| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 166 |
| Yesterday: | 251 |
| This Week: | 166 |
| Last Week: | 2221 |
| This Month: | 4754 |
| Last Month: | 6796 |
| Total: | 129353 |
 |
|  |
| 
| Articles - HIV/AIDS & HCV |
Drug Abuse
Fellow travellers: the narcotraffic and AIDS
by Pierre-Arnaud Chouvy
The starting-point of the alarming spread of AIDS in Asia was the spread of injecting drug use. These patterns are closely correlated with the heroin trafficking routes.
After sub-Saharan Africa, Asia is the continent which has been most severely hit by the epidemic of HIV and AIDS up to the year 2001. The total number of people contaminated in Asia has been estimated by UNAIDS to amount to 7.2 million people in all.
HOW TRADITIONAL IS OPIUM IN ASIA?
The consumption, of opium in Asia is not actually as traditional as one might imagine. It has been established that the cultivation of the opium poppy was imposed on Imperial China at the start by the British in the 19th Century, and that opium production also began in southeast Asia around that time, when the part of the population of southern China was forced to migrate to the northern highlands of Indochina.
As studies on the Mon societies-have-shown, the consumption of opium in the area now known as the Golden Triangle probably dates back no farther than the beginning of the 19th century. Burma is a typical example of this historical process, since the first legal references to opium, which is not mentioned in any of the religious texts, did not appear in print until the early 19th Century, when the British promoted the use of opium.
China used to be the country with the largest number of opium addicts in the world before the Communists carried out their large-scale detox and eradication programmes from 1949 onwards, but if one looks back at several thousand years of Chinese history, the so-called "tradition" of opium addiction was not actually all that strong. The only "traditional" aspect to have survived in Communist China was the use of poppy seeds in cooking, which has now been forbidden since 1991.
India is probably home to the most traditional habits of opium use, together perhaps with Iran, where this drug plays a role in some important social customs.
To the West, the only part of Afghanistan where opium consumption has been traditional is Badakhshan, in the north-east, and the country's present production certainly does not constitute the perpetuation of a long Afghan tradition. This situation is quite different from that which characterised neighbouring Persia, where opium was grown for a long time, and Iran, where some opium-growing has subsisted up to the present day.
Central Asia does have a tradition of opiate consumption. Koknar, a decoction made from poppy stalks, is widely consumed throughout central Asia where most family vegetable patches contain a few square feet of cultivated poppies. But here again, in the immense majority of cases, it is not opium which is used as an ingredient in the local recipes, but only poppy stalk juice. The parts of Asia which are witnessing an explosion in the consumption of opium and above all heroin nowadays are therefore involved in a perfectly new process, which is far removed from the traditions which the countries in question may have adopted in the course of their respective histories. The road from poppy stalk juice to heroin is long and devoid of all tradition.
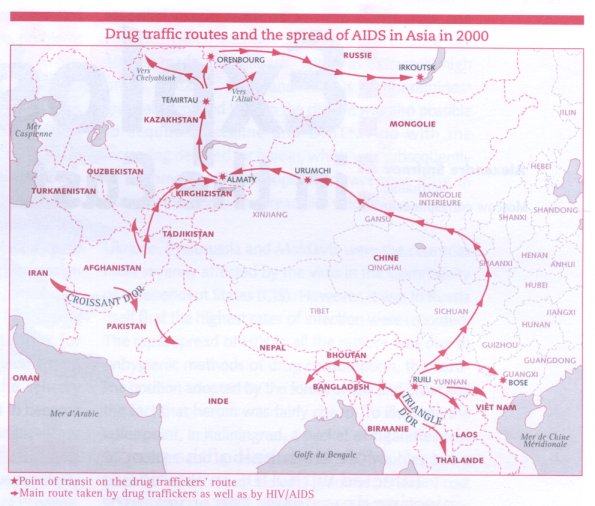
The most distinctive feature of the propagation of HIV and AIDS in Asia is the fact that injecting drug users (IDUs) seem to have been the starting-point of the pandemic*, and that this must be closely correlated with the presence on the Asian continent of the two largest illicit opiate* growing areas in the world. Although the drug consumers inhabiting the drug-producing areas were the first to be contaminated, heroin addiction has spread widely along the narcotrafficking routes, and the spread of HIV/AIDS also shows a similar pattern.
Although the AIDS epidemic arrived relatively late in Asia, where the first cases occurred in 1988, it literally rocketed in 1999, when a fifth of the current total number of infections were contracted. The CIS (1) now has the most rapid rate of contamination in the world and the statistics from Russia, for example, show that 70% of all cases of infection detected between 1985 and 1999 were diagnosed in 1999 alone: the eastern part of the Federation is particularly severely affected (2).
95% of the world's illicit opiate production is concentrated in the areas known as the Golden Triangle and the Golden Crescent, which overlap the contiguous frontier regions of Burma, Laos and Thailand and those of Afghanistan, Iran and Pakistan, respectively. The existence of these drug-producing areas has contributed during the last few decades to the considerable increase in the consumption of opiates among the respective populations, and this increase is spreading to those inhabiting neighbouring regions and places even further afield.
The outbreak of the HIV/AIDS epidemic in Asia between 1988 and 1990 coincided with the multiplication of the Asian drug trafficking routes and their re-orientation towards the north, as well as with the spread of heroin addiction throughout the Asian continent. Before 1990, heroin from the Golden Triangle and the Golden Crescent was almost invariably transported via the southern routes, until the traffic was suddenly re-oriented towards China, Central Asia and Russia when borders were opened and trading and customs agreements signed at the end of the Cold War: this enabled the narcotraffickers to diversify their shipping routes.
In Asian countries, a correlation can be seen to exist, in both time and space, between the spread of opiate trafficking, the increase in opiate consumption and the explosion, only slightly later, of the HIV/AIDS epidemic (3). China and Russia are extremely telling examples showing how the outburst of drug trafficking heroin addiction and the HIV/AIDS epidemic all tended to occur at practically the same time. The existence of a narcotrafficking route can indeed be inferred from the sharp, significant increase in the number of heroin addicts which occurred along it and the subsequent increase in the HIV infection rates.
On the Burmese frontier, for example, the province of Yunnan is the first stop on the Chinese side of the border.This point on the new narcotrafficking route was, significantly, home to 80% of all China's HIV-positive individuals in 1990 (4).The area is awash with Burmese heroin, which pours in via Chinese towns such as Ruili, where two thirds of the IDUs are HIV positive, as in Guangxi, the next stop on the traffickers' route (5). The correspondence which can be observed in Yunnan, for example, between the development of the heroin traffic, the emergence of intravenous injection, which is becoming the main mode of heroin consumption, and the near-simultaneous waves of heroin addiction and HIV/AIDS infection which have ensued is now particularly obvious all over Asia. A similar process occurred in north-east India, which is crossed by the routes along which increasingly large quantities of Burmese heroin are transported. Manipur, where 80% of all the heroin addicts are infected with HIV, is now the Indian state with the largest epidemic of HIV/AIDS: the disease which began to spread at a particularly fast rate after the bi-lateral Indo-Burman border agreement came into effect (6).
As far as Central Asia is concerned, this region is involved in around 65% of all the narcotraffic originating from Afghanistan, according to the UNDCP: heroin consumption has rocketed here since the start of the 1990's, and the HIV/AIDS epidemic has also broken loose. In Tadjikistan, for instance, the number of opiate users is thought to have increased by 50% between 1998 and 1999, while the drug traffic increased by 250%. And on the borders of Central Asia, the Chinese province of Xinjiang, where not a single case of HIV infection was recorded before 1995, the same pattern can again be detected: the epidemic hit 25% of all the drug addicts back in 1996 (7). Xinjiang is supplied with Burmese heroin, which travels from here to Kazakhstan: the capital Almaata recently saw an upturn in the HIV/AIDS epidemic, involving viral strains of the south-east Asian variety. This fact has enabled the experts to determine the origin of the drugs involved and to trace narcotics supply routes, the existence of which was hitherto unsuspected. Significantly, the viral strains in question are the same as those to be found in the towns of Ruili and Bose, on the road to Chinese taken by the Burmese heroin dealers.
Drug consumers are all potential petty dealers.
The spread of the epidemic to Kazakhstan from Urumchi in Xinjiang was predicted by Dr.C. Beyer, based on the results of an epidemiological study in which he established the existence of a significant correlation between the heroin trafficking routes and the spread of the HIV/AIDS epidemic due to the increase in intravenous drug consumption: "In every market town along a drug trafficking route, there are new outbreaks of drug use... Overland routes involve local people, highway travellers and local traders, and these people carry the AIDS epidemic to India, China and Vietnam" (8).
For similar reasons to those pertaining in south-east Asia and in China, heroin from Afghanistan has recently and increasingly begun heading for Russia, once again via Kazakhstan, which lies on the narcotrafficking routes. This has favoured an almost parallel upturn in opiate consumption and the spread of HIV/AIDS. At Temirtau, for example, which is the Kazakh town most severely affected by the HIV epidemic, and one of the main stops on the narcotraffickers' route, although the first case of HIV was reported as recently as 1996, one inhabitant in ten is now thought to be an IDU (9). Meanwhile in Russia, the oblasts of Chelyabinsk and Orenburg and the Altai region, which are the main entry points into the country for the Afghan heroin imported from neighbouring Kazakhstan, have shown a noticeable increase in heroin addiction and in the spread of HIV/AIDS since the late 1990s.
In the same way, the Afghan heroin introduced into Russia mainly by Tadjik traffickers had only reached the Irkutsk region in Eastern Siberia, which is very far from the Golden Crescent, at the start of 1999; just a few months later, however, the first cases of HIV were reported. Opium, which had already been in use there for a number of years was being swiftly and suddenly supplanted by heroin. Since the latter is mostly injected intravenously using shared needles, it soon became the main vector responsible for transmitting HIV/AIDS. In Russia, heroin consumption literally sky-rocketed in the course of 1999, increasing four and a half fold between June-July 1998 and the same period in 1999, while the number of HIV infections recorded doubled in 1999, mainly due t intravenous drug use. However, it has been estimated that the sudden massive increase in heroin addiction and in the incidence o HIV/AIDS in the oblast of Irkutsk, which has by now been deeply penetrated by the Tadjik trafficking networks, is probably one of the most serious examples of this process in the whole of Russia.
The rapid spread of heroin consumption i the countries crossed by the expanding narcotrafficking routes is a new and damaging process. At first, the traffickers begin transporting opiates along the main lines of communication, which quickly become new narcotrafficking routes. As they go, they lead to the consumption of opium and heroin, which become widely adopted by the population in these regions, and addictive practices soon take root. The traffic then tends to increase in volume and propagates all the more readily since the countries along the drug route have growing numbers of consumers, who are also potential small-time smugglers. The development of complex distribution networks and the extension and multiplication of the trafficking routes together quickly result in the emergence of a population of IDUs, and these conditions all favour the fast spread of HIV.
If one considers the enormous potential which narcotrafficking has to create new drug markets which will then sustain the production and flow of heroin, one can grasp the huge scale on which the AIDS pandemic* is liable to develop in the years to come in some parts of Asia and the rest of the world, where economic inequality is on the increase and where prostitution is rife. One has only to realize that the number of countries around the world where the IDUs have become contaminated with HIV has increased by 40% between 1996 and 1998 (10).The upsurge of heroin addiction and the raging HIV pandemic which have accompanied the development of the drug trafficking routes constitute one of the main challenges now facing Asia at the dawn of the 21 st century.
1 *Commonwealth of Independent States.
2.Beyrer C., 00, Accelerating and Disseminating Across Asia, The Washington Quarterly, Winter 2001, Vol. 24 N° 1, pp. 211-225.
3•This correspondence is partly attributable to an increasingly common practice among the petty user/traffickers, which consists of testing the heroin they intend to sell by injecting themselves. This occurs frequently in Vietnam and China as well as in Manipur.: Beyrer C et al., 2000, Op. cit.
4•BBC, Aids spreads in China, 14-07-00 ; Associated Press, AIDS Cases Rise in China, 29-03-00.
5•SAIN, 1998, Op. cit.
6•Central Asia- Caucasus Analyst Forum Summary, Drugs, A Threat to Central Asian Security, 15-03-00, Central Asia -Caucasus Institute, Washington, John Hopkins University.
7•in Central Asia - Caucasus Analyst, 05-07-00.
8 *Washington Post, AIDS Outbreaks Follow Asia's heroin Traffic, 06-03-00 ; BBC, 1000 HIV cases in Kazakhstan, 30-11-99 ; Beyrer C. et al., 2000, Op. cit.
9•BBCU, Central Asia's battle with drugs, 11-11-99.
10•UNAIDS - UNDCP, 1999, Drug Abuse - HIVAIDS, A devastating combination, Geneva, UNAIDSUNDCP.
Source: PEDDRO december 2001