| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 210 |
| Yesterday: | 251 |
| This Week: | 210 |
| Last Week: | 2221 |
| This Month: | 4798 |
| Last Month: | 6796 |
| Total: | 129397 |
Report 6 Drug problems
 |
|  |
| 
| Reports - A Report on Global Illicit Drugs Markets 1998-2007 |
Drug Abuse
2 Drug problems
2.1 Production
There are two main sources of estimates of illegal drug production specifically for cocaine and heroin: the UNODC (The World Drug Report) and the U.S. State Department (The International Narcotics Strategy Report). These data sources use different methods for estimating areas under cultivation. The U.S. State Department, for instance, relies primarily on satellite imagery, while the United Nations, having developed a strong presence in the major production countries, is able to evaluate on the grounds of the results of aerial surveys.
Area under cultivation – opium and coca plant
The resulting calculations of these two organisations often produce quite different estimates of the area under cultivation. For example, the United States (U.S. Department of State, 2006) reported 51,500 and 64,510 hectares of poppy cultivation in Afghanistan in 1999 and 2000 respectively, suggesting a substantial increase; the United Nations (UNODC, 2006), however, reported 90,583 and 82,171 hectares for the same years, suggesting a substantial decrease. The differences in the U.S. State Department and United Nations estimates for Afghan cultivation in 2004 are even more dramatic: the United States reported 206,700 hectares and the United Nations reported 131,000 hectares.
Opium and coca plant yield estimates
For annual production estimates of opium and coca leaf it is necessary to develop estimates of the yield per hectare of opium or coca leaf and the efficiency of processing. However, these estimates are sensitive to:
• Weather conditions over the year, since the surveys are conducted at a specific time during the growing and harvesting cycle;
• Definitions of cultivation areas; sampling strategies from other sources, for example, does not necessarily fit UNODC’s definition of an area under cultivation (UNODC, 2008);
• Production techniques used and the competence of the operators.
Transformation ratios used to calculate the potential production per hectare poppy field or coca bush, require detailed information about local morphine content in opium or alkaloid content in coca leaf. Since 2005, as a result of field studies, the UNODC has used a 7 to 1 ratio for the transformation of opium into heroin. Both the UNODC and the U.S. State Department have recognised that these ratios vary across sub-national areas and that they can vary over time. Updates of these ratios in official estimates occur infrequently, and at different times for the two organisations.
The United States government has occasionally announced major changes in its estimates, resulting from revisions in its assumptions about yields – in particular, the amount of opium, morphine or heroin that can be obtained from each hectare of poppies – in specific countries. For example Operation Breakthrough in Colombia led the United States Drug Enforcement Administration (DEA) to revise production estimates because it now believes that most poppy fields are harvested only twice annually, and not three times (Drug Availability Steering Committee, 2002).
Opium and cocaine production efficiencies
Yet another source of uncertainty is the efficiency with which the farm product is processed. A review of United States methods used for estimating drug availability highlighted the variability of these figures. “The estimate for cocaine base processing efficiencies in Colombia was changed from about 45 percent to 69 percent as a result of DEA research published in Operation Breakthrough, February 2001. The higher efficiency factor has been applied to all estimates going back to 1995” (Drug Availability Steering Group, 2002).
These computations therefore result in differences between the United Nations and United States estimates. For example, in 2004, the implied yield of opium per hectare in Afghanistan was 24 kg for the United States compared to 35 kg for the United Nations.
Cannabis
Marijuana differs from cocaine and heroin in that it is produced in many countries. It is considered the “globally most dispersed illegal drug” (UNODC, 2008). One hundred and seventy two countries report cannabis production in their territory, according to the UNODC World Drug Report 2007 (UNODC, 2007). Most produce only for domestic consumption and are able to satisfy most of the domestic demand. This makes it particularly difficult to estimate total production of cannabis (Leggett & Pietschmann, 2008), since the plant is not grown in large fields in concentrated areas of a few countries, as are opium and coca leaf.1 Yield estimates reported by European countries to the UNODC vary from 5 kg per hectare for wild cannabis to 17,500 kg per hectare for countries reporting high proportions of hydroponically grown cannabis (Legget & Pietschmann, 2008).
Cannabis production estimates may also vary because of differences in:
• Methods of determining the cultivation area (ground surveys, remote sense technologies, e.g., satellite image techniques) or searching for illegal grow factories of cannabis with analysis of, amongst other things, data on used electricity);
• Cultivation techniques used (e.g., the use of artificial light in growing rooms, inclusion of relative inert plant material, techniques for increasing the active parts of the plant);
• Type of end product (e.g., cannabis plant, resin, seeds or oil);
• Calculation of the potential production from cannabis plant (units or kg) to cannabis resin (kg) require detailed information about production techniques and THC content on a national level whereas, at best, there may be some data available on a local level.
A recent papers on production in Quebec by Martin Bouchard (forthcoming), using more detailed knowledge of the production process and more sophisticated estimation techniques, suggest that existing estimates are most probably too high.
Amphetamine type stimulants
Production of ATS is even more difficult to estimate, even though it is not produced in as many countries as cannabis. This is due to the geographic dispersion and temporary nature of laboratories that produce these synthetic drugs. Finding the laboratories requires specific expertise for targeted investigation and enforcement activities. Moreover, the measurement of the number of drug manufacturing sites (laboratories) differs both between and within countries and over time. For instance, there is no standard measure of what is a large or small lab and in many countries the size of the laboratories dismantled is not reported. The number of dismantled laboratories does not provide any information about the quantities actually produced.
Drug prices
Worldwide information systems covering data on prices of drugs are insignificant. The United States appears to be the only country to have developed a transaction level database, reflecting undercover purchases by federal agents and a few police agencies (Manski et al., 2001). The validity of these data (STRIDE: System to Retrieve Information from Drug Evidence) as a representation of actual market transactions has been a matter of dispute. Horowitz (2002) criticised STRIDE, while Caulkins (2002) and Rhodes & Kling (2001) defended them. A critical aspect of STRIDE is that each observation takes the drug’s purity into account, as well as its price and quantity. For European countries, apart from Norway (for heroin), no such comprehensive data exist. At best, as in the United Kingdom, Australia and New Zealand, there are data for price and purity separately. As many countries are reporting price data through a systematic questionnaire, the UNODC Annual Reports Questionnaire, there is simply no well-documented basis for the figures. Thus the data reported should be analysed with caution.
In Afghanistan and Myanmar the UNODC collects a substantial number of observations on farm gate prices and, at least in Afghanistan, is able to generate sub-national price series. In several reports, farm gate prices and wholesale prices are reported (cf. UNODC, 2008; Uribe-Ramirez & Navarrete-Frías, 2009; International Crisis Group, 2008). The agency also reports farm gate prices for coca and coca paste for each of the three Andean producers (UNODC, 2008a).
1 For a discussion of the absurdity of earlier U.S. estimates of Mexico’s marijuana production, see Reuter (1996).
2.2 Trafficking
Drug trafficking refers to the quantities of illegal drugs imported into, exported from and transhipped through a country. Apart from these quantities, it would also be advantageous to be able to describe how they are distributed among different trafficking routes, in order to have an insight into the international routes of transportation, and also into the flow of illegal drugs between countries. These hidden activities are difficult to capture with administrative records. Neither quantities nor routes can be directly determined.
It is hard to think of systems that would provide valid measures of either quantities trafficked or their distribution routes; certainly, none have been suggested. The only available indicator for trafficking is seizures of illegal drugs, annually reported in UNODC’s World Drug Report. In fact, it is a highly questionable proxy for the total quantities of drugs imported, exported and transhipped through a country. Moreover, it is not clear how a better indicator could be generated on a routine basis and at a reasonable cost. So instead, for quantities, two proxy-measurements have been used: the number of seizures and the quantities seized. Both are very unsatisfactory and require a great deal of detailed knowledge for interpretation.
The quantity of a drug seized in a country is a function of many factors: the intensity and efficiency of police and interdiction efforts; the methods used by traffickers; and the total quantity shipped. The price can also have an effect; if the purchase price in the exporting country declines, then smugglers will be willing to invest less in protecting the shipment and may thus use cheaper but more vulnerable trafficking methods.
Seizure statistics are not always complete. In the United States, with its federal system, the DEA only counts seizures by federal agencies (Customs, DEA and border patrol). Seizures by state and local agencies (e.g., the New York Police Department) are ignored, although they may be substantial. In unitary countries, such as France, the statistics may be more complete.
Though no reliable method exists for estimating the total quantities of drugs seized, drug seizures are used by the EMCDDA and the UNODC as an indicator for trends, patterns and routes of drug trafficking, especially over longer periods of time and over larger geographical entities (UNODC, 2008). Based on this approach, it is assumed, for instance, that North America is the largest market for cannabis herb (63% of global seizures in 2005), followed by Africa (18% in 2005). The percentage for Europe in this year is 2%. However, for cannabis resin, Western Europe is the largest market and is responsible for more than 70% of global seizures in 2005 (Leggett & Pietschmann, 2008).
Drug trafficking routes are assessed through international analysis of production, trafficking and consumption figures for specific drugs. Research in this area is still sparse (see also report 1). Such reports on international smuggling routes are often based on brief qualitative descriptions of the most important routes mentioned in literature, and on drug supply data of varying quality. Critical analysis of this information (often coming from the police, customs, etc.) is not widespread but this could be a basis for refuting perceived truths about drug trafficking routes.
2.3 Drug retail/trade
The difficulties in estimating the scale of total retail sales are covered in detail in Report 2. Here we provide only a brief summary.
The above-mentioned difficulties in determining drug trafficking and its revenues are also relevant for drug retail or smaller-scale drug trade. A variety of methods exist for estimating national retail quantities of illegal drugs. They may be based on drug use estimates or drug-related arrest data, but these offer no more than rough indications of the total amount of drug retailed among users or drug dealer networks.
An additional dimension that complicates retail quantity estimates is drug purity (estimated or tested). Low purity inflates the total weight of drug supplied (imported or exported), but this phenomenon takes place predominantly at the end of the supply chain (retail level); it does not necessarily inflate actual prices (Reuter, 2001). Moreover, prices of illegal drugs, “(…) whatever the drug and however calculated, appear to vary enormously across and within countries as well as over time“ (ibid.). Both the price per gram and data on drug purity are used as indicators for the identification of market trends (UNODC, 2008). These data may come from extremely varying sources (qualitative, exploratory data from users, testing of seized drug samples, etc.) and are usually inconsistent or limited, especially in developing countries. This makes comparisons across countries difficult to interpret. Worldwide, we have insufficient information about data collection methods, reliability and specified variations (UNODC, 2008).
2.4 Drug consumption
The most commonly reported consumption measure is population prevalence, namely the percentage of the population that uses specific drugs within a given period. Many countries conduct surveys to produce estimates of this percentage. Important as these surveys are, they have turned out to be quite frail as measures of the extent of drug use in various populations. Cross-national comparisons of prevalence rates are complicated by differences in study design.
Firstly, random surveys of the general population systematically underestimate drug use, in particular problem drug use. Problem drug users are difficult to identify by population surveys. Most studies use households (or those with telephones in households) as the source of participants. Several so-called indirect prevalence estimation methods, e.g., capture-recapture analysis, have been developed to improve the accuracy of estimates of drug use among these groups (EMCDDA, 2001) but these methods are not yet used in many countries.
Surveys also differ in age coverage. For example, the United States cover the population aged 12 and above; the Netherlands 15-64; Hungary 18-59; and the United Kingdom 16-59. Since prevalence rates differ for these different age groups, these differences in range may have large consequences for cross-country comparisons.
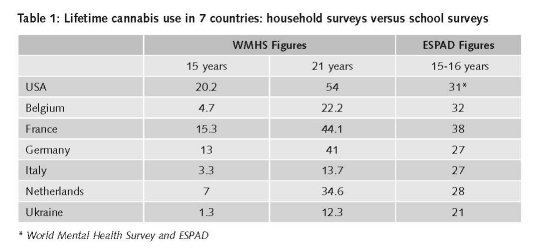
School versus household surveys
A sense of the importance of methodological differences can be gained by comparing a recent study of drug use based on the World Mental Health Survey (Degenhardt et al., 2008) with results from the ESPAD survey and Monitoring the Future in the United States. Table 1 shows figures for lifetime prevalence for cannabis, the drug best studied through general population surveys, at ages 15 and 21. ESPAD provides data on persons who turn 16 in the calendar year of the survey, so it should be moderately higher than the WMHS figures for age 16, which are based upon the retrospective reports of adults who are older by the time they were interviewed. In fact, the ESPAD survey shows much larger rates. In two countries (Belgium and Italy) the ESPAD rate is even higher than the WMHS rate for age 21! The source of these discrepancies has not been examined but is probably due to differences in study design, i.e., questionnaire construction.
Differences in period covered
Another data collection problem is inherent in making comparisons over time. Few countries mount national population surveys on drug use every year (as in the United States). More typically, these studies are carried out every three to five years, or with irregular intervals in time, even in high-income countries, e.g., Canada, where the last Canadian Addiction Survey data were reported in 2005, with additional analyses of the same study for youth and gender in 2007 and 2008. Another example is Switzerland. The most recent published general population survey is from 2002. A new survey was conducted in 2007, but as of January 2009 only a few initial results had been published. Important indicators may not be available for the same year, so that a country may have a drug use survey for 2004 but an estimate of problem drug use for 2006. If the drug situation is stable, this is a small problem, but if the country is still in the epidemic stage, with rapid change, aggregating these measures as though they came from one year will inevitably create distortions.
This also has consequences for comparisons across countries and global estimates. For one country the indicators may cluster in 2004, while in another they may cluster in 2006. This difference may be important. In Canada, for example, the availability of prevalence data is of limited value for this study, because three surveys were conducted in 1989 (National Alcohol and Drugs Survey - NADS), 1994 (Canada’s Alcohol and other Drugs Survey - CADS) and 2003-2004 (Canadian Addiction Survey - CAS). On the other hand, Australia published household survey results in 1998, 2004 and 2007 (Australian Ministry of Health and Welfare), covering exactly the measurement years we are aiming at.
Limited geographical coverage
General population surveys are expensive. As a result, some countries do not conduct them, or choose to conduct them under more easy-to-reach subpopulations. Brazil published, for example, a number of studies that were restricted to major urban areas, e.g., the ten largest state capitals (Galduróz et al., 2004). Rural data collection by face-to-face interviews (phone penetration is low) has not been considered feasible. Mexico and South Africa also conducted surveys primarily in major urban areas (Medina-Mora et al., 2003; Da Rocha Silva & Malaka, 2007). Though these decisions may well be justified, the result is that comparisons of prevalence rates across these countries require careful preliminary analysis to attempt to account for plausible differences between the covered and non-covered populations.
Differences in interview methods
Differences in interview methods can also affect estimates. It is evident that in-person surveys in households generate higher prevalence rates than telephone surveys. In turn, for youth, anonymous surveys within classrooms generate higher rates than in-person surveys, because of the greater guarantee of privacy. Mail surveys may lead to estimates of prevalence still lower than those from phone interviews. In-person surveys are substantially more expensive than phone interviews, so most countries use the latter, though, as the above-mentioned example of Brazil illustrates, this is only feasible in countries with high telephone coverage. These differences call into doubt the validity of comparisons across countries that employ different survey methods.
Finally, the period of drug use covered by the survey may be important. Most surveys ask whether a drug has been used at least once in the respondent’s lifetime. Many (but not all) surveys ask about use within the last year, which tells us more about current use. For instance, the last Mexican surveys were limited to lifetime prevalence. In EU Members States’ surveys, last month prevalence is also frequently covered. In the three Canadian surveys (NADS, 1989; CADS, 1994 and CAS, 2003-2004), drug use over the last three months among younger people (15-24 years) was reported (CAS, 2007: table 5.2).
Surveys may also differ in their definition of specific drug categories. It raises, for instance, the uncertainty on how to relate tables that present figures on ATS with tables that only present figures on (meth)amphetamines and ecstasy, or with tables that only report data on the use of speed. It is not entirely clear how to compare these figures under the concept of “ATS” (cf. CADS, 1994).
2.5 Problem drug use
As mentioned above, surveys on drug use are known to substantially underestimate rates of frequent use of drugs.
This under-reporting is often quite substantial for heroin and cocaine. For example, in the United States, the National Survey on Drug Use and Health (NSDUH), the annual general population survey, estimated that 595,000 persons had used cocaine in 1998, at least eight times in the previous month. However, indirect prevalence estimates that take into account data from arrestees (the Arrestee Drug Abuse Monitoring system - ADAM) produced an estimate of past month users that was more than 5 times higher, namely 2.8 million (ONDCP, 2001). For heroin use, the NSDUH is used solely to estimate the prevalence of occasional use; estimates of high frequency use rely entirely on ADAM. Prevalence of high rate cocaine and heroin use also seems to be substantially underreported in the household survey in the United Kingdom. Pudney et al. (2006) estimate the total cocaine and heroin consumption in the United Kingdom and, although they do not report prevalence among arrestees as compared to non-arrested respondents, they do report that arrestees account for the majority of total cocaine and heroin consumed.
Two guidelines were published in the European context: one on estimating problem drug use and a recent one on estimating the incidence of problem drug use (EMCDDA 2004a; 2008). Since 2001, problem drug use prevalence has been one of the five epidemiological key indicators used in the national reports that are annually sent to the EMCDDA (EMCDDA, 2001a). Before and after 2001, the EMCDDA worked hard to clarify this concept by trying to harmonize registrations, offering estimation methods, and finding ways to estimate development of problem drug use over time.
In countries outside Europe, the lack of consensus on problem drug use is more manifest. Brazilian data on problem drug use are, for instance, reported under headings such as ‘dependency’ or ‘frequent users’, the latter being defined as using a specific drug more than five times per month. Capacity problems may also have been an important factor in not measuring (or reporting) problem drug use at all in many countries.
2.6 Drug-related harm
“Drug-related harm” is a broad concept. It can be understood as adverse effects experienced by drug users (health consequences), their intimates (family, friends, school) or society (drug-related crime, nuisance, loss of workforce, etc.). It covers many domains, for example, drug-related death, infectious diseases, mental health, social functioning and crime.
Drug-related harm is both conceived and measured differently within and between countries. Drug-related death is one of the few indicators for which cross-national efforts have been made to produce national estimates on a consistent basis (EMCDDA, 2004). Nevertheless, even for this indicator, several fundamental difficulties remain.
Validity of data on drug-related deaths is hampered by several methodological shortcomings and differences (EMCDDA, 2007). Firstly, the quality of official drug-related death statistics varies from country to country. In general, “reported death rates amongst hidden populations are (…) understatements” (Darke et al., 2007). Due to the hidden nature of illicit drug use, some overdose cases may not be picked up as drug-related death. Wealthy countries are far more likely to have the resources and infrastructure to devote to collecting data on mortality and its specific causes than poorer countries (Darke et al., 2007).
Less important, but still noteworthy, are variations in definitions used. The EMCDDA restricts itself to direct or acute drug-related deaths, i.e., caused directly by the consumption of one or more drugs (EMCDDA, 2004), as do the United States and many other countries. This restriction excludes indirect drug use-related death, for instance death caused by drug-related chronic conditions, such as liver failure due to hepatitis that might be the consequence of injecting drug use. Indirect drug-related deaths may also be the result of drug-related violence towards drug users or amongst drug dealers or gangs. Finally, it also excludes suicide or accidents, that may be due (in part at least) to drug use.
As mentioned in the introduction, the differing definitions of the term ‘drug’ between English-speaking and other countries causes misunderstanding in comparing figures on drug-related deaths. For instance, discussions on a European definition of this concept led to the exclusion of medical drugs (used for suicide) from DRD reports for the EMCDDA. In some countries, the figures on drug-related death include overdose by medical drugs (e.g., in the Czech Republic), while in other countries only acute overdoses due to the use of illegal substances are included. The result is that the reliability of the European statistics, especially from earlier years, is low. Still, the monitoring work allows comparison of developments in one country over the years, unless the recording system has changed.
Epidemiological data on HIV infections are reported for the general population. Only a small number of countries present these data for the subpopulation of drug users. Collection of prevalence data on other diseases such as Hepatitis B and C started quite recently. They do not yet allow for international comparisons over a longer period of time. For HIV, the available statistics are often restricted to numbers of newly infected drug users. In many publications, no figures are reported on the total number of drug users who are infected.
| < Prev | Next > |
|---|