| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 201 |
| Yesterday: | 251 |
| This Week: | 201 |
| Last Week: | 2221 |
| This Month: | 4789 |
| Last Month: | 6796 |
| Total: | 129388 |
 |
|  |
| 
| Reports - WHO: The Use of Cannabis |
Drug Abuse
3. EPIDEMIOLOGICAL ASPECTS
In studying the epidemiology of cannabis use, it is important not only to inquire into the prevalence and incidence of such use in different localities and regions but also to ascertain (a) the properties of various cannabis preparations used,3 (b) the characteristics of persons who do and do not use such preparations,3 and (c) the sociocultural factors associated with their use in each locality studied.4
An element of communicability is associated with initiation into the use of cannabis preparations. Initial interest in taking these preparations appears often to be communicated directly or indirectly from a user to a non-user. This seems particularly relevant to the experimental or recreational use of cannabis by adolescents and young adults.
3.1 Manner of use (mode of consumption, frequency, amount, and duration)
The primary mode of consuming cannabis is by smoking, but it may be ingested as a food or beverage.3 India is the only country in which a significant amount is taken orally, in the form of a beverage made from bhang. Cannabis is also consumed in numerous confections and other food preparations, especially in India and sometimes in North Africa and other regions (Bouquet, 1951; Chopra & Chopra, 1939); however, in most parts of the world this mode of consumption is minor compared with smoking. The stronger preparations, e.g., ganja and hashish (or charas), are normally smoked in a pipe, which is sometimes so constructed that the smoke is first passed through water. The crude forms, which are less potent, may be smoked in either pipes or cigarettes.
Another aspect related to patterns of use is the extent to which admix-tures of other drugs are consumed together with cannabis. Tobacco is often a standard part of the smoking mixture in the Indo-Pakistan sub-continent and in some other regions of the world; however, mixtures with drugs other than tobacco appear to be relatively rare, except by persons who use cannabis in large amounts. In India and Pakistan datura (containing scopolamine, atropine, and other belladonna alkaloids) is occasionally added.'
A meaningful evaluation of the consequences of cannabis use for the individual and society must take into account the frequency, amount, and duration of use and the relative numbers of persons conforming to various usage patterns. Studies in the USA indicate that occasional users far outnumber those who use cannabis daily,2 whereas reports from the Indo-Pakistan subcontinent and North Africa are frequently concerned only with regular users; throughout the world, however, it appears that the majority of cannabis users take the drug occasionally rather than daily.3 In countries such as India and Morocco, where cannabis use has been more or less accepted, the daily use is measured in grams and only amounts in the upper range are considered " excessive ". In India, the usage is considered moderate if around 1-2 g of ganja per day,4 or an estimated 30-60 mg of 6.3-THC.6 The majority of daily users are reported to fall within the moderate range. Chopra & Chopra (1939) conclude that, in India, " moderate use is much more common and excessive use is exceptional ". The Indian Hemp Drugs Commission (1894) similarly estimated that excessive users represented only about 5 % of ganja smokers.
While the amount of cannabis used daily is usually discussed in terms of moderate and excessive (terms that have different meanings in different reports), the amounts consumed probably exhibit the same type of unimodal frequency distribution as alcohol consumption, i.e., the large majority fall within the low end of the continuum, and progressively smaller fre-quencies are obtained as the high end of the scale is approached.6
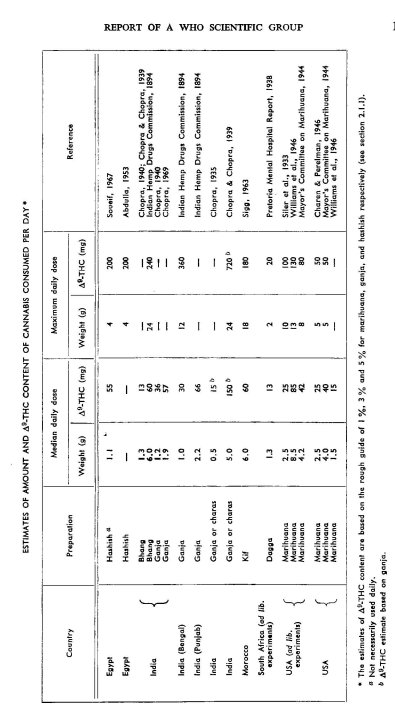
The table shows various estimates of daily use, as well as estimates of the A3-THC content based on the assumption that marihuana (and equivalents), ganja, and hashish (charas) contain 1 %, 3 % and 5 % of A3-THC respectively.7 In the compiling of these estimates, marihuana cigarettes were assumed to weigh 0.5 g. With the exception of one Indian study based on a sample of " heavy " users (Chopra & Chopra, 1939), the average daily dose of A9-THC for India and North Africa ranged from 13 to 66 mg. The maximum daily doses were in the range of 200-700 mg. The average amount of A9-THC consumed in ad libitum marihuana exper-iments in the USA,1 and by daily users in the 1940s (Charen & Perelman, 1946; Mayor's Committee on Marihuana, 1944), was comparable to that for users in India and North Africa; however, the maximum amounts were substantially lower. The amounts indicated in the table contrast sharply with the typical consumption of one or two marihuana cigarettes (5-10 mg of A9-THC) per day during the recent wave of marihuana use in North America and some other areas.
The duration of cannabis use is important. Many authors imply that, once the use of cannabis is well established, it is likely to continue on a daily basis for many years and is not infrequently a lifetime practice (Bouquet, 1951; Chopra & Chopra, 1939). However, longitudinal data on representative samples of users are seldom if ever cited, and there is some indication that, in India and North Africa, the period of time over which cannabis is used by individuals may have been exaggerated (Soueif, 1967). In other parts of the world there are frequent references to discontinuation of its use after adolescence (Robins et al., 1970; South Africa, Inderdepartmental Committee, 1952) and to intermittent use among others (Mayor's Committee on Marihuana, 1944). In one follow-up study of regular marihuana users in the USA, one-half were still using marihuana twice or more a week after 20 years (McGlothlin et al., 1970).
3.2 Reasons for starting and continuing to use cannabis
Association with other users, curiosity as to the effects of cannabis, and a desire for relaxation, relief from tension, or a pleasurable feeling are widely cited as reasons for starting to use cannabis.2 Becker (1953) stressed that initiation into the practice by other users plays an essential role, arguing that the novice must learn (a) to smoke effectively, (b) to recognize the effects, and (c) to define them as pleasurable. Especially in India, religious and medical purposes play a role in initiation (Chopra & Chopra, 1939). Many people said that they started using cannabis in an attempt to substitute it for alcohol, opium, cocaine, or other drugs (Chopra & Chopra, 1939; Ewens, 1904). The purported aphrodisiac property of cannabis is cited as a reason for starting its use by some individ-uals included in samples of users in India and North Africa (Chopra & Chopra, 1939; Soueif, 1967).
One of the more frequently stated reasons for continuing to use cannabis moderately is the sense of well-being, relaxation, and relief from tension experienced.' It is used less frequently in an attempt to enhance sexual satisfaction 2 and to increase the enjoyment of music and food.3 It is also reportedly taken to alleviate hunger (Chopra & Chopra, 1957; Indian Hemp Drugs Commission, 1894). Another stated reason for its continued use is relief from boredom, frustration, and depression (McGlothlin et al., 1970).
There are a number of references to its use among labourers for the purpose of allaying fatigue and increasing endurance 4 (cf. section 4.2.1). In Europe and North America, users sometimes cite enhanced performance in creative efforts as a reason for using cannabis (McGlothlin et al., 1970) (see section 4.2.1). In India, cannabis continues to be used for self-medication to relieve or prevent various symptoms (Chopra & Chopra, 1957). As noted earlier, there is a long history of cannabis use in religious practices, both in celebrating various religious holidays and in use by priests and other religious figures (Chopra & Chopra, 1939). Among the latter, it is used as an aid to meditation and to the attainment of mystical states. Wandering religious mendicants frequently remain in a state of chronic cannabis intoxication, which is interpreted as a religious trance by their followers (Chopra & Chopra, 1939; Indian Hemp Drugs Commission, 1894). The religious use of cannabis has been noted among certain cultural groups in Central and South Africa (Chopra, 1969), Brazil (Batista, 1959; Cordeiro de Farias, 1955), Jamaica (Blum & Associates, 1969a), and Mexico (Livet, 1920); it is generally limited to ceremonial use.
There are a few references to the use of cannabis in Africa to provide courage and bravado for fighting and sexual conquests.5 and an occasional mention in history of its use by certain warrior groups in India (Chopra & Chopra, 1939; Indian Hemp Drugs Commission, 1894). In general, its use for such purposes appears to be quite rare. According to Postel (1968), it is smoked by United States soldiers in Viet-Nam as a relaxant, but not in combat.
Social reasons are adduced for the use of cannabis. Cannabis, more than any other intcodcant, is used throughout the world in small social settings, so that the desire to achieve a sense of belonging to an intimate group is undoubtedly a significant factor both in beginning and in continuing to use it. The social intimacy may be intensified by the precautions required to avoid legal sanctions (Becker, 1953; Goode, 1969).
3.3 User characteristics
Attempts to discover a common set of characteristics among cannabis users of different cultures quickly reveal the necessity of distinguishing between " moderate " and " heavy " users. For the most part, moderate use appears to be influenced, more than does heavy use, by such factors as local customs and attitudes, the availability and cost of the drug and, perhaps most important, association of the individual with a peer group using the drug.1 However, users — though with numerous exceptions — tend to possess certain characteristics, despite differences in sociocultural setting and extent of use.
Cannabis use is related to age. It is generally most popular among adolescents and young adults ;2 however, consumption in India is said to show a fairly even age distribution at present (United Nations Economic and Social Council, 1957), while in Thailand it has reportedly been largely restricted to elderly persons (United Nations, Commission on Narcotic Drugs, 1965). At present initiation is most frequent during adolescence,3 but Chopra & Chopra (1939) found that 40 % of their sample of regular users began after the age of 30 years.
The extent of cannabis use is closely related to sex. Except in Europe and North America, the extent to which females use it is extremely low. Even in these areas, the extent to which it is regularly used among women is low compared with that among men.
In general, cannabis users have tended to belong to certain socio-cultural groups. Except in relation to the current upsurge in Europe and North America, its use —especially its regular use — has been mostly restricted to the lower socio-economic groups. This was true also among earlier users in Europe and North America.4 At one time cannabis pre-parations were widely used by the upper classes in India (Indian Hemp Drugs Commission, 1894), among whom the occasional ceremonial use of bhang is still quite common A few authors indicate that the use of cannabis preparations is widespread, but not readily apparent, among the upper sociocultural classes of North Africa (Bouquet, 1951; Roland 8c Teste, 1958). However, the use — especially the regular use — of cannabis is currently held in low esteem in almost all countries of the world. Its generally illegal status contributes to this attitude, although disapproval generally preceded rather than followed the imposition of legal controls (Indian Hemp Drugs Commission, 1894).
Within the broad " normal " range, certain personality characteristics are associated with some cannabis users. Individuals who appear to enjoy the effects of cannabis tend to prefer an unstructured and spontaneous style of life, are relatively prone to take risks, value states of altered consciousness, and tend to seek such effects both through drugs and through other methods (Cohen, 1970; McGlothlin et al., 1970). Thus cannabis users are most frequently young, male, unmarried, and exhibit some instability with respect to residence, work, school, and goals. Individuals who have no taste for the cannabis experience per se (regardless of moral or other considerations) are more apt to exhibit a preference for a controlled, structured, rational, and secure approach to life.
Excessive use is associated with personality inadequacies. Persons who exhibit emotional immaturity, low frustration tolerance, and a failure to assume responsibility tend to be over-represented in samples of heavy cannabis users.' In behavioural terms, these traits are manifested in an unrealistic emphasis on the present as opposed to the future, a tendency to drift along in a passive manner, failure to develop long-term disciplines and skills, and a tendency to favour regressive and magical to rational thinking.
3.4 Sociocultural factors
The taking of drugs, particularly cannabis, appears to be associated not only with certain individual and group beliefs and expectations about the effects but also with a broader system of beliefs and values concerning such matters as (a) the relative worth of material posessions and of spiritual, cultural, and traditional beliefs and experiences; (b) the respective im-portance of the rights, prerogatives, and responsibilities of the individual and of society; (c) the nature of practices that are considered good and evil; and (d) the meaning and value of life itself (Cameron, 1970).
Cannabis has been taken in modest amounts on a casual basis to foster a personal sense of ease. freedom, and relaxation, to serve as a social lubricant, and as evidence of friendship and of membership in a particular group.2 This has occurred in many geographic areas, among many different sociocultural Flroups, and at various points in time.
Considerably more intensive use than that just mentioned, as regards frequency and quantity, is often strongly associated with powerful socio-cultural forces in addition to those of friendship, peer group approval and pressures, and local customs. One such factor, associated with fairly regular and particularly with heavy use, is rapid sociocultural change.
This is often found in situations involving, for example, industrialization, urbanization, social conflict, and transition between periods of war and peace; there may or may not be substantial migration within the area affected. In such circumstances an individual's system of values may be changing and he may find himself somewhat removed from the usual cultural restraints placed upon his overt behaviour. Such removal from restraints may result from separation from family, friends, and familiar peer groups, from affiliation with new peer groups, or from changes in the system of values within the larger culture. Apparent increases in the use of dependence-producing drugs have been reported in such circum-stances.' In countries with a long history of cannabis use, extremely poor rural workers are often able to fit moderate use of cannabis into their routine of living, with little tendency to increase the frequency or amount; when they migrate to city slums, however, increased and undisci-plined patterns of use often develop.2
Poverty has been reported as being associated with cannabis use, but recent patterns of use have clearly not been confined to the poorer sections of the community.
Various degrees of social alienation have been noted in connexion with some use of cannabis (Blum & Associates, 1969b).
Cannabis use is also associated with prior use by the father or other members of the family, 3 and early initiation has been found to be positively correlated with long and heavy use by family members (Stringaris, 1933). Similar data have been reported for alcoholism.4
Sociocultural acceptance or rejection of particular behaviour is also an important epidemiological factor in drug use. As noted in section 3.1, alcohol consumption in a population tends to follow a unimodal frequency distribution. In addition, the proportion of the total population that consumes some amount of alcohol tends to be higher in cultures where social drinking is widely accepted than where it is less acceptable. Where drinking is widely accepted, too, the proportion of the total population that regularly consumes amounts above a given level tends to be larger than where it is less accepted (Ledermann, 1956; de Lint & Schmidt, 1968). It also follows logically that the proportion of the total population consti-tuting a health problem because of heavy consumption will be greater in " wide-use " areas. If this were true for cannabis — the few studies carried out tend to suggest that it may be (Popham, unpublished data) — the implications for the total number of cannabis-dependent persons one might expect to find are rather obvious (Popham, 1970).
In summary, the epidemiology of cannabis use involves three factors : (a) the personal characteristics of the actual or potential user, (b) the socio-cultural pressures on him, and (c) the pharmacological properties of various cannabis preparations. The extent to which its use satisfies conscious (stated or unstated) or unconscious needs will help to determine whether or not the behaviour is sustained. The use of cannabis tends to " bind " the user to certain persons, while often " alienating " others.
1 See section 2.2 for broad trends.
2 See section 4.
3 See section 3.3.
4 See section 3.4.
5 The psychoactive components of cannabis are insoluble in water, and are there-fore ineffective by the intravenous route. Furthermore, mixtures prepared from various preparations of cannabis contain macroscopic and microscopic particles and soluble pyrogens. A few attempts to inject suspensions of hashish or marihuana have been followed by severe physical symptoms (Gary & KeyIon, 1970; Henderson &Pugsley, 1968; King & Cowen, 1969).
1 Bouquet, 1951; Chopra & Chopra, 1957; Indian Hemp Drugs Commission,1894.
2 Bromberg, 1934; Mayor's Committee on Marihuana, 1944; McGlothlin et al., 1970; United States, Select Committee on Crime, 1970.
3 Chopra & Chopra, 1939; Roland & Teste, 1958; Soueif, 1967.
4 Chopra, 1935; Chopra, 1940; Indian Hemp Drugs Commission, 1894.
5 Not all taken at once, and perhaps not in a single drug-taking session.
6 Ledermann, 1956; de Lint & Schmidt, 1968; Smart et al., 1970b.
7 See section 2.1.1.
1 For references, see table.
2 A California Legislature, 1970; Canada, Commission of Inquiry, 1970; Chopra & Chopra, 1939; Goode, 1969; Koppiicar, 1948; Soueif, 1967.
1 Canada, Commission of Inquiry, 1970; Chopra & Chopra, 1957; McGlothlin et al., 1970; Roland & Teste, 1958; Tart, 1970.
2 See section 4.2.
3 Chopra & Chopra, 1957; Goode, 1969; McGlothlin et al., 1970; Tart, 1970.
4 Ames, 1958; Chopra, 1940; Indian Hemp Drugs Commission, 1894.
5 Ames, 1958; Asuni, 1964; Watt, 1961.
1 See section 3.4.
2 Manheimer et al., 1969; Soueif, 1967; Watt, 1961.
3 Robins et al., 1970; Sigg, 1963; Soueif, 1967; Watt, 1961.
4 Charen & Perelman, 1946; Freedman & Rockmore, 1946; Gaskill, 1945; Marko-vitz & Myers, 1944.
1 Mauer & Vogel, 1962; Mayor's Committee on Marihuana, 1944; Roland & Teste, 1958; Soueif, 1967.
2 Chopra & Chopra, 1939; Roland & Teste, 1958; Smart & Jackson, 1969.
1 Asuni, 1964; Chopra & Chopra, 1957; Lambo, 1965; Parreiras, 1949; Porot, 1942; Roland & Teste, 1958; Stringaris, 1933; Tanner, 1966.
2 Chopra & Chopra, 1957; Indian Hemp Drugs Commission, 1894; Roland & Teste, 1958.
3 Blum & Associates, 1969b; Chopra & Chopra, 1939; Smart et al., 1970a; Soueif, 1967.
4 Jellinek, 1945; McCord & McCord, 1962; Robins et al., 1968.
| < Prev | Next > |
|---|