugs into two classes. One class includes all the drugs defined as carrying an unacceptable risk. The other class contains all the other drugs. The maximum penalties for offences involving the possession of drugs in this second class are significantly milder, one month's detention as opposed to one year. The main aim of the law is to ensure that drug users are not caused more harm by prosecution and imprisonment than by the use of the drugs themselves.
43 Dutch drugs policy is aimed at separating the market for less harmful drugs - herbal cannabis and cannabis resin - from the market for drugs carrying an unacceptable risk - such as heroin and cocaine. The Dutch reject the idea that cannabis pharmacologically induces people to switch from soft to hard drugs. They do, however, accept that the more that users are part of a subculture where drugs of both classes are obtainable, the greater the risk of progression from soft to hard drugs.
44 Within this framework, the sale of cannabis from licensed or regulated coffee shops, for use either on or off the premises, is tolerated. The coffee shops and their regulation are seen as consistent with a broader public information and education policy. This is based on accurate information about the risks of drug use, as well as of alcohol and tobacco, and ways of limiting those risks.
45 There is a 5 gram limit on individual sales (originally 30 grams but reduced in 1995), and a 500 gram limit on the coffee shop stocks. Although possession and supply remain offences, prosecution is waived in the public interest provided these amounts are not exceeded under a formal written policy based on the principle of expediency. Other conditions that have to be met if the coffee shop is to remain in business are:
i) no sales of hard drugs;
ii) no sales to minors;
iii) no advertising;
iv) no sales of alcohol on the same premises;
v) no nuisance (specific local rules may be set about such matters as parking in front of the entrance or early closing times).
46 If coffee shops violate these conditions they risk being closed down, and since 1996 the number of coffee shops has been reduced by between 10% and 15%. There is a tripartite approach involving the local authority, police, and public prosecutor to deal with issues arising from the regulation of coffee shops.
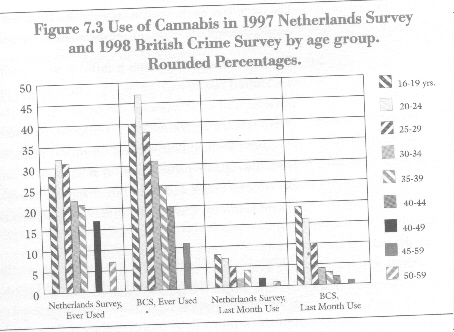
47 Holland's formal written policy of not prosecuting people found in possession of small amounts of cannabis dates from 1976, with coffee shop sales tolerated from 1980. It was not followed immediately by increases in the numbers using the drug. But, beginning in 1984, use increased sharply following increasing commercialisation. Increases in use in Holland since the early 1990s have paralleled increases taking place in the United States and in other countries with stricter enforcement policies. The recent publication of the survey of drug-taking prevalence in Holland [23] shows that the number of people ever taking cannabis there, or taking it in the last month, is significantly lower than that shown in the 1998 British Crime Survey.
Figure 7.3 Use of Cannabis in 1997 Netherlands Survey and 1998 British Crime Survey by age group. Rounded Percentages.
48 The following results are claimed for the Dutch drug policy:
i) Although cannabis use has increased since the coffee shop policy was introduced, similar or greater increases have taken place in other countries including the United Kingdom, the United States, the former West Germany, France, Spain, Sweden and Finland [24];ii) self-reported cannabis use amongst the youngest surveyed age group (16-19 years) is consistently lower in the Netherlands than the United Kingdom;
iii) the number of problem drug users has been stable for many years, and the average age of this group in Amsterdam has risen year on year and is now 36. (United Kingdom data suggest annually increasing numbers of problem drug users, the average age of new addicts is 25 or 26, while between 1991 and 1996 the proportion under 21 rose from 15% to 22%);
iv) drug-related deaths per million population are the lowest in Europe. In 1995, the figure for the Netherlands was 2.4 as against 31.1 for the United Kingdom. (We recognise the difficulty of comparing mortality statistics between countries on a like for like basis but the relative success of the Netherlands seems undeniable on any conceivable interpretation).
49 The coffee shop approach has not been without critics even in Holland itself. It seems, however, that Holland can justly claim to have separated the heroin and cannabis markets. As a result, young people are far less likely in Holland than elsewhere to experiment with heroin. Although there is room for argument over how precisely this has been achieved, it is difficult to deny that the policy of separation of markets, including the toleration of coffee shops, has made a contribution.
50 It should be noted that it is not certain that most sales of cannabis take place through the coffee shop system - one estimate puts the proportion at a third. We cannot therefore be certain that it is the policy of market separation that has achieved the Dutch success with heroin, although the possibility is a very real one. The same success in separating cannabis from heroin is not claimed for other drugs, particularly cocaine, amphetamines and ecstasy.
51 The coffee shop mechanism is difficult to reconcile fully with the requirements of the United Nations conventions. The policy of non-prosecution for the sale and possession of small amounts can be justified on the basis that the prosecution of offences is left to domestic law, under which discretion may be exercise if it is expedient in the public interest. A similar public interest criterion is applied by United Kingdom prosecutors. It is less easy to justify the holding of stocks of cannabis by coffee shops, and their supply through cultivation or importation (about half from each). The supply, at least, seems to take place in breach of the law.
52 Despite these difficulties and contradictions, we think that the Dutch experience holds two important lessons for the United Kingdom. The first is the potential benefit from treating the possession and personal use of all drugs - not just cannabis - primarily as health problems. This should ensure that young people who experiment with drugs remain integrated into society rather than becoming marginalised. The second is the potential benefit from separating the market for cannabis from that of heroin. By doing so, the Dutch have provided persuasive evidence against the gateway theory of cannabis use, and in favour of the theory that if there is a gateway it is the illegal market place.
53 We recognise that, in the present political and cultural climate, it is difficult to see the introduction of Dutch-style coffee shops in the United Kingdom. The contradictions between domestic and international law and these practices are too great. The Dutch may be able to live with them, but they are likely to cause greater difficulties here. Nevertheless there may be developments that move us towards the Dutch experience, particularly as greater autonomy is devolved to local communities.
54 Other international comparisons suggest that the law has a limited effect, if any, on use [25]. During the 1970s several states in the U.S.A. reduced the maximum penalty for the first offence of possession of small amounts of marijuana for personal use to a small fine. Levels of marijuana use increased between 1972 and l977 in those states but even more so in the states that had not reduced penalties. In fact the greatest rises in use took place in states with the most severe penalties.
55 Since 1987, South Australia has operated a cannabis expiation notice (CEN) scheme under which the payment of a small fine within 60 days enables offenders over 18 to avoid prosecution. The expiable offences include offences consistent with personal use. The number of notices issued under the scheme doubled between 1987 and 1996, probably due to the greater ease of CEN procedures compared with the arrest and charge procedures required for prosecution. In response to a decline in the rate at which fines were paid between 1987 and 1991/2 new legislation was introduced in 1996 intended to increase the rate of expiation by allowing the offender a greater range of payment options. Figures to 1995 indicated that there was an increase in cannabis use since the beginning of the CEN scheme. However, there were also increases over the same period in two other states where penalties had not changed. There were no greater increases either in weekly cannabis use or in use among 14 to 29 year olds in South Australia compared with the rest of the country [25].
Therapeutic use of cannabis
56 Until 1973, tincture of cannabis had been available for medical use for over 100 years. In 1973, the medical use of cannabis was prohibited in the United Kingdom following a long decline in its use in favour of what were considered more reliable drugs. Beginning in the 1980s, interest in the potential benefits of cannabis for the treatment of certain medical conditions was renewed, and has become a significant issue. The medical and scientific basis for this increased interest has been considered by the British Medical Association [27] and the House of Lords [28]. We have nothing to add to the detail of the reports of the expert members of both of these bodies. However, we recognise the importance of careful consideration of the issue because of the implications that therapeutic use of cannabis has for the MDA.
57 Cannabis, cannabis resin, cannabinol, and cannabinol derivatives are listed in Schedule 1 to the Misuse of Drugs Regulations 1985 (except dronabinol or its stereoisomers which are now in Schedule 2 of the regulations). In effect, this means that these substances cannot lawfully be produced, supplied, possessed, imported or prescribed except under licence from the Secretary of State issued under Regulation 5. The drugs are also designated by order under section 7 (4) of the MDA as drugs whose production, supply and possession are unlawful for any purpose other than research.
58 Two cannabinoid-type substances can be prescribed by doctors as part of the treatment of their patients. The first is nabilone. This is not a controlled drug. It is a synthetic analogue of THC which is licensed under the Medicines Act 1968 for prescription to patients with nausea or vomiting resulting from cancer chemotherapy and which has proved unresponsive to other drugs. The second is dronabinol, which is a synthetic THC in sesame oil and appears in Schedule 2 to the 1985 regulations. This allows it to be prescribed on a named-patient basis for the same purpose as nabilone.
59 The United Nations conventions are restrictive but there is more room for manoeuvre in the case of cannabis and cannabis resin than there is over cannabinols. Cannabis and cannabis resin are contained in Schedule IV to the Single Convention. Article 2.5 (b) of this states 'A Party shall, if in its opinion the prevailing conditions in its country render it the most appropriate means of protecting the public health and welfare, prohibit the production, manufacture, export and import, trade in, possession or use of any [Schedule IV] drug except for amounts which may be necessary for medical and scientific research only, including clinical trials therewith to be conducted under or subject to the control of the Party.' This does not impose a mandatory obligation on the United Kingdom to prohibit any of those activities in relation to cannabis or cannabis resin because it is subject to the proviso that the prevailing conditions in the country concerned make it the most appropriate means of protecting the public health and welfare. For example, heroin, another drug contained in schedule IV to the Single Convention, is in fact available on prescription in the United Kingdom for the treatment of organic disease or injury.
60 The position with cannabinoids is different. They are listed in schedule I of the 1972 United Nations Convention on Psychotropic Substances. Article 7 (a) of this requires states to 'prohibit all use except for scientific and very limited medical purposes by duly authorised persons, in medical or scientific establishments which are directly under the control of their Governments or specifically approved by them'. There is no saving for 'prevailing conditions' in the country concerned and the requirement is therefore binding. Because of it dronabinol had to be moved from Schedule I of the 1972 convention, before it was possible for the United Kingdom government, in 1995, to put it in Schedule 2 to the 1985 Regulations, thus allowing its prescription for medical purposes.
61 To summarise, the government has the power to allow cannabis and cannabis resin, including tinctures and extracts, to be prescribed in this country without renegotiation of the international conventions. But for cannabinols other than dronabinol and nabilone to be used therapeutically, the conventions would have to be renegotiated first.
62 The British Medical Association concluded [29] that cannabis in its plant form was unsuitable for medical use. The grounds were
a) cannabis contains over 400 chemical compounds and over 60 cannabinoids. Even if proved to have therapeutic benefits, it would not be possible to know which agents (or combination of agents) were beneficial, and medical knowledge would not be advanced or treatment improved;b) the difficulty at (a) is compounded by the variation in the concentration of cannabinoids present in different preparations (although it seems that standardised preparations might be possible);
e) the known toxic ingredients in cannabis smoke.
63 On cannabinoids (including apparently the cannabinols), the British Medical Association made the following recommendations, among others [30]:
'1. The World Health Organisation should advise the United Nations Commission on Narcotic Drugs to reschedule certain cannabinoids under the United Nations Convention on Psychotropic Substances, as in the case of dronabinol. In response the Home Office should alter the Misuse of Drugs Act accordingly.2. In the absence of such action from the World Health Organisation, the Government should consider changing the Misuse of Drugs Act to allow the prescription of cannabinoids to patients with particular medical conditions not adequately controlled by existing treatments.’
64 The House of Lords Select Committee on Science and Technology said [31] that there was not enough rigorous scientific evidence to prove conclusively that cannabis itself has or has not medical value of any kind. Nevertheless the anecdotal evidence convinced them that cannabis almost certainly does have genuine medical applications, especially in treating multiple sclerosis. Because of the delays inherent in the system for licensing new medicines, they recommended that the Government should take steps to transfer cannabis and cannabis resin from Schedule 1 to the Misuse of Drugs Regulations 1985 to Schedule 2. This would permit doctors to prescribe an appropriate preparation of cannabis, albeit as an unlicensed medicine and on the named-patient basis, and allow doctors and pharmacists to supply the drug prescribed.
65 The Select Committee said that the principal reason for recommending that the law be changed was compassionate. Illegal medical use of cannabis was quite widespread and exposed patients and, in some cases, their carers to all the distress of criminal proceedings, with the possibility of serious penalties. As a secondary reason, the Committee mentioned that the law appeared to be being enforced inconsistently and sometimes with a very light hand. Some cases were not brought to court, and when they were, sentences were sometimes light or juries even refused to convict. They felt that this brought the law into disrepute and that, rather than enforce it more rigorously, it should be changed.
Our view
66 We appreciate the doubts of the British Medical Association over how to control and assess dosages of raw cannabis. But these seem to us insufficient reasons for preventing prescription where doctors, at their own risk on a named-patient basis, believe that their patients will benefit. Also, while understanding the reservations expressed by the British Medical Association and the House of Lords Select Committee about administration by smoking, this seems to us a very minor matter given the seriousness of the conditions for which prescription of cannabis seems likely to be beneficial.
67 We conclude that there is evidence that there are therapeutic benefits from the use of cannabis by people with certain serious illnesses and that these benefits outweigh any potential harm to themselves. We therefore agree with the House of Lords Select Committee that cannabis and cannabis resin, together with tincture and extracts not covered by the 1971 convention, should be transferred from Schedule 1 to Schedule 2 to the 1985 regulations. That would automatically ensure that doctors who prescribed such substances were not criminally liable. The same would apply to their patients in possession and doctors or pharmacists who supplied cannabis. Arrangements would need to be worked out for pharmacies to secure legitimate supplies of stocks, but that should not pose insuperable problems. We do not share the Government's anxiety about the capacity of GPs to withstand pressure for the prescription of cannabis. There is no evidence that this has been a problem where the prescription of heroin for pain control is concerned.
68 As the Government has rejected the House of Lords recommendations and it will be some years before a standard licensed cannabis product is available, we recommend that there should be a new defence of duress of circumstances on medical grounds for those accused of possessing, cultivating or supplying cannabis. We recommend that the burden be on the accused to prove the defence. This approach would comply with our international obligations under the United Nations conventions and enable spurious defences to be rejected.
Arguments for and against change in the law
69 We are bound to accept that there is a risk that the changes in the law which we propose may lead to the use of cannabis by more people, some of whom may become dependent on it. But on the evidence of the current wide availability and use of the drug in the United Kingdom, and given the attitude of the public to the deterrent effect of the law, we do not think that the risk is significant. It is not possible to quantify it or to be sure that there will be an increase in use at all.
70 There may also be a risk of more people being dealt with more severely than at present if the Scottish system of fiscal fines is introduced in England and Wales as we recommend. Again we do not think that the risk is a serious one. The police are likely to be fairly selective in sending cannabis cases to the CPS for consideration of a fine. In any case, we envisage that statutory guidelines on these and on cautioning should define carefully the cases likely to be suitable for each disposal.
71 These are minor and largely speculative disadvantages compared to the real gains that we foresee from the changes that we recommend. They would lead to a law that fits better with public attitudes, and overcomes the present inhibition on accurate education about the dangers of cannabis, especially the long-term risks. It is this aspect of drug use which is usually absent from young people’s assessment of harm. Better education should in turn lead to more responsible norms of cannabis taking, especially where driving is concerned.
72 A primary concern of ours is minimising the adverse, unnecessary and disproportionate criminal consequences for very large numbers of otherwise law-abiding, usually young, people. Our recommendations are intended to support the education, prevention and treatment elements of a broader health agenda, which itself reflects the relative risks of different drugs including cannabis. Our recommendations are not in breach of the United Nations Conventions. All of the present cannabis offences are being retained. The recommendations are in fact closer to the spirit of the conventions in taking an approach to personal consumption that is less punitive and more orientated towards health and education.
Our conclusions and recommendations on cannabis
73 Weighing the harm from cannabis against the costs of the current system of control leads us to the conclusion that cannabis is in the wrong class in the MDA, both as a reflection of its dangers relative to other drugs and in respect of the penalties attached to its possession, cultivation and supply. International comparisons indicate that different approaches are possible within the United Nations Conventions, and do not pose significant risk of worsening the situation.
74 As long as cannabis is illegal and so widely used, it will be the drug that occurs most frequently in all enforcement activities against drug misuse, whatever their objective. Inevitably, cannabis offences and especially offences of cannabis possession, will dominate the operation of the law in statistical terms, reflecting very large numbers of arrests, prosecutions and criminal records. Despite this expense of time and resources by the courts, and especially the police, there is little evidence of the law's effectiveness as a deterrent. While we have accepted that the police need to retain the powers of stop and search conferred by the MDA, we have seen no evidence to persuade us that they need to retain the power of arrest following the discovery of cannabis, whether as a result of stop and search or other operations.
75 There can be no doubt that, in implementing the law, the present concentration on cannabis weakens respect for the law. We have encountered a wide sense of unease, indeed scepticism, about the present control regime in relation to cannabis. It inhibits accurate education about the relative risks of different drugs including the risks of cannabis itself. It gives large numbers of otherwise law-abiding people a criminal record. It inordinately penalises and marginalises young people for what might be little more than youthful experimentation. It bears most heavily on young people in the streets of inner cities who are also more likely to be poor and members of minority ethnic communities. The evidence strongly indicates that the current law and its operation creates more harm than the drug itself.
76 We see our recommendations as the first steps of an incremental process. The aims of this process are to achieve less coercive but more effective ways of reducing the harms of cannabis, and to bring those harms and the harms of the law into a better balance.
77 Our recommendations on the law on cannabis and its implementation are:
i) Cannabis should be transferred from Class B to Class C of Schedule 2 of the MDA and cannabinol and its derivatives should be transferred from Class A to Class C.ii) The possession of cannabis should not be an imprisonable offence. As a consequence, it will no longer be an arrestable offence in England and Wales under section 24 of PACE, and arrests will only be possible under section 25 of PACE where there are identification or preventative grounds.
iii) Prosecution of offences of cannabis possession should be the exception and only then should an offence, resulting in a conviction, incur a criminal record. An informal warning, a formal caution, a reprimand or warning in the case of those aged 17 or under, or a fixed out-of-court fine should be the normal range of sanctions.
iv) The cultivation of small numbers of cannabis plants for personal use should be a separate offence from production and should be treated in the same way as possession of cannabis, being neither arrestable nor imprisonable and attracting the same range of sanctions. Cultivation of cannabis for personal use under section 6 and production under section 4 should be mutually exclusive offences.
v) The maximum penalty for trafficking offences for Class C drugs, including cannabis, should be 7 years imprisonment and/or an unlimited fine. This is broadly in line with those European countries which we have studied and somewhat higher than most of them. Cannabis trafficking offences would, like all such offences, continue to attract the confiscation powers of the Drug Trafficking Act 1994.
vi) Permitting or suffering people to smoke cannabis on premises which one occupies or manages should no longer be an offence under section 8 of the Misuse of Drugs Act 1971.
vii) Statutory sentencing guidelines should include vicinity to schools, psychiatric services and prisons as aggravating factors for the purposes of sentencing for trafficking offences.
viii) Cannabis and cannabis resin should be moved from Schedule 1 to Schedule 2 of the MDA Regulations thereby permitting supply and possession for medical purposes. If there is to be any delay in adopting this recommendation pending the development of a plant with consistent dosage, we recommend a defence of duress of circumstance on medical grounds for those accused of the possession, cultivation or supply of cannabis.
Footnotes:
1. ‘Cannabis. Report by the Advisory Committee on Drug Dependence’, London, HMSO 1968, paragraph 68.
2. Office of National Statistics, ‘Smoking, Drinking and Drugs Use Among Young Teenagers’, London, The Stationery Office 1999.
3. 'Cannabis. The Scientific and Medical Evidence’, London, The Stationery Office 1998. (HL Paper 151, November). Paragraph 6.3.
4. Report cited in footnote 3, paragraphs 6.11-6.15
5. See Chapter Three, paragraph 31.
6. See paragraphs 8.19 and 8.21 of the report cited at footnote 3.
7. 'Annual Report on the State of the Drugs Problem in the European Union 1999.’ Luxembourg, Office of Official Publications of the European Union, 1999. Page 28.
8. See Chapter Two, paragraphs 14 and 15 for a fuller account.
9. Paragraph 6.3 of the report cited at footnote 1.
10 'Cannabis: a health perspective and research agenda’. Geneva, World Health Organisation, 1997. Section 5.4.
11. D.B. Kandel and others, ‘Stages of progression of drug involvement from adolescence to adulthood: further evidence for the gateway theory’, Journal of Studies on Alcohol, (53) 1992, pp. 447-457.
12. See report cited at footnote 2.
13 Institute of Medicine, ‘Marijuana and medicine: assessing the science base’. Washington, D.C., National Academy Press 1999. Chapter Three.
14. See paragraph 5.4 of report cited in footnote 10.
15 T. Bennet, ‘Drugs and crime: the results of research on drug testing and interviewing arrestees’, Home Office Research Study 183, London, Home Office 1998.
16. ‘Therapeutic uses of cannabis’, Amsterdam, Harwood Academic Publishers 1997. Page 65.
17. W. Hall and N. Solowi, 'Adverse effects of cannabis', The Lancet 14 November 1998, pp. 1611-1616.
18. See Chapter Two, paragraphs 59-61.
19. See Chapter One, paragraphs 5-14.
20. See Chapter Four, paragraphs 6 and 7, and Chapter Five, paragraphs 2 to 6.
21. Home Office Statistical Bulletin 2/99, ‘Operation of Certain Police Powers under PACE: England and Wales 1997/8’. London, Home Office 1999.
22. See Chapter One, paragraph 9 and 10.
23. 'Licit and illicit drug use in the Netherlands, 1997’ Centrum voor Drugsonderzoek, Universiteit van Amsterdam. 1999
24. The best data for this comparison are to be found in the Annual Reports of the European Monitoring Centre for Drugs and Drugs Addiction. Care must be taken in interpreting the data as there are differences between countries in the survey years, drugs covered and age range of samples.
25. E. Single. 'The impact of marijuana decriminalisation: an update'. Journal of Health Policy, (Winter, 1989), pages 456-466.
26 R. Ali, et al., ‘The social impacts of the Cannabis Expiation Notice scheme in South Australia’. Canberra: Department of Health and Family Services 1998.
27. See report cited at footnote 16.
28. See report cited at footnote 3.
29. See pages 68 and 69 of report cited at footnote 16.
30. See pages 78 and 79 of report cited at footnote 16.
31. See paragraph 8.1 of report cited at footnote 3.
| < Prev | Next > |
|---|