| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
6. Health Correlates and Consequences
 |
|  |
| 
| Reports - Annual Report Bulgaria |
Drug Abuse
6. Health Correlates and Consequences
Drug Related Deaths and Mortality Rate among the Drug Users
The statistical research of the death cases according to causes is based on the medical certificates for death, filled in by the physician who establishes the death. Since the beginning of 2005 in Bulgaria has been applied the Tenth Revision of the International Classification of Diseases /ICD/ and problems related to health of the World Health Organization. The causes for death are coded according to this classification.
When there is only one cause for death indicated, the coding is relatively simple. In most of the cases, however, there are two or three diseases which have caused the death. In accordance with the requirements of the WHO and the guidelines for compiling statistical tables of deaths depending on the causes, the so called primary cause for the death is coded. It is defined as "the cause or the trauma which triggered a series of diseases which directly caused the death, or the circumstances of the accident or the violence which caused the lethal trauma." The Ministry of Health issues instructions on coding the causes for death in accordance with the ICD. The coding of the causes for death is done by physicians working at the Regional Centers of Healthcare and respectively trained to apply the requirements of the ICD. For coding the causes for death the physician uses the medical certificate of death.
When coding the cause for death the three-sign code of the causes is used. This limits the options to analyze the data related to the intoxication by drugs and psychodysleptic (hallucinogenic) or psychoactive medicines.
Drug Related Deaths
National definition
In accordance with the requirements of EMCDDA (The DRD-Standard, version 3.0) the codes of the ICD — 10, which have to be considered in relation to intoxication (accidental, intended or with indefinite intentions) are combined with the T-codes to characterize the type of the substance. In accordance with the recommendations of the WHO for classifying the data for deaths according to the causes since such a combination cannot be made the inclusion only of a single code fromlhe two classes necessitates the choice of the code from class XX - External Causes for Morbidity and Deaths - namely the codes X and Y are preferred.
Under the terms of the DRD-Standard, version 3.0, when a combination is not possible of the codes X- and Y- codes with the T- codes, the alternative procedure is to include the deceased persons in the item of some additional causes, included in the class External Causes for Morbidity and Deaths. The data analysis however shows that the estimation of drug-related deaths, if all these causes are taken into consideration, is grossly overestimated. Considering the total number of deaths caused by intoxication with narcotic or psycholeptic (hallucinogenic) substances (T 40) and intoxication with psychoactive medical substances not classified elsewhere (T43), which does not differ significantly from the number of deaths caused by X41, X42, X61, X62, Yl 1, Y12, it was assumed that the estimation so done would not significantly differ from the estimation to be made if such a combination with the T-codes is possible.
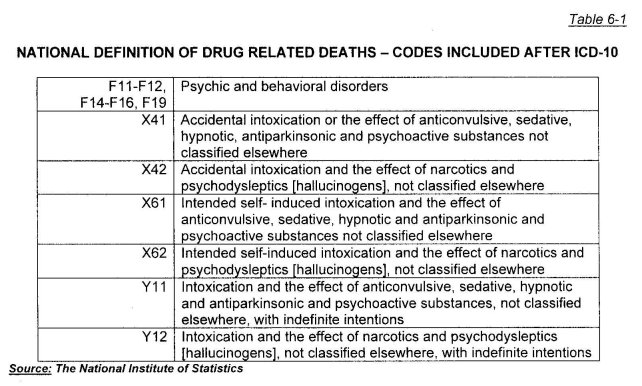
Having made the analyses we decided that in the tables supplemented to the report and in the present working out of the analysis of the drug-related deaths, the data for the following causes for deaths should also be included (see Table 6-1):
In compliance with the statistics so presented in 2006 the drug-related deaths nutnber 29 cases. The number of men is 26 and it is significantly greater than the number of women - 3 cases. (see Figure 6-1).
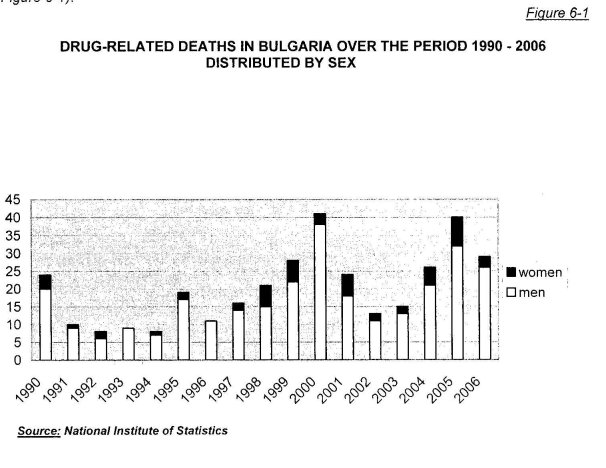
After the increase of the indicator intensity of deaths 52 for the previous year, in 2006 its overall value for the country was 0.38 per 100 000 persons of the population. The indicator is significantly higher for men (0.70 per 100 000 men) compared to the one for women (0.08 per 100 000 women). For the whole period from 1990 to 2006 the value of the coefficient was the highest in 2005— 0.52 per 100 000 persons from the population. Its lowest value was in 1993— 0.11 per
100 000 persons of the population.
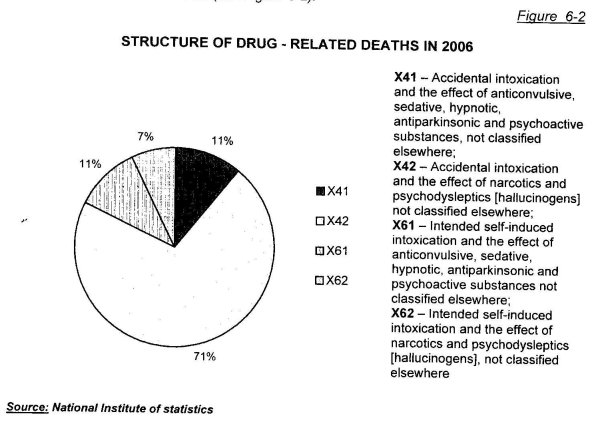
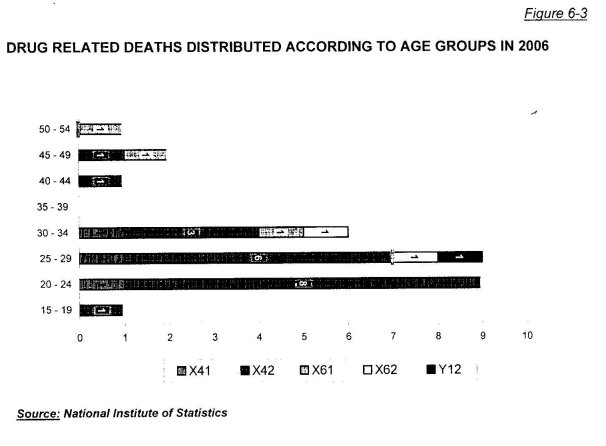
In the structure of deaths when distributed by causes the relative share of the deaths caused by accidental intoxication and by the effect of narcotics and psychodysleptics [hallucinogens], not classified elsewhere (X42), is the greatest. This is the cause of death in 71% of the cases.
Next come the deaths caused by accidental intoxication and by the effect of anticonvulsive, sedative, hypnotic and antiparkinsonic and psychoactive substances, not classified elsewhere (X41) and the intended self-induced intoxication and the effect of anticonvulsive, sedative, hypnotic, antiparkinsonic and psychoactive drugs, not classified elsewhere (X61) —11% for each.
7% of the deaths in 2006 were caused by intended self-induced intoxication and by the effect of narcotics and psychodysleptics [hallucinogens], not classified elsewhere (X62). In 2006 there are no deaths caused by the greater part of the causes used in the definition.
Unlike the previous one, this year there is not a single death caused by Psychic and Behavioral Disorders ICD — 10 revision (see Figure 6-2).
The distribution of deaths according to age shows that the intensity of deaths is the greatest in the age group 20 - 24 years. The intensity of deaths in this age group is 1.68 per 100 000 persons of the respective population. For the men this value is 3.28 per 100 000 men, and for the women in this age group there are no deaths caused by items included in the definition. The age group 25-29 years comes second in the intensity of deaths (1.58 per 100 000 persons) followed by the group aged 30— 34(1.05 per 100 000 persons) (see Table 6-2).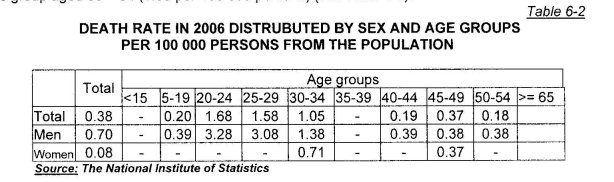
More than 80% of all the drug - related deaths are men and women aged 20 to 34 years. The mean age of the deceased persons continues to rise and from a mean age of 27.8 in 2004 it rose to 28.8 in 2006. There are no drug - related deaths in the age group 35 to 39 years, neither in the age group of 55 years and over.
Mortality Rate among Drug Users
The mortality rate among drug users is still not well enough studied in the country. In relation to the need of improving the information on the problem the National Focal Point on Drugs and Drug Addictions (NFPDDA) organized and carried out a cohort study on mortality rate among drug abusers 53, which encompassed the geographical region of Sofia - the biggest city in the country, where a considerable part of the population studied is concentrated and where there was relatively good archive of documents concerning treatment system. According to data from surveys (fi. estimated using the capture-recapture method) and expert estimations the proportion of the problem drug users in the capital is probably around the half of all the problem drug users in the country (the estimate of the number of problem heroin users in Bulgaria for the year 2005 was between 20 000 and 30 000 for the capital was between 9 136 and 15 909 when applying the capture-recapture method 54)
The objective of the study was to determine the standard of living of the problem drug users included in the sample and to help receive more complete and of a broader range data on the level of mortality rate and the main causes for death of the persons studied. The study was retrospective in respect to data collection. The specific years included in the period from which the persons studied were selected were chosen by the work team. The selection of the persons was made according to criteria chosen in advance. The choice of the criteria was aimed at achieving maximal reliability of the information initially received. The criteria of inclusion are described below.
Criteria for inclusion in the sample
For the study the following criteria for inclusion in the sample were determined:
• Heroin or other opioid users;
• Persons admitted for treatment in the specialized inpatient facilities or outpatient centers;
• In the city of Sofia ;
• At least once for the period from the beginning of 1995 to the end of 1999 (a five-year period);
• Those diagnosed according to the ICD-9 as suffering from — 292 (psychosis caused by narcotic substance use), 304 (narcotic substance addiction) or 305 (abuse without evidence of narcotic substance addiction);
• Their treatment because of drug use must have begun at a specialized treatment center during the period selected;
• Availability of complete data necessary for the further specifying of their standard of living as well as of exact information about the date they were admitted to the treatment center (corresponding to the selected 5-year period);
Spheres of the study
For the aims of the study three different options for treatment were selected which were accessible to the problem drug users during the period indicated:
1. Treatment in inpatient units — at the Hospital for treatment of addictions and alcoholism within the frames of the National Centre for Addictions in Suhodoi, Sofia;
2. Treatment in outpatient units — at the Program of Home Detoxification in the National Centre for Addictions in Sofia;
3. Substitution treatment — the Methadone Maintenance Program at the National Centre for Addictions in Sofia.
For each one of these treatment programs a register of the patients is kept, where the necessary information can be found. These three programs encompass more than half of the cases of treatment in Sofia during the selected period, especially in respect to the most problematic cases of drug use (heroin and other opioids).
Data collection
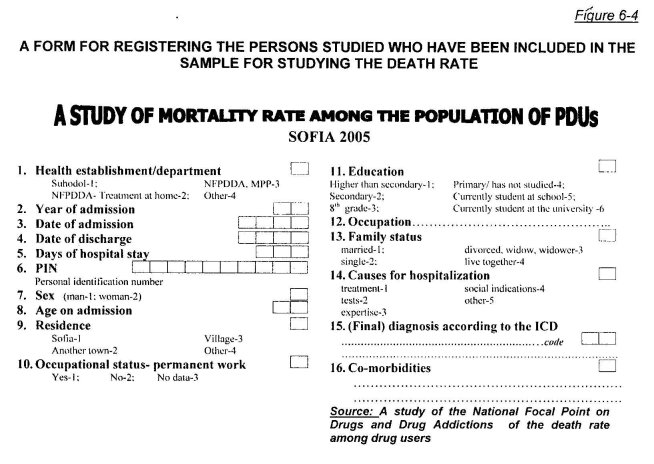
Because of the fact that for this study the patients' personal data were needed, the data collection was organized in such a way as to ensure their maximal protection. For this purpose the nurses working for the program were involved, because they have the right to process the patients' personal data. A standard form was worked out so that the necessary information could be collected from the registers (see Figure 6-4).
In the blank the following data are filled in:
• The treatment unit where the patient has been admitted (for the 1st time in the period);
• The year when he was admitted (for the first time) (1995 -1999);
• The dates of admission and of discharge (for the first treatment over the period);
• How many days lasted his/her hospital stay (during the first treatment);
• The personal identification number of the patient;
• The patient's sex;
• Age at the time of admission (for the first treatment);
• Place of residence (during the first treatment);
• Employment of the patient (during the first treatment);
• Highest level of education (during the first treatment);
• Occupation (during the first treatment);
• Family status (during the first treatment);
• Reasons for the admission (treatment, tests, etc.);
• Final diagnosis after the ICD - 9;
• Possible co-morbidity;
The data collected are checked so that double counting can be eliminated (for the different centers and for the different years). Having observed extremely strict measures to preserve the anonymity of the treated persons, a package of data was checked using the register of the National Institute of Statistics for the standard of living of the persons who had gotten into the cohort.
First results
The first results in respect to the standard of living of the patients from the treatment options numbered above who had covered by the sample, are given in Table 6-3.
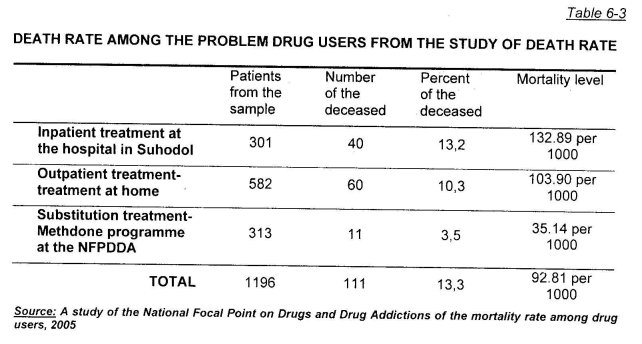
The difference in the level of mortality rate between the outpatients who are treated at home and the inpatients admitted for hospital treatment is impressive (132.89 and 103.09 per 1000 respectively) and on the other hand, there is a difference in mortality rate between these two groups o patients on the one hand and the group who are included in the methadone programme (35.14 per 1000). This may be due to the protective factor of the maintenance treatment in principle as well as to certain differences in the profile of the patients studied - in the hospital wards for treatment get severe and difficult to affect patients addicted to narcotic substances. It is till early to make definite estimations in respect to the differences in the level of mortality, because a finer data processing is still to be done. Probably other factors besides the hospital facilities are of importance for the lower death rate among the patients from the methadone programme, but unquestionably the first results showing a death rate among the methadone patients thrice lower than that among the other patients, are impressive.
The mean age of the patients who have got in the sample is 22.45 years. For comparison, the mortality rate for the same age among the general population is 0.5 — 2.0 per 1000 (for the patients from the sample the respective figure is 92.81 per 1000). The great difference existing between the two categories of population is obvious and indicative on its own. Still it is not so surprising (as a trend mostly) having in mind that the addicted patients (especially those addicted to heroin and other opioids) represent a risk group, including in respect to death, for a number of reasons related to the addiction itself and more often - to their hazardous way of life.
In relation to the distribution of deaths according to years (from the beginning of the study to the end of the period in 2004) as percentage they are distributed in the following way (see Figure 6-5):
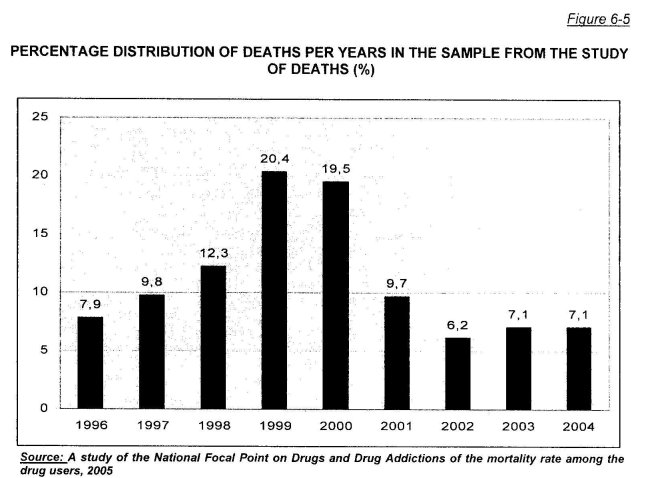
The highest mortality rate was observed in 1999 (20.4 %) and in 2000 (19.5 %). The rate was lowest in 2002 — 6.2 %.
The study of mortality rate among the drug users is a retrospective one, which, if some changes are made and new treatment programs are included in the database, can turn into a reliable routine source of information. A similar study of mortality rate can be conducted in some of the big cities of the country - Plovdiv, Varna - if there is an access to the necessary data. Similar studies present important information and can be recommended to the Regional Councils on drugs as future projects for work.
Drug Related Infectious Diseases
HIV/AIDS, viral hepatitis, sexually transmitted diseases and tuberculosis
The data presented for 2006 are taken from the laboratory of the National Centre for Addictions which is specialized for work with persons with drug addictions, and from the report of the National Committee for prophylaxis of AIDS and sexually transmitted diseases at the Ministry of Health. The data refer to patients of the National Centre for Addictions and to patients included in programs being implemented in the field in the country, as well as to a group of persons studied serving a term of imprisonment in several prisons in Bulgaria.
Short updated information on the prevalence of HIV/AIDS in Bulgaria over the period 1986 - 2007 55
By the autumn 2007 officially at the Ministry of Health a total of 803 HIV positive persons have been registered. By October the same year at the laboratories of the regional inspectorates for preserving and control of public health, the Dermatology and Venereology Dispensaries and at the Centers of Hematology and Transfusiology more than 200,000 persons have been tested for HIV.
The sexual way remains the main way of transmission - in around 83% of the cases, and for the last 2 years the number of men having sexual contacts with men has increased, and this way of transmission is followed by the blood transmission in drug users (13%), around 3% through blood and blood products (the last cases were registered in 1996) and the vertical way of transmission (from mother to child) is less than 1%.
The number of newly registered HIV-positive people for 2007 is 114, out of whom 95 are men and 19 are women, so it follows that 83,3% of the newly registered are men and 17,5% are women. For comparison - up to 2006 67% of the infected persons were men and 33% were women, i.e. there can be observed a significant increase in the number of men. 70% of the newly registered for this year HIV-positive persons are from Sofia (36 people) and from the region of Plovdiv (43 people).
Over the period observed the age of the HIV-positive persons registered varied widely - from 16 to 68 years, The mean age for men was 32 years and for women - 34 years. All the age groups are affected, and a critical decline of the lower age limit was observed - as low as 16 years. 35% of the newly registered for this year belong to the age group under 25 years.
As for the way of transmission there are two especially vulnerable groups: 36% of the newly registered are injecting drug users and 24% of all the newly registered HIV-positive are men, who have reported having had sexual contacts with men. Another 18% have been diagnosed as inpatients for whom AIDS was one of the possible differential diagnoses. The disturbing tendency still holds of identifying new HIV-positive injecting drug users. From 1986 to 22nd November 2007 their total number has risen to 105 people.
From the middle of 2006 a pilot testing, and from the beginning of 2007 a weekly testing was introduced - anonymous and voluntary - for HIV in all the places of detention. Over a period of 15 months 3 654 persons in imprisonment have been tested and consulted and among them 17 HIV-positive persons were diagnosed.
For the period 1st January — 30e' June 2007 19 surgeries for anonymous and free testing and consulting for HIV/AIDS were established (KABKIS), where 19 605 persons were tested and the total number of all the people who were tested at the surgeries since their establishment has reached 59 475 people. 60% of the newly-registered HIV-positive persons for the year 2007 were discovered by the NGOs and by KABKIS.
Data from the tests done to drug users in Sofia
At the laboratory of the National Centre for Addictions the addicted persons are tested for the following markers:
- Antibodies against HIV 1/2 — to diagnose HIV infection;
- Antibodies against HCV — to diagnose viral hepatitis C;
- HBsAg — to diagnose viral hepatitis B;
- TPHA — to diagnose Syphilis.
Diagnostics of tuberculosis and of the sexually transmitted diseases is not done because of lack of kits.
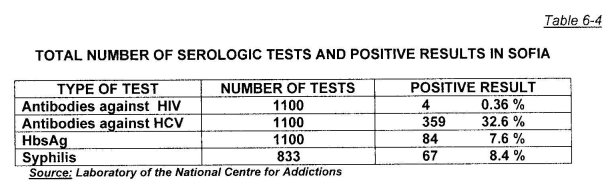
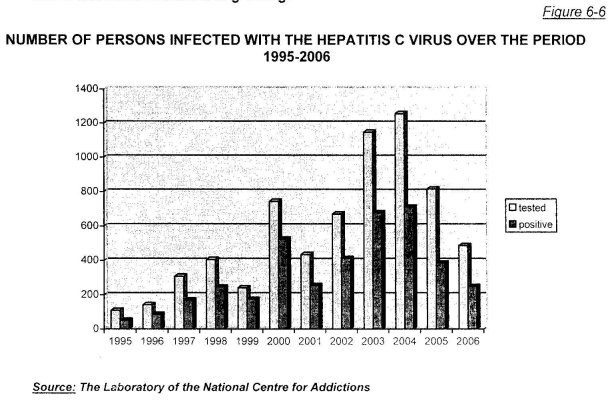
Tests and positive results for the year 2006
In Table 6-4 the total number of the tested persons in Sofia for 2006 is given, and also the positive results obtained at the laboratory of the NCA.
In Table 6-5 is given the total number of the tested iniectinq drug users at the laboratory of the NCA in the city of Sofia in 2006 and the obtained positive results.
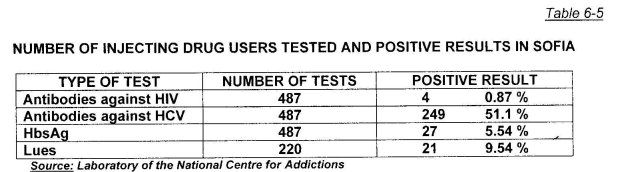
The injecting drug users tested at the laboratory of the NCA are patients of State Psychiatric Hospital for treatment of Drug and Alcohol Addictions (SPHTDAA) and clients in programs for outreach work with drug users - KARITAS and "Initiative for Health".
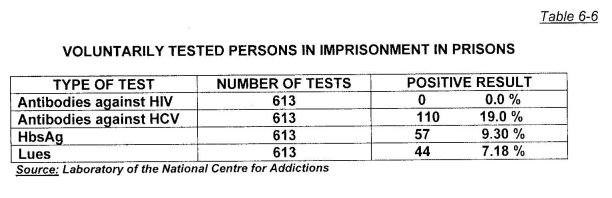
In Table 6-6 the total number of the anonymously and voluntarily tested prisoners in 6 prisons in 2006 is given and the positive results obtained from the serologic tests.
1. ANTI HIV (TYPE 1 & TYPE 2)
The total number of tested persons was 1100:
- 450 patients of the laboratory of the NCA from them 4 HIV positive; - 37 patients of the KARITAS program;
- 613 patients from the prisons.
Four of them were confirmed HIV carriers. It represents 0.36 % out of the total number of tested persons, but 0.87 % out of the number of the injecting drug users (487). Of the 4 confirmed HIV carriers the three injecting drug users have been diagnosed for the first time: 2 of them have been tested because of treatment at SPHTDAA, one of them was tested after he came back from treatment in Spain and 1 case had already been confirmed by the national AIDS laboratory, at the National Center for Contagious and Parasitic Diseases. Over the year a total of 7 cultures have shown primary reactivity, but three of them turned negative.
All the HIV - positive persons who were diagnosed at the laboratory of the NCA are also carriers of the hepatitis C virus.
2. HBsAg
Total number of tested -1100, of them 84 positive = 7.6%:
• 450 patients of the NCA - 23 positive = 5.1 %;
• 37 KARITAS patients -4 positive = 10.81 %;
• 613 patients from the prisons - 57 positive = 9.3 %.
We can note that the trend of low prevalence of hepatitis B viral infection still remains, which for the injecting drug users is within the limits of the mean rate for the country, and for the patients of the outreach programs the rate is around 50 `)/0 higher. The greatest number of HBsAg positive persons was in the prisons, but the persons tested there were anonymous and it is not known what number of them were injecting drug users.
3. ANTI HCV
Total number of persons tested - 1100, of them positive - 359:
• 450 persons from the NCA, positive - 241 = 53.6 %;
• 37 clients of KARITAS -8 positive = 21.6 %;
• 613 clients from the prisons - 110 positive = 19%.
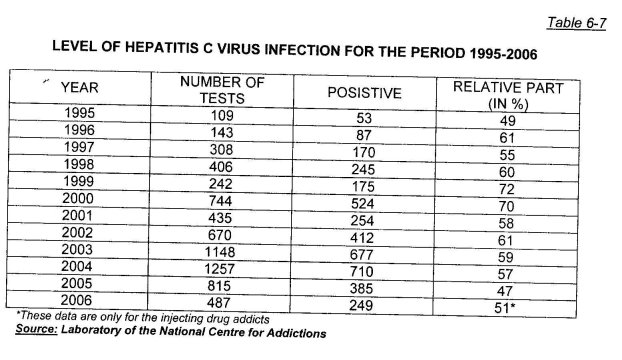
When analyzing the data a trend is outlined of stabilizing the number of the viral hepatitis C carriers, but this is due to a more precise reading of the primary testing and of the subsequent tests done.
4. SYPHILIS
The total number of tested was 833, the number of positive was 676 = 8.04 %, but for the IDUs it was 9.45%. There is an extremely lasting trend observed over the last years for the number of the ill with syphilis IDUs to remain around 10% of the tested.
Of all the 487 persons tested at the NCA 3 IDUs were carriers of both HIV and hepatitis C virus, one was infected with HIV, hepatitis C and syphilis, 16 persons were infected with hepatitis B and hepatitis C viruses; 9 persons were infected with hepatitis C and with syphilis and one person was infected with hepatitis B, hepatitis C and syphilis. It can be seen from the data that the number of co-infected with two and more infections persons among the injecting drug users is growing.
In 2006 3 babies of mothers from the methadone program — carriers of the hepatitis C virus were tested for hepatitis C infection and the results of the test were negative. With these children added the total number of the babies of mothers participating in the methadone programme tested over the last 5 years is 14 and all the results are negative.
From the analysis of the results the following points can be noted:
1. The level of the HIV infection is low, compared to the prevalence in other countries from the region, but for the last 2 years it has marked a trend of rising for the injecting drug users.
2. The level of hepatitis B infection remains at about 5 % (6.10%), and this value has remained constant for the last 10 years; it is comparable to the general hepatitis B morbidity in the country.
3. The level of infection with the hepatitis C virus for all the IDUs tested at the NCA,,is 53.63 %. It can be noted that there is a trend for the level of infection to remain constant, which may be due to the better work of the needle and syringe exchange programs.
4. From the data it can be seen that the number of persons among the IDUs co-infected with 2 and more infections is growing.
Psychiatric co-morbidity (double diagnosis)
On the data of the Toxicology Clinic at the "N.I.Pirogov" Multi-Profile Hospital for Active Treatment and Emergency Medicine /MHATEM/ over the period 2004 — 2006 there were treated a total of 537 patients with addictions. 112 of them (22%) had abscesses at the injection site. Two of all the patients had tuberculosis. No tetanus or botulism was diagnosed. Septic endocarditis was found on the post-mortem of one of the deceased.
In all the inpatients treated there was observed: personality disorders, depression, anxiety, and 10 of them had schizoaffective or bipolar disorder (they were admitted with this diagnosis).
In respect to the somatic co-morbidity the following cases have to be mentioned: 4 patients with heroin addiction had non-traumatic rhabdomyolysis with acute renal failure; 5 patients had inflammatory process of the lungs.
Other health correlates and drug related consequences
Drug related non-fatal emergency cases
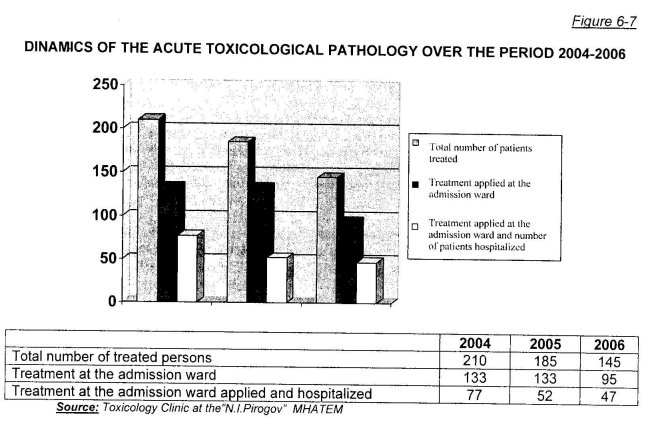
For the last 3 years (2004— 2006) at the Toxicology Clinic at "N.I.Pirogov" MHATEM 537 patients with drug addictions were treated (450 men and 87 women), who sought medical aid because of acute intoxication. They represent 2,9 % of all the patients who have visited the admission surgery of the Toxicology Clinic (24 678 clients). Of the total number of drug addicted persons the number of heroin abusers is 498.
The dynamics of this acute pathology in toxicology over the last 3 years is represented on Figure 6-7.
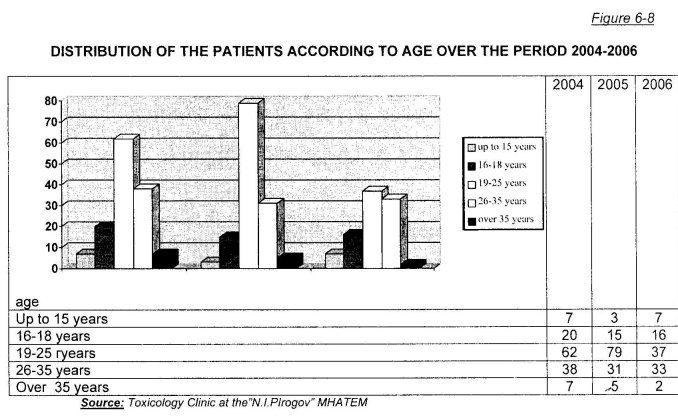
The distribution according to age is represented in Figure 6-8. The greatest number of drug-addicted patients is in the age sub-group 19-25 years —33 %.
For the heroin addicted persons the main way of applying the drug is the intravenous way — 90,97 %.
For the indicated period of 3 years 3 of the inpatients died - indirect deaths (2 patients had sepsis and 1 had non-traumatic rhabdomyolysis with acute renal failure).
In the group of patients admitted for an overdose of heroin, there were no deaths registered irrespective of the severity of the clinical condition (including lack of breathing). This is due to the reanimation done and adequate antidote treatment - bolus doses of naloxone.
Because of this the mortality rate for the period 2004-2006 year is extremely low-around 0,006 %. A number of the patients leave the hospital immediately after the resuscitation of the vital functions - explicit objection to treatment.
384 of the heroin abusers are hepatitis C virus carriers — 77,1 % on the data of their history. HIV carrier is one female patient — on the data from her history; other virology tests have been done to the rest of the patients and they were negative.
52 The intensity (frequency) of deaths according to causes is calculated as the ratio of the number of deaths for a definite cause and the average annual number of persons from the respective population. It is usually calculated per 100 000 persons of the population.
53 "A Study of the Mortality Rate among the Population of Drug Users — Sofia 2005' cohort, retrospective, National Focal Point on Drugs and Drug Addictions,1196 problem drug users included, who were treated in the city of Sofia over a 5- year period (1996— 1999)
54 See below in the "Problem Drug Use" chapter in the Annual Report on the condition of drug - related problems n Bulgaria - 2006
55 Source: "Prevention and Control of HIV/AIDS" Program — Ministry of Health (on-line at: )
| < Prev | Next > |
|---|