| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 189 |
| Yesterday: | 251 |
| This Week: | 189 |
| Last Week: | 2221 |
| This Month: | 4777 |
| Last Month: | 6796 |
| Total: | 129376 |
Cannabis Use in Canada
 |
|  |
| 
| Books - Cannabis and Culture |
Drug Abuse
ABSTRACT
The history of cannabis in Canada extends back to the early 17th century, but non-medical use can be conclusively documented only to the 1930s and popular use to the mid-1960s. Cannabis was first legally prohibited in 1923; criminal penalties for illegal possession, importation, cultivation and trafficking have increased in severity. Convictions of marihuana and hashish doubled annually from the mid-1960s until 1970, and have continued to rise, although at a less dramatic rate of increase, since 1970.
Marihuana and hashish are both routinely available throughout Canada, but the quantity and quality are insufficient to satisfy the demands. Consequently, both mari-huana and hashish are smuggled into Canada by sophisticated, criminally-oriented organizations dealing in hundred-pound shipments, and by youthful non-professionals importink§mall amounts.
The non-medical use of cannabis was primarily restricted to college-aged persons of middle-income families in the mid-1960s, but was quickly diffused to older and younger persons of all class levels. Today, Canada's cannabis-using population appears to increasingly mirror the social characteristics of the general population. Although cannabis users typically take other drugs as well, it is not clear to what extent the use of cannabis adds to, or substitutes for, the use of other drugs such as alcohol.
This paper presents the personal opinions of the authors and does not necessarily reflect the official position of the Commission of Inquiry into the Non-Medical Use of Drugs.
The preparation of the manuscript by Lynn Bryan and the editorial assistance of Linda Wright are gratefully acknowledged.
SOCIAL AND LEGAL HISTORY
The history of cannabis in North America began in 1606 with experimental cultivation in Nova Scotia (then Nova Francia) by Louis Hébert, who was Samuel de Champlain's apothecary. Commercial hemp cultivation was established soon after throughout both French and English New World colonies, encouraged by various systems of legal penalties and incentives. Hemp was considered to be an essential crop for both domestic require-ments such as clothing and cordage, and for the colonial powers' naval needs such as sails and rigging (Barash 1971). Commercial hemp produc-tion remained a viable industry only until the late 18th or early 19th cen-turies. Limited cultivation, however, continued in Canada until the early 1930s, when economic developments rendered hemp production an un-profitable enterprise. Unauthorized cannabis cultivation was legally pro-hibited in 1938, and all hemp fiber used in Canada since has been imported. Untended cannabis, generally of low potency, still grows in several pro-vinces, particularly in parts of Quebec where extensive hemp cultivation occurred a century or more ago. While early Canadian settlers were quick to exploit the agricultural and industrial potential of hemp, it was not until the 20th century that the psychotropic properties of cannabis were generally recognized.
Although cannabis apparently did not play an important'' role in Canadian medical practice, cannabis preparations were used in conjunc-tion with the treatment of a variety of ailments until relatively recently. Several over-the-counter remedies (primarily cough syrups, sleeping po-tions and corn removers) were available until 1939, and cannabis-con-taining medicines were produced for prescription use until 1954. Medical prescribing of cannabis is not prohibited, but there is presently no licit production of cannabinoid medicines. However, old stocks of some canna-bis-containing preparations still exist in certain pharmacies.
There are no reliable accounts of the non-medical use of cannabis in Canada which predate the 1930s. The Canadian Medical Association Journal first warned of "The Increasing Menace of Marihuana" in 1934 and reported the rising use of the drug in Ottawa, Toronto, Windsor, Montreal, and British Columbia (Canadian Medical Association 1934a). While there may have been small groups of users in these and other areas during the 1930s, cannabis use was not the subject of notable police or media attention until some thirty years later. Dominion Bureau of Statis-tics calculations, for example, show only twenty-five convictions for mari-huana possession in all of Canada betvveen 1930 and 1946, compared to over nineteen hundred convictions for possession of opiates during this period (Josie 1948). According to the Royal Canadian Mounted Police, who are entrusted with enforcing Canada's narcotic legislation: "Prior to 1962, isolated cases of cannabis use were encountered, but generally in con-nection with entertainers and visitors from the United States. Although marihuana arrests were effected sporadically in the middle 40s, its use on a more frequent basis appeared in Montreal only in 1962, in Toronto in 1963 and in Vancouver in 1965" (Royal Canadian Mounted Police 1969).
Marihuana smoking, however, was supposedly in vogue in the artistic community of Vancouver in the late '50s (Paulus and Williams 1966), and Toronto researchers have estimated that there were about fifteen hundred cannabis users in that city by 1960, and that some middle-class profession-als, entertainers and para-criminal persons in Toronto had been smoking marihuana or hashish since the early 1950s (Coleclough and Hanley 1968).
It appears that cannabis use did not develop as quickly or as extensively as in the United States. The virtual explosion of such use in Canada during the mid-'60s was apparently imitative of American developments and a product of the same social forces — such as the evolution of the psychedelic ethos, the mass media's publication of the drug, and the growth of under-ground newspapers — that can be considered to have contributed to the American situation. In 1962 the Royal Canadian Mounted Police reported only 20 cases connected with cannabis. In 1968 the number of cannabis-related cases had risen to over 2,300, and in 1972 there were nearly 12,000 cannabis convictions in Canada (Royal Canadian Mounted Police 1973).
The supposed dangers of cannabis have been sensationally described by the early Canadian feminist, Emily Murphy (1922), or "Janey Canuck," an Edmonton juvenile court judge and magistrate, in a chapter of her book The black candle devoted to "Marijuana — the new menace." This often racially biased monograph presented various flamboyant de-scriptions of the effects of cannabis which contributed to the prevailing marihuana mythology of that time. Quoting extensively from a letter writ-ten by the Chief of the Los Angeles Police, Murphy stated :
Persons using this narcotic smoke the dried leaves of the plant,which has the effect of driving them completely insane. The addict loses all sense of moral responsibility. Addicts to this drug, while under its influence, are inunune to pain.... While in this condition they become raving maniacs and are liable to kill or indulge in any form of violence to other persons, using the most savage methods of cruelty without, as said before, any sense of moral responsibility.
When coming from under the influence of this narcotic, these victims present the most horrible condition imaginable. They are dispossessed of their natural and normal will power, and their mentality is that of idiots. If this drug is in-dulged in to any great extent, it ends in the untimely death of its addict.
Murphy's book had an almost immediate influence on Canadian legisla-tion. One year after its publication — without any scientific evidence or sense of public urgency, and without any explanatory or rationalizing discussion in Parliament —"Indian Hemp "was included in the Schedule of the Opium and Narcotic Drug Act in 1923, and has been legally classified with the opiate narcotics ever since. Thus, cannabis was made illegal in Canada ten years before any empirical evidence of its non-medical use emerged, and fourteen years before federal legislation regarding cannabis was first adopted in the United States, where regional but widespread use had been extensively publicized since 1910 (Cook 1964).
The inclusion of cannabis in the opiate narcotic schedule, and later in the Narcotic Control Act (1961), has meant that occasional increases in the severity of penalties for narcotic offences have been automatically applied to cannabis as well. This situation prevailed until 1970 when the Narcotic Control Act was amended to allow the Crown to proceed by way of "indictment" or "summary conviction" in the case of unauthorized simple possession of cannabis. The indictment procedure was formerly the only option available and provides for a maximum sentence of seven years' imprisonment, while a summary conviction (similar to a misdemean-or in American courts) provides for a maximum sentence of six months' imprisonment and/or a fine of one thousand dollars for the first offense and one year's imprisonment and/or a fine of two thousand dollars for subse-quent offences. Since 1972, because of recent revisions in the Cinadian Criminal Code, persons convicted of cannabis possession offenses have sometimes been sentenced to "absolute" or "conditional" discharges which involve no fines or imprisonment and allow for the expungement of criminal records related to the offense after a one-year period without further convictions. However, most simple possession convictions result in fines (e.g. $ 150.00).
The penalties for cannabis-related offenses beyond simple possession have not, as yet, been legislatively altered or separated from the legisla-tion controlling opiate narcotics. Possession for the purpose of trafficking and trafficking itself carry maximum sentences of life imprisonment ; un-authorized importation or exportation provides a minimum sentence of seven years' imprisonment and a maximum sentence of life imprisonment; and unauthorized cultivation carries a maximum sentence of seven years' imprisonment. These maximum sentences have never been awarded in the case of cannabis offenders, but unlike the situation with simple possession the majority of persons convicted of trafficking and intent-to-traffic offences are still imprisoned. Importation convictions necessitate a mini-mum sentence of seven years' imprisonment (which may be reduced by parole), and between a third and a half of those annually convicted of il-legal cultivation of cannabis are sentenced to jail or prison terms. Generally speaking, sentencing is far less punitive today than it was during the mid and late 1960s for all cannabis-related offences. However, a consistent, humane and truly realistic legal control model must await the long-promised rewriting of Canadian drug legislation.
In May 1969 the Government of Canada appointed the Commission of Inquiry into the Non-Medical Use of Drugs (the "LeDain Commission"). The Commission has published an Interim report (1970), Treatment report (1972a), Cannabis report (1972b) and Final report (1973) in both French and English. The present paper is based primarily on studies con-ducted while the authors were members of the Commission research staff.
AVAILABILITY AND DISTRIBUTION
Marihuana and hashish are both routinely available throughout Canada, although the former predominates in the West Coast, and the latter is more common in the more Eastern provinces (Commission 1972b). For example, hashish was reported as the "most readily available" drug by three times as many cannabis-usingu niversity students as those who named marihua-na, British Columbia being the only province where marihuana was claimed to be more easily available than hashish. In most regions of the country high school students reported that the two forms of cannabis were about equally available to them, but in Ontario hashish was reportedly most com-mon, and in British Columbia marihuana was most frequently encountered (Lanphier and Phillips 1971). These data suggest that age, education, and/or social class may be significant factors in determining the relative availability and use of hashish and marihuana. Little research has been directed specifically at this question, but, with this exception, our own social and behavioral studies suggest that the two forms of cannabis are generally used interchangeably in Canada, and that the patterns of use, so-cial characteristics of the users, the general effects of the drugs and the avenues of initiation to use are essentially the same for both. The Canadian experience is significantly different from' that of the United States where hashish is relatively less frequently encountered.
In Canada, cannabis is rarely adulterated with other drugs, although various plant materials are sometimes represented as marihuana or are used to dilute or "cut" it. In our national survey of non-forensic "street drug" analysis facilities, and our collection of illicit drug samples, more than three-quarters of those samples presented to the analyst as hashish or marihuana were what they had been alleged to be ; almost all of the remain-der were inactive substances (Miller et al. 1973; Marshman and Gibbins 1970; Commission 1972b, 1973). The drugs submitted to non-forensic facilities for analysis are often those suspected of being in some way un-usual; consequently, these studies likely contain a disproportionate number of deviant samples and the data cannot be considered representative of the cannabis generally available in Canada. Tetrahydrocannabinol (THC), the principal active constituent in cannabis, has never been found in isolated form on the illicit market — most of the alleged THC samples analyzed were actually phencyclidine (PCP). Liquid cannabis extract or concentrate ("hash oil") has become intermittently available during the past two years.
The THC content of cannabis in Canada varies over a wide range, with typical values of approximately 5% and 0.6% Δ9 THC for hashish and marihuana respectively (Miller et al. 1973.). With the appropriate seeds, marihuana with high THC content can easily be grown in this country, although much of the domestic material on the illicit market seems to be of rather low potency (Commission 1972b ; Small 1971). Sometimes at-tempts are made to artificially improve the potency of marihuana. Some of these measures include moistening and burying for several days, boiling for several hours, storing with dry ice, or exposing the marihuana to ultra-violet lamp rays.
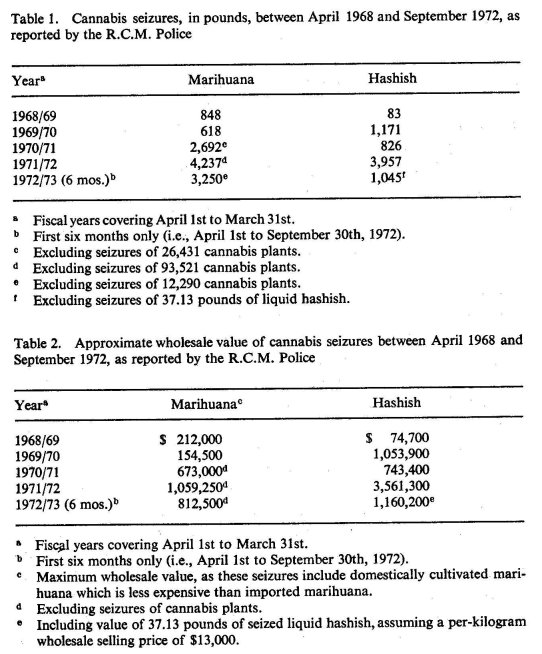
Royal Canadian Mounted Police (1973) statistics indicate that while the total weight of both marihuana and hashish seized annually has risen considerably since 1968, there has been a relatively greater increase in the hashish figures (See Table 1). The marihuana seizures include some do-mestically cultivated samples as well as imports, although many plant seizures are not included in the total weight figures. If these quantities are converted to their wholesale Canadian value (assuming a current per-pound selling price of $ 900 for hashish and $ 250 for marihuana), the im-portance of hashish becomes even more apparent (See Table 2).
On the other hand, the Federal Health Protection Branch (HPB) drug laboratories, which conduct most of the forensic drug analysis in Canada, report having analyzed more police seizure exhibits of marihuana than of hashish over the past three years, and that the predominance of marihuana exhibits is increasing (Canada 1973). Unfortunately, these two sets of seizure statistics come from different sources within the government and are not directly comparable. It may be that the R.C.M.P. hashish weight totals (Table 1) contain some very large seizures intercepted in Canada, but which were ultimately bound for the United States market. In contrast, large shipments of marihuana going to the U.S. are much less likely to be routed through Canada and therefore probably would not enter into the Canadian seizure statistics. Most of the individual exhibits analyzed by HPB apparently involve relatively small drug quantities seized in connec-tion with simple possession cases.
If the assumption were made, however, that the bulk of the cannabis seizures were destined for the Canadian market, and that law enforce-ment authorities are able, at best, to sein approximately ten per cent of the cannabis in Canada, then it would appear that trafficking in marihuana and hashish is at least a forty million dollar a year business at the whole-sale level alone. Final Canadian retail sales of marihuana and hashish might, in this case, account for between 75 and 100 million dollars annually.
The Canadian cannabis distribution system is far less tightly organized than some other illicit drug markets (e.g., heroin), is subject to sudden and drastic changes in structure and personnel, and, until recently, was relatively uninfected by professional criminal elements. Traditional criminal organizations have become increasingly involved in the financing and actu-al importation of large-scale hashish shipments, but most of the foreign cannabis distributed in Canada is smuggled into the country by persons whose criminal ventures are intermittent and generally non-opiate drug-related. The relatively loose structure of both the international and do-mestic cannabis markets, the wide variety of potential sources, and the ab-sence of any necessary chemical refinement process have made it virtually impossible for any single group or organization to monopolize the distrib-ution network. Generally speaking cannabis trafficking can be viewed as a relatively free market system with nearly infinite opportunities for ad-vancement to higher and more sophisticated levels of distribution.
Although illicit cultivation is becoming increasingly common, in most areas domestically grown cannabis is still considered supplemental to imported supplies of hashish and marihuana. Hashish is ordinarily im-ported from the Middle East, North Africa or the foothills of the Himalayas. Alternately, hashish importers will purchase the drug in European trans-shipment centers where the cost is much higher but the risks — particularly for the inexperienced smuggler — are considerably reduced.
Much of the marihuana entering Canada is grown in Mexico, purchased in American trans-shipment centers, usually on the west coast, and then smuggled into Canada for domestic distribution. However, American at-tempts to control Mexican cultivation and exportation of marihuana, coupled with the escalating North American demand for cannabis prod-ucts, has led to increased marihuana importation from other countries. Colombian and Jamaican marihuana are increasingly prevalent and popu-lar, and it would be of no surprise to discover the existence of long-estab-lished supply routes from parts of central Africa and Southeast Asia. The cannabis industry, like all commercial endeavors, is governed by the law of supply and demand and is motivated by the desire to realize a profit. The difficulties recently encountered by importers in some purchasing markets, in combination with a grovving number of consumers, has led to an international proliferation of supply avenues and, significantly, the direct transfusion of millions of dollars into the economies of several un-derdeveloped nations.
Increasing logistics problems related to the importation of cannabis have also led to some manufacturing and importing of liquid or viscous hashish concentrates, generally known as "hash oil." In Afghanistan (which is one of the major Canadian sources of "liquid hashish"), the "oil" is chemically extracted from high quality marihuana pollen which sells in situ for between ten and thirty dollars a kilogram. Ten kilograms of pollen are said to produce about one kilogram of potent liquid hashish which, in Canada, sells for between ten and sixteen thousand dollars. The decreased bulk of this substance enables a cannabis courier to transport an amount worth approximately ten times the value of the same volume of hashish smuggled across international borders. At the retail level, this "hash oil" is sold in approximately three gram vials for between fifty and sixty dollars a vial — although prices as high as thirty-five dollars a gram have been reported for particularly potent varieties.
Marihuana and more traditional hashish preparations are much less expensive for the user, but there has been dramatic inflation in price over the past few years as a result of increased international law enforcement efforts, rising world-wide demand, and the decline in value of the Cana-dian as well as the American dollar. Hashish may still be purchased for under a hundred dollars a pound at some production sources, but its cost in most European trans-shipment centers has risen from about three hundred dollars a few years ago to over five hundred dollars per pound during the past two years. This has had the effect of raising domestic hash-ish prices by between thirty and seventy per cent. Marihuana prices have escalated along similar lines, and it is not uncommon to find esoteric varieties selling for as much as five hundred dollars a pound in Canada — whereas two hundred and fifty dollars was almost unheard of as recently as 1970.
Most regular cannabis users buy relatively small amounts. In the case of marihuana, an ounce (costing between fifteen and thirty dollars) is the most common measure while hashish purchases may range from" nickel" (five dollar) and "dime" (ten dollar) quantities weighing between one and five grams to "quarter" or "half" ounces (costing between twenty-five and thirty and forty-five and fifty dollars, respectively). Larger purchases may be negotiated (at considerable per-weight savings), but these are usually not for individual consumption and are either divided among friends who provided the money for the purchase, or else some of the surplus may be resold at a profit to subsidize the purchaser's personal cannabis consump-tion. As noted earlier, in Canada hashish tends to be about five to ten times as potent (in THC) as marihuana — despite the fact that it is only four to five times as expensive throughout most of the country. On a per unit THC basis, then, hashish is by far the better buy,
Excluding "street" sales, very small or hurried purchases, and those in-volving a highly trusted dealer, most buyers "taste" the cannabis before agreeing to purchase. Except for very low potency cannabis, however, the decision to purchase is usually more of a function of immediate need and the availability of alternate sources than the quality of the tested sample. Individual cultivation of cannabis provides a very inexpensive marihuana supply that may terminate dependency on the commercial cannabis mar-ket. Although this practice is increasing, most smokers still find it more convenient and less anxiety-producing to purchase rather than grow their own cannabis. Canadians have only begun to exploit the potential of domestically grown cannabis. We can expect a dramatic impact on the market from local sources in the near future, especially if international controls of illicit importation become more stringent and effective.
Cannabis distribution in Canada can be seen as a complex and growing enterprise in which a few at the top reap healthy profits while many of those involved at the lower levels are fortunate to cover their expenses and escape arrest. Marihuana and hashish, as high-demand commodities, will probably always be available, but the structure of the market, the sources of these drugs, the methods of importation, and the individual participants will continue to change until such a time as distribution is legally sanc-tioned or professional criminal organizations gain stable monopoly control.
EXTENT AND PATTERNS OF USE
The only national surveys on the extent of cannabis use in Canada were conducted under the auspices of the Commission in the spring of 1970 (Lanphier and Phillips 1971). Three populations — high school students, college and university students, and adult members of randomly selected households — were surveyed, and the results indicated rapid and sharp increases in the use of cannabis by persons in all three categories over the previous five years. The percentage of non-student, adult Canadians who reported ever using marihuana or hashish rose from 0.6% for 1966 to 3.4% in the spring of 1970. The percentage of college and university students who reported ever using cannabis rose from 3.9% to 29.0% for this same period of time, and the percentage of high school students who reported ever having used marihuana or hashish increased from 1.9% to 10.3%. In total, the Commission estimated that at least 850,000 Canadians had used cannabis by the spring of 1970, and that between 1,300,000 and 1,500,000 Canadians had probably done so by the middle of 1971. However, "cur-rent" cannabis users appear to account for only about half of those who have "ever used" the drug. In the spring of 1970, for example, only 1.0% of Canadian adults (N ---- 126,000), 17.4% of college and university stu-dents (N = 48,000), and 7.4% of high school students (N = 180,000) reported current use of marihuana or hashish (Commission 1972b).
There has been considerable discussion in Canada as to whether or not the 1971 Commission projections represent a "peaking" of cannabis use rates or are simply indicative of a still-continuing upward trend. While there have been no national surveys conducted since the Commission's 1970 studies, the data collected in more recent local or regional studies including longitudinal surveys of high school populations, suggest that the incidence of cannabis use is still rising, primarily as a result of its diffusion to populations that had remained relatively insulated during the late 1960s.
The Addiction Research Foundation of Ontario conducted a survey of 1,200 randomly selected adults (persons eighteen years of age and over) in Toronto in the spring of 1971 and found that 8.4% had used cannabis at some time during the previous twelve months, and that half of these persons had done so seven or more times during this one year period. Of greater import — as regards future incidence of use figures — was the study's finding that the extent of cannabis use was inversely related to age : approximately 30% of the respondents between 18 and 25 years of age had used cannabis during the previous year, while only about 10% of those between 26 and 35 and only about 1% of those 36 years of age and over had done so (Smart and Fejer 1971). While Toronto survey findings can-not be appropriately generalized to the entire country, the incidence of use in this city is likely typical of that in Canada's larger metropolitan areas and suggests a significant increase over the 3.4% "ever used" rates found by the Commission's national adult survey in 1970. Conclusive evidence regarding contemporary rates of adult cannabis use must await new national survey findings, but, at the moment, there is no good reason to believe that the trend toward increasingly widespread use of marihuana or hashish among Canadian adults has in any way abated.
The Addiction Research Foundation of Ontario has studied the extent of cannabis use among Toronto high school students on several occasions since 1968 (Smart, Fejer and White 1972). In that year 6.7% of the surveyed students reported having used cannabis during the previous six months. Two years later, in 1970, the figure had risen to 18.3%, and by 1972 the percentage of users had further increased to 20.9%.
These longitudinal data indicate a decrease in the rate of cannabis diffu-sion among urban high school students, but still demonstrate that the in-cidence of cannabis use is continuing to rise.
Of related interest are the findings of high school surveys conducted in two rural school divisions in southern Alberta in early 1971 (Rootman 1972). Eight percent of the students in one of the school districts and 15.3% of those in the other reported the use of cannabis. While these estimates are not high by comparison with survey findings in Canadian urban communities, they suggest a significant increase in cannabis use since the Commission's national high school survey of one year earlier. If these Alberta findings can be generalized to other rural areas, and if the Toronto high school data is indicative of other urban trends, then the present in-cidence of cannabis use among Canadian high school students nationally is likely at least twice as high as the 10% "ever used" rates found in the Commission's 1970 study.
It is clear that the use of cannabis is no longer the urban phenomenon almost exclusively indulged in by middle-class young adults and adoles-cents which it appeared to be in the late 1960s. As use of marihuana and hashish has spread across age and class barriers over the past five years, those social characteristics that were once thought to be related to the use of these drugs have tended to lose significance. In fact, generally speaking, it seems that age and sex (since use tends to be much more common among males than females) are the only remaining social factors related to canna-bis use in Canada that have much predictive value.
Apparently, most of the Canadian cannabis-using population is en-gaged in seemingly very moderate levels of use. According to the Commis-sion's 1970 surveys, about 40% of cannabis- using students and the Major-ity of the adult consumers used marihuana or hashish only once a month or less. Approximately the same proportion of high school students and about one-third of college and university students reported using cannabis between once a month and once a week. Only very small percentages of the three nationally surveyed populations claimed to smoke marihuana or hashish more frequently than once a week (Commission 1972b). While more contemporaneous level-of-use data is not, as yet, available, it is not unreasonable to assume that the regular use of the drug (e.g., between once a month and once a week) will become increasingly common However, such "stable" patterns of use would likely change with any significant al-teration in cannabis availability in Canada.
Certain aspects of cannabis use, common to most consuming occasions involving experienced regular users, are a product of the drug's effects, its illlegal status, and other aspects of the social environment of its use. Although exceptions do occur (particularly in the case of very heavy users), the following discussion describes the social circumstances of regular mari-huana or hashish consumption for the majority of Canadian users.
Cannabis users are well aware that they are violating the law and, con-sequently, often take considerable precautions to avoid discovery of their caches. Some only obtain the drug for special occasions such as parties, while others, who use cannabis more frequently, may retain a minimal quantity in their residence. Larger quantities are frequently stored elsewhere, ideally in a public but secure location, until such time as they are required. Although cannabis may be consumed in a wide variety of cir-cumstances, its use is usually reserved for leisure periods in the evenings or on weekends when it is smoked with a few close friends in a private residence. In increasing numbers of cities the drug may be smoked in the streets, clubs or taverns with relatively little risk of arrest. Smoking in cars, natural outdoor settings and at entertainment activities such as concerts or pop festivals, is also common
The mode of consumption is very much a function of the drug's form. Marihuana is ordinarily hand-rolled or occasionally machine-rolled into thin cigarettes known as "joints," "J's," or "numbers." Two cigarette papers (often colored, perfumed, or emblazoned with various designs) are sometimes employed so as to retard burning and the "joint" is often thoroughly licked before lighting for same the reason. Mari-huana may also be smoked in any one of a large variety of ornate pipes, "hookahs" (water-pipes, which cool the smoke) or "chillums" (Indian-style cylindrical pipes which are held vertically, the smoke being drawn through the narrow bottom of the column), but this style of use is more common with hashish.
In a typical situation, small pieces of hashish are placed in the bowl of a pipe which is relit and refilled as required. Hashish may also be crumbled into small bits or a powder which is then mixed with tobacco and rolled in-to a joint or "spliff." It may also be smoked by placing a piece on the lit end of a cigarette and inhaling the smoke directly, or through a thin tube (such as a straw or rolled up dollar bill). A similar inhalation procedure is used for smoking burning hashish from the end of a pin or needle.
Typically very little cannabis is wasted during the process of smoking — "joints" or pipes are usually passed quickly from one user to another with relatively little "dead" burning time or lost "side-stream" smoke. Users also typically consume all the material in a "joint," including the butt or "roach." The common inhalation procedure is similarly parsimonious ; the smoke is typically taken deep into the lungs and held for a prolonged period before being exhaled, in order to maximize absorption of the active compounds. This style of smoking, common in North America and parts of Europe, results in a much greater proportion of the THC in the cannabis being absorbed, compared to the more casual puffing style with immediate exhalation commonly seen in non-industrial countries with a longer his-tory of cannabis use and easy availability, such as Jamaica or India. These factors, along with likely differences in the efficiency of THC delivery by various forms of pipes and cigarettes, greatly complicate at-tempts to make quantitative cross-cultural comparisons or estimates.
Both marihuana and hashish can be eaten although this mode of admin-istration is usually restricted to cannabis boiled in tea, or cooked in the proverbial brownies or other dishes that disguise its taste and appearance, as well as often increasing its potency. [Note that high temperatures con-vert inactive THC-acid to THC]. While eating cannabis produces a "high" of longer duration than smoking, the larger quantities required for inges-tion, the inconvenience involved in waiting for the effects to "come on" (usually an hour or more) and the impossibility of controlling the effects by titrating the dose render this method relatively unpopular except for public occasions (attending films or concerts, for example) when it is difficult to smoke in safety. In the past few years virtually an entire new industry has developed to service cannabis users, and in ahnost every Canadian city one can now purchase specifically manufactured pipes, rolling papers, and assorted other paraphernalia designed to enhance the experience of marihuana or hashish use.
Some persons (mainly long-time or heavy users) occasionally smoke can-nabis while alone ; the drug may also be consumed at large parties or other public or semi-public gatherings. The most common situation-of-use, however, includes only a few close friends or trusted acquaintances, some of whom may not be smoking. The host typically provides the cannabis (although guests may supplement it with their own supply) and the pipe or "joint" is passed from participant to participant in a circular fashion until the cannabis is consumed or the smokers feel sufficiently "high." Some may stop smoking before others, although they usually remain in the circle, passing the "dope" to the next user. Most smokers, however, continue to smoke even after they are high and, should any one express the desire for more during the session, a fresh "joint "or pipe is usually pre-pared for circulation. This sharing reinforces the sense of communality that characterizes marihuana or hashish smoking occasions. However, such rituals are increasingly less significant as the use of cannabis becomes more common in Canadian society.
In Canada, marihuana cigarettes rarely contain any tobacco, and may vary in size from a few hundred milligrams up to a several gram "bomber."' Our research suggests that a typical "joint" contains about one-third of a gram of marihuana and that, depending on the potency of the material and individual differences in smoking style and reaction, anything from a fraction of a "joint" up to one or two cigarettes might be considered a typical acute dose in this country. We have accumulated a substantial amount of direct and indirect evidence that most cannabis users usually smoke less than 6 mg of THC to get "high" or "stoned" (Commission 1972b ; Miller et al. 1971 ; Green et al. 1971).
While marihuana or hashish smoking sessions involving relatively novice users tend to be deliberate and planned, such use is routinized among more experienced users. Regular users develop increasingly casual attitudes toward cannabis and tend to associate its consumption with social gather-ings during which cannabis use is viewed as a means toward an end rather than an end in itself. Smoking-oriented sessions last from under an hour to half a day or longer, the average being several hours. Except for rare occasions when the cannabis is so potent that the users become temporari-ly immobilized, the duration of a smoking session is more a function of extraneous considerations than the quality of the marihuana or hashish.
The major acute physical and psychological effects of cannabis are generally well known and recognized, but it is worth noting that certain effects are never completely predictable from one occasion to another, even with the same users and identical cannabis samples. The physical and social setting and participants' moods are important variables in deter-mining many aspects of the reaction. Cannabis generally operates as a "social lubricant" and most using occasions are tranquil and relaxed affairs that, for naive observers, are often indistinguishable from many small alcohol-using or non-drug gatherings. Smokers engage in quiet con-versatlon or listen to recorded music in a dimly illuminated room. Argu-ments appear to occur less frequently than in many other drug-using situations, such as those involving alcohol, although periods of agitated activity are not uncommon. Conversations are often related to drug-as-sociated matters although a diverse range of subjects may be broached — often in a convoluted or seemingly unrelated fashion. While the mood is generally peaceful or jocular, there are occasions when serious discussions involving highly personal matters or existential or spiritual questions oc-cur. Sexual intercourse, reading, eating and watching television are addi-tional activities commonly engaged in by cannabis smokers when they are high. The Commission was unable to find any evidence that cannabis use was a significant factor in aggression, violence or non-drug crime in Canada (Commission 1972b).
Infrequently a user may experience an acute anxiety reaction. Such ad-verse reactions typically seem to center around fear of legal repercussions of illicit drug use, fear of insanity, fear of death, or basic sexual conflicts, and may be precipitated by a "hassle" or problem of real or imagined significance. Friends usually attempt to assist the individual by assuring him of the ephemeral nature of his condition, trying to distract him, or attempting to uncover the source of his anxiety and convince him that it is insignificant or "not-worth-worrying-about." On rare occasions the dis-turbed individual may be provided with "downers" (tranquilizers or other sedative-hypnotics, if available), or taken to a street clinic or hospital for professional attention.
During the past few years there have been numerous clinical case reports in Canada of individuals suffering from various acute or chronic psycho-logical problems allegedly associated with cannabis use. However, studies of hospital admissions and resident patients have uncovered an almost insignificant number of hospitalized persons with primary cannabis problems. No cases of so-called "cannabis psychosis" have been identified (Commission 1972b, 1973 ; Hemmings and Miller 1971; Miller, Brewster and Leathers 1971; Statistics Canada 1972). Although transient phases of anxiety and paranoia, and occasionally more significant panic reactions, occur in some inexperienced and regular cannabis users, it would appear that serious reactions are very infrequent, that only a small proportion of the adverse reactions which do occur come to medical attention, and that such cases rarely require hospitalization or prolonged treatment.
Changes in the extent and patterns of cannabis use in Canada will un-doubtedly alter the epidemiological picture of adverse reactions as well : as noted above, long-term or heavy use has up to now been rare. Further-more, as Becker (1953) suggested, as familiarity with acute effects of can-nabis in our culture increases, the frequency of short-term fright or panic reactions will likely decrease. There is some evidence that this process is already occurring in Canada.
For most regular marihuana and hashish smokers, continuous use serves to reinforce favorable interpretation of the cannabis experience and strengthens their defining the laws prohibiting use, rather than use of the drug itself, as immoral or improper. For increasing numbers of persons, then, persistent use of cannabis is evidence of a greater personal commit-ment to the primarily recreational use. For regular marihuana and hashish users there is no longer any debate : cannabis has been phenomenologically tested and sanctioned; its use is now institutionalized.
The institutionalization of cannabis goes far beyond its incorporation into the lived-in world of its users. Throughout much of urban Canada, cannabis use has been granted de facto legitimacy through a combina-tion of more tolerant handling of cannabis-related improprieties by vari-ous social control agencies, and by the localization of public use settings to certain bars, clubs and taverns that have come to represent territories generally liberated from the enforcement of cannabis laws (McMullan 1972). These modes of cannabis management may be considered as interim steps on the road to complete institutional normalization of cannabis use in Canada.
CANNABIS IN THE MULTIPLE-DRUG USE CONTEXT
The controversy surrounding the use of cannabis in Canada has resulted in public discussions of non-medical drug use generally — both licit and illicit.
On the basis of the often limited available data, we estimate that at present, Canada has about 15,000 daily heroin and methadone users, be-tween two and three thousand regular users of intravenous amphetamines, several hundred thousand persons who use oral amphetamines and seda-tives without benefit of prescription on at least an occasional basis, probably an equivalent number of current hallucinogen users, about one hundred thousand adolescent and pre-adolescent users of volatile solvents, about 12,000,000 alcohol drinkers (including an estimated 300,000 alco-holics), and approximately 7,000,000 daily users of tobacco products. Also, most adult Canadians are regular users of caffeine, in the form of coffee, tea, or cola drinks (Commission 1973).
Despite this extremely high incidence of alcohol and tobacco use — and the indisputable evidence regarding the personal and social potential for harm,associated with the use of these substances — it is only since the controversy surrounding the use of cannabis that alcohol and tobacco have begun to be publicly redefined as "drugs." This redefinitional pro-cess — which is not yet completed — is likely to have significant legal, educational and treatment consequences. The distinction between legal and illegal drugs — which reflects a moral discrimination at least fifty years old — is now undergoing serious questioning. Ideally, the end result of this process will be a system of drug regulations which discriminates be-tween drugs on the basis of a rational consideration of their potential for physical, psychological and social harm. While such legal developments are not inevitable, one certain result of this public debate will be the legal reclassification of cannabis.
It is clear that in Canadian society the regular use of a single drug is the exception rather than the rule : multiple drug use is the norm. In recent years considerable attention has been turned to the patterns and conse-quences of the simultaneous and sequential medical or non-medical use of various drugs. The role of cannabis in multiple drug use has been the sub-ject of some controversy. The majority of cannabis users studied in Canada have had regular experience with a variety of other psychoactive drugs — alcohol, tobacco and caffeine being the most frequently mentioned. Furthermore, the use of amphetamines, LSD and other hallucinogens, barbiturates and other sedative-hypnotics, volatile solvents, cocaine and opiate narcotics is more common among cannabis users than in the general population (Commission 1972b, 1973).
In Canada, cannabis has traditionally been closely tied to tobacco use and there seem to be relatively few regular cannabis smokers who did not initially learn the technique of smoke inhalation from prior experience with tobacco cigarettes. Unlike many non-industrial countries where can-nabis is routinely mixed with tobacco for smoking, in Canada, as noted earlier, marihuana is rarely taken with tobacco, although hashish is sometimes smoked in such a combination.
The relationship between cannabis and alcohol use has been the subject of considerable discussion. It has been suggested that cannabis may be a cure for society's alcohol ills. In general, survey studies in Canada indicate that those who use alcohol are much more likely than 'teetotallers' to use cannabis, that most cannabis users still drink alcohol, and that heavy users of cannabis tend to drink more alcohol than light or infrequent users (Bilodeau and Jacob 1971; Campbell 1970; Green and Leathers 1971; Lanphier and Phillips 1971; Russell 1970; Smart and Fejer 1971). On the other hand, in a recent survey in Toronto, heavy users of alcohol reported-ly used less cannabis than more moderate drinkers (Smart, Fejer and White 1972).
Many researchers have mistakenly assumed that cross-sectional survey data demonstrating a positive between subject correlation of cannabis and alcohol use, at a single point in time, implies a positive relationship be-tween the use of the two drugs within an individual over time, which is the relationship of ultimate interest. Such extrapolation is unjustified logically and statistically (Cattell 1952). Evidence of an association (either positive or negative) between the use of two drugs in a population at a given time provides little information as to the relationship (if any) between the levels of use of the drugs within the individuals involved. Changes in behavior within an individual, over time, must be studied directly. Even then, other information in addition to drug-use patterns must be considered in deter-mining causal factors.
The limited retrospective within-subject data now available suggest that cannabis use may reduce or interchange with alcohol consumption to some extent in the user population. In several Canadian studies a sub-stantial proportion of cannabis users claimed that they had significantly reduced their consumption of alcohol since using cannabis (Green and Leathers 1971; Green et al. 1971; Lanphier and Phillips 1971; Paulus 1969). There is also a reported tendency, with cannabis use, for a greater reduction in the use of hard liquor than of the milder forms of alcohol. However, it is clear that the combined consumption of cannabis with wine or beer is common in some social circles in Canada. None of these reports presents definite objective evidence of a reduction in alcohol use, so con-clusions must be guarded.
Apparently, individuals who actually quit alcohol use because of canna-bis are uncommon ; their choice of drugs may have more to do with their value systems than with the pharmacological properties of the drugs. The hostile attitude towards alcohol expressed in the past by some cannabis-using youth is clearly not reflected in the majority of Canadian users today. Systematic prospective studies have not been conducted, and it is not clear from available data whether, on a large scale, cannabis would tend to replace alcohol as an intoxicant in the user population of this country, or whether the use of these drugs would be additive without significant inter-action, or if the use of one might potentiate or increase the consumption of the other. Assessed separately, the incidence of use of alcohol and of cannabis are both increasing in Canada, especially among young people.
In the past two decades, the relationship between the use of cannabis and heroin has been the subject of much dispute. During this period, vari-ous reports from the United States suggested that the majority of heroin users had previously used cannabis, although in certain sections of the country this was apparently not the case (Ball, Chambers, and Ball 1968). Before 1950, there has been little evidence or serious discussion of a can-nabis-to-heroin progression in North America.
Until recently, there was no evidence of a relationship between the use of cannabis and of heroin in Canada. Heroin users studied had generally been heavy consumers of alcohol, barbiturates, and tobacco, but had little or no cannabis experience (Henderson 1970; Josie 1948; Paulus 1969; Stevenson et al. 1956; Williams 1969). The situation has apparently changed, and many young Canadian heroin users also report previous and concomitant use of mariuhana, amphetamines, barbiturate and non-bar-biturate sedatives and, less often, LSD (Green and Blackwell 1972; Johnston and Williams 1971).
Older studies of lower-class and/or delinquent populations do not readily generalize to the present phenomenon of middle-class cannabis consumption. It would appear that only a small minority of cannabis users in general have had experience with illicit opiate narcotics. However, an increase in opiate narcotic use in certain younger groups has been reported (Green and Blackwell 1972 ; Johnston and Williams 1971 ; Commission 1973).
Almost all of those who have used LSD and similar hallucinogens have also used cannabis, although the majority of cannabis users have not tried LSD. Heavy regular use of LSD is rare in Canada — very intermit-tent consumption is most common among even confirmed users. The use of "speed" is similarly correlated with cannabis use. Most "speeders" or "speed freaks" have had extensive experience with cannabis, although such individuals make up an almost insignificant proportion of the total cannabis-using population (Commission 1973).
In Canada, peer group values and the establishment of contacts with illicit drug distribution networks have apparently played the major role in concomitant and sequential illegal use of different drugs. Becoming accus-tomed to "breaking the barrier" of illegal drug use by the consumption of one illicit drug may, in some individuals, reduce inhibitions with respect to other such drugs. It has often been proposed that cannabis frequently provides the initial illicit drug experience in this context. Although previ-ous heavy illicit use of tobacco and alcohol during adolescence is common in adult chronic drug users, their use by young people, even though illegal, is largely condoned and, to some extent, encouraged by our society; it does not have the legal significance of cannabis use. It has been suggested that through the use of cannabis certain individuals may learn to use a drug as a mode of coping or as a simple primary source of reinforcement and satisfaction, and that this lesson might later generalize to other drugs. On the other hand, many investigators contend that persons who ultimate-ly become dependent on opiate narcotics, "speed," alcohol or other "hard" drugs are strongly predisposed in that direction by personal, social and economic factors, and that the use of transitional drugs is of little causal significance. Attempts to empirically identify personal predisposing factors in drug dependence have met with little success, however, and this hypothesis has yet to be scientifically confirmed.
The role of cannabis, if any, in the subsequent use of other drugs is not yet well understood ; it is unclear whether cannabis plays a specific pre-disposing role, or is causally unrelated to other illicit drug use and is often used earlier than certain other drugs simply because of its wider availability and social acceptance. Specific pharmacological properties of marihuana (or any other drug) which might lead to a need or craving for other drugs have not been documented. It would appear that dynamic and changing social, legal, economic and personal factors are the primary deter-minants of the multi-drug-using patterns seen in Canada, and that the specific pharmacology of the substances involved is often secondary.
It appears that the last few years have marked the beginning of the cul-tural institutionalization of cannabis in Canada. Cannabis is no longer morally aligned with the opiate narcotics and its legal classification with them must be seen as an historical and moral anachronism. Today canna-bis is more frequently equated with the use of alcohol than the use of opiates, and — in the face of common usage and the absence of popularly expected evidence of serious detrimental effects — its de jure legitimation for recreational purposes has become simply a matter of time.
1 Regular tobacco cigarettes usually weigh about one gram.
REFERENCES
BALL, J. C., C. D. CHAMBERS, M. J. BALL
1968 The association of marijuana smoking with opiate addiction in the United States. Journal of Criminal Law, Criminology and Police Science 59:171-182.
BARASH, L. A.
1971 "A review of hemp cultivation in Canada." Unpublished research project. Commission of Inquiry into the Non-Medical Use of Drugs. Ottawa.
BECKER, H. S.
1953 Becoming a marihuana user. American Journal of Sociology 59 : 235- 242.
BILODEAU, L., A. JACOB
1971 La prévelance de l'usage des drogues de 1969 1971, chez les étudiants du secondaire et du collegial de l'ile de Montréal: Quelques résultats généraux. Quebec: Office de la Prevention et du Traitment de l'Alcoolis-me et des Autres Toxicomanies.
CAMPBELL, I. L.
1970 "Non-medial psychoactive drug use at Bishop's University 1965 to 1970." Unpublished manuscript. Montreal: Sir George Williams Uni-versity.
CANADA, HEALTH PROTECTION BRANCH, DEPARTMENT OF NATIONAL HEALTH AND WELFARE, COMPUTER SERVICES BUREAU
1973 "Identity of police drug exhibits." Unpublished reports, Ottawa.
CANADIAN MEDICAL ASSOCIATION
1934a The increasing menace of marijuana. Canadian Medical Association Journal 31:561.
1934b Marijuana [editorial]. Canadian Medical Association Journal 31 : 544- 546.
CATTELL, R. B.
1952 The three basic factor-analytic research designs — their interrelations and derivatives. Psychological Bulletin 49:499-520.
COLECLOUGH, A., L. G. HANLEY
1968 "Marijuana users in Toronto," in Deviant behavior in Canada. Edited by W. E. Mann. Toronto: Social Science.
COMMISSION OF INQUIRY INTO THE NON-MEDICAL USE OF DRUGS
1970 Interim report. Ottawa: Information Canada. 1972a Treatment report. Ottawa: Information Canada.
1972b Cannabis report. Ottawa: Information Canada. 1973 in press.
Final report. Ottawa: Information Canada.
COOK, S. J.
1964 "Ideology and Canadian narcotics legislation." M. A. dissertation,
Department of Sociology. Toronto: University of Toronto.
GREEN, M., J. C. BLACKWELL
1972 "Continuing survey of sensitive observers in Canada: The final moni-toring project." Unpublished research project. Commission of Inquiry into the Non-Medical Use of Drugs. Ottawa.
GREEN, M., B. LEATHERS
1971 "Interviews with 'straight' adult cannabis users." Unpublished research project. Commission of Inquiry into the Non-Medical Use of Drugs, Ottawa.
GREEN, M., et aL
1971 "Self-reporting of drug consumption patterns by regular cannabis users: A log book study." Unpublished research project. Commission of Inquiry into the Non-Medical Use of Drugs, Ottawa. (Partial sum-mary in the Commission's Cannabis report, p. 40.).
HEMMINGS, B., R. D. MILLER
1971 "Non-medical drug use as a factor in hospitalization : A survey of Canadian psychiatric hospital diagnostic records." Unpubliahed re-search project. Commission of Inquiry into the Non-Medical Use of Drugs, Ottawa. (Published in part in the Commission's Cannabis report, pp. 88-90; and in the Final report, Table A.7 and related text.)
HENDERSON,
1970 An exploration of the natural history of heroin addiction. Vancouver: Narcotic Addiction Foundation of British Columbia.
JOHNSTON, W. E , H. R. WILLIAMS
1971 Drug use patterns and related factors of heroin addicts seeking treatment for their addiction. Vancouver: Narcotic Addiction Foundation of British Columbia.
JOSIE, G. H.
1948 A report on drug addiction in Canada. Ottawa: King's Printer and Con-troller of Stationery.
LANPHIER, C. M., S. B. PHILLIPS
1971 "(a) The non-medical use of drugs and associated studies: a national household survey. (b) Secondary school students and non-medical drug use: a national survey of students enrolled in grades seven through thirteen. (c) University students and non-medical drug use: a national survey." Unpublished Commission research project. Commission of Inquiry into the Non-Medical Use of Drugs." Ottawa. (Published in part in the Commission's Cannabis report and Final report.)
MARSHMAN, J. A., R. J. GIBBINS
1970 A note of the composition of illicit drugs. Ontario Medical Review 37:429-430,441.
MC MULLAN, J.
1972 "Suburbia in transition: patterns of cannabis use and social control in the suburban community," in Observations on the normalization of
Cannabis Use in Canada 519
cannabis. Co-ordinated by H. T. Buckner. Montreal: Department of Sociology, Sir George Williams University, 1-31.
MILLER, R. D., J. BREWSTER, B. LEATHERS
1971 "Survey of Ottawa-area physicians regarding the non-medical use of drugs." Unpublished research project. Commission of Inquiry into the Non-Medical Use of Drugs, Ottawa. (Published in part in the Comis-sion's Cannabis report, 86-88.)
MILLER, R. D. et al.
1971 "A comparison of the effects of A9THC and marijuana in humans." Unpublished research project. Commission of inquiry into the Non-Medical Use of Drugs. Ottawa, (Published in part in the Commission's Cannabis report).
1973 "Chemical analysis of illicit drugs in Canada." Unpublished research project. Commission of Inquiry into the Non-Medical Use of Drugs, Ottawa. (Published in part in the Commission's Cannabis report [Tables 1 and 2] and Final report [Tables A.8 and A.9] and related text.)
MURPHY, EMILY
1922 The black candle. Toronto: Thomas Allen.
PAULUS, I.
1969 Psychedelic drug use on the Canadian Pacific coast: notes on the new
drug scene. International Journal of the Addictions 4:77-88.
PAULUS, I., H. R. WILLIAMS
1966 Marihuana and young adults. British Columbia Medical Journal 8 (6): 240-244.
ROOTMAN, I.
1972 Drug use among rural students in Alberta. Canada's Mental Health 20 : 9-14.
ROYAL CANADIAN MOUNTED POLICE
1969 Unpublished brief presented to the Commission of Inquiry into the Non-Medical Use of Drugs, Ottawa.
1973 Unpublished information communicated to the Commission of In-, quiry into the Non-Medical Use of Drugs, Ottawa.
RUSSELL, J.
1970 Survey of drug use in selected British Columbia schools. Vancouver : Narcotic Addiction Foundation of British Columbia.
SMALL, E.
1971 "Interim report on studies of cannabis undertaken jointly by the Departments of Agriculture and National Health and Welfare." Un-published report to the Commission of Inquiry into the Non-Medical Use of Drugs, Ottawa.
SMART, R. G., D. FEJER
1971 "Marijuana use among adults in Toronto." Unpublished manuscript, Project J-183, Substudy 6-7 and Jo-71, Addiction Research Founda-tion, Toronto.
SMART, R. G., D. FEJER, J. WHITE
1972 "Drug use trends among metropolitan Toronto students : a study of changes from 1968 to 1972." Unpublished manuscript. Addiction Research Foundation of Ontario, Toronto.
STATISTICS CANADA
1972 Mental health statistics. Vol. 1. Institutional admissions and separa-tions (1970). Ottawa: Information Canada.
STEVENSON, G. H., et al.
1956 "Drug addiction in British Columbia." Unpublished manuscript, University of British Columbia, Vancouver.
WILLIAMS, H. R.
1969 Treatment of the narcotic addict with some observations on other drug dependencies. British Columbia Medical Journal 11:11-13.
| < Prev | Next > |
|---|