| 59.5% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 137 |
| Yesterday: | 251 |
| This Week: | 137 |
| Last Week: | 2221 |
| This Month: | 4725 |
| Last Month: | 6796 |
| Total: | 129324 |
 |
|  |
| 
| Articles - Khat |
Drug Abuse
A harm reduction approach to khat chewing based on development work with the Somali communities in the UK
Ahmed Suleman Omar/Kujog 1997
HISTORY OF KHAT
Khat is a plant or shrub which grows wild and is cultivated commercially on the hillsides of East Africa and Yemen. It was highlighted in an Arab manuscript in 1333 and sometimes is considered a possible cure to a range of diseases. It is generally accepted that the habit of khat chewing originated from the Yemen, travelled to the ancient Islamic city of Harar in Northern Ethiopia during the early days of Islam and gradually spread to the neighbouring countries of East Africa.
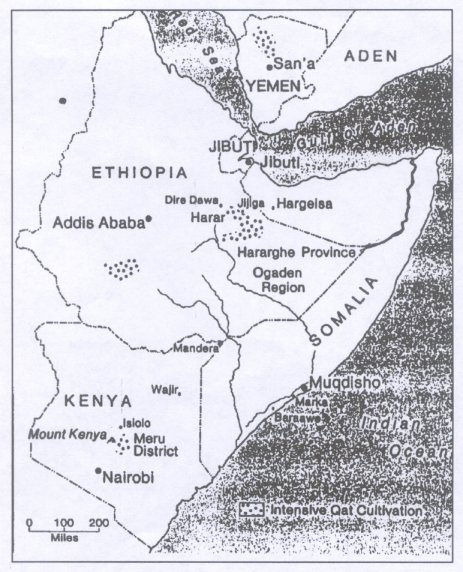
AREAS OF PRODUCTION
The major centres of khat production have always been highland areas which are often associated with the production of coffee. Khat is grown in eastern and northern Ethiopia, the hills on the north east of Kenya and the mountains of the Yemen. Smaller khat plantations exist in neighbouring Somaliland, Tanzania, Madagascar and Uganda. Presently, Ethiopia and Kenya remain the principle suppliers of khat.
PATTERNS OF KHAT USE
The habit of khat chewing is generally confined to the Muslim communities within countries of common use and to settler or refugee communities from these populations elsewhere in the world. With the exception of a small percentage of East African Asians, khat chewing rarely attracts other communities in any part of the world, despite its long history of use, and widespread dissemination across the globe following arrivals of refugees in Europe, the Middle East, USA and Canada mostly from East Africa during the early and late 1980s. With the establishment of large refugee and settler communities, who brought with them the social habit of khat chewing, secure markets were established for the khat suppliers from Kenya and Ethiopia.
THE USE OF KHAT
Khat is chewed and its juice is swallowed for its stimulating and reinforcing qualities. The active substance is best obtained from the youngest and freshest leaves and shoots. The active agent is cathinone (CTN) which chemically bears a close resemblance to amphetamine (APA). Cathinone affects the central nervous system but it remains difficult to determine the acute effect of khat use quantatively. Certainly environmental factors play a major role in its subsequent affects. The alkaloid contents of the leaves vary over a wide range and there are certainly individual differences in mastication efficiency and thus the absorbtion of the alkaloids.
TRADITIONAL PATTERNS OF USE
Khat chewing is not frequently used but is generally practised in a group, generally of adult males, led by guest where socialization develop with members of that community who often discuss topics of interest, listen to local music or poetry and solve individual or group disputes or conflicts. Drinks, mainly water, black tea and coca cola are often served during the session.
Khat sessions known as MAJLIS had their own traditional rules and social ethics (i.e time of use, duration of the session, style of use, age group, quantity of use and self discipline with the session members). It was a social and relaxing event after long hours of hard work.
Because of existing cultural and religious barriers, these communities are not able to access other social events enjoyed by non Muslim communities. Therefore, khat use is seen as the only acceptable socialising entertainment available to them.
EXCESSIVE PATTERN OF USE
Elderly khat users still adhere and observe these traditional patterns in the UK. New trends and patterns of excessive khat use are developing among younger people. These new trends have been identified within the countries of common use and beyond their borders as well.
To cope with their deepening social problems (i.e. unemployment, poor housing, racism affects of the civil war, cultural alienation etc.) a number of young khat users have been exposed to the probable risks of excessive khat chewing. In these situations, young people chew on a regular basis, for extended periods with khat use becoming part of a sense of exclusive, inactivity, boredom and despair. Living under similar social conditions a number of Somali women have developed the habit of khat chewing. Chewing more than two sessions a week, late night sessions, chewing in congested environments and lack of essential diets are all recognised as excessive use.
HEALTH RISKS
Khat chewing is not physically or mentally addictive, but however excessive and prolonged khat use could lead to serious health risks (i.e oral cancer, dental problems, acute constipation and loss of sexual drive in men). Acute loss of appetite, lack of ample rest and lack of regular exercise could also lead to much more serious consequences. In addition to the direct health risks a number of environmental[ issues or co-factors also exist. Drinking coffee and coca cola increases the intake of stimulants increasing the heart rate. As the stimulant effect of khat reduces the body temperature, windows are often kept closed. The effects of heavy smoking are compounded by passive smoking. As with other stimulants, chewers may use sleeping pills or sometimes alcohol to help sleep at the end of a session.
STRATEGIC HARM REDUCTION RESPONSE
Considering the social cultural role of khat use among the Somalis in the UK as well as the underlying socio--economic factors of massive unemployment, cultural alienation, effects of the civil war etc, any measures of legal restrictions are seemingly inappropriate as this might trigger escalated illicit drug use among this community.
Two measures of a strategic harm reduction response are considered most appropriate and positive: -
a) Addressing the underlying social problems of unemployment, poor housing, cultural alienation and to promote positive measures of community development.
b) To develop a health education response and raise awareness (i.e. publication of health guidelines, leaflets, peer support).
HEALTH GUIDELINES FOR KHAT CHEWERS
Through a community development approach with the Somali community the following advice has been developed and disseminated through khat chewing sessions.
Recommended health guidelines and advice:
1. the safest way to avoid any probable health risks of excessive khat use, is to avoid chewing;
2. try to reduce your quantity of khat use with reasonable intervals between sessions;
3. use less coke and black tea. Milk and ordinary clean water are positive substitutes;
4. limit your smoking (if you smoke). Avoid crowded sessions. Keep windows open to allow sufficient oxygen into your room;
5. eat balanced diet before and after your session. Avoid late night sessions
6. always clean your teeth after your khat session. Use regular mouth wash to reduce risks of oral infection;
7. avoid taking other drugs or alcohol during or after your khat session. Mixing drugs is highly dangerous;
8. never take sleeping pills to help you sleep unless prescribed by your doctor;
9. sit in a comfortable and relaxing position;
10. take regular exercises. 30 minutes of vigourous walking per day could contribute a lot to your health;
11. holding the chewing material in your cheek for a long time, might increase risks of oral infection.
12. Avoid khat chewing during period of pregnancy. This might lead to serious health risks to the baby.
This advice is available in a leaflet currently available in Somali but currently being translated into English and Arabic.
CONCLUSION
Khat is a drug which forms a cultural role within the Somali communities in the UK. Traditionally this has been a positive role. Excessive patterns of use reflects pressure on the community. Work to improve the situation of the Somali community is recommended along with health promotion advice delivered through khat chewing sessions.