| 59.5% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 137 |
| Yesterday: | 251 |
| This Week: | 137 |
| Last Week: | 2221 |
| This Month: | 4725 |
| Last Month: | 6796 |
| Total: | 129324 |
Section 5: Vein and other local damage
Drug Abuse
Section 5: Vein and other local damage
Vein blockage and collapse
Deep vein thrombosis (DVT)
Long-term consequences of vein collapse
Factors affecting healing
Key points
|
This section looks at damage to veins and infections of injecting sites. Vein blockage is discussed, as are the consequences of poor circulation such as ulcer formation. Evidence suggests that most injectors experience at least some of these complications and tend not to access appropriate treatment for them unless or until they have reached crisis point. This is likely to result in greater levels of permanent damage and the client requiring much more intensive and expensive treatment.98 It would be desirable to have staff with nursing and medical expertise available within all syringe exchanges. However, in reality this is not possible for many services. Some drug services have few, if any staff with a medical or nursing background. |
Figure 5.1: Collapsing and collapsed vein 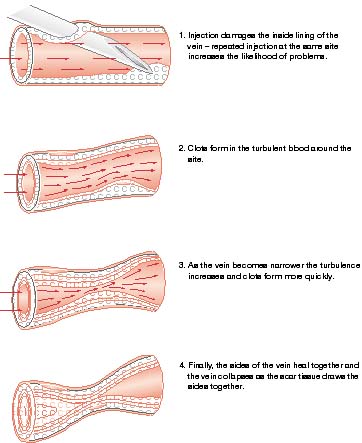
Adapted from The Safer Injecting Handbook, Andrew Preston and Jon Derricott, 1998, ISDD |
Veins may become temporarily blocked if the internal lining of the vein swells in response to repeated injury or irritation. This may be caused by the needle, the substance injected, or both. Once the swelling subsides the circulation will often become re-established. Permanent vein collapse (see Figure 5.1); occurs as a consequence of:
Smaller veins may collapse as a consequence of too much suction being used when pulling back against the plunger of the syringe to check that the needle is in the vein. This will pull the sides of the vein together and, especially if they are inflamed, they may stick together causing the vein to block. Removing the needle too quickly after injecting can have a similar effect. Thrombosis If the smooth blood flow through the vein is disrupted, clots can form on the lining of the vein. This process is called thrombosis. Over time, continuing to inject and the clots themselves will encourage further clotting. Eventually the vein can become completely blocked by the clot. Wherever blood clots in a vein (or elsewhere) it will eventually be transformed into scar tissue. Scar tissue forms to pull the edges of a wound together when it occurs on the inside of a vein the contraction leads to narrowing and blockage of the vein. Following this process the vein appears to collapse (Figure 5.1). A vein that is filled with scar tissue seldom recovers its ability to carry blood. Collateral circulation When a vein becomes thrombosed or obstructed, blood can no longer flow through it to return to the heart. The blood will therefore take an alternative route, using other smaller blood vessels to get around the blockage. This diversionary circulatory route is called 'collateral circulation'. This process may result in the appearance of 'new' superficial veins on or near the skin surface. Injectors should be discouraged from attempting to use these veins, as they are likely to be small veins that have become engorged by the necessity for them to carry more blood. They will therefore be under greater pressure than normal, so that injecting into them carries a greater risk of damage to the vein. The usual consequence of injecting into such veins is that within a few injections the vein becomes damaged and is no longer viable. If the collateral circulation becomes damaged, then the return of venous blood from the affected limb is likely to be even more severely restricted. |
|
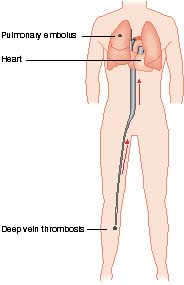
A DVT is a clot which completely or partially blocks a deep vein. Initially the clot consists of dense layers of platelets and fibrin; later it becomes a jelly-like mass of fibrin and red cells which may detach to form an embolus. This may result in a pulmonary embolism (see page 90). The most common site for a DVT is in the lower limbs, usually in the deep veins at the back of the calf (Figure 5.2). More rarely, it can also occur in the arms. The range of symptoms that can be produced by a DVT is wide, from no obvious ones at all to tissue breakdown and ulcer formation. Symptoms of the presence of a DVT can include:
A DVT which is not treated can, over time, cause a condition called post-phlebitic syndrome. The blockage of the vein and the destruction of valves leads to raised pressure in the remaining veins which may lead to:
A number of factors can increase the risk of a DVT. These include:
Treatment of a DVT If you suspect that a client has a DVT, they should be referred for urgent medical advice. Immediate treatment may include:
|
Figure 5.2: Position of a DVT and route to pulmonary embolus
|
|
For up to three months following discharge, warfarin treatment (an oral alternative to heparin) may be prescribed and closely monitored to prevent recurrence. Injecting should be discourged if anticoagulant treatment is taking place, as the likelihood of direct complications related to slower blood clotting is raised. Avoidance of a DVT For those who are at risk of a DVT, or have already experienced it, the possibility of further problems may be reduced if they are encouraged to:
|
|
When the flow of blood through the limbs has been severly affected, there are a number of problems that can arise. These include:
They are now discussed in detail.
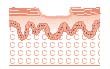
Figure 5.3: Cross-section of an ulcer Severely reduced flow of blood through the tissues leaves them vulnerable to infection and with a reduced healing capacity. The result of this process can be that painful areas of broken skin known as ulcers often form (Figure 5.3) following progressive damage to the veins from repeated and inexpert injecting. Once localised damage has occurred, the impaired venous return in the area, coupled with the fact that blood flow in the lower legs is slow, combines to make prompt healing of an injury less likely than it otherwise would be. This can then be compounded by infection. Ulcers can form either as the direct result of an injecting injury, or as a result of accidental injury after the veins have been damaged by injecting. Factors which may affect healing of injecting injuries include:
Treatment of ulcers Unless a project is specifically set up to provide primary health care to clients, the client should be referred to either their general practitioner or an A&E department for assessment and treatment. Ulcers take many months to heal and may require frequent attendance for treatment. There are strong arguments for advocating that these and other health care needs will best be met within drug treatment and needle exchange services, because:
Local infections As well as risks of systemic infections such as hepatitis and HIV, injecting carries the risk of introducing bacterial and fungal infections to the tissue surrounding the injection site. Often local infections are caused by bacteria which live harmlessly on the skin being picked up by the needle and forced below the skin where they multiply. The risks of local infection will be increased by:
Providing injectors with an understanding of the ways in which infection may be introduced is crucial. Ideally, they should be aware of the risks they may be exposed to and how to reduce them. Beneficial actions which can be taken by injectors range from the simple but effective, such as hand washing prior to injecting99 (where adequate facilities are available), to an elaborate aseptic ('germ free') injecting technique. Local infections include:
These are now discussed in detail. Abscess An infected abscess is a localised collection of pus that is encapsulated within inflamed tissue (Figure 5.4). It can be caused by a wide range of bacterial and fungal infections. An abscess is different from cellulitis in that it has a defined edge and shape. Figure 5.4: Abscess An abscess is characterised by:
People with abscesses should be referred for medical advice and treatment. The abscess will require antibiotic treatment and/or lancing to release the pus. Injectors should be told never to try to lance or puncture abscesses themselves. This can spread infection and without appropriate antibiotic cover they can quickly develop septicaemia (blood poisoning). They should be encouraged to alternate injecting sites as this will lessen the risk of localised inflammation, infection and abscess formation. Phlebitis is irritation of the smooth inner lining of a vein (tunica intima). The roughening of the vein lining can encourage the formation of clots. The vein is reddened or inflamed and can sometimes be felt as a thick cord beneath the skin. Phlebitis can occur as a result of:
An important complication of phlebitis is deep vein thrombosis leading to pulmonary embolism. If phlebitis is suspected the person should be referred for immediate medical advice. Treatment includes resting and raising the affected limb, antibiotics and anti-inflammatory drugs. Cellulitis Cellulitis refers to a painful spreading inflammation of the skin, which appears red and swollen with fluid (this is known as oedema). Cellulitis can occur as a result of:
It is usually the result of a 'missed hit' and/or poor circulation. Where cellulitis is suspected the client should be referred for immediate medical advice. Treatment includes resting and raising the affected limb, and treatment with antibiotics and anti-inflammatory drugs. Advice for people who have had cellulitis would include the following measures to prevent reinfection:
|

|
Figure 5.5: 'Missed hits' 'Missed hit' is a phrase used to describe swelling which appears around an injection site during or immediately after injection. It may be caused by fluid entering the tissue surrounding the vein because the needle has:
These problems can be prevented by encouraging injectors to:
A missed hit will mean that the drug is absorbed much more slowly by the body, so that the effect will be less pronounced. It can also lead to other problems discussed in this section such as:
|

|
Injectors often have various 'lumps and bumps' on their skin. These have differing causes. Blocked veins can leave hard 'knots' under the surface of the skin. Developing abscesses may first appear as a raised bump, although this is often accompanied by localised tenderness and heat. Other possible causes of 'lumps and bumps' are detailed here. A sterile abscess occurs as a result of injecting irritant substances such as crushed tablets and possibly as a consequence of a missed hit. It will often disperse without treatment but, over time, a granuloma may form around it. Cutaneous foreign body granulomas Granulomas are benign growths of scar tissue that are associated primarily with subcutaneous injecting or 'missed hits', where the solution has by accident or design ended up in the surrounding tissue. In such cases a residue may stay for many years, eventually leading to granuloma formation100. Many of the common cutting agents for injectable drugs, such as quinine, mannitol, dextrose and lactose, are not thought to cause foreign body granulomas. However the injection of crushed tablets will increase the risk. The principle filler of the tablet is often hydrogenous magnesium silicate, frequently referred to as 'chalk' by users. It should be noted that 'successful' intravenous injection of crushed tablets does not remove the risk of granuloma formation. It simply changes the place that they may be found, to the lungs. In Australia, attempts have been made to supply tablet injectors with commercially produced filters (Millipore filters) which are intended to remove the chalk from the solution. If beneficial and practical (they are relatively expensive), then this may be a rare example of a successful harm reduction strategy for those injecting tablets. However, there is the potentially much greater problem of transmission of blood-borne viruses if these filters are reused or shared. Because of this, the best harm reduction intervention is likely to remain clear advice not to inject crushed tablets.
Gangrene is the death of body tissues caused by impaired or absent blood supply. Gangrene can occur as a result of arterial or serious venous damage. The effect of gangrene can be disastrous, leading to loss of limbs. It can also cause the products of tissue breakdown to enter the bloodstream causing blood poisoning and threatening life. Arterial damage Gangrene as a result of arterial damage occurs when an artery is injected into instead of a vein. Often this is as a result of injecting irritant drugs such as Temazepam into the femoral artery rather than the femoral vein. However, it can occur when people inject into the smaller arteries in the arm. Gangrene as a result of injecting into an artery can occur in the following ways:
Venous damage Gangrene following venous damage may be slower to develop, and results when damage to the veins is such that the return of venous blood from the affected limb is no longer adequate; blood gets into the tissues at a faster rate than it can get out. In the end the reduced flow of blood through the tissues is inadequate to sustain them and they die. Signs and symptoms Signs and symptoms of gangrene include:
Prevention and treatment Injecting drug users need to be given advice on the following subjects to enable them to prevent gangrene occurring:
In the event of symptoms of gangrene occurring injectors must be aware that:
|
![]() Irritation and infection can cause veins to block temporarily.
Irritation and infection can cause veins to block temporarily.
![]() Vein collapse occurs as a consequence of long-term injecting. Repeated injections, especially with blunt needles, poor technique and of substances which irritate the veins, encourage vein collapse.
Vein collapse occurs as a consequence of long-term injecting. Repeated injections, especially with blunt needles, poor technique and of substances which irritate the veins, encourage vein collapse.
![]() Permanent vein blockage results from the formation of scar tissue in the vein, following blood clotting.
Permanent vein blockage results from the formation of scar tissue in the vein, following blood clotting.
![]() Severely reduced flow of blood through the tissues leave them vulnerable to infection and with reduced healing capacity.
Severely reduced flow of blood through the tissues leave them vulnerable to infection and with reduced healing capacity.
![]() All drug injectors should be warned that they should never inject into a blood vessel in which they can feel a pulse.
All drug injectors should be warned that they should never inject into a blood vessel in which they can feel a pulse.
![]() Injecting in the hands and fingers should be discouraged those who insist on these sites should be warned to remove rings prior to injecting.
Injecting in the hands and fingers should be discouraged those who insist on these sites should be warned to remove rings prior to injecting.
![]() Injectors should be warned of the symptoms of gangrene and advised to seek urgent medical advice if they suspect that it may be occurring.
Injectors should be warned of the symptoms of gangrene and advised to seek urgent medical advice if they suspect that it may be occurring.
![]() If in any doubt, get medical advice immediately.
If in any doubt, get medical advice immediately.
Last Updated (Wednesday, 05 January 2011 23:39)