| Long-term
consequences of vein collapse When the flow of blood through the limbs has
been severly affected, there are a number of problems that can arise. These include:
![bult57[1].gif (589 bytes)](../../../library/books/needle/bullet/bult57[1].gif) Ulcers Ulcers
Gangrene
Local infection.
They are now discussed in detail.
Ulcers
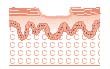
Figure 5.3: Cross-section of an ulcer
Severely reduced flow of blood through the tissues leaves them vulnerable to infection
and with a reduced healing capacity.
The result of this process can be that painful areas of broken skin known as ulcers
often form (Figure 5.3) following progressive damage to the veins from repeated and
inexpert injecting.
Once localised damage has occurred, the impaired venous return in the area, coupled
with the fact that blood flow in the lower legs is slow, combines to make prompt healing
of an injury less likely than it otherwise would be. This can then be compounded by
infection.
Ulcers can form either as the direct result of an injecting injury, or as a result of
accidental injury after the veins have been damaged by injecting.
Factors affecting healing
Factors which may affect healing of injecting injuries include:
Diet and nutrition
Stress
Poor accommodation
Drug and alcohol use.
Treatment of ulcers
Unless a project is specifically set up to provide primary health care to clients, the
client should be referred to either their general practitioner or an A&E department
for assessment and treatment.
Ulcers take many months to heal and may require frequent attendance for treatment.
There are strong arguments for advocating that these and other health care needs will
best be met within drug treatment and needle exchange services, because:
Users of drug
treatment agencies may not attend if referred to other agencies
Drug users may tend to
believe health problems are to be expected and therefore do little about them
They are less likely
to receive discriminatory treatment.
Local infections
As well as risks of systemic infections such as hepatitis and HIV, injecting carries
the risk of introducing bacterial and fungal infections to the tissue surrounding the
injection site. Often local infections are caused by bacteria which live harmlessly on the
skin being picked up by the needle and forced below the skin where they multiply.
The risks of local infection will be increased by:
Sharing of needles and
syringes
Reuse of unsterile
equipment
Sharing of
paraphernalia
The use of
contaminated equipment in the sharing of drugs
The use of
non-pharmaceutical medication
Unhygienic preparation
of drugs
Poor personal hygiene.
Providing injectors with an understanding of the ways in which infection may be
introduced is crucial. Ideally, they should be aware of the risks they may be exposed to
and how to reduce them.
Beneficial actions which can be taken by injectors range from the simple but effective,
such as hand washing prior to injecting99 (where adequate facilities are
available), to an elaborate aseptic ('germ free') injecting technique. Local infections
include:
Abscesses
Ulcers
Cellulitis.
These are now discussed in detail.
Abscess
An infected abscess is a localised collection of pus that is encapsulated within
inflamed tissue (Figure 5.4). It can be caused by a wide range of bacterial and fungal
infections.
An abscess is different from cellulitis in that it has a defined edge and shape.
Figure 5.4: Abscess

An abscess is characterised by:
Raised skin surface
Localised heat
Tenderness and pain
Redness of the skin
(in white people)
Pus formation
A foul smell if it has
begun to discharge.
People with abscesses should be referred for medical advice and treatment. The abscess
will require antibiotic treatment and/or lancing to release the pus.
Injectors should be told never to try to lance or puncture abscesses themselves. This
can spread infection and without appropriate antibiotic cover they can quickly develop
septicaemia (blood poisoning). They should be encouraged to alternate injecting sites as
this will lessen the risk of localised inflammation, infection and abscess formation.
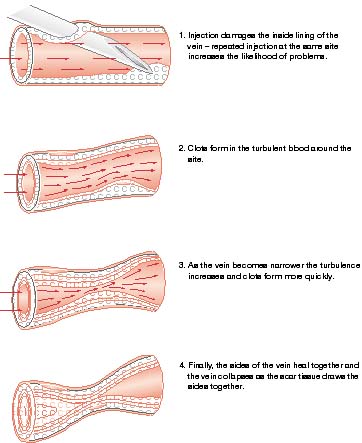
Phlebitis
Phlebitis is irritation of the smooth inner lining of a vein (tunica intima). The
roughening of the vein lining can encourage the formation of clots. The vein is reddened
or inflamed and can sometimes be felt as a thick cord beneath the skin.
Phlebitis can occur as a result of:
Injecting irritant
substances such as Temazepam
Poor injecting
technique
Infection
Accidental injury
(i.e. knocks or blows).
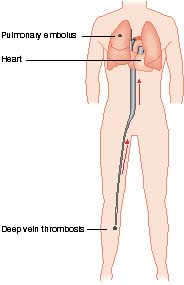
An important complication of phlebitis is deep vein thrombosis leading to pulmonary
embolism.
If phlebitis is suspected the person should be referred for immediate medical advice.
Treatment includes resting and raising the affected limb, antibiotics and
anti-inflammatory drugs.
Cellulitis
Cellulitis refers to a painful spreading inflammation of the skin, which appears red
and swollen with fluid (this is known as oedema).
Cellulitis can occur as a result of:
Irritant substances
lodged in body tissues
Infection.
It is usually the result of a 'missed hit' and/or poor circulation.
Where cellulitis is suspected the client should be referred for immediate medical
advice. Treatment includes resting and raising the affected limb, and treatment with
antibiotics and anti-inflammatory drugs.
Advice for people who have had cellulitis would include the following measures to
prevent reinfection:
Using sterile
injecting equipment
Using sterile water
where available and discussing alternatives where it is not
Avoiding the injection
of irritant or heavily adulterated drugs
Removing rings prior
to injecting if injecting in the hands. |