| Substance-specific
risks There are a number of risks of injecting which are unique to
particular substances and many that apply to some substances but not to others. These are
important areas of safer injecting information to be given to users and are now discussed
in detail.
Opiates
Heroin
Drug-specific risks of injecting street heroin are surprisingly few and include:
![bult57[1].gif (589 bytes)](../../../library/books/needle/bullet/bult57[1].gif) Overdose Overdose
Reactions to the
heroin or the 'cut'
Rarely, kidney damage.
The other risks such as transmission of viruses or bacteria are not confined to heroin
injecting. Other bodily reactions to opiates such as pinpoint pupils and constipation are
not dependent on injecting as the route of administration. The transmission of tetanus and
botulism has been associated with the use of 'black tar' heroin in the USA.
Oral methadone
There is clear anecdotal evidence that some people in the UK inject oral methadone
mixture 1mg/1mL, the psychoactive effect of which is likely to be minimal as even 10mg is
a very small dose for an opiate user with tolerance to the drug; and 10mLs is a large
amount of fluid to inject, especially as it is a thick, often sugary liquid.
The usual thick green syrup formulation is likely to cause slowing of the blood and
rapid vein collapse. This is an instance where, if harm reduction is the aim, there is
little that can be done to make the practice safe.
Workers should strongly discourage this practice. Attempts, such as those in Australia,
to make the practice safer by providing specific equipment are misguided as they are
unlikely to reduce drug-related harm.
In some centres people are prescribed methadone, usually for supervised consumption, in
a more concentrated
10mg/1mL form. Clearly if unsupervised this is more likely to be injected than 1mg/1mL.
In Australia, Darke et al.68 conducted one of the few studies of oral
methadone injectors.
The formulation of oral methadone in Australia (5mg/1mL) is more concentrated than that
usually available in the UK (1mg/1mL) and injectable preparations are not prescribed to
drug users.
Darke et al. observed in their study that injection of oral methadone was common
and was associated with more likelihood of:
Abscesses and
infections
Deep vein thrombosis
Heroin overdose
Poorer general health
Higher levels of
psychological distress.
Methadone ampoules
Approximately 10% of methadone prescriptions in the UK are for injectable methadone69,
which has been little researched.
The ampoules come in various strengths, the weakest of which is 10mg/ 1mL. The
strongest ş 50mg/1mL ş is only manufactured on the instructions of some doctors for
their patients.
There have been reports of significant injection site 'burning' and other damage from
the highly concentrated 50mg/1mL solution. As clients may be reluctant to show this damage
to their prescribing doctor for fear of 'losing their script', workers should be alert to
the problem.
The only things that can be done to reduce such damage are for clients to rotate sites
and/or ask their doctor for a less concentrated form, or to transfer to oral methadone
either on a temporary or permanent basis.
'Homebake'
'Homebake' is a phenomenon that appears to be limited to Australia and New Zealand. It
refers to the practice of using home chemistry to remove codeine from 'over the counter'
and 'prescription only' drugs, and subsequently converting the codeine to morphine and
then to heroin70 .
It seems to have arisen as a response to a lack of heroin in Australia in the early
1980s, probably as a result of effective enforcement of drug supply restrictions.
'Homebake' also sells more cheaply than alternatives such as heroin, which has helped
to maintain its presence in the Australian drug scene. The lack of consistency and
precision inherent in a home-produced drug means that the strength is often uncertain and
many of the agents or by-products of manufacture are left in the finished product. These
agents, such as chloroform, pyridine, hydrochloric acid and acetic acid may cause
significant damage.70
The use of homebake seems to be closely associated with localised injection related
damage, such as skin rashes and abscesses.
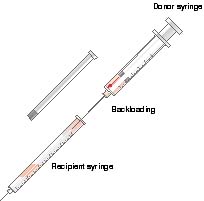
Perhaps the most worrying aspect of homebake use is that it has often been sold in
ready loaded syringes. Obviously, since the sterility of the syringes cannot be
guaranteed, this method of supply represents a considerable risk for transmission of
blood-borne viruses.
Kompot
Kompot is found in many parts of Central and Eastern Europe. It is made by various
methods which often involve boiling up poppy straw and distilling the residue until left
with a dark brown liquid.
It is very cheap to produce and buy, although it tends to be a seasonal product so the
price rises substantially in the winter.
The problems associated with the use of kompot are similar to those already described
for homebake. It is often sold in or from pre-loaded syringes, which brings with it an
increased risk of the spread of blood-borne viruses.
Stimulants
All stimulants have an effect of enhancing confidence and altering judgement about
risk. In circumstances where people are injecting while intoxicated they may be less
cautious about infection and other risks.
Workers can address this issue with people when they are not intoxicated, by helping
them to develop strategies for ensuring that they do not place themselves at risk when
they are intoxicated. An important factor is the necessity to have sufficient injecting
equipment for their needs: in some cases this may mean users taking large numbers of
syringes away from the needle exchange.
The use of considerable quantities of stimulants increases the likelihood of
development of psychosis71.
Amphetamine
After preparation on a spoon, the solution is usually drawn through a filter. Any
residue should be discarded or swallowed rather than injected.
King et al. studied the constituents of UK street amphetamine in 1993 and found
that the majority of amphetamine sulphate powder was of very low purity (on average about
5%). The bulk of the powder is probably made up of 'fillers' such as caffeine, dextrose
and other sugars. By comparing police and customs seizures they found that:
"...nearly all the amphetamine in the UK had been
imported from The Netherlands."72
The low purity may lead those who use amphetamine in quantity to become more likely to
inject it, in order to maximise the effect, and when they do, to inject large quantities.
In an Australian study of amphetamine users, Hall et al. found that injecting of
amphetamine was significantly related to the experience of hallucinations, violent
behaviour and paranoia71.
Amphetamine 'base' has become more widely available in the UK recently. This is usually
of greater purity than amphetamine powder. It is an irritant to the veins when injected.
Cocaine
Cocaine injecting is associated with higher rates of HIV infection than other drugs73
and with significantly more localised tissue damage than heroin injecting. There may be
several factors causing the tissue damage. Cocaine's duration of effect when injected is
very short and can be measured in minutes rather than hours. This means that cocaine
injecting is likely to be more frequent for those who use it as a primary drug. Also,
cocaine has been employed for centuries for its anaesthetic properties. Deadening of pain
at the injection site may lead the user to inadvertently cause more injury whilst
injecting. Cocaine has a constricting effect on peripheral blood vessels and therefore the
healing of injuries associated with cocaine injecting may be delayed74. It may
also be toxic to local blood vessels75.
Cocaine stimulates the cardiovascular system, raising the heart rate and blood
pressure, so users are at an increased risk of circulatory problems such as strokes or
heart attacks.
There is also an increased risk of seizures for cocaine users.
Drugs with local anaesthetic properties such as lidocaine may be used to adulterate
cocaine76.
Since cocaine injecting is likely to occur very frequently, this should be taken into
account when issuing injecting equipment.
Sedatives
Temazepam
Temazepam comes in several forms:
Tablets
Liquid-filled capsules
that are easily injectable ş the Home Office requested withdrawal of these capsules in
the late 1980s because they were beingwidely injected
Gel-filled capsules ş
introduced as a response to the problem of the injecting of liquid-filled capsules. Often
referred to as 'jellies' or Gelthix these were withdrawn from NHS prescription in 1996,
and are no longer manufactured in the UK, but may still be available occasionally on
thestreet
Elixir, which is in
liquid form and has a low concentration of temazepam.There are only occasional reports of
this being injected.
In a 1992 study, Ruben et al.77 found that reasons given for using
temazepam included:
The 'buzz' associated
with injecting
Its sedative/relaxing
effect
Increased confidence
when engaging in crime or prostitution
Self-medicating opiate
withdrawal
Heroin not available
Taking it with heroin
for the combined effect.
Because of the particular formulation, Temazepam, when injected, can cause severe
problems. It is highly irritant to the veins and when intoxicated, people can become very
reckless in their behaviour.
Temazepam injectors often quickly damage the peripheral veins in their arms and legs to
the point that they are no longer usable. This may lead them to look for alternative
deeper veins, often in the groin.
Gelthix temazepam causes particular problems because it is warmed to make it liquefy.
After injection it cools in the body and resolidifies, leading to vein blockage.
Injecting temazepam into the femoral vein increases the likelihood of deep vein
thrombosis in the legs. Other problems associated with injecting temazepam include:
Accidental injection
into an artery
Irritation of blood
vessels
Irritation/infection
of tissues at the injecting site.
Arterial injection of temazepam will often lead to amputation of the whole or part of a
limb.
The following experience of a vascular surgery unit is not unusual, or confined to
Merseyside.
"Of particular concern recently in the Merseyside area is
the increasing prevalence of disastrous complications arising from the intra-arterial
injection of soluble temazepam..."78
This report written in 1993 resulted from the admission of 11 injectors with
complications from arterial injection of temazepam within a six-month period. More
worryingly, this report noted that although six of the 11 had apparently injected into the
femoral artery by mistake, five had apparently injected into the radial artery in the arm,
because of mistaken instruction from their peers! In all of these five cases this resulted
in varying degrees of gangrene in the fingers.
Barbiturates
Barbiturates are now rarely injected in the UK. This mirrors the decline in general
prescribing of barbiturates. Their place in medicine began to be taken by benzodiazepines
in the 1960s.
Injecting injuries associated with barbiturates are similar to those found with
benzodiazepines, except that there tends to be more local tissue damage when injected
subcutaneously; tissue dies and sloughs off around the injecting site. Older textbooks
refer to these injuries as 'barb burns'.
Barbiturates are also associated with a high overdose risk, especially when used in
combination with other drugs. Withdrawal from dependent use can cause seizures which can
be fatal.
Alcohol
The injecting of alcohol seems to be something that occurs occasionally, either as an
experiment or as a feature of chaotic, compulsive drug use. The substance injected is
usually a spirit such as vodka. Alcohol injected intravenously is highly irritant to the
veins and has little psychoactive effect, except in volumes that will cause great damage. |