| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4.1% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 181 |
| Yesterday: | 251 |
| This Week: | 181 |
| Last Week: | 2221 |
| This Month: | 4769 |
| Last Month: | 6796 |
| Total: | 129368 |
6 COCAINE, MARIJUANA, AND THE MEANINGS OF ADDICTION
 |
|  |
| 
| Books - Dealing with Drugs |
Drug Abuse
6 COCAINE, MARIJUANA, AND THE MEANINGS OF ADDICTION
Robert Byck
Are cocaine and marijuana addicting? Are some drugs more ad-dicting than others? These two questions, although they seem "sci-entific," are semantic. In ordinary English the answer to both questions is "yes."
Ordinary English is not the language of pharmacology, medicine, public policy, or law. To answer the questions properly we must first know something about drugs, words, and prejudices. For this reason I will divide this chapter into sections. The first will be an introduc-tion to the variables of pharmacology and descriptions of the phar-macology of cocaine and marijuana. The second section discusses the words pharmacologists, lawyers, policy makers, and the public use in describing drug-taking behavior and its effects. The third sec-tion tries to make sensible distinctions about the way we might use terminology to be descriptive and communicative instead of political and obscurative.
VARIABLES OF PHARMACOLOGY
There are standard reference works describing the pharmacology of marijuana and cocaine in some detail.' There is a language of phar-macology with circumscribed definitions, used for the most part in a consistent way. One can use primary texts such as The Pharma-cological Basis of Therapeutics for pharmacological explanations of these terms. Although "drug abuse" occurs only in man, some of the measurable variables relevant to the topic can be measured only in animals. We will be concerned here with the effects of drugs in man, but some reference must be made to the animal behavioral studies that are the systematic scientific base for statements about drug dependency.
Before discussing the pharmacology of the drugs, I will present the pertinent pharmacological variables that are important to con-sider in evaluating the behavioral and physiological effects of all drugs. The word drug itself has acquired a common meaning relating to certain, but not all, abused chemicals. I will try to use the term in the broader sense of a chemical substance that causes physiolog-ical changes when administered to a living organism. Although "drugs" are commonly assumed to have unitary and specific effects, this is not the reality. Each drug has a spectrum of effects depending on form, dosage, route of administration, and chronicity. The hu-man variables of personality structure and circumstance of drug administration are equally important in judging the psycho-pharmacological results of drug taking.
Using familiar examples, I will illustrate the importance of pharmacological and human variables in the effects of drugs on hu-man behavior. The form of a drug is important. For example, "co-caine" is a small percentage of active substance in coca leaf, a substance chewed by 12 million people throughout the world. But "cocaine" might also be cocaine hydrochloride, a refined chemical, which is used in medical anesthetic practice. The effects of the sub-stances may be different because the form can limit the route and the dosage of the drug. A pure substance, such as cocaine hydro-chloride, can be taken by many routes and in unlimited dosage. Dos-age is restricted if one is chewing leaves with a maximum concentration of less than 2 percent cocaine. A large amount of sub-stance must be masticated before any significant amounts of cocaine can accumulate in the blood.
Form limits the route of administration. There is little one can do with leaves except chew them; on the other hand, the hydrochloride could be injected or swallowed or sniffed. The hydrochloride cannot be smoked, a popular method of taking in cocaine, since first it must be converted to the so-called "freebase" of cocaine by a chemical extraction process. Only the freebase or cocaine paste, a raw extract containing free alkaloid, will vaporize in with heat and give an ad-equate dosage when smoked.
Marijuana, in contrast to cocaine, is almost always the botanical dried leaf form, and the extracted active chemicals are probably never seen in the street drug-abuse market.
Dosage of a drug is a critical variable in determining its effects. It is quite clear that very tiny amounts of a potent substance may cause no effects, whereas huge amounts of relatively innocuous ma-terial may cause death. For the most part I will consider the dosages ordinarily self-administered by abusers of the drugs. It is a principle of pharmacology that dosage and effect are related. In a single ad-ministration, effect is usually linearly related to the log of dose. Var-ious effects may have different dose-effect relationships. It is an ancillary principle of pharmacology that almost all drugs have mul-tiple effects.
Dosage on the street is not always what it seems to be. If cocaine is heavily diluted or "cut," the amount or dosage of real cocaine that can be taken in is limited by the percentage of cut. In today's world most street cocaine is about 30 percent pure substance. The physical volume limits the amount that can be taken in, although the psychological effect of snorting a line of white powder is based on the belief that all of it is really cocaine. In general, street users have unwarranted faith in the unlabeled product they buy. Buyers of street drugs will usually insist that they have particularly good "stuff." Chemical analyses often indicate that street users are often taking small absolute quantities of active substance.
The route of administration is also an important factor in how drugs have their effect. Cocaine, for example, can be taken by chew-ing the leaves, by swallowing the hydrochloride, by snorting or sniff-ing the powder, by smoking the alkaloidal substance, or by injecting the material intravenously. Each of these routes produces a partic-ular pattern of drug usage that is more determined by the route than it is by the drug itself. For example, chewing the leaves provides a continuous, but low level, exposure to cocaine. Snorting is usually done in a series of small doses at intervals of about twenty minutes. With snorting there is a relatively rapid uptake into the blood stream. That uptake of the drug into the blood from the nasal mucosa is limited by the constriction of blood vessels by cocaine. Because there is less blood flow, large amounts cannot be taken up rapidly. When the drug is swallowed it is more effective than if taken intranasally. Most users ignore this because the traditional method of adminis-tration for cocaine is to snort it. The smoking and intravenous routes both provide a rapid and almost unlimited uptake of the drug into the bloodstream and therefore are associated with much more severe forms of abuse. Smoking, a recently popular method of administra-tion, is more acceptable to most drug users because it is accepted as a social method of drug ingestion. Intravenous use is usually reserved for more hardened drug takers. The assembling of the intravenous drug use paraphernalia represents an obvious shift out of normal life-style patterns and into the patterns of heavy drug users. Giving oneself an injection requires skill and a commitment to drug misuse.
The patterns of usage and problems that affect drug users are de-termined in part by these different routes of administration. The problems associated with intravenous drug use include infection and rapid overdose. Smoking creates lung problems. Snorting can dam-age the nasal mucosa. Intravenous cocaine users obviously are in the greatest danger, and snorters and chewers in the least.
The frequency and chronicity of taking drugs is also an important factor in their effects. Oftentimes scientific reports show the effects of only a single dosage of a drug. This is a standard approach to describe the effects of drugs in man. Such reports can only be par-tially extrapolated to the effects of chronic administration. Because there are limits to human experimentation, we are forced to gather much of our information from observation of street users.
Important data can be obtained from laboratory studies. If the drug is given in a single dosage, one can examine the time to the onset of effect, the plasma levels of the drug, and the specific drug effects from that single administration. If, however, a drug is taken in repeated administrations every fifteen minutes, the effects may be different. The effect may increase with each administration and, if the administration continues for a long period of time, the effects seen with chronic usage can differ markedly from those seen with a single drug dosage.
Each drug has its own typical pattern of usage. For example, co-caine and stimulant users take the drug in "runs": They will use whatever amount is available in continuous usage over hours or a day and then, when the drug runs out, stop using it. This is in con-trast to the usage of heroin, which is taken day and night almost continuously. The effects of the drugs and their ability to produce dependence or withdrawal syndromes are often governing factors in how the drug is used. Cocaine is usually used in short runs, but if large amounts of the drug are available, prolonged ingestion of the drug can occur. Whereas single doses of cocaine rarely produce strik-ing psychological effects, chronic and continuous usage of the drug can cause a paranoid state and a state of extreme edginess or ner-vousness associated, in some instances, with a psychosis.
Marijuana, the other substance to be considered, is often used chronically and daily by the drug users, who thus can remain in al-most a continuous state of intoxication. This form of usage would be rare for a cocaine abuser. There are cumulative effects that can be either the result of larger and larger amounts of drugs building up in the body or the result of the nervous system's adaptation to a continuous state of drug effect.
A simple unitary description of a drug is not likely to be accurate. The reader should be aware that drugs can have completely different effects at different dosages. It is possible to look at the effects of a drug as moving through a spectrum as concentrations in the body increase. The most familiar example would be alcohol. In a small dose, alcohol can cause relaxation and a decrease in anxiety. In a somewhat larger dose, alcohol can cause ataxia and drunkenness; and in an even larger dose, it will tend to cause sleep. In a high dose, alcohol can act as a general anesthetic; and in an even higher dose, it can be a lethal poison and cause death. So here we have one of the most commonly used drugs whose effects can differ not only quantitatively but even qualitatively, depending on the dosage in-gested. Alcohol can be examined with relation to the other factors given for cocaine above, in that it is obvious that an occasional social drink has a behavioral effect different from that of the continuous drinking of a chronic alcoholic, and the behavior of a chronic al-coholic is markedly different from the behavior of an occasional social drinker.
A reasonable first premise of drug abuse research is that the pharmacological properties of the substance must be known. The description of properties should include a description of the mate-rial, its pharmacological effects in man, its distribution and meta-bolism in the body, measures of its reinforcing properties, and estimates of abuse potential.
Cocaine
Although in the popular mind cocaine is considered an evil, it is a widely used therapeutic substance. Many physicians consider the drug to be indispensable as a vasoconstrictor and local anesthetic. Local anesthetics block nerve conduction when applied directly to nerves or in places where they can diffuse to the site of nervous tissue. They differ from the many compounds that can injure or permanently de-stroy nerve tissue in that their effect is reversible. All local anes-thetics, including cocaine and synthetic drugs such as procaine (novocaine) and lidocaine, work by a similar mechanism.
Nerve conduction proceeds by an ionic mechanism involving the passage of sodium and potassium ions across the nerve membrane. This action is prevented by local anesthetics. The specific details of how local anesthetics change the membrane are not known, but it is now presumed that the effects are the result of both dissolution into the nerve membrane and binding at a receptor site within the sodium channel. Vasoconstrictor drugs, which diminish local blood flow, are often mixed with other local anesthetics to prolong their effect. Co-caine has its own sympathomimetic vasoconstrictor activity and so combines the two effects.
Sympathomimetic, a term coined in 1910 by the English phar-macologists Barger and Dale, refers to a drug action that mimes the effects of activation of the sympathetic nervous system. This sym-pathomimetic action is partially the result of cocaine's ability to re-strict the reuptake of neurotransmitters such as norepinephrine and dopamine into the cells of the sympathetic nervous system.
One way by which the organism stops the action of sympathomimetic drugs is to pump the unused amine back into the cell ter-minal that released it. If by some mechanism this pumping or reuptake is blocked, the sympathetic effects are both enhanced and prolonged by the continued presence of the transmitter. Reuptake block is a property of many of the antidepressant drugs used in psy-chiatry that do not have the immediate stimulant and euphorigenic properties of cocaine. This implies that we cannot totally explain the central stimulant effect of cocaine simply by its known sympatho-mimetic action.
Most of the current interest in cocaine is concerned with its sym-pathomimetic action and stimulant effects. Sympathomimetic refers to peripheral effects on heart and blood vessels, whereas stimulant implies activation of the central nervous system. Caffeine, for ex-ample, is a stimulant but not a sympathomimetic. Cocaine is a typ-ical sympathomimetic drug in its peripheral effects. It increases blood pressure and heart rate and, in large doses, increases temperature. With high doses or regular use, the pupillary size is increased. Small arterial blood vessels are constricted, thereby restricting the drug's passage into the body when applied topically.
Cocaine, easily soluble in alcohol as the base or in water as the hydrochloride, has high fat solubility. This property makes it likely that it is quickly taken up into the brain from the bloodstream. The effects of cocaine in the brain and on the emotional state of the in-dividual may be in part governed by this rapid transfer. There is some evidence that brain concentrations of cocaine markedly exceed those in plasma.
Cocaine, like all local anesthetics, is a convulsant at high doses. Repeated small doses of cocaine in animals may eventually lead to convulsions. Some have postulated that this "kindling" effect, (i.e., repeated small doses eventually producing the equivalent response of a much larger dose) may account for the sudden appearance of psychosis in chronic users. Except for the heart rate increase, there is no effect on the electrocardiogram after 2 mg/kg cocaine admin-istered intranasally. At this dose there is no reliable dilatation of the pupil but there is a slight temperature increase. Larger doses increase pupillary size. It has been postulated that hyperthermia is a major reason for the deaths that have resulted from massive cocaine overdosage.
The psychological effects of cocaine described by Conan Doyle through Sherlock Holmes as "transcendently stimulating and clarifying to the mind" are less spectacular when examined in the laboratory.
In a dose effect study of intranasal cocaine (0.20, 0.75, and 1.50 mg/kg), our group found that higher doses produced higher peak plasma levels and more intense psychological effects.2 The peak psy-chological effects occurred within fifteen to thirty minutes after the drug was administered. In all our subjects, cocaine produced a "high" and pleasant feeling without any dysphoric effects. Javaid et al. in Chicago found that 10 mg of cocaine could not be differ-entiated from placebo, but doses of 25 and 100 mg produced eu-phoria.3 Some of the subjects in these experiments experienced dysphoria forty-five to sixty minutes after the 100 mg dose. The dys-phoria was characterized by anxiety, depression, fatigue, and a desire for more cocaine. A crash, or period of extreme discomfort and dys-phoria, reliably occurs after intravenous or smoked cocaine but is less common after intranasal use. This crash is not the model opiate withdrawal syndrome but obviously would encourage repeated self-administration of the drug.
Doses of 25 and 100 mg of intranasal cocaine produce increases in heart rate of 10 to 15 beats/minute, and in systolic and diastolic blood pressures of 10 to 20 mm Hg. These effects peak at fifteen to twenty minutes after drug administration. The size of these phys-iological changes is well within the changes seen in response to fear-ful or exciting stimuli.
A group at the University of Chicago found that their experimen-tal subjects could not distinguish the immediate effects of intrave-nous cocaine from amphetamine. At Yale we found that single intranasal doses of lidocaine, a synthetic local anesthetic, could not be differentiated from the same small dose of cocaine. Findings for chronic administration would probably differ.
Psychologists have determined that monkeys in an experimental situation will work for procaine (novocaine) injections (i.e., procaine is a reinforcing drug), and some recent reports indicate that procaine is perceived as a rewarding and pleasurable experimental stimulus by human subjects.
In the form of the hydrochloride salt, cocaine is readily absorbed through mucous membranes and enters the systemic circulation. The most popular route of administration is through the nasal mucosa, but almost any route is possible for cocaine.
Cocaine is broken down in the plasma by pseudocholinesterase, an enzyme responsible for breakdown of natural substances such as acetylcholine and drugs such as succinylcholine. We found that some individuals who, because of a genetic abnormality, lack pseudocho-linesterase activity also do not metabolize cocaine rapidly.
Cocaine has the reputation of being a short-acting drug. None-theless the half-life of cocaine in man is about an hour and its psy-chological effects persist much longer than the five to fifteen minutes that is commonly assumed. When the drug is applied locally in the nose, traces of the material are still present on the membranes hours after application. If the drug is applied repeatedly, damage to the nasal mucosa can occur.
If we look at the psychological effects of cocaine in relationship to plasma levels of the drug, we find that the effects are most marked as the plasma concentration is rising and the effects have almost dis-appeared on the descending limb of the plasma curve. This effect, seen with other drugs such as alcohol or the benzodiazepines, could be interpreted either as acute tolerance (i.e., the receptors once oc-cupied become less responsive), or as a redistribution phenomenon whereby the large initial plasma concentrations lead to a high brain level, which quickly diffuses out and equilibrates with the circulating drug.
Cocaine causes a "high." This drug effect is akin to euphoria or elation, but also contains elements of a sense of power or clarity of thought. This central effect, seen at moderate doses of cocaine, is accompanied by peripheral sympathetic signs, predominantly a heart rate and blood pressure increase that may in turn enhance the in-dividual's psychic state.
The smoking of cocaine paste, a crude derivative of coca leaves with 30 percent to 90 percent cocaine freebase, has become a new form of abuse among the urban youth of South America. In the United States a material refined from street "cocaine" (i.e., "free-base") is pyrolyzed in "base pipes" and inhaled through the lungs. When burned, cocaine is destroyed, but the hot gases from the smok-ing device vaporize much of the drug. Cocaine smoking causes a drug dependence with many of the characteristics of intravenous amphetamine use. There is an intense euphoria followed by a crash and an almost irresistible craving for more drug. An equivalently malignant form of abuse is the intravenous injection of cocaine hydrochloride.
Drug dependence on intranasal cocaine shows a pattern similar to other stimulant dependencies. An individual will use the drug in a "run" of continued use until supplies are no longer available. He may then not use the drug for long periods, but when it is available, he will use it. In contrast, smoking or intravenous use leads to almost continuous usage and drug seeking behavior. The strength of the drug dependence is related to the form and method of taking the drug.
Chronic use of cocaine produces sleeplessness, loss of appetite, and after high doses or long use, an uncomfortable anxious paranoid state. The question of whether cocaine produces a true psychosis re-mains moot, but there is increasing evidence that a hallucinatory par-anoid state can result from intense cocaine use.
There is reasonable evidence for tolerance to the cardiovascular effects of cocaine, and it is true that chronic users often take large doses, implying some degree of tolerance to the psychological effects of cocaine. This "tolerance" is, however, short-lived, since even heavy users will start off with small doses after a drug-free day.
It has been difficult to define a withdrawal syndrome from co-caine despite the reported crash involving a depressive state and in-creased sleep. This either could be a drug effect or simply a physiological response to any prolonged exciting or euphorigenic stimulus. Prolonged wakefulness often results in prolonged sleep when the reasons for the wakefulness are no longer present. This blurring of pharmacological withdrawal from the expected conse-quences of the drug-induced state makes it difficult to make un-equivocal statements about the importance of a withdrawal syndrome after cocaine usage.
Marijuana
Like cocaine, marijuana is a substance that has been known for centuries and used for its psychoactive effects in many societies. The pharmacology of the drug has been the subject of extensive reports and summaries and so only a brief account will be given here.4
The source of marijuana is the cannabis plant (Cannabis sativa) and the plant form is almost universally used without significant modification. There is some popularity of concentrated extracts such as hashish, but the use of the pure psychoactive ingredients is all but unknown outside the laboratory. Synthetic cannabis-like substances have been produced and some have a limited use in medicine. There are sixty-one cannabinoids unique to the cannabis plant but hundreds of other chemicals are also present. It is generally accepted that the primary psychoactive ingredient is delta-9-tetrahydrocannabinol (delta-9-THC or THC).
The most striking pharmacological effects of marijuana are on mind and behavior, and most of these can be duplicated with delta-9-THC. Marijuana is almost always smoked, usually in home-rolled cigarettes, but animal research depends usually on the administration of more pharmacologically pristine substances.
Smoking is an efficient method of drug delivery. Because of the large absorptive area of the lungs, the drug is quickly taken up into the bloodstream and reaches the brain within seconds. Cannabinoids are very soluble in fat and the brain is largely made up of fatty sub-stances. For this reason the drug is taken up into the brain prefer-entially. Over time the drug and its metabolites are redistributed throughout the body and slowly eliminated.
Because of the wide variety of marijuana plants and their varying content of THC, the dosage taken by average users is harder to eval-uate with marijuana than with cocaine. The smoking route of ad-ministration is also highly variable and is dependent on the experience and style of the user. Dosage is, of course, critical in evaluating pharmacological effect, but for marijuana only rough estimations can be made. These factors make it difficult to make meaningful parallels between laboratory experiments with marijuana and street usage.
Certain evidence is clear. Acute use of marijuana is highly unlikely to kill a person. The drug has almost no lethal potential. This makes it similar to tobacco in its acute effects and different from alcohol and heroin. Marijuana does resemble alcohol in some respects. It is a rapid onset intoxicant widely used in social situations, forbidden by some societies and accepted by others.
Marijuana is taken by users for the "high," as is cocaine. The high from marijuana is different from the cocaine high. Marijuana is sedative and cocaine is stimulant. They produce different types of pleasurable experiences and have different specific pharmacological effects and patterns of use.
Marijuana impairs motor coordination and accuracy of the exe-cution of movements. Various skills related to driving are impaired by usual street doses of marijuana. Attention is diminished. Single doses impair short-term memory. Modification of time sense is a re-liable effect of marijuana and is often sought by users as part of the drug experience.
In many ways marijuana resembles a mild sedative drug. It re-duces anxiety. It produces relative quiescence in users as well as a selective indifference to the environment. Marijuana, however, is different from the sedatives in many respects. The active pharma-cological substance is a hallucinogen in high doses. Marijuana and its metabolites tend to remain in the body and have residual effects for days to months. About a third of users report that while under the influence of the drug, they have had panic reactions, halluci-nations, changes in body image, and paranoid reactions. First-time users will occasionally have acute anxiety or fearfulness. Some peo-ple have an acute dysphoric (unpleasant) reaction to the drug and this has limited its medical usefulness. The reader should recognize that the medical usefulness of a drug is a red herring when one is considering the problems of street use. Many medically useful drugs are abused, and some totally innocuous drugs are "scheduled" as dangerous because of their chemical properties.
A major concern about long-term users of marijuana has been the occurrence of the so called "amotivational syndrome." Clinical re-ports on chronic users describe a washed-out state with apathy, dif-ficulty in carrying out plans, loss of ambition, and difficulty in concentrating. Acceptable scientific evidence has not established marijuana as a unique cause for such behavior, but one cannot ig-nore the repeated clinical reports of this syndrome in marijuana users.
The existence of large numbers of chronic daily users, particularly among the young, has led to the conceptualization of marijuana as an "addicting" drug. It does not have the use pattern of the opioids, but nonetheless some of the traditional characteristics of addiction can be shown for marijuana.
In 1946 tolerance to the psychological and physiological effects of marijuana were demonstrated in human subjects. When high doses were given, decreased effects on temperature, pulse, respiration, blood pressure, and mood state were seen after a few days of ad-ministration. It turns out that it is much more difficult to show such tolerance after exposure to lower doses, even for considerable pe-riods of time. This is but another demonstration that none of the drug properties are absolute at all doses.
After two weeks or more of administration of delta-9-THC every four hours, a moderate withdrawal syndrome with sweating, sali-vation, tremor, and irritability occurred.5 This evidence of depen-dence is of pharmacological interest but of dubious social policy significance. As with cocaine it is possible to demonstrate repeated self-administration of marijuana by humans in a laboratory as well as a naturalistic setting.
TERMINOLOGY OF "ADDICTION"
Marijuana and cocaine can to some degree fulfill the most rigid re-quirements for addicting drugs. They are rewarding, they will sup-port self-administration, there is demonstrable tolerance and physical dependence. Why then is there any doubt about their status? For both drugs the tolerance and physical dependence are not the driving forces behind the self-administration. It is also clear that there are many drug users who do not become either drug dependent or ad-dicted to these substances.
To responsibly answer the question about addiction for purposes of setting or defining policy, I will categorize the generally accepted evidence about cocaine and marijuana in respect to their pharma-cological properties, chronic and acute threat to individuals, epide-miology, and lastly their social and economic effects.
Although they share some characteristics with the opioid drugs, neither cocaine nor marijuana has a pharmacologically significant withdrawal syndrome that would, by its presence, enforce the con-tinued taking of the drug. This is not to say that withdrawal cannot be demonstrated; it can. Users do not continue involvement with the drugs primarily to avoid withdrawal.
Similarly, although tolerance to pharmacological effects can be demonstrated, neither cocaine nor marijuana creates a tolerance in human use that forces a significant increase in the amounts of drug taken by individuals. We do not see the form of continuous esca-lation in dosage characteristic of the opioid drugs.
Tolerance, physical dependence, and withdrawal are properties of many drugs that are not abused and are neither pleasurable nor rein-forcing. For example propranolol, a widely prescribed drug for heart problems, can produce each of these phenomena. We should be aware of, but not totally rely on, these characteristics in assessing the chronic human pharmacology of abused drugs. Even if cocaine and marijuana share some of these characteristics, it is important to note that drug seeking and drug taking behavior can be maintained at doses that do not cause noticeable tolerance or physical dependence.
Whether they harm all users, both cocaine and marijuana harm some users. The selection of "victims" is not biologically capricious but is dependent upon pharmacological variables; the health, per-sonality, physiology, age, and genetics of the individuals; social cir-cumstance; the chronicity and route of use; and the purity of the substances. Since these are often not quantifiable for an individual, it is possible to consider that a certain percentage of a population at risk will suffer some harm. Epidemiological studies to define that percentage are not yet satisfactory. We must therefore make gener-alizations based on inadequate studies and often flawed figures. A useful analogy might be to consider that one of every fifty cocaine users will become involved in compulsive use. We have no way of telling which one will become the victim. This means that it will ap-pear that many casual users can "get away with it," but at the same time every first-time user takes a risk that can be quantified. The time course of development of compulsive drug use is such that this dependency may not become apparent for a year or so after initial regular exposure, or it may occur rapidly. The existence of users who have not become overwhelmingly involved with the drug lends cre-dence to the mistaken thought that cocaine is "safe." A similar sit-uation exists for marijuana, but the population at risk is much greater, supplies of the drug are cheaper, and the young population may be more vulnerable because of their developmental stage.
From the above it should be clear that cost of drug and availability of supply are also critical variables in the resultant drug problem. These are economic parameters. Human, social, pharmacological, political, and economic factors determine the importance of a drug problem. The magnitude of that problem decides whether we refer to particular drug use as "addictive." Addiction is viewed by the public as a societally harmful state resulting from an evil property of a drug.
Each of these drugs can, in some populations, produce drug de-pendencies that meet all the commonly accepted attributes of addic-tion. In that sense they are addicting. Each of these drugs can produce harm to individuals in particular groups, depending on the characteristics of the individuals, the dosage, the form, and the chronicity of drug usage. In that sense the drugs also meet the im-plied quality of addiction in that they can cause harm. For both co-caine and marijuana, the societal impact of significant groups of drug dependent persons is considerable. For both drugs, the economic ef-fects and criminal involvement with trade are important factors in using the pejorative "addicting." Despite these congruencies with the term addiction, it is necessary to be aware that there is a behav-ioral spectrum around every drug of abuse. We must consider the situation of the drug user or abuser before he takes a drug, we must consider the behavior when he is taking a drug, and lastly we must consider the behavior consequent to the drug ingestion.
Some drugs are more reinforcing than others. Some drugs are more pleasurable than others. Some drugs have a higher dependence lia-bility than others. An agreed-upon set of definitions for a society is necessary before one can establish whether, within the spectrum of misused drugs, some drugs are more "addicting" than others.
WORDS DESCRIBING ATTITUDES TOWARD ADDICTION
The National Institute of Drug Abuse in 1982 assembled a group of definitions for drug abuse research.6 The definition of addiction quoted in part below is a starting point for discussion.
ADDICTION: From the Latin verb "addicere," to give or bind a person to one thing or another. Generally used in the drug field to refer to chronic, compulsive, or uncontrollable drug use, to the extent that a per-son (referred to as an "addict") cannot or will not stop the use of some drug. Beyond this, the term is ambiguously used with a wide variety of often arbitrary meanings and connotations; sometimes interchangeably with, sometimes in contrast to, two other ill-defined terms, HABIT-UATION and (DRUG) DEPENDENCE, the former imprecisely refer-ring to some lesser form of chronic drug use, the latter capable of being either of psychological or physical origin, often in varying combinations depending on the drug. It usually implies a strong (PSYCHOLOGICAL) DEPENDENCE resulting in a WITHDRAWAL SYNDROME when use of the drug is stopped. Many definitions place primary stress on psy-chological factors, such as loss of self-control and overpowering desires; i.e., addiction is any state in which one craves the use of a drug and uses it frequently. Others use the term as a synonym for physiological depen-dence; still others use it as a combination.
The primary popular stereotype, what has been called the "classical definition of addiction," is that it is an extraordinarily debilitating vice or disease—even an evil and sinful state—rooted in the invariable pharmacological effects of a drug on the human body, an irrevocable process that involves the presence of tolerance and results in a with-drawal syndrome that can be avoided only by total abstinence.' The clas-sical definition of addiction further links this phenomenon particularly to the OPIATE NARCOTICS. Like the popular concept of narcotics, this classical definition emerged in the 1920s out of a blending of popular and scientific terminology laden with emotional and imprecise meanings. The term "addict" began to be increasingly stigmatized and used by both the scientific and lay communities to express that the compulsive use of opiates was not just a bad habit but was worse both to the individual and society than other forms of habituation, such as to tobacco and alcohol, and resulted in debility, insanity, crime, and death.
Consultation with the Oxford English Dictionary shows that in 1597 Shakespeare is the source of the first quote that mentioned a drug (alcohol) in relationship to the word addicted. He wrote, "To forsweare thinne Potations and to addict themselves to Sack" (Sec-ond Part of Henry IV, act 4, sc. 3).8 Of course the word is much older than that and it is only recently that addiction can once again be used to refer to alcohol. Shakespeare was probably using the term in the sense of "to devote to," but he did find ethanol more appro-priate than books to team with the verb addict.
Although the first meaning of addict in Webster's Ninth Colle-giate Dictionary is "one who is addicted to a drug," the definition of addiction gives "the quality or state of being addicted (to read-ing)" as a first meaning.9 Webster gives for the second meaning "compulsive physiological need for a habit forming drug (as her-oin)." The analogy is an opiate and the emphasis is on physiological need. One definition of the verb addict in the Oxford English Dic-tionary gives "to devote, give up, or apply habitually to a practice. (A person addicts his mind, etc., or his tastes addict him.)" This strikes to the major point that generates wobbly semantics around the word addiction. Do drugs addict people or do people addict themselves to drugs? The state of addiction in all senses requires both an activity, or drug, and a population at risk. Are the drug char-acteristics or the population characteristics more important? This chapter focuses more on drug characteristics than on the many pop-ulations who might be considered. Despite this emphasis, addiction is not a problem without addicts.
When we speak of addiction, our interest is in humans and their behavior in their environment. The definition of the term is most meaningful for humans. There are, however, terms used in phar-macology that are associated with addiction and that can best be quantified in animal experimental situations. To make the descrip-tion of cocaine and marijuana more useful, I will first give defini-tions of some words used in describing the results of chronic drug-taking behaviors.
Reinforcement is a term most frequently used in animal behav-ioral pharmacology. In that context it is a measure of whether, and how hard and long, an experimental animal will "work" for ad-ministration of a drug. The animal experiments are therefore not subject to the variables of human societal influences. They are, how-ever, both route- and dose-specific. Standard methods for the mea-surement of reinforcement are well established. The first question is whether a drug will be self-administered by animals or humans. For example delta-9-THC, the pharmacologically active ingredient of marijuana, is a poor reinforcer as measured by the response rates of animals. Despite this the drug's enduring popularity among humans indicates that the animal experiments are missing some important characteristics of the human situation. Cocaine on the other hand is a powerful reinforcer, and one might conclude that the current ex-treme popularity of the drug is primarily the result of this property. The historical evidence indicates that there have been times when cocaine was simply not a major drug-abuse problem. It has been available in South American countries for many years and was not perceived as a public health problem. The fact that this is no longer true is obviously not the result of a change in the drug but in the perception of its desirability as a self-administered substance. Rein-forcing properties are only one factor in the equation of "addiction."
Tolerance was once considered to be a requirement for addictive drugs but experience has changed this viewpoint. One should re-member that the model for addiction has always been the opioid or narcotic drugs. The pharmacological characteristics of this group have been assumed to be a model, and this misconception has led to most of the semantic difficulties around the concept of addiction to other drugs. There are several variants of tolerance, which are de-scribed in the following definitions.
Tolerance in general is the phenomenon of decreased responsive-ness to a specific effect of the same dose of a drug as a result of prior exposure to the drug. When the same decreased responsiveness is seen after administration of a different drug, the phenomenon is known as cross-tolerance. A parallel terminology is used for depen-dence, i.e., a dependence on one drug can be supported with another in the same class. For example, methadone shows cross-tolerance and cross-dependence with morphine. Sometimes the reverse phenom-enon is seen; there is increased responsiveness to an effect of a drug as a result of prior exposure. This is called reverse tolerance or sen-sitization. Acute tolerance can be seen on a single administration of a drug and refers to an observation of less effect at the same ap-parent plasma level of a drug when the drug level is falling compared to the effect when the level was rising. The mechanism that produces the tolerance may be related to the metabolism of the drug or its interaction with receptors. If a drug increases its own metabolism and thereby decreases the effect of successive doses, this is known as dispositional tolerance. If the reason for the decreased respon-siveness is not the result of metabolism, it is known as pharmaco-logical tolerance or pharmacodynamic tolerance or adaptive tolerance or functional tolerance. Sometimes there is a change in sen-sitivity to a behavioral effect of a drug as a result of prior exposure to the drug. This is known as behavioral tolerance and may not be-come apparent until the behavioral test is given.i°
Dependence is a separate characteristic from tolerance and, in both pharmacological and common usage, has been combined with many modifying terms. The distinction often made between psychological and physical dependence is hard to define in operational terms. My discussion of this terminology draws heavily from a 1984 document by the Committee on Problems of Drug Dependence." The term itself is used in both biological and behavioral contexts. Biologically the term is used to describe the biochemical and physiological con-sequences of repeated exposure to a drug and is often intertwined with the concept of tolerance. This biological definition is synony-mous with the term neuroadaptation as used in the World Health Organization's memorandum on nomenclature and classification.'2 This "neuroadaptation" is, for the most part, inferred from the appearance of a withdrawal syndrome when either the drug is with-drawn or a specific antagonist to the drug is given. "Neuroadapta-tion" does not involve behavior and it is possible to exhibit dependence when there is no evidence of neuroadaptation. Depen-dence in this broader sense refers to the physiological and behavioral effects that occur when drug administration is stopped after a period of repeated exposure to the drug.
Neither tolerance nor dependence is a necessary concomitant to "drug abuse." Drug abuse is a societally relative term, which is as unsatisfactory for science as it is necessary for society. The words become tangled in inconsistencies. Expert committees have often at-tempted without success to reach a universally acceptable definition. The WHO expert committee of 1969 defined drug abuse as " . . . persistent or sporadic excessive drug use inconsistent with or unre-lated to acceptable medical practice." The WHO committee of 1981 criticized this and commented, "Since alcohol is not usually pre-scribed by the medical profession, then any excessive use would be abuse. But then what is excessive?" They then suggested a division into (a) unsanctioned use, (b) hazardous use, (c) dysfunctional use, and (d) harmful use." Whatever the semantic distinctions, it seems that drug abuse, sanctioned by an institute name, is here to stay, and "addiction" is etymologically incurable.
We must deal with the terms as they are but have a recognition that the ambiguities will always confuse communications. In those instances we can drop back to the more precise definitions of phar-macology as sanctioned by textbooks and the World Health Orga-nization. In our present use of the language, addiction has a pejorative connotation in some—but not all—contexts. It sounds "right" with some subjects and not others. For example a sports addict is all right; a videogame addict is questionable. A cigarette addict sounds wrong, but a marijuana addict sounds more fitting. The natural modifier seems to be heroin. There is nothing seman-tically distressing about a heroin addict. "He is addicted to good books and fine wine," is in no way a pejorative statement and would be acceptable colloquial American English.
Is there a relationship between the terminology of addiction and the concept of dangerousness? This is the case with public acceptance of undesirable activities, e.g., sports are not dangerous but video-games might "rot the mind." In a consideration of marijuana and cocaine, an examination of danger is in order. "Dangerous Drugs" is an alliterative and acceptable combination of words that comes easily to the typewriters of reporters. What do we think of? Heroin, once again, and cocaine. Not marijuana and probably not cigarettes. Almost certainly not alcohol. In the perception of the reader, neither cigarettes nor alcohol is a drug and so cannot be subsumed under the terms.
The use of the term drug should also be examined. In common parlance, a drug is a drug of abuse. Substances like alcohol, clearly drugs to the pharmacologist, are considered to be something else to the public. "Dangerous drugs" is often true when referring to the self-administration of substances. Dangerous behavior with chemi-cals is more descriptive of the reality.
Danger can be a threat to the individual, to his immediate surround-ings, or to society in general. It can be the result of acute or chronic usage of a drug. If an addiction is not considered dangerous in any way, the use of the term is neutral. Sports addicts are not con-demned. Heroin, the prototype, can be acutely dangerous to the in-dividual by a direct pharmacological respiratory depressant action. The intravenous route of administration is inherently chronically dangerous because of possibilities of contamination of needles and syringes. Marijuana is acutely dangerous to a much lesser degree. The intoxication by marijuana can impair driving performance, but death by overdosage is not a possibility in ordinary usage. The smok-ing route of administration and the natural plant form of dosage limit the possibilities of acute harm. There is still a debate on whether marijuana is chronically dangerous to the individual, but the prob-abilities are that any substance delivered to the lungs by smoking will turn out to have a significant risk. Societal danger from the use of marijuana is related to the population group at risk, the young. We see here that pure pharmacological factors are often not the issue. Who uses what, when, and how—these are the issues that often cre-ate the questions of risk. Cocaine, too, exemplifies the population and environmental factors in assessing dangerousness. Its usage, for-merly limited, now has spread through all society. The youth of the country are not the major consumers. A high middle-class involve-ment in the use of the drug causes a different danger to society. The acute effects of the drug in ordinary dosages by the intranasal route are not considered "dangerous" by many authors. The threat to the individual from overwhelming involvement with cocaine use can be considerable. This is more because of psychological and social fac-tors rather than any health effects of the substance. Heavy use can cause health effects, but this is rare. The health effects of smoking and intravenous usage are less properties of the drug than charac-teristics of anything taken by these routes.
We do not know what percentage of casual users become inten-sively involved with cocaine use, nor do we know how to identify the population at greatest risk. As with many substances, the risk is statistical; some people get away with it and others don't. Of course the first-time user always assumes he will not become one of those who is damaged by the drug. The most conservative strategy is to condemn all self-administered drug use. Despite this, can we call all self-administered agents "addicting"? The term is so broadly used that this might be an acceptable but probably useless exercise.
A REASONABLE USE OF WORDS
Given the understandable meaning of addiction as equivalent to a pejorative version of WHO's "drug dependence," why has any con-fusion ever developed about marijuana and cocaine? First, the def-inition of drug dependence, "a socio-psycho-biological syndrome manifested by a behavioral pattern in which the use of a given psy-choactive drug (or class of drugs) is given a sharply higher priority over other behaviors which once had significantly greater value [i.e., drug use comes to have a greater relative value]. . . . A key descrip-tive element is the priority given to drug-seeking over other behav-iors."'4 This is a semantic mouthful but anyone who has ever examined serious marijuana or cocaine users will have no trouble matching them up to the definition.
The difficulty has developed over an ambivalence about certain drug usages that are accepted by society 'and are thus not appropri-ately condemned by the harsh word "addiction." When this situa-tion occurs, the definers of words look for loopholes. Tolerance and dependence used to be loopholes for cocaine and marijuana. That was in the late sixties and early seventies, when a generation accus-tomed to marijuana use and unaware of the dangers of cocaine use felt that these were safe additions to the armamentarium of pleasure. The broad middle-class use of these drugs required that they be la-beled as safe in as many ways as possible. The media, certainly in-cluding some chemical habitues, made every effort to minimize the risk of drugs. In 1943 Life magazine, using the word narcotics in a pharmacologically incorrect fashion in its article title, said, "Co-caine, extracted from the leaves of the tropical coca bush, and mar-ijuana, the resin of the ubiquitous hemp weed, are not physiologically habit-forming but they get their users into more immediate trouble. The "snowbird" (cocaine sniffer) and "hay-burner" (marijuana smoker) are carried off into a state equivalent to deep alcoholic in-toxication. In this state, which is characterized by irresponsible vio-lence, the swing musician ascends to new peaks of virtuosity and the ordinary criminal becomes a spectacular public enemy."15
This quote, typical of the time, is almost entirely incorrect in its description. Even in the early years of the eighties, deliberate or care-less misquotations were used to advance the idea that cocaine, for instance, was not "addicting.,916
We need condemnatory words to speak of behaviors we do not like. We also need descriptive terms that are accurate. It is humanly necessary to have summary terms that give both description and opinion. Addiction is such a term. Drug dependence can be defined with less emotion but still carries the stigma of societal disapproval. Is the diabetic drug-dependent? The answer "no" seems obvious, because diabetes is an accepted disease that is being self-treated by the patient's use of insulin. We have chosen to make the traditional drug dependencies diseases as well, thereby blurring the distinction. The discovery of the enkephalins and endorphins, providing a bio-logical basis for a need for opiates, has further blurred the semantic picture. In the novel Nineteen Eighty-four George Orwell described a new set of languages. The "C" language was used by technicians and scientists and contained unambiguous meanings. The pharma-cological definitions presented in this paper are in the "C" language, but the word "addiction" has all the characteristics of Newspeak.
The difficulties in understanding can be exemplified by the sum-mary of drug characteristics shown in Table 6-1. I have attempted to compare cocaine and marijuana with two legal but dangerous drugs, cigarettes and alcohol; two older drug-abuse problem centers, barbiturates and the hallucinogens (LSD and similar drugs); the pro-totype of addicting drugs, heroin; and one of the most widely pre-scribed prescription drugs, propranolol. The scores given in the table are based on an interpretation of the published literature but prob-ably would be concurred with by most experts. To summarize in this way, I have had to compress some definitions. In the table, "Tol-erance" is a sum of all forms of tolerance. "Physical Dependence" is a measure of both the range of effects where physiological with-drawal can be demonstrated and the intensity of the combined with-drawal syndromes. "Self-Administered" is an estimate of the ease of making experimental animals administer the drug to themselves by any route. "Reinforcement" as used in the table is a relative mea-sure of the amount of work animals in an experimental situation will do to receive a single dose of the drug. "Acute Toxicity" is the prob-ability of physical damage to an individual from all causes as the result of less than a single day of self-administered drug. "Chronic Toxicity" is a combination of the probability of and seriousness of the effects of each of these drugs when given or taken for periods of months to many years. "Problem Today" is my estimate of the net social, individual, political, and economic significance of the widespread use of this drug in the United States in 1985.
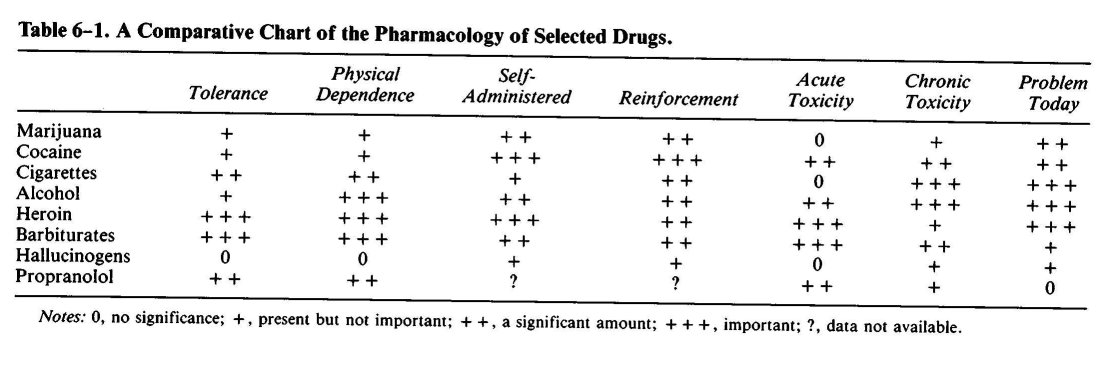
The reader should note that by summarizing ideas in a table, I have immediately destroyed the concept of accurate definition in de-scribing drugs of abuse. This sort of summation is only an insignif-icant version of the condensation of the popular press. If you do not have the table, I cannot condense a wide range of information about drugs. If you do have the table, you will to some degree be misled by the information.
Given these shortcomings, what is the substance of the impression created by the table? First, tolerance and physical dependence as drug characteristics have little to do with the magnitude of a drug abuse problem. Second, reinforcement potential also is poorly related to the problem today. Third, acute and chronic toxicities are not related to society's acceptance of drug usage.
Rules, regulations, and laws are based on the degree of conden-sation of information that can be held in the minds of the rule mak-ers. Unfortunately, there are no simple definitions of drug characteristics that lend themselves to law or policy making. The be-havior of individuals in their interaction with drugs makes rule mak-ing even more frustrating.
This chapter started with the assertion that cocaine and marijuana are addicting and that some drugs are more addicting than others. It should end with a realization that the question is not clear but the answers are.
1. J . H. Jaffe, "Drug Addiction and Drug Abuse," and J. M. Ritchie and N. M. Greene, "Local Anesthetics," both in A. G. Gilman, L. S. Goodman, and A. Gilman, eds., The Pharmacological Basis of Therapeutics, 6th ed. (New York: Macmillan, 1980), pp. 535-84 and 300-320 respectively. See also, R. Byck and C. Van Dyke, "What Are the Effects of Cocaine in Man?" in R. C. Petersen and R. C. Stillman, eds., Cocaine 1977, National Institute on Drug Abuse (NIDA) Research Monograph 13 (Rockville, Md.: DHEW, 1977), pp. 97-117; Institute of Medicine, Marijuana and Health (Washington, D.C.: National Academy Press, 1982).
2. C. Van Dyke et al., "Intranasal Cocaine: Dose Relationships of Psychological Effects and Plasma Levels," International Journal of Psychiatry in Medicine 12, no. 1 (1982): 1-13.
3. J. I. Javaid et al., "Cocaine Plasma Concentration: Relation to Physiological and Sub-jective Effects in Humans," Science 202 (1978): 227-28.
4. J. H. Jaffe, "Drug Addiction and Drug Abuse"; Institute of Medicine, Marijuana and Health.
5. N. L. Benowitz and R. T. Jones, "Effects of Delta-9-tetrahydrocannabinol on Drug Distribution and Metabolism," Clinical Pharmacology and Therapeutics 22 (1977): 259-68; R. T. Jones, N. L. Benowitz, and R. I. Herning, "Clinical Relevance of Cannabis Tolerance and Dependence," Journal of Clinical Pharmacology 21 (1981): 143s-52s.
6. J. E. Nelson et al., eds., Research Issues 26: Guide to Drug Abuse Research Terminology (Rockville, Md.: USPHS [NIDA], 1982); Webster's Ninth New Collegiate Dictionary (Springfield, Mass.: Merriam-Webster, 1983); Oxford English Dictionary, s.v. "addiction."
7. S. Peele, "Redefining Addiction. I. Making Addiction a Scientifically and Socially Useful Concept," International Journal of Health Services 7, no. 1 (1977): 103-24. (Cited in Nelson et al., eds., Research Issues 26.)
8. Quoted in the Compact Edition of the Oxford English Dictionary, vols. 1 and 2 (New York: Oxford University Press, 1971).
9. Webster's Ninth New Collegiate Dictionary.
10. N. A. Krasnegor, ed., Behavioral Tolerance: Research and Treatment Implications, NIDA Research Monograph 18 (Washington, D.C.: Government Printing Office, 1977).
11. J. V. Brady and S. E. Lukas, eds., Testing Drugs for Physical Dependence Potential and Abuse Liability, NIDA Research Monograph 52 (Washington, D.C.: Government Printing Office, 1984).
12. World Health Organization (WHO), "Nomenclature and Classification of Drug- and Alcohol-Related Problems: A WHO Memorandum," Bulletin of the World Health Organi-zation 59, no. 2 (1981): 225-42.
13. Ibid.
14. Ibid.
15. G. Piel, "Narcotics: War Has Brought Illicit Traffic to All-Time Low but U.S. Treasury Fears Rising Postwar Addiction," Life, July 19, 1943, pp. 82-84, 86, 88, 91-92, 94.
16. R. Byck, "History and Sociology of Cocaine Use and Research: Three Histories of Cocaine," in S. Fisher and U. Ulenhuth, eds., Cocaine: Clinical and Biobehavioral Aspects (New York: Oxford University Press, 1986).
| < Prev | Next > |
|---|