| 59.5% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 137 |
| Yesterday: | 251 |
| This Week: | 137 |
| Last Week: | 2221 |
| This Month: | 4725 |
| Last Month: | 6796 |
| Total: | 129324 |
Section 3: Viral transmission, drugs and their preparation
Drug Abuse
Section 3: Viral transmission, drugs and their preparation
Transmission of blood borne viruses
Injecting paraphernalia
Preparing different drugs for injection
Using injecting equipment to share drugs
Substance-specific risks
Other injected drugs
Cutting agents
Key points
|
The preparation and sharing of drugs have tended to be overlooked as potential points of transmission for blood-borne disease. The singular focus on needles and syringes in the messages given to drug injectors, although valuable in shaping behaviour, has also encouraged the erroneous belief amongst users that, as long as needles and syringes are not directly shared, then they are safe. The risks posed to injecting drug users from hepatitis infection are such that all workers they come into contact with need to feel confident about discussing the detail of the injecting process, to enable clients to make changes to protect themselves. There is also a need for an understanding of the ease by which any of the equipment involved in the preparation of an injection (including lighters, knives, etc.) may transmit hepatitis C. Simple changes to the practice of preparation, such as using a personal area and washing hands before and after injecting, will significantly lower the risk of bacterial and viral infection. This section describes the injecting process and the equipment used in detail. The potential infection and other risks involved at each stage are examined. It also addresses the risks that are specific to particular substances.
Blood-borne viruses are transmitted when blood cells from an infected individual are passed into the bloodstream of another person. The infective dose for hepatitis B may be 0.00004mL of blood59, i.e. less than one five hundredth of a drop of blood. Hepatitis and HIV can potentially be passed on by any equipment which has been in contact with an infected person's blood. The understanding that many things in addition to syringes and needles may be involved in the transmission of blood-borne viruses has increased since the late 1980s. Ethnographic research into injecting behaviour has developed understanding of the potential for transmission of blood-borne viruses. It has brought to light previously unrecognised risk practices in the injecting process which may facilitate transmission of infections, that have a social element which involves the sharing of drugs rather than just the sharing of injecting equipment. The range of behaviours that may be employed for the sharing of drugs, including frontloading and backloading (which are discussed on page 48), is so wide as to preclude any simple messages for avoiding risk. Rather than long lists of things they should or should not do, drug injectors need information on how cross infection may occur, so that they can work out risks and ways of minimising them for themselves. In 1997 Timothy Moore summed this up saying: "Simplistic health messages are inappropriate for the complexity of hepatitis C. Messages such as 'Just say no to sharing' do not provide enough information to provide guarantees of safe practices. Injecting drug users need to be provided with sufficient information, opportunity and equipment to carry out aseptic injecting technique at each injecting event... The fact that drug use and the learning of ritual and practice occurs in cultural and social contexts provides an avenue for public health measures to be incorporated into the behaviour of drug users."60 For these more complex messages to be conveyed effectively a range of health information will need to be presented in a variety of culturally appropriate ways. In Australia, a key to getting complex information into injecting networks has been to help facilitate and support drug user forums and support systems. In contrast, UK drug user organisations have tended to receive little support from drug services or drug service purchasers. Factors associated with continued sharing of syringes and needles Although the sharing of syringes and needles has been substantially reduced as a result of increased knowledge amongst injectors about the transmission risks of HIV, Power61 suggests several reasons why it may continue to occur:
And most commonly:
Drug workers need to raise these issues with injectors and help them identify where and when sharing may occur, and develop strategies for avoiding such situations. |
|
Apart from syringes and needles, other paraphernalia associated with injecting includes:
All these paraphernalia are associated with the transmission of blood-borne viruses, most notably hepatitis B and C, although HIV transmission is a possibility. The risk of infection from separate injecting events is likely to be low, but repeated exposure to low-risk events may result in infection. Drug workers need to discuss all types of paraphernalia and the enviroment in which they are used, with injectors. Many are dealt with in detail in the following pages. Spoons Spoons are often used as a receptacle in which to mix drugs prior to injection. Contact of the spoon with another person's needle which has been previously used (e.g. when drawing up communally), may be enough to transmit some infections, such as hepatitis C. Injectors should be encouraged to mark their spoons for easier identification and keep them for sole personal use in a place to which other injectors do not have access. Spoons should be cleaned with bleach and rinsed thoroughly before use. Similar precautions should be taken with other receptacles used for drug preparation, such as the bases of soft drink cans. Lending and borrowing of spoons amongst injectors appears to be a common behaviour, at least amongst those attending needle exchange schemes in the North West of England.55 Ensuring that drug users are educated about the risks of this behaviour is one of the key tasks for needle and syringe exchanges for the future. Water Sterile water for injection is the ideal option where it is available. This should be for personal use only and discarded afterwards. Once opened it should not be kept for subsequent injection, as it will contain bacteria from the air, and may have been used by another person. Many UK projects do not give out sterile water because of legal restrictions (see page 108) and budget constraints. Water that has been boiled for five minutes and allowed to cool in a covered pan is sterile. It must be reserved for personal use and discarded after a single injecting session. Water that has been boiled in a kettle and allowed to cool is unlikely to contain any living bacteria and, given that nearly all the components of the injecting process (other than a new needle and syringe) are not sterile, it is usually 'clean enough'. Water drawn straight from the tap is better than bottled water, distilled water or 'pure bottled water' which may have been exposed to bacteria in the air and kept warm for some time, and are therefore likely to contain far more organisms. Drawing up from a communal pot of water represents a risk behaviour for the transmission of hepatitis and HIV if another person's used needle and syringe come into contact with the water source. Very small amounts of blood which will not be visible to the naked eye can transmit infection. Filters Filters are used by injecting drug users to minimise the risks associated with injecting undissolved particles which may be contained in the drug solution. Ways in which filters can be associated with harm include:
In important research examining a previously neglected area, Scott et al.62 explored how effective different types of filter were at removing particulate matter from the solution when preparing different drugs. As Scott et al. comment: "In the microcirculation of the body, the smallest vessels are the capillaries, which are approximately 8 microns in diameter. Next are the terminal arterioles which are between 20 and 50 microns. The more particles there are (in a solution for injection) and the bigger they are, the greater the risk to health."62 Their initial work has concentrated on the effects of filters on tablets and street heroin prepared for injection. The results are not directly applicable to the street, because wide variations in preparation practice occur, which will result in differing amounts of particles in the solution prior to filtering and therefore after filtering as well. However there are some broad indications from this work which are useful. They tested a variety of filters cigarette filters, Rizla, cotton buds and a commercial syringe filter called an Acrodisk. These filters were tested on drug solutions prepared from Physeptone (methadone) 5 mg tablets, Diconal, Temgesic and street heroin. Although all filters reduced the number of particles in the solutions, the Physeptone tablets formed a slurry at the bottom of the syringe, causing loss of 10% of the active drug and also representing a risk if injected. Scott et al. found that none of the filters was effective with the Physeptone solution: "The Physeptone solutions were thick and did not pass through the filters quickly or easily. Several filters had to be used as they clogged and it took longer than was deemed acceptable to the IDU."62 All other injections were able to be filtered. The most effective filter was perhaps, unsurprisingly, the commercially produced Acrodisk. Of the makeshift filters, the most effective was the Rizla, for both the tablets and the street heroin. An important point was the necessity of handling the filter as little as possible prior to use, to minimise the potential for contamination with bacteria.63 There are several different types of commercial syringe filters on the market. Some of these are designed to filter out the bacteria which can cause skin infections and abscesses. Although these filters may prove to be valuable, they should be viewed and employed with caution as they may:
Acidifiers are used to enable brown heroin which is manufactured principally for smoking to be more easily dissolved into a solution for injecting. They do not need to be used with the more refined hydrochloride form of heroin (as it is highly soluble in water) or in the preparation of other drugs such as cocaine (except in the form of crack) or amphetamine for injection. Various acids such as lemon juice and vinegar are used for heroin preparation. Any substance already in liquid form may contain bacteria or become contaminated with hepatitis or HIV viruses. Lemon juice, whether fresh or bottled, has been associated with thrush and other fungal infections within the body, which have been reported to cause loss of vision and blindness due to retinal damage (candidal endophthalmitis)64,65. It has also been associated with endocarditis and other conditions.Ascorbic acid (vitamin C) or citric acid are thought to be the safest options. These can cause irritation to veins and tissues, so the smallest amount possible should be used. The more acid the solution, the more irritant it will be. Ascorbic acid is probably less caustic than citric acid and may therefore cause less irritation. Injectors may find difficulty in obtaining ascorbic or citric acid from pharmacists as their supply is illegal under Section 9a of The Misuse of Drugs Act 1971 if they know or suspect the person requires them for injecting (see page 108). |
|
The environment in which injecting takes place can be a factor in the transmission of blood-borne viruses. The risks associated with injecting will be reduced if there is adequate:
For homeless injectors, few if any of these may be available. For these injectors at least, there is an argument for the provision of safer injecting rooms. Injecting with another person present lowers the risks of an undetected overdose, but will increase the risk of viral transmission if any equipment is shared. Surfaces If a surface used to prepare injections is contaminated with blood or with water from flushing out syringes, there is a risk of transmission of infection. Ideally surfaces should be cleaned with bleach before injecting. A more practical approach for many injectors would be to prepare an injection on something disposable such as a newspaper or magazine. This will also serve to mark out a 'personal area' for injecting. Tourniquets Tourniquets should only be used if they are really needed. Many injectors, at least early in their injecting careers, will be able to access superficial veins without using tourniquets. If left in place for too long they can cause a limb to be deprived of its blood supply and eventually, cause gangrene. If a tourniquet is not loosened prior to injection, excess pressure has to be used to get the solution into the vein which can lead to leakage of the drug into the tissues or to rupture of the vein. If an injector is frequently complaining of 'missed hits' (see page 79), check that they are releasing the tourniquet before injecting. If tourniquets are contaminated with blood and subsequently shared, they represent a hepatitis C transmission risk. Raising veins without using tourniquets Various techniques can be used to help superficial veins become more accessible, including:
When working with people who inject depressants (usually opiates) it is important to point out the dangers of injecting in a bath a period of unconsciousness could easily result in drowning. |
|
Heroin Heroin bought on the street in the UK usually comes as a brown powder of varying purity. It is mixed with water in a suitable receptacle, usually a spoon. An acidifying agent is then added. The solution is heated to help the heroin dissolve, allowed to cool and then drawn into a syringe, usually through a filter to attempt to remove any insoluble particles. The following field note from Jean-Paul Grund's research illustrates a typical heroin injecting process: "The man starts to prepare a shot. He puts his spoon on the table and throws in a knife tip of heroin. He adds some lemon juice and with his syringe he gets some water which he carefully squirts in the spoon, around the heroin powder just under the edge of the spoon. He heats the spoon and when the stuff has dissolved he stirs and draws the solution into the syringe through a piece of cotton. After checking the syringe for air bubbles, he puts his syringe on the table. Then he takes his belt and puts it around his left arm. Making a fist he pumps up his veins. He looks carefully at his arm and then sticks in the needle. When he pulls the piston back, blood immediately runs into the syringe, then he pushes the piston about halfway. Then he draws up some blood and pushes the mixture into his vein. He moves the syringe a little, draws plus or minus 1.5cc blood and pushes it in again. All the time his hand is a fist. Then he unties the belt, pulls the needle out, puts it down and waits about two minutes, concentrating on the rush."66 The subject in the above process has exposed himself to additional risks by using lemon juice to acidify the solution and by not releasing his tourniquet until after he has injected (indeed until after he has flushed his works through with blood). Not releasing the tourniquet raises the pressure in the vein whilst injecting and will significantly increase the likelihood of vein damage and of the drug flowing out of the vein into surrounding tissue the consequent 'bump' often being called a 'miss'. Amphetamine Amphetamine sulphate powder does not need to be heated or acidified in order to dissolve it for injection. The preparation process is otherwise similar to that of heroin for injection, although it may also be mixed in the syringe.
The preparation of cocaine hydrochloride for injection is similar to that of amphetamine, although some cocaine injectors may mix the solution in the syringe. An acidifier is needed to prepare crack cocaine for injection. |
|
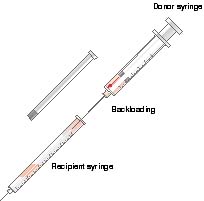
The sharing of drugs is also associated with cross infection risk. The following are the main sources of risk. Frontloading and backloading Frontloading and backloading are terms that describe methods of sharing drug solutions using the syringe as a measuring device. It should be noted that frontloading and backloading are sociological terms coined by the researcher who first observed and recorded the practice.66 It may be necessary for workers to describe the processes, rather than use terms which may be unfamiliar to injectors who are nevertheless engaging in the process. Terms used by users themselves include dividing, splitting, halfing and slurping.67 Neither frontloading nor backloading increase the risks of transmission of blood-borne viruses if all the equipment involved is sterile and previously unused. However it is difficult for drug injectors to be certain that this is the case, in what can be a busy and confused environment. For this reason education around this issue would aim to discourage these practices. Frontloading Frontloading is the practice of drawing up a drug solution into a 'donor' syringe, and then measuring out appropriate amounts into one or more other syringes (Figure 3.1). It is termed 'frontloading', because the solution is squirted through the hub or front of the syringe. Frontloading is done with syringes which have detachable needles: the donor syringe has a needle attached, the 'recipient' syringes do not. Figure 3.1 Donor syringe Recipient syringe Frontloading
Backloading Backloading differs from frontloading in that it is done with insulin type syringes with fixed needles (Figure 3.2). The plunger is removed from the recipient syringe and the drug solution squirted in through the back opening. It requires considerably more dexterity than frontloading, as an air gap has to be allowed between the drug solution and the front of the syringe, to allow for the reintroduction of the plunger without pushing out the drug solution. Figure 3.2
Sharing from the spoon Sharing from the spoon simply involves drawing up directly from the spoon used for preparing the solution. Again, this should not increase the risks of virus transmission as long as new sterile equipment is used once only by all participants. If a previously used spoon, syringe or needle is employed, then everyone who subsequently draws up from the spoon is at risk of contracting whatever blood-borne viruses that equipment may be carrying. Others at risk include those who might reuse the filter. Because it is so easy for these risk events to occur, it is simpler and better if drug users have a rule for themselves that they will never share (lend or borrow) spoons or filters. |
|
There are a number of risks of injecting which are unique to particular substances and many that apply to some substances but not to others. These are important areas of safer injecting information to be given to users and are now discussed in detail. Heroin Drug-specific risks of injecting street heroin are surprisingly few and include:
The other risks such as transmission of viruses or bacteria are not confined to heroin injecting. Other bodily reactions to opiates such as pinpoint pupils and constipation are not dependent on injecting as the route of administration. The transmission of tetanus and botulism has been associated with the use of 'black tar' heroin in the USA. Oral methadone There is clear anecdotal evidence that some people in the UK inject oral methadone mixture 1mg/1mL, the psychoactive effect of which is likely to be minimal as even 10mg is a very small dose for an opiate user with tolerance to the drug; and 10mLs is a large amount of fluid to inject, especially as it is a thick, often sugary liquid. The usual thick green syrup formulation is likely to cause slowing of the blood and rapid vein collapse. This is an instance where, if harm reduction is the aim, there is little that can be done to make the practice safe. Workers should strongly discourage this practice. Attempts, such as those in Australia, to make the practice safer by providing specific equipment are misguided as they are unlikely to reduce drug-related harm. In some centres people are prescribed methadone, usually for supervised consumption, in a more concentrated 10mg/1mL form. Clearly if unsupervised this is more likely to be injected than 1mg/1mL. The formulation of oral methadone in Australia (5mg/1mL) is more concentrated than that usually available in the UK (1mg/1mL) and injectable preparations are not prescribed to drug users. Darke et al. observed in their study that injection of oral methadone was common and was associated with more likelihood of:
Methadone ampoules Approximately 10% of methadone prescriptions in the UK are for injectable methadone69, which has been little researched. The ampoules come in various strengths, the weakest of which is 10mg/ 1mL. The strongest 50mg/1mL is only manufactured on the instructions of some doctors for their patients. There have been reports of significant injection site 'burning' and other damage from the highly concentrated 50mg/1mL solution. As clients may be reluctant to show this damage to their prescribing doctor for fear of 'losing their script', workers should be alert to the problem. The only things that can be done to reduce such damage are for clients to rotate sites and/or ask their doctor for a less concentrated form, or to transfer to oral methadone either on a temporary or permanent basis. 'Homebake' 'Homebake' is a phenomenon that appears to be limited to Australia and New Zealand. It refers to the practice of using home chemistry to remove codeine from 'over the counter' and 'prescription only' drugs, and subsequently converting the codeine to morphine and then to heroin70 . It seems to have arisen as a response to a lack of heroin in Australia in the early 1980s, probably as a result of effective enforcement of drug supply restrictions. 'Homebake' also sells more cheaply than alternatives such as heroin, which has helped to maintain its presence in the Australian drug scene. The lack of consistency and precision inherent in a home-produced drug means that the strength is often uncertain and many of the agents or by-products of manufacture are left in the finished product. These agents, such as chloroform, pyridine, hydrochloric acid and acetic acid may cause significant damage.70 The use of homebake seems to be closely associated with localised injection related damage, such as skin rashes and abscesses. Perhaps the most worrying aspect of homebake use is that it has often been sold in ready loaded syringes. Obviously, since the sterility of the syringes cannot be guaranteed, this method of supply represents a considerable risk for transmission of blood-borne viruses. Kompot Kompot is found in many parts of Central and Eastern Europe. It is made by various methods which often involve boiling up poppy straw and distilling the residue until left with a dark brown liquid. It is very cheap to produce and buy, although it tends to be a seasonal product so the price rises substantially in the winter. The problems associated with the use of kompot are similar to those already described for homebake. It is often sold in or from pre-loaded syringes, which brings with it an increased risk of the spread of blood-borne viruses.
All stimulants have an effect of enhancing confidence and altering judgement about risk. In circumstances where people are injecting while intoxicated they may be less cautious about infection and other risks. Workers can address this issue with people when they are not intoxicated, by helping them to develop strategies for ensuring that they do not place themselves at risk when they are intoxicated. An important factor is the necessity to have sufficient injecting equipment for their needs: in some cases this may mean users taking large numbers of syringes away from the needle exchange. The use of considerable quantities of stimulants increases the likelihood of development of psychosis71. Amphetamine After preparation on a spoon, the solution is usually drawn through a filter. Any residue should be discarded or swallowed rather than injected. King et al. studied the constituents of UK street amphetamine in 1993 and found that the majority of amphetamine sulphate powder was of very low purity (on average about 5%). The bulk of the powder is probably made up of 'fillers' such as caffeine, dextrose and other sugars. By comparing police and customs seizures they found that: "...nearly all the amphetamine in the UK had been imported from The Netherlands."72 The low purity may lead those who use amphetamine in quantity to become more likely to inject it, in order to maximise the effect, and when they do, to inject large quantities. In an Australian study of amphetamine users, Hall et al. found that injecting of amphetamine was significantly related to the experience of hallucinations, violent behaviour and paranoia71. Amphetamine 'base' has become more widely available in the UK recently. This is usually of greater purity than amphetamine powder. It is an irritant to the veins when injected. Cocaine Cocaine injecting is associated with higher rates of HIV infection than other drugs73 and with significantly more localised tissue damage than heroin injecting. There may be several factors causing the tissue damage. Cocaine's duration of effect when injected is very short and can be measured in minutes rather than hours. This means that cocaine injecting is likely to be more frequent for those who use it as a primary drug. Also, cocaine has been employed for centuries for its anaesthetic properties. Deadening of pain at the injection site may lead the user to inadvertently cause more injury whilst injecting. Cocaine has a constricting effect on peripheral blood vessels and therefore the healing of injuries associated with cocaine injecting may be delayed74. It may also be toxic to local blood vessels75. Cocaine stimulates the cardiovascular system, raising the heart rate and blood pressure, so users are at an increased risk of circulatory problems such as strokes or heart attacks. There is also an increased risk of seizures for cocaine users. Drugs with local anaesthetic properties such as lidocaine may be used to adulterate cocaine76. Since cocaine injecting is likely to occur very frequently, this should be taken into account when issuing injecting equipment. Temazepam Temazepam comes in several forms:
In a 1992 study, Ruben et al.77 found that reasons given for using temazepam included:
Because of the particular formulation, Temazepam, when injected, can cause severe problems. It is highly irritant to the veins and when intoxicated, people can become very reckless in their behaviour. Temazepam injectors often quickly damage the peripheral veins in their arms and legs to the point that they are no longer usable. This may lead them to look for alternative deeper veins, often in the groin. Gelthix temazepam causes particular problems because it is warmed to make it liquefy. After injection it cools in the body and resolidifies, leading to vein blockage. Injecting temazepam into the femoral vein increases the likelihood of deep vein thrombosis in the legs. Other problems associated with injecting temazepam include:
Arterial injection of temazepam will often lead to amputation of the whole or part of a limb. The following experience of a vascular surgery unit is not unusual, or confined to Merseyside. "Of particular concern recently in the Merseyside area is the increasing prevalence of disastrous complications arising from the intra-arterial injection of soluble temazepam..."78 This report written in 1993 resulted from the admission of 11 injectors with complications from arterial injection of temazepam within a six-month period. More worryingly, this report noted that although six of the 11 had apparently injected into the femoral artery by mistake, five had apparently injected into the radial artery in the arm, because of mistaken instruction from their peers! In all of these five cases this resulted in varying degrees of gangrene in the fingers. Barbiturates Barbiturates are now rarely injected in the UK. This mirrors the decline in general prescribing of barbiturates. Their place in medicine began to be taken by benzodiazepines in the 1960s. Injecting injuries associated with barbiturates are similar to those found with benzodiazepines, except that there tends to be more local tissue damage when injected subcutaneously; tissue dies and sloughs off around the injecting site. Older textbooks refer to these injuries as 'barb burns'. Barbiturates are also associated with a high overdose risk, especially when used in combination with other drugs. Withdrawal from dependent use can cause seizures which can be fatal. Alcohol The injecting of alcohol seems to be something that occurs occasionally, either as an experiment or as a feature of chaotic, compulsive drug use. The substance injected is usually a spirit such as vodka. Alcohol injected intravenously is highly irritant to the veins and has little psychoactive effect, except in volumes that will cause great damage. |
Steroids
In the past steroid injecting was confined to sport particularly body building. However, now other groups, most notably young men, are using steroids to develop muscle for more cosmetic reasons.
Steroid injectors often perceive themselves as being 'different' to other injectors of illicit drugs. This may be true in that rather than using their drug of choice for any specific immediate psychoactive effect, they are injecting steroids as part of their pursuit of 'fitness'.
However, steroid injectors run the same risks of transmission of blood-borne viruses as any other injecting drug users who may share their equipment or paraphernalia. In fact the relative risk may be greater, as practices such as different people drawing up from 'multi-dose' vials may occur79.
The attraction of steroid injectors to generic agency needle and syringe exchange may be made more difficult because of an unwillingness to be associated with the stigma surrounding the injection of drugs such as heroin, cocaine and amphetamines.
Other risks associated with steroid injecting centre on overuse and the fact that there are many fake or mis-described 'steroids' available on the illicit market.
Although their use can incur cardiovascular and liver problems, the health risks of using steroids, such as liver cancers and psychological problems, tend to have been over emphasised. Perhaps this is an attempt to discourage their use. Also, research reports tend to concentrate on cases that have developed severe problems.80 The value of giving accurate, credible information is as important in this area of drug use as it is in any other.
Steroids are usually injected intramuscularly.
Cyclizine
Cyclizine is an antihistamine with an anti-emetic effect (i.e. intended to help prevent sickness). It is recommended for the treatment and prevention of motion sickness, post-operative vomiting and Menières disease.
Use of cyclizine in the UK by opiate users probably resulted from 'home psychopharmacology' experiments. Drug injectors were trying to recreate the effects of injecting Diconal, a tablet containing 30mg of cyclizine and 10mg of dipipanone.
Cyclizine is no longer available as an 'over the counter' item, as pharmacists are now not allowed to break down dispensary stock and repackage it for over the counter sale, and there is no commercially available 'over the counter' cyclizine pack81.
Cyclizine was previously a constituent of Marzine. The formulation of Marzine has been changed so that it includes a different
anti-emetic which does not produce the
same psychoactive effects, if injected, as cyclizine .
Drug users using cyclizine almost invariably inject it. Its use is closely associated with injecting injuries, which may be as a result of:
![]() Injecting crushed tablets
Injecting crushed tablets
![]() Poor technique
Poor technique
![]() Frequency of injecting.
Frequency of injecting.
There is a lack of research into the exact nature of the physical and psychoactive effects of cyclizine when used in conjunction with illicit drugs, but it does appear to enhance some of the effects of opiates and opioids82.
This enhancing effect appears to be particularly pronounced in the case of methadone and has been described as lasting between 30 minutes and six hours. Users reported various, mostly positive effects at the time of taking the drug, but all reported feelings of depression afterwards and most described cravings to use the drug again.82
It is not possible to offer advice that can reduce the risk of injecting cyclizine. Workers need to guide and support clients towards stopping, by helping them weigh up the pros and cons of continuing and giving them clear reasons as to why they should stop.83
Drug preparations containing cyclizine are:
![]() Cyclimorph injection (cyclizine and morphine)
Cyclimorph injection (cyclizine and morphine)
![]() Diconal tablets (cyclizine and dipipanone)
Diconal tablets (cyclizine and dipipanone)
![]() Migril tablets (an anti-migraine drug containing cyclizine, ergotamine and caffeine)
Migril tablets (an anti-migraine drug containing cyclizine, ergotamine and caffeine)
![]() Injectable cyclizine.
Injectable cyclizine.
Although widespread availability of the injectable form of cyclizine would not alter the problems of behaviour associated with its use if taken by opiate users, it has been suggested that it could eliminate much of the physical damage associated with the injection of crushed tablets. This is a complex ethical dilemma for clinicians. However, it would be very difficult to be certain that you were complying with the first principle of medicine to do no harm in prescribing injectable cyclizine.
It is commonly believed that drugs are often bulked out with substances which may be very injurious to health, such as brick dust, scouring powder, rat poison, etc. Whilst it is not possible to assert that this has never happened, it is certainly a widely propagated myth that it takes place on a widespread and regular basis84.
Where harmful adulteration does occur it is likely to be as a result of accident rather than design.
Perhaps the origins of this belief are bound up in attempts to dissuade people from beginning injecting, whilst at the same time furthering familiar stereotypes of disgust for injectors and injecting behaviour.
It does not appear to make economic sense for a drug dealer to bulk out the product with dangerous substances which would endanger the lives of customers. Where cutting does occur, it tends to be with substances which are (or at least are intended to be) inert.
Coomber, in a survey of drug dealers undertaken via the internet, found that almost none of them indulged in bulking out of drugs by cutting them with other substances, cutting usually having taken place further up the supply chain, often before importation.85
This finding has been supported by analysis of seized street heroin, nearly half of which had not been cut at all86. Of those seizures that had been diluted, the most common diluent was paracetamol, closely followed by caffeine. These are used because they melt at a similar temperature to heroin. Caffeine actually helps to give a higher yield of heroin vapour than would be possible were it not present, acting like a flux to help the heroin vaporise87.
Recent seizures in Merseyside of paracetamol that had been baked in an oven to use as a cutting agent for heroin demonstrate that cutting does happen further down the supply chain.88
Average UK purity levels
According to the Institute for the Study of Drug Dependence89, average purity for different drugs in the UK in 1995 was as follows:
![]() Heroin 42.5%
Heroin 42.5%
![]() Cocaine 53%
Cocaine 53%
![]() Crack cocaine 80% plus
Crack cocaine 80% plus
![]() Amphetamine 10%.
Amphetamine 10%.
![]() Rather than long lists of things they should or should not do, drug injectors need information on how cross infection may occur, so that they can work out risks and ways of minimising it for themselves.
Rather than long lists of things they should or should not do, drug injectors need information on how cross infection may occur, so that they can work out risks and ways of minimising it for themselves.
![]() Workers need a good understanding of the injecting process so that they can discuss individual risks such as backloading, and offer advice.
Workers need a good understanding of the injecting process so that they can discuss individual risks such as backloading, and offer advice.
![]() Repeated exposure to 'low-risk events' such as sharing spoons, increases the likelihood of eventual infection.
Repeated exposure to 'low-risk events' such as sharing spoons, increases the likelihood of eventual infection.
![]() Spoons used for preparing injections should be marked for identification and kept for sole personal use in a place to which other injectors do not have access.
Spoons used for preparing injections should be marked for identification and kept for sole personal use in a place to which other injectors do not have access.
![]() Water drawn straight from the tap is better than bottled water and distilled water (even if it says 'pure water') which are likely to contain far more organisms.
Water drawn straight from the tap is better than bottled water and distilled water (even if it says 'pure water') which are likely to contain far more organisms.
![]() Of the injecting paraphernalia, it is probably hardest to discourage people from re-using filters. The fact that they represent a real risk of viral transmission means that users must be alerted to the dangers of sharing them.
Of the injecting paraphernalia, it is probably hardest to discourage people from re-using filters. The fact that they represent a real risk of viral transmission means that users must be alerted to the dangers of sharing them.
![]() Different drugs may present particular risks for injectors; they need to be given enough information about their drug of choice in order to minimise those risks.
Different drugs may present particular risks for injectors; they need to be given enough information about their drug of choice in order to minimise those risks.
Last Updated (Wednesday, 05 January 2011 23:38)